Back to Journals » Journal of Blood Medicine » Volume 17
Nafamostat Mesilate as an Anticoagulation Strategy for Heparin-Induced Thrombocytopenia: A Case Report
Authors Mei S ![]() , Xue C
, Xue C ![]() , Liu L, Cui L, Lv J, Ruan M, Mao Z
, Liu L, Cui L, Lv J, Ruan M, Mao Z ![]() , Lu C, Sun L, Dai B
, Lu C, Sun L, Dai B
Received 1 September 2025
Accepted for publication 17 January 2026
Published 23 January 2026 Volume 2026:17 564615
DOI https://doi.org/10.2147/JBM.S564615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chang Kim
Shuqin Mei,1,* Cheng Xue,1,* Lingling Liu,1 Linlin Cui,1 Jiayi Lv,1 Mengna Ruan,1 Zhiguo Mao,1 Chunlai Lu,2 Lijun Sun,3 Bing Dai1
1Kidney Institute of PLA, Department of Nephrology, Shanghai Changzheng Hospital, Naval Medical University, Shanghai, People’s Republic of China; 2Department of Nephrology, 905th Hospital of PLA Navy, Shanghai, 200000, People’s Republic of China; 3Department of Nephrology and Endocrinology, Shanghai 411 Hospital, Shanghai University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lijun Sun, Department of Nephrology and Endocrinology, Shanghai 411 Hospital, Shanghai University, Shanghai, People’s Republic of China, Email [email protected] Bing Dai, Kidney Institute of PLA, Department of Nephrology, Shanghai Changzheng Hospital, Naval Medical University, Shanghai, People’s Republic of China, Email [email protected]
Abstract: Heparin-induced thrombocytopenia (HIT) is a serious and potentially life-threatening reaction to heparin, affecting 0.1% to 5% of patients. Those with end-stage renal disease face an and even higher risk because of repeated exposure to heparin during dialysis. HIT Type II, an immune-mediated condition, results from antibodies against heparin/platelet factor 4 (PF4) complexes, leading to platelet activation and thromboembolism. We present a 78-year-old woman with end-stage kidney disease (ESRD) who developed HIT Type II after low-molecular-weight heparin (LMWH) and unfractionated heparin (UFH) exposure during hemodialysis. Despite a negative PF4/heparin ELISA, a 4T score of 7 confirmed the presence of clinical HIT. She experienced thrombocytopenia (30× 109/L) and severe thrombotic events. Heparin was discontinued, and anticoagulation transitioned to argatroban and later nafamostat mesilate (NM) due to argatroban shortage. Platelet counts normalized (223× 109/L), and NM was effective without clotting complications. This case highlights the challenges in HIT diagnosis, emphasizing the role of clinical evaluation over laboratory tests, and underscores the utility of NM as an alternative anticoagulant in resource-limited settings. Key questions remain regarding heparin rechallenge safety, causative agent identification in multi-heparin exposure, and rapid differentiation of HIT from anaphylactoid reactions. Further studies are needed to optimize HIT management in high-risk populations.
Keywords: heparin-induced thrombocytopenia, hemodialysis, anticoagulants, coagulation, anti-PF4/heparin complex antibodies
Introduction
Heparin-induced thrombocytopenia (HIT) is a potentially life-threatening, immune-mediated adverse reaction to heparin, characterized by a paradoxical increase in thrombotic risk despite falling platelet counts. It affects approximately 0.1% to 5% of patients exposed to heparin, with variability depending on clinical context, heparin type, and patient population. Among patients with end-stage kidney disease (ESKD) undergoing chronic hemodialysis, the risk is particularly heightened due to recurrent exposure to unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) for anticoagulation and catheter maintenance. The development of HIT in this population poses significant clinical challenges—not only in timely diagnosis and differential evaluation, but also in the safe selection of alternative anticoagulants in resource-limited settings. Moreover, the limited availability of functional assays, especially during public health emergencies, further complicates management.
