Back to Journals » Clinical Interventions in Aging » Volume 21
Native Platelet Function and Clinical Outcomes in Very Elderly Patients: A Retrospective Cohort Study
Received 24 March 2026
Accepted for publication 9 June 2026
Published 25 June 2026 Volume 2026:21 611696
DOI https://doi.org/10.2147/CIA.S611696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Nanzhu Yang, Xiuyuan Zhao, Xin Li
Department of Neurology, the Second Hospital of Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Xin Li, Email [email protected]
Purpose: This study examined native platelet function in very elderly patients (≥ 80 years) not receiving antiplatelet or anticoagulant therapy, its correlation with routine laboratory parameters, and factors associated with poor 90-day outcomes.
Methods: This retrospective cohort study included 94 very elderly inpatients (80– 89 years, n=50; ≥ 90 years, n=44). Patients on antiplatelet, anticoagulant, or glucocorticoid therapy within 7 days before admission were excluded. Baseline data, laboratory parameters—including ADP‑ and AA‑induced aggregation, platelet count, and 90‑day outcomes were collected. Adverse clinical outcomes occurred in 13 patients during this period. Spearman correlation and Firth penalized logistic regression were used.
Results: No differences were found between age groups in platelet count or aggregation rates (all P > 0.05). Prothrombin time was longer in the ≥ 90 group (13.32± 1.31 vs. 12.08± 1.63 s, P < 0.001). Platelet function showed no meaningful correlation with white blood cell count, hemoglobin, or fibrinogen (|r| < 0.2, all P > 0.05). Among the 94 patients, 13 had poor outcomes. In Firth regression, neither age ≥ 90 years (OR=2.86, 95% CI: 0.85– 9.62, P=0.090) nor coronary heart disease (OR=1.61, 95% CI: 0.50– 5.21, P=0.424) reached statistical significance. The model’s area under the ROC curve was 0.657 (bias‑corrected 0.640).
Conclusion: In this cohort of very elderly patients not on antiplatelet or anticoagulant therapy, native platelet function did not differ between octogenarians and nonagenarians and showed no correlation with routine hematological parameters. No statistically significant predictor of poor 90‑day outcomes was identified. The small number of outcome events (n=13) limits statistical power, so these findings should be considered exploratory. Larger prospective studies are needed to validate these findings.
Keywords: very elderly, platelet aggregation, platelet function, clinical outcome, risk factor
Introduction
Global population aging has accelerated over the past decades. Individuals aged 80 years and older now represent the fastest-growing demographic segment worldwide.1 This shift creates challenges for clinical management and prognostic assessment, as very elderly patients often have multiple comorbidities, reduced physiological reserve, and altered responses to treatment.2
Platelets are central to hemostasis and thrombosis. Their aggregation function is closely linked to cardiovascular and cerebrovascular diseases, the leading causes of death and disability in older populations.3 Aging brings structural and functional changes to platelets, but studies on age-related alterations in platelet function have yielded inconsistent results, especially in those aged 90 years and older.4,5 Aging is associated with chronic low-grade inflammation, endothelial dysfunction, and remodeling of hematopoietic stem cells. These changes may alter platelet production and function. Previous studies reported conflicting findings on platelet reactivity in the elderly, possibly due to differences in comorbidities, medication use, and survival bias.
Most existing research on native platelet function and clinical outcomes has focused on middle-aged and younger elderly patients with established cardiovascular disease, many of whom were on antiplatelet drugs. Consequently, dedicated investigations targeting very elderly individuals aged ≥80 years remain scarce. This population is characterized by multiple comorbidities, age-related organ dysfunction, and complex medication regimens, which are the factors that may modify platelet function and its relationship with clinical outcomes in ways distinct from younger cohorts.5,6
This study compared platelet function between patients aged 80–89 years and those aged ≥90 years, examined its correlation with routine laboratory parameters, and identified factors associated with poor 90‑day outcomes by integrating platelet measures with clinical characteristics. Our goal was to characterize platelet function in this population and assess its prognostic value to support individualized clinical decision‑making.
