Back to Journals » Journal of Experimental Pharmacology » Volume 12
Multiple Pathway–Mediated Gut-Modulatory Effects of Maerua subcordata (Gilg) DeWolf
Authors Palla AH ![]() , Sibhat GG, Karim A
, Sibhat GG, Karim A ![]() , Rehman NU
, Rehman NU ![]() , Hiben MG
, Hiben MG ![]()
Received 20 March 2020
Accepted for publication 1 July 2020
Published 14 July 2020 Volume 2020:12 Pages 203—211
DOI https://doi.org/10.2147/JEP.S254818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bal Lokeshwar
Amber Hanif Palla,1 Gereziher Gebremedhin Sibhat,2 Aman Karim,2 Najeeb Ur Rehman,3 Mebrahtom Gebrelibanos Hiben2
1Department of Basic Medical Sciences, Faculty of Pharmacy, Barrett Hodgson University, Karachi, Pakistan; 2Department of Pharmacognosy, College of Health Sciences, Mekelle University, Mekelle, Ethiopia; 3Department of Pharmacology and Toxicology, College of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-Kharj 11942, Saudi Arabia
Correspondence: Mebrahtom Gebrelibanos Hiben
Mekelle University, PO Box 1871 Tel +251 91-118-3120
Fax + 251-34-441-66-81/40-93-04
Email [email protected]
Background: Gastrointestinal disorders are often poorly managed, especially in developing countries, where there are limited resources and therapeutic options. Despite the rich diversity of medicinal plants that offer effective treatment options with fewer side effects, studies that provide scientific verification are lacking. Maerua subcordata (Gilg) DeWolf is among the plants claimed to have wide traditional medicine, use, including as a remedy against gastrointestinal problems. Therefore, this work aimed to evaluate the gut-modulatory effects of a crude leaf extract of M. subcordata (MSL.Cr), as well as its possible mechanism of action.
Methods: A castor oil (10 mL/kg)–induced diarrheal mouse model was used to evaluate the antidiarrheal effect of MSL.Cr, and the spasmodic/antispasmodic effect of the extract was assessed using isolated rabbit jejunum with and without addition of standard cholinergic agonists/antagonists to predict the possible mechanism of action.
Results: MSL.Cr exhibited 40% and 80% protection against castor oil–induced diarrhea in mice at doses of 500 and 1,000 mg/kg, respectively. In isolated rabbit jejunum, the extract increased spontaneous contractions at low doses (0.01– 0.1 mg/mL), and was sensitive to atropine, whereas it showed complete inhibition at higher doses (0.3– 1 mg/mL). It was shown that the relaxant effect was possibly mediated by the involvement of phosphodiesterase-enzyme inhibition and K+-channel activation. The extract potentiated the control concentration–response curve of carbachol, shifting it to the left, similarly to the control drug papaverine. The potassium-channel opening–like activity of MSL.Cr was possibly mediated by the involvement of aspecific K+-channels inhibition, since tetraethylammonium, anunselective antagonist of K+ channels, significantly reversed its inhibitory effect.
Conclusion: This study showed that the M. subcordata leaf extract demonstrated gut-modulatory effects, possibly mediated by a combination of muscarinic-receptor stimulation, phosphodiesterase inhibition, and aspecific K+-channel activation.
Keywords: Maeruaa subcordata, constipation, diarrhea, phosphodiesterase inhibition, K+ channel activation
Introduction
In the developing world, gastrointestinal (GI) diseases often cause substantial morbidity and mortality. Since countries of the developing world have limited resources and therapeutic options, diarrhea and/or constipation are usually not properly managed and tend to be chronic, requiring lifelong treatment. For instance, one such chronic diseases of the gut is irritable bowel syndrome, which has alternating diarrhea and/or constipation events.1 The treatment protocols for chronic GI diseases are lifelong, which often raises major compliance issues, with patients needing to follow on different combinations of medications, ranging from antidiarrheals (eg, loperamide) and/or laxatives (eg, lactulose), to antispasmodic agents (eg, mebeverine hydrochloride).2 This situation not only accounts for cost issues but also side effects of such medications, resulting in noncompliance problems. For this reason, a large percentage of the human population has now reverted to the use of medicinal plants for treatment of such ailments.3 Plant extracts are known to contain multiple constituents that offer disease-modifying effects and sideeffect–neutralizing potential,4 yet few natural products enter clinical trials, owing to their lack of pharmacological validation. As such, in order to achieve maximum benefits for patients and the community, traditional and modern therapeutic skills should work in a complementary manner.5 This could be achieved by combining rich traditional knowledge about natural products with sound pharmacological studies, which would lead to enrichment of the library of natural products and hence predict potential new candidates for the management of chronic diseases. Among medicinal plants, many Maerua (Capparaceae/Capparidaceae spp. are well known for their ethnomedicinal use as herbal medicines to manage various GI disorders. To mention some, M. angolensis (bark, leaf, root) is used as a purgative and a remedy for stomachache, diarrhea, and vomiting,6−8 M. calophylla (bark, leaf, root) drunk to treat stomach ache and diarrhea;9 M. crassifolia (leaf) used in African traditional medicine for the management of various GI disorders,10−13 M. oblongifolia (bark, root, leaves, and whole) for such disease conditions as stomachache, colic pain, severe abdominal cramps, and hookworm,14,15 M. sessiliflora (bark)against intestinal worms and tapeworm,16 and M. triphylla (leaf) to treat gastric disease.17 Likewise, M. subcordata (Gilg) DeWolf has wide traditional medicinal claims, including such GI problems as abdominal disturbances (nausea, vomiting, and diarrhea) and swelling (distended abdomen).18,19 However, scientific verification of these traditional claims, including antispasmodic and antidiarrheal activities, is lacking. Therefore, this study aimed to evaluate the gut-modulatory effects of the leaf extract of M. subcordata.