Type I HIT is characterized by a transient and mild decrease in platelet count shortly after the initiation of heparin therapy. This non-immune-mediated process is not associated with any clinical manifestations, and platelet levels typically normalize after discontinuation of heparin. In contrast, Type II HIT is an immune-mediated condition caused by the development of antibodies against complexes of heparin and platelet factor 4 (PF4). These antibody/PF4/heparin complexes bind to platelets via the FcγRIIA receptor and cause platelet activation, leading to platelet activation and subsequent venous or arterial thromboembolism. Type II HIT typically manifests 5–10 days after heparin initiation, although it can occur immediately in patients with recent heparin exposure (within the past 100 days). Thrombocytopenia is usually moderately severe, with a greater than 30–50% decline from baseline in platelet count, less than 100×109/L and results in a prothrombotic state. The platelet counts generally recovered within 5 to 10 days after heparin was withdrawn.
Despite advances in the understanding of HIT, its diagnosis remains challenging—especially when laboratory confirmation is lacking or delayed. The absence of reliable functional assays in many clinical settings often necessitates reliance on clinical scoring systems such as the 4T’s score, which, while practical, may lead to both over- and under-diagnosis. Moreover, while direct thrombin inhibitors such as argatroban are recommended as alternatives to heparin, their high cost, limited availability, and risk of bleeding may restrict their use in some countries. In this context, nafamostat mesilate (NM)—a short-acting serine protease inhibitor widely used in East Asia—has emerged as a potential alternative, particularly in patients undergoing hemodialysis. However, evidence regarding its safety and efficacy in HIT management is sparse and largely anecdotal. Therefore, the purpose of this case report is to describe a clinically confirmed HIT in an ESKD patient with a negative PF4 ELISA result, who was successfully managed with NM in a resource-constrained environment.
Case Presentation
A 78-year-old Asian woman, with a medical history of stage 5 chronic kidney disease (CKD), type 2 diabetes mellitus, hypertension, and stent graft insertion following myocardial infarction was admitted due to heart failure, hyperkalemia, and edema. She also had a history of atrial fibrillation and had been taking rivaroxaban irregularly before admission on December 24, 2021. 4 days post-admission, hemodialysis was initiated via the right internal jugular vein, with LMWH selected as the anticoagulant. UFH was used for catheter locking. Her condition improved following dialysis, and an arteriovenous fistula (AVF) was created between the left radial artery and cephalic vein on January 6, 2022. On day 11 post-admission, the patient developed acute dyspnea, hypotension, and cardiac arrest, within 10 minutes of initiating hemodialysis. She was successfully resuscitated with manual cardiopulmonary resuscitation (CPR) and oxygen therapy. An electrocardiogram revealed controlled atrial fibrillation at a rate of 90 beats per minute. Duplex ultrasonography of the lower limbs was performed, which did not reveal any evidence of deep vein thrombosis (DVT) at that time. Subsequent echocardiography showed an ejection fraction of 53%, and a CT pulmonary angiogram ruled out major pulmonary embolism (PE). Laboratory evaluation revealed a 50% reduction in platelet count (from 158×109/L to 59×109/L) without evidence of thrombosis, which