Materials and Methods
Study Population
This retrospective cohort study enrolled 94 very elderly patients admitted to the Department of Geriatrics at our hospital between January 2022 and December 2024.
Inclusion criteria were: (1) age ≥80 years at admission; (2) complete clinical data, laboratory results, and follow-up information; (3) voluntary participation with written informed consent provided by the patient or a legal surrogate.
Exclusion criteria were: (1) hematological disorders, immune-mediated diseases, or active malignancies that could affect platelet function; (2) use of antiplatelet agents, anticoagulants, or glucocorticoids within 7 days prior to admission; (3) severe hepatic or renal dysfunction (serum creatinine >265 μmol/L or Child-Pugh class C); (4) acute infectious diseases, major trauma, or surgery within 30 days before admission; (5) incomplete data or loss to follow-up.
The study was approved by the Medical Ethics Committee of The Second Hospital of Tianjin Medical University (Approval No. KY2026K253) and conducted in accordance with the Declaration of Helsinki.
Data Collection
Clinical data were retrieved from the hospital electronic medical record system, including age, sex, and comorbidities. Diagnoses of hypertension, diabetes mellitus, and coronary heart disease were made following established clinical guidelines, smoking history (≥1 cigarette daily for >1 year), alcohol consumption (≥50 mL liquor daily for >1 year), and vital signs (systolic and diastolic blood pressure).
Definitions:7–10
Hypertension: systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least two occasions, or current use of antihypertensive medication (2018 Chinese Guidelines for the Management of Hypertension).
Diabetes mellitus: fasting plasma glucose ≥7.0 mmol/L, HbA1c ≥6.5%, or current glucose-lowering therapy (2020 Chinese Diabetes Society guidelines).
Coronary heart disease (CHD): prior myocardial infarction, coronary revascularization, or angiographic evidence of ≥50% stenosis in a major epicardial artery, according to the 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes and the 2018 Chinese Guidelines for the diagnosis and treatment of acute myocardial infarction.
Laboratory parameters were obtained from the first fasting blood sample after admission, including white blood cell count (WBC), hemoglobin (Hb), prothrombin time (PT), fibrinogen (FIB), platelet count (PLT), and ADP‑ and AA‑induced platelet aggregation rates. Complete blood cell counts were tested using the BC-7500(NR) analyzer produced by Mindray in China. Coagulation function was detected with the STA Compact Max Evolution analyzer from Diagnostica Stago, France. Platelet aggregation induced by ADP and AA was examined by the Aggregation Remote Analyzer of Helena Company in the United States.11 All assays were completed within 2 hours of blood collection.
We selected WBC, Hb, and FIB because these are widely used clinical indicators. White blood cell count serves as an inflammatory biomarker, hemoglobin reflects oxygen-carrying capability and anemia status, while fibrinogen acts as a core coagulation protein and acute-phase reactant. These indicators were pre-selected given their wide clinical applicability, well-documented correlations with adverse clinical events in older populations, as well as their potential confounding and interactive effects on platelet function. Further analyses of other biomarkers may be conducted in subsequent investigations.
Outcome Assessment
All patients underwent 90-day follow-up through telephone interviews and outpatient visits. Clinical outcomes were categorized as good or poor. Poor outcome was defined as any of the following within 90 days: all-cause mortality; severe disability (Barthel Index <60) resulting from cardiovascular or cerebrovascular events; or hospital readmission due to major adverse cardiovascular and cerebrovascular events (MACE), including acute myocardial infarction, ischemic stroke, or heart failure. Good outcome was defined as the absence of these events with stable or improved clinical status.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 and R 4.1.0. Normally distributed continuous variables are presented as mean ± standard deviation and were compared between groups using independent samples t-tests. Categorical variables are expressed as frequencies (n, %) and were compared using chi-square tests or Fisher’s exact tests, as appropriate.
