Back to Journals » International Journal of Nanomedicine » Volume 21
Nanotechnology-Driven Precision Modulation of Transplant Immunity: From Mechanistic Insights to Clinical Tolerance
Authors Zhang L ![]() , Wu K, Si S, Zhang X, Jia F, Xu X
, Wu K, Si S, Zhang X, Jia F, Xu X ![]() , Jin X
, Jin X
Received 6 November 2025
Accepted for publication 23 January 2026
Published 19 February 2026 Volume 2026:21 579655
DOI https://doi.org/10.2147/IJN.S579655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Eng San Thian
Long Zhang,1– 3,* Kunzhe Wu,1– 3,* Shuhan Si,4 Xiaoyu Zhang,4 Feiran Jia,4 Xiaohua Xu,4 Xuefei Jin1– 3
1Department of Urology, Second Ward, China-Japan Union Hospital of Jilin University, Changchun, 130033, People’s Republic of China; 2Jilin Provincial Key Laboratory of Molecular Diagnosis of Urological Tumors, Changchun, Jilin, 130033, People’s Republic of China; 3Jinlin Provincial Key Laboratory of Urological Tumors, Changchun, Jilin, 130033, People’s Republic of China; 4Department of Nephrology, China-Japan Union Hospital of Jilin University, Changchun, 130033, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohua Xu, Email [email protected] Xuefei Jin, Email [email protected]
Abstract: Organ transplantation represents a definitive therapeutic modality for end-stage organ failure, yet it is plagued by formidable challenges encompassing allogeneic immune rejection and the inherent limitations of conventional immunosuppressive regimens. Nonspecific immunosuppression not only precipitates severe adverse events such as opportunistic infections and malignancies but also fails to precisely modulate the local immune microenvironment. The core innovation of this review lies in the systematic integration of the distinctive advantages of nanotechnology—including targeted delivery, multifunctional synergy, and stimuli-responsive intelligence—with transplant immune regulation, encompassing a comprehensive analysis spanning mechanistic elucidation, strategic optimization, and clinical translation. We first delineate the pivotal mechanisms underlying immune rejection, including the regulatory roles of the transplant immune microenvironment, T lymphocytes, macrophages, and oxidative stress in ischemia-reperfusion injury (IRI). Subsequently, we conduct a critical comparison between conventional immunosuppressants and emerging therapeutic strategies, with a particular focus on how nanoplatforms enable spatiotemporally precise immune modulation. This includes targeting the transplant immune microenvironment, reprogramming T cell/macrophage functions, mitigating oxidative stress, facilitating tissue repair and regeneration, as well as inducing immune tolerance via both active and passive approaches. Additionally, we discuss innovative nanotechnological strategies such as the optimization of organ cryopreservation protocols. In summary, nanotechnology offers a targeted, multifunctional, and long-acting paradigm for transplant immune regulation, albeit confronted with formidable translational bottlenecks. Future integration with interdisciplinary technologies will undoubtedly propel the field toward the goal of precision immune modulation in organ transplantation.
Keywords: transplant immunity, nanotechnology, immune rejection, immune tolerance, nanodrug delivery, immunosuppression
Introduction
Although organ transplantation is an effective treatment for end-stage organ failure, the shortage of organs remains the primary challenge in the field of global clinical organ transplantation.1,2 The Clinical Trials of Organ Transplantation—or CTOT—is a group that provides money for research on solid organ transplants in adult patients. They fund research at different centers, and they do both clinical and translational research. Donor families express a desire for a greater understanding of organ donation and transplantation. However, long-term recipient survival is still limited by allogeneic immune rejection. Existing immunosuppressants (eg, tacrolimus and rapamycin) significantly reduce the risk of acute rejection. However, their non-specific immunosuppressive properties can cause severe side effects, including opportunistic infections, malignancies, and metabolic disorders. For instance medications like calcium-phosphorus regulators increase the risk of skin cancer.3,4 Current therapies primarily rely on systemic immunosuppression. This approach fails to precisely regulate the local immune microenvironment and inadequately suppresses the abnormal activation of antigen-presenting cells (APCs), such as dendritic cells (DCs) and macrophages. Thus, there is an urgent need for the development of highly targeted and safe immunomodulatory strategies.5,6
Nano-drug delivery systems provide a new approach to overcoming the limitations of traditional therapies. These systems leverage their tunable physicochemical properties, including size, charge, and surface functionalization.7 Size is often closely related to aggregation and is a key determining factor. Conjugates with disparate sizes assemble into aggregates of distinct morphologies, and their dimensions exert a profound impact on internalization by non-phagocytic cells. Once internalized by cells, these conjugates are entrapped within endosomal vesicles, with only a small fraction likely reaching the cytoplasm to exert functional effects.8 Additionally, surface-engineered nanoparticles have enabled precise drug delivery. This precise targeting can be achieved through passive methods, such as the enhanced permeability and retention (EPR) effect, or active approaches, such as ligand modification. These methods enable the accumulation of nanoparticles within the local vascular endothelium of the graft, thereby enhancing drug delivery efficiency. Biodegradable PLGA nanoparticles, for example, are known for their stability and can encapsulate siRNA to silence the CD40 gene. This simultaneously inhibits DC maturation and the differentiation of hematopoietic stem cells into APCs.5 Additionally, surface engineering strategies, such as PEGylation and cell membrane mimicry, can reduce the effects of Regulon, extend its circulating half-life, and establish the basis for precise immune regulation.5,9 Autoimmune diseases, allergies, transplant rejection, and other immune disorders have a widespread impact. Conventional systemic immunosuppressive therapies present challenges regarding efficacy and safety. Tolerogenic vaccines can induce antigen-specific tolerance by generating regulatory T cells; however, they require precise modulation of the immune microenvironment. Engineered nanoparticles and microparticles with optimized designs can enhance targeted immune modulation and antigen-specific tolerance induction. Particle-based tolerance vaccines show promise for clinical translation in treating these disorders.5
This paper systematically explores strategies for suppressing transplant rejection through the synergistic inhibition of multiple mechanisms by nanocarrier platforms. This approach reveals the necessity of coordinating multiple targets and overcoming the limitations of single-pathway intervention. Examples include the targeted delivery of immunomodulators to APCs or T cell subsets, the regulation of intercellular communication via exosomes or biomimetic carriers, and the spatiotemporal control of drug release through responsive hydrogels, metal-organic frameworks, and other materials. We emphasize the unique efficacy of nanocarriers in suppressing immune responses and transplant rejection while addressing challenges of clinical translation, such as scalable manufacturing and long-term safety. The scope of this review encompasses two major scenarios: solid organ transplantation (SOT) and hematopoietic stem cell transplantation (HSCT). For SOT, the focus is directed toward core issues including ischemia-reperfusion injury (IRI) and the dysregulation of the local immune microenvironment. For HSCT, priority is given to the modulation of graft-versus-host disease (GVHD) and the maintenance of a balanced graft-versus-leukemia (GVL) effect. By systematically contrasting the immunopathological features of these two transplantation modalities, this review highlights the universality and specificity of nanotechnology, thereby providing a unified yet differentiated therapeutic strategy for immune regulation across distinct transplantation types. Our goal is to lay the theoretical groundwork for developing next-generation smart anti-rejection nano therapies and drive paradigm shifts in transplant immunology.
Molecular Mechanisms of Immune Rejection
Transplant Immune Microenvironment
Notably, the long-term success of transplanted organs fundamentally depends on precisely regulating the immune microenvironment at the transplant site.10,11 The transplant immune microenvironment is a highly complex, dynamic regulatory hub formed by the parenchymal cells of the transplanted organ, adjacent tissues, infiltrating immune cells, the extracellular matrix (ECM), and numerous soluble signaling molecules, particularly cytokines.10–12 This unique local niche is not a passive bystander in immune responses; rather, it is a core determinant of immune outcomes. Its composition and functional state directly influence whether the immune system induces tolerance toward the transplant or initiates robust rejection.10,11 Changes in the microenvironment directly drive the rejection cascade. The intricate interactions and signaling exchanges among its various components regulate the initiation, amplification, and effector phases of the immune response in a dynamic manner.12 Immune cells in the transplantation milieu modulate allograft rejection via synergistic or antagonistic crosstalk. Emerging evidence shows donor-derived regulatory dendritic cell (DCreg) adoptive transfer orchestrates allogeneic immune responses in living donor liver transplantation (LDLT) recipients multi-facetedly. At 12 months post-transplant, DCregs reduce peripheral effector T/NK cell proportions, enrich tolerogenic DC subsets, suppress pro-inflammatory factor release and donor-reactive T cell proliferation, and inhibit intra-graft effector cell infiltration and TH1 pathway activation. Collectively, DCregs mitigate rejection by remodeling immune microenvironments, providing critical support for personalized immunosuppressive regimen optimization in clinical liver transplantation.13
Cytokines are among the numerous soluble factors that constitute the immune microenvironment. They function as core regulatory elements and have garnered extensive attention and undergone in-depth investigation.14 Clinical evidence indicates that characteristic alterations in the immune microenvironment are significantly correlated with postoperative survival in kidney transplant patients, highlighting the pivotal role of this field in clinical translation.15 Remarkably, the functions of specific key factors exhibit significant dependence on the signaling context and are targeted to specific cells, demonstrating multifaceted and even contradictory functional properties. For instance, the cytokine TGF-β can have opposing functions when acting on different target cells, such as T cells, macrophages, or fibroblasts, depending on the microenvironmental signaling context. Tolerogenic/anti-inflammatory effects: Induces regulatory T cell (Treg) differentiation and suppresses effector T cell function. Fibrogenic/pro-inflammatory effects: Activates fibroblasts to promote extracellular matrix (ECM) deposition or, under specific conditions, promotes pro-inflammatory polarization of macrophages. These effects confer a complex and profound role in maintaining tissue homeostasis and mediating injury responses.14,16,17 Therefore, conducting a precise analysis of the composition and dynamic changes within the immune microenvironment at the transplant site, along with its core regulatory factors (such as TGF-β), is essential for developing effective strategies to suppress rejection and enhance long-term graft survival rates. A deeper understanding of its regulatory networks, including the multifaceted mechanisms of TGF-β and its determining factors, will help answer the fundamental question of how TGF-β dictates the trajectory of immune responses.12,14,16,17 This will establish the fundamental theoretical basis and research direction for designing next-generation precision intervention strategies that target microenvironment regulation and achieve graft-specific immune tolerance.
Biological Characteristics of T Cells and Rejection Mechanisms
T cells are the core effector cells of adaptive immunity and play a pivotal role in transplant rejection. They recognize allogeneic antigens via the T cell receptor (TCR), and under the mediation of co-stimulatory signals, they undergo activation, proliferation, and differentiation. Ultimately, the T cells migrate to the graft, where they mediate cytotoxic effects or recruit inflammatory cells, creating a chain reaction that leads to graft damage.18 Based on their functional phenotypes, T cells are primarily classified into two categories: CD4+ helper T cells and CD8+ cytotoxic T cells. Allogeneic reactive T cells have been identified as the core effector cells in acute cellular rejection.18 Recent research has primarily focused on precise interventions in T cell immune responses using the following approaches: In recent years, studies on precise interventions targeting T cell immune responses have focused on three main areas: First, enhancing the function of regulatory T cells (Tregs). Second, precisely screening T cell subsets prior to transplantation. Third, targeting interventions at tissue-resident memory T cells (TRMs).
In inflammatory diseases, particularly graft-versus-host disease (GVHD), a deficiency or dysfunction of regulatory T cells (Tregs) is a key pathological mechanism. John Koreth’s team conducted research on patients with steroid-refractory chronic GVHD and demonstrated that low-dose interleukin-2 (IL-2) therapy can induce Treg expansion to 20 times baseline levels within two weeks while maintaining long-term homeostasis. This expansion significantly suppresses the overactive immune system and has been clinically proven to effectively alleviate GVHD symptoms (P < 0.01).19 The key to transplant tolerance is the functional activation of antigen-specific regulatory T cells (Tregs) rather than their numerical expansion. Resting thymic Tregs (tTregs) transform into activated Tregs when exposed to effector cytokines. These activated Tregs enhance immune regulation through the high expression of inhibitory molecules (eg, CTLA-4/CD25) and chemokine receptors. Monitoring activated Treg subsets (CD45RO⁺/Foxp3⁺⁺) precisely enables a dynamic assessment of tolerance status. This assessment guides personalized immunosuppression regimens, reducing drug toxicity and improving long-term graft survival.20 FOXP3⁺ Treg cells maintain immune homeostasis by suppressing T cell activation and regulating antigen presentation. They also mediate tissue repair. Defects in their function can trigger autoimmune and kidney diseases. Transplant tolerance and targeted immunosuppression can be established through the in vivo expansion of natural Tregs using IL-2 or via adoptive transfer therapy, which involves the ex vivo expansion or conversion of antigen-specific Tconv cells.21 In the field of hematopoietic stem cell transplantation, a “precision trimming” strategy has been adopted. Since naïve T cells in the donor graft primarily drive chronic graft-versus-host disease (GVHD), while memory T cells mediate the graft-versus-leukemia (GVL) effect, researchers have developed techniques to eliminate naïve T cells while preserving memory T cells prior to transplantation. Compared to untreated groups, in which chronic GVHD incidence ranges from 30% to 70%, this technique reduced chronic GVHD incidence to 7% (P < 0.001), significantly alleviating symptoms. It also maintained the GVL effect, achieving a 77% three-year survival rate.22 Following lung transplantation, single-cell sequencing reveals the oligoclonal expansion of recipient-derived CD8⁺ T cells that differentiate into tissue-resident memory T cells (TRMs) and persist in cases of acute rejection. Although glucocorticoid therapy downregulates cytotoxic genes, it fails to eliminate TRMs in the airways. This clonal expansion originates from in situ activation rather than circulating infiltration, suggesting that TRM accumulation is a core feature of lung graft immune surveillance. Its long-term clinical implications are still unclear.23
Tissue-resident memory T cells (TRMs) at prior infection sites provide protection against reinfection at those sites. However, their role is unclear when homologous antigens persist in organ transplants, which is a critical issue in transplantation. Using a kidney transplant mouse model, we discovered that the recipient’s antigen-specific and polyclonal effector T cells differentiate into TRMs within the graft. These TRMs reside persistently in the new kidney, recognizing it as an “invader” and initiating and maintaining allogeneic graft rejection. These TRMs exhibit characteristics including non-recirculation, local proliferation, re-stimulation-induced IFN-γ production, non-exhaustion, and self-renewal capacity. In vivo depletion of TRMs attenuates rejection. The study also elucidates tissue-residency-associated transcriptional programs. Khodor I. Abou-Daya’s team reported that blocking TRM survival signals, targeting TRM-specific markers, and employing localized interventions instead of systemic immunosuppression are long-term therapeutic options for improving kidney transplant outcomes.24
T cells are at the core of adaptive immunity and play a crucial regulatory role in transplant rejection and chronic graft-versus-host disease (GVHD) (Figure 1).
 |
Figure 1 Injuries, infections, drugs, or abnormalities in organs (heart, kidney, lung, skin) release damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs). Antigen-presenting cells (APCs) recognize these patterns, then present antigens via MHC I to naive CD8⁺ T cells (differentiating into cytotoxic T lymphocytes, CTLs) and via MHC II to naive CD4⁺ T cells (differentiating into effector T cells, Teffs). Cytokines (IL-1, IL-6, TNF-α, INF-γ, IL-12/23) modulate this process. Regulatory T cells (Tregs), affected by immunosuppressants, regulate Teffs. Besides, natural killer (NK) cells and CTLs target graft⁺ cells, and Tregs also interact with APCs to modulate immune responses. |
1) In vivo tracing technology for TRM-specific targets.
2) Optimization of nanoparticle drug platform delivery efficiency in modulating the local immune microenvironment.
3) Establishing multi-target synergistic intervention strategies.18,19,22,24 The introduction of nanotechnology offers a new paradigm for overcoming the systemic toxicity limitations of traditional immunosuppressants and enhancing long-term graft survival.