was excluded by the ultrasound results. And the D-Dimer was elevated from 1.4μg/mL to 2.43μg/mL. Prothrombin time (PT) was 11.9s and activated partial thromboplastin time (aPTT) was 33.4s. She received 2 units of platelet transfusion, but her platelet counts further dropped to 30×109/L. Blood samples were drawn for heparin-induced thrombocytopenia (HIT) testing, including ELISA for immunoglobulin IgG, IgA, and IgM antibodies against the PF4/heparin complex (GTI-PF4 ELISA, GTI, Wis., USA), which returned negative. However, based on a 4T score of 7 (Table 1), HIT was clinically diagnosed. On day 17 post-admission, anticoagulation was withheld during dialysis. However, due to the high risk of thromboembolic complications from cardiac arrhythmia and HIT, rivaroxaban was restarted at 10 mg twice daily. Concurrently, ultrasonography revealed multiple venous and arterial thrombotic events, acrocyanosis, distal ischemic limb necrosis, dialysis circuit clotting, and catheter thrombosis. The patient required two central venous catheter replacements due to vascular access thrombosis and venous thrombosis. Within 10 days of heparin discontinuation and the use of tissue plasminogen activator (tPA) for catheter locking, her platelet count increased to 67×109/L. On day 27 post-admission, argatroban was initiated for dialysis anticoagulation, while rivaroxaban (10 mg twice daily) was continued. Her platelet counts subsequently recovered to 223×109/L. On day 47 post-admission, argatroban was discontinued, and the dose of rivaroxaban was reduced to 10 mg daily due to mucosal bleeding, bright red blood per rectum, and an elevated INR. During the SARS-CoV-2 pandemic, the patient was transferred to another hospital on day 90 post-admission (Figure 1). Due to a shortage of argatroban, NM (dissolved in 5% glucose and injected at a dose of 25 mg per hour) was the anticoagulant during hemodialysis. Nearly one year after initiating hemodialysis, rivaroxaban was discontinued following ultrasonographic confirmation of no further venous thrombosis (Figure 2). During weekly outpatient follow-ups, her platelet count remained within the normal range, and her dialysis flow rate was maintained at 200–220 mL/min.
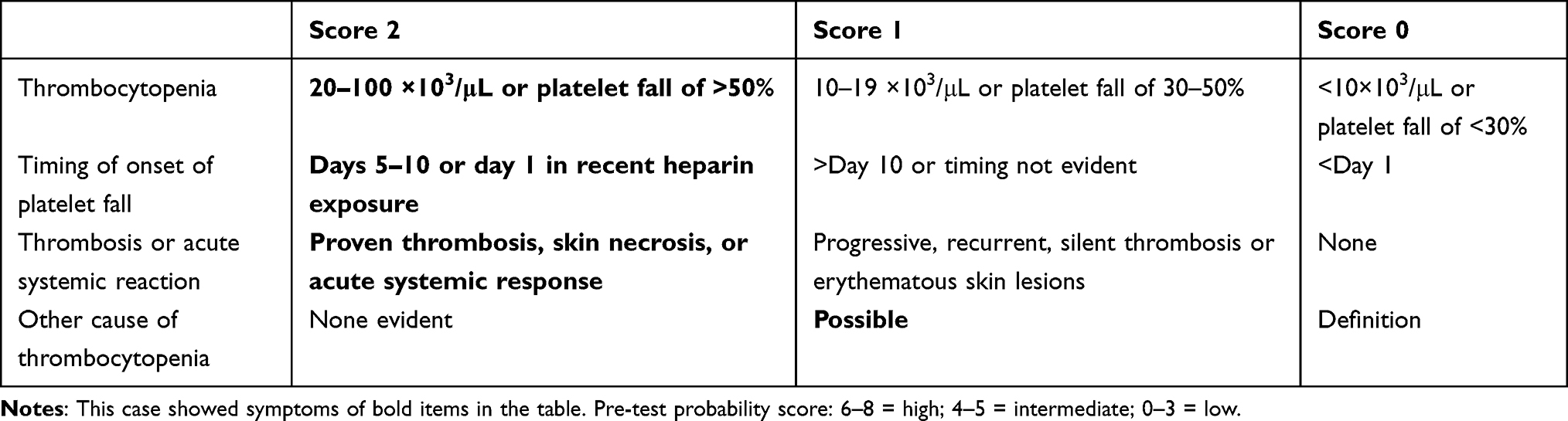 |
Table 1 Pre-Test Probability Score Criteria of HIT |
 |
Figure 1 Timeline in case presentation. Abbreviations: PLT, platelet; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; NM, nafamostat mesylate; tPA, tissue plasminogen activator. |
 |
Figure 2 Typical pictures of limb ischemia and venous limb gangrene. |
Discussion
HIT is triggered by the formation of anti-platelet factor 4 (PF4)/heparin complex antibodies following heparin exposure. In approximately 80% of cases, these antibodies belong to the immunoglobulin G (IgG) isotype, as IgG is the only class capable of binding to platelet FcγRIIA receptors. However, rare cases involving IgM and IgA antibodies with pathogenic potential have also been documented. UFH and LMWH are the most commonly used anticoagulants to maintain filter patency and extracorporeal circuit integrity during hemodialysis.1,2 Notably, studies indicate that the incidence of HIT is significantly lower in patients receiving LMWH compared to those receiving UFH. T The primary complications of HIT Type II are venous and arterial thrombotic events, including pulmonary embolism (PE), DVT, myocardial infarction, skin necrosis, limb ischemia, and venous limb gangrene. Additionally, atypical manifestations such as acute systemic reactions, acute respiratory distress syndrome (ARDS), transient global amnesia, and cardiopulmonary arrest have been reported.3 Thrombotic events often coincide with or immediately follow the onset of thrombocytopenia, underscoring the critical importance of timely diagnosis.4
