Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Nail Amino Acid and Trace Element Profiles and Their Association with Clinical Severity in Nail Psoriasis
Authors Özen T ![]() , Gürel MS, Erdem O
, Gürel MS, Erdem O ![]() , Özçelik D, Pastacı Özsobacı N, Selek Ş, Köktaşoğlu F
, Özçelik D, Pastacı Özsobacı N, Selek Ş, Köktaşoğlu F
Received 7 November 2025
Accepted for publication 23 January 2026
Published 12 February 2026 Volume 2026:19 578960
DOI https://doi.org/10.2147/CCID.S578960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Tunç Özen,1 Mehmet Salih Gürel,1 Ozan Erdem,1 Derviş Özçelik2 ,† Nural Pastacı Özsobacı,2 Şahabettin Selek,3 Fatmanur Köktaşoğlu3
1Department of Dermatology, Istanbul Medeniyet University, İstanbul, Türkiye; 2Department of Biophysics, Cerrahpaşa Faculty of Medicine, İstanbul, Türkiye; 3Department of Biochemistry, Bezmialem Vakıf University, İstanbul, Türkiye
†Derviş Özçelik passed away on October 15, 2025
Correspondence: Tunç Özen, Department of Dermatology, Istanbul Medeniyet University, İstanbul, Türkiye, Tel +905389515911, Email [email protected]
Background: Nail involvement is common in psoriasis, yet objective and non-invasive biomarkers of nail disease activity are limited. The biochemical composition of the nail plate may reflect local pathophysiological changes and could provide measurable indicators of disease severity.
Objective: To compare the nail biochemical composition between psoriatic patients with and without nail involvement, and to examine its associations with nail severity.
Methods: In this case-control study, nail clippings from adults with psoriasis were analyzed for trace elements (Cr, Cu, Fe, Mn, Mg, Se, Zn) by ICP-OES and for amino acids by LC-MS/MS. Group comparisons and correlation analyses with the Nail Psoriasis Severity Index (NAPSI) were conducted, and multivariable logistic regression identified independent predictors of nail involvement.
Results: Fifty-seven patients were included (30 with nail involvement; 27 without). Compared with patients without nail involvement, those with nail psoriasis showed significantly lower nail levels of several trace elements and amino acids, whereas histidine was higher (all p < 0.05). NAPSI correlated negatively with selenium, zinc, glycine, and proline, and positively with histidine. In multivariable analysis, lower nail selenium and asparagine and higher histidine independently predicted nail involvement.
Conclusion: Psoriatic nail dystrophy is associated with a distinct biochemical profile in the nail plate. Selected trace elements and amino acids correlate with clinical severity and may represent potential biochemical indicators of nail disease activity. Prospective studies are warranted to validate these findings.
Plain Language Summary: Psoriasis can affect the nails and impair appearance and daily functioning. To monitor nail changes, practical and non-invasive biomarkers are needed. In this study, we compared two groups of people with psoriasis: those with nail problems and those without. Small nail clippings were collected from each participant. We measured very small amounts of certain minerals (trace elements, such as zinc and selenium) and building blocks of proteins (amino acids) in these samples.We found that some minerals and amino acids were lower in patients with nail problems, while histidine was higher. These values also tracked with how severe the nail findings were. This suggests that analyzing nail clippings could provide a laboratory-based, non-invasive way to follow nail disease in psoriasis. Larger studies are needed to confirm these results before they can be used routinely in clinics.
Keywords: psoriasis, nail involvement, trace elements, amino acids, NAPSI, LC-MS/MS, ICP-OES
Introduction
Psoriasis is a chronic, immune-mediated inflammatory disease that affects approximately 2–3% of the global population.1 It frequently extends to skin appendages, particularly the nails, leading to significant functional impairment and psychosocial distress. Nail involvement is observed in 50–79% of patients with cutaneous psoriasis and up to 80% of those with psoriatic arthritis.2 Common nail changes including pitting, subungual hyperkeratosis, onycholysis, and discoloration not only reflect disease severity but may also serve as early indicators of psoriatic arthritis.3,4
The Nail Psoriasis Severity Index (NAPSI) is widely used in research to quantify nail involvement.5 Yet, it does not directly reflect the underlying biological changes in the nail. Non-invasive biochemical markers may serve as a useful complement by indicating disease activity at a molecular level and helping relate these changes to clinical severity.6,7
The nail unit is a biologically active structure composed of keratinized tissues, requiring a coordinated supply of amino acids and trace elements for proper growth and differentiation. These biochemical components serve as structural and enzymatic cofactors essential for keratin production and nail integrity.8,9 Despite this, there is a significant lack of studies investigating the biochemical composition of nails in patients with psoriasis, particularly regarding essential amino acids and trace elements.
The rationale of this study originated from the attempt to understand the biochemical background underlying the altered nail morphology observed in psoriasis. Just as the distinction between a diamond and a rock lies not only in their appearance but in their chemical composition, the difference between dystrophic and non-dystrophic nails in psoriasis may also stem from biochemical, rather than purely structural, alterations. This concept is supported by prior literature on nail biology8 and biochemical alterations in inflammatory skin diseases.10 Therefore, instead of including healthy individuals as controls, we selected psoriasis patients without nail involvement. A similar disease-internal comparison strategy has been applied in previous studies, in which psoriasis patients were evaluated according to the presence or absence of nail involvement rather than compared with healthy controls.11 This design allowed us to identify nail-specific biochemical differences associated with morphological changes, independent of the systemic effects of psoriasis itself. A comparison with healthy subjects could have highlighted psoriasis-related but nail-nonspecific alterations, potentially masking these subtle distinctions. The study does not aim to define a mechanistic pathway, but rather to characterize how the biochemistry of the affected nail differs from that of the unaffected nail within the same disease spectrum.
