Back to Journals » Clinical Ophthalmology » Volume 20
Myopic and Astigmatic Laser in situ Keratomileusis Using a Ray Tracing−Based Treatment Algorithm with a Personalized Ablation Profile
Authors Krueger RR, Thompson V, Solomon K, Wexler SA, Clinch TE, Whitman J, Moyes A, Price F, Gordon M
Received 4 November 2025
Accepted for publication 11 February 2026
Published 17 March 2026 Volume 2026:20 567933
DOI https://doi.org/10.2147/OPTH.S567933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ronald R Krueger,1 Vance Thompson,2 Kerry Solomon,3 Stephen A Wexler,4 Thomas E Clinch,5 Jeffrey Whitman,6 Andrew Moyes,7 Francis Price,8 Michael Gordon9
1Department of Ophthalmology and Visual Sciences, Truhlsen Eye Institute, University of Nebraska Medical Center, Omaha, NE, USA; 2Vance Thompson Vision, University of South Dakota Sanford School of Medicine, Sioux Falls, SD, USA; 3Carolina Eyecare Physicians, LLC, Mount Pleasant, SC, USA; 4Department of Ophthalmology and Visual Sciences, Washington University School of Medicine, St. Louis, MO, USA; 5Eye Doctors of Washington, Chevy Chase, MD, USA; 6Key-Whitman Eye Center, Dallas, TX, USA; 7Moyes Eye Center, PC, Kansas City, MO, USA; 8Price Vision Group, Indianapolis, IN, USA; 9Gordon Schanzlin New Vision Institute, San Diego, CA, USA
Correspondence: Ronald R Krueger, Department of Ophthalmology and Visual Sciences, Truhlsen Eye Institute, University of Nebraska Medical Center, 985540 Nebraska Medical Center, Omaha, NE, 68198, USA, Tel +1 402-559-3092, Email [email protected]
Purpose: Evaluate the safety and efficacy of ray tracing‒based LASIK surgery to correct myopia in eyes with and without astigmatism.
Patients and Methods: This prospective study included adults with myopia up to − 10.00 D, with or without astigmatism (NCT04219891). For each eye, a 3D virtual model and personalized ablation profile were developed using data from InnovEyes™ Sightmap and ray-tracing algorithm, followed by a wavelight plus LASIK treatment. Efficacy endpoints included percentage of eyes achieving manifest refraction spherical equivalent (MRSE) within 1.00 and 0.50 D of emmetropia at refractive stability and uncorrected distance visual acuity (UDVA) assessments. Follow-up was up to 12 months. Safety endpoints included percentage of eyes that lost ≥ 2 lines corrected distance visual acuity (CDVA) at refractive stability versus preoperative CDVA and non‒flap-related ocular serious adverse events (SAEs). Mean optical aberrations were assessed. Dry eye symptoms were evaluated using ocular surface disease index scores. Patient-reported outcomes were assessed using Patient-Reported Outcomes With LASIK questionnaire.
Results: A total of 163 patients (326 eyes) completed the study. Refractive stability was achieved at 3 months; during a 1- to 3-month interval, 99.4% of eyes had ≤ 1.00 D change in MRSE. MRSE within 0.50 and 1.00 D of emmetropia was achieved in 92.0% and 98.5% of eyes. At 12 months, 94.4% of eyes achieved UDVA of 20/20 or better. No eyes lost ≥ 2 lines of CDVA; no ocular SAEs or non-ocular adverse device effects were reported. Slight increase in coma (0.086 μm) and decrease in spherical aberration (− 0.030 μm) were reported at 12 months. Dry eye symptoms improved after procedure (preoperative, 14.90± 13.07; 12 months, 7.69± 8.12). Postoperatively, 98% of patients reported being very/completely satisfied with their vision.
Conclusion: Ray tracing‒guided LASIK treatment was safe and effective for correcting myopia in individuals with and without astigmatism, producing stable visual outcomes and high satisfaction.
Keywords: myopia, personalized ablation profile, personalized eye model, ray tracing‒guided treatment, refractive surgery
Introduction
The 1999‒2004 National Health and Nutrition Examination Survey estimates that clinically relevant refractive error, such as myopia, hyperopia, and astigmatism, affects half of all adults in the United States.1 Globally, myopia is the most common refractive error, with prevalence estimated to reach 50% by 2050.2,3 Laser-assisted in situ keratomileusis (LASIK) is a safe and effective procedure used to correct refractive error.4,5 The goals of refractive surgery are to reduce refractive error, achieve the desired uncorrected visual acuity (VA), and preserve or improve corrected VA.
Early conventional LASIK ablation profiles provided good refractive outcomes but failed to account for the effect of corneal curvature, resulting in small optical zones, induction of higher-order aberrations, and poor night vision.6,7 Custom ablation treatments to improve outcomes have been developed, including wavefront-guided, wavefront-optimized, and topography-guided ablation.8–10 Current wavefront-based and topography-based methods for calculating the ablation profile use simplified eye models (such as the Gullstrand model eye)11 that do not account for the multiple refractive elements of the eye that may result in residual (or increased) higher-order aberrations, particularly at higher refractive corrections.12 A more accurate and personalized calculation of the corneal laser ablation profile is needed to achieve better surgical outcomes.
Ray tracing‒guided vision correction uses a treatment algorithm for calculating and optimizing ablation profiles12 and has been reported to be safe and effective in patients with and without astigmatism in a proof-of-concept study.13,14 More recently, data from the InnovEyes™ Sightmap (Alcon Vision LLC, Fort Worth, TX, USA) was used to develop a ray tracing algorithm. InnovEyes Sightmap is a single device that integrates wavefront profile, whole eye biometry, and Scheimpflug tomography. These data are used by the ray-tracing algorithm to generate a personalized 3-dimensional (3D) virtual eye model.15 This computer-based, iterative method takes into consideration the multiple refractive interfaces of the eye and uses the personalized eye model to optimize the treatment plan. Ray tracing‒guided vision correction using the InnovEyes Sightmap has been reported to be safe and effective in patients with and without astigmatism.15,16 In a prospective study, personalized LASIK ablation profiles based on optical ray tracing were used to successfully treat eyes with moderate-to-high myopic astigmatism, with no unexpected complications.13 A multicenter study that evaluated the efficacy and safety of the InnovEyes Sightmap‒guided treatment at 4 sites in 212 eyes with preoperative myopia ≤−9.00 diopters (D) and astigmatism of 0 to −4.00 D reported that corrected and uncorrected VA of 20/20 was achieved in 100% and 98% of eyes, respectively, at 3 months postoperatively; there were no procedure-related safety signals.15 A single-center, retrospective review of 400 consecutive eyes with a preoperative myopia ≤−8.25 D sphere found that all eyes achieved 20/20 corrected and uncorrected VA and a decrease in spherical aberrations after 3 months.16
The purpose of this prospective multicenter clinical study, designed in accordance with ANSI Z80.11-2012(R2017), was to evaluate the safety and efficacy of ray tracing‒based LASIK surgery for the correction of myopia in eyes with and without astigmatism as part of a premarket approval submission in the United States. This multicenter prospective study provided a larger treatment range and longer follow-up than previously published studies. Additionally, this study included higher-order aberrations and Patient-Reported Outcomes with LASIK (PROWL).