Given the modest sample size, Spearman rank correlation analysis was used to examine relationships between platelet function indices (ADP, AA, PLT) and routine laboratory parameters (WBC, Hb, FIB). Correlation coefficients (r) and corresponding P-values are reported.
Because only 13 outcome events occurred among 94 patients, we used Firth penalized logistic regression to reduce small‑sample bias. Variables with P<0.2 in univariate analysis (age group, sex, diabetes, CHD, ADP, AA, PLT) were considered, but to avoid overfitting we retained only age group and CHD in the final model. Results are presented as odds ratios (OR) with 95% confidence intervals (CI). Model discrimination was assessed by the area under the receiver operating characteristic curve (AUC) with optimism correction using 200 bootstrap resamples. A two‑tailed P<0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 94 very elderly patients were enrolled, 50 aged 80–89 years and 44 aged ≥90 years (57.4% male). Baseline characteristics are shown in Table 1. The two groups differed significantly only in age (95.16 ± 3.09 vs. 84.90 ± 2.73, P<0.001) and prothrombin time (13.32±1.31 vs. 12.08±1.63 s, P<0.001). No significant differences were observed in systolic or diastolic blood pressure, white blood cell count, hemoglobin, fibrinogen, platelet count, ADP‑induced aggregation, or AA‑induced aggregation (all P>0.05). The ≥90 years group had a higher proportion of men (65.9% vs. 50.0%) and a lower prevalence of diabetes (15.9% vs. 32.0%), but neither difference was statistically significant. Hypertension, coronary heart disease, smoking, and alcohol use were similar between groups. 13 patients (13.8%) had poor outcomes: 4 (8.0%) in the 80‑89 years group and 9 (20.5%) in the ≥90 years group (P=0.148).