Methods
Plant Material
M. subcordata leaves were collected from around Shiraro (14.3970° N, 37.7743° E), northwest Tigray, northern Ethiopia. The plant was authenticated by Melaku Wendafrash in the National Herbarium, Department of Biology, Addis Ababa University, where a voucher specimen (MG001/2007) was deposited.
Drugs
Acetylcholine chloride, atropine sulfate, loperamide hydrochloride, carbachol (CCh), papaverine, verapamil hydrochloride, glibenclamide (Gb), tetraethylammonium (TEA), and potassium chloride were procured from Sigma-Aldrich and castor oil from a local pharmacy (Karachi Chemical Industries, Pakistan). Isoflurane injection (Abbott Pharmaceuticals) was procured from a local pharmacy. Composition of the physiological solution was done according to the method described by Rehman et al.20
Plant Extract
A 70% ethanol crude extract was prepared from dried and powdered leaves of M. subcordata using maceration extraction three times, each for 72 hours at room temperature in the Department of Pharmacognosy, School of Pharmacy, Mekelle University. The extracts were filtered, combined, concentrated, and dried in an oven at 40°C. Dried extracts were then stored in a refrigerator in vials until used.
Animals
Albino mice (BALB/c) weighing 20–25 g and locally bred New Zealand rabbits (aged 6–7 months and weighing 1–1.5 kg) of either sex were kept at the animal house of Barrett Hodgson University under a controlled environment (23°C–25°C). Swiss albino mice were obtained from the Laboratory of Pharmacology and Toxicology, College of Health Sciences, Mekelle University and used for acute-toxicity studies. Animals were kept in their respective cages with sawdust (changed every 48 hours) and fasted for 24 hours before starting the experiment. They were routinely given tap water ad libitum and a standard diet. Experiments were performed as per the rulings of the Institute of Laboratory Animal Resources, Commission on Life Sciences, National Research Council.21–23 The study was approved by the ethical review committee of Barrett Hodgson University (BR-ER/Pharmacy-001/2020/PI-Dr Amber Hanif Palla).
Acute-Toxicity Studies
The limit-test principle of the Organization for Economic Cooperation and Development guideline 425 was followed to carry out acute-toxicity studies using five female Swiss albino mice (nulliparous, not pregnant) of 6–8 weeks’ age.24 On the first day of the experiment, a single female mouse that had been fasted for 4 hours but with water ad libitum was orally administered 2,000 mg/kg of the extract. The mouse was kept under strict observation for any behavioral or physical changes within the 24 hours. After 24 hours, the other four female mice were treated in the same manner. The mice were observed for 14 days for any mortality, diarrhea, gross behavioral changes like loss of appetite, lacrimation, tremors, and hair erection, and other signs of toxicity.24
In Vivo Antidiarrheal Activity
Diarrhea was induced in BALB/c albino mice by castor oil as per the procedure described by Rehman et al.20 Briefly, mice fasted for 24 hours were divided into four groups of five each. Mice in the negative-control group received saline (10 mL/kg orally) using oral gavage while mice in the second and third groups received 500 and 1,000 mg/kg orally of MSL.Cr, respectively. The fourth group served as the positive-control group, and received loperamide (10 mg/kg orally). After an hour, all mice were orally exposed to castor oil (10 mL/kg), and 4 hours after castor-oil administration, their assigned cages were inspected for diarrhea spots.
In Vitro Experiments
To support the in vivo antidiarrheal experiment, the in vitro effect of MSL.Cr was also tested using isolated rabbit jejunum. To prepare jejunal tissue, a previously described method20 was followed. Briefly, after anestheia with isoflurane followed by cervical dislocation,approximately 2 cm jejunal tissue was suspended in tissue baths with Tyrode’s solution at 37°C and bubbled with carbogen (95% O2 and 5% CO2). After 30 minutes’ incubation of the tissue, increasing doses of MSL.Cr were added to the organ bath to observe any spasmogenic/spasmolytic effect. Usually, plant extracts exhibit gut-stimulatory activity by cholinergic-like actions20 and gut-inhibitory effects by a Ca2+ channel–blocker (CCB) effect,25 phosphodiesterase (PDE) inhibition,26 and/or K+-channel activation.26 To determine whether MSL.Cr also possessed such mechanism(s), low K+ (25 mM)–, high K+ (80 mM)–, and CCh-induced spasms were produced in the tissue and corresponding effects of the different doses of MSL.Cr on relaxation concentration–response curves (CRCs) obtained.27–30
Statistical Analysis
Data are presented as means ± SEM. EC50 values are presented as medians with 95% CIs. CRCs were analysed using nonlinear regression and x2-tests for comparison of antidiarrheal assays. Statistical analysis was performed using GraphPad Prism 8.