Macrophage Functions and Regulation in Transplantation
As core effector cells of the innate immune system and key regulators of tissue homeostasis, macrophages occupy a pivotal position in the early decision-making process that governs immune rejection versus tolerance following organ transplantation. This section categorizes macrophage functions into two classical subtypes: pro-inflammatory M1 and anti-inflammatory/repair-promoting M2. Comparative analysis highlights the opposing functional roles of these subpopulations (Figure 2).
 |
Figure 2 Schematic illustration of monocyte differentiation into M1 and M2 macrophages and their distinct functions. Monocytes, upon recognition of pathogen - associated molecular patterns (PAMPs) via Toll - like receptors (TLR - 2, TLR - 4, TLR - 5), differentiate into M1 macrophages under stimulation by cytokines such as IFN - γ, TNF - α, IL - 32, IL - 23, and LPS. M1 macrophages exert anti - pathogenic effects through releasing reactive oxygen species (ROS), nitric oxide (NO), lysosomal enzymes, and pro - inflammatory cytokines (MCP - 1, MIP - 1α, IL - 8, IL - 1β, IL - 6, TNF - α), and promote inflammation. In contrast, under IL - 4, IL - 13, and IL - 10 stimulation, monocytes differentiate into M2 macrophages, which secrete cytokines like TGF - β, IL - 10, PDGF, and FGF to inhibit inflammation and facilitate tissue repair and fibrosis. |
The transplantation event triggers a sequential mechanism of macrophage polarization, beginning with the effects of ischemia-reperfusion injury (IRI). Lung transplantation studies indicate that following IRI in donor lungs, endogenous pulmonary monocytes rapidly activate and initiate a nonspecific inflammatory response.25 Takata et al discovered that IRI induces early M1-like polarization by upregulating CD86, an M1 co-stimulatory molecule, and TREM-1, a pro-inflammatory receptor. This confirms IRI as the core trigger of the rejection cascade.25 Subsequently, the secondary mechanism of molecular pathway regulation in polarization was explored. Using a liver transplantation rejection model, Cao et al revealed that downregulation of miR-449a expression resulted in the de-inhibition of its target gene, PLOD1. This activated the non-canonical NF-κB pathway and drove the transformation of macrophages toward the M1 phenotype.26 Additionally, comparative studies indicate that soluble CD83 (sCD83) in corneal transplantation effectively suppresses rejection by inducing a tolerogenic phenotype in macrophages, locally establishing an immunosuppressive microenvironment, and amplifying Treg cells.27 Knockout of the S100A9 gene significantly reduced the infiltration of hepatic monocytes and macrophages (p<0.05), as well as neutrophils, and downregulated proinflammatory factors. It also inhibited M1 polarization. In vitro studies confirmed that S100A9-TLR4 binding activates NF-κB, and that recombinant protein treatment directly induces the M1 phenotype in macrophages (p < 0.05). These findings establish the S100A9-TLR4/NF-κB-M1 pathway as a core mechanism of injury (IR) during fatty liver transplantation. Consequently, upstream pathways that regulate M1 macrophages often influence transplantation outcomes.28
The CD226/TIGIT-PVR signaling axis plays a key role in regulating macrophage polarization and determining transplant outcomes. TIGIT activation promotes the IL-10⁺/Arg1⁺ M2 phenotype by driving the ERK1/2-MSK1-CREB pathway, which suppresses proinflammatory factors and expands Treg cells, thereby establishing a tolerant microenvironment. However, CD226 antagonizes this effect by amplifying Th1/Th17-mediated rejection. Targeting this pathway synergistically suppresses in situ inflammation and adaptive immune responses, significantly prolonging graft survival.29 ADAR1 downregulates mature miR-21 by binding to its precursor (RIP validation), thereby releasing its inhibition on Foxo1, driving IL-10 secretion, and promoting macrophage M2 polarization. Overexpression of ADAR1 suppresses LPS-induced M1 conversion and significantly enhances graft survival in transplantation models (increased spleen macrophage M2 expression/reduced infiltration). This ADAR1-miR-21-Foxo1-IL-10 axis provides a novel strategy for targeting RNA editing to regulate transplant immunity.30 The immunoregulatory function of M2 macrophages does not exist in isolation; their interaction with regulatory T cells (Tregs) is a core mechanism for maintaining transplant tolerance. In allografts experiencing acute T cell-mediated rejection (TCMR), IL-34 expression is significantly downregulated. Overexpression of IL-34 can reduce the degree of rejection and directly promote M2 macrophage polarization, but it cannot directly induce naïve T cells to differentiate into Tregs—indicating that its regulation of Tregs depends on an indirect pathway mediated by anti-inflammatory factors secreted by M2. This process coordinately increases the ratio of Tregs to M2 in the recipient spleen and the graft, downregulates pro-inflammatory cytokines such as IFN-γ, IL-17, and TNF-α, and establishes an anti-inflammatory immune microenvironment.31 Overall, IL-34 plays a central hub role through M2 polarization, mediating Treg-M2 interactions to suppress the progression of TCMR and providing potential targets for clinical immunotherapy.
The available evidence suggests that the polarization state of macrophages (M1/M2) is an early factor that determines transplant outcomes. The regulatory mechanisms involved include IRI triggering, epigenetic regulation (such as microRNA), and soluble molecular cascades (like sCD83). Current prevailing views include the following: 1) M1 polarization is a common driving mechanism of rejection,26,32–34 and the core pathway of tolerance is M2 induction and Treg expansion.27 In the future, developing strategies to regulate specific polarization signaling networks and maintain M2 phenotype homeostasis will be essential for extending graft survival.
Oxidative Stress Mechanisms in Transplant IRI
Ischemia-reperfusion injury (IRI) is a critical clinical challenge in organ transplantation. The pathological cascade begins during the ischemic-hypoxic phase following organ procurement and leads to the collapse of cellular energy metabolism and ATP depletion. When blood flow is restored during reperfusion, dysfunction in the damaged mitochondrial electron transport chain triggers the production of an excessive amount of reactive oxygen species (ROS), which completely disrupts oxidative-antioxidative homeostasis.35,36 Excessive reactive oxygen species (ROS) exacerbate graft injury through a dual-damage mechanism. The pathological process of IRI can be divided into four interconnected stages. First is the initial “latency phase” during ischemia, which is characterized by metabolic disruption and redox imbalance. Next is an immediate post-reperfusion burst of ROS. This is followed by direct cellular damage from oxidative stress and intensified inflammatory responses. Ultimately, cell death pathways are activated, causing complete disruption of the endogenous antioxidant system. Throughout the process, these stages interact with other injury mechanisms.
In liver transplantation, IRI induces a collapse of the mitochondrial membrane potential, generating superoxide anions (O2−) and hydroxyl radicals (·OH). These radicals directly damage the phospholipid bilayer of hepatocyte membranes. This process activates Kupffer cells, which release proinflammatory factors such as TNF-α and IL-1β. It also induces ferroptosis through the Fenton reaction.37 In the early stages of ischemia-reperfusion injury, Kupffer cells (KCs), as resident macrophages of the liver, undergo a phenotypic switch, transforming from an anti-inflammatory M2 phenotype to a pro-inflammatory M1 phenotype.38 Current preclinical studies primarily use mitochondrial-targeted antioxidants, such as MitoQ, and iron chelators, such as deferoxamine, to block free radical chain reactions in this mechanism.39,40 In kidney transplantation, IRI leads to the detachment of the brush border of renal tubular epithelial cells, forming casts that cause obstruction. Meanwhile, the abnormal activation of the TLR4/MyD88/NF-κB signaling pathway promotes the release of inflammatory mediators, such as IL-6, COX-2, and iNOS. This activates the caspase-9/3-dependent apoptotic pathway, inducing acute tubular necrosis.41 Therapeutic strategies that target this mechanism focus on developing and applying TLR4 antagonists and caspase inhibitors.42 In renal ischemia/reperfusion (I/R) injury, AMPKα activity in renal tubular epithelial cells is dephosphorylated at the Thr172 site by ceramide-activated PP2A phosphatase. This process inhibits ULK1-mediated mitochondrial autophagy, resulting in the accumulation of dysfunctional mitochondria, impaired fatty acid oxidation, lipid deposition, and exacerbated apoptosis.43
Traditional systemic antioxidant therapies, such as N-acetylcysteine, fail to effectively block localized reactive oxygen species (ROS) surges in organs. This is due to their inability to penetrate cell membranes, low targeting efficiency, and short half-lives. Recent therapeutic research has focused on three areas: mitochondrial-targeted antioxidants, precise modulation of inflammatory pathways, and cross-regulation of programmed cell death. Meanwhile, advancements in cryopreservation and perfusion machines aim to reduce ischemic time. Antioxidants (such as N-acetylcysteine) and targeted drugs have also emerged as key areas of research.
Immunosuppressive Therapies of the Traditional Kind and Intervention Strategies That are Emerging
Current Status of Traditional Immunosuppressants
Traditional immunosuppressants inhibit rejection by interfering with the activation of immune cells and inflammatory pathways within the immune microenvironment. This class of drugs includes glucocorticoids; calcineurin inhibitors, such as tacrolimus; antiproliferative agents, such as mycophenolate mofetil; mTOR inhibitors, such as sirolimus; biologics, such as anti-CD25 antibodies; and JAK inhibitors.44 The immune microenvironment is a dynamic network of local immune cells, stromal cells, the extracellular matrix, and soluble factors within the transplanted organ that directly determine the fate of graft tolerance or rejection.10–12 These drugs have systemic immunosuppressive effects, which they achieve by blocking T-cell activation, cytokine signaling, and lymphocyte proliferation pathways. Table 1 summarizes the mechanisms of action, clinical applications, and limitations of traditional immunosuppressants. The significant side effects of traditional treatments, particularly long-term systemic immunosuppression, have limited their further clinical application. Studies have confirmed that corticosteroids, mTOR inhibitors, and calcineurin inhibitors significantly increase the risk of skin cancer, raising safety concerns.3 Analysis of bronchoalveolar lavage fluid from lung transplant rejection patients using single-cell RNA-seq and TCR sequencing revealed oligoclonal expansion of recipient-derived cytotoxic CD8⁺ T cells during rejection. Although high-dose glucocorticoid therapy reduced the expression of these cytotoxic mediators, the clonal cells were not eliminated. Instead, the cells transformed into tissue-resident memory T cells (TRMs) within the allograft and persisted in the peribronchial space.23 Calcineurin inhibitors (CNIs), such as cyclosporine A (CsA) and tacrolimus (Tac), are key immunosuppressive drugs used to prevent rejection after solid organ transplantation. However, they can impair transplanted kidneys due to their significant nephrotoxic side effects.45–47 Mycophenolate mofetil, a highly effective prescription medication, is an antiproliferative immunosuppressant that frequently causes gastrointestinal side effects of unknown origin.48–50 mTOR inhibitors (sirolimus and everolimus) may cause drug-induced pneumonia (DIP), which is a toxicity related to the class of drugs. Sirolimus and everolimus are also representative drugs among them.51,52 The core mechanism involves abnormal immune activation due to inhibition of the mTOR pathway, which leads to lymphocytic alveolitis and interstitial infiltration. Computed tomography (CT) features include diffuse exudative/ground-glass opacities. Clinical data indicate: Incidence: - Radinol: 11% (13/122)- Sirolimus: 5% (4/77).53 In addition, biologics (such as anti-CD25 antibodies) and JAK inhibitors (such as tofacitinib) play an important role in combating immune rejection during organ transplantation, but their side effects still need to be taken seriously. This is introduced in Table 1.54,55 Hricik, DEet al, conducted a randomized, double-blind, controlled trial using infliximab in kidney transplantation research. Although infliximab is commonly used to treat autoimmune diseases, the drug was found to double the risk of infection in kidney transplant studies due to its ability to weaken the immune system’s defenses. This finding underscores the need for caution when using drugs for different conditions.56 A Phase II study examined a new combination therapy for preventing bone marrow transplant rejection. The new regimen, which includes cyclophosphamide, tacrolimus, and mycophenolate mofetil, demonstrated significantly greater efficacy in preventing graft-versus-host disease (GVHD) than the traditional baseline regimen of tacrolimus and methotrexate. During the critical first year after transplant, patients receiving the new regimen experienced fewer and milder episodes of GVHD and were able to stop taking anti-rejection medications earlier. However, there was no significant change in overall survival or cancer recurrence rates.57
 |
Table 1 Mechanism of Action, Clinical Applications, and Limitations of Traditional Immunosuppressants |
Traditional immunosuppressants are fundamental to graft survival because they broadly inhibit key pathways in the immune microenvironment. However, their nonspecific mechanisms of action result in severe side effects and therapeutic limitations. These limitations underscore the urgent need for novel intervention strategies with high targeting specificity and controllable side effects. Is there a better option?
Emerging Intervention Strategies
Emerging strategies that focus on reshaping the transplant immune microenvironment and targeting key immune regulatory nodes aim to overcome the limitations of traditional immunosuppression and achieve more precise, safe, and durable transplant tolerance. These strategies include microbiome modulation, novel biologic agents, and nanotechnology interventions, which are innovative directions in current transplant immunology research.
The regulation of the microbiome before and after transplantation is an area that requires further exploration. The microbiome profoundly influences organ transplant recipients. The dynamically evolving microbial community continuously engages in a “dialogue” with the host’s immune system, directly determining whether the graft and host can achieve “peaceful coexistence”.58 After a lung transplant, the lung microbiome shows signs of dysbiosis, including higher microbial abundance and altered composition.59 Lei and his team discovered that normal mice undergoing skin and heart transplants exhibited the most intense and rapid rejection responses to the new organs. Meanwhile, germ-free mice and those injected with antibiotics showed slower and weaker responses. Therefore, reducing the microbial community temporarily prior to transplantation can increase the chances of success.60 Emerging strategies, such as microbiome interventions, offer novel approaches to transplant tolerance by reshaping the environment of the immune dialogue. However, challenges remain regarding their clinical application, including the precision of microbial targeting and the development of personalized regulatory protocols.
Biologics are a class of drugs produced through biotechnology that specifically target key molecules or cells within the immune system. Below are the primary biologics and their mechanisms of action. In kidney transplantation, anti-T cell antibodies (such as rabbit anti-thymocyte globulin, rATG) are widely used to treat acute rejection resistant to glucocorticoids. Studies indicate that early administration of rATG significantly improves long-term graft function, with efficacy unaffected by Banff classification or rejection severity. Additionally, anti-T cell antibodies reduce acute rejection incidence by decreasing T cell receptor (TCR) turnover.61,62 Anti-B cell antibodies, such as rituximab, reduce antibody-mediated rejection by eliminating B cells. Although rituximab has demonstrated efficacy in treating chronic antibody-mediated rejection, its long-term effects require further investigation.63 Patients who receive solid organ transplants usually need long-term immunosuppressive therapy to prevent rejection of the transplanted organ. However, this immunosuppressed state increases their risk of developing cancer. The use of ICIs may disrupt this immune balance, potentially triggering rejection of the transplanted organ. Studies indicate that ICIs are associated with graft rejection rates as high as 40% in transplant recipients.64 Cytokines, such as IL-10, play a crucial role in immune tolerance. Genetically engineered anti-CD25/IL-10/CXCR3 fusion proteins can stimulate the production of regulatory T cells (Tregs) and inhibit the differentiation of Th1 and Th17 cells. This mitigates rejection reactions.65 Although immune checkpoint inhibitors have revolutionized cancer treatment, they carry a significant risk of transplant rejection in recipients of solid organ transplants.
Cell therapy involves extracting living cells from the body, modifying their functions, and/or expanding them in vitro. The cells are then reinfused into the patient to treat specific diseases. This technique has been used to treat hematological malignancies and immunological disorders. FOXP3+ regulatory T cells (Tregs) play a crucial role in maintaining immune tolerance and tissue homeostasis. These cells control immune responses by suppressing T cell activation and regulating antigen-presenting cells. They also promote tissue repair. Deficiencies in Treg function or numbers can predispose individuals to autoimmune and inflammatory diseases, including kidney disorders. Therapeutic approaches include expanding endogenous Tregs (eg, with IL-2) or using adoptive cell therapy involving ex vivo modification and expansion, such as generating antigen-specific or CAR-Treg cells, to treat immune disorders and induce transplant tolerance.21 Chimeric antigen receptor (CAR) technology has revolutionized adoptive cell therapy (ACT) by reprogramming cellular targeting and significantly enhancing precision while reducing off-target effects observed in tumor CAR-T therapies. CARs applied to regulatory T cells (Tregs) are called CAR-Tregs. The goal is to harness their immunosuppressive functions to treat autoimmune diseases, graft-versus-host disease (GVHD), and organ transplant rejection. CAR-Tregs show significant potential in inducing transplant tolerance. However, compared to CAR-T, research on CAR-Tregs is in its infancy, and their design and application are shrouded in uncertainty.66
Against this backdrop, nanotechnology emerges as a pivotal force in overcoming existing limitations thanks to its precise delivery, intelligent response, and ability to regulate multiple targets. We will further explore its innovative applications in suppressing immune rejection.
