Back to Journals » International Journal of Nanomedicine » Volume 21
Nanomedicine-Based Strategies for Multiple Myeloma Therapy
Authors Wu A, Zhang M, He H, Zhao P
Received 28 April 2026
Accepted for publication 30 June 2026
Published 16 July 2026 Volume 2026:21 620686
DOI https://doi.org/10.2147/IJN.S620686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Eng San Thian
Aihua Wu,1 Meng Zhang,2 Haiyan He,1 Pengfei Zhao3
1Department of Pharmacy, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, 310016, People’s Republic of China; 2Department of Pharmacy, Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, 310006, People’s Republic of China; 3Center of Clinical Pharmacology, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310009, People’s Republic of China
Correspondence: Pengfei Zhao, Center of Clinical Pharmacology, The Second Affiliated Hospital, Zhejiang University School of Medicine, 88 Jiefang Road, Hangzhou, 310009, People’s Republic of China, Tel +86-571-8778-2027, Email [email protected] Haiyan He, Department of Pharmacy, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, 3rd East Qingchun Road, Hangzhou, 310016, People’s Republic of China, Email [email protected]
Abstract: Multiple myeloma (MM) belongs to the hematological malignancies and the overall incidence of MM is on the rise across the world. Over the last few decades, increased attention has been paid to the development and pathogenesis of MM. Significant changes have also been witnessed in the paradigm for the treatment of MM, including proteasome inhibitors, immunomodulators and anti CD38 monoclonal antibodies, which have significantly improved the survival of patients. The increasing focus on nanomedicine stems from its capacity to enhance the treatment of MM—by reducing systemic side effects and enabling more precise therapeutic targeting. This review summarizes current advances in nanomedicine-based treatment options for MM and disscusses the superior efficacy of biomimetic nanoparticles exploiting bone marrow homing. It also covers the potential of mRNA nano‑vaccines (eg, Galsomes and BCMA‑mRNA LNPs) and the improved safety profiles of liposomal formulations compared to free drugs. This review will provide further insight into developing treatment strategies for MM.
Keywords: multiple myeloma, nanomedicine, targeted drug delivery, bone marrow microenvironment, nanoparticles
Introduction
Multiple myeloma (MM) constitutes approximately 1% of all malignancies and 10% of hematological cancers,1 ranking as the second most prevalent hematological malignancy globally, with an incidence rate of 2.1 per 100,000 individuals annually.2 Notably, epidemiological trends in China indicate a rising prevalence and a concerning downward shift in the average age at diagnosis. In the United States, the burden remains significant, with over 32,000 new diagnoses and nearly 13,000 attributable deaths annually, as estimated by the World Health Organization (WHO) in 2022.3 Clinically, MM originates from the clonal expansion of malignant plasma cells within the bone marrow. This clonal proliferation leads to the overproduction of monoclonal (M) protein and widespread infiltration of vital organs.4 These pathophysiological processes culminate in end-organ damage, clinically defined by the CRAB criteria: Calcium; Renal impairment; Anemia, and Bone disease.5 Beyond these cardinal features, patients frequently experience additional significant complications, including systemic amyloidosis, hyperviscosity syndrome, debilitating fatigue, and recurrent infections stemming from profound immunodeficiency.6 The emergence of extramedullary disease, indicating malignant plasma cell proliferation outside the bone marrow, portends an aggressive disease course and a poorer prognosis. Despite substantial therapeutic advancements, MM remains an incurable disease, highlighting the critical need for ongoing research into novel treatment modalities. This underscores the importance of clinical pharmacists in optimizing current regimens, managing complex drug toxicities, and identifying patients who may benefit from emerging therapies or clinical trial participation.
In recent years, significant advancements have been made in understanding the pathogenesis of MM, with key insights being made into the following areas:7 cytogenetic alterations. It has been established that 90% of MM patients have abnormal chromosome number and structure, which are critical in disease progression and prognosis. Interaction between bone marrow microenvironment (BMM) and myeloma cells. Myeloma cells and stromal cells in the BMM interact to stimulate the transcription and secretion of a variety of cytokines. This interaction promotes mutual growth and forms a vast network, leading to the proliferation of myeloma cells, the development of bone disease, and alterations in signaling pathways. The intracellular transcription factor of nuclear factor kappa-B (NF-κB) exists in two states: active and inactive. Active NF-κB is a heterodimer composed of p50 and p65 subunits. Inactive NF-κB contains an inhibitory subunit, which releases I-κB under the stimulation of activation signals, converting into active NF-κB. This active form binds to initiators in the nucleus, promoting cell growth and the expression of various cytokines. The expression of these cytokines, in turn, has been observed to stimulate stromal cells to secrete more cytokines, potentially leading to drug resistance. Notch signaling, which facilitates direct cell-to-cell contact, is frequently overexpressed in MM cells. Jun et al suggested that MM results from the interaction between Notch receptors and ligands.8
Nanomedicine has demonstrated the potential to overcome the limitations of current therapies by developing advanced drug delivery systems (DDS) that can target the complex BMM and, consequently, myeloma cells. Nanomedicines possess extraordinary chemical and physical properties that enable high surface area for incorporating drugs and/or imaging agents, and enhanced tissue specificity.9 Nanomedicine can address the challenge of relapse by providing maintenance therapy in a controlled, sustained manner, which could improve long-term disease control. Additionally, nanomedicine can enhance targeted delivery and reduce systemic exposure, thereby improving quality of life by minimizing side effects associated with long-term treatment.10 This review summarizes the latest advances in nanomedicines for MM and explores the challenges and future opportunities of developing nanomedicines for the targeted treatment of MM.
BMM
The BMM plays a pivotal role in the pathophysiology of MM, encompassing both cellular and non-cellular components.11 The cellular elements include bone marrow stromal cells (BMSCs), osteoclasts, endothelial cells, and osteoblasts, while the non-cellular components consist of the extracellular matrix and critical cytokines such as interleukin (IL)-6, IL-21, tumor necrosis factor alpha (TNF-α), and growth factors like insulin-like growth factor (IGF) and vascular endothelial growth factor (VEGF).12 Such soluble mediators trigger intracellular signaling cascades that modulate the proliferation, migration, and the resistance of malignant plasma cells. The interaction between BMSCs and malignant cells is particularly significant, influencing tumor cell proliferation, survival, and disease progression, as well as contributing to drug resistance.13 The interactions of malignant cells with BMSCs and other cells in the BMM are shown in Figure 1. This complex interplay involves cell surface molecules. For instance, intercellular adhesion molecule 1 (ICAM 1) and vascular cell adhesion molecule 1 (VCAM 1) on BMSCs interact with lymphocyte function-associated antigen 1 (LFA-1) and very late antigen 4 (VLA-4) on malignant cells, respectively. These interactions trigger the activation of the NF-κB pathway, inducing the secretion of IL-6 by BMSCs, and this subsequently promotes the production of VEGF in malignant cells.14 Beyond the NF-κB pathway, other signaling pathways such as MAPK, JAK/STAT, and PI3K/AKT/mTOR are also involved in mediating the response within the BMM. Additionally, molecules like α4β7 integrin, P-selectin glycoprotein ligand-1, and CD147 contribute to cell adhesion and migration.15
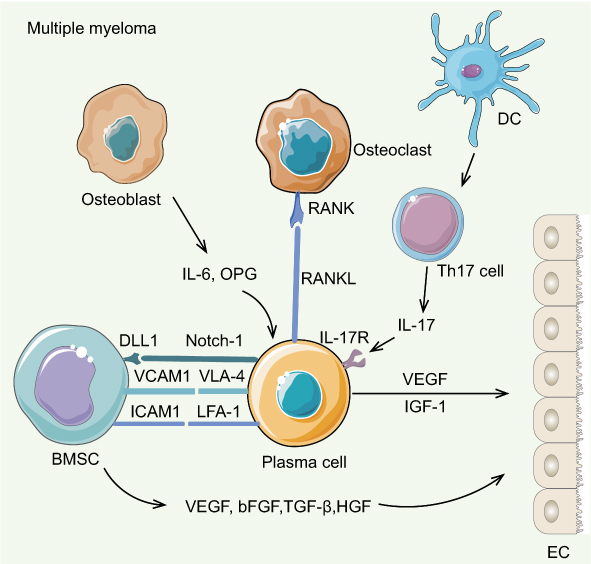 |
Figure 1 Schematic diagram of the bone marrow microenvironment. Abbreviations: BMSC, Bone marrow stromal cell; DC, Dendritic cell; VCAM 1, Vascular cell adhesion molecule 1; VLA-4, Very late antigen 4; ICAM 1, Intercellular adhesion molecule 1; LFA-1, Lymphocyte function-associated antigen 1; IGF-1, Insulin-like growth factor 1; HGF, Hepatocyte growth factor; OPG, Osteoprotegerin; RANK(L), Receptor activator of nuclear factor kappa B (ligand); VEGF, Vascular endothelial growth factor; bFGF, basal fibroblast growth factor; TGF-β, Transforming growth factor beta; IL, interleukin; OPG, Oesteoprotegerin; LFA-1, Lymphocyte function-associated antigen 1; EC, Endothelial cell. |
A hallmark of the advancing disease is the abnormal proliferation of osteoblasts and osteoclasts. For instance, the balance between osteoclast activation and osteoblast proliferation is disrupted in MM, resulting in bone injury. Bone formation and resorption are typically regulated by the NF-κ receptor activator of NF-κB ligand (RANKL) and osteoprotegerin (OPG).16 During disease progression, RANKL secreted by BMSCs, and macrophage inflammatory protein 1 alpha (MIP-1α) from MM cells, promote the activation of osteoclasts. Although OPG can restrict osteoclast formation, its expression can be downregulated by elevated local levels of IL-3, Dickkopf-related protein 1 (DKK-1), and hepatocyte growth factor (HGF).14 Notch signaling promotes the generation of IGF, VEGF, and IL-6, thereby contributing to the proliferation and survival of malignant cells.17 Robust signaling via direct intercellular communication and soluble signaling molecules induces hypervascularization and angiogenesis in leukemic bone marrow, which promotes the proliferation and survival of malignant cells, and consequently contributes to elevated drug resistance.18
Medication resistance poses a critical challenge in tumor therapy. The interaction between MM cells and BMSCs gives rise to cell adhesion-mediated resistance. Macrophages, stromal cells, endothelial cells and other components in the BMM participate in the formation of vascular niches, promote the proliferation and survival of MM cells, and protect them from anti-myeloma drugs.19 In addition, factors in the microenvironment, such as VEGF family, monocyte chemoattractant protein-1 (MCP-1), TNF-α and IL-8, which are important for enhancing angiogenesis in MM, parallel disease progression.19 Immune escape can be induced by the BMM through the immunosuppressive effects exerted by regulatory T cells, regulatory B cells, and myeloid derived suppressor cells (MDSCs). The immunosuppressive activity of MDSCs is largely driven by activation of the STAT3 pathway and extends to the inhibition of the proliferation of both cytotoxic T lymphocytes and natural killer (NK) cells.20 Furthermore, osteoclasts serve a crucial function in the immunosuppressive microenvironment. When signaling is stimulated, the bone marrow microenvironment becomes antiapoptotic by upregulating antiapoptotic regulatory proteins.21 For example, there is a marked upregulation of BCL-XL, BCL-2, and MCL-1. The elevation of soluble factors and surface molecules, including transforming growth factor beta (TGF-β), IL-6, IL-10, ICAM 1, APRIL, and CD40, promotes immune escape and resistance.
