Back to Journals » International Medical Case Reports Journal » Volume 14
Multiple Approaches for Managing Complex Ophthalmic Blunt Trauma: A Case Report
Authors Irawati Y ![]() , Soedarman S, Arianti A, Widyasari A, Reksodiputro MH
, Soedarman S, Arianti A, Widyasari A, Reksodiputro MH
Received 28 January 2021
Accepted for publication 12 March 2021
Published 31 March 2021 Volume 2021:14 Pages 205—210
DOI https://doi.org/10.2147/IMCRJ.S304193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yunia Irawati,1,2 Soefiandi Soedarman,3 Alia Arianti,4 Amira Widyasari,5 Mirta Hediyati Reksodiputro6
1Division of Plastic and Reconstructive Surgery, Department of Ophthalmology, Dr. Cipto Mangunkusumo Hospital, Faculty of Medicine, University of Indonesia, Jakarta, Indonesia; 2Orbital and Oculoplastic Service, JEC Eye Hospitals and Clinics, Jakarta, Indonesia; 3Vitreo-Retina Service, JEC Eye Hospitals and Clinics, Jakarta, Indonesia; 4Neuro-Ophthalmology Service, JEC Eye Hospitals and Clinics, Jakarta, Indonesia; 5Research, JEC Eye Hospitals and Clinics, Jakarta, Indonesia; 6Division of Plastic Reconstruction, Department of Ear, Nose and Throat, Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Correspondence: Yunia Irawati
Division of Plastic and Reconstructive Surgery, Department of Ophthalmology, Dr. Cipto Mangunkusumo Hospital, Faculty of Medicine, University of Indonesia, Jalan Kimia No. 8, Jakarta, 10430, Indonesia
Tel +62 816789595
Fax +62 2131934878
Email [email protected]
Introduction: Ophthalmic trauma is defined as injuries affecting the ocular structures, including the globe, eyelid, lacrimal system, and surrounding orbital walls. Blunt trauma acts as the leading cause of injury and it may affect both the anterior and posterior parts of the globe. Prompt diagnosis, early management, and sustained follow-up are mandatory for an optimal outcome.
Purpose: This report presents a one-step surgery management process for an intricate case of blunt facial trauma with complex ophthalmic and nasal injury.
Patients and Methods: A 45-year-old male with blunt force trauma of the left eye from a wooden block, suffered from naso-orbital-ethmoidal fractures, eyelid laceration with canalicular, close-globe injuries of traumatic cataract and vitreous hemorrhage with retinal detachment. A simultaneous one-step surgery was performed by a trauma team of ophthalmological and ENT surgeons during the height of the COVID-19 pandemic to lessen the risk of cross-transmission. After ruling out the possibility of open-globe rupture, traumatic cataract extraction, retinal detachment surgery, the repair of an eyelid laceration with canalicular involvement, and septorhinoplasty were performed on concomitantly.
Results: Anatomical success was achieved for the repair of the nasoorbitoethmoidal (NOE) type II fracture and close-globe injuries, including the anatomical reattachment of the retina. However, the functional outcome remained unsatisfactory. Visual acuity failed to show further improvement at a later follow-up. Traumatic optic neuropathy was, at the final follow-up, considered to be the cause of the suboptimal visual acuity.
Conclusion: A single-step multi-procedure for a complex ophthalmic blunt trauma, as demonstrated in this case, may be beneficial for reducing the complications that might arise due to treatment delay. The complex nature of the injury, however, creates the higher possibility for residual post-operative complications. Risks of residual functional impairment should be considered in such complex trauma prior to surgery, to determine the surgical prognostic value and provide appropriate consent to the patient.