The nail plate is primarily composed of hard keratin, whose structural integrity depends on keratin-associated proteins, disulfide bonding, and a balanced composition of specific amino acids and trace elements.2,12 Alterations in these biochemical components may influence nail rigidity, cohesion, and growth.8 Based on their known structural or metabolic relevance to nail biology, selected trace elements and amino acids have been investigated to better understand their potential association with nail pathology in psoriasis. This approach may help determine whether biochemical changes within the nail plate are associated with nail involvement and clinical severity.
Therefore, this study aimed to evaluate the levels of selected trace elements and amino acids in nail samples of patients with psoriasis, comparing those with and without nail involvement. Furthermore, we explored the correlation between the severity of nail involvement and biochemical alterations to identify potential biomarkers that may reflect disease activity and assist in clinical monitoring.
Materials and Methods
Study Design and Participants
This study was designed as an exploratory, hypothesis-generating investigation aimed at characterizing nail-specific biochemical profiles in psoriasis.
This case-control study was conducted at the Department of Dermatology, Istanbul Medeniyet University Prof. Dr. Suleyman Yalçın City Hospital between October and December 2023. The study included adult patients clinically diagnosed with psoriasis who were not receiving any systemic treatment.
Participants were categorized into two groups based on the presence of clinical nail involvement. The Nail psoriasis group consisted of 30 patients diagnosed with psoriasis who exhibited clinically evident nail changes. In contrast, the control group included 27 psoriasis patients who showed no signs of nail involvement upon clinical examination. Nail samples were not obtained from unaffected nails of patients with nail psoriasis.
Inclusion criteria were: psoriasis duration ≥1 year, age ≥18 years, and nail involvement duration ≥6 months. Exclusion criteria included use of systemic medications, vitamin supplementation, comorbid chronic diseases (eg, diabetes, cardiovascular disease, cancer), positive KOH findings, or exposure to nail cosmetics or chemicals within one week prior to sample collection. Topical treatments for nail psoriasis were not included as an exclusion criterion, as such therapies are widely accessible and frequently used intermittently in routine clinical practice. Given that the study was conducted in a tertiary referral center, excluding patients with prior topical treatment would have substantially limited the representativeness of the study population.
All participants provided informed consent. Demographic data including age, sex, smoking and alcohol use, presence of joint pain, disease duration, and Nail Psoriasis Severity Index (NAPSI) scores were recorded.
Ethical approval was obtained from the institutional review board (approval number: 2023/0633), and written informed consent was acquired from all participants. The study was funded by the Turkish Dermatology Association.
Sample Collection
Sterile nail clippings were collected from all participants. Care was taken to avoid contamination with external material. The samples were stored at +4°C in sterile containers. Nail clippings were obtained from a single fingernail of each participant. In the nail psoriasis group, the sampled nail was selected based on clinical involvement, with priority given to the thumbnail if affected. If the thumbnail was unaffected, another clinically involved fingernail was chosen. In the control group, nail clippings were collected from the thumbnail. Toenails were not included in the study. Each nail clipping was carefully divided into two equal portions to allow for separate analyses of trace elements and amino acids.
Biochemical Analysis
Nail samples were subjected to trace element and amino acid profiling.
Trace Elements Analysis
Nail concentrations of chromium (Cr), copper (Cu), zinc (Zn), iron (Fe), manganese (Mn), magnesium (Mg), and selenium (Se) were measured using Inductively Coupled Plasma Optical Emission Spectroscopy (ICP-OES). Nail samples were digested with concentrated nitric acid followed by perchloric acid under controlled heating. After cooling and dilution with ultrapure water, the samples were filtered and analyzed in duplicate. Element-specific calibration curves and reagent blanks were used to ensure accuracy. Final values were expressed as micrograms per gram (µg/g) of dry tissue.
Amino Acids Analysis
Twenty amino acids (Phenylalanine, Leucine, Serine, Tyrosine, Cysteine, Tryptophan, Proline, Histidine, Glutamine, Arginine, Isoleucine, Methionine, Threonine, Asparagine, Lysine, Valine, Alanine, Aspartic acid, Glutamic acid, and Glycine) were quantified using Liquid Chromatography–Tandem Mass Spectrometry (LC-MS/MS). Nail samples were rinsed with deionized water and cleaned with a mixture of chloroform, methanol, and acetone. After drying, the nail samples were transferred into glass tubes with screw caps. Subsequently, 200 µL of 6M hydrochloric acid (HCl) and 200 µL of a reagent containing amino acid standards (R1) were added to each sample at a 1:1 ratio. The samples were hydrolyzed by incubation at 110°C for 24 hours to release amino acids through protein degradation.
After cooling to room temperature, the hydrolyzed samples were filtered through a 0.22 µm PVDF membrane filter and transferred into microcentrifuge tubes. The filtered samples were then placed in a vacuum concentrator at 45°C for approximately 4 hours until complete evaporation of the liquid phase. The resulting dry residues were reconstituted in 400 µL of a solution containing 20% methanol and 0.1% formic acid, followed by filtration through a 0.22 µm PVDF membrane filter before analysis. Results were normalized to dry tissue mass and reported in nanomoles per milligram (nmol/mg). All samples were analyzed in duplicate.