Multiple mechanisms within the BMM contribute directly to drug resistance in MM. First, cell adhesion-mediated drug resistance (CAM-DR) arises from the interaction between MM cells and BMSCs via adhesion molecules such as VLA-4, LFA-1, and their respective ligands VCAM-1 and ICAM-1, activating the NF-κB pathway and promoting the secretion of protective cytokines like IL-6.14 Second, soluble factors within the BMM, including IL-6, IGF-1, VEGF, and TGF-β, activate downstream signaling cascades (including JAK/STAT3, PI3K/AKT, and MAPK pathways) that upregulate anti-apoptotic proteins such as BCL-2, BCL-XL, and MCL-1.21 Third, hypoxic conditions in the bone marrow niche further exacerbate resistance. Zhang et al reported that hypoxic BMSCs secrete extracellular vesicles enriched with miR-140-5p and miR-28-3p, which target SPRED1 and activate MAPK signaling to confer bortezomib (BTZ) resistance in MM cells.22 Additionally, immune evasion mechanisms driven by regulatory T cells, regulatory B cells, and MDSCs within the BMM create an immunosuppressive niche that protects MM cells from both conventional chemotherapy and immunotherapies.20
Challenges to the Targeting of MM
Conventional Therapy Limitations
The conventional therapies for MM include immunomodulators, proteasome inhibitors, chemotherapy, BCL-2 inhibitors, and more.23 The key limitations of these therapies for MM stem primarily from the inadequate targeting of tumor cells, as well as systemic toxicity, adverse side effects, and a low therapeutic index. Additionally, the poor solubility of most anti-MM agents is another bottleneck.24 For example, doxorubicin (DOX) is an anthracycline chemotherapy drug commonly used in the clinical treatment of malignant hematological tumors. Its therapeutic effect on hematological tumors is significant. However, due to the side effects of DOX in practical applications, such as cardiotoxicity, hepatotoxicity, bone marrow suppression, etc, the clinical application of DOX is limited to some extent.
Multiple active targeting strategies have been proposed for the delivery of imaging agents or chemotherapeutic agents to tumors. Antibody couplers carrying multiple small-molecule drugs or imaging agents are able to effectively target tumor cells following intravesical administration.25 However, such couplings pass through the bloodstream, which may lead to premature loss of the drug/imaging agent. To date, the majority of antibody-drug conjugates (ADCs) that have been developed exhibit predominantly hematological toxicity. GSK2857916, for instance, is a humanized IgG1 anti-BCMA antibody conjugated with monomethyl auristatin E (MMAE) that has been approved for the treatment of MM.26 While this delivery strategy employs anti-BCMA antibodies to target MMAF toxins to MM cells, most malignant plasma cells reside in the bone marrow, that may cause greater hematologic toxicity with ADC-based delivery than when such toxins are applied to solid tumors. Nanoparticle-drug couplings circumvent some of these limitations as they improve drug complexation capacity (due to larger size) and more favorable pharmacology (ie, shorter circulation time leading to faster tumor accumulation, less systemic exposure, and more rapid clearance compared to ADCs). They are further designed for tumor targeting via peptides,27 small molecules,28 or antibodies.29
Dose-limiting toxicities and drug resistance are major obstacles to MM treatment. Tumor cell chemoresistance serves as a key driver of ineffective chemotherapy and cancer relapse, while boosting intratumoral drug accumulation represents a promising approach to strengthen the tumor-eliminating effect. Drug-encapsulated nanoparticles are capable of substantially enhance the cellular uptake and accumulation of the loaded agents, which in turn improves the therapeutic efficacy compared to free chemotherapeutic drugs.30 Cell surface ion channel proteins serve a crucial function in regulating drug resistance, with P-glycoprotein being notably important for mediating drug resistance in cancer cells. There is an urgent need for new therapies to overcome the bottleneck in MM treatment.
Chimeric antigen receptor (CAR) T-cell therapy represents a transformative advancement in the treatment of MM. The approval of idecabtagen vicleucel (ide-cel) and ciltacabtagen autoleucel (cilta-cel) manifested the new era of cellular immunotherapy for MM therapy.31 However, an increasing amount of long-term clinical follow-up data, related studies, and real-world evidence have revealed the limitations of CAR-T therapy. A significant number of patients never achieve a molecular response, and many ultimately relapse.32,33 The majority of patients ultimately experience a relapse, during which the target antigen expression of MM cells often changes.31 In addition, patients in the late stage have not responded to multiple treatments and have limited options for bridging therapy. Consequently, they tend to bear a substantial disease burden, thereby elevating the likelihood of adverse events associated with CAR-T therapy, such as cytokine release syndrome, immune effector cell-associated neurotoxicity syndrome, and late neurologic syndromes.34,35
Key Challenges for Nanomedicine Targeting in MM
The versatile functionalities and robust loading capabilities of nanomedicines render them appealing candidates for designing MM-targeted delivery and treatment approaches, while numerous obstacles still remain to be addressed. One of the key challenges of effectively leveraging nanomedicine effectively in MM treatment is developing nanocarriers with targeted biophilic affinity for MM cells and effective binding ability in the local microenvironment. Unlike solid tumors, the research and application of nanocarriers in MM is limited.28,36 Following intravenous administration, nanocarriers undergo passive absorbed via the enhanced permeability retention (EPR) effect in solid tumors, while hematologic malignancies pose relatively fewer obstacles to efficient drug delivery. Specifically, nanoparticle accumulation in MM is facilitated by three factors: (i) the distribution of high-flow blood/infusion agents into the bone marrow via fenestrated gap junctions, (ii) neovascularization in plasmacytomas, which further increases passive tumor delivery, and (iii) the absence of a stromal barrier.37 Consequently, unlike most solid tumors, nanoparticulate agents entering the systemic circulation can reach MM cells at a close enough proximity to interact directly with them. The remaining nanoparticles disperse to other organs, including the liver, lung, and spleen, before being degraded and/or cleared by the kidney. However, a patient’s tumor pathophysiological characteristics and the physical parameters of the nanoparticles may restrict the efficiency of the passive targeting mechanism.38 Additionally, the correlation between the EPR effect and the clinical uptake of nanoparticles in human tumors is controversial.39 Therefore, the natural barriers formed by the body are the primary challenges that must be overcome to achieve effective interactions of nanoparticles with MM cells.
The uniform distribution of nanoparticles is hindered by alterations in mesenchymal pressure within the tumor site after intravenous injection, which limits their interaction with tumor cells.40 Subsequently, the rate of internalization and downregulation of surface receptors on tumor cells may impede MM binding. The shape, size, and surface properties of nanoparticles can influence their interaction with immune cells and cellular components of the tumor microenvironment, which may interfere with tumor cellular internalization.41 Cylindrical shapes exhibit the highest internalization rates,38 while nanoparticles smaller than 10 nm are easily filtered out by the kidney after circulating in the bloodstream.42 Conversely, nanoparticles exceeding 15 nm in size may causetoxicity due to incomplete renal clearance.38 Consequently, passive targeting remains the primary delivery of nanoparticles in hematological tumors and the development of active targeting mechanisms is a critical challenge for effectively applying nanomedicines in MM.
Nanotherapeutics for the Treatment of MM
The development of nanotechnology has had a profound impact on the biomedical field, mainly in the diagnosis and treatment of tumors. Nanomedicine has attracted increasing attention due to its scientific value and potential application prospects. Nanomedicine exhibits the capacity to overcome these limitations by developing advanced DDS that are capable of being delivered into the intricate BMM and effectively target myeloma cells. This improved the pharmacokinetics and biodistribution of therapeutic drugs. At the same time, nanocarriers can protect the therapeutic molecules from degradation, improve circulation with a stable drug retention time in the body, and enhance the solubility of hydrophobic drugs due to the high specific surface area of nanoparticles. Previous studies have demonstrated that the application of nanocarriers can enhance drug tolerance and therapeutic efficacy, and facilitate drug across biological barriers, including endothelial and epithelial barriers, with minimal immunogenicity.43
The utilisation of drug carriers based on nanoparticles and intrinsically active nanodrugs in the treatment of MM has the potential to enhance therapeutic efficacy and mitigate adverse effects through preferential effects in the bone marrow niche of the development of myeloma cells. The delivery of anticancer drugs using nanoparticles can be achieved in a number of ways, which can be divided into passive, active, or trigger positioning.9 The passive target method employs passive diffusion nanoparticles, which traverse the tumor vascular endothelial barrier and the EPR effect, particularly for nanoparticles characterised by prolonged blood circulation, such as liposomes.44 Active targeting involves the coupling of nanoparticles with high-affinity ligands, which can be selectively recognized by surface receptors on cancer cells, thereby triggering receptor-mediated endocytosis, or surface receptors on endothelial cells to minimize the systemic toxicity of conventional drugs.45 Finally, nanodrugs have been developed for targeted drug release at tumor sites. These can be triggered by responsive mechanisms, including pH, temperature, magnetic field, ultrasound, or light.46