Results
Acute Oral–Toxicity Study
A single-dose (2 g/kg) oral administration of of MSL.Cr to female Swiss albino mice had not caused any signs of toxicity during the 14 observation days, and hence it was considered safe to do further experiments.
Effect of M. subcordata Extract on Castor Oil–Induced Diarrhea in Mice
Table 1 shows dose-dependent protection (40% and 80%) from castor oil–induced diarrhea in mice treated with MSL.Cr 500 and 1,000 mg/kg, respectively. The control (saline group) did not show any protection. Loperamide 10 mg/kg, used as positive control, exhibited 100% protection (Table 1).
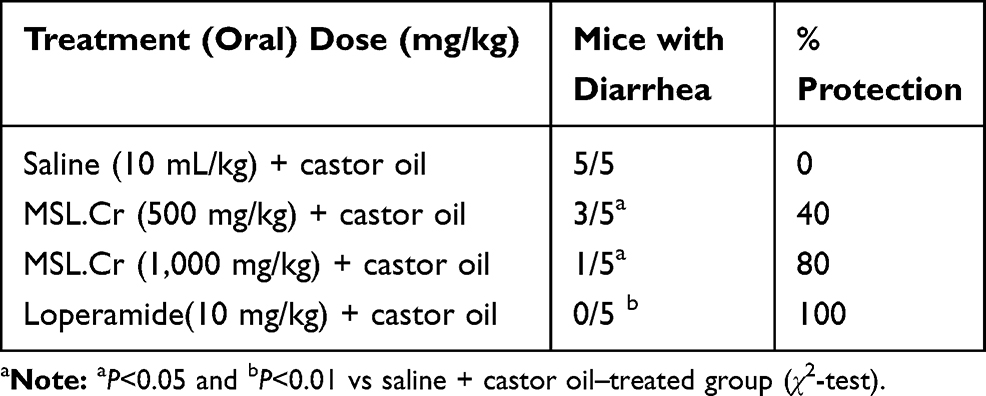 |
Table 1 Antidiarrheal Activity of Crude Extract of Maerua Subcordata Leaves (MSL.Cr) in Mice with Castor Oil (10 mL/kg)–Induced Diarrhea |
Effect of M. subcordata Extract on Isolated Rabbit Jejunum
At lower doses (0.01–0.1 mg/mL), the crude extract dose-dependently increased the baseline contractions of isolated jejunal preparations, reaching a maximum of 178.5±6.5 at 0.1 mg/mL increase compared to the control group, whereas at higher doses (0.3 and 1 mg/mL) it showed an inhibitory effect. These results show a biphasic response of a stimulatory effect at lower doses and an inhibitory effect at higher doses. As shown in Figure 1, pretreatment of jejunal preparations with 0.1 µM atropine completely inhibited the stimulatory effect, whereas the inhibitory effect was potentiated (0.3 mg/mL) compared to nonatropinized preparations (1 mg/mL). At higher doses (0.3 and 1 mg/mL), MSL.Cr inhibited the rhythmic contractions of rabbit jejunum, thus exhibiting an antispasmodic effect. When tested against high K+ (80 mM)–induced contractions, MSL.Cr showed a partial inhibitory effect, whereas it completely reversed the CCh (1 µM)- and low K+ (25 mM)–induced contractions (Figure 2A) at comparable concentrations, with resultant EC50 of 0.42 mg/mL and 0.56 mg/mL, respectively. Verapamil, used as a positive-control drug, was found to be more potent against low and high K+–induced contractions, with respective EC50 values of 0.07 µM and 0.06 µM, compared to CCh-induced contractions (Figure 2B), with an EC50 of 0.44 µM. In PDE-inhibitory experiments, pretreatment of jejunal tissue with MSL.Cr 0.01–0.03 mg/mL deflected the isoprenaline-mediated relaxation CRCs to the left (Figure 3A), similarly to the pattern in papaverine (1–3 µM, Figure 3B), but no such potentiation was observed with verapamil (Figure 3C). After the selective efficacy against low K+– compared to the partial inhibitory effect against high K+–induced contractions had been observed, MSL.Cr inhibitory CRCs against low K+ were reproduced using jejunal tissue pretreated with Gb (10 µM) and TEA (10 mM). Interestingly, the inhibitory effect of MSL.Cr was significantly (P<0.05) reversed in the presence of TEA, thus confirming the involvement of aspecific K+-channel activation (Figure 4).
