Back to Journals » International Medical Case Reports Journal » Volume 19
Multimodal Imaging Evaluation of Non-Dilated Left Ventricular Cardiomyopathy: The Importance of Cardiac Magnetic Resonance Imaging
Received 24 January 2026
Accepted for publication 27 March 2026
Published 7 April 2026 Volume 2026:19 594841
DOI https://doi.org/10.2147/IMCRJ.S594841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Chunlong Yan, Lei Xu
Department of Radiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart Lung and Blood Vessel Diseases, Beijing, People’s Republic of China
Correspondence: Lei Xu, Department of Radiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart Lung and Blood Vessel Diseases, Beijing, People’s Republic of China, Email [email protected]
Introduction: Non-dilated left ventricular cardiomyopathy was first proposed by the European Society of Cardiology in 2023, and imaging evaluation research on this cardiomyopathy remains insufficient.
Case Report: We report a case of a 68-year-old female patient who experienced chest tightness and shortness of breath six months ago. Electrocardiogram revealed sinus bradycardia with a ventricular rate of 54 beats per minute. Coronary angiography showed generally normal results, while echocardiography indicated a reduced left ventricular ejection fraction. Cardiac magnetic resonance imaging revealed mildly impaired left ventricular function (LVEF 47.4%), with focal mid-myocardial fibrosis in the basal anterior, septal, and inferior walls of the left ventricle, meeting the diagnostic criteria for non-dilated left ventricular cardiomyopathy. According to ESC guidelines, the patient is currently under follow-up observation.
Conclusion: The imaging diagnosis of non-dilated left ventricular cardiomyopathy requires a comprehensive multimodal imaging approach. Cardiac magnetic resonance plays a crucial clinical role in the multimodal imaging evaluation of NDLVC.
Keywords: nondilated left ventricular cardiomyopathy, cardiac magnetic resonance, echocardiography, dilated cardiomyopathy, left ventricular function
Introduction
In 2023, the European Society of Cardiology (ESC) Cardiomyopathies Working Group published the 2023 ESC Guidelines for the management of cardiomyopathy. These guidelines introduced a novel phenotypic classification and definition of cardiomyopathies based on cardiac structure, function, and histological features. Notably, the phenotype of non-dilated left ventricular cardiomyopathy (NDLVC) was proposed for the first time.1 This new entity encompasses patients with non-ischemic myocardial scarring or fatty infiltration in the absence of left ventricular dilation, often representing an early or subtle manifestation of an underlying cardiomyopathy. Currently, clinical studies on NDLVC remain limited, and its clinical significance lies in the fact that affected patients may be at increased risk of life-threatening ventricular arrhythmias, even before significant systolic dysfunction or ventricular remodeling becomes apparent.2–4 Therefore, early identification, accurate diagnosis, and optimized treatment are highly significant in clinical practice, as they enable timely risk stratification and potential intervention to prevent adverse outcomes, as illustrated in the case presented below.
Case Presentation
Written informed consent for publication of their details was obtained from the patient. A 68-year-old female presented with paroxysmal chest tightness and shortness of breath for six months. On examination, the lungs were clear to percussion with normal breath sounds, and no dry or wet rales or pleural friction rubs were detected. There was no abnormal precordial bulge, the apical impulse was normal, and no thrills were palpable. The cardiac dullness border was normal, with a heart rate of 66 beats per minute and a regular rhythm. No pathological murmurs were heard over any valve areas, and no pericardial friction rub was present. The abdomen was flat without abdominal wall varicose veins, soft, and without tenderness, rebound tenderness, or palpable masses. No edema was observed in the lower extremities. Publication of the case details was approved by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University.
Electrocardiogram (ECG) revealed sinus bradycardia with a ventricular rate of 54 beats per minute (Figure 1). Laboratory findings revealed an elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) level of 330.01 pg/mL (reference range: 0–312.85 pg/mL). Echocardiography indicated mildly reduced global left ventricular wall motion and impaired left ventricular function (LVEF) 43% (Figure 2). Cardiac magnetic resonance (CMR) further demonstrated normal cardiac architecture (Figure 3A–C), albeit with mildly impaired left ventricular function (LVEF 47.4%) and focal mid-myocardial fibrosis in the basal anterior wall, interventricular septum, and inferior wall of the left ventricle (Figure 3D–F). Coronary angiography performed at an external hospital showed no significant stenosis, suggesting a non-ischemic cardiomyopathy. The findings were consistent with the diagnostic criteria for NDLVC.