Statistical Analysis
Data was analyzed using SPSS software version 25.0. Normality of distribution was assessed with the Shapiro–Wilk test. Student’s t-test or Mann–Whitney U-test was used to compare continuous variables between groups. Spearman correlation analysis was used to assess relationships between NAPSI scores and biochemical parameters. A p-value of <0.05 was considered statistically significant.
In addition, post-hoc power analyses were conducted based on the observed effect sizes for the two-group comparisons (two-tailed, α=0.05). Medium-to-large effect sizes were observed for iron, chromium, manganese, selenium, zinc, as well as proline, histidine, glycine, asparagine, and threonine, with achieved power ranging between 70–95% in the current sample. In contrast, variables with small effect sizes yielded limited statistical power, and ≥80–100 participants per group would be required to reach 80% power. For correlations with NAPSI scores (r=0.32–0.44), the achieved power was 40–60%, indicating that a total sample size of approximately 50–85 patients would be necessary to achieve 80% power.
The exploratory nature and limited sample size of this pilot study should be acknowledged. Due to the lack of previous data on nail-based biochemical alterations in psoriasis, an a priori power calculation was not feasible. As a result, certain analyses did not reach 80% statistical power, indicating that larger multicenter studies will be required to confirm our preliminary findings and establish more definitive effect estimates.
Results
Demographic Characteristics
