Back to Journals » International Medical Case Reports Journal » Volume 15
Necrotizing Fasciitis: A Side Effect of Rituximab Administration in Steroid-Dependent Nephrotic Syndrome
Authors Safdar OY ![]() , Basunbul LI, Alhazmi LS, Almughamisi SA, Habib LA, Basaeed AJ, Kalaktawi NM, Alharithi ET, Aljaaly HA, Alzahrani WA
, Basunbul LI, Alhazmi LS, Almughamisi SA, Habib LA, Basaeed AJ, Kalaktawi NM, Alharithi ET, Aljaaly HA, Alzahrani WA
Received 9 December 2021
Accepted for publication 17 September 2022
Published 18 October 2022 Volume 2022:15 Pages 587—592
DOI https://doi.org/10.2147/IMCRJ.S347389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Osama Yousif Safdar,1 Lama Islem Basunbul,2 Lenah Sulaiman Alhazmi,2 Shahad Amro Almughamisi,2 Laura Ahmed Habib,2 Amani Jamaan Basaeed,2 Nada M Kalaktawi,1 Elaf Turki Alharithi,2 Hataan A Aljaaly,3 Walaa A Alzahrani2
1Pediatric Nephrology Department, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 2Pediatric Department, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 3Plastic Surgery Department, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Correspondence: Walaa A Alzahrani, Pediatric Department, King Abdulaziz University Hospital, Jeddah, Saudi Arabia, Tel +966 546239898, Email [email protected]
Abstract: Steroid-dependent nephrotic syndrome (SDNS) is a common type of childhood nephrotic syndrome. Remission following steroid therapy is achieved in 80– 90% of the patients, while the remainder show steroid-resistant nephrotic syndrome (SRNS). Rituximab is an anti-CD20 chimeric monoclonal antibody with proven therapeutic effects in several diseases and has been used with great success in the treatment of NS since its discovery. We report a case of a 4-year-old girl diagnosed with SDNS at the age of 3. As treatment with steroids, enalapril, and mycophenolate failed to produce complete remission, rituximab was initiated, and remission was successfully achieved after administration of the first dose. Due to this response, rituximab therapy was continued; however, a day after being admitted to the nephrology ward for the second dose, she started to develop a high fever, which reached up to 40°C. In addition, she also displayed symptoms of upper respiratory tract infection and an ulcerated wound on her left cheek. The patient became drowsy with reactive pupils, cold peripheries, and weak peripheral pulses. The capillary refill time was prolonged to 3– 4 seconds and it was decided to withhold the second dose of rituximab. The patient was shifted to the PICU as a case of septic shock secondary to facial cellulitis and started on inotropes (epinephrine and norepinephrine), meropenem, vancomycin, and hydrocortisone 15 mg. Thereafter, surgical debridement of the wound was carried out. The patient remained in remission with regard to nephrotic syndrome and was discharged in a healthy condition. In conclusion, rituximab used in conjunction with steroids and other immunosuppressants may increase the risk of serious infections like necrotizing fasciitis (NF). Further studies are needed to explore the relationship between rituximab and NF.