Keywords: facial injury, ocular trauma, blunt trauma, closed-globe injury, nasal fracture, canalicular laceration
Introduction
Ocular trauma remains one of the leading causes of visual disability and blindness worldwide.1 The term “ophthalmic trauma” is widely employed nowadays since it represents all traumas of the globe and periocular area, including the eyelid, lacrimal system, and orbital wall. From an estimated incidence of 2.0 to 2.4 million cases worldwide, traumatic ocular injuries have been reported to account for almost 1 million cases of permanent visual loss.2
Closed-globe blunt trauma, according to the Birmingham Eye Trauma Terminology System (BETTS), may cause various forms of structural and functional damage in both the anterior and posterior orbital segments. Damage that occurs in the structures of the posterior segment might be more complex, involving vital structures such as the retina and optic nerve, with greater risks of significant, permanent visual loss.3 The signs and symptoms displayed by patients may vary, sitting on a large spectrum that ranges from asymptomatic patients to those with various ophthalmological problems, such as swelling, eye pain, bleeding, visual acuity loss, glaucoma, diplopia, and even permanent blindness. The prognosis of ocular blunt trauma depends largely on the original injury, with timely and optimal management reduces the risks of further complications.4 The aim of this study is to present a one-step surgical management process for an intricate blunt facial trauma with complex ophthalmic and nasal injury.
Patients and Methods
A 45-year-old man suffered an occupational injury of a blunt force trauma to the left eye from a wooden block. The patient presented with upper and lower eyelid lacerations and decrease visual acuity. No significant past medical history was present. Following the incident, the patient was immediately brought to the emergency department of a local hospital and treated for emergency eyelid repair. Three days after the initial injury, the patient was referred to our hospital for further management. The visual acuity of the injured eye was light perception with intraocular pressure of 12 mmHg. Detailed examination of the eyelid area revealed multiple prolene sutures with poor wound apposition of the eyelid, canalicular laceration on both the superior and inferior eyelids, and medial canthal rupture (Figure 1). Further ophthalmological examination showed subconjunctival bleeding, hyphema and traumatic cataract. The pupil was mid-dilated and non-reactive to light, with no view of the posterior segment (Figure 2). Ultrasound examination of the posterior segment detected the presence of vitreous opacities and retinal detachment (Figure 3). The right eye examination was within normal limits. Detailed ENT examination found crepitation, bilateral epistaxis, mildly depressed nasal dorsum and deviated septum, visible septal hematoma, open nasal laceration, nasal ecchymosis, significant dorsal asymmetry, and severe swelling with ecchymosis of the periorbital area. An orbital CT scan with three-dimensional reconstruction showed nasoorbitoethmoidal (NOE) type II fracture and nasal septum deviation (Figure 4).
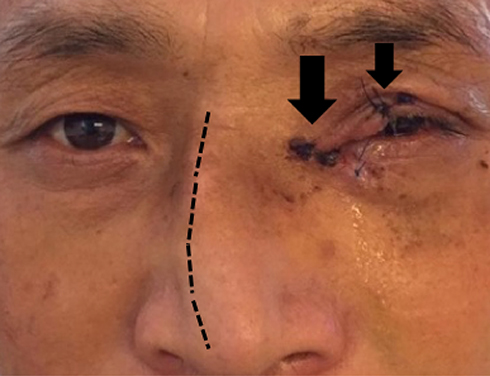 |
Figure 1 Patient with multiple sutures on his eyelid, canalicular laceration (arrows) and nasal septum deviation (dotted-line). |
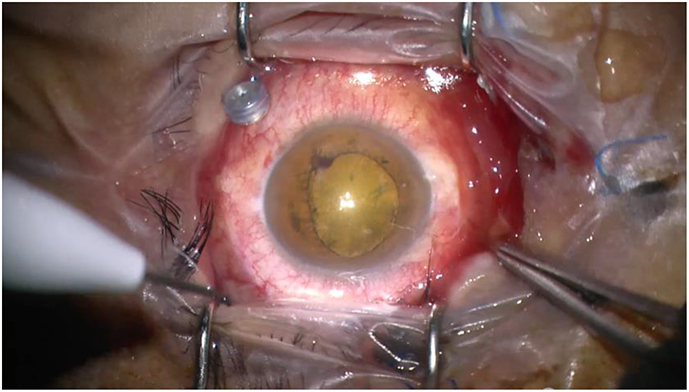 |
Figure 2 Intraoperative view of the anterior segment showing the dense traumatic cataract. |
 |
Figure 3 Retinal detachment shown in the ultrasound examination. |
 |
Figure 4 CT scan images showed presence of NOE type II fracture and deviated nasal septum. |
After ruling out the possibility of open-globe rupture: absence of chemosis (conjunctival edema and subconjunctival bleeding), ocular movement limitation, and ocular hypotony, the patient was then hospitalized for surgical preparation. The patient was then hospitalized for surgical preparation. The incidence occurred during the height of the COVID-19 pandemic in Indonesia; therefore, extra tests were carried out prior to the surgery, including screening for COVID-19 infection using nasopharyngeal and oropharyngeal PCR swab test. A further decision was made to complete the repair in a one-step strategy, to reduce the number of hospitalization and manipulation of the airway for intubation during general anesthesia, therefore minimizing the risk of COVID-19 cross-infection. The sequence of the one-step surgery carried out by ophthalmologists and ENT surgeons was as follows: (1) exploration of possible open-globe rupture, (2) phacoemulsification with intraocular lens implantation for the traumatic cataract, followed by (3) vitrectomy with 23G and silicone oil tamponade for the vitreous hemorrhage and retinal detachment, (4) eyelid and canalicular rupture repair with silicone insertion and medial canthal reconstruction, and finally (5) septorhinoplasty procedure.