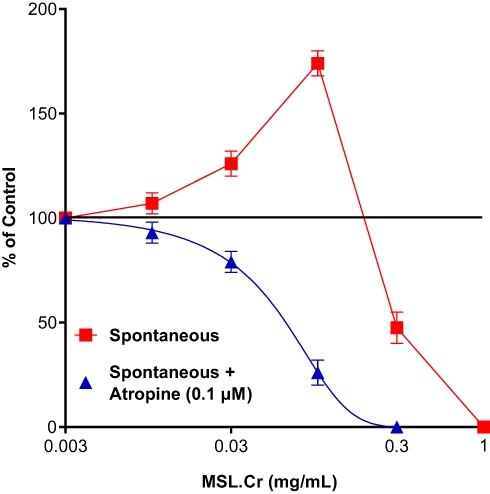 |
Figure 1 Effects of a crude extract of Maerua subcordata leaves (MSL.Cr) on the contraction of isolated rabbit jejunal preparations, both in the absence (■) and presence (▲) of atropine (0.1 µM). Results presented as percentage change compared to control and data as means ± SEM from four to five determinations. |
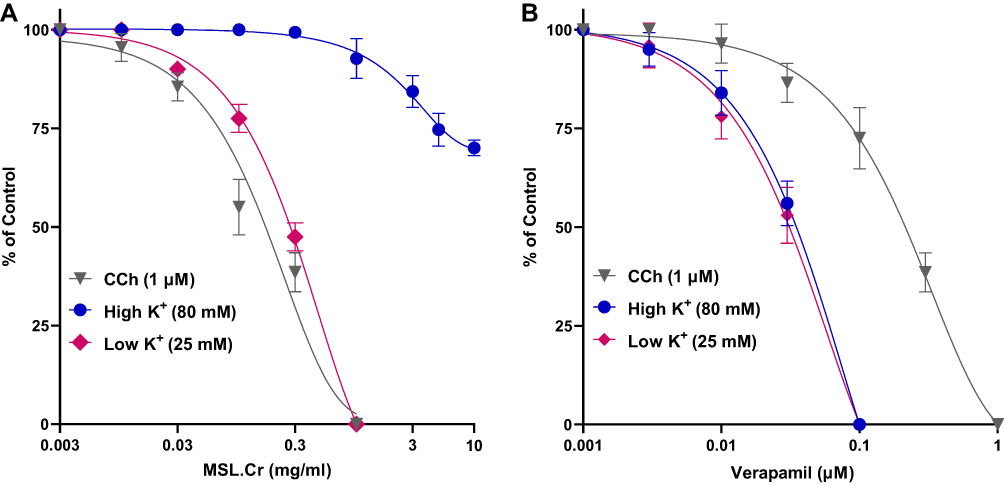 |
Figure 2 Concentration–response curves showing the inhibitory effect of a crude extract of Maerua subcordata leaves (MSL.Cr) (A) and verapamil (B), against carbachol (CCh 1 µM), low (25 mM), and high (80 mM) K+-induced contractions in isolated rabbit jejunal preparations. Results presented as percentage change compared to control and data as means ± SEM, n=3–5. |
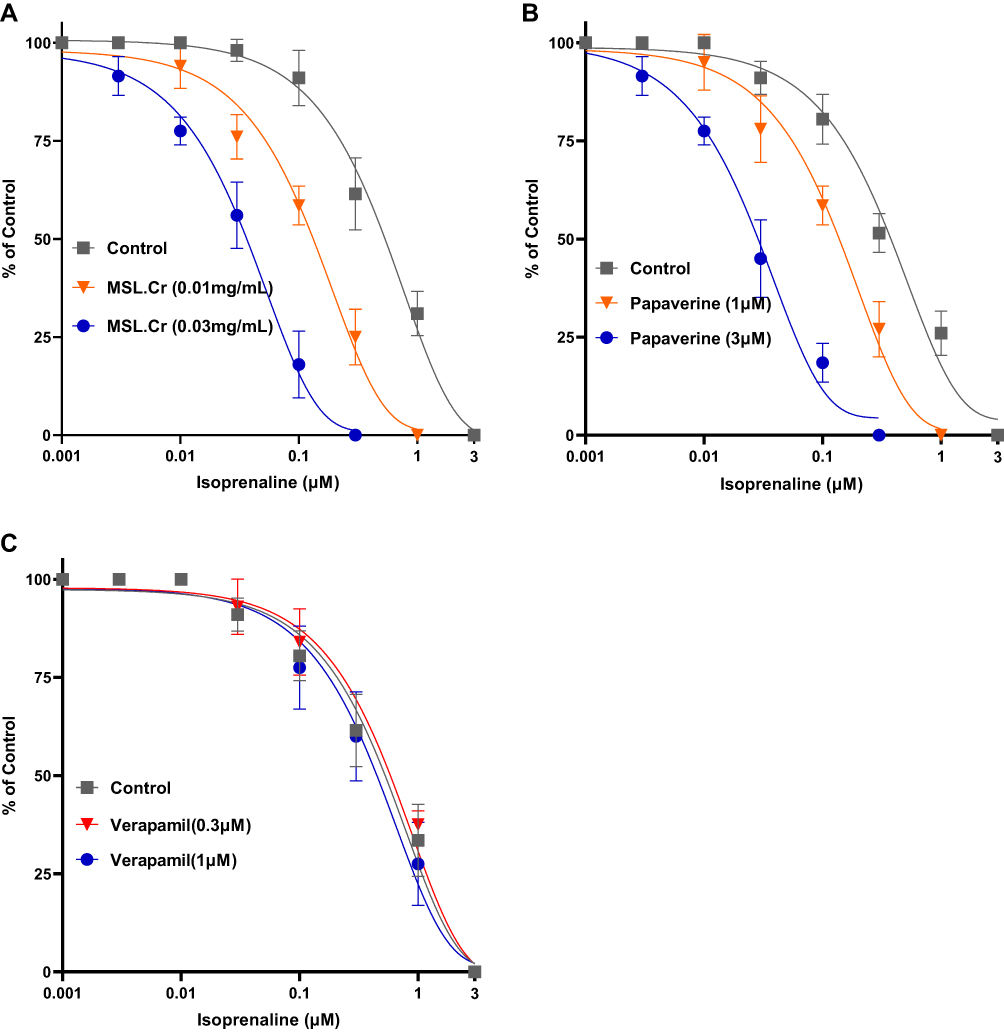 |
Figure 3 Inhibitory concentration–response curves of isoprenaline against carbachol-induced contractions in the absence and presence of different concentrations of a crude extract of Maerua subcordata leaves (MSL.Cr) (A), papaverine (B), and verapamil (C) in isolated rabbit jejunum preparations. Values shown as means ± SEM from four to five determinations. |
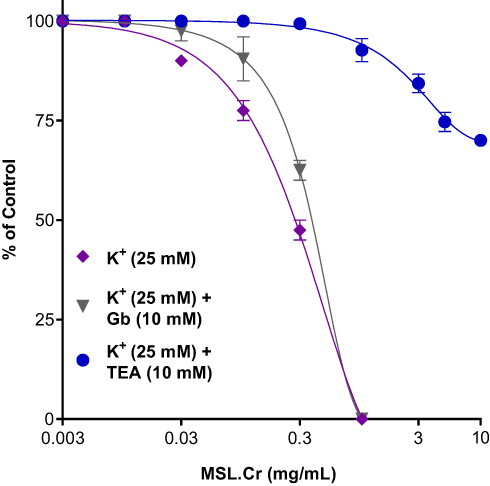 |
Figure 4 Concentration–response curves showing inhibitory effect of a crude extract of leaves of Maerua subcordata (MSL.Cr) against low K+ (25 mM)–induced contractions in the absence and presence of pretreated preparations with Gb (10 µM) and TEA (10 mM) in isolated rabbit jejunal preparations. Values shown as means ± SEM, n=3–5. |
Discussion
Keeping the view that plants belonging to the genus Maerua have had many reports related to their medicinal uses for the management of GI disorders,6,31,32 this study tested the antidiarrheal effect of a hydroalcoholic extract of M. subcordata leaves using castor oil–induced diarrhea in mice. Also, the effect of the extract on the nature of spasmogenic/spasmolytic effects was assessed using isolated rabbit jejunal preparations. The crude extract (MSL.Cr) protected the mice against castor oil–induced diarrhea at 500 and 1,000 mg/kg, similarl to loperamide, a standard antidiarrheal drug,33 which showed 100% protection, whereas the saline-treated group did not show any protection. It has been shown that castor oil causes a significant increase in intestinal fluid contents