Keywords: pediatric, steroid-dependent, steroid-resistant, remission, adverse reaction
Introduction
Childhood nephrotic syndrome (NS) is a challenging condition for pediatric patients. Although the exact pathology leading to disturbance of the glomerular filtration barrier and proteinuria is still unknown, this disorder remains the most common chronic glomerular disease found in children.1,2 It affects approximately 2–16.9 per 100,000 children worldwide, with great variability in the incidence rates among different races.1,3,4
In addition to the symptomatic care, corticosteroids have been the mainstay of treatment for idiopathic NS (INS) for decades. The majority of INS cases are steroid sensitive with a good clinical outcome, which is defined as complete resolution of proteinuria with daily prednisone administration (2 mg/kg/day or 60 mg/m2/day, maximum = 60 mg/d for 6 weeks). Only 10–15% of the NS cases do not show remission with steroid therapy and are said to be steroid-resistant nephrotic syndrome (SRNS).5
If a patient with steroid-sensitive nephrotic syndrome presents with frequent relapses, the condition is known as frequent relapsing nephrotic syndrome (FRNS) and is defined as at least four relapses per year or at least two relapses within 6 months of initial presentation. On the other hand if the patient shows two consecutive relapses during steroid tapering or within 14 days of therapy cessation, the condition is called as steroid-dependent nephrotic syndrome (SDNS). In such cases, second-line steroid-sparing immunosuppressants are indicated for treatment, including antiproliferative agents, levamisole, calcineurin inhibitors, mycophenolate mofetil, and rituximab.5,6
Rituximab is a promising new agent that has shown proven clinically efficacy in treatment of FRNS/SDNS and refractory SRNS.7 It is a monoclonal antibody directed against the B lymphocyte CD20 marker, which induces depletion of B cells.5 Due to its mechanism of action, it has been mainly used in the treatment of B cell non-Hodgkin’s lymphoma; however, it has also shown great benefits in the treatment of numerous chronic conditions affecting the kidney, such as lupus nephritis, Wegener’s granulomatosis, rheumatoid arthritis, and microscopic polyangiitis.2,5 Although rituximab is generally considered to be a well-tolerated drug that is relatively safe, multiple serious adverse events have been reported to be associated with its use in children with complicated FRNS/SDNS. These include pulmonary fibrosis,8 fulminant myocarditis,9 pneumocystis pneumonia,10 immune-mediated ulcerative colitis,11 agranulocytosis,12 and superimposed infection, which still remains the leading cause of death after initiation of rituximab therapy.13
It is well known that infection is a chief complication of NS due to numerous factors, including hypogammaglobinemia, interstitial edema, disturbance of humoral immunity, and chronic use of steroids and other immunosuppressive medications. Peritonitis, cellulitis, and sepsis due to Streptococcus pneumoniae and Haemophilus influenzae are common infections associated with this disease.14
However, deep soft tissue infection in nephrotic syndrome, such as necrotizing fasciitis (NF), is a very rare and unlikely complication and very few cases of NF associated with NS have been reported in the English literature to date. NF is a fatal and serious condition that requires a prompt and effective management to minimize associated morbidity and mortality.15–19 Furthermore, some cases of NF as a side effect of rituximab therapy have been reported previously. It is agreed that further studies are required to investigate the link between rituximab therapy in nephrotic syndrome and NF.20–23
After obtaining Informed written consent from the parents of the patient for the publication of the case report. Here we present a case of a 4-year-old girl with SDNS, who started to develop septic shock secondary to NF after receiving the first dose of rituximab therapy. This adverse reaction was thought to be a side effect of rituximab.
Case Presentation
A 4-year-old Saudi girl was diagnosed with nephrotic syndrome when she was 3 years old. As she suffered from frequent relapses post diagnosis, she was labelled as SDNS. Thereafter, she was put on mycophenolate mofetil 180 mg twice daily, prednisolone 36 mg on every alternate day and enalapril 1.4 mg once daily. However, with this regimen, she failed to achieve full remission, and to avoid steroid toxicity by increasing the steroid dosage, we decided to add rituximab to the regimen. Rituximab is administered intravenously and is known to be well tolerated by most patients with SDNS. After receiving the first dose of rituximab (dose: 375 mg/m2) the patient achieved full remission, with negative proteinuria. B-cell analysis following therapy revealed about 0.03% cells that were positive for CD22 and CD24 and negative for CD19 and CD20. Patient’s immunoglobulin (Ig) G level was also measured and was found to be low (2.02 g/L). Two weeks after the first rituximab dose, we admitted her electively for the second dose; however, the day after admission, the patient developed a high-grade fever (40°C), in conjunction with neutropenia, signs of upper respiratory tract infection, and an ulcerated wound on the left cheek measuring 2×3 cm with red margins and necrotic tissue in its center.
The patient was drowsy and exhibited reactive pupils, cold peripheries and weak peripheral pulses with a capillary refill of 3 seconds. Her vitals were as follows: temperature: 39.3°C; heart rate: 180 beats per minute; and blood pressure: 65/35 mmHg. O2 saturation on non-rebreathing mask was measured at 87% in room air.