In this case, the patient initially received LMWH as the primary anticoagulant during hemodialysis, while UFH was used solely for catheter locking due to institutional protocol. The use of both agents in parallel was not due to therapeutic switching but rather due to differing clinical purposes. LMWH was administered intravenously at the start of dialysis sessions, whereas UFH was employed in small doses to maintain catheter patency between sessions. The onset of thrombocytopenia and acute cardiopulmonary deterioration occurred after approximately 10 days of exposure to both agents. Based on the temporal correlation, we suspect LMWH as the more likely trigger, given the higher immunogenicity associated with initial exposure. However, because both agents were used simultaneously and no specific antibody testing (eg, PF4 subtype-specific assay) was performed, we could not definitively distinguish which heparin product was the primary sensitizer. There was no change in drug brand or supplier during the treatment course.
Although anti-PF4/heparin ELISA has high sensitivity (90–98%), its limited specificity means it cannot confirm HIT on its own. Functional assays like the serotonin release assay (SRA) or heparin-induced platelet aggregation (HIPA) offer greater diagnostic accuracy but are rarely available in routine clinical settings. In this case, due to the unavailability of functional testing, diagnosis was based on a 4T score of 7, consistent with American Society of Hematology (ASH) guidelines that prioritize clinical evaluation when laboratory results are inconclusive. Potential antibodies beyond PF4, such as anti-IL8, have been proposed in experimental studies, but relevant testing was not accessible during the COVID-19 pandemic.
In this case, alternative causes of thrombocytopenia and thrombosis were systematically excluded. There was no evidence of infection or sepsis-induced coagulopathy, with stable vital signs and normal inflammatory markers. Coagulation studies ruled out DIC, and peripheral smear findings did not support thrombotic microangiopathies such as TTP or HUS. Antiphospholipid syndrome was excluded by negative anticardiolipin and β2-glycoprotein I antibodies. No new medications were introduced during the relevant period, making drug-induced thrombocytopenia unlikely. Although no active bleeding was observed, platelet transfusion was administered as a precaution due to the critically low platelet count (<30×109/L), in accordance with institutional practice.
According to ASH guidelines, all forms of heparin—including heparin flushes or catheter locks—should be discontinued immediately upon HIT suspicion, due to their potential to worsen thrombocytopenia and trigger thrombosis. In the absence of functional assays, clinical judgment and prompt initiation of alternative anticoagulation are essential. Recommended agents include argatroban, bivalirudin, danaparoid, and hirudin. In our case, due to an argatroban shortage during the COVID-19 pandemic, the patient was transitioned to nafamostat mesilate (NM), a serine protease inhibitor with a very short half-life (5–8 minutes), offering a safer bleeding profile during dialysis. NM exerts its anticoagulant effect by inhibiting multiple serine proteases involved in coagulation, including thrombin, factor Xa, and kallikrein, which contribute to both anticoagulation and anti-inflammatory effects.