Methods
Study Design
This was a prospective, single-arm, multicenter, interventional study (March 2020‒November 2022; NCT04219891) conducted at 9 sites in the United States. Patients received bilateral wavelight plus LASIK treatment. Data collected from the InnovEyes Sightmap device were used to generate a 3D eye model, which was used by the ray-tracing algorithm to create the ablation profile. All eyes were targeted for emmetropia using data generated by the algorithm; planning was not required. Nomograms were not used. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and in compliance with good clinical practice guidelines. The University of Nebraska Medical Center deferred this study’s approval to a central institutional review board (Advarra Inc., Columbia, MD, USA; registration number, 00000971). The study was approved by Advarra Inc. (Pro00040863), and all patients provided informed consent before the initiation of any study-specific procedures.
Patients were ≥18 years old with myopia up to −10.00 D with or without astigmatism. Other inclusion criteria were astigmatism up to −4.50 D, manifest refraction spherical equivalent (MRSE) up to −12.00 D, photopic corrected distance VA (CDVA) of 20/20 or better (≤0.04 logarithm of the minimum angle of resolution [logMAR]), photopic uncorrected distance VA (UDVA) of 20/40 or worse (≥0.34 logMAR), <0.75 D difference between InnovEyes Sightmap measured refraction and subjective manifest refraction, and stable refraction (≤±0.50 D) for ≥12 months before surgery.
Key exclusion criteria were history of corneal disease or retinal vascular disease, keratoconus, or glaucoma; previous intraocular or corneal surgery; intent to have monovision treatment; systemic medications that may confound the outcome of the study; predicted residual stroma bed thickness <250 µm; and pregnancy or breastfeeding.
Visits included screening; surgery; day 1; week 1; and postoperative months 1, 3, 6, 9, and 12. The full analysis set included all eyes that underwent successful surgery. The safety analysis set included all eyes that underwent surgery or attempted surgery (eyes that received eye drops for flap creation).
Intervention
The WaveLight FS200 femtosecond laser (Alcon Vision LLC) was used to create a corneal flap using standard procedure. Flap parameters, including thickness and diameter, were determined by each surgeon (recommended parameters: flap thickness, 100‒120 µm; flap diameter, 8.5‒9.0 mm). The WaveLight EX500, a stationary scanning-spot excimer laser system (WaveLight GmbH, Erlangen, Germany), was used to perform wavelight plus LASIK treatment using the preoperative data from the InnovEyes Sightmap. Preoperative data collected using the InnovEyes Sightmap device included measurements of corneal shape and thickness, pupil diameter, axial length, optical aberrations (astigmatism, coma, sphere/focus, spherical aberration, tilt, trefoil, and root mean square height [RMSh]), and refractive error. InnovEyes Sightmap was used by specially trained physicians, medical staff, and optometrists according to the user manual instructions. The personnel ensured that measurements, such as cylinder and axis, were consistent. To avoid excessive accommodation, the difference between InnovEyes Sightmap and manifest refractions was within 0.75 D, per protocol, and preferably within 0.5 D. WaveLight EX500 software included the InnovEyes ray-tracing algorithm. A 3D virtual model was generated for each individual eye using the data captured by InnovEyes Sightmap, and a specific ablation profile was calculated for refractive correction.
Efficacy and Safety Assessments
Efficacy measures included MRSE, UDVA, and CDVA under photopic conditions (85 cd/m2 luminance). Monocular CDVA and UDVA were assessed at 4 m. Co-primary efficacy endpoints were the percentage of eyes with MRSE within 0.50 and 1.00 D of emmetropia at refractive stability, percentage of eyes with UDVA of 20/40 or better at refractive stability, and percentage of eyes that achieved refractive stability. Other efficacy endpoints included percentage of eyes with MRSE predictability within ±0.50, ±1.00, and ±2.00 D, and percentage of eyes with UDVA equal to or better than preoperative CDVA. Mean aberrations, including astigmatism, sphere, trefoil, coma, spherical aberration, and RMSh were assessed using the InnovEyes sightmap. Aberrometry was performed without dilation under mesopic conditions, with pupils >4.5 mm.
Co-primary safety endpoints were percentage of eyes that lost ≥2 lines of CDVA, percentage of eyes with CDVA worse than 20/40, percentage of eyes with an increase of manifest refractive astigmatism >2.00 D of absolute cylinder compared with preoperative refraction, and percentage of eyes with a non‒flap-related ocular serious adverse event (SAE). Safety criteria were met if the percentage of eyes was lower than the target rate at the time of refractive stability.
Patient-Reported Outcomes
For patients receiving LASIK treatment, PROWL is a psychometrically sound questionnaire determined to be reliable and valid.17,18 PROWL was used to assess satisfaction with treatment, visual symptoms (double images, halos, glare, and starbursts), and ocular surface disease index (OSDI). OSDI was based on a composite score from 0 to 100. OSDI scores were 0–12 for normal eyes, 13–22 for mild, 23–32 for moderate, and 33–100 for severe dry eye disease.
Statistics
Refractive stability was achieved if the following criteria were met when comparing two visits (MRSE assessed ≥3 months apart or comparing MRSE at 1-month and 3-month visits): ≥95% of treated eyes had MRSE change ≤1.00 D, mean rate of change in MRSE was ≤0.50 D per year, mean rate of change in MRSE decreased monotonically over time (projected asymptote of 0 or a rate of change attributable to normal aging), 95% CI for mean rate of MRSE change included 0; stability was confirmed ≥3 months after the stability time point by ≥80% of the cohort. Statistical analysis was performed using SAS® software (SAS Institute Inc., Cary, NC, USA).
Results
Patient Disposition
A total of 168 patients (336 eyes) successfully received bilateral surgical treatment. Five patients discontinued after attempted surgery: 2 withdrew and 3 were lost to follow-up; 163 patients (326 eyes) completed the study. The full analysis set, defined as all eyes that successfully underwent surgery, included 167 patients (334 eyes; 1 patient was excluded because of pregnancy).