A total of 57 patients were included in the study. Of these, 30 patients had clinical nail involvement (nail psoriasis group) and 27 had no nail involvement (control group). There were no statistically significant differences between the two groups in terms of age, sex, smoking, alcohol use. However, disease duration was significantly longer in patients with nail involvement compared to those without (13.3 ± 10.9 vs 8.7 ± 8.6 years, p = 0.048) (Table 1). In the Nail Psoriasis Group, the mean NAPSI score was 44.1 ± 20.6 (median: 49, range: 12–80), indicating a wide spectrum of nail involvement severity among patients. Inclusion of this metric provides further insight into the clinical heterogeneity of the group and enables biochemical correlations to be interpreted in light of clinical severity.
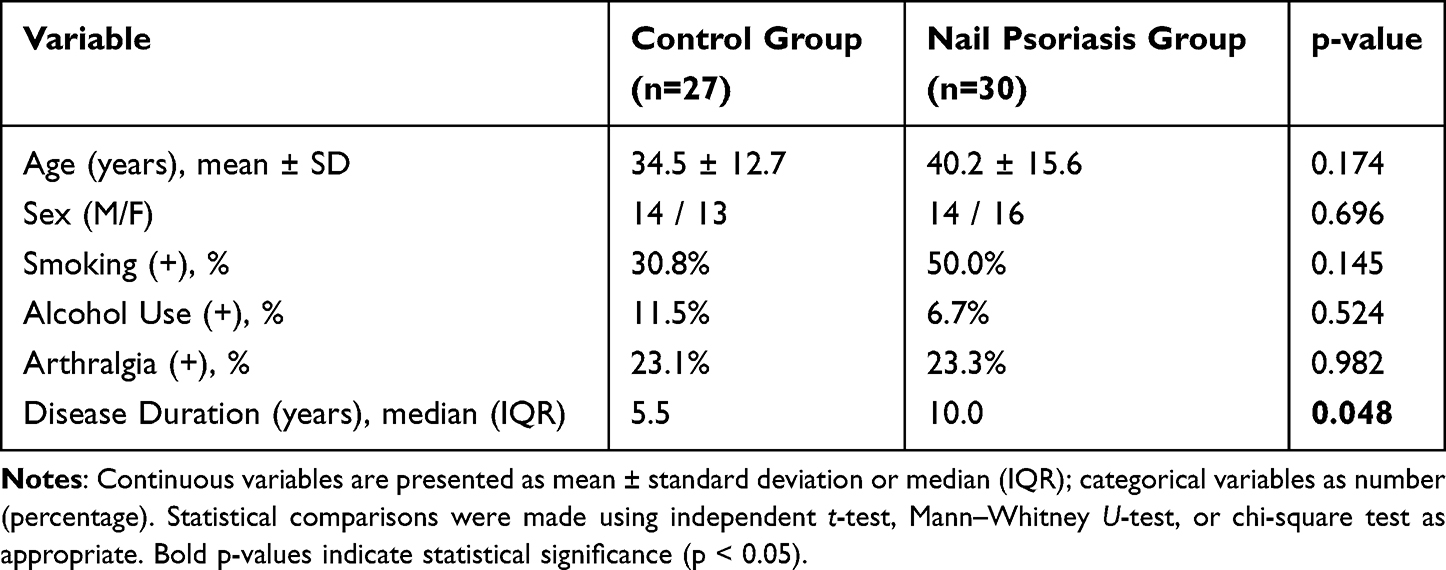 |
Table 1 Demographic and Clinical Characteristics of Study Groups |
Trace Element Levels in Nail Samples
The mean levels of several trace elements in nail samples differed significantly between the two groups (Table 2):
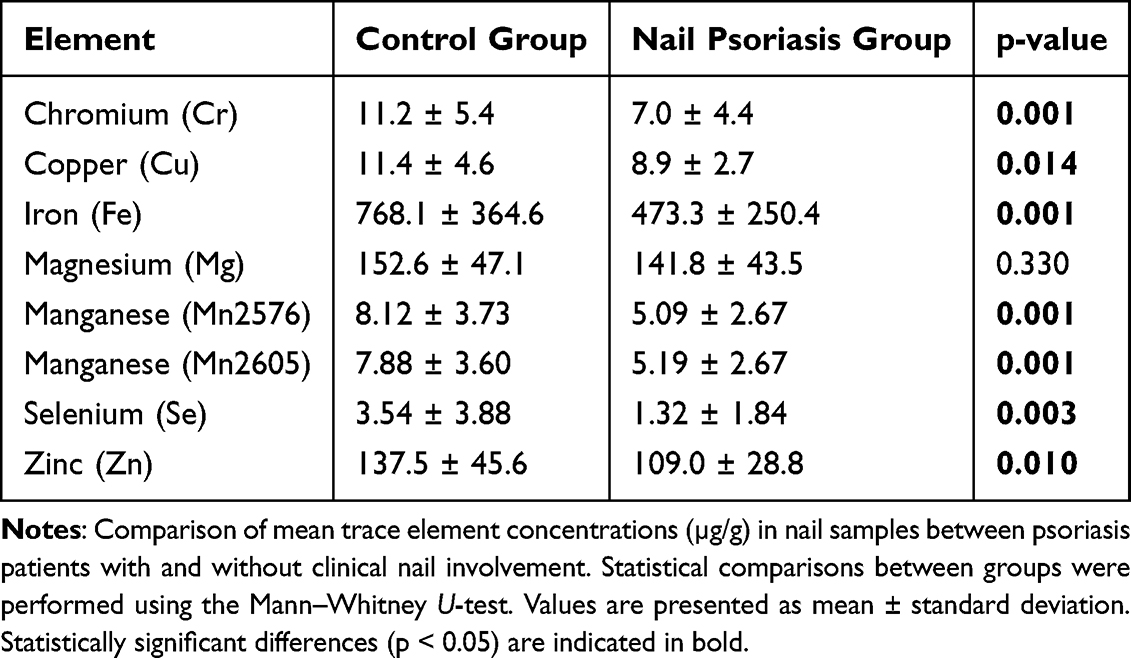 |
Table 2 Nail Trace Element Levels in Psoriasis Patients (Mean ± SD) |
Chromium (Cr): Significantly lower in the nail psoriasis group (p = 0.001)
Copper (Cu): Significantly lower in the nail psoriasis group (p < 0.014)
Iron (Fe): Significantly lower in the nail psoriasis group (p = 0.001)
Manganese (Mn): Both Mn2576 and Mn2605 isotopes were significantly lower (p = 0.001 each)
Selenium (Se): Decreased in the nail psoriasis group (p = 0.003)
Zinc (Zn): Significantly reduced (p = 0.010)
No significant difference was observed for Magnesium (Mg) (p = 0.330).
Amino Acid Levels in Nail Samples
Among the 20 amino acids analyzed, several showed significant differences (Table 3):
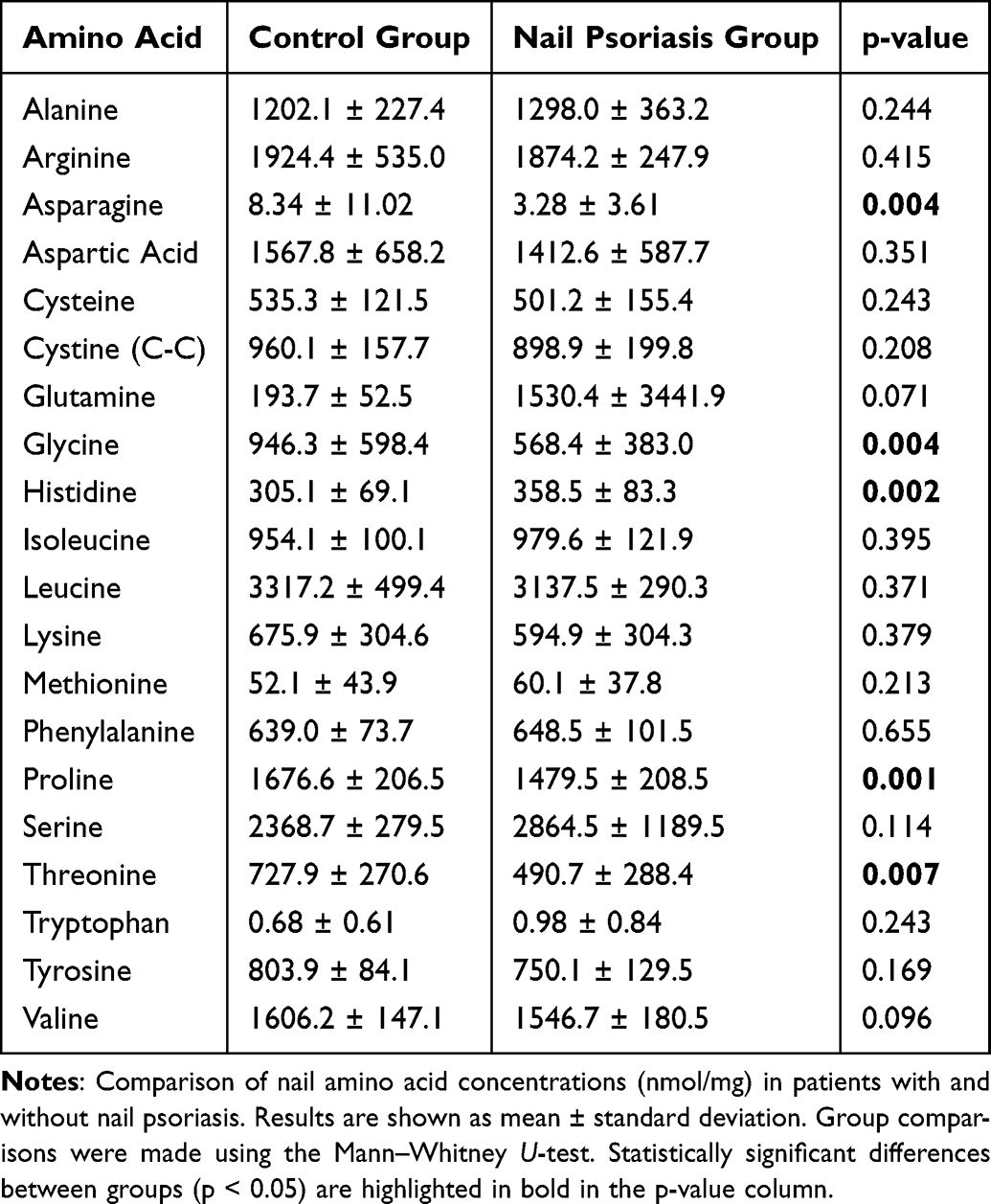 |
Table 3 Nail Amino Acid Levels in Psoriasis Patients (Mean ± SD) |
Asparagine (p = 0.004), Glycine (p = 0.004), Proline (p = 0.001), and Threonine (p = 0.007) levels were significantly lower in the nail psoriasis group.
Histidine was found to be significantly higher in patients with nail involvement (p = 0.002)