Results
One week after the surgery, visual acuity improved to 0.05 with impaired color vision, with the patient failed to identify any of the Ishihara plate (0/17). Anterior segment examination revealed symmetrical eyelids with good wound apposition and silicone tube in place, absence of intraocular inflammatory signs, a fixed-dilated pupil with no light reaction, and decreased consensual reflex of the right eye. The posterior segment of the left eye showed a normal appearance of the optic nerve head with a cup-disc ratio of 0.2, an anatomically attached retina and no obvious structural damage (Figure 5A and B). The nasal splint was taken off at week two post-surgery with no signs of nasal obstruction, passable airway flow and normal breathing of the patient. The nose was symmetrical with good nasal and tip projection and no septal deviation or narrowing of the internal nasal valve.
 |
Figure 5 (A) Post-operative follow-up showed good optic disc appearance with pink rim, distinct edge and CDR od 0.2. (B) Anatomical attachment of the retina was achieved. |
The lack of visual acuity improvement persisted in this patient until the final follow-up, which then raised the possibility of traumatic optic neuropathy (TON) as the culprit. Visual loss with no significant damage to the anterior and posterior segments, impaired color vision and decreased consensual reflex of the fellow eye might be consistent with clinical signs of traumatic optic neuropathy. Further visual pathway function assessment including visual field test, and electrophysiology tests were planned. Pulse steroid therapy was also considered for this patient.
Discussion
Orbital blunt trauma may cause variable complications, depending on the severity and mechanism of the initial injury. Management of orbital trauma should be performed accordingly to the extent and location of the injury. Intraocular trauma, especially in the presence of open-globe injuries, should always be managed first. Sight-saving procedures must always be prioritized in the setting of ocular trauma management. Surgical repairs of the periocular structures, including eyelid lacerations and orbital wall fractures, could be performed at a later time. This case presentation highlights the one-step surgery strategy to manage orbital blunt-force trauma injury involving multiple structures of the globe and orbit, in order to achieve optimum results in a timely fashion.
For the intraocular injuries, immediately after ruling out the possibility of open-globe injuries, the patient underwent combined cataract extraction and vitrectomy with silicone oil tamponade surgery. The one-week post-operative visual acuity of the patient was 0.05, improving from the pre-operative status of light perception.
Among the most common potential complications of orbital blunt trauma is visual impairment, the causes of which may vary, with traumatic cataract serves as common sequela, as was the case for this patient.5 Sharma et al6 reported that 45.8% of the patients with blunt ocular trauma injury presented with a traumatic cataract. Poonam et al7 reported phacoemulsification with PCIOL as an important modality for the treatment of traumatic cataract.
The decision to perform early vitrectomy surgery combined with cataract extraction was made to help retain the patient’s sight, supported by several publications. Guo et al8 reported that early vitreous surgery can improve the curative effect for a vitreous hemorrhage caused by a blunt ocular trauma. Yang et al9 reported that early vitrectomy, when combined with silicone oil tamponade, helps achieve better retinal reattachment of the remaining retina, which may give a better chance for the severely traumatized eyes to regain visual acuity of at least light perception, or better. Mathews et al10 also reported that the significant predictive factors for the final visual outcome of patients with a traumatic retinal detachment were the pre-operative visual acuity of “hand motions or better” and a close globe injury. Hui et al11 reported that a vitrectomy combined with IOL implantation in one operation could be a safe, fast, and effective means of visual recovery for selected patients with complicated ocular traumas.