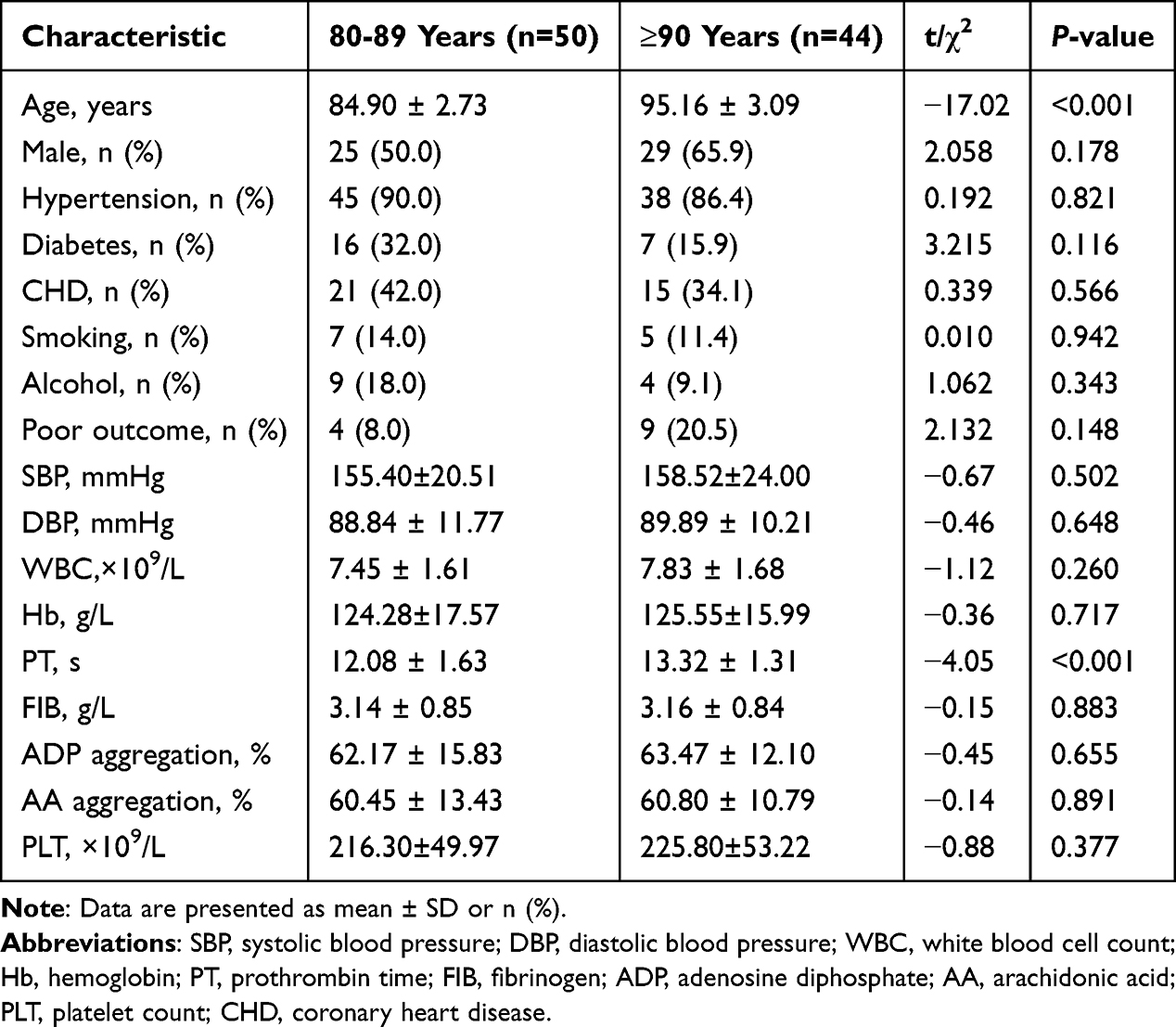 |
Table 1 Baseline Clinical and Laboratory Characteristics by Age Group |
Platelet Function Across Age Groups
No significant differences were found between the two age groups in ADP‑induced aggregation (P=0.655), AA‑induced aggregation (P=0.891), or platelet count (P=0.377) (Figure 1). These findings suggest that within this very elderly population (≥80 years), further aging is not associated with systematic changes in platelet number or aggregation capacity.
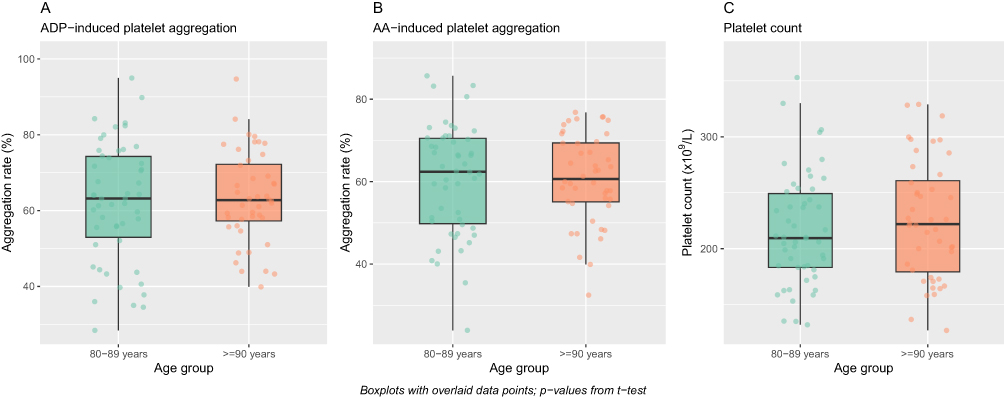 |
Figure 1 Comparison of platelet function indices between age groups (n=50 for 80‑89 years, n=44 for ≥90 years). (A) ADP-induced platelet aggregation rate; (B) AA-induced platelet aggregation rate; (C) Platelet count. Data are presented as mean ± SD. Comparisons were performed using independent samples t‑tests; no significant differences were observed between groups (all P>0.05). |
Correlations with Routine Laboratory Parameters
Spearman correlation analysis was performed to examine relationships between platelet function indices and routine hematological parameters. As shown in Figure 2, all correlation coefficients were of small magnitude (|r| < 0.2) and none reached statistical significance (all P > 0.05). These results indicate that in very elderly patients, platelet function operates independently of basic hematological and coagulation profiles.