Therapeutic Approaches Corresponding to Nanoscale and Molecular Mechanisms
Nano-Drug Delivery for Immune Microenvironment Modulation
Immune rejection remains the primary obstacle to successful allogeneic organ transplantation. Traditional strategies for modulating the immune microenvironment have significant limitations. One limitation is poor local targeting. Systemic administration has difficulty acting precisely on the transplant site, resulting in inadequate efficacy and pronounced systemic side effects. (2) Limited regulatory approaches: There is difficulty addressing the complex, networked interactions formed by multiple cell types (eg, T cells, dendritic cells, and macrophages) and multifactorial elements (eg, pro-inflammatory and anti-inflammatory cytokines) within the immune microenvironment. (3) Short duration of action: Exogenous immunomodulators are rapidly cleared or metabolized by the body, making it difficult to sustain long-term immune homeostasis. Nano-drug delivery platforms offer revolutionary solutions that overcome these limitations by providing unique advantages, such as localized high-concentration delivery, multifunctional target modification, and intelligent responsiveness.
Of all allogeneic organs, the liver exhibits the strongest relative immune tolerance. Researchers explored the mechanisms underlying this tolerance by comparing allogeneic transplantation mouse models of the liver, heart, and kidney. Transcriptomic analysis revealed that the liver graft microenvironment contains unique immune regulatory cell subsets. For example, CD11b+ dendritic cells within liver grafts were shown to suppress the activation of cytotoxic T cells by secreting anti-inflammatory cytokines, such as IL-10. This promotes the development of a locally tolerant microenvironment.67 To address the increased tendency for rejection in non-liver organ transplants, researchers have focused on using nanotechnology to create protective microenvironments. One innovative strategy is to engineer mesenchymal stem cell membrane-derived vesicles (MMVs) to specifically increase the expression of immune checkpoint molecules, such as Fas ligand (FasL) and programmed death-ligand 1 (PD-L1), on their surfaces. The functionalized MMVs are then cross-linked and immobilized within a hydrogel network to form MMV-gel complexes. This platform enables the MMVs to be retained at the transplantation site for a prolonged period. The sustained presentation of FasL and PD-L1 locally induces apoptosis in infiltrating allogeneic reactive T effector cells (Teff) and promotes the generation of regulatory T cells (Treg), effectively constructing an immune-protective microenvironment. Consequently, immune rejection is significantly suppressed and the survival of allogeneic transplants is protected.68 (Figure 3). The success of islet transplantation depends heavily on the precise regulation of the local immune microenvironment. Following implantation, islet grafts undergo an intense immediate blood-mediated inflammatory response (IBMIR) and are subsequently attacked by immune cells (eg, macrophages and T cells) and pro-inflammatory cytokines (eg, IL-1β, TNF-α, and IFN-γ). The release of these factors triggers a cascade amplification effect that further activates immune cells, ultimately leading to β-cell damage in the pancreas and transplant failure. Therefore, precisely intervening in the immune microenvironment surrounding the islet transplant to suppress harmful inflammatory cascades and immune activation is a core strategy for improving survival rates.69
 |
Figure 3 (a). Construction of engineered mesenchymal stem cell membrane-derived vesicles (MMVs): Gene editing up-regulates Fas ligand (FasL) and programmed death ligand 1 (PD-L1) on MMVs’ surface. MMVs are then modified with thiolated PEGylated phosphatidylethanolamine (DSPE-PEG-SH), enabling crosslinking with acrylated hyaluronic acid (a-HA) via thiol-acrylate Michael addition reaction. (b). MMV-Gel-mediated graft immune protection mechanism: Grafts encapsulated in MMV-Gel form a local immuno-protective microenvironment after transplantation. When alloreactive T cells infiltrate, MMVs’ FasL binds to T cells’ Fas receptor to induce apoptosis, and PD-L1 binds to T cells’ PD-1 receptor to promote T cell exhaustion. These dual effects inhibit immune rejection. (Reproduced from Wang et al, Nat Commun, 2024, 15:5176 with permission). |
In summary, nanomaterials can overcome the limitations of traditional methods through biomimetic design and intelligent response strategies. These nanomaterials enable the specific accumulation of drugs or modulators at the lesion site, achieve multi-target, synergistic regulation of immune cell and factor networks, and maintain long-lasting immune balance. These breakthroughs demonstrate that nanocarrier platforms have emerged as a pivotal strategy for precisely regulating the transplant immune microenvironment and have immense potential for clinical translation. Future research should focus on the long-term safety and efficacy of these platforms in large animal models and complex clinical settings. It should also focus on optimizing response strategies to accommodate individual variations and advancing the development of multimodal, synergistic therapeutic platforms.
Nanoparticle-Mediated T Cell Targeting for Rejection Suppression
T cells play a key role in adaptive immune responses, and precisely regulating their activation and function is essential for maintaining immune homeostasis. T cell activation depends on the specific recognition of antigen peptides bound to major histocompatibility complex (MHC) molecules by the T cell receptor (TCR). It also depends on secondary signaling via co-stimulatory molecules, such as CD28/B7, and the subsequent intracellular signaling cascades triggered by these signals. Meanwhile, immune checkpoint molecules, such as programmed cell death protein 1 (PD-1) and cytotoxic T lymphocyte-associated protein 4 (CTLA-4), suppress excessive T cell activation through negative signaling regulation. This ensures that immune responses are appropriate.
Regulatory T cells (Tregs) are key inducers of immune tolerance to transplants. Research indicates that Tregs effectively suppress allogeneic immune rejection and promote tissue repair and regeneration by inducing M2 macrophage polarization through the secretion of specific cytokines, such as TGF-β and IL-10.70,71 A traditional approach to preventing transplant rejection is to extend graft survival by suppressing or eliminating immune cells non-specifically. However, nanocarrier-mediated targeted immunosuppression strategies demonstrate superior potential. For example, poly(lactic-co-glycolic acid) (PLGA)-based nanoparticle delivery systems enable the selective depletion of specific immune cell subsets, which significantly prolongs graft survival in allogeneic skin transplant models.72 On the other hand, traditional approaches based on therapeutic antibodies to eliminate B or plasma cells often result in poor patient outcomes for antibody-mediated rejection (ABMR). Targeting specific T cell subsets is an effective strategy for suppressing rejection. Follicular helper T cells (Tfh) play a crucial role in promoting antibody production and chronic rejection and are a key intervention target. Functionalized mesoporous nanoparticles can deliver the immunosuppressant tacrolimus (Tac) efficiently to helper T (CD4+) cells, which significantly inhibits Tfh cell differentiation following allogeneic antigen exposure. This strategy reliably prevented rejection in a mouse kidney transplantation model.73 Exosome-like nanovesicles (NVs) have been found to exhibit dysregulation of splenic immune checkpoint molecules, such as PD-L1/PD-1 and CTLA-4/CD80, in cardiac and skin transplantation models. Based on these findings, researchers developed bioengineered PD-L1/CTLA-4 dual-targeted NVs that bind specifically to PD-1 on T cell surfaces and to CD80 on dendritic cell surfaces. Studies have demonstrated that these dual-targeted NVs effectively suppress CD8+ T cell density and cytokine secretion, enrich Treg cell populations, and significantly prolong transplanted organ survival. This is due to the synergistic enhancement of two critical immunosuppressive pathways: PD-L1/PD-1 and CTLA-4/CD80. These pathways have been shown to markedly reduce T cell activation and proliferation in both in vitro and in vivo studies.74
The nano-platform-induced and amplified regulatory T cells (Tregs) represent a core strategy for establishing tolerance. In vivo tracking studies reveal the role of innate immune cells in the homing of polyclonal human Tregs.75 Preclinical studies have confirmed that the adoptive transfer of regulatory T cells (Tregs) effectively prevents graft rejection, and early clinical trials have demonstrated its safety. Consequently, using nanotechnology to precisely modulate Treg function and numbers has become a promising area of research. One such approach is the use of tolerogenic artificial antigen-presenting cells (aAPCs or TolAPCs) based on poly(lactic-co-glycolic acid)/poly(β-amino ester) (PLGA/PBAE) loaded with transforming growth factor-β (TGF-β). These cells effectively promote the in vivo phenotypic polarization of regulatory T cells and enhance their immunosuppressive function76 (Figure 4). The curcumin-based nanocarrier platform significantly enhanced FoxP3 gene expression and Treg activity in patients with ankylosing spondylitis (AS), suggesting its potential application in the field of transplant immunology.77 PLGA nanoparticles loaded with the house dust mite allergen Der p 1 and the insulin-like growth factor 1 (IGF-1) (Der p 1/IGF-1 NPs) have been shown to effectively promote Treg cell differentiation in vitro, offering a novel approach to restoring immune tolerance function.78 Furthermore, nanoparticles (NPs) loaded with IL-2 and TGF-β and targeting T cells successfully induced the generation of polyclonal Treg cells, protecting mouse models from graft-versus-host disease (GvHD). Mechanistic studies revealed that reduced allograft reactivity coincided with a several-fold expansion of CD4+ and CD8+ Treg cells in NP-treated mice, alongside the acquisition of a tolerant phenotype by recipient dendritic cells.79
 |
Figure 4 Schematic illustration of the mechanism for regulating the function of regulatory T cells (Treg) based on nanotechnology. Preclinical models have demonstrated that adoptive transfer of regulatory T cells (Treg) can effectively prevent graft rejection, and its safety has been supported in preliminary clinical trials. Thus, using nanotechnology to precisely regulate the function or quantity of Treg has become a highly promising direction. As shown, poly(lactic - co - glycolic acid)/poly(β - amino ester) (PLGA/PBAE) - based artificial antigen - presenting cells (aAPCs, TolAPC) loaded with transforming growth factor - β (TGF - β) can effectively promote the phenotypic polarization of Treg cells in vivo and enhance immunosuppressive function through the synergistic effect of surface signals.1 Adapted from the article “Biomimetic tolerogenic artificial antigen presenting cells for regulatory T cell induction” by Rhodes K R, Meyer R A, Wang J, Tzeng S Y, Green J J, published in Acta Biomaterialia (Volume 112, August 2020, Pages 136–148), used with permission. |
In summary, the targeted modulation of T cell function via nanotechnology, particularly through the depletion of pathogenic subsets, the induction or expansion of immunosuppressive regulatory T (Treg) cells, and the enhancement of immune checkpoint inhibition pathways to suppress transplant rejection, has emerged as a key research focus in transplant immunology. Compared to traditional non-specific immunosuppression, these strategies demonstrate higher selectivity and potentially lower toxicity. In conclusion, multi-targeted, combined strategies represent the future direction. Nanotechnology-based research on immune tolerance induction is rapidly emerging. One frontier of this research is the development of “tolerogenic vaccines.” Rather than enhancing immune responses, the objective of these vaccines is to use engineered nanoparticle platforms to deliver specific antigens or immunomodulatory molecules to actively induce antigen-specific immune tolerance.5,80,81 For instance, the modification of therapeutic antigen peptides with polyethylene glycol significantly reduces the inflammatory response induced by peptide-based tolerance vaccines. This provides a theoretical foundation for the safe and effective application of these vaccines in the treatment of autoimmune diseases, allergies, and transplant rejection.82 In summary, strategies for the targeted depletion of specific pathogenic T cell subsets and the effective induction and expansion of Tregs using nano-platforms are relatively mature and reliable. Dual/multi-target immune checkpoint synergistic regulation strategies show tremendous potential. Engineered “tolerogenic vaccines” represent a new paradigm for inducing antigen-specific tolerance. Future research presents both challenges and opportunities and requires focused efforts to enhance the potential for clinical translation. Key priorities include improving biomaterial safety, optimizing carrier targeting, and achieving scalable production. Further exploration is needed into the mechanisms of nanoplatform-mediated precise T cell reprogramming and expanding synergistic therapeutic approaches with other tolerance-inducing pathways, such as non-T cell pathways, which are discussed below.
Nanoscale Effects on Macrophage Function
As core effector cells of the innate immune system, macrophages serve as key regulators that mediate early post-transplant inflammation and immune rejection.83 As research has progressed, the molecular mechanisms by which graft-infiltrating myeloid cells mediate rejection have gradually become clearer. Upon exposure to allogeneic grafts, recipient monocytes rapidly differentiate into functionally heterogeneous macrophage subpopulations, where polarization toward Ly6C⁺ regulatory macrophages (Mregs) has been shown to significantly attenuate rejection by suppressing effector T cell activation and promoting regulatory T cell (Treg) expansion. Conversely, polarization toward M2 macrophages has been demonstrated to markedly inhibit rejection.84–87 (Figure 5).
 |
Figure 5 Schematic of myeloid cell regulatory mechanisms in graft immunity. Combining mTORi-HDL therapy with CD40-TRAF6-specific nanobiota (TRAF6i-HDL) revealed that short-term mTOR-specific high-density lipoprotein (HDL) nanobiota therapy (mTORi-HDL) can prevent aerobic glycolysis of macrophages and epigenetic modifications resulting in inflammatory cytokine production. The resulting regulatory macrophages can prevent allogeneic reactive CD8+ T cell-mediated immune responses and promote the expansion of tolerant CD4+ regulatory T cells (Tregs). Reproduced from (Braza et al, 2018, Immunity 49: 819–828) with permission from Immunity. |
The introduction of nanomaterials offers novel strategies for precisely regulating macrophage polarization. Current research achieves immune regulation through three major pathways. The first approach is the polarization-suppressive pathway. In a liver transplantation-associated ischemia-reperfusion injury (IRI) model, platinum nanozymes (Pt-iNOS@ZIF) exert the following pleiotropic effects: they not only efficiently scavenge reactive oxygen species (ROS) generated by neutrophil infiltration via peroxidase-mimetic activity, but also sustainably release nitric oxide (NO) at physiologically relevant concentrations. Ultimately, while downregulating the expression of tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), Pt-iNOS@ZIF simultaneously blocks the signal transducer and activator of transcription 1/interferon regulatory factor 5 (STAT1/IRF5) signaling axis. This strategy enables precise modulation of the local microenvironment, thereby significantly reducing the incidence of acute immune rejection.88 The second strategy entails M1 phenotype reprogramming. He et al engineered RBCM@CeO2/TAK-242 nanoparticles with a biomimetic delivery system, which circumvents clearance by the mononuclear phagocyte system (MPS) via specific recognition of the CD47 molecule on the red blood cell (RBC) membrane. Specifically, TAK-242 blocks toll-like receptor 4 (TLR4) receptors, thereby potently inhibiting TLR4 dimerization. In parallel, CeO2 nanozymes scavenge reactive oxygen species (ROS) in the nuclear factor kappa-B (NF-κB) signaling pathway, which in turn prevents inhibitor of nuclear factor kappa-B alpha (IκBα) degradation and p65 nuclear translocation. These synergistic actions markedly reduce the positivity rate of M1 phenotypic markers (CD86⁺/HLA-DR⁺), while concomitantly boosting the secretion of the anti-inflammatory cytokine interleukin-10 (IL-10). This nanoplatform effectively overcomes the limitations of free TAK-242, such as a short half-life and off-target toxicity.89 The third approach focuses on M2 polarization induction. Graphene oxide nanomaterials exert dual physical and biochemical regulatory effects: structurally, they inhibit matrix metalloproteinase (MMP) activity, mimic the natural mechanical microenvironment of liver tissue, enhance elastic modulus, and improve scaffold stability; biochemically, they activate the integrin β1-FAK axis and trigger the PI3K/Akt pathway, which drives signal transducer and activator of transcription 6 (STAT6) phosphorylation. This phosphorylation induces the expression of M2 phenotypic markers (Arg-1⁺/CD206⁺) and promotes M2 polarization, allowing interleukin-10 (IL-10)-loaded engineered liver grafts to effectively suppress inflammation and facilitate tissue repair.90
Notably, this polarization-based regulatory strategy is equally effective in autoimmune diseases. The LDH-CeO2 nanocatalytic platform efficiently transforms M1 to M2 in rheumatoid arthritis models through acid neutralization and metal ion bioactivity, providing a cross-disease-validated theoretical foundation for extending autoimmune disease regulation approaches to transplantation.91 Current research confirms the significant potential of nanoparticle drug delivery systems in reducing transplant rejection, preserving graft function, and promoting tissue regeneration through the polarization of macrophages. However, challenges remain in achieving spatiotemporal precision in polarization regulation, assessing the long-term biosafety of nanoparticle carriers, and validating their effectiveness across organ transplantation systems. Future research should focus on developing organ-specific delivery systems, identifying new targets such as epigenetic regulation, and translating laboratory findings into clinical applications.
