Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Multimodal Considerations Concerning Basal Cell Carcinoma Clefting – Profile of Structural and Aggressive Traits – Perspectives
Authors Niculet E ![]() , Bobeica C
, Bobeica C ![]() , Craescu M, Nicolescu AC
, Craescu M, Nicolescu AC ![]() , Tocu G
, Tocu G ![]() , Onisor C
, Onisor C ![]() , Arbune M
, Arbune M ![]() , Tatu AL
, Tatu AL ![]()
Received 5 August 2022
Accepted for publication 11 September 2022
Published 29 September 2022 Volume 2022:15 Pages 2087—2095
DOI https://doi.org/10.2147/CCID.S385213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Elena Niculet1,2 *, Carmen Bobeica1 *, Mihaela Craescu,1,2 Alin Codrut Nicolescu3 *, George Tocu,4 Cristian Onisor1 *, Manuela Arbune5 *, Alin Laurentiu Tatu2,5,6
1Department of Morphological and Functional Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, Romania; 2Multidisciplinary Integrated Center of Dermatological Interface Research MIC-DIR (Centrul Integrat Multidisciplinar de Cercetare de Interfata Dermatologica - CIM-CID), “Dunărea de Jos” University, Galați, Romania; 3Roma Medical Center for Diagnosis and Treatment, Bucharest, Romania; 4Department of Pharmaceutical Sciences, “Dunărea de Jos” University, Galati, Romania; 5Clinical Medical Department, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, Galați, Romania; 6Dermatology Department, “Sf. Cuvioasa Parascheva” Clinical Hospital of Infectious Diseases, Galați, Romania
*These authors contributed equally to this work
Correspondence: Mihaela Craescu, Department of Morphological and Functional Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, 35 Alexandru Ioan Cuza Street, Galați, 800008, Romania, Tel +40751869864, Email [email protected] George Tocu, Department of Pharmaceutical Sciences, Faculty of Medicine and Pharmacy, “Dunărea de Jos” University, 35 Alexandru Ioan Cuza Street, Galați, 800008, Romania, Tel +40773819438, Email [email protected]
Abstract: Although basal cell carcinoma is a well-known tumor with confirmed clinical and histopathology traits, prognosis factors and treatment options, new facets of this tumor emerge as innovative approach methods develop. Reflectance confocal microscopy (RCM) and optical coherence tomography (OCT) allow a basal cell carcinoma’s in vivo analysis of its depth of invasion, tumor margins prior to surgical approach and the tumor’s response to a non-invasive treatment, evaluating simultaneously the tumor’s vasculature. By RCM and OCT analysis, basal cell carcinoma has registered a groundbreaking discovery regarding a small (but with predictive factor potential) trait – the cleft, developing in between the tumor islands/nodules/chords and the surrounding tumor stroma; it was considered to date as a consequence of the tissue’s histopathology processing. RCM and OCT revealed that the “clefting artifact”, as it is frequently found in the medical literature, is not actually an artifact of laboratory processing, but a tumor trait found in vivo, with apparent mucin deposits. This review aims at merging the methods of evaluating basal cell carcinoma, both non-invasive (dermoscopy, RCM, OCT) and invasive ones (histopathology – with newly proposed classification), with special emphasis on the cleft issue – its assessment with the aforementioned techniques, with potential implications in the patient’s prognosis.