The patient was administered 40 mL/kg normal saline as a bolus, but it failed to improve her blood pressure, and the systolic blood pressure remained in the range of 60–70 mmHg. Broad-spectrum antibiotics (piperacillin-tazobactam) were initiated to control the infection, and the patient was admitted to the PICU with the diagnosis of septic shock secondary to facial cellulitis. Epinephrine and norepinephrine, along with meropenem, vancomycin, and 15 mg hydrocortisone, were administered to counter the shock; however, keeping in mind the severity of her condition, we did not start the second dose of rituximab and also put mycophenolate mofetil administration on hold.
Computed tomography images revealed inflammatory changes in the left cheek and buccal space with fat stranding and soft tissue thickening, suggestive of cellulitis. Culture of the swab taken from the cheek cellulitis revealed the presence of Pseudomonas aeruginosa; but the blood culture and urine culture returned negative.
Debridement of the facial wound was performed, followed by re-debridement and closure with a local flap. Laboratory findings of the tests conducted during fever are presented in Table 1. After surgical debridement and a cumulative stay of 10 days in the PICU, the fever subsided and patient’s status improved. She was then shifted to the pediatric ward, where she stayed for a total of 4 days before being discharged. No relapse was seen with regard to nephrotic syndrome during her PICU and pediatric ward stay as evidenced by persistently negative urine dipstick test for proteinuria. The patient was discharged from the hospital in a good state and was put on prednisolone 25 mg and prophylactic antibiotic.
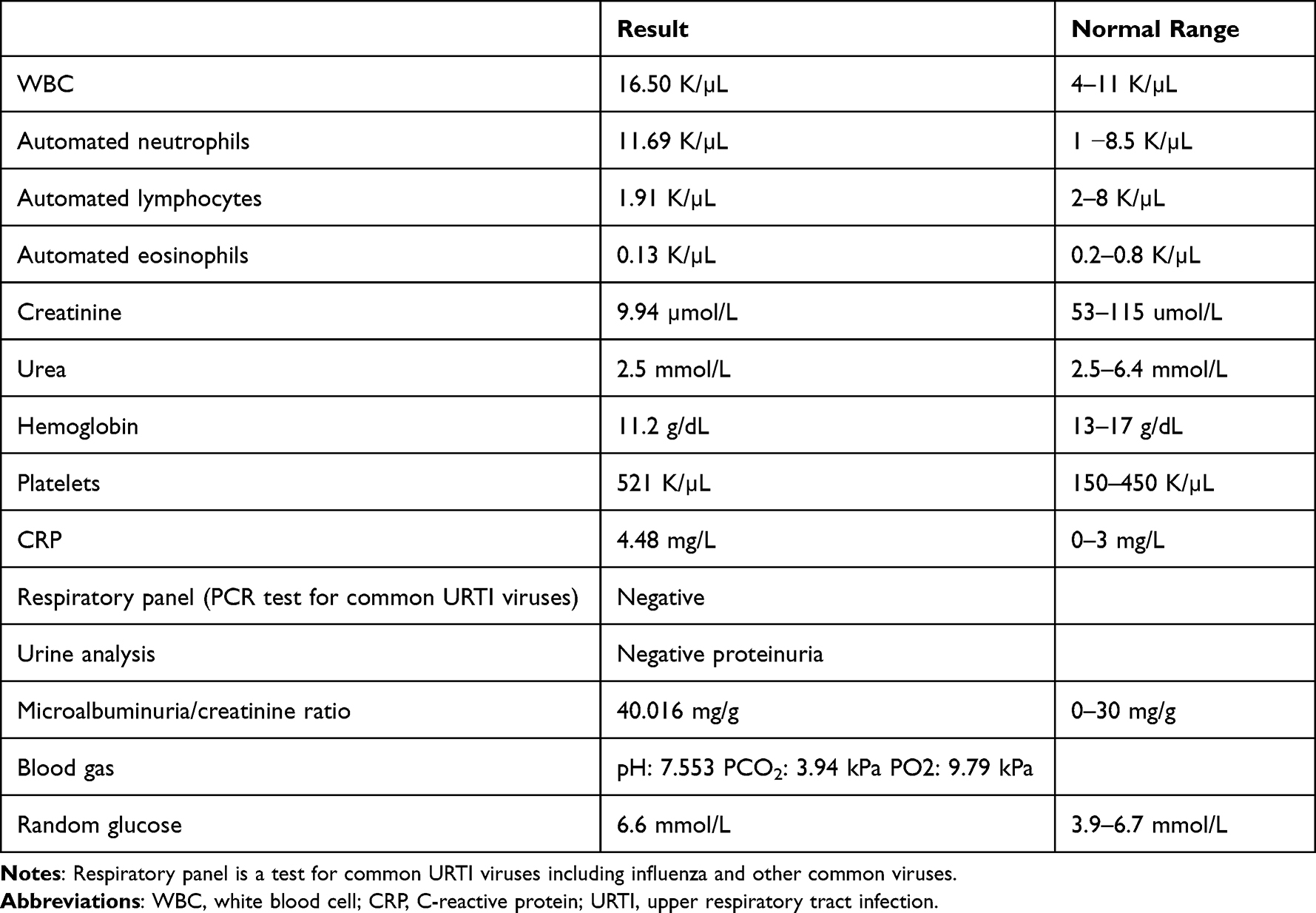 |
Table 1 Laboratory Test Results During the Febrile Episode |
Discussion
NS is diagnosed by massive proteinuria (greater than 40 mg/m2/hour) and a triad of clinical findings associated with large urinary protein loss, including edema, hypoalbuminemia, and hyperlipidemia.24,25 SDNS is a common type of NS diagnosed during childhood.26 Approximately 80–90% of the children can achieve remission with steroid therapy, while the remainder develop SRNS.27
Rituximab is an anti-CD20 chimeric monoclonal antibody with substantial therapeutic efficacy. Since its discovery, rituximab has been used with great success, primarily in the treatment of hematological malignancies.28 This success has led to the expansion of its use in other conditions, such as refractory rheumatoid arthritis that does not respond to one or more classes of medications (including anti-TNFs), certain vasculitides, such as granulomatosis with polyangiitis, and even systemic lupus erythematosus.29–31 In case of SDNS, rituximab is used as a steroid-sparing agent, resulting in a longer remission period. In a prospective observational study conducted in Shanghai, rituximab was found to be effective in treating 91.67% of the children with refractory nephrotic syndrome, albeit with some side effects, such as skin rashes, hypotension, and fever.32 Another multicenter, double-blind, randomized, placebo-controlled trial on the use of rituximab in pediatric-onset, complicated, frequently relapsing SDNS concluded that there was no noticeable difference in the incidence of infections necessitating treatment between the placebo and rituximab treatment arms. Nonetheless, during the B-cell depletion period (post-rituximab infusion), the rate of infections that required intervention was higher in the treatment group than in the placebo group.33
At the cellular level, rituximab use has been associated with a decrease in the B-cell count and serum Ig levels. The number of circulating B cells reportedly returns to normal 4.4 months after a single dose of rituximab, and the use of multiple doses of rituximab has been suggested to result in a prolonged depletion of B cells.32 Low B-cell numbers and serum Ig levels leave the treated subject vulnerable to infections such as upper respiratory tract infections and pneumonia.32 Pneumocystis jirovecii is an infectious pathogen that has been linked to rituximab treatment-related pneumonia. A previous case report has stated that one of the major risk factors for this infection is corticosteroid use.34 The reactivation of hepatitis B virus (HBV) has also been linked to rituximab treatment. Thus, screening of all patients receiving rituximab for HBV is strongly recommended.34 Studies have also shown that rituximab treatment is associated with serious viral infection caused by the John Cunningham virus, which leads to progressive multifocal leukoencephalopathy, a lethal demyelinating disease of the brain. Although this disease is rare, the increase in its incidence following rituximab treatment, as reported in several studies, resulted in a MedWatch alert by the FDA, a black box warning, and a letter from the manufacturer to physicians using rituximab.34
Other grade 3–4 adverse events associated with rituximab treatment include hypoproteinemia, lymphocytopenia, and neutropenia. Pulmonary fibrosis in one case8 and fulminant viral myocarditis in another9 have been reported as other fatal side effects.