Nanoparticles: Antioxidation, IRI Mitigation and Tissue Repair
During organ transplantation, IRI is a major unavoidable challenge. Its core mechanism is destructive oxidative stress. Ischemia during organ procurement leads to hypoxia and the collapse of energy metabolism. When blood flow is restored during reperfusion, impaired mitochondrial function triggers the explosive production of reactive oxygen species (ROS), which disrupts the balance between oxidation and antioxidants. Common approaches to counteract this phenomenon include antioxidant therapy for donors and recipients, antioxidant treatment of the graft, and enhancing ischemic tolerance to protect the transplant process.92 Traditional antioxidants, such as edaravone, have short half-lives and difficulty penetrating the blood-brain barrier. However, nanotechnology offers three actions: scavenging free radicals, regulating endogenous antioxidant enzymes, and suppressing inflammation. The advantages of nanotechnology—precision delivery, smart responsiveness, efficient drug loading, and multifunctional integration—provide innovative solutions to these challenges through two primary mechanisms.
Nanoparticle Regulation of Oxidative Stress and IRI
As a core driver of IRI, oxidative stress damages cellular structures directly and activates multiple harmful signaling pathways. Nanotechnology interventions focus on multi-target, synergistic effects to mitigate oxidative stress-related damage effectively, primarily through the following mechanisms:
A prominent mechanism is targeted delivery and efficient cellular uptake. Studies have shown that targeted rapamycin micelles (TRaMs), synthesized from poly(ethylene glycol)-poly(ethylene imine)-amine (PEG-PEI-amine) and N-palmitoylhomocysteine (PHC), have a diameter of approximately 10 nm and are functionalized with far-red fluorescent labeling. These characteristics significantly enhance their internalization efficiency in human umbilical vein endothelial cells (HUVECs), with further improvements observed upon the addition of specific targeting groups. This strategy effectively reduces the production and release of pro-inflammatory cytokines, including interleukin-6 (IL-6) and interleukin-8 (IL-8), in both mouse cardiac endothelial cells (MCECs) and HUVECs under normoxic and hypoxic conditions.93
Secondly, issues of delivery efficiency optimization and organ protection must be addressed. Taurine has been demonstrated to alleviate acute liver injury induced by hepatic ischemia-reperfusion injury (IRI); however, its enrichment in target organs is limited after systemic administration. Recent studies have developed neutrophil membrane-coated taurine nanoparticles (nano-taurine), which significantly enhance targeted accumulation and bioavailability in damaged liver tissue. Experimental results confirm that nano-taurine substantially reduces serum levels of aspartate transaminase (AST) and alanine transaminase (ALT), mitigates tissue damage, and restores liver function.94 Similarly, in a renal IRI model, the oral administration of nano-silicon (nano-Si) particles significantly reduced levels of serum creatinine, urinary protein, and oxidative stress markers (urinary 8-hydroxy-2’-deoxyguanosine). Transcriptomic and gene ontology enrichment analyses revealed that nano-Si intake downregulates oxidative stress-related biological processes. Immunohistochemical analysis confirmed its immunomodulatory effects (inhibiting interstitial macrophage infiltration) and anti-apoptotic actions (reducing tubular cell apoptosis).95
The next critical mechanism involves mitochondrial-targeted repair and restoration of function. In an innovative study, ischemia-targeted peptides (PEPs) were combined with a mitochondrial-targeted cation (TPP⁺) to form a PEP-TPP-mitochondria complex. This complex successfully transported functional mitochondria into ischemic myocardial tissue (PEP-mediated homing). The mitochondria were then delivered to cardiomyocytes via endothelial cells, which significantly improved their respiratory function and mechanical contractility. In a mouse myocardial IRI model, the intravenous administration of the complex demonstrated superior acute-phase protection, significantly improving cardiac function and reducing infarct size, as well as a favorable long-term prognosis. In vitro experiments confirmed its efficacy in mitigating hypoxia-reoxygenation injury in cardiomyocytes. Mechanistic studies revealed that the complex inhibits cardiomyocyte apoptosis by downregulating cleaved caspase-3 expression and modulating the proapoptotic protein (Bax)/anti-apoptotic protein (Bcl-2) ratio, while simultaneously suppressing the infiltration of CD11b⁺F4/80⁺ macrophages and reducing the expression of key inflammatory factors (NLRP3, IL-6, and cleaved IL-1β). These effects mitigate inflammatory cascade damage and maintain myocardial tissue homeostasis.96 After lung transplantation, ischemia-reperfusion injury (IRI) often leads to primary graft dysfunction. Given the limitations of existing ex vivo lung perfusion (EVLP) techniques, a team developed a targeted and ROS-responsive nanotherapeutic platform, SOD2-Fer-1@CVs hybrid vesicles. This platform clears reactive oxygen species (ROS) by overexpressing superoxide dismutase 2, inhibiting oxidative damage-mediated endothelial cell apoptosis, and simultaneously inhibiting ferroptosis, thereby protecting mitochondrial function.97
Last but certainly not least is the synergistic role of immune regulation and antioxidant mechanisms. In cases of transplantation where immune rejection is a prominent issue, nanostrategies demonstrate potent immune-modulating functions that counteract IRI synergistically. For example, immune rejection is the primary cause of graft failure in corneal transplantation.98 Rapa-loaded nanomicelle eye drops (RAPA-NM) have been shown to prevent allogeneic corneal transplant rejection effectively by inhibiting NLRP3 inflammasome activation specifically.99 Further characterization studies confirm that the RAPA-NM developed based on PVCL-PVA-PEG exhibits excellent membrane permeability, cell compatibility, and biostability.100 A study developed a novel delivery system (Met@PBN@Neu-CVs) for neutrophil membrane-coated Prussian blue nanozymes (PBN) and metformin (Met) to address IRI associated with liver transplantation/resection. This particle utilizes the properties of the neutrophil membrane to mediate targeted enrichment and adsorption of inflammatory factors, while the multi-enzyme activity of PBN clears ROS. Met and PBN synergistically repair mitochondrial function and induce macrophage polarization from M1 to M2. This system demonstrates excellent biocompatibility and provides a new approach for intervening in ischemia-reperfusion injury during future liver transplantation.38 In the field of kidney transplantation, inflammatory monocytes are the primary infiltrating cells in rejection reactions. Research indicates that polystyrene immunomodulatory nanoparticles (IMPs) with a diameter of 500 nm efficiently bind to inflammatory monocytes via the specific scavenger receptor MARCO. This significantly improves acute rejection in kidney transplant mouse models and enhances survival rates, demonstrating the IMPs’ potential clinical translational value.101 Quaternary ammonium phosphocholine-chitosan (PC-QCH) and tetrahydropyrantriazolobenzene-alginate (TZ-AL) form an immunoprotective nanocoating with an average thickness of ~540 nm via electrostatic self-assembly. This coating significantly reduces the secretion of pro-inflammatory factors (tumor necrosis factor-α, TNF-α; interleukin-6, IL-6) induced by exposure to THP-1 macrophage derivatives or RAW264.7 macrophages, while preserving the viability, metabolic activity, and insulin secretory function of MIN6 β-cell spheroids. Notably, the nanocoating also exerts a marked inhibitory effect on IL-6 secretion triggered by THP-1 macrophage derivatives or RAW264.7 macrophages. In vivo studies further demonstrated that this nanocoating restores normal blood glucose levels in diabetic NOD-SCID mice, highlighting its potential as an ideal candidate for cell-based therapy in type 1 diabetes.102 Similarly, transplanting alginate-microencapsulated porcine islets coated with a dexamethasone (Dexa)-containing chitosan coating into diabetic mice significantly suppressed perivascular fibrosis without impairing islet function or survival.103 A South Korean team developed an in vivo bioreactor (IVB) system comprising a silicone tube and a cellulose nano-pore membrane. This system has been demonstrated to effectively promote cartilage matrix synthesis, maintain cartilage phenotype, and delay calcification when implanted subcutaneously in the host and subsequently placed at the site of the cartilage defect. This system shows promise as an anti-rejection solution.104 Additionally, biomaterials such as nano-hydroxyapatite/polybutylene succinate-co-butylene glycol scaffolds exhibit excellent biocompatibility and controllable degradability. These materials can effectively suppress immune rejection caused by foreign body reactions. These materials have been extensively studied for use in orthopedic tissue engineering due to their superior mechanical properties, biocompatibility, and biodegradability.105
Strategies for Nanotechnology-Enhanced Graft Repair and Tissue Regeneration
Ensuring the long-term functional stability of grafts requires mitigating initial IRI/oxidative stress damage and actively promoting the effective repair and regeneration of injured tissues. Persistent IRI and immune rejection can severely impede tissue reconstruction. Nanotechnology plays a pivotal role in advancing graft repair and regeneration through multiple pathways, often synergistically enhancing immunomodulation.
The most prevalent related research involves using extracellular vesicles (EVs) as multifunctional therapeutic carriers. Various cell-derived EVs have demonstrated immunomodulatory, antioxidant, anti-inflammatory, and tissue-repairing properties. They mediate tissue repair and signaling pathway regulation through endocytosis by target cells. In IRI animal models, EV administration before, during, or after injury significantly reduces tissue damage and accelerates repair.106 In organ transplantation scenarios, the timing of extracellular vesicle (EV) administration can be flexible. Examples include pre-ischemia, the ex vivo organ preservation-perfusion period, and pre- or post-reperfusion. However, clinical applications require the optimization of EV dosage and administration frequency based on the type of IRI.106 Systemic infusion of mesenchymal stem cells (MSCs) has been shown to reduce transplant-associated injury through mechanisms that suppress inflammation, downregulate innate and adaptive immunity, and promote organ regeneration. Further studies reveal that delivering extracellular vesicles (EVs) during ex vivo dynamic organ preservation can overcome potential “device barrier” limitations. In lung and liver perfusion models, EVs have been shown to effectively enter cells, producing significant anti-inflammatory and regenerative effects.107 Compared to direct use of MSCs, EV therapy may offer greater efficiency advantages in promoting repair and regeneration of ex vivo preserved organs. Additionally, acellular EV therapy avoids risks associated with resident monocyte activation, malignant transformation, and recipient sensitization (observed in allogeneic stem cell transplantation).107
A crucial research direction involves engineering the production and functional optimization of extracellular vesicles (EVs). One study examined the impact of tauroursodeoxycholic acid (TUDCA) pretreatment on mesenchymal stromal cells (MSCs) and their secreted EVs. The study found that TUDCA significantly increased the production of MSC-EVs by over twofold by reducing intracellular cholesterol levels in MSCs and upregulating CAV1 expression. CAV1 is a protein associated with exocytosis. Notably, EVs derived from TUDCA-pretreated MSCs (T-EVs) exhibited higher levels of anti-inflammatory factors (IL1RN, IL6, IL10, and IL11) and osteogenesis-related proteins (ALP, RUNX2, BMP2, and BMPR1 and BMPR2) than controls (C-EVs). Functional validation revealed that T-EVs regulate monocyte differentiation into M2 macrophages and effectively promote MSC osteogenic differentiation. This significantly enhances bone tissue regeneration in rat bone defect models. This strategy opens new avenues for enhancing EV yield and functionality. T-EVs show promise as potent therapeutic materials for bone regeneration and could be applied to other tissue regeneration fields.108
A promising future research focus is utilizing smart bioscaffolds to mediate synergistic, multi-effect regeneration. Zinc gradient-doped ZnO-SiO2 nanofibers, which are constructed via electrospinning technology, self-assemble into three-dimensional composite aerogel scaffolds. These scaffolds feature a biomimetic, multi-level, ordered pore structure. The controlled release of their synergistic Si4⁺/Zn2⁺ ions and aspirin effectively activates the endothelial cell-mesenchymal stem cell interaction network, promoting both angiogenesis and osteogenesis simultaneously. Additionally, they induce M2-type macrophage polarization and downregulate TNF-α expression, actively regulating the inflammatory microenvironment. These intelligent scaffolds integrate both “angiogenic-osteogenic dual induction” and “immunomodulation” functions, offering an innovative solution for complex bone defect regeneration.109 In spinal cord injury repair, a functional hybrid gelatin/hyaluronic acid hydrogel (F-G/H), which is modified with cationic polymers and anti-inflammatory cytokines, achieves perfect adhesion and matching through in situ gelation at both ends of allogeneic adult spinal cord tissue (aSCT) grafts. The F-G/H hydrogel can clear damage-associated molecular patterns (DAMPs), sustain the release of anti-inflammatory factors, and reduce lymphocyte infiltration. F-G/H effectively modulates the immune microenvironment at the transplant interface, enhancing aSCT survival and function. Combined with systemic immunosuppressants, F-G/H significantly improves motor function following rat spinal cord injury.100 A genetically crosslinked adipose-derived stem cell-derived extracellular matrix (ECM)-nanographene composite sponge has been developed to enhance the healing of difficult-to-heal wounds. These ECM scaffolds derived from cells have garnered significant attention due to their low risk of pathogen transfer and minimal tendency for immune rejection.110 In tissue-engineered tracheal reconstruction, polymer tissue scaffolds (PTS) that are constructed using optimized 3D-printed pore structures and surface modification techniques, such as the use of silica nanoparticles, have been shown to maintain structural integrity following allogeneic implantation in vivo. This approach significantly reduces the risk of acute immune rejection following implantation, revealing the immense potential of PTS as a material for tracheal reconstruction.111 An innovative strategy involving autologous, endogenous protein-modified gold nanorods (GNRs) is used in photothermal therapy (PTT) to treat fractures. The outermost layer of autologous proteins gives GNRs excellent immunocompatibility. Unlike PEG-modified counterparts, GNRs neither activate immune cells in vitro nor induce rejection reactions in vivo. Due to the effects of hemorrhaging and edema at fracture sites, GNRs rapidly accumulate in the affected area following intravenous injection. Under near-infrared (NIR) light irradiation, the mild photothermal effect generated by the accumulated GNRs effectively promotes fracture healing in mice. Transcriptome sequencing and validation experiments reveal that the osteogenic mechanism involves the activation of key signaling pathways (MAPK and PI3K-Akt) and the upregulation of multiple core osteogenic factors.112
In summary, nanocarrier drug delivery technology demonstrates diverse and highly effective strategies against transplant-related oxidative stress and IRI (such as targeted delivery of antioxidants, mitochondrial repair, and immune regulation coordination). Simultaneously, it provides multi-level, multifunctional solutions for promoting graft repair and tissue regeneration (such as optimizing EV therapy, constructing smart responsive scaffolds, and developing biocompatible materials). These approaches not only directly promote tissue structural recovery and functional restoration but also frequently synergize with mechanisms that suppress inflammation and precisely modulate immune responses. Together, they create favorable local and systemic environments conducive to long-term graft survival and functional stability. However, significant challenges remain in current research: (1) MSC-EV production efficiency remains insufficient to meet large-scale clinical demands; (2) The specific mechanisms of MSC-EV action in different tissue regenerations require further exploration; (3) Numerous promising nanocarrier strategies (eg, PEP-TPP-mitochondria, Nano-taurine, T-EV, autologous endogenous protein-modified GNRs) remain primarily in animal testing phases, with their clinical translation safety, efficacy, and scalable production processes requiring systematic validation. Future research must focus on overcoming these bottlenecks to accelerate the practical application of nanotechnology in transplant medicine.
Nanotechnology-Driven Immune Tolerance
The ultimate goal of organ transplantation is to achieve donor-specific tolerance. This means that the recipient’s immune system will selectively silence graft antigens while still being able to defend against pathogens.113 Unlike traditional immunosuppressive systemic suppression strategies, this process fundamentally restores dynamic equilibrium through active immune regulation. Leveraging its programmable physicochemical properties, nanotechnology has pioneered a dual-track tolerance induction paradigm combining “active induction and passive exemption”.74,114 This section will systematically elaborate on innovative tolerance strategies that go beyond direct T cell intervention (as discussed in Section 4.2).