and promotes diarrhea through ricinoleic acid, the active constituent formed by hydrolysis of the oil components. Ultimately, it alters the electrolytes and water transport, eliciting massive contractions in transverse and distal segments of the colon. As such, any test material that exhibits inhibitory effects against castor oil–induced diarrhea is considered to possess marked antidiarrheal activity.34–36 M. subcordata appears to possess marked antidiarrheal effects, which could be due to the possible presence of gut-relaxant constituent(s). In line with our findings, Akuodor et al12 reported antidiarrheal effects of the methanol-leaf extract of a similar species, M. crassifolia, with a proposed mechanism of action linked partly to direct inhibitory effects on the propulsive movement of GI-tract smooth muscle.12
Further tests that were intended to explain the possible mechanism(s) interestingly show that the plant extract showed biphasic effects: at lower doses (0.01–0.1 mg/mL), the extract demonstrated a stimulant effect on the basal contractions of spontaneously contracting rabbit jejuna, followed by antispasmodic effect at higher doses (0.3–1 mg/mL). To understand the mechanism of spasmogenic effects observed at lower doses, the preparations were pretreated with atropine, an antimuscarinic drug,37 and the effect of the extract was reproduced. Interestingly, the stimulant effect of the extract at lower doses was abolished by atropine, implying the possible presence of components in the extract with an acetylcholine-like effect. Previous reports have shown that quaternary ammonium compounds, including tetramethylammonium (TMA), 3-hydroxyl-1,1-dimethylpyrrolidiniurn, glycinebetaine, proline betaine (stachydrine), proline betaine ethyl ester, 3-hydroxyprolinebetaine (3-hydroxy-stachydrine), choline, and feruloyl choline, were identified in different Maerua spp., including M. subcordata.38,39 Also, it was shown that acetylcholine, TMA, and related quaternary ammonium compounds acted on muscarinic receptors in the intestinal smooth muscle and that TMA exhibited a biphasic effect. Contractions caused by TMA in the presence of hyoscine have been suggested to be probably due to “rebound contractions”.40 Therefore, TMA and related compounds may contribute at least partly to the observed effect of MSL.Cr.