The aforementioned treatments have been developed using different classes of nanoparticles from organic or inorganic sources (eg, liposomes, micelles, polymers, and biomimetic nanoparticles) and inorganic nanoparticles with different shapes, sizes, and degrees of surface functionalization (Figure 2 and Table 1). The most salient features of the material under discussion are its biodegradability and biocompatibility. The substance’s combination with hydrophilic and hydrophobic small molecules or macromolecules has been demonstrated to be effective in preventing degradation and ensuring sustained drug release. Furthermore, the possibility of surface functionalization to improve the interaction with biomaterials has been identified, as well as the ability to target specific organs, cells, or proteins.47
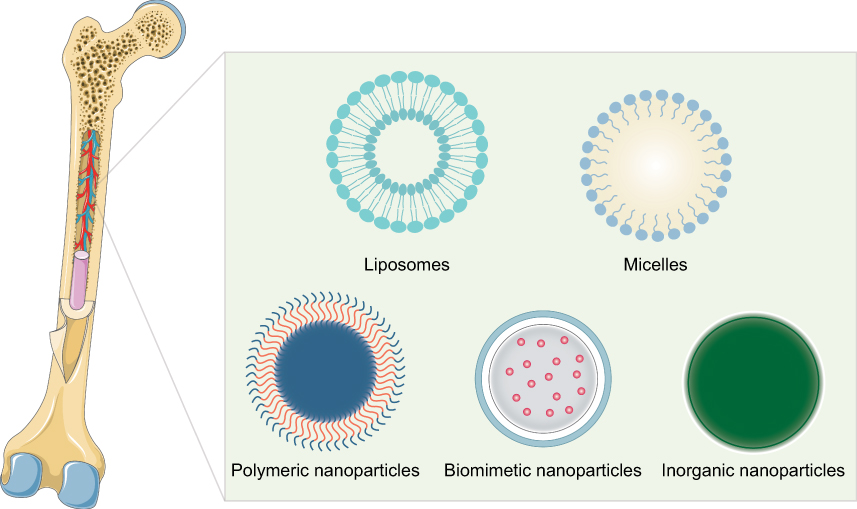 |
Figure 2 Nano-drug delivery system in MM. |
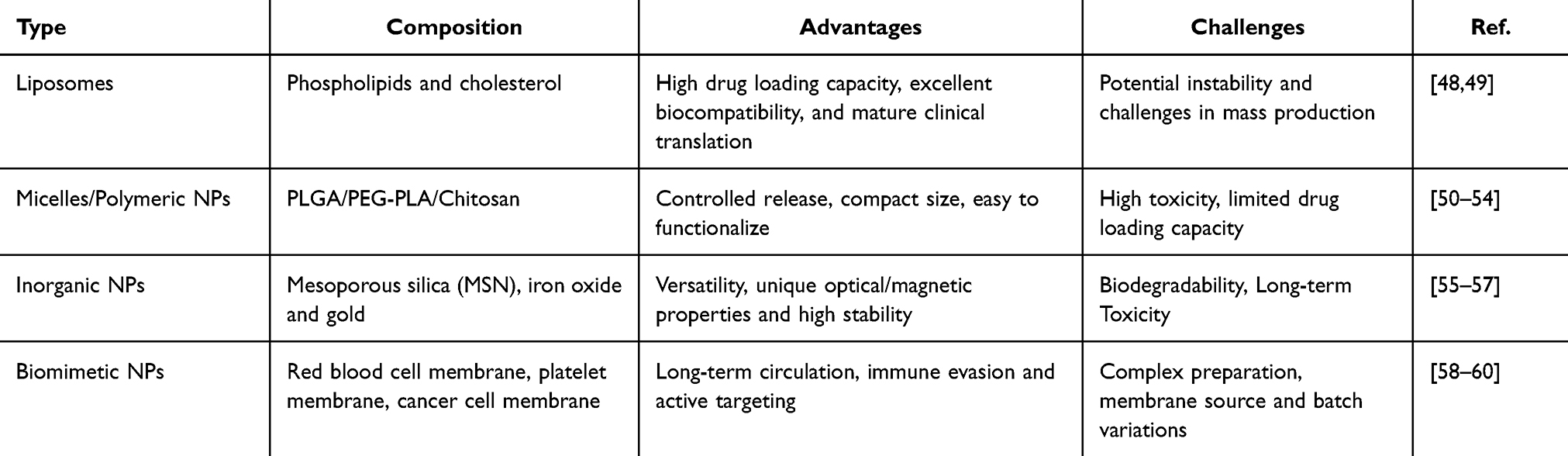 |
Table 1 List of Nano-Drug Delivery Systems in MM and the Advantages and Challenges |
Liposomes
Liposomes represent the most commonly clinically accepted drug delivery system. The advantages of this system include biocompatibility, biodegradability, and non-immunogenicity. These characteristics contribute to the system’s strengths in targeted delivery and sustained release of loaded drugs. Besides, liposomes could also prolong blood circulation time, improve the therapeutic effect of the loaded drug, and reduce the toxicity.61 Liposomes are composed of phospholipids and cholesterol, which can be loaded with either hydrophobic or hydrophilic drug molecules.62 Doxil® is the first chemotherapeutic nanomedicine to be clinically approved, having been authorised by the FDA in 1995. The circulation time of Doxil is one hundred times longer than that of free DOX.63 In recent years, significant advancements in liposome technology have catalysed the swift development of novel pharmaceutical liposomal applications.64 In the domain of liposome delivery systems, PEGylated liposomal nanoparticles have been shown to exhibit several advantageous properties. These include high drug-loading capabilities, ease of incorporation of different functionalities, elevated biocompatibility, and precise control over particle size. The PEGylated liposomal formulation of DOX has been demonstrated to reduce cardiotoxicity. The loading of carfilzomib (CFZ) into liposomes in conjunction with DOX was undertaken to enhance the anticancer effects of the combination at its optimal synergistic ratio. The combination of the aforementioned elements with the specific delivery method demonstrated high stability and repeatability. Furthermore, it was found that the efficacy of the combination was improved in comparison to the efficacy of the free drug combination.44
Federico et al improved the treatments for MM by synchronizing the delivery of BTZ and BMM-disrupting agents to overcome BMM-induced drug resistance. They found that co-delivery of BTZ and a ROCK inhibitor via P-selectin glycoprotein ligand-1 (PSGL-1)-functionalized targeting liposomes to the BMM is more effective than free drugs, non-targeted liposomes, or single-agent controls, and the liposome also reduces severe BTZ-associated side effects.65 The present study investigates the potential of liposomal dexamethasone to accumulate in cancer-bearing human bone scaffolds, with the objective of inhibiting tumour growth. In comparison, the investigation of free dexamethasone revealed its inactivity at an equivalent dose.66 Bilgicer et al designed a BTZ prodrug liposome based on a boronic ester bond-linked lipid-BTZ, which can significantly inhibit proteasome activity and kill myeloma cells.49 Kolemen et al summarized the latest developments in the application of targeted liposomal nanoparticles as a drug carrier system for the management of MM.67
Polymeric Nanoparticles
The formation of polymeric nanosystems typically occurs through the process of self-assembly of amphiphilic polymers in an aqueous environment. These nanosystems encompass a variety of structures including polymeric nanoparticles and polymer micelles. The encapsulation of hydrophobic and hydrophilic drugs within these nanosystems has proven to be a highly effective therapeutic approach.68,69 Polymer nanomedicines have been widely used in cancer treatment due to their advantages of good stability, controllable structure and chemical diversity. At present, polymer micelle paclitaxel nanomedicine (Genexol-PM) based on polyethylene glycol-b-polylactide (PEG-PLA) has been approved by the FDA for the treatment of breast and ovarian cancer.70 In addition, there are a number of different types of polymer nanomedicines in clinical trials at various stages.71,72 Among them, the polymer nanodrugs used to treat MM mainly include micelles and nanoparticles.
Qian et al prepared camptothecin (CPT)-encapsulated nanodrugs based on N,N,N-trimethylchitosan, and studied its antitumor effect in the MPC-11 MM model of subcutaneous tumors.73 It was found that compared with free CPT, CPT nanodrugs could inhibit tumor growth more effectively, thereby significantly prolonging the mental survival of tumor-bearing mice, indicating that chitosan nanoparticles could effectively improve the stability and anti-tumor activity of CPT. Lee utilized polyethylene glycol-b-polycaprolactone (PEG-PCL) micelles to encapsulate the proteasome inhibitor CFZ to prevent CFZ degradation during cycling.74 The results showed that compared with free CFZ, the stability of CFZ in polymer nanoparticles was greatly improved, and the killing effect on MM cells was further enhanced.
Micelles are artificial vesicles that are structurally analogous to liposomes. They are formed by self-assembly of amphiphilic lipids, encapsulating hydrophobic cores that can carry hydrophobic drugs. Polymer micelles represent a particularly promising class of nanocarrier for tumor-targeted delivery due to a number of factors. Firstly, they exhibit excellent biocompatibility. Secondly, they have an extended cycle time. Thirdly, they have a suitable particle size (10–100 nm). Finally, they can dissolve various insoluble drugs. This ability has led to the development of several types of drug-loaded micelles, which are currently being tested in preclinical and clinical trials. Among polymer micelles, lipid core micelles form special groups, namely micelles formed by the coupling of soluble copolymers and lipids, such as polyethylene glycol phosphatidyl ethanolamine (PEG-PE) conjugates.75
CFZ has been introduced into the market as a treatment option for refractory MM, and many efforts have been made to increase its short cycle time. A core disulfide cross-linked biodegradable micelle labelled with A6 peptide (KPSSPPEE), known as A6 polysilicone micelle (A6-PM), was recently synthesized from poly(ethylene glycol)-b-poly(dithiolane trimethylene-co-ε-caprolactone) (PEG-P(DTC-co-CL)) copolymer for CFZ delivery in overexpressing CD44 receptors in human MM cell line LP-1. A6 is a 40 nm small octapeptide with favourable anti-angiogenic properties and stable CFZ loading in mice, high stability, ability to target CD44, and relative to other CFZ sulfobutylether-β-cyclodextrin (CFZ-CD) has low systemic toxicity; on the contrary, its half-life is short, lacks selectivity and has poor anti-cancer activity.76
NK012 is a polymer micelle that self-assembles in an aqueous solution from the amphiphilic block polymer PEG-b-polyglutamic acid while loaded with 7-ethyl-10-hydroxycamptothecin (SN-38) (Figure 3A).77 NK012 has been shown to have significant antitumor activity in a variety of tumor models. At the same time, the treatment of NK102 for triple-negative breast cancer, small cell lung cancer, and colorectal cancer has entered the clinical Phase I/II. Morino et al investigated NK012 as a single agent or in combination with BTZ for the treatment of in situ U266B1 MM.78 The study found that NK012 effectively slowed down the osteolytic lesions of tumor-bearing mice and greatly prolonged the survival of mice (Figure 3B). When NK102 was combined with BTZ, the median survival of mice was further prolonged compared with the BTZ treatment group alone, indicating that NK102 had good anti-MM activity and had a certain synergistic therapeutic effect when combined with BTZ (Figure 3C).
 |
Figure 3 Antimyeloma activity of NK012. (A) Schematic structure of NK012. Reproduced from ref.77 with permission. Copyright © 2006, American Association for Cancer Research. (B) X-ray images and H and E staining results of tibial bone destruction after NK012 treatment. Reproduced from ref.78 with permission. Copyright © 2013, John Wiley and Sons. (C) The combination of NK012 and BTZ prolongs median survival in an orthotopic MM model. Reproduced from ref.78 with permission. Copyright © 2013, John Wiley and Sons. |
Chen et al developed micellar nanoparticles that use pH-induced surface charge reversal and reactive oxygen species (ROS) amplification to trigger accelerated drug release.79 These nanoparticles exhibited significant antitumor activity against human prostate cancer cells. Over the past two decades, there has been rapid progress in developing surface-charge-reversible systems for delivering drugs and diagnosing solid tumors. However, there are research gaps in the field of non-solid tumors, including leukemia, lymphoma, and MM. Because of the acidic microenvironment of MM, pH-responsive charge-reversal systems could be a feasible treatment option for this hematologic malignancy. Currently, this is only a theoretical hypothesis. In the future, more efforts will be needed to develop surface-charge-reversible systems that can specifically target hematological tumors.