After the intraocular procedures, the next step was to proceed to the eyelid and canalicular laceration repairs. For the eyelid canalicular laceration, a modified bicanalicular intubation (MBCI) procedure using a silicone tube insertion was performed, followed by medial canthal reconstruction. This modified bicanalicular intubation method has recently been proven to be an effective, atraumatic procedure for managing canalicular lacerations with fewer complications compared to the traditional procedure.12 In patients with combined upper and lower canalicular lacerations, as was the case in this patient, the Crawford stent is the preferred type of bicanalicular stent that can be appropriately utilized for the intervention. In a previous study, the MBCI was found to be an effective technique with an anatomical success rate of 97.14%.13 The result for our patient was also satisfactory: post-surgical symmetrical eyelids with no complications.
Periorbital involvement in orbital trauma, such as NOE fracture, should be suspected in the presence of external deformity, palpation of fragments, bone instability, and crackling. Nasal fracture is often accompanied by signs of epistaxis, nasal swelling, symptoms of nasal obstruction, and local pain, as was seen in this patient.14 According to the Markowitz and Manson classification system, this patient could be categorized as an NOE, type II fracture.15 This diagnosis was supported by orbital CT scan imaging.
A closed reduction with digital manipulation for the management of nasal fractures in this patient was performed after completing the intraocular and eyelid surgeries as the final step of the repair. This procedure is safer during this Covid-19 pandemic situation. Walsham’s nasal reduction forceps and Asch’s septal forceps were utilized to manipulate the nasal bone and frontal processes of the maxillae and septum, respectively. Nasal fracture management can be manipulated through “closed” or “open” surgical procedures with open formal incisions, while the management of the nasal bones and septum can be arranged through conventional septorhinoplasty. The closed path is indicated for unilateral and bilateral fractures with deviations of less than half the depth of the nasal tip.16 The open approach is usually reserved for cases of residual cosmetic deformity and complex or comminuted fractures.14
In this case, the satisfactory anatomical surgical outcome did not go in accordance with the functional outcome. Although the retina was successfully reattached, the visual outcome remained unsatisfactory, with visual acuity of only 0.05 on follow-ups. Better visual outcome was reported by Sharma et al6 in blunt trauma cases, due to better capsular bag support of the intraocular lens and lower number of postoperative complications. The discordant findings, in this case, may be caused by other culprits. The cause of the persistent visual loss, in this case, was difficult to elaborate on precisely. A coexisting traumatic optic neuropathy, global retinal dysfunction, or post-traumatic retinal detachment, especially considering the several-days window before surgical intervention, should be considered as the cause of the suboptimal final visual acuity in this patient.
The diagnosis of traumatic optic neuropathy, or TON, for this patient, however, remained problematic. Persistent visual loss with a fixed dilated pupil and decreased consensual reflex of the fellow eye might clinically have been caused by TON. However, in the presence of global retinal dysfunction, the relative afferent pupillary defect (RAPD) of the involved eye or a decreased consensual reflex of the fellow eye may also have occurred. Several other diagnostic modalities might have helped to predict the presence of TON such as a CT scan, diffusor tensor imaging (DTI) MRI, or the use of visual electrophysiology comprising electroretinography (ERG) and visual evoked potential.17 However, these are mere suggestions as, in our case, the patient was lost to follow-up.
Conclusion
In conclusion, a single-step multi-procedure approach might be beneficial for patients with complex ophthalmic trauma, as it lessens the waiting time for subsequent procedures, therefore minimizing the complications that may arise from delayed treatment. Also, in the situation of the COVID-19 pandemic, it could also reduce the likelihood of cross-transmission from repeated hospitalization. The failure of optimal visual acuity recovery, despite the anatomical success, reminds us of the possibility of optic nerve complications of blunt trauma, such as traumatic optic neuropathy, the risks of which should be presented to the patient prior to surgical intervention, especially in complex cases.
Abbreviations
BETTS, Birmingham eye trauma terminology system; NOE, nasoorbitoethmoidal; TON, traumatic optic neuropathy.