NF after rituximab treatment is rare. Nonetheless, several studies have reported such cases. One such study reported a case of a 69-year-old man with chronic lymphocytic leukemia (CLL), who was initially treated with six cycles of bendamustine and rituximab, after which he was in complete remission. Eight years later, he was re-treated with a 4-week course of rituximab for CLL relapse, which resulted in the development of Clostridium septicemia, manifesting as NF and requiring amputation.20
Another study that further highlighted the association between rituximab and NF was a case of a 76-year-old man who was diagnosed with Waldenström macroglobulinemia on the basis of elevated serum levels of IgM (1944 mg/dL) and relevant findings on bone marrow biopsy. Chemotherapy with bortezomib, dexamethasone, and rituximab was initiated for rapid disease control, resulting in reduced IgM levels. After treatment, the patient complained of severe pain and swelling in his right thigh in the absence of a visible wound. The white blood cell count was 15.0 × 109/L with a predominance of neutrophils. Two sets of blood culture samples were taken and a fascia biopsy was performed from the right thigh by an orthopedic surgeon. Pathological examination revealed neutrophilic infiltration and the presence of multiple gram-negative rods, which morphologically resembled Enterobacteriaceae.21
According to the Cancer Research and Treatment Center of the University of New Mexico for Health Sciences, two out of 20 patients with non-Hodgkin’s lymphoma who received rituximab as part of their chemotherapy regimen developed NF. The first case was of a 48-year-old female diagnosed with recurrent follicular B-cell non-Hodgkin’s lymphoma. The patient was initially treated with chemotherapy alone. Five years later, the patient relapsed and was treated with chemotherapy combined with corticosteroids. Subsequently, she received four weekly rituximab infusions. One month after therapy completion, the patient developed NF in the left lower extremity. P. aeruginosa was isolated from the wound and identified as the causative agent.22 Similarly, in our case, the patient was steroid-dependent and underwent treatment with rituximab, which was complicated by NF caused by the P. aeruginosa. The second case was of a 59-year-old man who had a recurrence of follicular B-cell non-Hodgkin’s lymphoma 1 year after undergoing remission following mono-chemotherapy. During relapse, the patient received rituximab as part of his chemotherapeutic regimen. Following the administration of only three weekly doses, he developed a severe systemic infusion reaction, which started with chills and fever and then intensified to NF in the flank region. Escherichia coli was isolated from the blood and affected tissues, in this case.22 This presentation was similar to that of our case, in which NF was preceded by pyrexia. However, the causative organism E. coli was different in that it is considered to be part of the normal flora of human gut and stains gram-negative, while the isolated organism in our case report belonged to Pseudomonas spp., which stains gram-positive and is known to cause opportunistic infection in immunocompromised individuals with severe manifestations that may result in a necrotizing, gangrenous process.35
Rituximab has also been used successfully to control the flares of rheumatoid arthritis. A 62-year-old woman with rheumatoid arthritis, who did not respond to traditional therapeutic regimens, including methotrexate and disease-modifying anti-rheumatic drugs, was treated with rituximab in addition to daily prednisone for 6 months. The patient developed a swollen painful left arm preceded by rigors 18 days after the first rituximab cycle. The patient was diagnosed with NF caused by group A streptococcus.23 Similar to our case, the patient in the aforementioned case was considered immunocompromised due to steroid-dependency.
Conclusion
In conclusion, although there exists a black box warning for mucocutaneous reactions to rituximab, few cases of such reactions have been reported to date. Through this case report, we encourage physicians to be alert and vigilant when diagnosing and treating this severe and fatal side effect of rituximab therapy.
Abbreviations
CLL, chronic lymphocytic leukemia; FRNS, frequent relapsing nephrotic syndrome; HBV, hepatitis B virus; INS, idiopathic NS; Ig, immunoglobulin; NF, necrotizing fasciitis; NS, nephrotic syndrome; SRNS, steroid-resistant nephrotic syndrome; SDNS, steroid-dependent nephrotic syndrome.
Ethical Approval and Informed Consent
This study was conducted with the approval of the research ethics committee and the Institutional Review Board of the Pediatric department at King Abdulaziz University Hospital. Informed written consent was obtained from the parents of the patient for the publication of the case report.