Likewise, to further understand the possible mechanism(s) of the antispasmodic effect observed at higher doses, contractions were induced in the jejunal preparations by different spasmogens. The plant extract showed similar potency for its inhibitory effect against CCh and low K+–induced contractions, thus showing PDE-inhibitory and K+-channel opening–like activities,41 whereas partial inhibition was seen against high K+–induced contractions, implying weak involvement of Ca2+-channel inhibition, as concentrations of K+ >30 mM, regarded as high K+, are known to cause smooth-muscle contractions through opening of voltage-dependent Ca2+ channels.36,41 On the other hand, verapamil, a standard CCB,41 inhibited spasms mediated by K+ at distinctly lower concentrations, as expected from typical CCBs.28 The inhibitory actions of the plant extract on the PDE enzyme was confirmed by the observation that pretreatment of jejunal tissue with the extract shifted the inhibitory CRCs of isoprenaline to the left, similarly to papaverine, a known inhibitor of PDE41 that produces spasmolytic effects through increased cAMP as a result of PDE inhibition,43,44 while verapamil did not affect the isoprenaline curves, as was expected from a standard Ca2+ antagonist.41
Since the plant extract was selectively more potent against low K+ (<30 mM), further experiments were conducted to know the nature of K+ channels. Interestingly, the plant extract’s inhibitory effect against low K+ was reversed in tissue pre-treated with TEA,an unselective antagonist of K+ channels,30 indicating the activation of aspecific K+-channels as additional antispasmodic activity, whereas no effect was observed in the presence of Gb, an ATP-dependent K+-channel opener.45 Indeed, it has been identified that K+-channel openers show a range of potential therapeutic uses, including GI spasms, asthma, hypertension, and urinary incontinence.46,47 These compounds open K+ channels and cause membrane hyperpolarization through the increase in K+ efflux, thus causing a decrease in intracellular free Ca2+, leading to smooth-muscle relaxation.30,48,49
The importance of the therapeutic potential of PDE inhibitors, K+-channel openers, and CCBs in diarrhea and hypermotility-related gut disorders have been reported by several researchers.33,46,47,50,51 However, mono-drug therapy with PDE inhibitors will have some limitations, as they are known to cause cardiac stimulation.52 The combination of K+-channel activation and weak CCBs with PDE inhibitor(s) in M. subcordata might offset the cardiac stimulation associated with PDE inhibitors, as both K+-channel openers and CCBs are cardiosuppressants.53
Conclusion
The findings of this study indicate that the crude extract of M. subcordata leaves possesses gut-stimulant, antidiarrheal, and antispasmodic activities, mediated possibly through a combination of cholinergic stimulations, PDE inhibition and activation of K+ channels, followed by a weak Ca2+-antagonist effect. M. subcordata leaves may be a potential therapeutic candidate for the management of dual-disease states of gut, eg, constipation and diarrhea, and hence further phytochemical and safety studies are suggested.
Abbreviations
ATP, adenosine triphosphate; cAMP, cyclic adenosine monophosphate; CCB, Ca2+-channel blocker; CCh, carbachol; CRCs, concentration–response curves; Gb, glibenclamide; TEA, tetraethylammonium; GI, gastrointestinal; MSL.Cr, crude extract of M. subcordata leaf; PDE, phosphodiesterase; TMA, tetramethylammonium.
Data-Sharing Statement
All data sets used and analyzed during this study will be available from the corresponding author on reasonable request.
Ethical Approval
The study was approved by the ethical review committee of Barrett Hodgson University (BR-ER/Pharmacy-001/2020/PI-Dr Amber Hanif Palla).
Acknowledgments
The authors are thankful to Barrett Hodgson University, Karachi, Pakistan and Mekelle University, Mekelle, Ethiopia for providing necessary facilities to carry out this research.
Author Contributions
MGH and GGS collected the plant material, prepared the extract, and did the acute-toxicity studies. AK helped in the extraction and transporting of samples from Ethiopia to Pakistan. AHP and NUR did the antidiarrheal tests and related experiments, data analysis, and description. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors do not have any conflicts of interest to disclose.
References
1. Occhipinti K, Smith JW. Irritable bowel syndrome: a review and update. Clin Colon Rectal Surg. 2012;25(01):046–052. doi:10.1055/s-0032-1301759
2. Annaházi A, Rók R, Rosztóczy A, et al. Role of antispasmodics in the treatment of irritable bowel syndrome. World J Gastroenterol. 2014;20(20):6031. doi:10.3748/wjg.v20.i20.6031
3. Rokaya MB, Uprety Y, Poudel RC, et al. Traditional uses of medicinal plants in gastrointestinal disorders in Nepal. J Ethnopharmacol. 2014;158:221–229. doi:10.1016/j.jep.2014.10.014
4. Gilani AH, Atta-ur-Rahman. Trends in Ethnopharmacology. J Ethnopharmacol. 2005;100:43–49. doi:10.1016/j.jep.2005.06.001
5. Patwardhan B, Ashok Vaidy DB, Chorghade M. Ayurveda and natural products drug discovery. Curr Sci. 2004;86(6):789–799.
6. Chhabra S, Mahunnah R, Mshiu E. Plants used in traditional medicine in Eastern Tanzania. II. Angiosperms (Capparidaceae to Ebenaceae). J Ethnopharmacol. 1989;25(3):339–359. doi:10.1016/0378-8741(89)90038-X
7. Mabogo DEN, van Wyk AE The Ethnobotany of the Vhavenda. Master’s Thesis, University of Pretoria, Pretoria–South Africa; 1990.