Ethics and Consent Statement
Written informed consent was obtained from the patient for publication of these case reports and any accompanying images. The patient understands that their names and initials will not be published and due efforts will be made to conceal their identity. Institutional approval was required to publish the case details, and this case report has obtained a publish permit from our institution.
Acknowledgment
The authors thank the Directors and all staff of JEC Eye Hospitals and Clinics for providing the patients’ medical records.
Funding
The authors declare that there is no source of funding in this report.
Disclosure
The authors report no conflicts of interest nor competing interest in this work.
References
1. Odebode T, Ademola-Popoola D, Ojo T, Ayanniyi A. Ocular and visual complications of head injury. Eye. 2004;19(5):561–566. doi:10.1038/sj.eye.6701566
2. Ahn S, Woo S, Park K, Lee B. Retinal pigment epithelium sequelae caused by blunt ocular trauma: incidence, visual outcome, and associated factors. Sci Rep. 2017;7(1). doi:10.1038/s41598-017-14659-4
3. Kuhn F, Morris R, Witherspoon C. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15(2):139–143. doi:10.1016/S0896-1549(02)00004-4
4. Sukati V. Ocular injuries - a review. African Vision Eye Health. 2012;71(2). doi:10.4102/aveh.v71i2.73
5. Iftikhar M, Latif A, Farid U, Usmani B, Canner J, Shah S. Changes in the incidence of eye trauma hospitalizations in the united states from 2001 through 2014. JAMA Ophthalmol. 2019;137(1):48. doi:10.1001/jamaophthalmol.2018.4685
6. Sharma A. Visual outcome of traumatic cataract at a tertiary eye care centre in north india: a prospective study. J Clin Diagnostic Res. 2016;10(1):5–8.
7. Poonam N. Kalyanpad, Chhaya A. Shinde. Traumatic cataract: different modalities of treatments and its outcome. Med Pulse Int Med J. 2014;1:217–218.
8. Guo XR, Guo GY, Tian QF, Dong YL, Zhao ZX, Huang AG. The surgical timing and effects for vitreous haemorrhage caused by ocular blunt trauma. Zhonghua Yan Ka Za Zhi. 2003;39(7):419–421.
9. Yang SS, Jiang T. Vitrectomy combined with silicone oil tamponade in the treatment of severely traumatized eyes with the visual acuity of no light perception. Int J Ophthalmol. 2013;6(2):198–201. doi:10.3980/j.issn.2222-3959.2013.02.18
10. Mathews GP, Das A, Brown S. Visual outcome and ocular survival in patients with retinal detachments secondary to open or closed globe injuries. Ophthalmic Surg Lasers. 1998;29(1):48–54.
11. Hui Y, Huang W, Wang L, Cao X. Vitrectomy combined with intraocular lens implantation for 103 selected cases of complicated ocular trauma. Yan Ke Xue Bao. 2000;16(2):109–111.
12. Raj A, Thakur S, Arya K, Kesarwani P, Sinha U. Canalicular lacerations in a tertiary eye hospital: our experience with monocanalicular stents. Romanian j Ophthalmol. 2020;64(2):146–152. doi:10.22336/rjo.2020.26
13. Liang X, Lin Y, Wang Z, et al. A modified bicanalicular intubation procedure to repair canalicular lacerations using silicone tubes. Eye. 2012;26(12):1542–1547. doi:10.1038/eye.2012.212
14. Granjeiro R, Maurício C, Andrade P, Vilela F. Applicability and effectiveness of closed reduction of nasal fractures under local anesthesia. Int Arch Otorhinolaryngol. 2014;18(3):266–271. doi:10.1055/s-0034-1368138
15. Gómez Roselló E, Quiles Granado A, Artajona Garcia M, et al. Facial fractures: classification and highlights for a useful report. Insights Imaging. 2020;11(1). doi:10.1186/s13244-020-00847-w
16. Murray JAM, Maran AGD. The treatment of nasal injuries by manipulation. J Laryngol Otol. 1980;94(12):1405–1410. doi:10.1017/S0022215100090241
17. Bodanapally UK, Shanmuganathan K, Shin RK, et al. Hyperintense optic nerve DWI in TON. Am J Neuroradiol. 2015;36:1536–1541. doi:10.3174/ajnr.A4290
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.