Active Immunomodulatory Mechanism of Nanoplatforms
Micron- and nanoscale drug delivery systems made of biomaterials, such as poly(lactic-co-glycolic acid) (PLGA), significantly reduce the required dosage of drugs and minimize systemic toxicity by enabling the controlled release and targeted delivery of pharmaceuticals.113 As a classic carrier, PLGA can bypass non-specific adverse reactions and suppress immune responses to allogeneic transplants.113
Early studies established the use of a tacrolimus (Tac)-loaded collagen hydrogel (Col/Tac) for the targeted delivery of Tac in spinal cord injury repair via a local, sustained-release system. In a rat model of complete transverse spinal cord injury, combining this strategy with allogeneic adult spinal cord tissue (aSC) transplantation significantly enhanced local immune regulation efficiency (eg, reduced T-cell infiltration and the inflammatory response) and substantially reduced tacrolimus’s systemic toxicity (eg, hepatic and renal dysfunction). Further studies confirmed that the mechanical properties of the Col/Tac hydrogel (eg, energy storage modulus and stability) and Tac’s sustained-release kinetics are critical to ensuring therapeutic efficacy.115 (Figure 6). Subsequent studies further explored the targeting of signaling pathways. The histidine-grafted poly(β-amino ester) nanocarrier induces liver transplant tolerance by inhibiting the signaling of MyD88. In MyD88-deficient models, the nanocarrier significantly prolonged recipient survival, reduced graft rejection, and decreased serum levels of IL-2 and IFN-γ.116
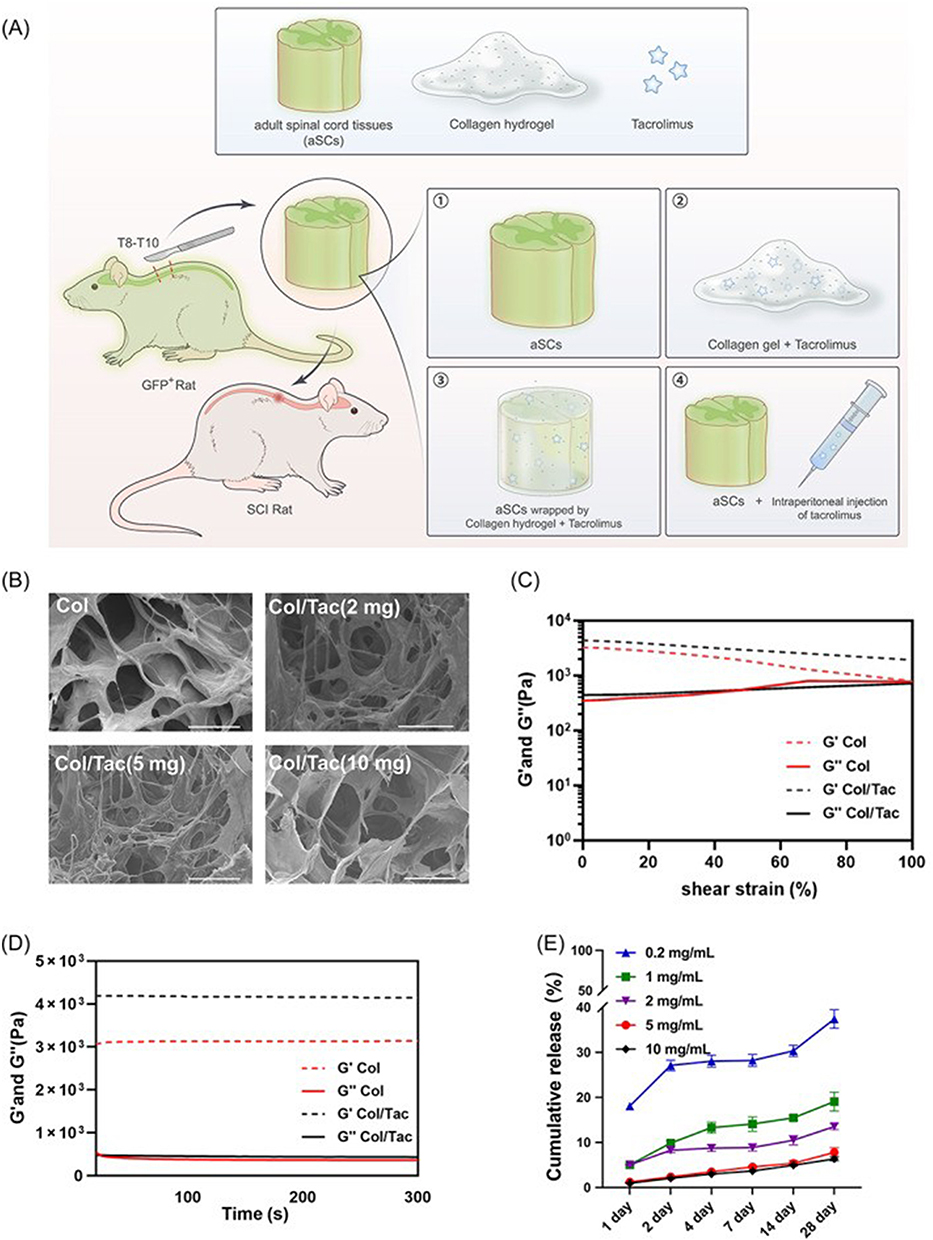 |
Figure 6 (A) A collagen hydrogel (Col/Tac) system loaded with tacrolimus (Tac) was constructed for local sustained release in spinal cord injury (SCI). Precise delivery of tacrolimus and regulation of the immune microenvironment were achieved by encapsulating allogeneic adult spinal cord tissues (aSCs) and filling the host-graft interface. Rats with SCI underwent the following treatments: 6(A) ① Adult spinal cord tissue transplantation; 6(A) ② Collagen/tacrolimus hydrogel transplantation; 6(A) ③ Adult spinal cord tissue combined with collagen/tacrolimus hydrogel transplantation; 6(A) ④ Adult spinal cord tissue transplantation combined with intraperitoneal injection of tacrolimus. 6(B) Scanning electron microscopy image of the collagen/tacrolimus hydrogel (scale bar = 100 μm). 6(C) Shear strain curves of the collagen hydrogel and collagen/tacrolimus hydrogel scaffold, and 6(D) Modulus. 6(E) In vitro release of tacrolimus from collagen hydrogel (n=3). Schematic diagrams and data reproduced from (Zhao et al, 2023) with permission from Cell Proliferation (DOI: https://doi.org/10.1111/cpr.13451). |
Subsequently, the multi-target synergistic mechanism demonstrated outstanding performance. PD-L1/CTLA-4 dual-targeted nanovesicles (NVs) inhibited T cell activation by blocking the PD-L1/PD-1 and CTLA-4/CD80 immune checkpoints simultaneously. This design significantly reduced T-cell proliferation in both in vitro and in vivo experiments compared to single-target strategies, thereby prolonging the survival of skin and cardiac grafts in mice.74 In the field of liver cancer treatment, poly(chitosan)-cisplatin (PC-CP) demonstrates superior permeability and weaker foreign body reactions compared to polyethyleneimine-cisplatin (PEI-CP). By enhancing regulation through the mTOR/P-Akt/LC3/p53 pathway, it significantly improves tumor apoptosis efficiency. This confirms the targeted impact of carrier material properties on therapeutic efficacy, offering a novel approach for liver cancer transplantation.117
The aforementioned broad immunosuppressive strategies have achieved remarkable success in controlling acute rejection. However, their non-specific nature may lead to risks associated with systemic immunosuppression, such as infections and tumors. Therefore, the ideal goal for achieving long-term graft survival is to induce antigen-specific immune tolerance against specific transplant antigens. Tolerance vaccines are a key strategy for achieving this goal using nanotechnology platforms that precisely manipulate antigen presentation and immune cell fate decisions. Efficiently inducing antigen-specific tolerance requires the targeted delivery of transplant-associated antigenic epitopes to dendritic cells (DCs), which are key cells responsible for antigen presentation. PEGylated antigen-peptide-liposome complexes exemplify this approach. This system achieves exceptionally efficient antigen delivery by actively targeting CD11c⁺ DCs in lymph nodes. Studies confirm that this approach enhances MHC-II-mediated antigen presentation efficiency by several orders of magnitude and induces apoptosis in highly antigen-specific T cells. This potent effect establishes a robust immunological foundation for achieving long-term, specific graft tolerance.82 In addition to controlling the quantity and location of antigen presentation, another core strategy for inducing tolerance is reprogramming the differentiation state of immune cells to promote the generation and function of regulatory T cells (Tregs). Histone modifications play a pivotal role in regulating gene expression. Nanoparticles loaded with the histone deacetylase inhibitor trichloroacetic acid (TSA) have been developed to epigenetically reprogram immune cells. They specifically target the promoter region of the FoxP3 gene, significantly enhancing histone H3K9 acetylation in this area. This critical epigenetic modification strongly upregulates the expression of a series of Treg-associated functional genes, achieving profound epigenetic remodeling of the T cell functional profile. This transformation shifts the profile from an effector to a regulatory state.81 Furthermore, gene editing and nanocarrier synergy have emerged as precise tools for active tolerance induction. Nanoplatforms can serve as either viral or non-viral delivery vectors to target key immunoregulatory molecules. Adenovirus nanoparticles efficiently deliver the heme oxygenase-1 (HO1) gene to grafts, reducing the release of damage-associated molecular patterns (DAMPs) like HMGB1 and prolonging islet transplant survival in rodent models without systemic immunosuppression.118 Non-viral carriers such as liposomal nanoparticles, via surface functionalization, can specifically target transplanted endothelial cells to mediate CRISPR knockout of MHC-II genes, successfully inducing local immune privilege in non-human primate models.119 While viral vectors offer high delivery efficiency, their inherent immunogenicity and insertion mutation risks limit application; non-viral carriers boast superior biosafety but require further optimization of targeting precision and delivery efficacy for clinical translation.
Addressing post-transplant infections that exacerbate rejection, dual-functional antibacterial-immune nanomaterials integrate infection control with immune modulation to reinforce active tolerance. Nano-titanium dioxide (nTiO2)-based composite bone graft scaffolds generate reactive oxygen species (ROS) via photocatalysis to eliminate pathogens, while surface hydroxyl groups modulate the TLR signaling pathway, inducing macrophage M2 polarization and mitigating local inflammation.120 Silver-based immunomodulatory coatings on porous zirconia implants enable sustained Ag⁺ release to inhibit biofilm formation, simultaneously reducing excessive neutrophil infiltration and pro-inflammatory cytokine storms to synergistically alleviate foreign body reactions.121 These materials break the infection-rejection vicious cycle, expanding the application scenarios of active tolerance strategies.
Passive Exemption: Bionic Barriers and Physical Isolation
Using nanomaterials to build physical barriers that protect drugs from host immune recognition can reduce drug dependency and avoid side effects. There are currently three approaches to this strategy:
Researchers prepared a laminin/Vitrogen/type IV collagen composite nanomembrane (NB-LVF4, with a thickness of approximately 200 nm) that achieved 90% coverage of the renal vascular endothelium within three hours of in vitro perfusion. In a canine kidney transplantation model, this barrier significantly delayed the onset of rejection from six days to 30 days without the use of systemic immunosuppression. These studies primarily focus on vascular interface engineering.114
Another approach involves modifying the surface of the implant to create a dual-functional, antibacterial-immune coating. According to research findings, micro-nano porous silver-coated implants can enhance antibacterial properties through sustained release of Ag⁺ ions, while their porous structure promotes bio-sealing formation. This achieves dual-pathway regulation to avoid immune responses.121 In contrast, polyvinylpyrrolidone-iodine (PVP-I) solution treatment of allogeneic grafts operates on a slightly different principle. It simultaneously enhances mechanical properties and osteogenic activity by optimizing surface characteristics and leveraging residual disinfectants retained through surface immersion.122 Larger implants can be coated, and surface modification for smaller implants can be achieved through encapsulation techniques. As the following report describes, we envision future applications for implanting mechanical devices, such as pacemakers. Encapsulating islets in a functionalized polyethylene glycol (PEG) nanocoating enhances insulin secretion, shields islets from host immune responses to prevent graft rejection, and enables sufficient islet transplantation in minimal volumes to reverse diabetes. Therefore, it is essential to develop islet encapsulation strategies that minimize transplant volume.123 Encapsulating islets with biocompatible materials as an immune barrier holds great promise. However, clinical trials face limitations due to central hypoxia in islet beads, impurities within the beads, and issues with recyclability. Consequently, 3D bioprinting has emerged as a solution. Artificial pancreases can precisely position living cells at desired locations, enabling vascularization of the artificial pancreas. This novel approach aims to evade immune responses as much as possible.124
Biomarker Monitoring and Precision Regulation
Suppressing immune rejection effectively is crucial for successful transplantation. Real-time, precise monitoring of rejection occurrence and progression is vital for clinical decision-making. Early research in this field focused on identifying key biomarkers associated with acute rejection. For example, Japanese researchers were the first to use highly sensitive nano-liquid chromatography-tandem mass spectrometry (nanoLC-MS/MS) technology in liver transplantation. This approach successfully identified 11 antigens associated with rejection, four of which were detected specifically in patients with acute rejection (AR). These findings highlight their potential value as diagnostic markers and provide important targets for noninvasive clinical monitoring.125
A deep understanding of antigenic epitopes is fundamental to optimizing monitoring strategies. In the field of xenotransplantation, researchers have conducted precise characterizations of α-galactosylated O-glycan structures in porcine kidney and endothelial cells to overcome significant carbohydrate antigen barriers. Compared to previous findings, the clarity of this structural information will significantly advance clinical research targeting carbohydrate-mediated humoral immune rejection in xenotransplantation.126 Studies have confirmed that dynamic changes in donor-specific antibodies (DSAs) and autoantibodies are powerful prognostic indicators for islet transplantation. Elevated levels of these antibodies after transplantation are significantly associated with poor outcomes. Precise identification and monitoring of these antibodies hold clear clinical significance for improving the efficacy of islet cell transplantation.127 The introduction of imaging technology has revolutionized monitoring methods. Integrating 3D printing technology with near-infrared (NIR) fluorescence imaging pioneered a novel approach to assessing implant immunocompatibility in vivo, non-invasively, and dynamically. By tracking implant degradation behavior and changes in NIR signals within the surrounding tissue, one can indirectly reflect the intensity of the host’s immune response in vivo. The successful validation of this technique in a rat cranial bone defect model suggests it is a promising approach for addressing complex implant-related immune rejection issues.128 To precisely manage drug concentrations, researchers developed a novel quantitative method based on two-dimensional tungsten disulfide nanosheets (WS2 NSs) for laser desorption ionization mass spectrometry (LDI-MS). This method can accurately quantify trace immunosuppressants in blood samples from organ transplant patients. It offers high sensitivity, excellent reproducibility, and high-throughput analytical capabilities. This method provides a reliable tool for developing personalized medication regimens.129
In summary, current biomarker research and advanced technology development are deeply integrated and dedicated to constructing a comprehensive framework that encompasses drug concentration (eg, novel LDI-MS monitoring technology),129 key antigens (eg, antigen identification via nanoLC-MS/MS and α-galactosyl epitope structural information)126 — antibody response (eg, DSA and autoantibody monitoring)127 — tissue microenvironment changes (eg, responses revealed by near-infrared fluorescence imaging).128 Established technologies such as antibodies and mass spectrometry detection have been clinically validated as reliable. They deepen our understanding of rejection mechanisms and significantly enhance the precision and efficiency of assessing immune status and treatment efficacy over time. Future research should focus on the following: 1) deep mining and clinical validation of multi-omics biomarkers, 2) standardized integration of multiple monitoring technologies and expansion of application scenarios, and 3) intelligent regulation of closed-loop feedback immunosuppression protocols driven by real-time monitoring data. This systematic strategy holds promise for achieving precise early warning, personalized intervention, and optimized therapeutic outcomes in the rejection of transplanted organs and cells. Finally, we present a comparative summary of different types of nanoparticles in tabular form, highlighting the discrepancies among the respective nanotechnologies while elucidating their inherent advantages, limitations, and core physicochemical properties (Table 2).