Inorganic Nanoparticles
Inorganic nanoparticles exhibit unique characteristics in the field of nanomedicine. Metallic nanoparticles exhibit high stability, high purity, and optical properties and can be readily modified at the surface level. For instance, Zhang et al developed iron oxide magnetic materials to modify dimercaptosuccinic acid. BTZ and garcinic acid (GA) were encapsulated within nanoparticles. The combination of BTZ-GA/MNP enhanced the inhibitory effect on cell proliferation and induced cell apoptosis. Conversely, the administration of free BTZ and GA at equivalent doses resulted in a marginal antitumour effect.80 In addition, inorganic nanoparticles improve the performance of chemotherapy agents, enhancing clinical benefits. To overcome the clinical shortcomings of paclitaxel (Taxol), researchers synthesized Fe3O4 nanoparticles loaded with paclitaxel (PTX-NP), which demonstrated the strongest tumor inhibition effect among all the groups.81 Attempts have been made to improve the performance of vincristine due to its high lipophilicity and severe side effects. The risk of side effects was reduced by gold nanoparticles loaded with low doses of vincristine, where the nanogold acted as both drug carriers and therapeutic ingredients, blocking the cells in the S phase.82
The radionuclide 89Zr has been found to naturally attach to the bone, thus allowing it to enhance the therapeutic effect of drugs.83 Titanium dioxide (TiO2) nanoparticles coated with Tf and radiolabeled with 89Zr were found to be capable of targeting bone marrow and imaging the distribution of nanoparticles in a mouse model. Moreover, in the presence of 89Zr, the TiO2 nanoparticles were capable of generating ROS and inducing cell death via the apoptotic pathway.84 Silica is a safe and biocompatible inorganic material, and mesoporous silica nanoparticles (MSNs) are readily degraded and excreted in urine.85 Nigro et al developed a nanomedicine, FOL-MSN-BTZ, which encapsulates BTZ into MSNs and is surface-modified with folic acid to alter metabolism and induce death in MM cells.86 The present study demonstrated that FOL-MSN-BTZ impaired mitochondrial function and decreased ATP levels, whilst concomitantly increasing ROS production. Concurrently, FOL-MSN does not affect normal cellular metabolism, thereby ensuring the safety of the material. The efficacy and safety of treatment is enhanced by this drug delivery system. Zinc oxide nanoparticles have been extensively utilised in biomedical fields. Moreover, the extant evidence suggests that zinc oxide nanoparticles could significantly induce human MM cell death in a time- and dose-dependent manner in vitro (Figure 4A). In the meantime, it has been demonstrated that zinc oxide nanoparticles have the capacity to reduce ATP, thereby effectively enhancing the generation of ROS, increasing Cyt-C, Apaf-1, Caspase-9, and Caspase-3 expression at the mRNA and protein levels in human MM cells, and initiating MM cell apoptosis. This indicates that Cyt-C, Apaf-1, Caspase-9, and Caspase-3 play crucial roles in zinc oxide nanoparticles-induced, mitochondria-mediated apoptosis in human MM cells (Figure 4B and C).87 In addition, arsenic trioxide has been suggested as a potential treatment for patients with refractory MM.88
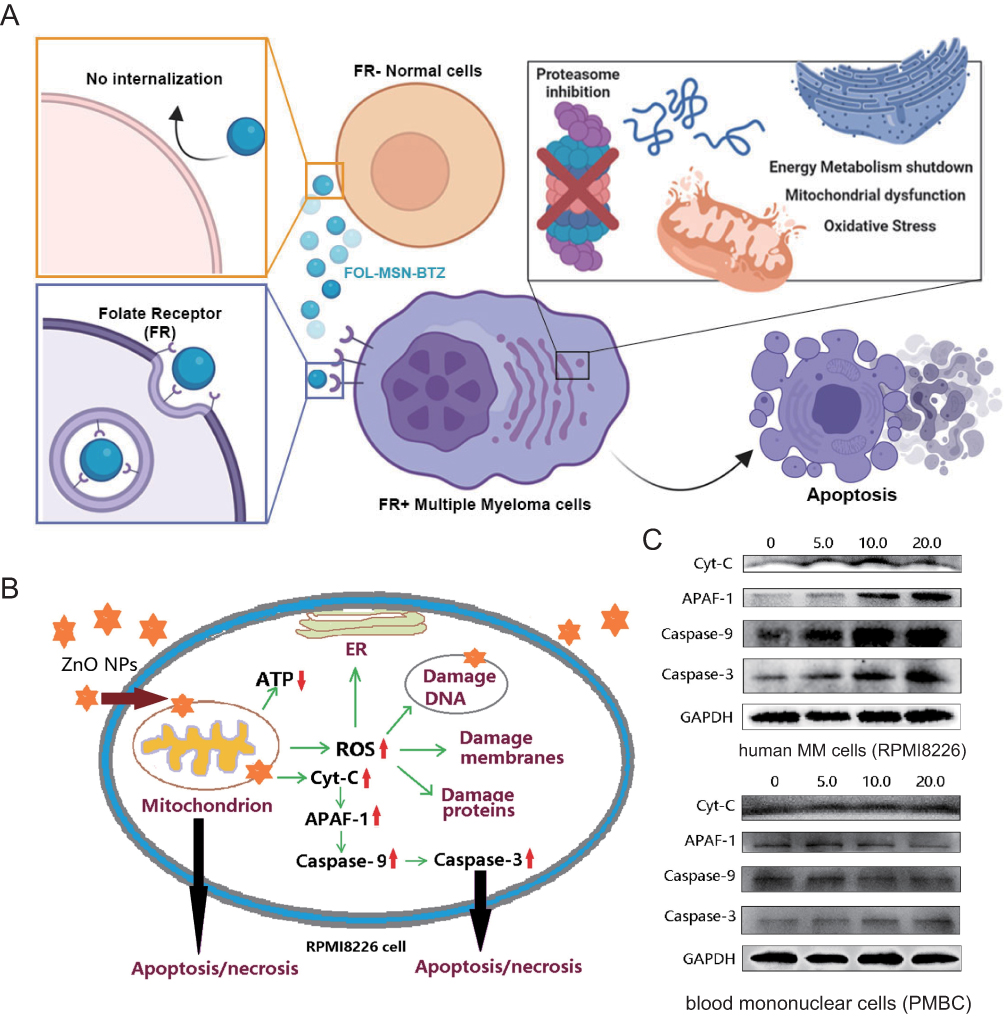 |
Figure 4 The future of MM therapy based on inorganic nanoparticles. (A) Schematic of the FOL-MSN-BTZ mechanism for MM treatment. Reproduced from ref.86 under a Creative Commons CC BY license. Copyright © 2020 MDPI. (B and C) ZnO NPs induced the human MM cell death via ROS and Caspase-dependent signaling pathways. Reproduced from ref.87 under a Creative Commons CC BY license. Copyright © 2020 Elsevier. |
Biomimetic Nanoparticles
It has been reported that circulating bone marrow cells can only survive and proliferate when they migrate and return to the BMM, a process referred to as “bone marrow homing (BMH)”.89 BMH is a distinctive and significant characteristic of bone marrow cells. The phenomenon under discussion has been observed to occur not only in the early stage of myeloma, but also throughout the development process of MM including the occurrence, development, metastasis and treatments of the disease.90 In recent years, there has been a growing interest in biomimetic nanoparticles that are based on cell membrane-coated nanoparticles. It should be noted that many biomimetic nanoparticle systems incorporate a polymeric nanoparticle core to provide structural stability and drug-loading capacity. Cell membrane-coated nanoparticles inherently mimic the characteristics of their membrane-derived source cells, thereby endowing them with a wide range of functions, such as long circulation, homologous targeting, immune escape, and disease-related targeting, because the antigen profiles are retained on the cell membrane. A considerable number of studies have been conducted on the development of platelet,58 red blood cell (RBC),59 and tumor cell membranes91 coated nanoparticle systems, as well as a “molecular decoy” strategy mediated by extracellular vesicles (eg, exosomes) (Figure 5 and Table 2).92
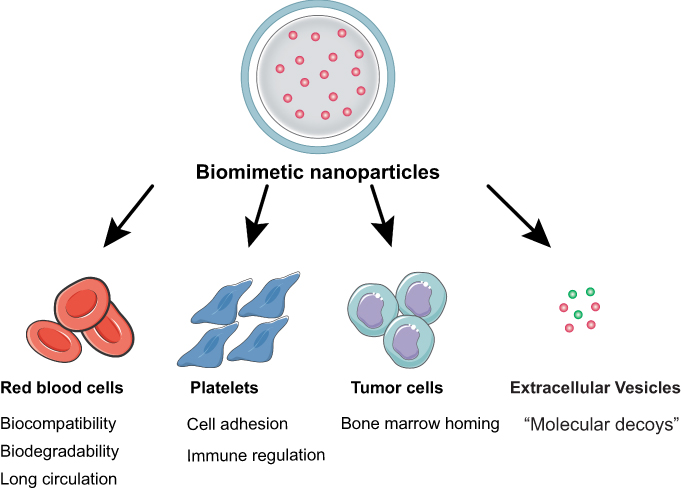 |
Figure 5 Classification of biomimetic nanoparticles and their characteristics. |
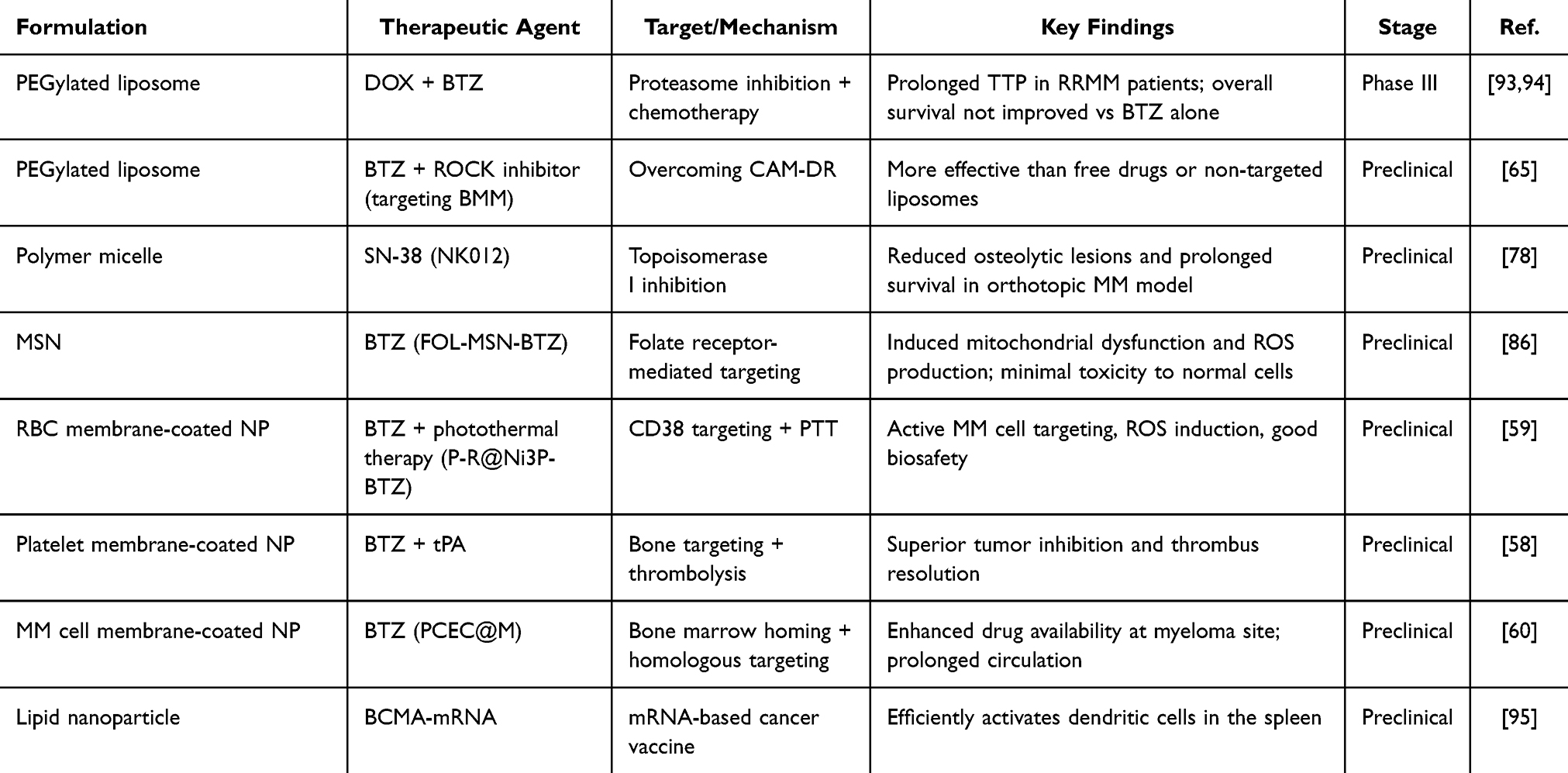 |
Table 2 Representative Nanomedicine Formulations for Multiple Myeloma Therapy in Preclinical and Clinical Studies |
RBCs are the most abundant circulating cells in the blood and have been extensively utilised in DDS due to their biocompatibility, biodegradability, and prolonged circulating half-life. Consequently, the “camouflage” provided by the RBC membrane renders nanoparticles a platform to combine the advantages of natural RBC membranes with those of nanomaterials. Zhang et al designed and constructed an innovative nanoparticle-based drug delivery system, P-R@Ni3P-BTZ.59 P-R@Ni3P-BTZ is a nanocomposite material that consists of two parts, as illustrated in Figure 6A. The first component is a drug carrier (Ni3P), which combines photothermal therapy (PTT) with chemotherapy by loading BTZ. The second component is the shell (P-R), which consists of a CD38 targeting peptide P-modified erythrocyte membrane nanovesicle. It has been demonstrated that P-R@Ni3P-BTZ has significant antitumor effects, as it is capable of actively targeting MM cells in both in vitro and in vivo settings. The P-R@Ni3P-BTZ compound has been demonstrated to induce significant intracellular ROS and to increase the apoptosis of MM cells. Furthermore, P-R@Ni3P-BTZ demonstrated favourable biocompatibility and biosafety in vitro and in vivo.