Correlation with Nail Psoriasis Severity (NAPSI)
Correlation analysis revealed that decreased levels of specific trace elements and amino acids (eg, Zinc, Selenium, Glycine, Proline) were negatively correlated with NAPSI scores, indicating that more severe nail involvement was associated with lower levels of these biochemical markers. A positive correlation was observed between histidine levels and NAPSI scores (r = 0.42, p = 0.002) (Table 4).
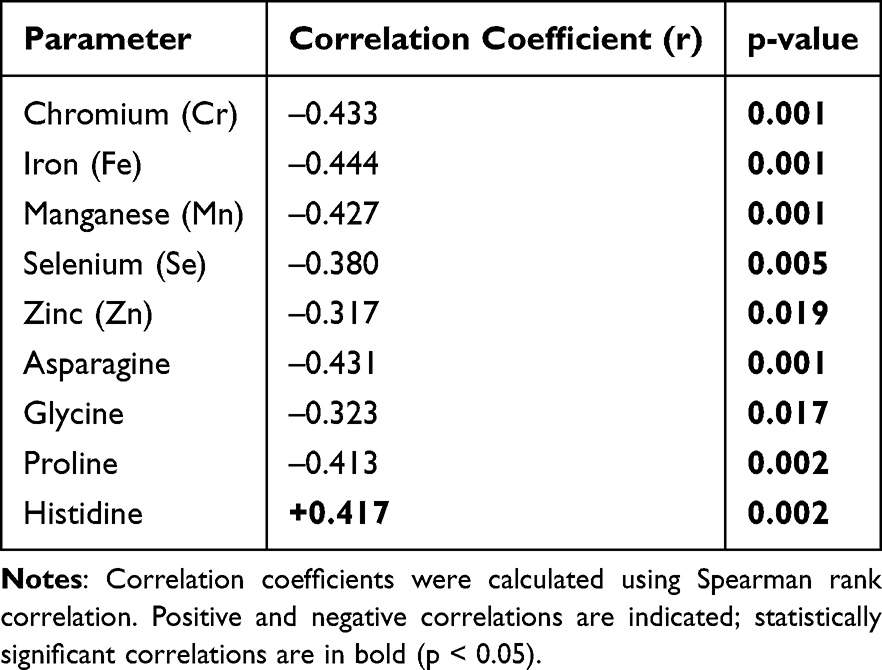 |
Table 4 Correlation of Nail Trace Elements and Amino Acids with NAPSI Score |
Multivariate Logistic Regression
Multivariate logistic regression identified nail selenium (OR = 0.585, p = 0.011), nail histidine (OR = 1.033, p = 0.019), and nail asparagine (OR = 0.959, p = 0.016) as independent predictors of nail involvement.
Subgroup Analysis by Disease Duration
Patients with longer disease duration (≥10 years) showed greater reductions in nail trace element and amino acid levels compared to those with a disease duration <10 years, particularly for Selenium and Proline.
Discussion
This study investigated the biochemical composition of nails in patients with psoriasis, focusing specifically on trace element and amino acid profiles. We demonstrated that patients with nail psoriasis had significantly lower levels of chromium, copper, manganese, selenium, and zinc compared to psoriasis patients without nail involvement. Similarly, several amino acids particularly asparagine, glycine, proline, and threonine were also reduced. Notably, histidine levels were increased in the nail psoriasis group. Our findings demonstrate an association between nail involvement in psoriasis and altered biochemical profiles within the nail unit. However, the directionality and underlying mechanisms of this association remain to be clarified.