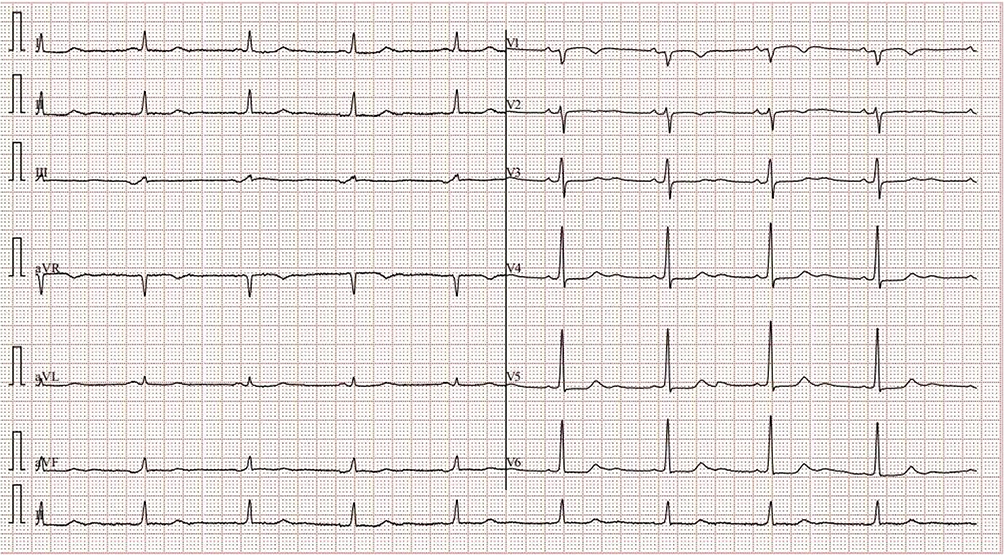 |
Figure 1 Electrocardiogram of a 68-year-old female patient with NDLVC. Abbreviation: NDLVC, non-dilated left ventricular cardiomyopathy. |
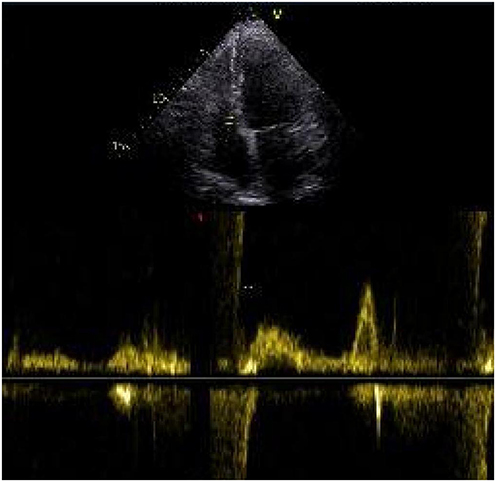 |
Figure 2 Echocardiogram of a 68-year-old female patient with NDLVC. Abbreviation: NDLVC, non-dilated left ventricular cardiomyopathy. |
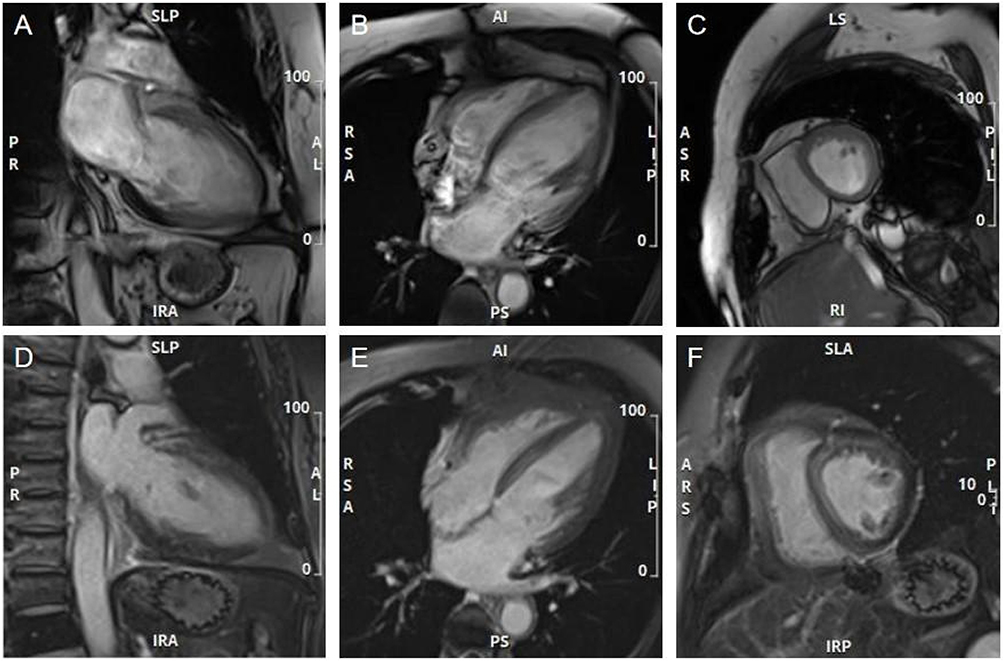 |
Figure 3 Cardiac magnetic resonance imaging of a 68-year-old female patient with NDLVC. Two-chamber cine image (A); four-chamber cine image (B); short-axis cine image (C); LGE two-chamber image (D); LGE four-chamber image (E); LGE short-axis image (F). Abbreviations: NDLVC, non-dilated left ventricular cardiomyopathy; LGE, late gadolinium enhancement. |
Discussion
In 2023, the ESC Working Group on Myocardial Diseases released the 2023 ESC Guidelines for the Management of Cardiomyopathies, introducing for the first time the phenotypic classification of NDLVC. NDLVC is defined by non-ischemic scarring or fatty replacement (with or without global/regional wall motion abnormalities) in structurally normal myocardium, or isolated left ventricular hypokinesis without fibrosis. It underscores the crucial value of NDLVC phenotyping, genetic testing, and CMR imaging in cardiomyopathy diagnosis and risk stratification.5,6 This advancement facilitates more accurate identification and diagnosis of distinct cardiomyopathy subtypes, thereby providing more precise guidance for clinical management.7
Currently, CMR imaging offers comprehensive evaluation of cardiac structure, function, and myocardial tissue characteristics—including fibrosis and fatty infiltration—through a “one-stop” approach, demonstrating high clinical utility.8,9 Some researchers have investigated the clinical profiles and prognoses of NDLVC patients with reduced LVEF compared to dilated cardiomyopathy (DCM) patients. The study found that both groups require equal emphasis on follow-up and regular LV function assessment.10 Emerging evidence from clinical studies indicates that mid-myocardial delayed enhancement has been identified as a key predictor of major adverse arrhythmic events.11 This finding reinforces the central role of CMR in risk stratification and provides an objective basis for clinical decision-making.