Mean ± SD age was 33.3±7.0 years; 62.9% (105/167) of patients were female, and 76.6% (128/167) were White (Table 1). Baseline mean ± SD UDVA, CDVA, and MRSE were 1.188±0.400 logMAR, −0.080±0.062 logMAR, and −4.71±2.31 D, respectively; 45.2% (151/334) of eyes had minimal to no preoperative astigmatism (manifest refraction cylinder 0 to ≤−0.50 D); 54.8% of eyes (183/334) had astigmatism with manifest refraction cylinder treatment >−0.50 to ≤−4.00 D.
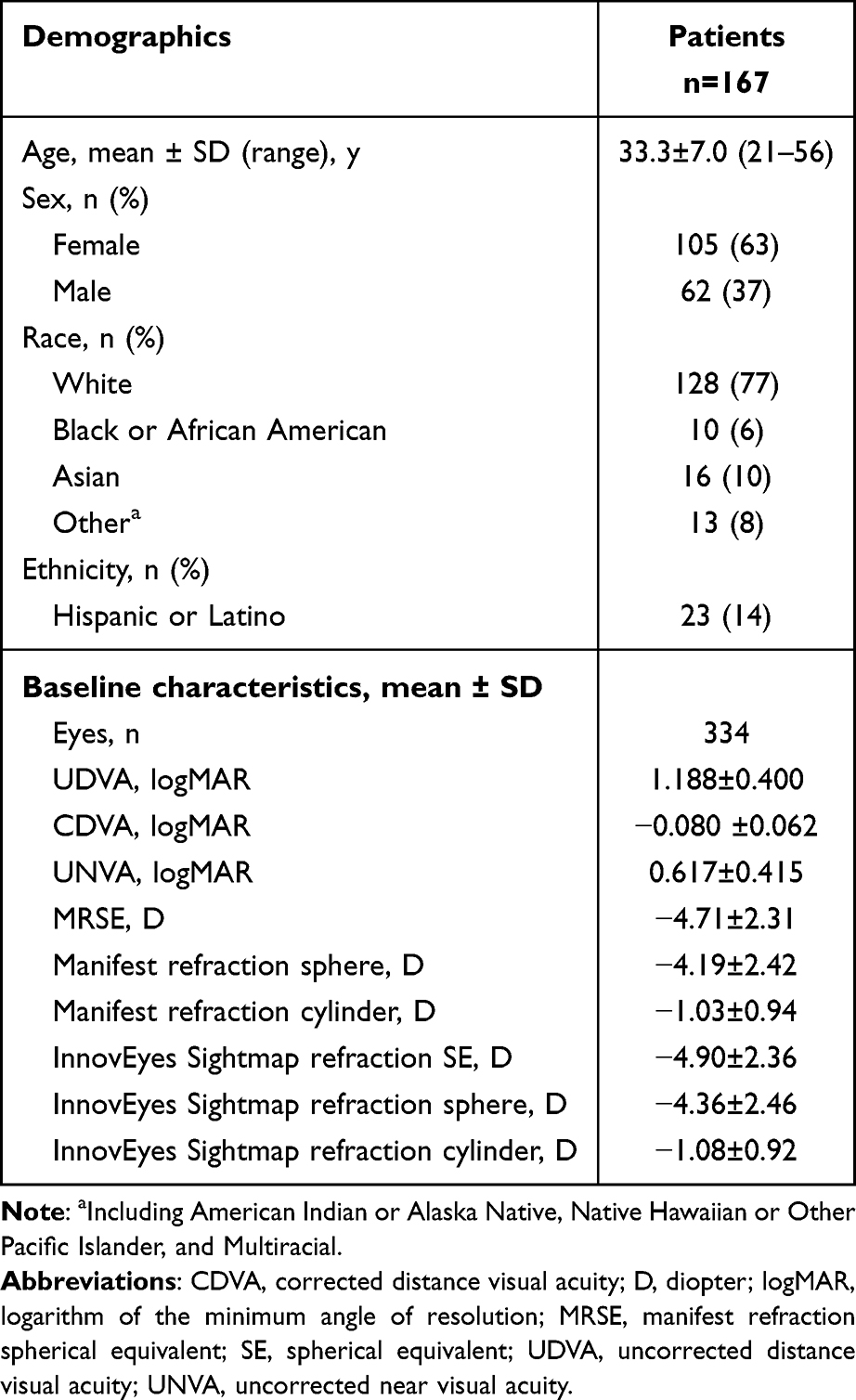 |
Table 1 Patient Demographics and Baseline Characteristics |
Refractive and Safety Outcomes
Refractive stability was achieved postoperatively at 3 months, defined as ≥95% of eyes with ≤1.00-D change in MRSE, mean rate of change ≤0.04 D/month, and the 95% CI included 0. During the 1- to 3-month interval, 99.4% (324/326) of eyes had ≤1.00-D change in MRSE; mean rate of MRSE change was −0.005 D/month. Refractive stability was confirmed at the 3- to 6-month interval (98.5% [321/326] of eyes had ≤1.00-D MRSE change).
Mean ± SD MRSE was −0.049±0.349 and −0.061±0.325 D at 3 and 12 months, respectively (Table 2). At 3 months, 92.0% (300/326) and 98.5% (321/326) of eyes achieved MRSE within 0.50 and 1.00 D of emmetropia, respectively. At 12 months, 94.4% (304/322) and 99.7% (321/322) of eyes achieved MRSE within 0.50 and 1.00 D of emmetropia, respectively. At 3 months, 3 eyes (0.9%) were overcorrected by >1.00 D and 2 eyes (0.6%) were undercorrected by >1.00 D. At 12 months, 1 eye was overcorrected by >1.00 D and none were undercorrected by >1.00 D. Undercorrection occurred in the same patient and was attributed to severe dry eye.