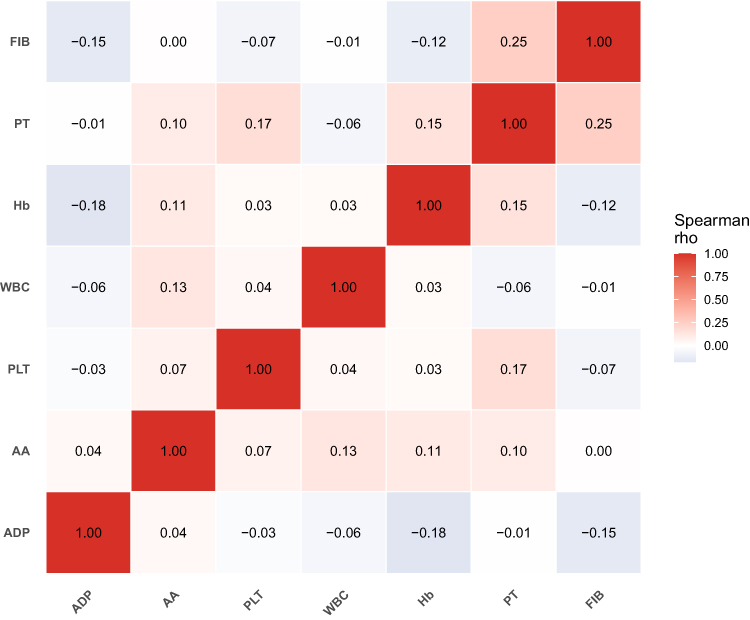 |
Figure 2 Correlation heatmap of platelet function indices and laboratory parameters. Spearman correlation coefficients are displayed; blue indicates negative correlation, red indicates positive correlation. Color intensity reflects correlation strength. All correlations were non-significant (all P>0.05). Abbreviations: WBC, white blood cell count; Hb, hemoglobin; FIB, fibrinogen; AA, AA-induced aggregation; ADP, ADP-induced aggregation; PLT, platelet count. |
Risk Factors for Poor Clinical Outcomes
Given the small number of outcome events (n=13), we used Firth penalized logistic regression to reduce estimation bias. Univariate screening identified several variables with P<0.2 (age group, sex, diabetes, coronary heart disease, ADP, AA, and platelet count). However, to avoid overfitting, the final model included only two clinically relevant predictors: age group (≥90 vs. 80‑89 years) and coronary heart disease.
As shown in Table 2 and Figure 3, neither age ≥90 years (OR=2.86, 95% CI: 0.85–9.62, P=0.090) nor coronary heart disease (OR=1.61, 95% CI: 0.50–5.21, P=0.424) reached statistical significance. Platelet function indices were not retained in the final model due to the event‑per‑predictor constraint.