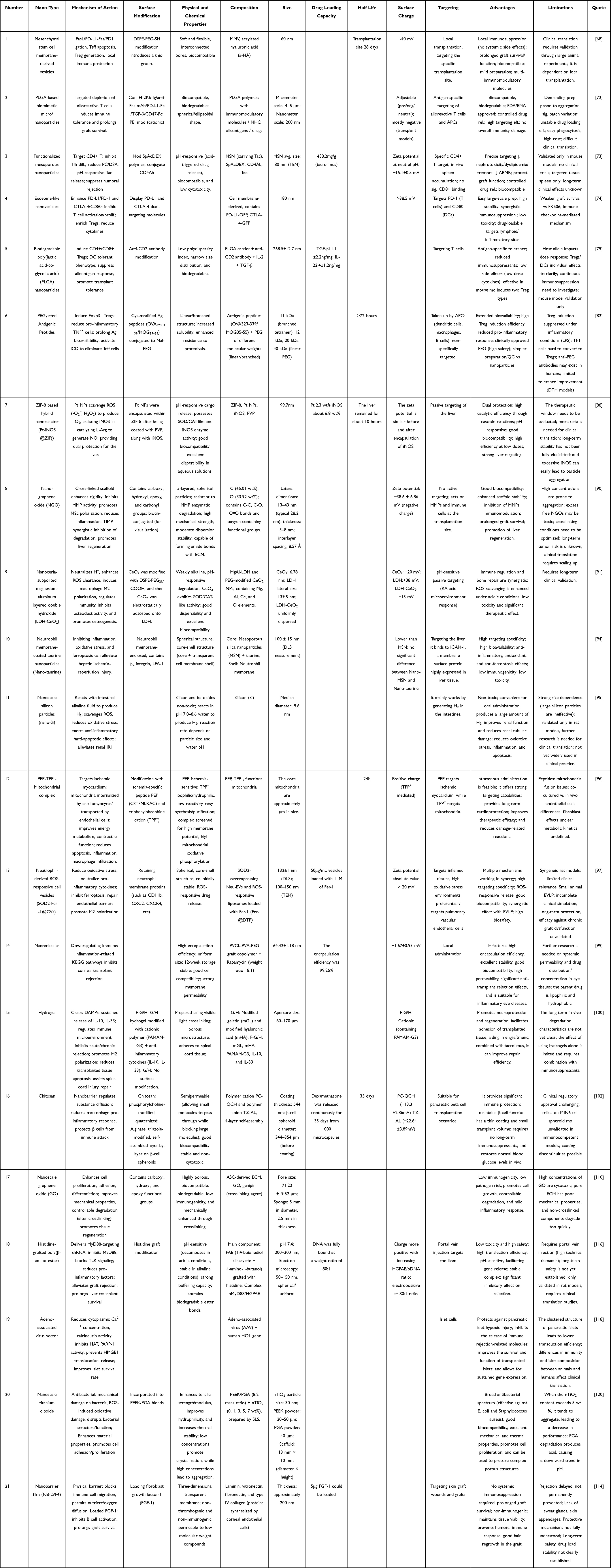 |
Table 2 Key Characteristics of Nanocarriers for Transplant Immune Modulation |
Other Innovative Nano Strategies and Cross-Application
One of the main obstacles to successful organ transplantation is preserving the viability of organs outside the body. Traditional preservation solutions, such as UW solution, are ineffective at preventing cold injury and IRI, and they have a limited storage duration. In recent years, however, nanotechnology has achieved two major breakthroughs in cryobiology.
The first is micro-nano scale precision ice control technology. Researchers used a vitrification cryopreservation strategy with 0.1–0.5 μL quartz microdroplets to significantly suppress ice crystal formation and reduce cellular mechanical damage. Compared to traditional programmed slow-freezing methods, this approach increases the survival rate of pancreatic islet cells by over 30%, providing a new preservation method for fragile cell populations, such as islets.130 Second is the bionic nano-antifreeze coating: Based on the structural biomimicry of cold-tolerant proteins in freeze-resistant organisms, organ perfusion solutions modified with nano-engineered trehalose derivatives form a stable hydration layer that inhibits ice crystal growth. This innovation successfully extends the safe ex vivo preservation time of large organs (such as the liver) to 48 hours—a significant improvement over the 12-hour limit achieved by traditional methods.131
Nanocryopreservation technology has significant advantages, but its large-scale clinical application requires overcoming potential cryotoxicity issues and scaling challenges.130
Conclusion
Compared to traditional systemic immunosuppressants, nanoplatforms have achieved a paradigm shift through targeted delivery, multi-mechanism synergy, and intelligent response. This transformation is embodied in three core advantages: First, precise targeting capabilities. Through enhanced permeability and retention effect, active targeting ligands, and biomimetic cell membrane technology, nanocarriers can efficiently accumulate at the transplant site, significantly reducing systemic toxicity. Second, multifunctional integration. A single carrier can simultaneously regulate the immune microenvironment, scavenge reactive oxygen species, and promote tissue regeneration, overcoming the inherent limitations of single-target therapies. Third, long-lasting intelligent regulation. The “on-demand release” mode of drugs mediated by responsive materials effectively addresses the shortcomings of traditional drugs with short half-lives and the need for repeated administration.
Currently, nanotechnology has shown clear potential for clinical translation in areas such as immune tolerance induction and local delivery systems, but existing research still has significant shortcomings, hindering its leap to clinical practice. On the one hand, research models are limited; most transplant immunology research remains at the mouse model stage, and validation data based on large animals are relatively scarce. Large animals are closer to humans in terms of organ size and physiological and pathological characteristics, and the lack of data from them leads to insufficient assessment of the clinical applicability of nano formulations. On the other hand, there are bottlenecks in key aspects of clinical translation. First, there are difficulties in large-scale production. Biomimetic carriers such as biomimetic cell membrane nanoparticles have batch-to-batch variability, and products such as mesenchymal stem cell-derived exosomes (MSC-EVs) have low yields, making it difficult to meet the needs of large-scale clinical applications. Second, quality control and regulatory systems are incomplete. There is a lack of unified standards for key quality attributes of nano formulations, such as particle size distribution, targeting efficiency, and drug loading capacity, and the approval process and technical specifications at the regulatory level are not yet clear. Finally, long-term safety remains a concern. The long-term metabolic fate and potential accumulation toxicity of inorganic materials such as silver nanoparticles and organic carriers such as PLGA in the body have not been fully elucidated, and relevant long-term tracking data are lacking. In addition, before large-scale clinical translation, the high cost of individualized design and donor-specific targeting schemes also poses a significant obstacle to their replacement of traditional therapies. Driving breakthroughs in nanotechnology for transplant immune rejection requires interdisciplinary collaboration and core technological innovation. At the basic research level, we should strengthen the integration of nanoplatforms with cutting and-edge technologies such as gene editing and artificial intelligence: utilizing tools such as CRISPR-Cas9-loaded liposomes to efficiently knock out major histocompatibility complex class II (MHC-II) genes in transplanted organs, and combining this with immune tolerance induction strategies to construct low-immunogenic engineered organs; using machine learning to predict the interaction between nanocarriers and immune cells, guiding carrier structure optimization and targeting ligand screening, and improving the design precision of nano systems. At the translational research level, we need to establish “diagnosis and treatment integration” and “medical-engineering interdisciplinary integration” as core development directions: relying on integrated fluorescent nano sensors and artificial intelligence recognition technology to achieve precise tracking and diagnosis of immune rejection; achieving synergistic regulation of immunosuppression, tissue repair, and body adaptation through precise delivery of responsive drugs; and promoting the development of biomimetic organ-related technologies such as 3D bioprinted scaffolds with immune-shielding coatings, highlighting the convenience and low immunogenicity advantages of transplant treatment.
To systematically advance clinical translation, a phased, gradual approach and a comprehensive support system are necessary. In terms of the translation pathway, priority should be given to the research and application of local formulations such as eye drops and subcutaneous implants – these formulations have advantages such as convenient administration, localized effects, and easy monitoring and control of efficacy and adverse reactions, serving as a breakthrough point for the clinical translation of nanotechnology; after the technology matures, it can be gradually extended to systemic delivery systems. In terms of building a support system, the core task is to establish a standardized evaluation system and regulatory norms: clarifying quantitative methods for key indicators such as nanocarrier targeting efficiency and drug release kinetics, and unifying efficacy and safety evaluation standards; accelerating multi-center, large-sample large animal trials and early clinical studies to accumulate evidence-based medical evidence closer to clinical practice; and collaborating with regulatory authorities to improve the approval process and technical specifications for nano formulations, providing institutional guarantees for large-scale production and clinical application.
In summary, nanotechnology is driving transplant immunology into an era of precise regulation by reshaping immune homeostasis, overcoming spatiotemporal limitations, and integrating tissue repair functions. Over the next ten years, research should focus on the following key areas: First, strengthening validation using large animal models to fill critical data gaps in preclinical translational research. Second, overcoming challenges in large-scale production and quality control technologies to establish a standardized nanomedicine manufacturing system. Third, conducting long-term safety studies to clarify the metabolic pathways and potential risks of nanomaterials in biological systems. Fourth, promoting interdisciplinary innovation to build an integrated “diagnosis-treatment-monitoring” nanoplatform. Through breakthroughs in these key areas, nanotechnology is expected to generate personalized immune tolerance strategies, ultimately achieving the core goal of long-term graft survival without the need for long-term medication, thus bringing about a revolutionary breakthrough in transplant medicine.
Statement on the Use of Generative AI
Generative artificial intelligence has been used in this article to polish the language and enhance its expression.
Abbreviations
Antigen-Presenting Cell (APC), Antibody-Mediated Rejection (ABMR), Calcineurin Inhibitor (CNI), Cytokine Release Syndrome (CRS), Damage-Associated Molecular Patterns (DAMPs), Dendritic Cell (DC), Donor-Specific Antibody (DSA), Enhanced Permeability and Retention (EPR), Extracellular Vesicle (EV), Fas Ligand (FasL), Graft-Versus-Host Disease (GVHD), Graft-Versus-Leukemia (GVL), Human Leukocyte Antigen (HLA), Immediate Blood-Mediated Inflammatory Response (IBMIR), Ischemia-Reperfusion Injury (IRI), Interleukin (IL), Mammalian Target of Rapamycin (mTOR), Major Histocompatibility Complex (MHC), Mouse Insulinoma 6 Cell (MIN6), Mesenchymal Stem Cell Membrane-Derived Vesicle (MMV), Pro-Inflammatory Macrophage (M1), Anti-Inflammatory/Repair-Promoting Macrophage (M2), Regulatory Macrophage (Mreg), Nuclear Factor-Kappa B (NF-κB), NOD-Like Receptor Pyrin Domain-Containing Protein 3 (NLRP3), Exosome-Like Nanovesicle (NV), Polyamidoamine (PAMAM), Programmed Cell Death Protein 1 (PD-1), Programmed Death-Ligand 1 (PD-L1), Polyethylene Glycol (PEG), Ischemia-Targeted Peptide (PEP), Poly(Lactic-Co-Glycolic Acid) (PLGA), Poly(β-Amino Ester) (PBAE), N-Palmitoylhomocysteine (PHC), Procollagen-Lysine, 2-Oxoglutarate 5-Dioxygenase 1 (PLOD1), Polyvinylpyrrolidone-Iodine (PVP-I), Reactive Oxygen Species (ROS), Soluble CD83 (sCD83), S100 Calcium Binding Protein A9 (S100A9), Signal Transducer and Activator of Transcription (STAT), Tacrolimus (Tac), T Cell Receptor (TCR), T Effector Cell (Teff), Transforming Growth Factor-Beta (TGF-β), Follicular Helper T Cell (Tfh), T Cell Immunoreceptor With Ig And ITIM Domains (TIGIT), Toll-Like Receptor (TLR), Regulatory T Cell (Treg), Tissue-Resident Memory T Cell (TRM), Mitochondrial-Targeted Cation (Triphenylphosphonium) (TPP⁺), Tumor Necrosis Factor-Alpha (TNF-α), University of Wisconsin (Preservation Solution) (UW), Zeolitic Imidazolate Framework (ZIF), Artificial Antigen-Presenting Cell (aAPC), Adult Spinal Cord Tissue (aSC), Acrylated Hyaluronic Acid (a-HA), Antibodies Against the Drug (ADA), Adenosine Deaminase Acting on RNA 1 (ADAR1), Alkaline Phosphatase (ALP), Banff Classification (of Kidney Transplant Rejection) (Banff), B-Cell Lymphoma 2 (Bcl-2), Bcl-2-Associated X Protein (Bax), Cluster of Differentiation (CD), Cluster of Differentiation 226 (CD226), Cytotoxic T Lymphocyte-Associated Protein 4 (CTLA-4), Cyclosporine A (CsA), Drug Delivery System (DDS), Thiolated PEGylated Phosphatidylethanolamine (DSPE-PEG-SH), Extracellular Matrix (ECM), Focal Adhesion Kinase (FAK), Forkhead Box P3 (FOXP3), Glomerular Filtration Rate (GFR), Hypoxia-Inducible Factor 1 Alpha (HIF1α), High Mobility Group Box 1 (HMGB1), Human Umbilical Vein Endothelial Cell (HUVEC), In Vivo Bioreactor (IVB), Janus Kinase (JAK), Lactate Dehydrogenase (LDH), Laser Desorption Ionization Mass Spectrometry (LDI-MS), Lipopolysaccharide (LPS), Macrophage Receptor With Collagenous Structure (MARCO), Mouse Cardiac Endothelial Cell (MCEC), Mitochondrial-Targeted Antioxidant (Mito quinone) (Mito Q), Matrix Metalloproteinase (MMP), Myeloid Differentiation Factor 88 (MyD88), Nano-Liquid Chromatography-Tandem Mass Spectrometry (nano LC-MS/MS), Near-Infrared (NIR), Nitric Oxide (NO), Pathogen-Associated Molecular Patterns (PAMPs), Quaternary Ammonium Phosphocholine-Chitosan (PC-QCH), Platelet-Derived Growth Factor (PDGF), Phosphoinositide 3-Kinase (PI3K), Poly(Lactic-Co-Glycolic Acid)/Poly(β-Amino Ester) (PLGA/PBAE), Protein Phosphatase 2A (PP2A), Polyvinylpyrrolidone (PVP), Rapamycin-Loaded Nano micelle (RAPA-NM), Red Blood Cell Membrane (RBCM), Runt-Related Transcription Factor 2 (RUNX2), Sterol Regulatory Element-Binding Protein (SREBP), Signal Transducer and Activator of Transcription 6 (STAT6), TLR4 Antagonist (Resatorvid) (TAK-242), Tauroursodeoxycholic Acid (TUDCA), Tetrahydropyrantriazolobenzene-Alginate (TZ-AL), Unc-51 Like Autophagy Activating Kinase 1 (ULK1), Vascular Endothelial Growth Factor (VEGF), Tungsten Disulfide Nanosheets (WS2 NSs), Zeolitic Imidazolate Framework-8 (ZIF-8)
Data Sharing Statement
No datasets were generated or analysed during the current study.
Consent for Publication
All authors contributed to the article and approved the final manuscript.
Acknowledgments
Previously reported data were used to support this study and are available at DOI. These prior studies (and datasets) are cited at relevant places within the text as references.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the Science and Technology Development Plan Projects of Jilin Province (Grant No. YDZJ202501ZYTS007);Jilin Province Health Technology Capacity Enhancement Initiative (2025WS-YA008); Special Project of Health Talents of Jilin Province (2023SCZ22, 2024SCZ28) Foreign Expert Project (D20250133).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Chuan L, Zhaonan S, Fang Y, et al. Mechanism of indoleamine 2, 3-dioxygenase inhibiting cardiac allograft rejection in mice. J. Cell. Mol. Med. 2020:0206. doi:10.1111/jcmm.15024.