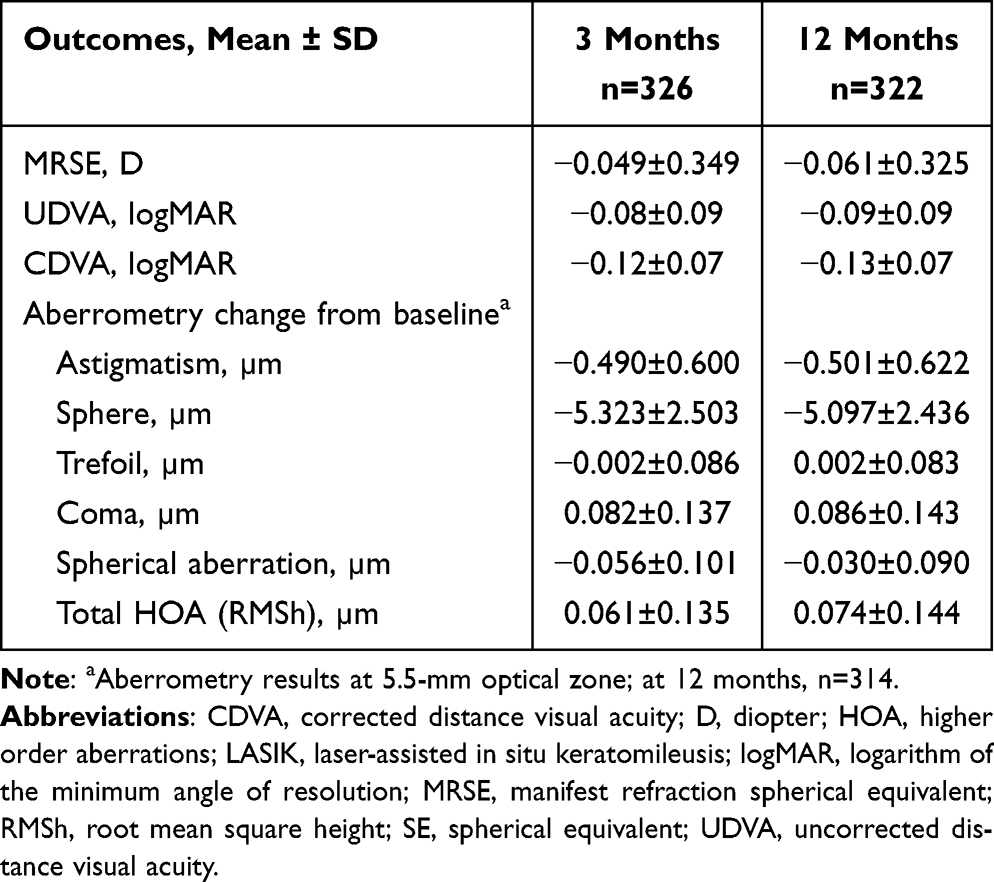 |
Table 2 Efficacy Outcomes at 3 and 12 Months Postoperatively |
All eyes (100%) achieved UDVA of 20/40 or better, and 92.3% (301/326) of eyes achieved UDVA of 20/20 or better at 3 months (Figure 1A), with 94.4% (304/322) achieving UDVA 20/20 or better at 12 months. Mean ± SD UDVA improved from 1.19±0.40 logMAR preoperative to −0.08±0.09 and −0.09±0.09 logMAR at 3 and 12 months, respectively (Table 2). At 3 months, postoperative UDVA was equivalent to preoperative CDVA in 72.4% (236/326) of eyes and was ≥1 line better in 12.9% (42/326) and ≥1 line worse in 14.7% (48/326) of eyes (Figure 1B). At 12 months, postoperative UDVA was equivalent to preoperative CDVA in 76.1% (245/322) of eyes and was ≥1 line better in 14.0% (45/322) and ≥1 line worse in 9.9% (32/322) of eyes.
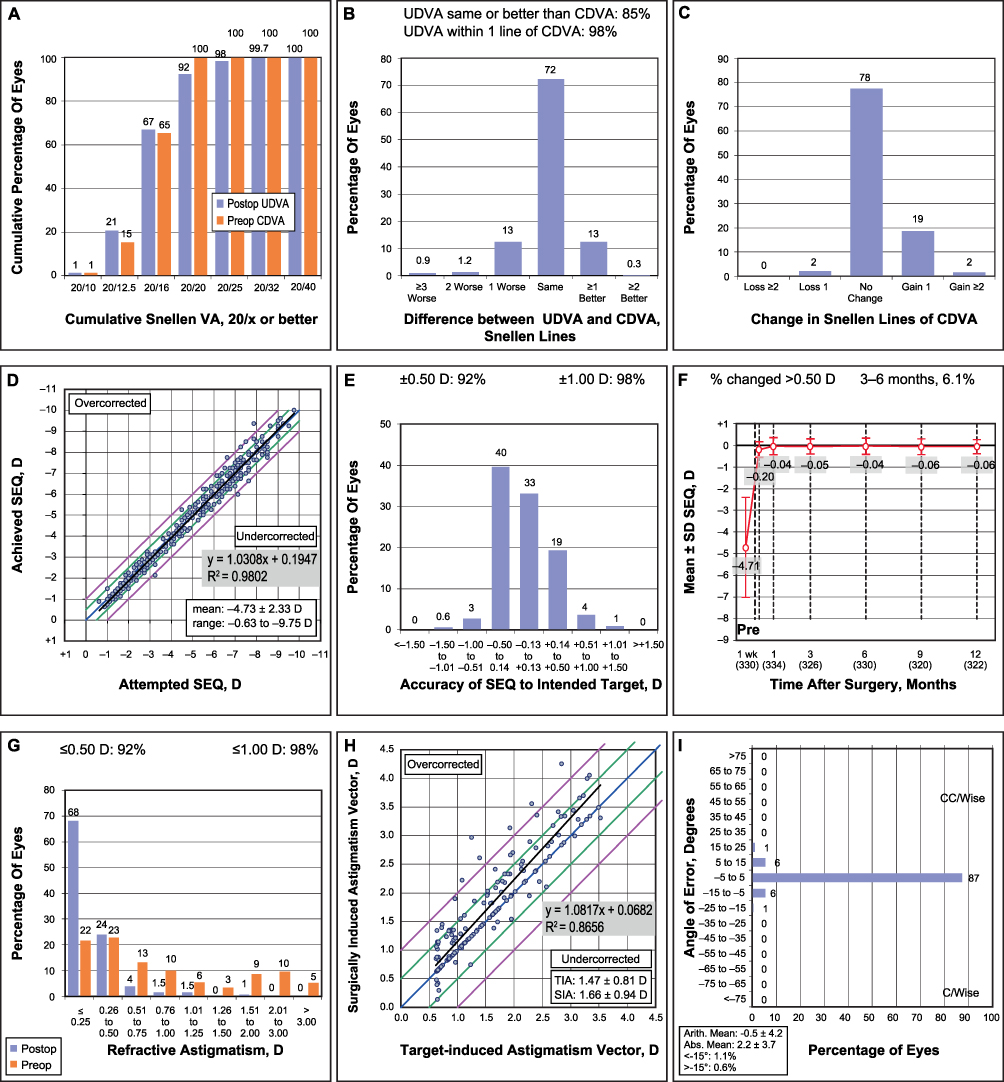 |
Figure 1 Standard graphs for reporting refractive surgery outcomes and astigmatism correction at 3 months postoperatively in 326 eyes targeted for Plano. Cumulative postoperative UDVA and CDVA (A), changes in Snellen lines for postoperative UDVA compared with preoperative CDVA (B), changes in Snellen lines for postoperative compared with preoperative CDVA (C), attempted versus achieved spherical equivalent refraction (D), accuracy of spherical equivalent refraction (E), spherical equivalent refraction by visit (F), refractive astigmatism (G), target induced versus surgically induced astigmatism in 181 astigmatic eyes (H), and refractive astigmatism angle of error in 181 astigmatic eyes (I). Abbreviations: Abs mean, absolute mean; Arith mean, arithmetic mean; CDVA, corrected distance visual acuity; preop, preoperative; postop, postoperative; SEQ, spherical equivalent refraction; SIA, surgically induced astigmatism; TIA, target-induced astigmatism; UDVA, uncorrected distance visual acuity; VA, visual acuity. |
Mean ± SD CDVA improved from −0.08±0.06 preoperative to −0.12±0.07 and −0.13±0.07 logMAR at 3 and 12 months, respectively (Table 2). At 3 months, 77.6% (253/326) of eyes had no change in postoperative versus preoperative CDVA (Figure 1C), 20.2% (66/326) gained ≥1 line, and 2.1% (7/326) lost 1 line. At 12 months, 71.1% (229/322) of eyes had no change in CDVA, 26.7% (86/322) gained ≥1 line, and 2.2% (7/322) lost ≥1 line.