Although not FDA-approved, NM is widely used in Japan, Korea, and increasingly in China, particularly in patients with high bleeding risk or contraindications to systemic anticoagulation.5,6 In this case, NM was used successfully for long-term dialysis without extracorporeal circuit clotting. After discontinuing argatroban on Day 47 due to mucosal bleeding, the patient temporarily underwent heparin-free dialysis. However, following transfer to another hospital during the pandemic, NM was initiated on Day 90 as the only available anticoagulant. Additionally, rivaroxaban was prescribed for systemic anticoagulation due to HIT-associated thrombosis and atrial fibrillation. Despite requiring dose reduction for mucosal bleeding, the patient remained free of thrombotic recurrence during follow-up, suggesting the potential utility of DOACs in similar scenarios.
This case has several limitations that merit further exploration. First, the absence of data on allergic symptoms limited our ability to distinguish between anaphylactoid reactions and early systemic HIT. Second, the safety and timing of heparin rechallenge in dialysis-dependent patients remain unclear, with only limited case-based evidence and no established guidelines. Third, both LMWH and UFH were used concurrently, making it difficult to identify the primary sensitizing agent. Finally, due to pandemic-related constraints, comprehensive thrombophilia testing was not performed. These gaps highlight the need for further studies on diagnostic strategies and anticoagulation planning in HIT, particularly in resource-limited settings.
Conclusion
This case demonstrates that nafamostat mesilate may be a viable anticoagulation strategy for patients with suspected HIT during hemodialysis, particularly in settings where conventional agents are unavailable. It also highlights the importance of clinical evaluation when laboratory results are inconclusive. Further studies are needed to validate the safety and efficacy of NM in broader HIT populations.
Data Sharing Statement
All data collected from the patient were obtained from Changzheng Hospital and were available in this paper.
Ethics Statement
Written informed consent for publication of their details was obtained from the patient, including the images and further use for educational purposes. The publication of the case details was approved by the Ethics Committee of Shanghai Changzheng Hospital.
Acknowledgments
All authors thank the patient and her family for their support.
Funding
This paper was supported by the National Natural Science Foundation of China (grant NO.81800681, 81970640, and 82370735).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hvas AM, Favaloro EJ, Hellfritzsch M. Heparin-induced thrombocytopenia: pathophysiology, diagnosis and treatment. Expert Rev Hematol. 2021;14(4):335–6. doi:10.1080/17474086.2021.1905512
2. Hamadi R, Sakr F, Aridi H, et al. Heparin-induced thrombocytopenia in chronic hemodialysis patients. Clin Appl Thromb Hemost. 2023;29:10760296231177993. doi:10.1177/10760296231177993
3. Murakami Y, Tomoda A, Fujita S, et al. Heparin-induced thrombocytopenia with anaphylactoid reaction during hemodialysis. Intern Med. 2024;63(16):2321–2324. doi:10.2169/internalmedicine.2859-23
4. Warkentin TE. Immunologic effects of heparin associated with hemodialysis: focus on heparin-induced thrombocytopenia. Semin Nephrol. 2023;43(6):151479. doi:10.1016/j.semnephrol.2023.151479
5. Liu D, Zhao J, Xia H, et al. Nafamostat mesylate versus regional citrate anticoagulation for continuous renal replacement therapy in patients at high risk of bleeding: a retrospective single-center study. Eur J Med Res. 2024;29(1):72. doi:10.1186/s40001-024-01660-7
6. Kawamoto S, Kusudo E, Fukuda K. Use of argatroban in combination with nafamostat mesilate in open-heart surgery for a pediatric patient with heparin-induced thrombocytopenia type II: a case report. JA Clin Rep. 2020;6(1):3. doi:10.1186/s40981-020-0310-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.