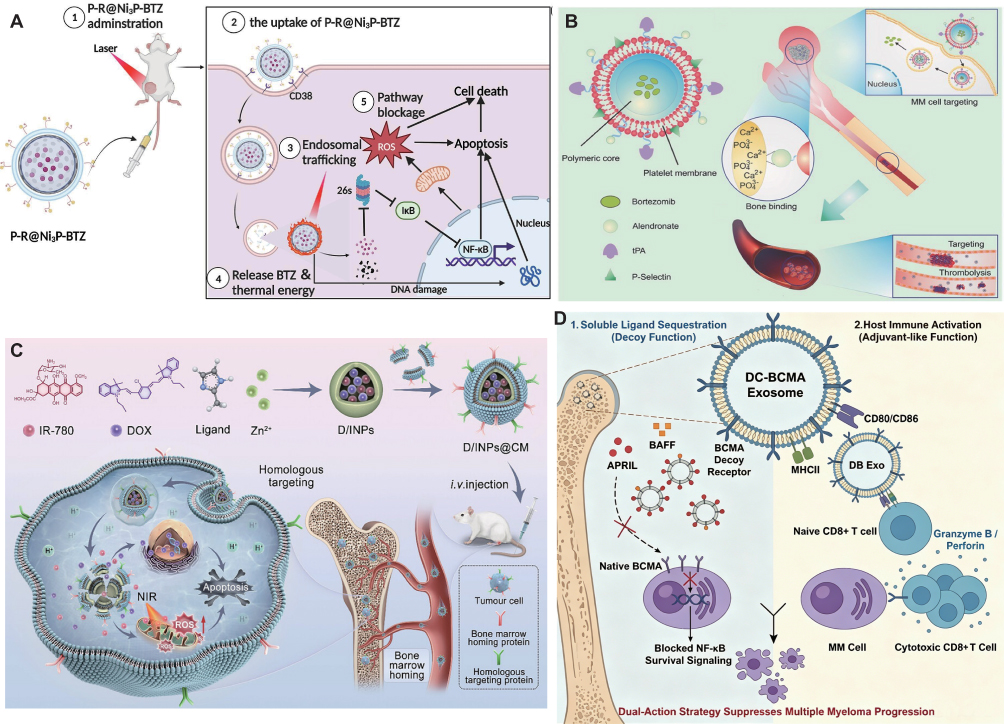 |
Figure 6 Biomimetic nanoparticle systems in MM. (A) A novel nanomedicine delivery system that employs RBC membrane camouflage for the delivery of photothermal and chemotherapy agents in the treatment of multiple myeloma. Reproduced from ref.59 under a Creative Commons CC BY license. Copyright © 2023 Elsevier. (B) The schematic of acid-responsive MM-targeted polymeric nanoparticles with platelet membrane modification, which was developed for inhibiting MM growth. Reproduced from ref.58 with permission. Copyright © 2016 John Wiley and Sons. (C) Novel biomimetic zeolitic imidazolate framework-8 (ZIF-8) co-loading DOX and IR-780 and coated with the MM cell membrane (D/INPs@CM) for the targeted treatment of multiple myeloma. Reproduced from ref.91 under a Creative Commons CC BY license. Copyright © 2024 John Wiley and Sons. (D) Schematic of a cell-free, dual-function therapeutic agent based on BCMA, engineered to exhibit both “decoy-like” and “adjuvant-like” functions, with the goal of reversing the immunosuppressive state of the bone marrow microenvironment. Reproduced from ref.92 under a Creative Commons CC BY license. Copyright © 2024 John Wiley and Sons. |
Platelets are a distinctive cellular component that has the capacity to bind to a variety of disease-related substrates. The resulting nanoparticles possess a right-side-out unilamellar membrane coating functionalized with immunomodulatory and adhesion antigens associated with platelets. In comparison with uncoated particles, the platelet membrane-cloaked nanoparticles have reduced cellular uptake by macrophage-like cells and lack particle-induced complement activation in autologous human plasma. The cloaked nanoparticles have been demonstrated to display platelet-mimicking properties, including the capacity for selective adhesion to damaged human and rodent vasculatures as well as enhanced binding to platelet-adhering pathogens. Hu et al developed a platelet membrane-coated biomimetic nanocarrier for the targeted delivery of BTZ, which could sequentially target the bone microenvironment and myeloma cells to enhance the drug availability at the myeloma site and decrease off-target effects, was developed for inhibiting MM growth and simultaneously eradicating thrombus complications (Figure 6B).58 The pH-responsive nanoparticles were wrapped with platelet membrane (PM-NP) and the nanoparticles were targeted to NCI-H929 cells via CD44. Once the nanoparticles were internalized by the myeloma cells, the intracellular drug was released due to the acid-responsive behavior. Additionally, alendronate was attached to the surface of the nanoparticles to target the accumulation at the bone site. Co-delivery of BTZ with tissue plasminogen activator (tPA) has been demonstrated to facilitate the inhibition of tumour growth, the dissolution of thrombus, and the reduction of the risk of thrombotic complications. It was demonstrated that targeted NP-BTZ exhibited elevated levels of cellular toxicity in NCI-H929 cells. Furthermore, its therapeutic efficacy in targeting strategies for both bone and MM cells was superior.58
MM cells are known to survive primarily in the bone marrow and have been observed to exhibit BMH properties (Figure 5). The hypothesis that cell membrane-coated nanomedicines can inherit the properties of the source cells is one that merits further investigation. Gao et al presented a novel biomimetic zeolitic imidazolate framework-8 (ZIF-8) nanoparticle (D/INPs@CM) by integrating DOX, IR-780, and the MM cell membrane. The D/INPs@CM can target BMM due to the BMH and homologous targeting properties of the MM cell membrane (Figure 6C).91 The ZIF-8 nanoparticles can burst and release the co-loaded DOX and IR-780 in response to an acidic tumor microenvironment, enabling targeted PDT/PTT/chemotherapy without noticeable systemic toxicity. These features suggest that biomimetic nanocarriers have great potential for precisely targeting MM and other hematological malignancies.
Zeng et al developed DB Exo, an allogeneic DC-derived exosome platform engineered to surface display BCMA that acted as molecular decoys, predominantly sequestering soluble APRIL with partial BAFF attenuation, thereby effectively disrupting NF-κB pro-survival signaling in MM cells, and their findings established DB Exo as a promising cell-free strategy for MM treatment by integrating targeted cytokine blockade with in situ immune activation (Figure 6D).92 Furthermore, Zhang et al developed a bone-marrow-targeting bispecific nanosystem (CSF@E-Hn) based on hematopoietic-stem-cell-derived nanovesicles that activated endogenous NK cells for MM treatment, offering a novel strategy to target the bone marrow niche.96
Beyond conventional nanocarriers, emerging mRNA-based nano-vaccines have shown considerable promise in preclinical MM models. Van der Vreken et al developed Galsomes—lipid nanoparticles co-encapsulating antigen mRNA and the iNKT agonist α-galactosylceramide—which activated both CD8⁺ T cells and iNKT cells and significantly reduced MM growth when combined with a CD40 agonist.97 Additionally, Dutta et al reported a BCMA-mRNA lipid nanoparticle vaccine that elicited BCMA-specific CD8⁺ cytolytic T cells capable of lysing BCMA⁺ MM cells in vitro and inhibiting tumor growth in murine MM models.95 In the domain of CAR-T delivery, nanobody-based CAR constructs incorporating dual VHHs targeting BCMA have demonstrated a high overall response rate of 96.3% in RRMM patients, extending efficacy to those with high-risk cytogenetic abnormalities and extramedullary lesions.98
A plethora of studies have explored the potential of various types of nanoparticles and nanocarriers in the treatment of myeloma (Table 2). The utilisation of nanomedicines confers a number of distinct advantages with respect to drug delivery and specificity to the tumour site. The efficacy of nanotechnology-based myeloma therapies has been demonstrated in preclinical and clinical studies, often showing potential improvements over conventional therapies. These advances collectively demonstrate the evolving landscape of nanomedicine strategies for MM, with clinical translation representing the next critical frontier.
Clinical Applications of Nanomedicine for MM Therapy
The application of nanomedicine in MM is rapidly evolving, providing new strategies for the treatment of this refractory hematological tumor by improving drug targeting, reducing toxicities, and overcoming drug resistance. The use of nanomedicine, such as liposomes, polymer nanoparticles, and micelles, has emerged as a significant advancement in the field of chemotherapy. These carriers can encapsulate chemotherapeutic agents, including BTZ and DOX, enhancing their solubility, prolonging their circulation time, and reducing systemic toxicity. For instance, DOX liposome (Doxil®) has been utilized in relapsed/refractory MM, and its capacity to target the BMM is superior to that of conventional agents. PEGylated DOX liposomes have been evaluated in different combination regimens including protease inhibitors or immunomodulatory drugs. The triple regimen of BTZ, PEGylated DOX liposomes, and dexamethasone has been used in the initial treatment of MM. Patients receiving PEGylated DOX liposomes and BTZ had significantly better outcomes than the BTZ monotherapy group.93 However, in long-term follow-up, this combination did not improve overall survival compared to monotherapy.94
An exploratory investigation was conducted into the utilization of nanoparticle albumin-bound paclitaxel (Abraxane®) in the context of recurrent myeloma. A Phase I trial (NCT01365559) enrolled 38 patients and investigated the combination of Abraxane with lenalidomide and dexamethasone.99 The study’s findings were encouraging, with a response rate of 78% and a favorable safety profile. Nevertheless, the study also identified potential challenges associated with the use of nanoparticle-based therapies. For instance, the trial highlighted the necessity for vigilant monitoring of adverse effects potentially attributable to the nanocarriers themselves. This case study exemplifies the potential of nanotechnology to enhance drug delivery and mitigate off-target effects, thereby enhancing the therapeutic index of a treatment.