In this case, the patient presented with paroxysmal chest tightness and shortness of breath for six months. While CMR provided the definitive diagnostic information—particularly the detection of focal mid-myocardial fibrosis that is pathognomonic for the underlying cardiomyopathy—the initial echocardiogram played an essential role in the diagnostic pathway. Echocardiography first identified the mildly reduced global left ventricular wall motion and impaired LVEF (43%), which prompted the clinical suspicion of myocardial pathology and justified the decision to pursue CMR for tissue characterization. However, this case also illustrates a key limitation of echocardiography in the evaluation of NDLVC: despite its utility in assessing global and regional systolic function, echocardiography was unable to detect the subtle mid-myocardial fibrosis subsequently revealed by CMR. This limitation stems from echocardiography’s lower spatial resolution and inability to perform tissue characterization (eg, late gadolinium enhancement) Thus, a truly multimodal approach involves recognizing that echocardiography serves as an effective screening and functional assessment tool, while CMR is essential for definitive tissue characterization and diagnosis. The integration of both modalities—each with its distinct strengths—was critical in establishing the final diagnosis of NDLVC in this patient. Additionally, an important consideration in this case is the relationship between NDLVC and arrhythmogenic left ventricular cardiomyopathy (ALVC). According to the 2023 ESC Guidelines, the NDLVC phenotype is an umbrella term that includes ALVC as one of its constituent entities. ALVC is characterized by predominant left ventricular involvement with subepicardial or mid-myocardial fibrosis and a propensity for ventricular arrhythmias. In our patient, CMR demonstrated focal mid-myocardial fibrosis in the basal anterior wall, interventricular septum, and inferior wall—findings that are entirely consistent with the NDLVC phenotype and, more specifically, could represent a form of ALVC. However, in the absence of desmosomal gene mutations or a family history of arrhythmogenic cardiomyopathy, we have classified this case under the broader NDLVC designation. This case illustrates the phenotypic spectrum captured by the NDLVC classification and highlights the importance of comprehensive evaluation—including family history and, where available, genetic testing—to further refine the diagnosis within this heterogeneous category.