Keywords: basal cell carcinoma, cleft, structural aggressive traits, reflectance confocal microscopy, optical coherence tomography, pathology
Introduction
Basal cell carcinoma (BCC) is one of the most prevalent malignant skin tumors worldwide, having an increasing incidence each year, with variations according to the region. The characteristic-affected population has been represented up until now by the elderly men (having a steep rise in incidence over 40 years of age), with increasing numbers among female patients in the last years, a change reflected in the living style and/or environmental factors’ exposure.1–3 The pathogenesis of BCC is highly complex, with interplay between lifestyle factors, phenotype and genotype, the most important risk factor remaining the ultraviolet (UV) light exposure. The patient’s education will play an important role in the future concerning sun exposure and avoidance, with emphasis on (childhood and/or adolescence) protective measures (sun protection creams), the precocious tumor detection and expeditious positive diagnosis, and early treatment measures (invasive or not, with updated management alternatives such as Hedgehog pathway inhibitors or immune checkpoint inhibitors).2,3
BCC is a skin tumor clinically possessing certain traits which aid in its positive diagnosis, such as the presence of an ulcerated or eroded nodule or papule or plaque, translucency, telangiectasia (dilated blood vessels), pigmentation (black/blue hue) and rolled borders.1 BCC development is frequently associated with sun exposure, appearing on sun-exposed areas of the face and body; some anatomical areas are considered to be of high-risk, such as facial periorificial zones which frequently develop aggressive types of BCCs.1,4
Clinically, BCC should not be confused with a large variety of differential diagnoses which include skin tumors or inflammatory disorders, such as: Darier’s disease, adult-onset xanthogranuloma, epidermal cysts, lymphoma, rhabdomyomatous mesenchymal hamartoma, adnexal tumors (having either follicular, sebaceous or sweat gland differentiation), squamous cell carcinoma, Ewing’s sarcoma, Merkel cell carcinoma, trichoblastoma, allergic contact dermatitis, irritant contact dermatitis, psoriasis, lymphoepithelioma-like carcinoma, pomade crust, and many others, all of these presenting with traits which could determine a physician to give an erroneous positive diagnosis of BCC.1,3,5–7
The positive BCC diagnosis is made on the basis of the clinical traits, the dermoscopic analysis and histopathologic evaluation (considered to be the gold standard and an invasive procedure); other new, emerging non-invasive procedures have been taken into consideration for BCC diagnosis, as indicated below.8
Dermoscopy and Other Innovative Non-Invasive Procedures
A well-known, non-invasive, in vivo examination procedure is dermoscopy, having a sensitivity of up to 91.2% and a specificity up to 95%. This allows clinical examination of the lesion’s traits which cannot be visible directly (meaning, with the open-eye). In order to make a positive diagnosis of BCC, the following three features have to be found: vascular traits (fine, arborizing, corkscrew/glomerular vessels), pigmented traits (white-shiny areas, alternating with white-reddish areas, and multiple dots-like or ovoid blue-grayish nests) and ulceration. These three traits, associated with melanocytic lesions traits (network-like zones) establish a positive BCC diagnosis. These traits, mixed and matched, give the overall aspect of BCC, with some variability according to the subtype of the tumor, the patient’s age, race and gender, the location of the tumor and the existence of pigment in the tumor islands.9–11
Currently, there are other new, emerging non-invasive procedures which aid in making a positive BCC diagnosis: the reflectance confocal microscopy (RCM) and the optical coherence tomography (OCT).8
RCM is a technology which uses a near-infrared laser in studying a BCC lesion and offers imaging of thin sections from this cutaneous lesion.8 Besides the characteristics of a BCC’s subtype, RCM examination has revealed, in vivo, a somewhat particular trait, considered an artifact in the past: the tumor-stroma separation/cleft which looks like areas of low refractility in-between the tumor mass and the surrounding stroma, thus raising the question whether the mucin found here is the culprit for such separation, and whether this suggests a more aggressive behavior or not.12
OCT is a technology which uses infrared light in order to give real-time images of the BCC lesion, based on the sum of the light refractions of the different cutaneous structures with different optical traits; the general characteristics of BCCs under OCT examination are revealed in Table 1 and Figure 1.8,13,14
 |
Table 1 BCC Characteristics Revealed by OCT |
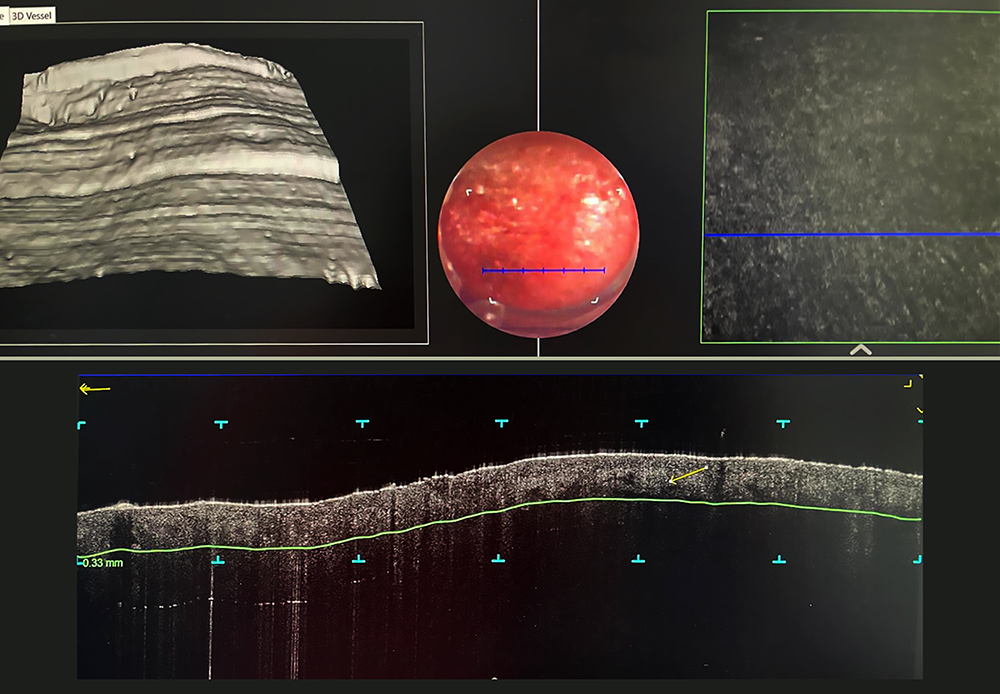 |
Figure 1 Optical coherence tomography of a superficial basal cell carcinoma – the arrow indicates the cleft. |
Histopathology