2. Hao F, Tao L, Jiaxiang D, et al. Both natural and induced anti-sda antibodies play important roles in gtko pig-to-rhesus monkey xenotransplantation. Front Immunol. 2022. doi:10.3389/fimmu.2022.849711
3. Margaret Ann K, Mary Margaret BN, Sailesh K, María Isabel L, Rodrigo VR. Risk of melanoma and nonmelanoma skin cancer with immunosuppressants, part I: calcineurin inhibitors, thiopurines, IMDH inhibitors, mTOR inhibitors, and corticosteroids. J Am Acad Dermatol. 2022. doi:10.1016/j.jaad.2022.11.044
4. Allen BT, Krishna G, Kevin RS, Jamal SL. Harnessing immunomodulatory polymers for treatment of autoimmunity, allergy, and transplant rejection. Annu. Rev. Biomed. En. 2024. doi:10.1146/annurev-bioeng-110122-014306
5. Qi L, Guoqiang C, Xingchi L, Tao L, Yubo F, Tian X. Tolerogenic nano-/microparticle vaccines for immunotherapy. Article ACS Nano. 2024. doi:10.1021/acsnano.3c11647
6. Siawosh KE, Andrea D, Jamil A. Chimeric antigen receptor T reg therapy in transplantation. Trends Immuno. 2023;1219. doi:10.1016/j.it.2023.11.005
7. Wenjing C, Tuyue S, Chenyu Q, et al. Stable triangle: nanomedicine-based synergistic application of phototherapy and immunotherapy for tumor treatment. J Nanobiotechnol. 2024. doi:10.1186/s12951-024-02925-3
8. Joanna M, Łukasz U, Stanisław W, Wojciech R. Biotin TRANSPORT-TARGETING POLYSACCHARIDE-MODIfied PAMAM G3 dendrimer as system delivering α-mangostin into cancer cells and c. elegans worms. Int J Mol Sci. 2021. doi:10.3390/ijms222312925
9. Jialiang W, Kuirong M, Xiuxiu C, et al. Nanoparticle delivery of CD40 siRNA suppresses alloimmune responses by inhibiting activation and differentiation of DCs and macrophages. Sci Adv. 2022. doi:10.1126/sciadv.abq3699
10. Arianna B, Brittany R, Sarah B, et al. Spatially resolved immune exhaustion within the alloreactive microenvironment predicts liver transplant rejection. Sci Adv. 2024. doi:10.1126/sciadv.adm8841
11. Patrick GS, Yi Y, Emily W, et al. Thrombin-PAR1 signaling in pancreatic cancer promotes an immunosuppressive microenvironment. J Thromb Haemost. 2020. doi:10.1111/jth.15115
12. Lucile EW. Role of the microenvironment in immune responses to transplantation. Article. Springer Semin Immunopathol. 2003. doi:10.1007/s00281-003-0138-y
13. Tran L, Macedo C, Zahorchak AF, et al. Donor-derived regulatory dendritic cell infusion modulates effector CD8 + T cell and NK cell responses after liver transplantation. Sci, trans med. 2023;15. doi:10.1126/scitranslmed.adf4287
14. Babak JO, Bonnie EL, Annette MJ, et al. Splenic irradiation for the treatment of severe antibody-mediated rejection. Am J Transplant. 2016. doi:10.1111/ajt.13882
15. Chun-Lian H, Xinyu F, Yi F, et al. Relationship between the microenvironment and survival in kidney transplantation: a bibliometric analysis from 2013 to 2023. Front Immunol. 2024. doi:10.3389/fimmu.2024.1379742
16. Josep MC, Pablo Í, Sergio L, Bescós M, Federico O. Role of transforming growth factor-beta1 in the progression of chronic allograft nephropathy. Article. Nephrol Dial Transplant. 2001. doi:10.1093/ndt/16.suppl_1.114
17. Merve K, Judith V, Daymé González R, et al. Intrinsic TGF-β signaling attenuates proximal tubule mitochondrial injury and inflammation in chronic kidney disease. Nat Commun. 2023. doi:10.1038/s41467-023-39050-y
18. Hidekazu N, Antonio P, Yasuhisa Y, et al. Foxp3+ regulatory T Cells Maintain Bone Marrow Microenvironment for B Cell Differentiation from Hematopoietic Stem Cells. Article Division of Blood and Marrow Transplantation, Stanford University, Stanford, CA Department of Hematology, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan Division of Endocrinology, Stanford University, Stanford, CA Division of Blood and Marrow Transplantation, Stanford University, Stanford, CA Division of Blood and Marrow Transplantation, Stanford University, Stanford, CA Division of Blood and Marrow Transplantation, Stanford University, Stanford, CA Division of Blood and Marrow Transplantation, Department of Medicine, Stanford University Medical Center, Stanford, CA Division of Endocrinology, Stanford University, Stanford, CA Department of Hematology, Faculty of Medicine, University of Tsukuba, Tsukuba, Ibaraki, Japan Division of Blood and Marrow Transplantation, Stanford University, Stanford, CA. Blood. 2016. doi:10.1182/blood.v128.22.431.431
19. John K, Ken‐ichi M, Haesook TK, et al. Interleukin-2 and regulatory T cells in graft-versus-host disease. New Eng. J. Med. 2011. doi:10.1056/NEJMoa1108188
20. Michael SA, James SY, Jared MP, Dengping Y, Maria‐Luisa A, Anita SC. Linked sensitization by memory CD4+ T cells prevents costimulation blockade-induced transplantation tolerance. JCI Insight. 2022. doi:10.1172/jci.insight.159205
21. Norihisa M, Shimon S. Regulatory T cells in autoimmune kidney diseases and transplantation. Nat Rev Nephrol. 2023. doi:10.1038/s41581-023-00733-w
22. Marie B, Alison RS, Stuart S, et al. Naive T-cell depletion to prevent chronic graft-versus-host disease. J clin oncol. 2022. doi:10.1200/jco.21.01755
23. Mark ES, Kaveh M, Anna B, et al. Modulation of tissue resident memory T cells by glucocorticoids after acute cellular rejection in lung transplantation. J Exp Med. 2022. doi:10.1084/jem.20212059
24. Khodor IAD, Roger T, Daqiang Z, et al. Resident memory T cells form during persistent antigen exposure leading to allograft rejection. Sci immunol. 2021. doi:10.1126/sciimmunol.abc8122
25. Kate T, Kieran POD, Rosalba R, et al. Intravascular donor monocytes play a central role in lung transplant ischaemia-reperfusion injury. Article Thorax. 2017. doi:10.1136/thoraxjnl-2016-208977
26. Zhenrui C, Wei-Xiong Z, Yu-Xin J, et al. miR-449a ameliorates acute rejection after liver transplantation via targeting procollagen-lysine1,2-oxoglutarate5-dioxygenase 1 in macrophages. Article. Am J Transplant. 2023. doi:10.1016/j.ajt.2022.12.009
27. Katrin P-M, Alfrun S, Andreas BW, et al. Pre-incubation of corneal donor tissue with sCD83 improves graft survival via the induction of alternatively activated macrophages and tolerogenic dendritic cells. Article. Am J Transplant. 2021. doi:10.1111/ajt.16824
28. Mingwei S, Weihua L, Zhangjiu L, Yuanbang L, Wenli Y. S100A9 regulates M1 macrophage polarization and exacerbates steatotic liver ischemia-reperfusion injury. Transpl. Immuno. 2024. doi:10.1016/j.trim.2024.102134
29. Dongliang Z, Yitian L, Jingchang M, et al. Competitive binding of CD226/TIGIT with poliovirus receptor regulates macrophage polarization and is involved in vascularized skin graft rejection. Article. Am J Transplant. 2023. doi:10.1016/j.ajt.2023.04.007
30. Junjie L, Jiangang X, Shanshou L, et al. ADAR1 attenuates allogeneic graft rejection by suppressing miR-21 biogenesis in macrophages and promoting M2 polarization. Article. FASEB J. 2018. doi:10.1096/fj.201701449R
31. Ni B, Zhang D, Zhou H, et al. IL-34 attenuates acute T cell-mediated rejection following renal transplantation by upregulating M2 macrophages polarization. Heliyon. 2024;10. doi:10.1016/j.heliyon.2024.e24028
32. Chen YN, Hu MR, Wang L, Chen WD. Macrophage M1/M2 polarization. Eur. J. Pharmacol. 2020;877173090. doi:10.1016/j.ejphar.2020.173090
33. Claire EW, Kimheak S, Becky KB, et al. Regulation of extracellular matrix assembly and structure by hybrid M1/M2 macrophages. Biomaterials. 2021. doi:10.1016/j.biomaterials.2021.120667
34. Massimo L, Graziella C, Diversity AM. Mechanisms, and Significance of Macrophage Plasticity. Annu. Rev. Pathol. 2019. doi:10.1146/annurev-pathmechdis-012418-012718
35. Meng Z, Qian L, Hui M, et al. Ischemia-reperfusion injury: molecular mechanisms and therapeutic targets. Signal Transduct Target Ther. 2024;9. doi:10.1038/s41392-023-01688-x
36. Xiaobing L, Qing W, Yue L, et al. Isoliquiritigenin alleviates cerebral ischemia-reperfusion injury by reducing oxidative stress and ameliorating mitochondrial dysfunction via activating the Nrf2 pathway. Article Redox biol. 2024. doi:10.1016/j.redox.2024.103406
37. Caishi L, Mengqi H, Mengying A, et al. Ultra-small copper-based multienzyme-like nanoparticles protect against hepatic ischemia-reperfusion injury through scavenging reactive oxygen species in mice. Small. 2024. doi:10.1002/smll.202403313
38. Shen P, Huang K, Zhang X, Qin M, Wang X, Fan Z. Neutrophil-Mimicking Prussian blue nanozymes for synergistic targeted immuno-metabolic therapy of hepatic ischemia–reperfusion injury. J Nanobiotechnol. 2025;23(1):736. doi:10.1186/s12951-025-03806-z
39. Egor YP, Dmitry BZ. Pros and cons of use of mitochondria-targeted antioxidants. Antioxidants. 2019. doi:10.3390/antiox8080316
40. Esther Maria G, Claus DS, Patrick D, et al. The iron chelator Deferasirox causes severe mitochondrial swelling without depolarization due to a specific effect on inner membrane permeability. Sci Rep. 2020. doi:10.1038/s41598-020-58386-9
41. Jinhui W, Haibo M, Jingbo H, Shunhua C, Hao S. Engineering of phosphatidylserine-targeting ROS-responsive polymeric prodrug for the repair of ischemia-reperfusion-induced acute kidney injury. J Control Release. 2024. doi:10.1016/j.jconrel.2024.10.063
42. Hailin Z, Jessica Santiváñez P, Kaizhi L, Andrew JTG, Daqing M. Role of Toll-like receptor-4 in renal graft ischemia-reperfusion injury. Am J Physiol Renal Physiol. 2014;0213. doi:10.1152/ajprenal.00469.2013
43. Haijian M, Xiaozhen G, Shichao C, et al. Dephosphorylation of AMP-activated protein kinase exacerbates ischemia/reperfusion-induced acute kidney injury via mitochondrial dysfunction. Kidney Int. 2021. doi:10.1016/j.kint.2021.10.028
44. Viktor A, Winston C, Suze AJ, et al. Corticosteroids impair epithelial regeneration in immune-mediated intestinal damage. J Clin Invest. 2024. doi:10.1172/jci155880
45. Hasan D, Sunčica P, Carsten D, et al. Immunosuppression with cyclosporine versus tacrolimus shows distinctive nephrotoxicity profiles within renal compartments. Acta Physiol. 2024. doi:10.1111/apha.14190
46. Combs MP, Krysta W, Haley H, et al. Impact of tacrolimus vs cyclosporine on chronic lung allograft dysfunction incidence and allograft survival in the International society of heart and lung transplantation registry. J Heart Lung Transplant. 2024. doi:10.1016/j.healun.2024.10.013
47. Paige V, Jocelyn E, Hubert KE, et al. Tacrolimus-induced neurotoxicity after transplant: a literature review. Article Drug Safety. 2024. doi:10.1007/s40264-024-01398-5
48. Michael RT, Kyle LF, Hannah R, et al. Vancomycin relieves mycophenolate mofetil-induced gastrointestinal toxicity by eliminating gut bacterial β-glucuronidase activity. Sci Adv. 2019. doi:10.1126/sciadv.aax2358
49. Michele K, Jorge Henrique Cavalcanti Orestes C, Luis Eduardo Rodrigues S, et al. Azathioprine and risk of non-melanoma skin cancers in organ transplant recipients: a systematic review and update meta-analysis. Clin Transl Oncol. 2025. doi:10.1007/s12094-024-03839-0
50. F ZA, Michiel GHB, Willem AD, Ron AMF, Marlies EJR, EdW A. Mycophenolate mofetil hampers antibody responses to a broad range of vaccinations in kidney transplant recipients: results from a randomized controlled study. J. Infect. 2024. doi:10.1016/j.jinf.2024.106133
51. Faisal K, Zaid A, Aahd K, Yousef AA, Fadi S. CT Findings in solid organ transplant patients with sirolimus-associated lung toxicity. article department of internal medicine, university of toledo, toledo, oh department of internal medicine, university of toledo, toledo, oh department of internal medicine, university of toledo, toledo, oh department of internal medicine, university of toledo, toledo, OH. Chest. 2017. doi:10.1016/j.chest.2017.08.640
52. Morviducci L, Francesca Silvia R, Laura R, et al. Everolimus is a new anti-cancer molecule: metabolic side effects as lipid disorders and hyperglycemia. Diabetes Res Clin Pract. 2018;143:428–37. doi:10.1016/j.diabres.2018.04.001
53. Kahn DY, Alain CM, Bincy G, et al. Mammalian target of rapamycin (mTOR)-induced pneumonitis: single-institution experience and treatment. J clin oncol. 2010;28:e13520–e13520. doi:10.1200/jco.2010.28.15_suppl.e13520
54. Trevor TH, Harald K, Thomas PS, Jane AM, Andrew JTG. The safety and side effects of monoclonal antibodies. Nat Rev Drug Discov. 2010. doi:10.1038/nrd3003
55. Sara A, Hanieh M, Mohammad Hossein N. JAK Inhibitors in Solid Organ Transplantation. Article. J. Clin. Pharmaco. 2023. doi:10.1002/jcph.2325
56. Donald EH, Brian A, Tarek A, et al. Infliximab induction lacks efficacy and increases bk virus infection in deceased donor kidney transplant recipients: results of the ctot-19 trial. J Am Soc Nephrol. 2022. doi:10.1681/asn.2022040454
57. Javier BM, Mehdi H, Juan W, et al. Post-transplantation cyclophosphamide-based graft-versus-host disease prophylaxis. New Engl J Med. 2023:0621. doi:10.1056/NEJMoa2215943.