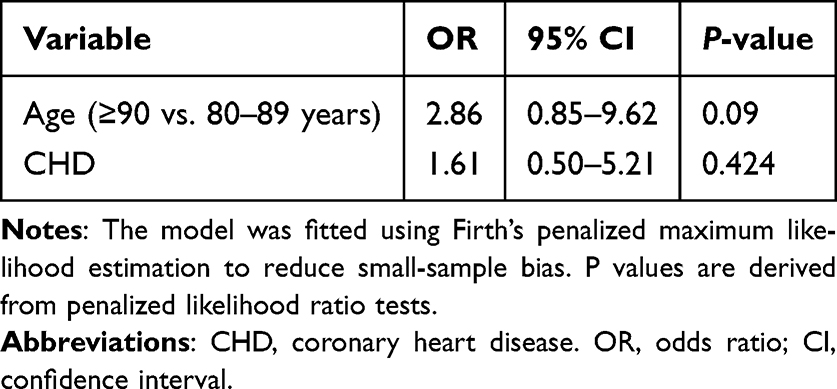 |
Table 2 Firth Penalized Logistic Regression Analysis of Factors Associated with Poor 90‑day Clinical Outcomes |
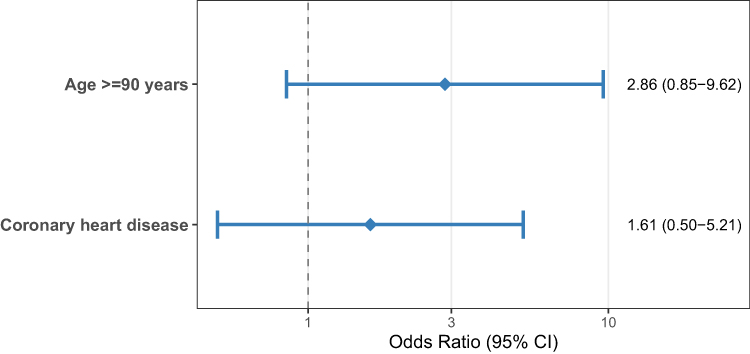 |
Figure 3 Forest plot of factors associated with poor clinical outcomes. Horizontal lines represent 95% confidence intervals; black squares represent odds ratios. The vertical dashed line indicates the null value (OR=1). Factors with confidence intervals crossing the reference line are not statistically significant. |
The model’s discriminative ability was modest. The area under the ROC curve was 0.657 (95% CI: 0.512–0.802), and after bootstrap correction for optimism, the bias‑corrected AUC was 0.640 (Figure 4). These results suggest that the combination of age and coronary heart disease provides only weak‑to‑moderate prognostic information in this cohort.
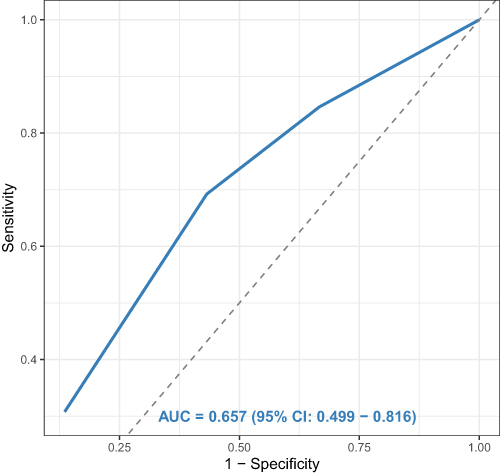 |
Figure 4 ROC curve of the simplified model (age group + coronary heart disease) for predicting poor clinical outcomes. The solid line represents the model. Area under the curve (AUC) = 0.657 (95% CI: 0.512–0.802); bias‑corrected AUC = 0.640. The dashed diagonal line represents the reference line (AUC = 0.5). |
Discussion
This study characterized native platelet function in very elderly patients aged ≥80 years not taking antiplatelet or anticoagulant drugs. Several findings merit discussion.
Platelet Function Stability in the Very Elderly
We found no difference in ADP‑ or AA‑induced aggregation between the 80‑89 years group and the ≥90 years group. This suggests that within the ≥80 years population, further aging does not systematically alter native platelet aggregation. One explanation is that major age‑related changes may occur before age 80. Another is that chronic low‑grade inflammation, common in this age group, may chronically activate platelets and mask further decline.12 Survival bias could also play a role, as individuals who reach age 90 or older may have inherently robust platelet function. Prothrombin time was significantly prolonged in the ≥90 years group, consistent with prior reports,13,14 indicating mild coagulopathy likely due to reduced hepatic synthesis. This finding suggests that the oldest old may have a mildly increased bleeding risk, warranting caution when considering antithrombotic therapy.