At 12 months, all eyes (326/326) achieved CDVA of 20/32 or better and 98.7% (322/326) achieved CDVA of 20/20 or better. At any postoperative visit, 4/336 eyes (1.2%) had a loss of ≥2 lines in CDVA compared with preoperative and 4/336 eyes (1.2%) had non‒flap-related ocular SAEs. Two eyes had a loss of ≥2 lines in CDVA before refractive stability; these eyes recovered to within 2 lines of baseline CDVA at refractive stability. Two additional eyes had a loss of >2 lines in CDVA after refractive stability was achieved. Of these, one eye had a decrease in CDVA from −0.12 logMAR at baseline to 0.14 logMAR at 9 months; this patient had an adverse event of corneal opacity after probable viral infection, and CDVA improved to −0.08 logMAR at 12 months. Another eye had a decrease in CDVA from −0.16 logMAR at baseline to 0.08 logMAR at 12 months; the patient had extreme dry eye related to a lack of sleep before the visit. Reduced visual acuity was not related to the device in these eyes. No eyes with preoperative CDVA 20/20 or better had postoperative CDVA worse than 20/40, and no eyes had a postoperative increase in manifest refractive astigmatism >2.00 D of absolute cylinder compared with preoperative refraction.
Additional standard graphs for reporting refractive surgery outcomes, including attempted versus achieved spherical equivalent refraction, accuracy of spherical equivalent refraction, and mean spherical equivalent refraction as a function of time, are shown in Figure 1D‒F. Mean preoperative SEQ was −4.73±2.33 D (Figure 1D), with 92% and 98% of eyes achieving SEQ within 0.50 and 1.00 D of intended target, respectively (Figure 1E), and mean ± SD SEQ at 12 months of −0.06±0.32 (Figure 1F).
Refractive astigmatism results are summarized in Figure 1G. In a sub-analysis of eyes with astigmatism (preoperative manifest refraction cylinder >0.50 D; n=181), postoperative manifest refraction cylinder at 3 months was within 0.50 D and 1.00 D in 88.4% and 96.1% of eyes, respectively. Analysis of target-induced astigmatism (1.47±0.81 D) and surgically induced astigmatism (1.66±0.94 D) in 181 astigmatic eyes at 3 months is summarized in Figure 1H; refractive astigmatism angle of error in this subgroup is shown in Figure 1I. Based on a vector analysis in these 181 astigmatic eyes, mean correction ratio was 1.138, representing an overcorrection of ~14% in treatment magnitude with application at the correct axis; absolute error of angle was within ±15° in 98.3% of astigmatic eyes overall, with only those eyes in the lowest cylinder bin for preoperative astigmatism (>–0.50 to ≤–1.00 D) having absolute error of angle values outside this range. Standard graphs for reporting astigmatism correction are shown in Figure 2.
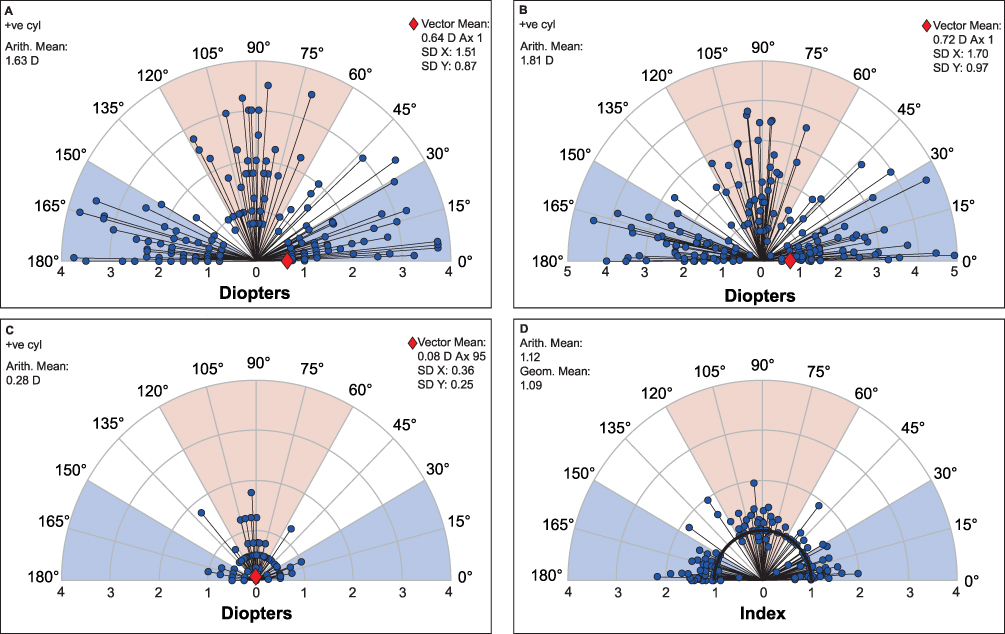 |
Figure 2 Single-angle polar plots for the target-induced astigmatism vector (A), surgically induced astigmatism vector (B), difference vector (C), and correction index (D). Abbreviations: Arith. mean, arithmetic mean; Geom. mean, geometric mean; +ve cyl, positive cylinder; SD, standard deviation. |
Most eyes (>84%) had no change or a clinically significant improvement (>0.30 logMAR improvement at ≥2 spatial frequencies) in contrast sensitivity, with or without glare, at 12 months. Specifically, 48.2% (157/326) and 34.0% (111/326) of eyes had a clinically significant improvement in contrast sensitivity with and without glare, respectively, at 12 months (Table 3). Clinically significant decrease in contrast sensitivity at 12 months was observed in 17.5% and 11.3% of eyes with and without glare. Postoperative mean contrast sensitivity increased numerically from preoperative values at all spatial frequencies (except 9 months at 1.5 cycles per degree [mean change, –0.024 log contrast]). Mean improvement in postoperative versus preoperative contrast sensitivity at 12 months was 0.119–0.208 and 0.008–0.157 log contrast with and without glare, respectively.