In our study, disease duration was significantly longer in patients with nail involvement compared to those without (13.3 ± 10.9 years vs 8.7 ± 8.6 years, p = 0.048). This finding suggests that nail changes may develop progressively in the context of chronic inflammation. The observed association between prolonged disease duration and biochemical alterations in the nail matrix may reflect cumulative effects of chronic inflammation. However, whether these metabolic changes contribute to or merely result from nail pathology remains uncertain. Alternatively, nail involvement might reflect a more persistent, treatment-resistant, or extensive form of psoriasis.
Trace elements are essential cofactors in numerous enzymatic and cellular processes, including keratinocyte differentiation, oxidative stress regulation, and epithelial barrier maintenance. The reduction in selenium and zinc observed in our study aligns with previous findings suggesting their role in antioxidant defense and keratin metabolism.13–15 Selenium, in particular, is incorporated into selenoproteins such as glutathione peroxidase, which may modulate inflammatory processes in psoriatic tissue.15,16 Selenium, asparagine, and histidine were identified as independent variables statistically associated with nail involvement in psoriasis. These findings suggest that biochemical markers in nail tissue may hold potential for further exploration as non-invasive indicators.
Zinc is also critical for matrix metalloproteinase activity and tissue remodeling. Zinc is essential for keratinocyte proliferation and DNA synthesis and has known anti-inflammatory effects.15,17,18 Reduced nail zinc levels in this study align with earlier findings of low serum zinc in psoriasis and suggest potential depletion at the site of keratin production.19–21 The discrepancy between serum and nail copper levels is noteworthy: while previous reports describe elevated serum copper in psoriasis,19 our study found significantly decreased nail copper. This may reflect differential compartmentalization or altered incorporation of copper into keratinized tissue under inflammatory stress.
The amino acids found to be decreased in the nail psoriasis group—glycine, proline, threonine, and asparagine—are integral to collagen synthesis and keratin structure.22 Their deficiency may impair the integrity and function of the nail matrix and nail bed, potentially contributing to dystrophic changes observed clinically.10,23,24 Glycine and proline are not major structural components of keratin; however, their role in collagen synthesis and extracellular matrix organization may still be relevant to nail unit biology. However, these observations should be interpreted as biologically plausible associations rather than direct explanations for the classical structural changes seen in psoriatic nail dystrophy.
Histidine plays a multifaceted role in cutaneous homeostasis and immunity. As a histamine precursor, it contributes to inflammation by promoting vasodilation, pruritus, and leukocyte recruitment. It also provides antioxidant defense by scavenging reactive oxygen species and supporting epidermal barrier integrity through its role in natural moisturizing factor and urocanic acid production.22 In our study, the elevation of histidine levels in psoriatic nails may represent a compensatory metabolic response aimed at counteracting oxidative stress and maintaining local barrier integrity in the inflamed nail unit.
Glutamine levels showed marked variability in the nail psoriasis group (1530.4 ± 3441.9 nmol/mg), with a standard deviation exceeding the mean. This may reflect outliers or high interindividual variability, potentially affecting statistical significance. Future studies should consider robust analyses or data verification to address this skewness.
A significant negative correlation between NAPSI scores and the levels of specific trace elements and amino acids suggests that as the severity of nail involvement increases, the metabolic disturbances become more pronounced. These observations raise the possibility that these biochemical markers may reflect nail disease burden in psoriasis.
In a serum-based LC–MS metabolomic study of psoriasis, significant reductions in glycine, proline, and asparagine levels were demonstrated, with these alterations correlating with inflammatory disease activity.25 Similarly, in a plasma metabolomic profiling study of psoriasis, markedly reduced levels of asparagine, threonine, and glycine were reported, while histidine levels were preserved or increased in certain patient subgroups.26 In a metabolomic comparison of lesional and non-lesional psoriatic skin, disruptions in amino acid metabolism were shown to be closely associated with keratinocyte hyperproliferation and tissue remodeling.27 Furthermore, targeted serum amino acid profiling in generalized pustular psoriasis identified a characteristic “amino acid starvation” signature, marked by reduced levels of glycine, proline, asparagine, and threonine.28 Finally, systematic evaluations of toenail clippings as biomarkers demonstrated that nail measurements of trace elements such as zinc, copper, manganese, and selenium reliably reflect long-term biological status.29
To our knowledge, this is one of the few studies to focus specifically on the biochemical composition of psoriatic nails. There is growing evidence supporting the use of nail tissue, particularly toenails, as a biomarker for evaluating biochemical alterations in both localized and systemic conditions. For instance, Kilinc et al reported significantly lower levels of zinc, magnesium, and manganese in the toenails of patients with onychomycosis compared to healthy controls, while no significant differences were observed in onychocryptosis, a non-inflammatory nail disorder.30 Similarly, Matthews et al demonstrated associations between toenail trace element levels and the risk of skin cancer, further supporting the relevance of nail tissue in biomarker studies.31 Moreover, large-scale reviews emphasize the value of nail trace element analysis for assessing long-term exposure and metabolic status.32 Collectively, these findings highlight the broader applicability of nail biochemical analyses; however, direct comparisons of nail biochemical profiles across different dermatological diseases remain limited and warrant further investigation.