58. Anoma N, Jay AF. The microbiome, systemic immune function, and allotransplantation. Clin Microbiol Rev. 2015. doi:10.1128/cmr.00063-15
59. John EM, Samantha AW, Áurea SS, et al. The lung microbiome in lung transplantation. Article. J Heart Lung Transplant. 2021. doi:10.1016/j.healun.2021.04.014
60. Mandy LF. Micromanaging alloimmunity. J Clin Invest. 2016. doi:10.1172/jci88621
61. Tara KS, Paul F, Juliane L, et al. Perturbations of the T-cell immune repertoire in kidney transplant rejection. Front Immunol. 2022. doi:10.3389/fimmu.2022.1012042
62. Marieke van der Z, CvG M, Anne PB, et al. Efficacy of rabbit anti-thymocyte globulin therapy for severe acute rejection in kidney transplant patients using calcineurin inhibitor and mycophenolate mofetil based immunosuppressive therapy. Transplantation. 2018. doi:10.1097/01.tp.0000542664.96769.e0
63. Patrick GD, Memory MDGB. CD4 T cell presensitization fosters antibody-mediated kidney transplant rejection. article department of nephrology, galway university hospitals, saolta university health group, galway, ireland|regenerative medicine institute at cúram centre for research in medical devices, school of medicine, college of medicine, nursing and health sciences, national university of ireland, galway, Ireland. J Am Soc Nephrol. 2016. doi:10.1681/asn.2016040470
64. Bo H, Xiaobo Y, Xinting S. Liver graft rejection following immune checkpoint inhibitors treatment: a review. Article. Med Oncol. 2019. doi:10.1007/s12032-019-1316-7
65. Sun Woo L, Yoo Jin S, Sheng C, et al. Therapeutic effect of multiple functional minicircle vector encoding anti-CD25/IL-10/CXCR3 in allograft rejection model. Korean J Intern Med. 2022. doi:10.3904/kjim.2021.299
66. Sabrina W, Conor H, Joanna H, Fadi I. Chimeric antigen receptors and regulatory t cells: the potential for HLA-Specific immunosuppression in transplantation. Engineering. 2021. doi:10.1016/j.eng.2021.10.018
67. Jun P, Fang Y, Hui L, et al. Dissecting the immune discrepancies in mouse liver allograft tolerance and heart/kidney allograft rejection. Cell Proliferation. 2023. doi:10.1111/cpr.13555
68. Yuqian W, Renqi H, Yougong L, Mingqi L, Ran M. Immuno-protective vesicle-crosslinked hydrogel for allogenic transplantation. Nat Commun. 2024. doi:10.1038/s41467-024-49135-x
69. Qidong C, Long L, Xiaohong Z, Junbo L, Shao-wei L. Challenges and opportunities in the islet transplantation microenvironment: a comprehensive summary of inflammatory cytokine, immune cells, and vascular endothelial cells. Front Immunol. 2023. doi:10.3389/fimmu.2023.1293762
70. Johannes W, Ulrich H, Niklas B, et al. Foxp3+ CD4+ T cells improve healing after myocardial infarction by modulating monocyte/macrophage differentiation. Circulation Research. 2014. doi:10.1161/circresaha.115.303895
71. Dietmar MZ, Carlos MM, Johanna AK. Immune- and non-immune-mediated roles of regulatory T-cells during wound healing. Immunology. 2019. doi:10.1111/imm.13057
72. Khawar Ali S, Muhammad N, Lei Z, et al. Design and Optimization of PLGA particles to deliver immunomodulatory drugs for the prevention of skin allograft rejection. Immunol invest. 2019. doi:10.1080/08820139.2019.1695134
73. Jia S, Chang L, Pengpeng Y, et al. Helper T Cell (CD4 +) targeted tacrolimus delivery mediates precise suppression of allogeneic humoral immunity. Research. 2022. doi:10.34133/2022/9794235
74. Zhanxue X, Hsiang‐i T, Youmei X, et al. Engineering programmed death ligand-1/cytotoxic t-lymphocyte-associated antigen-4 dual-targeting nanovesicles for immunosuppressive therapy in transplantation. ACS nano. 2020. doi:10.1021/acsnano.9b09065
75. Jacinta J, Suchita N, Alessia V, et al. Spatiotemporal in vivo tracking of polyclonal human regulatory T cells (Tregs) reveals a role for innate immune cells in Treg transplant recruitment. Mol Ther Meth Clin Develop. 2020. doi:10.1016/j.omtm.2020.12.003
76. Kelly RR, Randall AM, Justin W, Stephany YT, Jordan JG. Biomimetic tolerogenic artificial antigen presenting cells for regulatory T cell induction. Acta Biomater. 2020. doi:10.1016/j.actbio.2020.06.004
77. Liuting Z, Tiejun Y, Kailin Y, et al. Efficacy and safety of curcumin and curcuma longa extract in the treatment of arthritis: a systematic review and meta-analysis of randomized controlled trial. Front Immunol. 2022. doi:10.3389/fimmu.2022.891822
78. Longpeng M, Xiang‐Qian L, Lihua M, Jialiang F, Dabo L. Mechanism of Der f 1/IGF-1 nanoparticle promoting the production of regulatory T cell. Lin chuang er bi yan hou tou jing wai ke za zhi = J clin otorhinolaryngol, head neck surg. 2023. doi:10.13201/j.issn.2096-7993.2023.04.007
79. David AH, Ju Hua W, Dongin K, et al. Nanoparticles loaded with IL-2 and TGF-β promote transplantation tolerance to alloantigen. Front Immunol. 2024. doi:10.3389/fimmu.2024.1429335
80. Giuseppe C, Hugo A, Chiara C, Umberto D, Annalisa C. Nano-microparticle platforms in developing next-generation vaccines. Vaccines. 2021. doi:10.3390/vaccines9060606
81. Chiara P, Elena B, Casimiro Luca G, et al. Cutting-edge delivery systems and adjuvants in tolerogenic vaccines: a review. Pharmaceutics. 2022. doi:10.3390/pharmaceutics14091782
82. Jennifer P, Mario S, Uta L, et al. Tolerogenic Immunomodulation by PEGylated Antigenic Peptides. Front Immunol. 2020. doi:10.3389/fimmu.2020.529035
83. Stéphanie B, Olivier D, Patrice V, Caroline B, Sacha ADS. Innate immunity in solid organ transplantation: an update and therapeutic opportunities. Expert Rev. Clin. Immunol. 2015. doi:10.1586/1744666x.2015.1008453
84. Quan Z, Quan L, Sherrie JD, et al. Graft-infiltrating host dendritic cells play a key role in organ transplant rejection. Nat Commun. 2016. doi:10.1038/ncomms12623
85. Mounia SB, MTvL M, Marnix L, et al. Inhibiting Inflammation with myeloid cell-specific nanobiologics promotes organ transplant acceptance. Immunity. 2018. doi:10.1016/j.immuni.2018.09.008
86. Yue Z, Song C, Peixiang L, et al. Macrophage subpopulations and their impact on chronic allograft rejection versus graft acceptance in a mouse heart transplant model. Am J Transplant. 2017;18:102–112. doi:10.1111/ajt.14543
87. Chao G, Xiaodong W, Jian L, et al. Mesenchymal stem cells transfected with sFgl2 inhibit the acute rejection of heart transplantation in mice by regulating macrophage activation. Stem Cell Res Ther. 2020. doi:10.1186/s13287-020-01752-1
88. Jing M, Chunxiao L, Yu S, et al. Protective effect of platinum nano-antioxidant and nitric oxide against hepatic ischemia-reperfusion injury. Nat Commun. 2022;13. doi:10.1038/s41467-022-29772-w
89. Yu H, Ejun P, Xiaozhuo B, et al. ROS responsive cerium oxide biomimetic nanoparticles alleviates calcium oxalate crystals induced kidney injury via suppressing oxidative stress and m1 macrophage polarization. Small. 2024. doi:10.1002/smll.202405417
90. Da‐Hyun K, Minji K, Seon‐Yeong K, et al. Bioengineered liver crosslinked with nano-graphene oxide enables efficient liver regeneration via MMP suppression and immunomodulation. Nat Commun. 2023. doi:10.1038/s41467-023-35941-2
91. Hao F, Yuedong G, Wenming F, Jiaxing W, Ping H, Jianlin S. Anti-acidification and immune regulation by nano-ceria-loaded mg-al layered double hydroxide for rheumatoid arthritis therapy. Adv. Sci. 2023. doi:10.1002/advs.202307094
92. Shaojun S, Feng X. Current Antioxidant Treatments in Organ Transplantation. Oxid Med Cell Longev. 2016. doi:10.1155/2016/8678510
93. Satish NN, Suraj D, Natalie L, et al. Immunosuppressive nano-therapeutic micelles downregulate endothelial cell inflammation and immunogenicity. RSC Adv. 2015. doi:10.1039/c5ra04057d
94. Shijie Q, Xuyi L, Jingyan Z, et al. Neutrophil membrane-coated taurine nanoparticles protect against hepatic ischemia-reperfusion injury. Eur. J. Pharmacol. 2023. doi:10.1016/j.ejphar.2023.175712
95. Masataka K, Ryoichi I, Kobayashi Y, et al. Oral administration of si-based agent attenuates oxidative stress and ischemia-reperfusion injury in a rat model: a novel hydrogen administration method. Front Med. 2020. doi:10.3389/fmed.2020.00095
96. Xiaolei S, Hang C, Rifeng G, et al. Intravenous transplantation of an ischemic-specific peptide-tpp-mitochondrial compound alleviates myocardial ischemic reperfusion injury. ACS nano. 2023. doi:10.1021/acsnano.2c05286
97. Yuan H-X, Ye -Y-Y, Shen P, et al. Engineering neutrophil vesicles for synergistic protection against ischemia/reperfusion injury after lung transplant. Adv. Sci. 2025;12(42):e06127. doi:10.1002/advs.202506127
98. Christina L, Steven JC, Yik Wen L, et al. Targeting inflammatory monocytes by immune-modifying nanoparticles prevents acute kidney allograft rejection. Kidney Int. 2022. doi:10.1016/j.kint.2022.06.024
99. Ting Z, Chao W, Xianggen W, et al. Characterization and Evaluation of Rapamycin-Loaded Nano-Micelle Ophthalmic Solution. J. Funct. Biomater. 2023. doi:10.3390/jfb14010049
100. Xu G, Zhifeng Y, Yue L, et al. Multifunctional hydrogel modulates the immune microenvironment to improve allogeneic spinal cord tissue survival for complete spinal cord injury repair. Acta Biomater. 2022. doi:10.1016/j.actbio.2022.11.015
101. Xuejie F, Huilin Y, Hui Z, et al. Improved osteogenesis and upregulated immunogenicity in human placenta-derived mesenchymal stem cells primed with osteogenic induction medium. Stem Cell Res Ther. 2016. doi:10.1186/s13287-016-0400-6
102. Michael Yilma Y, Marco G, Ling L, Steven P, Maryam T. An investigation of functionalized chitosan and alginate multilayer conformal nanocoating on mouse beta cell spheroids as a model for pancreatic islet transplantation. Int J Biol Macromol. 2024. doi:10.1016/j.ijbiomac.2024.134960
103. Min Jung K, Heon-Seok P, Jiwon K, et al. Suppression of fibrotic reactions of chitosan-alginate microcapsules containing porcine islets by dexamethasone surface coating. Endocrinol Metab. 2021. doi:10.3803/EnM.2021.879
104. Xue Guang L, In‐Su P, Byung Hyune C, Ung‐Jin K, Byoung‐Hyun M. In vivo bioreactor using cellulose membrane benefit engineering cartilage by improving the chondrogenesis and modulating the immune response. Tissue Eng and Regener Med. 2020. doi:10.1007/s13770-019-00236-5
105. Shiva P, Tung Thanh P, Jee‐Heon J, Youngro B. Immunoisolation of pancreatic islets via thin-layer surface modification. J Control Release. 2019. doi:10.1016/j.jconrel.2019.04.034
106. Mojahid A, Anthony P, Xinghua W, Joy W, Si MP. Extracellular vesicles for treatment of solid organ ischemia-reperfusion injury. Am J Transplant. 2020. doi:10.1111/ajt.16164
107. Nicholas G, Joris B, Jacques P, Renato R, Giovanni C, Diethard M. organ repair and regeneration during ex situ dynamic preservation: the future is nano. Transplant Int. 2023. doi:10.3389/ti.2023.11947
108. Kyung-Yup C, Woongjin C, Sunghyun P, et al. Generation of bioactive MSC-EVs for bone tissue regeneration by tauroursodeoxycholic acid treatment. J Control Release. 2023. doi:10.1016/j.jconrel.2022.12.053
109. Yue Z, Caiqi C, Xinyi W, et al. Aspirin-loaded anti-inflammatory zno-sio 2 aerogel scaffolds for bone regeneration. ACS Appl. Mater. Interfaces. 2024. doi:10.1021/acsami.3c17152
110. Batzaya N, Chih‐Hwa C, Pei‐Chun W, Chih-Wei C, Mantosh Kumar S, Er‐Yuan C. Genipin-crosslinked adipose stem cell derived extracellular matrix-nano graphene oxide composite sponge for skin tissue engineering. J Mat Chem B. 2018. doi:10.1039/c7tb02480k
111. Shu P, Yi Z, Yibo S, Xueying L, Yuanfan X, Hongcan S. Selection of the optimum 3D-printed pore and the surface modification techniques for tissue engineering tracheal scaffold in vivo reconstruction. J Biomed Mater Res Part A. 2018. doi:10.1002/jbm.a.36536
112. Huajian S, Xuanfang Z, Bo T, et al. Gold nanorods modified by endogenous protein with light-irradiation enhance bone repair via multiple osteogenic signal pathways. Biomaterials. 2022. doi:10.1016/j.biomaterials.2022.121482
113. Sanaz Keshavarz S, Farshad F, Ehsan S, Tannaz J, Peter EP, Amirhossein S. Application of PLGA nano/microparticle delivery systems for immunomodulation and prevention of allotransplant rejection. Expert Opin Drug Delivy. 2020. doi:10.1080/17425247.2020.1748006
114. Lauren B, Glowacki P, Bart MS. Bioengineered skin allografts: a new method to prevent humoral response. ASAIO J. 2011. doi:10.1097/MAT.0b013e3182155e52
115. Xinhao Z, Rui G, Yannan Z, et al. Adult spinal cord tissue transplantation combined with local tacrolimus sustained-release collagen hydrogel promotes complete spinal cord injury repair. Cell Proliferation. 2023. doi:10.1111/cpr.13451
116. Fanguo H, Hanjie W, Shuang‐Nan Z, et al. Inhibition of myeloid differentiation factor 88 signaling mediated by histidine-grafted poly(β-amino ester) ester nanovector induces donor-specific liver allograft tolerance. Int J Nanomed. 2015. doi:10.2147/ijn.S81413
117. Xiangyu F, Hai-Yun W, Lisong Z, Xu G. A poly-chitosan and cis-platinum conjugated composite nanoparticle system for liver cancer therapy. J. Biomed. Nanotechnol. 2021. doi:10.1166/jbn.2021.3157
118. Min Jun K, Yong Hwa H, Jin Wook H, Zahid A, Dong Yun L. Heme oxygenase-1 gene delivery for altering high mobility group box-1 protein in pancreatic islet. J Control Release. 2022;0124. doi:10.1016/j.jconrel.2022.01.031
119. Bin M, Xiangguo D, Qiunan Z, et al. Use of aspirin in the prevention of colorectal cancer through TIGIT-CD155 pathway. J Cell & Mol Med. 2019. doi:10.1111/jcmm.14332
120. Cijun S, Chenying S, Pei F, Chengde G, Shuping P, Youwen Y. Antibacterial capability, physicochemical properties, and biocompatibility of ntio2 incorporated polymeric scaffolds. Polymers. 2018. doi:10.3390/polym10030328
121. Min P, Jun-Lan C, Gaoping Z, Qiang F. Construction of silver-coated high translucent zirconia implanting abutment material and its property of antibacterial. Article. Artif. Cells Nanomed. Biotechnol. 2023. doi:10.1080/21691401.2023.2244013
122. Yantao Z, Xiantong H, Zhonghai L, et al. Use of polyvinylpyrrolidone-iodine solution for sterilisation and preservation improves mechanical properties and osteogenesis of allografts. Sci Rep. 2016. doi:10.1038/srep38669
123. Seda K, Andrew S, Xiang L, et al. Encapsulation of pancreatic islets within nano-thin functional polyethylene glycol coatings for enhanced insulin secretion. Article Tissue Engineering Part A. 2010. doi:10.1089/ten.TEA.2009.0640
124. Seon Jae L, Jaebin L, Young-Woo P, Dong Yun L. 3D Bioprinting for Artificial Pancreas Organ. Adv Exp Med Biol. 2018. doi:10.1007/978-981-13-0445-3_21
125. Nozomi A, Kaname O, Masaaki H, et al. Immune complexome analysis of antigens in circulating immune complexes from patients with acute cellular rejection after living donor liver transplantation. Transpl. Immuno. 2018. doi:10.1016/j.trim.2018.02.011
126. Haemin P, Yung‐Hun Y, Byung‐Gee K, Yun‐Gon K. Structural characterization of α-galactosylated O-glycans from miniature pig kidney and endothelial cells. Carbohydr. Res. 2013. doi:10.1016/j.carres.2012.12.024
127. Lorenzo P, Matthew JE, Paola M, et al. Alloantibody and autoantibody monitoring predicts islet transplantation outcome in human type 1 diabetes. Diabetes. 2012. doi:10.2337/db12-1258
128. Yong Joon S, Tae Hyeon L, Hak Soo C, et al. 3D printing and nir fluorescence imaging techniques for the fabrication of implants. Materials. 2020. doi:10.3390/ma13214819
129. Sunho J, Hee-Kyung N, Jin Gyeong S, et al. Quantitative analysis of immunosuppressive drugs using tungsten disulfide nanosheet-assisted laser desorption ionization mass spectrometry. ACS nano. 2021. doi:10.1021/acsnano.1c02016
130. Xiao Hui Z, Paolo NC, Umut AG, Imran K, Utkan D. Emerging technologies in medical applications of minimum volume vitrification. Article. Nanomedicine. 2011. doi:10.2217/nnm.11.71
131. He S, Xi C, Xing L, Ke J, Zhifeng X, Jianwu D. Transplantation of adult spinal cord grafts into spinal cord transected rats improves their locomotor function. Sci China Life Sci. 2019. doi:10.1007/s11427-019-9490-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.