The enhanced accumulation of nanoparticles at the tumor site is achieved through surface modifications that target MM cell markers, such as CD38, BCMA, and CD138, or by leveraging the EPR effect, which occurs when small molecules with high permeability are traversed by the vasculature of the bone marrow. A notable example is the combination of anti-CD38 antibodies, such as Daratumumab, with nanocarriers, which have been shown to enhance the precision of targeting MM cells. The results of clinical trials have shown that CPX-351 is effective for the treatment of high-risk or secondary acute myeloid leukemia in elderly patients (NCT01696084).100 On October 25, 2022, the US FDA accelerated the approval of Johnson and Johnson’s teclistamab (trade name: tecvayli) for adult patients with relapsed or refractory MM who had undergone at least fourth-line treatment. Previously, on August 23 this year, the European Union EMA also approved the listing of teclistamab, which is the first BCMA/CD3 dual antibody to be listed in the world. Unlike nanomedicines, teclistamab functions as a bispecific antibody that redirects CD3+ T cells to mediate the lysis of BCMA-expressing myeloma cells. The pivotal MajesTEC-1 trial demonstrated an overall response rate of 61.8% (95% CI 52.1–70.9) among heavily pretreated RRMM patients, with a manageable safety profile.92,101 Although teclistamab is an antibody-based therapy rather than a nanomedicine, its development and applications can provide valuable information for designing BCMA/CD3 bispecific targeting strategies. The growing number of clinical trials for nanoparticle-based drugs reflects the expanding interest in applying nanomedicine to MM rather than establishing a “new era centered on nanomedicine” as an established clinical reality.
Notwithstanding the considerable potential of nanomedicine-based therapies in the treatment of myeloma, numerous challenges persist in their clinical implementation. The primary concern is to ensure patient safety. While the utilization of nanocarriers holds great promise in enhancing the delivery of therapeutic agents, it is imperative to acknowledge the concomitant emergence of novel safety concerns. For instance, the materials utilized in the construction of nanocarriers have the potential to elicit adverse biological reactions, including toxicity or inflammatory responses.102 Consequently, rigorous preclinical and clinical testing is imperative to ensure the safety of these nanomaterials.
Conclusions and Outlook
In this review, we have systematically summarized nanomedicine delivery systems for the treatment of MM, covering four major categories of carriers. Liposomal formulations, exemplified by PEGylated liposomes, represent the most clinically advanced category, which has undergone extensive clinical trials and are expected to be gradually incorporated into the clinical treatment of MM. Biomimetic nanoparticles represent one of the most promising strategies, For example, MM cell membrane-camouflaged nanoparticles enter the bone marrow via homing to the bone marrow, while systems coated with platelet and red blood cell membranes provide extended circulation and adhesion capabilities. Beyond these well-studied carrier categories, emerging strategies such as mRNA nano-vaccines and nanobody-based CAR-T constructs are expanding the frontiers of MM nanomedicine. Additionally, novel biomimetic systems with dual targeting modalities have demonstrated enhanced precision therapy in orthotopic models.
Despite the significant potential advantages, achieving effective myeloma targeting of nanomedicines necessitates further detailed investigation and understanding of the challenges associated with systemic drug delivery at preclinical and clinical levels. A further consideration in the realm of targeted drug delivery to bone pertains to the phenomenon of drug accumulation in bone tissue over time, a process that has the potential to engender protracted side effects within the organism. It is imperative that future studies evaluate the long-term effects of targeted formulations coupled with nanomedicines and their efficacy over the course of treatment. Furthermore, effective collaboration between clinicians and researchers specialising in nanomaterials and nanotechnology will enhance research efforts and accelerate the translation of targeted nanomedicines for MM to the clinic in the near future.
Abbreviations
A6-PM, A6 polysilicone micelle; ADCs, antibody-drug conjugates; BMH, bone marrow homing; BMM, bone marrow microenvironment; BMSCs, bone marrow stromal cells; BTZ, bortezomib; CAR, Chimeric antigen receptor; CFZ, Carfilzomib; CFZ-CD, CFZ sulfobutylether-β-cyclodextrin; CPT, camptothecin; DDS, drug delivery systems; DKK-1, Dickkopf-related protein 1; DOX, doxorubicin; EC, Endothelial cell; EPR, enhanced permeability retention; GA, garcinic acid; HGF, hepatocyte growth factor; ICAM 1, intercellular adhesion molecule 1; IGF, growth factors like insulin-like growth factor; IL, interleukin; LFA-1, lymphocyte function-associated antigen 1; MCP-1, monocyte chemoattractant protein-1; MDSCs, myeloid derived suppressor cells; MIP-1a, macrophage inflammatory protein 1 alpha; MM, Multiple myeloma; MMAE, monomethyl auristatin E; MSNs, mesoporous silica nanoparticles; NF-κB, nuclear factor kappa-B; NK, natural killer; OPG, osteoprotegerin; PCEC, poly(ε-caprolactone)–poly(ethylene glycol)–poly(ε-caprolactone); PEG-P (DTC-co-CL), poly(ethylene glycol)-b-poly(dithiolane trimethylene-co-ε-caprolactone); PEG-PCL, polyethylene glycol-b-polycaprolacton; PEG-PE, polyethylene glycol phosphatidyl ethanolamine; PEG-PLA, polyethylene glycol-b-polylactide; PSGL-1, P-selectin glycoprotein ligand-1; PTT, photothermal therapy; RANKL, receptor activator of NF-κB ligand; RBC, red blood cell; ROS, reactive oxygen species; SN-38, 7-ethyl-10-hydroxycamptothecin; TGF-β, transforming growth factor beta; TNF-α, tumor necrosis factor alpha; tPA, tissue plasminogen activator; VCAM 1, vascular cell adhesion molecule 1; VEGF, vascular endothelial growth factor; VLA-4, very late antigen 4; WHO, World Health Organization.
Data Sharing Statement
All data and materials are available from publications, and the sources have been cited.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We are thankful for the support from the Zhejiang Provincial Natural Science Foundation of China (LQ24H300006) and the National Natural Science Foundation of China (82204282).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024;99(9):1802–19. doi:10.1002/ajh.27422
2. Landgren O, Rajkumar SV. New developments in diagnosis, prognosis, and assessment of response in multiple myeloma. Clin Cancer Res. 2016;22(22):5428–5433. doi:10.1158/1078-0432.Ccr-16-0866
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
4. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11):1046–1060. doi:10.1056/NEJMra1011442
5. Raje NS, Bhatta S, Terpos E. Role of the RANK/RANKL pathway in multiple myeloma. Clin Cancer Res. 2019;25(1):12–20. doi:10.1158/1078-0432.Ccr-18-1537
6. Chakraborty R, Majhail NS. Treatment and disease-related complications in multiple myeloma: implications for survivorship. Am J Hematol. 2020;95(6):672–690. doi:10.1002/ajh.25764
7. Kuehl WM, Bergsagel PL. Molecular pathogenesis of multiple myeloma and its premalignant precursor. J Clin Invest. 2012;122(10):3456–3463. doi:10.1172/jci61188
8. Jundt F, Pröbsting KS, Anagnostopoulos I, et al. Jagged1-induced Notch signaling drives proliferation of multiple myeloma cells. Blood. 2004;103(9):3511–3515. doi:10.1182/blood-2003-07-2254
9. Zheleznyak A, Shokeen M, Achilefu S. Nanotherapeutics for multiple myeloma. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2018;10(6):e1526. doi:10.1002/wnan.1526
10. Pant A, Laliwala A, Holstein SA, Mohs AM. Recent advances in targeted drug delivery systems for multiple myeloma. J Control Release. 2024;376:215–230. doi:10.1016/j.jconrel.2024.10.003
11. Mu CF, Shen J, Liang J, et al. Targeted drug delivery for tumor therapy inside the bone marrow. Biomaterials. 2018;155:191–202. doi:10.1016/j.biomaterials.2017.11.029
12. Balakumaran A, Robey PG, Fedarko N, Landgren O. Bone marrow microenvironment in myelomagenesis: its potential role in early diagnosis. Expert Rev Mol Diagn. 2010;10(4):465–480. doi:10.1586/erm.10.31
13. Meads MB, Hazlehurst LA, Dalton WS. The bone marrow microenvironment as a tumor sanctuary and contributor to drug resistance. Clin Cancer Res. 2008;14(9):2519–2526. doi:10.1158/1078-0432.Ccr-07-2223
14. García-Ortiz A, Rodríguez-García Y, Encinas J, et al. The role of tumor microenvironment in multiple myeloma development and progression. Cancers. 2021;13(2):217. doi:10.3390/cancers13020217
15. Martínez-Moreno M, Leiva M, Aguilera-Montilla N, et al. In vivo adhesion of malignant B cells to bone marrow microvasculature is regulated by α4β1 cytoplasmic-binding proteins. Leukemia. 2016;30(4):861–872. doi:10.1038/leu.2015.332
16. Ramakrishnan A, Deeg HJ. A novel role for the marrow microenvironment in initiating and sustaining hematopoietic disease. Expert Opin Biol Ther. 2009;9(1):21–28. doi:10.1517/14712590802603093
17. Sison EA, Brown P. The bone marrow microenvironment and leukemia: biology and therapeutic targeting. Expert Rev Hematol. 2011;4(3):271–283. doi:10.1586/ehm.11.30
18. Ayala F, Dewar R, Kieran M, Kalluri R. Contribution of bone microenvironment to leukemogenesis and leukemia progression. Leukemia. 2009;23(12):2233–2241. doi:10.1038/leu.2009.175