Funding
The present study received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Study of Kidney Disease in Children. Nephrotic syndrome in children: prediction of histopathology from clinical and laboratory characteristics at time of diagnosis. Kidney Int. 1978;13(2):159–165. doi:10.1038/ki.1978.23
2. Iijima K, Sako M, Nozu K. Rituximab for nephrotic syndrome in children. Clin Exp Nephrol. 2016;21(2):193–202. doi:10.1007/s10157-016-1313-5
3. McKinney P, Feltbower R, Brocklebank J, Fitzpatrick M. Time trends and ethnic patterns of childhood nephrotic syndrome in Yorkshire, UK. Pediatr Nephrol. 2001;16(12):1040–1044. doi:10.1007/s004670100021
4. Chanchlani R, Parekh R. Ethnic differences in childhood nephrotic syndrome. Front Pediatr. 2016;4. doi:10.3389/fped.2016.00039
5. Kallash M, Smoyer W, Mahan J, Cai X-Y, Kuo H-C. Rituximab use in the management of childhood nephrotic syndrome. Front Pediatr. 2019;7:7. doi:10.3389/fped.2019.00007
6. RESERVED, I. Orphanet: idiopathic steroid sensitive nephrotic syndrome; 2022. Available from: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=EN&Expert=69061.
7. Nagano C, Sako M, Kamei K, et al. Study protocol: multicenter double-blind, randomized, placebo-controlled trial of rituximab for the treatment of childhood-onset early-stage uncomplicated frequently relapsing or steroid-dependent nephrotic syndrome (JSKDC10 trial). BMC Nephrol. 2019;20:1. doi:10.1186/s12882-019-1470-3
8. Chaumais M, Garnier A, Chalard F, et al. Fatal pulmonary fibrosis after rituximab administration. Pediatr Nephrol. 2009;24(9):1753–1755. doi:10.1007/s00467-009-1195-9
9. Sellier-Leclerc A, Belli E, Guérin V, Dorfmüller P, Deschênes G. Fulminant viral myocarditis after rituximab therapy in pediatric nephrotic syndrome. Pediatr Nephrol. 2013;28(9):1875–1879. doi:10.1007/s00467-013-2485-9
10. Guigonis V, Dallocchio A, Baudouin V, et al. Rituximab treatment for severe steroid- or cyclosporine-dependent nephrotic syndrome: a multicentric series of 22 cases. Pediatr Nephrol. 2008;23(8):1269–1279. doi:10.1007/s00467-008-0814-1
11. Ardelean D, Gonska T, Wires S, et al. Severe ulcerative colitis after rituximab therapy. Pediatrics. 2010;126(1):e243–e246. doi:10.1542/peds.2009-3395
12. Kamei K, Takahashi M, Fuyama M, et al. Rituximab-associated agranulocytosis in children with refractory idiopathic nephrotic syndrome: case series and review of literature. Nephrol Dial Transplant. 2014;30(1):91–96. doi:10.1093/ndt/gfu258
13. Tony H, Burmester G, Schulze-Koops H, et al. Safety and clinical outcomes of rituximab therapy in patients with different autoimmune diseases: experience from a national registry (GRAID). Arthritis Res Ther. 2011;13(3):R75. doi:10.1186/ar3337
14. Clark AG, Barrat TM. Steroid-responsive nephrotic syndrome. In: Barrat TM, Avner ED, Harmon WE, editors. Pediatric Nephrology.
15. Huang JW, Fang CT, Hung KY, Hsueh PR, Chang SC, Tsai TJ. Necrotizing fasciitis caused by Serratia marcescens in two patients receiving corticosteroid therapy. J Formos Med Assoc. 1999;98(12):851–854.
16. Ogawa D, Shikata K, Wada J, Matsuda M, Makino H. Successful treatment of necrotizing fasciitis associated with diabetic nephropathy. Diabetes Res Clin Pract. 2003;60(3):213–216. doi:10.1016/S0168-8227(03)00034-2
17. Delibaş A, Bek K, Bülbül M, Demircin G, Ş B, Öner A. Necrotizing fasciitis in a child: a rare complication of idiopathic nephrotic syndrome. Pediatr Nephrol. 2004;20(1):99–101. doi:10.1007/s00467-004-1669-8
18. Audard V, Pardon A, Claude O, et al. Necrotizing fasciitis during de novo minimal change nephrotic syndrome in a kidney transplant recipient. Transpl Infect Dis. 2005;7(2):89–92. doi:10.1111/j.1399-3062.2005.00097.x
19. Bagri N, Saha A, Dubey NK, Rai A, Bhattacharya S. Skin grafting for necrotizing fasciitis in a child with nephrotic syndrome. Iran J Kidney Dis. 2013;7(6):496–498.