Independence of Platelet Function from Routine Parameters
The lack of correlation between platelet function indices and WBC, Hb, or fibrinogen differs from patterns observed in younger populations, where inflammatory markers and fibrinogen often correlate positively with platelet aggregation.9,15 In younger individuals, inflammation activates platelets and promotes aggregation, creating measurable correlations between platelet function and inflammatory markers.16 In the very elderly, however, age‑related dysregulation of physiological systems may disrupt these relationships. The aging of hematopoiesis and its microenvironment leads to complex remodeling of hematopoietic stem cells and immune cells, making their regulatory pathways increasingly independent and their outputs less predictable from individual parameters.13 In very elderly individuals, the link between systemic inflammation and platelet reactivity is modified by multiple factors, including cumulative burden of comorbidities, polypharmacy, and genetic background, thereby obscuring simple linear correlations. Our findings suggest that in very elderly patients, platelet function should be considered a relatively independent biological domain rather than a simple reflection of systemic inflammatory or hematological status.
Predictors of Poor Clinical Outcomes and Model Performance
Neither age ≥90 years nor coronary heart disease reached statistical significance in the multivariable analysis, with odds ratios of 2.86 (95% CI: 0.85–9.62, P=0.090) and 1.61 (95% CI: 0.50–5.21, P=0.424), respectively. The wide confidence intervals reflect limited statistical power due to the small sample size and low number of outcome events (n=13).
Coronary heart disease is well established as a major determinant of prognosis in older adults, contributing to myocardial ischemia, heart failure, and arrhythmic complications.9 The oldest old (≥90 years) represent a uniquely vulnerable population characterized by multisystem physiological decline, reduced physiological reserve, and heightened susceptibility to complications from intercurrent illnesses.14 The combination of advanced age and cardiovascular comorbidity may synergistically increase risk, consistent with frailty concepts emphasizing the cumulative burden of deficits.16
Unlike previous studies in middle‑aged and younger elderly patients with acute coronary syndromes, where heightened platelet reactivity predicts adverse events,15,16 we found no independent association between native platelet function indices and clinical outcomes in this cohort. Several factors may explain this difference. Our patients were stable and community‑dwelling, so platelet function may be less variable and offer less prognostic value than in acutely ill populations. Outcomes in the very elderly are shaped by a complex interplay of factors such as organ function, comorbidity burden, nutritional status, and polypharmacy, with platelet function likely playing a minor role.17 By design, patients on antiplatelet agents were excluded from this study, so our findings reflect native platelet function, whereas most cardiovascular cohorts include treated patients whose on‑treatment platelet reactivity is measured. Additionally, the composite outcome combining mortality, severe disability, and readmission may have diluted the predictive value of platelet function, which might be more closely tied to thrombotic events than to disability or heart failure readmissions.
Our initial 7‑predictor model was overfitted given only 13 events. After simplifying to two predictors and using Firth regression, the AUC dropped to 0.657 (bias‑corrected 0.640), indicating only weak‑to‑moderate discrimination. Therefore, we do not claim clinical utility for this model.
Limitations
This study has several limitations. The single‑center retrospective design and small sample size (94 patients, 13 events) limited statistical power, as reflected in wide confidence intervals. The 90‑day follow‑up may be too short to capture longer‑term prognosis. We did not account for potential use of SSRIs or NSAIDs, which can affect platelet function and may represent unmeasured confounders. Our assessment of platelet function was confined to conventional aggregation measures; we did not assess in vivo activation markers (eg, P‑selectin). The study population consisted of relatively stable, community‑dwelling individuals, so findings may not generalize to acutely ill, institutionalized, or frail very elderly patients. Lack of external validation means our model’s performance cannot be confirmed. Larger prospective multicenter cohorts with extended follow‑up are needed to validate our findings. Future studies should incorporate comprehensive geriatric assessments (frailty, cognitive function, nutritional status) and serial measurements of platelet function, as well as a broader panel of platelet assays and inflammatory markers.