19. Ria R, Vacca A. Bone marrow stromal cells-induced drug resistance in multiple myeloma. Int J Mol Sci. 2020;21(2):613. doi:10.3390/ijms21020613
20. Görgün GT, Whitehill G, Anderson JL, et al. Tumor-promoting immune-suppressive myeloid-derived suppressor cells in the multiple myeloma microenvironment in humans. Blood. 2013;121(15):2975–2987. doi:10.1182/blood-2012-08-448548
21. Holthof LC, Mutis T. Challenges for immunotherapy in multiple myeloma: bone marrow microenvironment-mediated immune suppression and immune resistance. Cancers. 2020;12(4):988. doi:10.3390/cancers12040988
22. Zhang H, Du Z, Tu C, Zhou X, Menu E, Wang J. Hypoxic bone marrow stromal cells secrete miR-140-5p and miR-28-3p that target SPRED1 to confer drug resistance in multiple myeloma. Cancer Res. 2024;84(1):39–55. doi:10.1158/0008-5472.Can-23-0189
23. Bhatt P, Kloock C, Comenzo R. Relapsed/refractory multiple myeloma: a review of available therapies and clinical scenarios encountered in myeloma relapse. Curr Oncol. 2023;30(2):2322–2347. doi:10.3390/curroncol30020179
24. Guedes RA, Aniceto N, Andrade MAP, Salvador JAR, Guedes RC. Chemical patterns of proteasome inhibitors: lessons learned from two decades of drug design. Int J Mol Sci. 2019;20(21):5326. doi:10.3390/ijms20215326
25. Beck A, Goetsch L, Dumontet C, Corvaïa N. Strategies and challenges for the next generation of antibody-drug conjugates. Nat Rev Drug Discov. 2017;16(5):315–337. doi:10.1038/nrd.2016.268
26. Tai YT, Mayes PA, Acharya C, et al. Novel anti-B-cell maturation antigen antibody-drug conjugate (GSK2857916) selectively induces killing of multiple myeloma. Blood. 2014;123(20):3128–3138. doi:10.1182/blood-2013-10-535088
27. Liu L, Xu K, Wang H, et al. Self-assembled cationic peptide nanoparticles as an efficient antimicrobial agent. Nat Nanotechnol. 2009;4(7):457–463. doi:10.1038/nnano.2009.153
28. Xiao H, Qi R, Li T, et al. Maximizing synergistic activity when combining rnai and platinum-based anticancer agents. J Am Chem Soc. 2017;139(8):3033–3044. doi:10.1021/jacs.6b12108
29. Kumar S, Aaron J, Sokolov K. Directional conjugation of antibodies to nanoparticles for synthesis of multiplexed optical contrast agents with both delivery and targeting moieties. Nat Protoc. 2008;3(2):314–320. doi:10.1038/nprot.2008.1
30. Markman JL, Rekechenetskiy A, Holler E, Ljubimova JY. Nanomedicine therapeutic approaches to overcome cancer drug resistance. Adv Drug Delivery Rev. 2013;65(13):1866–1879. doi:10.1016/j.addr.2013.09.019
31. Rasche L, Hudecek M, Einsele H. CAR T-cell therapy in multiple myeloma: mission accomplished? Blood. 2024;143(4):305–310. doi:10.1182/blood.2023021221
32. Bethge WA, Martus P, Schmitt M, et al. GLA/DRST real-world outcome analysis of CAR T-cell therapies for large B-cell lymphoma in Germany. Blood. 2022;140(4):349–358. doi:10.1182/blood.2021015209
33. Munshi NC, Anderson LD Jr, Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. doi:10.1056/NEJMoa2024850
34. O’Leary D, Bachanova V. CAR-T for multiple myeloma: practice pearls. Bone Marrow Transplant. 2025;60(7):940–947. doi:10.1038/s41409-025-02582-6
35. Cohen AD, Parekh S, Santomasso BD, et al. Incidence and management of CAR-T neurotoxicity in patients with multiple myeloma treated with ciltacabtagene autoleucel in CARTITUDE studies. Blood Cancer J. 2022;12(2):32. doi:10.1038/s41408-022-00629-1
36. Detappe A, Thomas E, Tibbitt MW, et al. Ultrasmall silica-based bismuth gadolinium nanoparticles for dual magnetic resonance-computed tomography image guided radiation therapy. Nano Lett. 2017;17(3):1733–1740. doi:10.1021/acs.nanolett.6b05055
37. Ghobrial IM, Detappe A, Anderson KC, Steensma DP. The bone-marrow niche in MDS and MGUS: implications for AML and MM. Nat Rev Clin Oncol. 2018;15(4):219–233. doi:10.1038/nrclinonc.2017.197
38. Blanco E, Shen H, Ferrari M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat Biotechnol. 2015;33(9):941–951. doi:10.1038/nbt.3330
39. Torrice M. Does nanomedicine have a delivery problem? ACS Cent Sci. 2016;2(7):434–437. doi:10.1021/acscentsci.6b00190
40. Chauhan VP, Stylianopoulos T, Martin JD, et al. Normalization of tumour blood vessels improves the delivery of nanomedicines in a size-dependent manner. Nat Nanotechnol. 2012;7(6):383–388. doi:10.1038/nnano.2012.45
41. Chithrani BD, Ghazani AA, Chan WC. Determining the size and shape dependence of gold nanoparticle uptake into mammalian cells. Nano Lett. 2006;6(4):662–668. doi:10.1021/nl052396o
42. Sancey L, Kotb S, Truillet C, et al. Long-term in vivo clearance of gadolinium-based AGuIX nanoparticles and their biocompatibility after systemic injection. ACS Nano. 2015;9(3):2477–2488. doi:10.1021/acsnano.5b00552
43. Wicki A, Witzigmann D, Balasubramanian V, Huwyler J. Nanomedicine in cancer therapy: challenges, opportunities, and clinical applications. J Control Release. 2015;200:138–157. doi:10.1016/j.jconrel.2014.12.030
44. Ashley JD, Quinlan CJ, Schroeder VA, et al. Dual carfilzomib and doxorubicin-loaded liposomal nanoparticles for synergistic efficacy in multiple myeloma. Mol Cancer Ther. 2016;15(7):1452–1459. doi:10.1158/1535-7163.Mct-15-0867
45. Maes A, Menu E, Veirman K, Maes K, Vand Erkerken K, De Bruyne E. The therapeutic potential of cell cycle targeting in multiple myeloma. Oncotarget. 2017;8(52):90501–90520. doi:10.18632/oncotarget.18765
46. Sun T, Jiang C. Stimuli-responsive drug delivery systems triggered by intracellular or subcellular microenvironments. Adv Drug Deliv Rev. 2023;196:114773. doi:10.1016/j.addr.2023.114773
47. Zhong H, Chan G, Hu Y, Hu H, Ouyang D. A comprehensive map of FDA-approved pharmaceutical products. Pharmaceutics. 2018;10(4):263. doi:10.3390/pharmaceutics10040263
48. Deshantri AK, Metselaar JM, Zagkou S, et al. Development and characterization of liposomal formulation of bortezomib. Int J Pharm X. 2019;1:100011. doi:10.1016/j.ijpx.2019.100011
49. Ashley JD, Stefanick JF, Schroeder VA, Suckow MA, Kiziltepe T, Bilgicer B. Liposomal bortezomib nanoparticles via boronic ester prodrug formulation for improved therapeutic efficacy in vivo. J Med Chem. 2014;57(12):5282–5292. doi:10.1021/jm500352v
50. Lee ALZ, Voo ZX, Chin W, et al. Injectable coacervate hydrogel for delivery of anticancer drug-loaded nanoparticles in vivo. ACS Appl Mater Interfaces. 2018;10(16):13274–13282. doi:10.1021/acsami.7b14319
51. Gu Z, Wang X, Cheng R, Cheng L, Zhong Z. Hyaluronic acid shell and disulfide-crosslinked core micelles for in vivo targeted delivery of bortezomib for the treatment of multiple myeloma. Acta Biomater. 2018;80:288–295. doi:10.1016/j.actbio.2018.09.022
52. Ye S, Hou Z, Su Y, et al. Rationally engineered Losmapimod encapsulating polymeric nanoparticles for treatment of human multiple myeloma cells. Appl Nanosci. 2021;11(9):2447–2457. doi:10.1007/s13204-021-02010-3
53. Che F, Chen J, Dai J, Liu X. Inhibition of multiple myeloma using 5-Aza-2’-deoxycytidine and bortezomib-loaded self-assembling nanoparticles. Cancer Manag Res. 2020;12:6969–6976. doi:10.2147/cmar.S255682
54. de la Puente P, Luderer MJ, Federico C, et al. Enhancing proteasome-inhibitory activity and specificity of bortezomib by CD38 targeted nanoparticles in multiple myeloma. J Control Release. 2018;270:158–176. doi:10.1016/j.jconrel.2017.11.045
55. De Santo M, Giovinazzo A, Fava M, et al. Engineered mesoporous silica-based nanoparticles as smart chemotherapy nanodevice for bortezomib administration. Mater Chem Front. 2023;7(2):216–229. doi:10.1039/D2QM01009G
56. Cholujova D, Koklesova L, Lukacova Bujnakova Z, et al. In vitro and ex vivo anti-myeloma effects of nanocomposite As(4)S(4)/ZnS/Fe(3)O(4). Sci Rep. 2022;12(1):17961. doi:10.1038/s41598-022-22672-5
57. Bariana M, Zhang B, Sun J, et al. Targeted lymphoma therapy using a gold nanoframework-based drug delivery system. ACS Appl Mater Interfaces. 2023;15(5):6312–6325. doi:10.1021/acsami.2c17214
58. Hu Q, Qian C, Sun W, et al. Engineered nanoplatelets for enhanced treatment of multiple myeloma and thrombus. Adv Mater. 2016;28(43):9573–9580. doi:10.1002/adma.201603463
59. Zhang F, Yang Q, Tang S, et al. CD38-targeted and erythrocyte membrane camouflaged nanodrug delivery system for photothermal and chemotherapy in multiple myeloma. Int J Pharm. 2023;643:123241. doi:10.1016/j.ijpharm.2023.123241
60. Qu Y, Chu B, Wei X, et al. Cancer-cell-biomimetic nanoparticles for targeted therapy of multiple myeloma based on bone marrow homing. Adv Mater. 2022;34(46):e2107883. doi:10.1002/adma.202107883
61. Pattni BS, Chupin VV, Torchilin VP. New developments in liposomal drug delivery. Chem Rev. 2015;115(19):10938–10966. doi:10.1021/acs.chemrev.5b00046
62. Jeong K, Kang CS, Kim Y, Lee YD, Kwon IC, Kim S. Development of highly efficient nanocarrier-mediated delivery approaches for cancer therapy. Cancer Lett. 2016;374(1):31–43. doi:10.1016/j.canlet.2016.01.050
63. Barenholz Y. Doxil®--the first FDA-approved nano-drug: lessons learned. J Control Release. 2012;160(2):117–134. doi:10.1016/j.jconrel.2012.03.020
64. Zylberberg C, Matosevic S. Pharmaceutical liposomal drug delivery: a review of new delivery systems and a look at the regulatory landscape. Drug Deliv. 2016;23(9):3319–3329. doi:10.1080/10717544.2016.1177136
65. Federico C, Alhallak K, Sun J, et al. Tumor microenvironment-targeted nanoparticles loaded with bortezomib and ROCK inhibitor improve efficacy in multiple myeloma. Nat Commun. 2020;11(1):6037. doi:10.1038/s41467-020-19932-1