20. Abdulkareem A, D’Souza R, Shogbesan O, Donato A. A case of rituximab-induced necrotizing fasciitis and a review of the literature. Case Rep Hematol. 2017;2017:1–5. doi:10.1155/2017/6971027
21. Morita T, Ugai T, Tanimoto T, Matsue K. Necrotising fasciitis after bortezomib and dexamethasone-containing regimen in an elderly patient of Waldenstrom macroglobulinaemia. Case Rep. 2014;2014(mar26 1):bcr2013203399–bcr2013203399.
22. Krieger J, Merin J, Rabinowitz I. Necrotizing fasciitis following rituximab therapy. J Oncol Pharm Pract. 2002;8(4):127–129. doi:10.1191/1078155202jp097oa
23. Raghuvanshi S, Menon A. AB0575 A fulminant case of necrotizing fasciitis secondary to rituximab in a patient with rheumatoid arthritis. Ann Rheum Dis. 2013;71:671. doi:10.1136/annrheumdis-2012-eular.575
24. Sinha MD, MacLeod R, Rigby E, Clark AG. Treatment of severe steroid-dependent nephrotic syndrome (SDNS) in children with tacrolimus. Nephrol Dial Transplant. 2006;21(7):1848–1854. doi:10.1093/ndt/gfi274
25. Yousefichaijan P, Salehi B, Rafiei M, Dahmardnezhad M, Naziri M. The correlation between attention deficit hyperactivity disorder and steroid-dependent nephrotic syndrome. Saudi J Kidney Dis Transpl. 2015;26(6):1205–1209. doi:10.4103/1319-2442.168624
26. Takura T, Takei T, Nitta K. Cost-effectiveness of administering rituximab for steroid-dependent nephrotic syndrome and frequently relapsing nephrotic syndrome: a preliminary study in Japan. Sci Rep. 2017;7:46036. doi:10.1038/srep46036
27. Horinouchi T, Sako M, Nakanishi K, et al. Study protocol: mycophenolate mofetil as maintenance therapy after rituximab treatment for childhood-onset, complicated, frequently-relapsing nephrotic syndrome or steroid-dependent nephrotic syndrome: a multicenter double-blind, randomized, placebo-controlled trial (JSKDC07). BMC Nephrol. 2018;19(1):302. doi:10.1186/s12882-018-1099-7
28. Coiffier B, Lepage E, Briere J, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;364(4):235–242. doi:10.1056/NEJMoa011795
29. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med. 2572–2581;350(25):2004.
30. Niles J. Rituximab in induction therapy for anti-neutrophil cytoplasmic antibody (ANCA) vasculitis. Clin Exp Immunol. 2011;164(1):27–30. doi:10.1111/j.1365-2249.2011.04363.x
31. Ng KP, Cambridge G, Leandro MJ, Edwards JC, Ehrenstein M, Isenberg DA. B cell depletion therapy in systemic lupus erythematosus: long-term follow-up and predictors of response. Ann Rheum Dis. 2007;66(9):1259–1262. doi:10.1136/ard.2006.067124
32. Sun L, Xu H, Shen Q, et al. Efficacy of rituximab therapy in children with refractory nephrotic syndrome: a prospective observational study in Shanghai. World J Clin Pediatr. 2014;10(1):59–63. doi:10.1007/s12519-014-0453-5
33. Iijima K, Sako M, Nozu K, et al. Rituximab for childhood-onset, complicated, frequently relapsing nephrotic syndrome or steroid-dependent nephrotic syndrome: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet. 2014;384(9950):1273–1281. doi:10.1016/S0140-6736(14)60541-9
34. Gea-Banacloche JC. Rituximab-associated infections. In: Seminars in Hematology. Vol. 47. 2010:187–198.
35. Fujitani S, Moffett KS, Yu VL. Pseudomonas aeruginosa. Antimicrobe. Infectious Disease & Antimicrobial Agents; 2017. Available from: http://www.antimicrobe.org/new/b112.asp.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.