Limitations of this study include its cross-sectional design and relatively small sample size. Additionally, while we excluded systemic treatment, other confounding variables such as diet, comorbidities, or supplement use may have influenced biochemical levels. Given the cross-sectional nature of this study, it is not possible to determine whether the observed biochemical alterations are a cause or consequence of nail involvement. Post-hoc power analyses further indicated that while medium-to-large effects were adequately powered, smaller effects and correlations remained underpowered, requiring larger cohorts for confirmation. The inclusion of patients with clinically evident nail psoriasis may limit the generalizability of the findings across the full spectrum of nail involvement, and this should be considered when interpreting the results. Future longitudinal studies with larger cohorts and functional assays are warranted to validate these findings and explore causality.
Furthermore, while nail biochemical analysis may provide additional insights into localized metabolic changes in psoriasis, its clinical utility remains uncertain. As this method relies on distal nail clippings, it may not accurately reflect current disease activity or allow early detection of treatment effects.
Conclusion
This study demonstrates that nail involvement in psoriasis is associated with significant alterations in the levels of specific trace elements and amino acids within the nail plate. Patients with nail psoriasis exhibited reduced levels of chromium, copper, manganese, selenium, zinc, as well as key amino acids such as asparagine, glycine, proline, and threonine. These biochemical changes were correlated with the severity of nail involvement, as assessed by NAPSI scores.
Our findings indicate that biochemical analysis of nail tissue may provide additional information about localized metabolic changes in psoriasis. In particular, selenium, asparagine, and histidine levels were significantly associated with nail involvement. These parameters may have potential as non-invasive biomarkers, but this requires confirmation in future prospective studies.
Further longitudinal and mechanistic studies are warranted to confirm these associations and to better understand the role of trace elements and amino acids in the pathophysiology of nail psoriasis.
Abbreviations
Cr, Chromium; Cu, Copper; Fe, Iron; HCl, Hydrochloric acid; ICP-OES, Inductively coupled plasma optical emission spectroscopy; IQR, Interquartile range; KOH, Potassium hydroxide; LC-MS/MS, Liquid chromatography–tandem mass spectrometry; Mg, Magnesium; Mn, Manganese; NAPSI, Nail Psoriasis Severity Index; n, Number of subjects; p, Probability value; PVDF, Polyvinylidene difluoride; r, Correlation coefficient; SD, Standard deviation; Se, Selenium; SPSS, Statistical Package for the Social Sciences; Zn, Zinc; µg/g, Micrograms per gram; nmol/mg, Nanomoles per milligram; α, Significance level.
Declaration of Generative AI and AI-Assisted Technologies in the Manuscript Preparation Process
During the preparation of this work the author(s) used ChatGPT (OpenAI, San Francisco, CA, USA) for language editing and improvement of English clarity. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of Istanbul Medeniyet University, Prof. Dr. Süleyman Yalçın City Hospital (Approval No. 2023/0633).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
This study was funded by the Turkish Dermatology Association.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Turkish Dermatology Association.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Jnwn B. Psoriasis. Lancet. 2021;397(10281):1301–10. doi:10.1016/S0140-6736(20)32549-6
2. Canal-García E, Bosch-Amate X, Belinchón I, Puig L. Nail psoriasis. Actas Dermosifiliogr. 2022;113(5):481–490. doi:10.1016/j.ad.2022.01.006
3. Fratton Z, Giovannini I, Zabotti A, Errichetti E. Skin and nail predictors of psoriatic arthritis development: a holistic overview integrating epidemiological and physiopathological data. J Clin Med. 2024;13(22):6880. doi:10.3390/jcm13226880
4. Nielsen ML, Petersen TC, Maul LV, et al. Predicting psoriatic arthritis in psoriasis patients - a Swiss registry study. J Psoriasis Psoriatic Arthritis. 2024;9(2):41–50. doi:10.1177/24755303231217492
5. Rich P, Scher RK. Nail psoriasis severity index: a useful tool for evaluation of nail psoriasis. J Am Acad Dermatol. 2003;49(2):206–212. doi:10.1067/S0190-9622(03)00910-1
6. Youn SW. Nail psoriasis: clinical features and severity assessment. Ann Dermatol. 2024;36(4):191–196. doi:10.5021/ad.24.026
7. Horikawa H, Tanese K, Nonaka N, et al. Reliable and easy-to-use calculating tool for the nail psoriasis severity index using deep learning. NPJ Syst Biol Appl. 2024;10:130. doi:10.1038/s41540-024-00458-x
8. Baswan S, Kasting GB, Li SK, et al. Understanding the formidable nail barrier: a review of the nail microstructure, composition and diseases. Mycoses. 2017;60(5):284–295. doi:10.1111/myc.12592