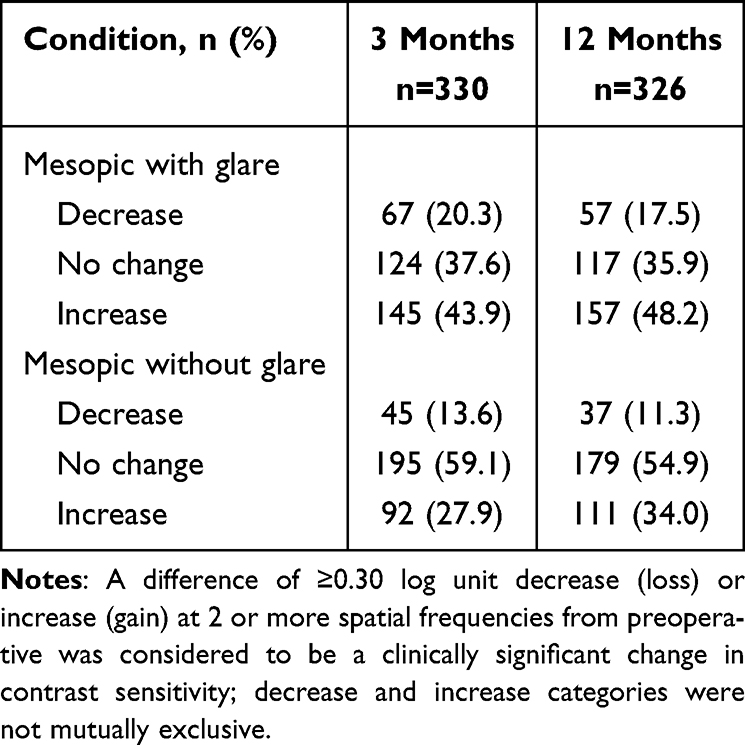 |
Table 3 Percentage of Eyes with Clinically Significant Changes in Corrected Distance Contrast Sensitivity |
A small increase in mean ± SD total higher-order aberrations for the 5.5-mm optical zone was observed at 12 months (0.074±0.144 µm; Table 2), including an increase in coma (mean change ± SD, 0.086±0.143 µm) and a decrease in astigmatism (mean change ± SD, −0.501±0.622 µm), sphere (mean change ± SD, −5.097±2.436 µm), and spherical aberration (mean change ± SD, −0.030±0.090 µm); trefoil remained relatively unchanged (mean change ± SD, 0.002±0.083 µm).
The safety analysis set included 336 eyes. At 3 months, no eyes had a loss of ≥2 lines in postoperative versus preoperative CDVA, no eyes with preoperative CDVA ≥20/20 had postoperative CDVA worse than 20/40, no eyes had an increase >2.00 D of absolute cylinder in postoperative versus preoperative manifest refraction astigmatism, and no eyes had non‒flap-related ocular SAEs. There were no reported ocular or non-ocular adverse device effects.
Patient-Reported Outcomes
Based on the PROWL questionnaire, 78% versus 53% of participants had ≥1 symptom preoperatively versus postoperatively. Double images, glare, halos, and starbursts were reportedly less prevalent and bothersome postoperatively versus preoperatively (Figure 3A). Most patients (98%; 159/163) were “completely satisfied” or “very satisfied” with their vision, and 91% reported spectacle independence (including distance and near vision combined). At 12 months, 98% (158/161) of patients who drove reported no difficulty driving during the daytime in familiar places; 1.9% (3/161) of patients reported a little difficulty. Throughout the postoperative period, no patients reported that they had stopped driving because of their vision.
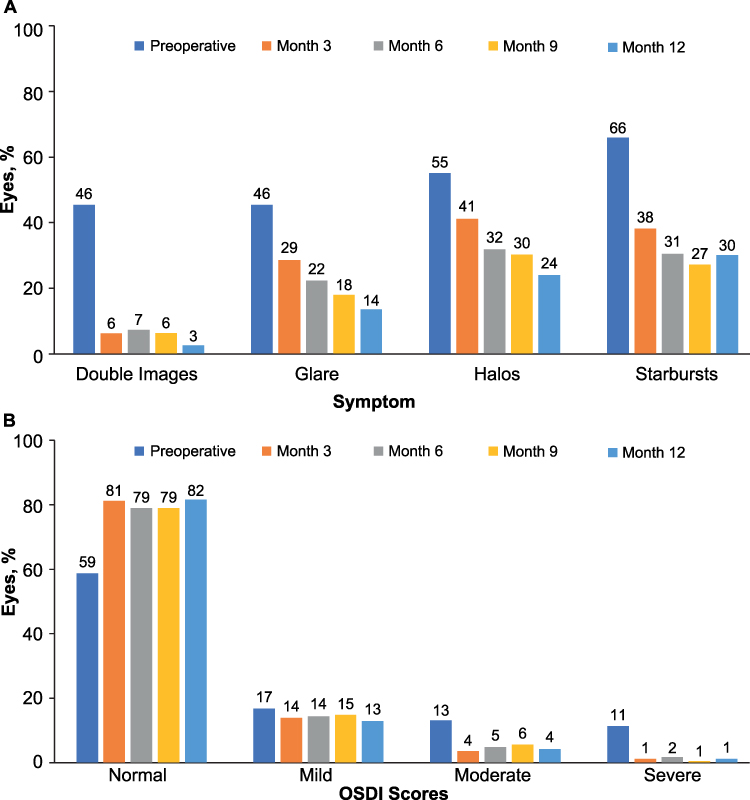 |
Figure 3 Symptom prevalence (A) and OSDI score distribution (B) from the PROWL questionnaire (safety analysis set). Abbreviations: LASIK, laser-assisted in situ keratomileusis; OSDI, ocular surface disease index; PROWL, Patient-Reported Outcomes With LASIK. |
At 3 months, mean OSDI scores improved versus preoperative scores (mean reduction ± SD, −6.48±12.95; Figure 3B); mean scores remained stable at 12 months. Based on OSDI scores, dry eye symptoms improved after the procedure.
Discussion
The ray tracing‒based LASIK surgery using the InnovEyes Sightmap diagnostic device was safe and effective for correcting myopia with and without astigmatism. This study presents the US Food and Drug Administration–approved clinical trial data for a new class of personalized laser vision correction, which derives its ablation profile from a ray-tracing algorithm and personalized 3D eye model generated by the InnovEyes Sightmap device. This device co-axially captures the 3 essential components used in generating each unique eye model: the eye’s tomography, biometry, and ocular wavefront profile. The ray-tracing algorithm iterates the passage of light through the eye model to the ideal corneal ablation profile and accounts for biomechanics and epithelial remodeling corresponding to the shape and profile of tissue removed. The personalization offered by this ablation profile considers the patient’s unique external and internal ocular features and represents a step forward in personalized medicine for laser vision correction.