Biopsy of the lesion (either shave, punch or excisional) is of utmost importance when addressing BCC, and, from a histopathological standpoint, the type of BCC and other morphological characteristics have real impact on the patient’s prognosis and further therapeutic management.8,15,16
In general, BCCs are represented by various-sized groups/nodules of basaloid-looking cells, similar to basal cells found in the first layer of the interfollicular epidermis and/or from the squamous epithelium of the pilosebaceous unit.8,15 The tumor nodules are characterized by a peripheral palisading of cells (and nuclei) and by a separation space in-between the tumor nodule and the stroma, the latter being considered up until now as an artifact appearing in the course of laboratory processing.8,12,15 The initial biopsy gives the physician a view of the subtype of BCC with which one deals, and also directs the appropriate treatment; however, in many cases it does not correctly identify the BCC subtype, having a concordance of roughly 54% between the shave specimen subtype and the following full lesion excision; the punch biopsy, though, has better chances of revealing the aggressive pattern of growth in BCCs.8,15
In 2021, a group of researchers has proposed a simpler classification for BCC, unifying into a single category of infiltrative BCCs, the following three – infiltrating, micronodular and sclerosing BCC, improving physician concordance in reporting this type of tumors and making this classification more practical, with a better highlighting of the high-risk tumors with deep involvement. The subtypes of BCC that remained valid in the classification were infiltrative, nodular, superficial, infundibulocystic, basosquamous, with sarcomatoid differentiation, and fibroepithelial.16 Furthermore, BCC types can be classified into two main groups, low-risk and high-risk ones, respectively, according to the recurrence risk of this tumor (Tables 2 and 3).16–20
 |
Table 2 BCC Classification According to Recurrence Risk |
 |
Table 3 Clinically Relevant BCC Subtypes and Their Morphological Traits |
The Cleft Issue
What is “the cleft” or “clefting” or “the clefting artifact”? For some BCC subtypes, such as nodular BCC, the separation between the malignant tumor nodules and the surrounding stroma (meaning the cleft) is a characteristic trait, either seen as an empty space or an area with a bluish material (hyaluronic acid); it can also be visible in superficial BCC and it was considered to be a retraction artifact during the histopathology laboratory routine practices, the fibromyxoid stroma retracting itself from the tumor nodules. For other types of BCC, such as morpheaform/sclerosing having a more fibrotic stroma and aggressive behavior, retraction spaces are usually absent.12,21
Then…
The BCC’s basal lamina has been an issue to discuss even since the 1980s (and, indirectly, has also been the BCC clefting).22 The basement membrane is a thin layer of extracellular matrix underlying epithelial cells, separating them from and also connecting them to the stroma or interstitial matrix.23 In 1980, Tosca et al concluded that basement membrane antigenic loss (meaning the bullous pemphigoid antigen) is a general and early trait of neoplasia, being directly linked to the characteristic neoplastic cell’s loss of control, making it able to further disseminate and metastasize.22
In a study done by Stanley et al, the BCC’s basal lamina was characterized by using indirect immunofluorescence studies and it was found to be made up from laminin, type IV collagen and bullous pemphigoid antigen; the first two display a linear, continuous pattern, while the latter has a rather discontinuous and linear pattern, or it is even absent. This matter is a specific defect of BCC, the normal epidermal cells being able to synthetize it. Other epidermal tumors, such as benign ones (trichoepithelioma, wart, seborrheic keratosis, cylindroma) or malignancies (squamous cell carcinoma – keratoacanthoma-like, superficially invasive or invasive one), do not have this particular trait, presenting all three antigens in their basal lamina which surrounds the epithelial tumor nests, as well as in the normal epidermis.22,24
In 1984, Mérot et al described the cleft as being a dynamic process by involving a degenerative phase of the palisading tumoral basal cells. As such, yet again with the help of indirect immunofluorescence studies, they have found that two antigens – collagen IV and laminin, were found only on the stromal side of the cleft when the peritumoral cleft was present, while in cases where the cleft was not present, these antigen deposits were found as linear, continuous deposits surrounding the tumor nests. At the same time, the bullous pemphigoid antigen, which was present in a continuous and/or discontinuous pattern along the basement membrane of the tumor islands in cases where the cleft was missing, was absent where the cleft was present, raising the question whether it plays a role in the cleft formation.25 In fact, an important role in bullous pemphigoid antigen production by the BCC tumor cells might be the epithelial-stromal interaction; this antigen production is involved in basal cell differentiation, but its defective synthesis is present in BCC, thus impairing their maturation.24,25