Conclusion
In this cohort of very elderly patients not on antiplatelet or anticoagulant therapy, native platelet function did not differ between octogenarians and nonagenarians and showed no correlation with routine hematological parameters. No statistically significant predictor of poor 90‑day outcomes was identified. The small number of outcome events (n=13) limits statistical power, so these findings should be considered exploratory. Larger prospective studies are needed to validate these findings.
Ethical Considerations
The study protocol was approved by the Medical Ethics Committee of the Second Hospital of Tianjin Medical University (Approval number: KY2026K253) and conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We would like to acknowledge two science and technology key project awards (Grant No. TJYXZDXK-3-017C and Grant No. TJWJ2023XK007) from Tianjin Health and Family Planning Commission, China (to Li Xin).
Disclosure
The authors declare that they have no competing interests.
References
1. United Nations, Department of Economic and Social Affairs, Population Division. World population ageing 2023: challenges and opportunities of population ageing. New York: United Nations; 2023.
2. Beard JR, Officer A, de Carvalho IA, et al. The world report on ageing and health: a policy framework for healthy ageing. Lancet. 2016;387(10033):2145–9. doi:10.1016/S0140-6736(15)00516-4
3. van der Meijden PEJ, Heemskerk JWM. Platelet biology and functions: new concepts and clinical perspectives. Nat Rev Cardiol. 2019;16(3):166–179. doi:10.1038/s41569-018-0110-0
4. Le Blanc J, Lordkipanidzé M. Platelet Function in Aging. Front Cardiovasc Med. 2019;6:109. doi:10.3389/fcvm.2019.00109
5. Cowman J, Dunne E, Oglesby I, et al. Age-related changes in platelet function are more profound in women than in men. Sci Rep. 2015;5:12235. doi:10.1038/srep12235
6. Favaloro EJ, Franchini M, Lippi G. Aging hemostasis: changes to laboratory markers of hemostasis as we age - a narrative review. Semin Thromb Hemost. 2014;40(6):621–633. doi:10.1055/s-0034-1384631
7. Writing Group of 2018 Chinese Guidelines for the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology, et al. 2018 Chinese guidelines for the management of hypertension writing group of 2018. Chin J Cardiovasc Med. 2019;24(1):24–56.
8. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition)[J]. Chin J Endocrinol Metab. 2021;37(4):311–398.
9. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes[J]. Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
10. Chinese Society of Cardiology, Editorial Board of Chinese Journal of Cardiology. 2018 Chinese guidelines for the diagnosis and treatment of acute myocardial infarction. Chinese J Cardiol. 2019;47(4):268–298.
11. Cattaneo M, Cerletti C, Harrison P, et al. Recommendations for the standardization of light transmission aggregometry: a consensus of the working party from the platelet physiology subcommittee of SSC/ISTH. J Thromb Haemost. 2013;11(6):1183–1189. doi:10.1111/jth.12231
12. Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524–533. doi:10.1038/s41586-021-03392-8
13. Kovtonyuk LV, Fritsch K, Feng X, et al. Inflamm-Aging of Hematopoiesis, Hematopoietic Stem Cells, and the Bone Marrow Microenvironment. Front Immunol. 2016;7:502. doi:10.3389/fimmu.2016.00502
14. Clegg A, Young J, Iliffe S, et al. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
15. Breet NJ, van Werkum JW, Bouman HJ, et al. Comparison of platelet function tests in predicting clinical outcome in patients undergoing coronary stent implantation. JAMA. 2010;303(8):754–762. doi:10.1001/jama.2010.181
16. Angiolillo DJ, Galli M, Collet JP, et al. Antiplatelet therapy after percutaneous coronary intervention. EuroIntervention. 2022;17(17):e1371–e1396. doi:10.4244/EIJ-D-21-00904
17. Fried LP, Tangen CM, Walston J, et al;Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–156. doi:10.1093/gerona/56.3.M146
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.