8. Magaji MG, Yaro AH, Maiha BB, et al. Preliminary gastrointestinal studies on aqueous methanolic stem bark extract of Maerua angolensis (CAPPARACEAE). Nigerian J Pharmaceut Sci. 2008;7(1):108–113.
9. Geissler PW, Harris SA, Prince RJ, et al. Medicinal plants used by Luo mothers and children in Bondo district, Kenya. J Ethnopharmacol. 2002;83:39–54. doi:10.1016/S0378-8741(02)00191-5
10. Diallo D, Hveem B, Mahmoud M, et al. An ethnobotanical survey of herbal drugs of Gourma District, Mali. Pharmaceut Biol. 1999;37(1):80–91. doi:10.1076/phbi.37.1.80.6313
11. Abouri M, El Mousadik A, Msanda F, et al. An ethnobotanical survey of medicinal plants used in the Tata Province, Morocco. Int J Med Plant Res. 2012;1(7):099–123.
12. Akuodor GC, Ibrahim JA, Akpan JL, et al. Phytochemical and Anti-diarrhoeal Properties of Methanolic Leaf Extract of Maerua crassifolia Forssk. Europ J Med Plants. 2014;4(10):1223–1231. doi:10.9734/EJMP/2014/11246
13. Heuzé V, Tran G, Delagarde R, Renaudeau D. Atil (Maerua crassifolia). Feedipedia, a programme by INRA, CIRAD, AFZ and FAO, 2015. 2015;14:32.
14. Agize M, Demissew S, Asfaw Z. Ethnobotany of medicinal plants in Loma and Gena bosa districts (woredas) of dawro zone, southern Ethiopia. Topclass J Herbal Med. 2013;2(9):194–212.
15. Andarge E, Shonga A, Agize M, et al. Utilization and conservation of medicinal plants and their associated indigenous knowledge (IK) in Dawuro Zone: an ethnobotanical approach. Int J Med Plant Res. 2015;4:330–337.
16. Teklehaymanot T, Giday M. Ethnobotanical study of wild edible plants of Kara and Kwego semi-pastoralist people in Lower Omo River Valley, Debub Omo Zone, SNNPR, Ethiopia. J Ethnobiol Ethnomed. 2010;6:23. doi:10.1186/1746-4269-6-23
17. Hassan-Abdallah A, Merito A, Hassan S, et al. Medicinal plants and their uses by the people in the Region of Randa, Djibouti. J Ethnopharmacol. 2013;148:701–713. doi:10.1016/j.jep.2013.05.033
18. Morgan AMA, Lim CH, Kim YH. Lignans, cyclolignans and neolignans from the leaves of Boscia senegalensis (Pers.) Lam. ex Poir. Biochem Systematics Ecol. 2015;59:226–228. doi:10.1016/j.bse.2015.01.020
19. Hiben MG, Louisse J, de Haan LHJ, et al. Ethnomedicine and ethnobotany of Maerua subcordata (Gilg) DeWolf. J Ethnic Foods. 2019a;6:23. doi:10.1186/s42779-019-0032-4
20. Rehman N, Khan A, Fatima U, et al. Presence of laxative and antidiarrheal activities in Periploca aphylla: a Saudi medicinal plant. Int J Pharmacol. 2013;9:190–196. doi:10.3923/ijp.2013.190.196
21. NRC (National Research Council). Guide for the Care and Use of Laboratory Animals. Washington: National Academy Press; 1996:1–7.
22. NRC (National Research Council). Guide for the Care and Use of Laboratory Animals. National Academies Press; 2010.
23. Albus U. Guide for the Care and Use of Laboratory Animals.
24. OECD/OCDE. OECD Guideline for the Testing of Chemicals. Acute Oral Toxicity; Up-And-Down Procedure (UDP). Paris, France: OECD; 2008.
25. Khan M, Khan A, Gilani AH. Pharmacological basis for the medicinal use of Morus alba in gut and airways disorders. Bangladesh J Pharmacol. 2012;7(4):289–298. doi:10.3329/bjp.v7i4.12873
26. Mandukhail S, Ahmed AF, Al-Yousef HM, et al. The mechanism underlying the spasmolytic and bronchodilatory activities of the flavonoid-rich red onion” Allium cepa L.” Peel extract. Int J Pharmacol. 2014;10(2):82–89. doi:10.3923/ijp.2014.82.89
27. Farre AJ, Colombo M, Fort M, et al. Differential effects of various Ca2+ antagonists. Gen Pharmacol. 1991;22(1):177–181. doi:10.1016/0306-3623(91)90331-Y
28. Godfraind T, Miller R, Wibo M. Calcium antagonism and calcium entry blockade. Pharmacol Rev. 1986;38:321–416.
29. Lorenz KL, Wells J. Potentiation of the effects of sodium nitroprusside and of isoproterenol by selective phosphodiesterase inhibitors. Mol Pharmacol. 1983;23(2):424–430.