Differential Diagnoses: Given the presentation of non-ischemic myocardial fibrosis with mildly reduced systolic function in the absence of ventricular dilation, several alternative etiologies were systematically considered and excluded. ① Ischemic cardiomyopathy was ruled out by the absence of significant coronary stenosis on angiography and the mid-myocardial (rather than subendocardial) pattern of late gadolinium enhancement (LGE) on CMR. ② DCM was excluded as left ventricular dimensions were within normal limits, consistent with the 2023 ESC definition of NDLVC. The presence of mid-myocardial fibrosis without dilation further supports NDLVC over early DCM. ③ Prior myocarditis was considered unlikely due to: (1) no clinical history of viral prodrome or chest pain; (2) mid-myocardial fibrosis lacking the subepicardial or patchy distribution typical of post-inflammatory scarring; and (3) no elevated troponin or inflammatory markers. ④ Inflammatory cardiomyopathy (eg, cardiac sarcoidosis) was excluded based on: (1) no extracardiac manifestations; (2) normal ACE/lysozyme and no hypercalcemia; (3) focal mid-myocardial fibrosis without nodular or multifocal LGE; and (4) no conduction abnormalities beyond sinus bradycardia ⑤ Hypertrophic cardiomyopathy was excluded by the absence of left ventricular hypertrophy (wall thickness <15 mm) and an LGE pattern inconsistent with the typical septal-inferior junction involvement. In summary, the diagnosis of NDLVC is strongly supported by the systematic exclusion of alternative etiologies through integrated clinical, laboratory, and imaging findings.
Based on the echocardiographic and cardiac magnetic resonance (CMR) findings, this patient meets the 2023 ESC definition of non-dilated left ventricular cardiomyopathy (NDLVC). In accordance with current recommendations, patients with this diagnosis should undergo regular clinical and imaging follow-up to monitor for potential disease progression, including the development of systolic dysfunction, ventricular dilation, or arrhythmic events. This case underscores that establishing the diagnosis of NDLVC is not an endpoint but rather the beginning of a long-term surveillance strategy aimed at early detection of complications and timely intervention.
Conclusion
Multimodal imaging is beneficial for the diagnostic evaluation of NDLVC, with CMR playing a clinically significant role in its multimodal imaging assessment.
Acknowledgments
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has received funding by the National Key R&D Program of China (2022YFE0209800), the National Natural Science Foundation of China (No. 82271986), the Beijing Anzhen Hospital High Level Research Funding (No. 2024AZC2002), and Beijing Postdoctoral Research Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arbelo E, Protonotarios A, Gimeno JR, et al. 2023 ESC guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44(37):3503–5. doi:10.1093/eurheartj/ehad194
2. Eda Y, Nabeta T, Iikura S, et al. Non-dilated left ventricular cardiomyopathy vs. dilated cardiomyopathy: clinical background and outcomes. ESC Heart Fail. 2024;11(3):1463–1471. doi:10.1002/ehf2.14711
3. Tkaczyszyn M. Dilated versus non-dilated left ventricular cardiomyopathy: same same but different? ESC Heart Fail. 2024;11(5):2681–2683. doi:10.1002/ehf2.14923
4. Narducci ML, Scacciavillani R, Nano RL, et al. Prognostic value of electroanatomic-guided endomyocardial biopsy in patients with myocarditis, arrhythmogenic cardiomyopathy and non dilated left ventricular cardiomyopathy. Int J Cardiol. 2024;416:132489. doi:10.1016/j.ijcard.2024.132489
5. Reddy YNV, Borlaug BA, Gersh BJ. Management of atrial fibrillation across the spectrum of heart failure with preserved and reduced ejection fraction. Circulation. 2022;146(4):339–357. doi:10.1161/CIRCULATIONAHA.122.057444
6. Dziewięcka E, Winiarczyk M, Wiśniowska-śmiałek S, et al. Comparison of clinical course and outcomes between dilated and hypokinetic non-dilated cardiomyopathy. Cardiology. 2023;148(5):395–401. doi:10.1159/000531534
7. Filomena D, Vandenberk B, Dresselaers T, et al. Cardiac diagnoses and long-term outcomes in ring-like late gadolinium enhancement evaluated by cardiac magnetic resonance. Eur Heart J Cardiovasc Imaging. 2025;18(12):jeaf055.
8. Botis I, Bazmpani MA, Daios S, et al. The role of cardiovascular magnetic resonance imaging in the assessment of mitral regurgitation. Diagnostics. 2024;14(6):644. doi:10.3390/diagnostics14060644
9. Coraducci F, De Zan G, Fedele D, et al. Cardiac magnetic resonance in advanced heart failure. Echocardiography. 2024;41(6):e15849. doi:10.1111/echo.15849
10. Castrichini M, De Luca A, De Angelis G, et al. Magnetic resonanceimaging characterization and clinical outcomes of dilated and arrhythmogenic left ventricular cardiomyopathies. J Am Coll Cardiol. 2024;83(19):1841–1851. doi:10.1016/j.jacc.2024.02.041
11. Leo I, Dellegrottaglie S, Scatteia A, et al. Cardiac magnetic resonance for prophylactic implantable-cardioverter defibrillator therapy in non-dilated left ventricular cardiomyopathy: a sub-study from the derivate registry. Eur Heart J Cardiovasc Imaging. 2025;3(2):jeaf043.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.