66. Deshantri AK, Fens MH, Ruiter RWJ, et al. Liposomal dexamethasone inhibits tumor growth in an advanced human-mouse hybrid model of multiple myeloma. J Control Release. 2019;296:232–240. doi:10.1016/j.jconrel.2019.01.028
67. Hanafy NAN, Kolemen S. Liposomal nanoparticles as a drug delivery system for improved treatment of multiple myeloma. RSC Adv. 2026;16(16):13995–14009. doi:10.1039/d5ra09823h
68. Rawal S, Patel MM. Threatening cancer with nanoparticle aided combination oncotherapy. J Control Release. 2019;301:76–109. doi:10.1016/j.jconrel.2019.03.015
69. George A, Shah PA, Shrivastav PS. Natural biodegradable polymers based nano-formulations for drug delivery: a review. Int J Pharm. 2019;561:244–264. doi:10.1016/j.ijpharm.2019.03.011
70. Gong J, Chen M, Zheng Y, Wang S, Wang Y. Polymeric micelles drug delivery system in oncology. J Control Release. 2012;159(3):312–323. doi:10.1016/j.jconrel.2011.12.012
71. Cirstea D, Hideshima T, Rodig S, et al. Dual inhibition of akt/mammalian target of rapamycin pathway by nanoparticle albumin-bound-rapamycin and perifosine induces antitumor activity in multiple myeloma. Mol Cancer Ther. 2010;9(4):963–975. doi:10.1158/1535-7163.Mct-09-0763
72. Taylor CA, Liu Z, Tang TC, et al. Modulation of eIF5A expression using SNS01 nanoparticles inhibits NF-κB activity and tumor growth in murine models of multiple myeloma. Mol Ther. 2012;20(7):1305–1314. doi:10.1038/mt.2012.94
73. Li Z, Li X, Cao Z, et al. Camptothecin nanocolloids based on N,N,N-trimethyl chitosan: efficient suppression of growth of multiple myeloma in a murine model. Oncol Rep. 2012;27(4):1035–1040. doi:10.3892/or.2012.1635
74. Ao L, Reichel D, Hu D, et al. Polymer micelle formulations of proteasome inhibitor carfilzomib for improved metabolic stability and anticancer efficacy in human multiple myeloma and lung cancer cell lines. J Pharmacol Exp Ther. 2015;355(2):168–173. doi:10.1124/jpet.115.226993
75. Sawant RR, Torchilin VP. Multifunctionality of lipid-core micelles for drug delivery and tumour targeting. Mol Member Biol. 2010;27(7):232–246. doi:10.3109/09687688.2010.516276
76. Zhang C, Wang X, Cheng R, Zhong Z. A6 peptide-tagged core-disulfide-cross-linked micelles for targeted delivery of proteasome inhibitor carfilzomib to multiple myeloma in vivo. Biomacromolecules. 2020;21(6):2049–2059. doi:10.1021/acs.biomac.9b01790
77. Koizumi F, Kitagawa M, Negishi T, et al. Novel SN-38-incorporating polymeric micelles, NK012, eradicate vascular endothelial growth factor-secreting bulky tumors. Cancer Res. 2006;66(20):10048–10056. doi:10.1158/0008-5472.Can-06-1605
78. Miyazaki O, Sekine K, Nakajima N, et al. Antimyeloma activity of NK012, a micelle-forming macromolecular prodrug of SN-38, in an orthotopic model. Int J Cancer. 2014;134(1):218–223. doi:10.1002/ijc.28333
79. Xu C, Song R, Lu P, et al. A pH-responsive charge-reversal drug delivery system with tumor-specific drug release and ROS generation for cancer therapy. Int J Nanomed. 2020;15:65–80. doi:10.2147/ijn.S230237
80. Zhang W, Qiao L, Wang X, Senthilkumar R, Wang F, Chen B. Inducing cell cycle arrest and apoptosis by dimercaptosuccinic acid modified Fe3O4 magnetic nanoparticles combined with nontoxic concentration of bortezomib and gambogic acid in RPMI-8226 cells. Int J Nanomed. 2015;10:3275–3289. doi:10.2147/ijn.S80795
81. Howat S, Park B, Oh IS, Jin YW, Lee EK, Loake GJ. Paclitaxel: biosynthesis, production and future prospects. N Biotechnol. 2014;31(3):242–245. doi:10.1016/j.nbt.2014.02.010
82. Patra HK, Dasgupta AK, Sarkar S, Biswas I, Chattopadhyay A. Dual role of nanoparticles as drug carrier and drug. Cancer Nanotechnol. 2011;2(1–6):37–47. doi:10.1007/s12645-010-0011-3
83. Abou DS, Thorek DL, Ramos NN, et al. (89)Zr-labeled paramagnetic octreotide-liposomes for PET-MR imaging of cancer. Pharm Res. 2013;30(3):878–888. doi:10.1007/s11095-012-0929-8
84. Tang R, Zheleznyak A, Mixdorf M, et al. Osteotropic radiolabeled nanophotosensitizer for imaging and treating multiple myeloma. ACS Nano. 2020;14(4):4255–4264. doi:10.1021/acsnano.9b09618
85. Morelli C, Maris P, Sisci D, et al. PEG-templated mesoporous silica nanoparticles exclusively target cancer cells. Nanoscale. 2011;3(8):3198–3207. doi:10.1039/c1nr10253b
86. Nigro A, Frattaruolo L, Fava M, et al. Bortezomib-loaded mesoporous silica nanoparticles selectively alter metabolism and induce death in multiple myeloma cells. Cancers. 2020;12(9):2709. doi:10.3390/cancers12092709
87. Li Z, Guo D, Yin X, et al. Zinc oxide nanoparticles induce human multiple myeloma cell death via reactive oxygen species and Cyt-C/Apaf-1/Caspase-9/Caspase-3 signaling pathway in vitro. Biomed Pharmacother. 2020;122:109712. doi:10.1016/j.biopha.2019.109712
88. Röllig C, Illmer T. The efficacy of arsenic trioxide for the treatment of relapsed and refractory multiple myeloma: a systematic review. Cancer Treat Rev. 2009;35(5):425–430. doi:10.1016/j.ctrv.2009.04.007
89. Hideshima T, Mitsiades C, Tonon G, Richardson PG, Anderson KC. Understanding multiple myeloma pathogenesis in the bone marrow to identify new therapeutic targets. Nat Rev Cancer. 2007;7(8):585–598. doi:10.1038/nrc2189
90. Zhu D, Wang Z, Zhao JJ, et al. The Cyclophilin A-CD147 complex promotes the proliferation and homing of multiple myeloma cells. Nat Med. 2015;21(6):572–580. doi:10.1038/nm.3867
91. Gao G, Che J, Xu P, Chen B, Zhao Y. Biomimetic cell membrane decorated ZIF-8 nanocarriers with IR-780 and doxorubicin loading for multiple myeloma treatment. Aggregate. 2024;5(6):e631. doi:10.1002/agt2.631
92. Zeng Y, He C, He Z, Chen H, Cheng F, Zheng Y. BCMA-engineered dendritic cell-derived exosomes as Bi-functional therapeutics orchestrating cytokine sequestration and immune activation for multiple myeloma. Adv Sci. 2026:e75686. doi:10.1002/advs.75686
93. Orlowski RZ, Nagler A, Sonneveld P, et al. Randomized phase III study of pegylated liposomal doxorubicin plus bortezomib compared with bortezomib alone in relapsed or refractory multiple myeloma: combination therapy improves time to progression. J Clin Oncol. 2007;25(25):3892–3901. doi:10.1200/jco.2006.10.5460
94. Orlowski RZ, Nagler A, Sonneveld P, et al. Final overall survival results of a randomized trial comparing bortezomib plus pegylated liposomal doxorubicin with bortezomib alone in patients with relapsed or refractory multiple myeloma. Cancer. 2016;122(13):2050–2056. doi:10.1002/cncr.30026
95. Dutta D, Liu J, Wen K, et al. A BCMA-mRNA vaccine is a promising therapeutic for multiple myeloma. Blood. 2025;146(19):2322–2335. doi:10.1182/blood.2025028597
96. Zhang Y, Deng Y, Zhai Y, et al. A bispecific nanosystem activates endogenous natural killer cells in the bone marrow for haematologic malignancies therapy. Nat Nanotechnol. 2024;19(10):1558–1568. doi:10.1038/s41565-024-01736-9
97. Van der Vreken A, Thery F, Tu C, et al. Immunopeptidomics identified antigens for mRNA-lipid nanoparticle vaccines with alpha-galactosylceramide in multiple myeloma therapy. J Immunother Cancer. 2025;13(4). doi:10.1136/jitc-2024-010673
98. Zhang XG, Wang L, Yang J, et al. Efficacy and safety of BCMA nanobody CAR T-cell therapy in relapsed or refractory plasma cell myeloma. Blood Adv. 2025;9(18):4543–4552. doi:10.1182/bloodadvances.2025016322
99. Berenson JR, Hilger JD, Yellin O, et al. Replacement of bortezomib with carfilzomib for multiple myeloma patients progressing from bortezomib combination therapy. Leukemia. 2014;28(7):1529–1536. doi:10.1038/leu.2014.27
100. Cortes JE, Lin TL, Uy GL, Ryan RJ, Faderl S, Lancet JE. Quality-adjusted Time Without Symptoms of disease or Toxicity (Q-TWiST) analysis of CPX-351 versus 7 + 3 in older adults with newly diagnosed high-risk/secondary AML. J Hematol Oncol. 2021;14(1):110. doi:10.1186/s13045-021-01119-w
101. Garfall AL, Nooka AK, Donk NW, et al. Long-term follow-up from the Phase 1/2 MajesTEC-1 trial of teclistamab in patients with relapsed/refractory multiple myeloma. J Clin Oncol. 2024;42(16_suppl):7540. doi:10.1200/JCO.2024.42.16_suppl.7540
102. Fadeel B, Farcal L, Hardy B, et al. Advanced tools for the safety assessment of nanomaterials. Nat Nanotechnol. 2018;13(7):537–543. doi:10.1038/s41565-018-0185-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Camptothecin-Loaded and Manganese Dioxide-Coated Polydopamine Nanomedicine Used for Magnetic Resonance Imaging Diagnosis and Chemo-Photothermal Therapy for Lung Cancer

Su M, Chen Y, Jia L, Zhang Z
International Journal of Nanomedicine 2022, 17:6687-6705
Published Date: 28 December 2022
Folate-Functionalized CS/rGO/NiO Nanocomposites as a Multifunctional Drug Carrier with Anti-Microbial, Target-Specific, and Stimuli-Responsive Capacities
Obireddy SR, Ayyakannu A, Kasi G, Sridharan B, Lai WF, Viswanathan K
International Journal of Nanomedicine 2025, 20:1965-1981
Published Date: 14 February 2025
Development of Cytolytic Iridium-Complexed Octaarginine Peptide Albumin Nanomedicine for Hepatocellular Carcinoma Treatment
Sun X, Wang D, Chang S, Yin L, Zhang H, Ji S, Fei H, Jin Y
International Journal of Nanomedicine 2025, 20:2395-2409
Published Date: 25 February 2025
Triphenylphosphine-Based Mitochondrial Targeting Nanocarriers: Advancing Cancer Therapy

Ali MS, Gowda BHJ, Shukla R, Kesharwani P
Clinical Pharmacology: Advances and Applications 2025, 17:119-141
Published Date: 10 June 2025
Emerging Role of Plant-Derived Nanostructures in Nanomedicine
Xing H, Li G, Qi C, Zhang M, Ding N, Zhang X
International Journal of Nanomedicine 2025, 20:12715-12731
Published Date: 21 October 2025