In this study, a postoperative UDVA of ≥20/20 was achieved by 92% and 94% of eyes at 3 and 12 months, respectively, and ≥20/16 by 67% and 70% of eyes; >20% of eyes achieved UDVA of ≥20/12.5. The proportions of eyes gaining ≥1 line of postoperative UDVA compared with preoperative CDVA were 13% and 14% at 3 and 12 months, respectively. Patient satisfaction was high, with 98% completely or very satisfied. Complete spectacle independence was high despite the inclusion of early presbyopes in the study. A small overall increase in mean total high-order aberrations at 12 months was attributed primarily to increased coma, with trefoil remaining essentially unchanged. The increase in coma has been proposed to be linked to potential eye movement during ablations.19 There was no increase but rather a non-significant decrease in spherical aberration and no device-related adverse effects. This decrease in spherical aberrations is consistent with a previous report (right eye, −0.047±0.095 µm; left eye, −0.051±0.091 µm).16 The small increase in total high-order aberrations at 12 months may have been due to flap creation, epithelial and stromal healing, dry eyes, or changes that occur with each blink during measurements or as a result of eye movement with mildly decentered ablations.19,20
The safety and efficacy outcomes reported in this study were consistent with previous reports for ray tracing‒guided LASIK. A retrospective study that assessed 1-year clinical outcomes in 47 eyes after LASIK treatment demonstrated safety and efficacy of the ray-tracing algorithm. All eyes in the ray-tracing group had ≥20/20 vision, and 91% achieved CDVA ≥20/16 at 12 months. Mean CDVA and UDVA were 0.11 and 0.05 logMAR, respectively. At 6 months, 73% of eyes gained ≥1 line, 2% lost 1 line, and no eyes lost >1 line of CDVA. At 12 months, 48% of eyes gained ≥1 line and no eyes lost ≥1 line of CDVA.14
Another retrospective study that assessed ray tracing‒guided LASIK in 400 myopic eyes at a single site in Australia reported a postoperative UDVA of ≥20/20 in all eyes, ≥20/16 in 89% of eyes, and ≥20/12.5 in 51% of eyes at 3 months. Mean UDVA was −0.14 logMAR, 39% of eyes gained ≥1 line of UDVA versus preoperative CDVA, and 48% gained ≥1 line of CDVA versus preoperative CDVA. No eyes lost ≥2 lines of CDVA.16 There were non-significant increases in total higher-order aberrations (right eye, 0.064; left eye, 0.066) and a statistically significant decline in spherical aberration (right eye, −0.047; left eye, −0.051), similar to the trend in the current report.16 Participants in the earlier study required a lower range of correction compared with the current report (preoperative myopia ≤–8.25 D versus ≤–9.50 D).16 Furthermore, an increase in total high-order aberrations was also reported in a recent study that assessed ray tracing‒guided LASIK, with postoperative ocular higher-order aberrations significantly increasing at 3 months versus preoperative (0.209 to 0.330 µm; P<0.001).21
Effectiveness and safety data for ray tracing‒guided LASIK suggest that it is a suitable alternative to other custom ablation methods, such as topography-guided LASIK. A study that used a topography-guided LASIK procedure (Contoura Vision; Alcon Vision LLC) in 249 eyes reported that refractive stability was achieved at 3 months. UDVA of ≥20/20 was achieved in 93% (229/247) of eyes at 3 months and 93% (213/230) at 12 months. UDVA of ≥20/16 was achieved in 69% of eyes at 3 months and 65% at 12 months. Furthermore, 26% (63/244) and 31% (71/230) of eyes gained ≥1 line of UDVA at 6 and 12 months, respectively, compared with preoperative CDVA. At 12 months, a UDVA loss of 1 and ≥2 lines were reported in 7.8% and 1.7% of eyes, respectively.10 A recent study reported that significantly better postoperative UDVA and spherical aberration were achieved in eyes after ray tracing‒guided (n=42) compared with topography-guided (n=42) LASIK (P<0.05 for both).22 Spherical aberration was significantly different for the two groups at 3 months after the procedure (P<0.05); there was a substantial decrease in spherical aberration for the ray tracing‒guided LASIK method (P<0.05) but no significant change in spherical aberration for topography-guided LASIK.22 In another comparison of 2 LASIK methods (34 eyes in each group), ray tracing‒guided LASIK was also reported to achieve significantly better UDVA compared with Q value–adjusted ablation (P<0.05); however, MRSE and refractive astigmatism were better in the Q value–adjusted group (P<0.05).23
One advantage of ray tracing‒based technology over topography-guided procedures is that refractive error can be measured using the InnovEyes Sightmap. Although this standardizes an important variable for outcomes, it may introduce a source of error if the patient is accommodating. The current recommendation is to consider the Sightmap refraction valid if it is within ±0.50 D of the manifest refraction. Future clinical use of this system should improve outcomes because treatments are adjusted and the effect of accommodation is further controlled. The application of treatment adjustments and optimizations can lead to improved outcomes, as evident in the real-world data reported by He and Bala.16
Limitations of this study include the single-arm, open-label design, which may introduce bias. Additionally, the study did not enroll patients in the highest myopia range of −10.00 to −11.00 D, limiting the confirmation of the advantages of ray tracing‒guided LASIK in this population. Additional studies will need to evaluate the potential disadvantages of ray tracing‒based LASIK, such as overcorrection,16 and compare the economic burden of ray tracing‒based LASIK with conventional LASIK methods.
Conclusion
Ray tracing‒guided LASIK treatment using personalized eye models was safe and effective for correcting myopia, providing good predictability and visual outcomes as well as high satisfaction in patients with or without astigmatism. The data from this study can be used for updating the treatment algorithm and training of surgeons, therefore contributing to the optimization of surgical treatment outcomes.
Abbreviations
CDVA, corrected distance visual acuity; D, diopters; LASIK, laser-assisted in situ keratomileusis; logMAR, logarithm of the minimum angle of resolution; MRSE, manifest refraction spherical equivalent; OSDI, ocular surface disease index; PROWL, Patient-Reported Outcomes With LASIK; RMSh, root mean square height; SAE, serious adverse event; SE, spherical equivalent; UDVA, uncorrected distance visual acuity; VA, visual acuity.
Data Sharing Statement
The data used to support the findings of this study are available upon reasonable request from the study sponsor, Alcon Research LLC.
Acknowledgments
Medical writing assistance was provided by Natalia Zhukovskaya, PhD, of ICON plc (Blue Bell, PA, USA) and was funded by Alcon.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by Alcon Research LLC.