30. Cook NS. The pharmacology of potassium channels and their therapeutic potential. Trends in Pharmacol Sci. 1989;9(1):21–28. doi:10.1016/0165-6147(88)90238-6
31. Etkin NL, Ross PJ. Food as Medicine and Medicine as Food. An adaptive framework for the interpretation of plant utilization Among the Hausa of Northern Nigeria. Soc Sci Med. 1982;16:1559–1573. doi:10.1016/0277-9536(82)90167-8
32. Waterman C, Smith RA, Pontiggia L, et al. Anthelmintic screening of Sub-Saharan African plants used in traditional medicine. J Ethnopharmacol. 2010;127(3):755–759. doi:10.1016/j.jep.2009.11.025
33. Reynolds I, Gould RJ, Snyder SH. Loperamide: blockade of calcium channels as a mechanism for antidiarrheal effects. J Pharmacol Exper Ther. 1984;231(3):628–632.
34. Iwao I, Terada Y. On the mechanism of diarrhoea due to castor oil. Jap J Pharmacol. 1962;12:137–145. doi:10.1254/jjp.12.137
35. Croci T, Landi M, Elmonds-Alt X, et al. Role of tachykinins in castor oil-induced diarrhea in rats. Br J Pharmacol. 1997;121:375–380. doi:10.1038/sj.bjp.0701130
36. Ali MZ, Janbaz KH, Mehmood MH, et al. Antidiarrheal and antispasmodic effects of Polygonum bistorta rhizomes are mediated predominantly through K+ channels activation. Bangladesh J Pharmacol. 2015;10:627–634. doi:10.3329/bjp.v10i3.23714
37. Gilani AH, Shaheen F, Christopoulos A, et al. Interaction of ebeinone, an alkaloid from Fritillaria imperialis, at two muscarinic acetylcholine receptor subtypes. Life Sci. 1997;60:535–544. doi:10.1016/S0024-3205(96)00691-1
38. McLean WFH, Blunden G, Jewers K. Quatenary ammonium compounds in the Capparaceae. Biochem Systematics Ecol. 1996;24(5):427–434. doi:10.1016/0305-1978(96)00044-0
39. Hiben MG, de Haan L, Spenkelink B, et al. Effects of Maerua subcordata (Gilg) DeWolf on electrophile-responsive element (EpRE)-mediated gene expression in vitro. PLoS One. 2019;14(4):e0215155. doi:10.1371/journal.pone.0215155
40. Hobbiger F, Mitchelson F, Rand MJ. The actions of some cholinomimetic drugs on the isolated taenia of the guinea-pig caecum. Br J Pharmacol. 1969;36:53–69. doi:10.1111/j.1476-5381.1969.tb08303.x
41. Fleckenstein A. Specific pharmacology of calcium in myocardium, cardiac pacemakers, and vascular smooth muscle. Ann Rev Pharmacol. 1977;17:149–166. doi:10.1146/annurev.pa.17.040177.001053
42. Rang H, Dale M, Ritter J, et al. Textbook of Pharmacology. UK: Churchill Livingstone; 1999:199–242.
43. Kaneda T, Takeuchi Y, Matsu H, et al. Inhibitory mechanism of papaverine on carbachol-induced contraction in bovine trachea. J Pharmacol Sci. 2005;98:275–282. doi:10.1254/jphs.FPJ05013X
44. Takayanagi I, Uchida M, Inatomi N, et al. Intracellular cyclic adenosine 3,5-monophosphate and relaxing effects of isoprenaline and papaverine on smooth muscle of intestine. Jap J Pharmacol. 1972;22:869–871. doi:10.1254/jjp.22.869
45. Frank H, Puschmann A, Schusdziarra V, et al. Functional evidence for a glibenclamide-sensitive K+ channel in rat ileal smooth muscle. Europ J Pharmacol. 1994;271:379–386. doi:10.1016/0014-2999(94)90797-8
46. Empfield JR, Russell K, Trainor DA. Potassium channel openers: therapeutic possibilities. Pharmaceut News. 1995;6:23–27.
47. Mannhold R. K+ ATP channel openers: structure-activity relationships and therapeutic potential. Med Res Rev. 2004;24:213–266. doi:10.1002/med.10060
48. Quast U. Potassium channel openers: pharmacological and clinical aspects. Fundam Clin Pharmacol. 1992;6(7):279–293. doi:10.1111/j.1472-8206.1992.tb00122.x
49. Lenz T, Wagner G. Potential Role of Potassium Channel Openers for the Treatment of Cardiovascular Disease. New York: Raven Press; 1995.
50. Findling R, Frishman W, Javed MT, et al. Calcium channel blockers and the gastrointestinal tract. Am J Ther. 1996;3:383–408. doi:10.1097/00045391-199605000-00009
51. Schwarz ER, Kapur V, Rodriguez J, et al. The effects of chronic phosphodiesterase-5 inhibitor use on different organ systems. Int J Impot Res. 2007;19:139–148. doi:10.1038/sj.ijir.3901491
52. Nawrath H. Action potential, membrane currents and force of contraction in cat ventricular heart muscle treated with papaverine. J Pharmacol Exper Therapeut. 1981;218(2):544–549.
53. Billman GE. The antiarrhythmic and antifibrillatory effects of calcium antagonists. J Cardiovas Pharmacol. 1991;18:S107–117. doi:10.1097/00005344-199118101-00019
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.