9. Coroaba A, Pinteala T, Chiriac A, Chiriac AE, Simionescu BC, Pinteala M. Degradation mechanism induced by psoriasis in human fingernails: a different approach. J Invest Dermatol. 2016;136(1):311–313. doi:10.1038/JID.2015.387
10. Ottas A, Fishman D, Okas TL, Kingo K, Soomets U. The metabolic analysis of psoriasis identifies the associated metabolites while providing computational models for the monitoring of the disease. Arch Dermatol Res. 2017;309(7):519–528. doi:10.1007/s00403-017-1760-1
11. Bedair NI, El-Komy MHM, Elhamy N, Hafez V. Nail involvement among psoriasis patients: a comparative retrospective cohort analysis of 2888 egyptian patients. Exp Dermatol. 2025;34(5):e70105. doi:10.1111/exd.70105
12. de Berker DA, André J, Baran R. Nail biology and nail science. Int J Cosmet Sci. 2007;29(4):241–275. doi:10.1111/j.1467-2494.2007.00372.x
13. Lv J, Ai P, Lei S, Zhou F, Chen S, Zhang Y. Selenium levels and skin diseases: systematic review and meta-analysis. J Trace Elem Med Biol. 2020;62:126548. doi:10.1016/j.jtemb.2020.126548
14. Kazi AG, Afridi HI, Arain MB, Kazi TG. Adverse impact of occupational exposure on laborers of cement industry having scalp psoriasis and pityriasis amiantacea with deficiency of zinc and selenium: impact of mineral supplement. Environ Sci Pollut Res. 2021;28(48):68330–68337. doi:10.1007/s11356-021-15307-1
15. Kirmit A, Kader S, Aksoy M, Bal C, Nural C, Aslan O. Trace elements and oxidative stress status in patients with psoriasis. Postepy Dermatol Alergol. 2020;37(3):333–339. doi:10.5114/ada.2020.94265
16. Gangadevi V, Thatikonda S, Pooladanda V, Devabattula G, Godugu C. Selenium nanoparticles produce a beneficial effect in psoriasis by reducing epidermal hyperproliferation and inflammation. J Nanobiotechnol. 2021;19(1):101. doi:10.1186/s12951-021-00842-3
17. Ogawa Y, Kinoshita M, Shimada S, Kawamura T. Zinc and skin disorders. Nutrients. 2018;10(2):199. doi:10.3390/nu10020199
18. Ogawa Y, Kawamura T, Shimada S. Zinc and skin biology. Arch Biochem Biophys. 2016;611:113–119. doi:10.1016/j.abb.2016.06.003
19. Lei L, Su J, Chen J, Chen W, Chen X, Peng C. Abnormal serum copper and zinc levels in patients with psoriasis: a meta-analysis. Ind J Dermatol. 2019;64(3):224–230. doi:10.4103/ijd.IJD_475_18
20. Ala S, Shokrzadeh M, Golpour M, Salehifar E, Alami M, Ahmadi A. Zinc and copper levels in Iranian patients with psoriasis: a case-control study. Biol Trace Elem Res. 2013;153(1–3):22–27. doi:10.1007/s12011-013-9643-6
21. Nigam PK. Serum zinc and copper levels and Cu:Zn ratio in psoriasis. Ind J Dermatol Venereol Leprol. 2005;71(3):205–206. doi:10.4103/0378-6323.16242
22. Wu G. Amino acids in nutrition and health: amino acids in systems function and health. Adv Exp Med Biol; 2020;2020:1. ISBN: 978-3-030-45328-2.
23. Kang H, Li X, Zhou Q, et al. Exploration of candidate biomarkers for human psoriasis based on GC-MS serum metabolomics. Br J Dermatol. 2017;176(3):713–722. doi:10.1111/bjd.15008
24. Rashaid AHB, Harrington P, Jackson GP. Profiling amino acids of jordanian scalp hair as a tool for diabetes mellitus diagnosis: a pilot study. Anal Chem. 2015;87(14):7078–7084. doi:10.1021/acs.analchem.5b00460
25. Kamleh MA, Snowden SG, Grapov D, et al. LC–MS metabolomic profiling of psoriasis patients reveals disease severity–associated metabolic signatures and treatment response biomarkers. J Proteome Res. 2015;14(12):5576–5585. doi:10.1021/acs.jproteome.5b00737
26. Chen C, Hou G, Xie Y, et al. Plasma metabolomics reveals dysregulated amino acid and carnitine metabolism in patients with psoriasis. Theranostics. 2021;11(9):4237–4250. doi:10.7150/thno.54535
27. Pohla L, Ottas A, Kaldvee B, et al. Metabolic signatures of lesional and non-lesional skin in psoriasis vulgaris. Sci Rep. 2020;10(1):15920. doi:10.1038/s41598-020-72867-4
28. Yu N, Li X, Song Z, et al. Amino acid starvation signatures characterize metabolic dysregulation in generalized pustular psoriasis. Front Immunol. 2021;12:666031. doi:10.3389/fimmu.2021.666031
29. Gutiérrez-González E, García-Esquinas E, Pérez-Gómez B, et al. Toenail clippings as biomarkers of trace metal exposure in clinical and epidemiological research: a systematic review. Environ Res. 2019;171:312–322. doi:10.1016/j.envres.2019.01.025
30. Kilinc E, Buturak B, Alkan FA. Level of trace elements in serum and toenail samples of patients with onychocryptosis (ingrown toenail) and onychomycosis. J Trace Elem Med Biol. 2020;61:126509. doi:10.1016/j.jtemb.2020.126509
31. Matthews NH, Koh M, Li W-Q, et al. A Prospective study of toenail trace element levels and risk of skin cancer. Cancer Epidemiol Biomarkers Prev. 2019;28(9):1534–1543. doi:10.1158/1055-9965.EPI-19-0214
32. He K. Trace elements in nails as biomarkers in clinical research. Eur J Clin Invest. 2011;41(1):98–102. doi:10.1111/j.1365-2362.2010.02373.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.