Disclosure
RRK: Consultant for Alcon, Bausch & Lomb, Glaukos, and Senogen. VT: Consulting and research funding from Alcon, Bausch and Lomb, BVI, Carl Zeiss Meditec, Glaukos, Johnson & Johnson, Rayner, and RxSight; consultant for Tarsus; and received stock options from Rayner and Tarsus. KS: Consultant for Alcon, Glaukos, Rayner, and RxSight; lecture fees from Alcon; received grant support from Alcon, Bausch & Lomb, Johnson & Johnson, Rayner, RxSight, and Zeiss; and equity ownership in CVC Capital Partners, Glaukos, Mati Therapeutics, Octane Visionary VC Fund, Pogotec, Rayner, RxSight, TearLab, US Eye, and Versuant. SAW: Consulting and research funding from Alcon. TEC: Research funding from Alcon; serves on the scientific advisory board for Adaptilens. JW: Consultant for Alcon, Bausch & Lomb, Glaukos, Iantrek, Johnson & Johnson, and Tarsus. AM: Research funding from Alcon. FP: Consultant for Aurion, B&L, EyeYon and Staar Surgical; received other fees from RxSight and Strathspey Crown; consulted for Alcon regarding Laser refractive surgery in the last 2 to 3 years unrelated to the study. MG: Consulting and research funding from Alcon. The authors report no other conflicts of interest in this work.
References
1. Vitale S, Ellwein L, Cotch MF, Ferris FL 3rd, Sperduto R. Prevalence of refractive error in the United States, 1999–2004. Arch Ophthalmol. 2008;126(8):1111–12. doi:10.1001/archopht.126.8.1111
2. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
3. Modjtahedi BS, Ferris FL 3rd, Hunter DG, Fong DS. Public health burden and potential interventions for myopia. Ophthalmology. 2018;125(5):628–630. doi:10.1016/j.ophtha.2018.01.033
4. Wen D, McAlinden C, Flitcroft I, et al. Postoperative efficacy, predictability, safety, and visual quality of laser corneal refractive surgery: a network meta-analysis. Am J Ophthalmol. 2017;178:65–78. doi:10.1016/j.ajo.2017.03.013
5. Price MO, Price DA, Bucci FA Jr, et al. Three-year longitudinal survey comparing visual satisfaction with LASIK and contact lenses. Ophthalmology. 2016;123(8):1659–1666. doi:10.1016/j.ophtha.2016.04.003
6. Lawless M, Hodge C. LASIK. Int Ophthalmol Clin. 2013;53(1):111–128. doi:10.1097/IIO.0b013e318271346e
7. Mrochen M, Seiler T. Influence of corneal curvature on calculation of ablation patterns used in photorefractive laser surgery. J Refract Surg. 2001;17(5):S584–S587. doi:10.3928/1081-597X-20010901-15
8. Gambato C, Catania AG, Vujosevic S, Midena E. Wavefront-optimized surface ablation with the Allegretto Wave Eye-Q excimer laser platform: 12-month visual and refractive results. J Refract Surg. 2011;27(11):792–795. doi:10.3928/1081597X-20110407-01
9. Manche E, Roe J. Recent advances in wavefront-guided LASIK. Curr Opin Ophthalmol. 2018;29(4):286–291. doi:10.1097/ICU.0000000000000488
10. Stulting RD, Fant BS, Bond W, et al. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42(1):11–18. doi:10.1016/j.jcrs.2015.08.016
11. Gullstrand A. Procedure of the rays in the eye. Imagery-laws of first order. In: Southall JPC, editor. Helmholtz’s Treatise on Physiological Optics, Translated From the Third German Edition. Vol. 1. Rochester, NY: The Optical Society of America; 1924:350–358.
12. Mrochen M, Bueeler M, Donitzky C, Seiler T. Optical ray tracing for the calculation of optimized corneal ablation profiles in refractive treatment planning. J Refract Surg. 2008;24(4):S446–S451. doi:10.3928/1081597X-20080401-23
13. Schumacher S, Seiler T, Cummings A, Maus M, Mrochen M. Optical ray tracing‒guided laser in situ keratomileusis for moderate to high myopic astigmatism. J Cataract Refract Surg. 2012;38(1):28–34. doi:10.1016/j.jcrs.2011.06.032
14. Cummings AB, Kelly GE. Optical ray tracing‒guided myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol. 2013;7:1181–1191. doi:10.2147/OPTH.S44720
15. Kanellopoulos AJ, Maus M, Bala C, et al. International multicenter, myopic and myopic astigmatism femto LASIK, customized by automated ray-tracing ablation profile calculation: a postmarket study. Clin Ophthalmol. 2024;18:525–536. doi:10.2147/OPTH.S435581
16. He G, Bala C. Ray-tracing-guided myopic LASIK: real-world clinical outcomes. J Cataract Refract Surg. 2023;49(11):1140–1146. doi:10.1097/j.jcrs.0000000000001286
17. Hays RD, Tarver ME, Spritzer KL, et al. Assessment of the psychometric properties of a questionnaire assessing patient-reported outcomes with laser in situ keratomileusis (PROWL). JAMA Ophthalmol. 2017;135(1):3–12. doi:10.1001/jamaophthalmol.2016.4597
18. Eydelman M, Hilmantel G, Tarver ME, et al. Symptoms and satisfaction of patients in the Patient-Reported Outcomes With Laser In Situ Keratomileusis (PROWL) studies. JAMA Ophthalmol. 2017;135(1):13–22. doi:10.1001/jamaophthalmol.2016.4587
19. Thananjeyan AL, Bala C. Higher-order aberrations following ray trace LASIK and the impact of eye movement on coma. Clin Ophthalmol. 2024;18:3389–3398. doi:10.2147/OPTH.S497131
20. Kligman BE, Baartman BJ, Dupps WJ Jr. Errors in treatment of lower-order aberrations and induction of higher-order aberrations in laser refractive surgery. Int Ophthalmol Clin. 2016;56(2):19–45. doi:10.1097/IIO.0000000000000113
21. Luo L, Fan Y, Wang X, et al. Ray tracing‒guided LASIK for high myopia and astigmatism: initial clinical outcomes. Photodiagnosis Photodyn Ther. 2025;55:104715. doi:10.1016/j.pdpdt.2025.104715
22. Cao X, Zhang J, Shao J, Zhang Y, Zheng L. Study of the InnovEyes Sightmap platform in comparing ray-tracing-guided LASIK and topography-guided LASIK. J Refract Surg. 2024;40(12):e994–e1002. doi:10.3928/1081597X-20241030-03
23. Yuan Y, Zhang R, Wang Z, et al. Ray-tracing-guided or Q-value-adjusted FS-LASIK for correction of myopia and myopic astigmatism: a comparative contralateral eye study. J Refract Surg. 2024;40(11):e804–e813. doi:10.3928/1081597X-20240917-01
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.