The 1989 study by Basset-Séguin also supports the finding in regard to the antigenic alteration of the bullous pemphigoid antigen (from the lamina lucida) inside the tumor island’s basement membrane (significant reduction or even total absence), with the normal presence of laminin and type IV collagen antigens. The idea that malignant keratinocytes do not produce certain antigens – such as bullous pemphigoid antigen, is further supported.22,24–26
C3d,g is a fragment of the third complement component and it is normally present in the epidermal basement membrane, more specifically, the lamina densa. In the BCC’s basement membrane, C3d,g is significantly diminished or even absent, just like in the case of the bullous pemphigoid antigen, revealing a more complex series of changes at this level of the malignant tumor islands. Moreover, each subregion of the basement membrane presents its own changes: lamina lucida, with the reduced/absent bullous pemphigoid antigen; lamina densa, with the KF-1 antigen reduction and the C3d,g reduction/absence (at the base of the lamina densa and within the sublamina densa region).26
Puizina-Ivić et al, in their study from 2008, have highlighted the role of Bcl-2 in BCC variants and squamous cell carcinoma. Bcl-2 is very important in cell death regulation, protecting the cell against it and against apoptosis. Concerning the nodular, adenoid and cystic variants of BCC, the peripheral palisading of tumor cells proved to have intense immunoreactivity, ensuring the extension of the tumor. Another BCC subtype, the morpheaform one, proved reduced immunostaining intensity, showing high proliferation rates and the origin in the basal keratinocytes (as squamous cell carcinoma, for example, is negative for Bcl-2).27
In 2018, Hirakawa et al concluded that besides collagen IV, nidogen-1 (a main structural component of the normal basement membrane of the epidermis) has a role in BCC (but also actinic keratosis and squamous cell carcinoma) tumor development, being increased in the BCC’s basement membrane and in the surrounding stroma, with patterns similar to collagen IV. A possible explanation could be the fact that the stromal cells (such as fibroblasts) surrounding the tumor islands start to produce basement membrane components, as a reactive response to the tumor islands, and thus making and acting like a restrictive enclosure, limiting the tumor at its primary development site. Cancer-associated fibroblasts have been reported as having a possible role in malignant tumor development and progression. Fibroblasts surrounding BCC might produce more nidogen-1, and, alongside other basement membrane components, might be involved in limiting its progression, infiltration and metastatic potential.23
…and Now
The now available, novel in-vivo evaluation techniques such as RCM and OCT (both based on the backscattering of light and used either as separate clinical evaluation techniques, or as an integrated one, complementing each other) have highlighted the fact that “the artificial cleft” might not be secondary to routine processing or to the reduced adhesiveness of the tumor, but that rather it is a BCC “structure” (or BCC trait) which is present in the patient’s skin, prior to excision and processing.12,28 RCM allows for an increased image resolution to be obtained, while OCT has a minimum resolution and is considered to have a lowered specificity and sensitivity. A combination of RCM-OCT ensures the highest rates of a BCC entire volume examination, being also a good tool in studying the subtype of BCC examined (with excellent results regarding the infiltrative component which indicates high risk, with same terminology as in the histopathological examination – angulation, small nests or chords), while OCT alone does not have the necessary resolution for cellular-level studying.12,28
RCM has revealed that the BCC tumor islands have areas of low refractility, separating them from the surrounding stroma and deposits such as mucin might be found here.12 Table 4 presents some RCM and histopathological characteristics correlation for the superficial subtype of BCC. Some features, such as streaming of the epidermis, are highlighted by RCM evaluation and offer more information on BCC morphology, without being specific for a certain subtype. This trait is evidenced by the nuclei of the spinous layer keratinocytes which are elongated and oriented in the same axis; moreover, large, plump, bright cells are also found and are considered to be melanophages.29
 |
Table 4 Superficial BCC - RCM and histopathology evaluation |
A study done by Ulrich et al has found that between the histopathological measurement of mucin deposits (done with special stains such as Alcian blue) and the dark areas’ diameter there is good correlation. However, they have also highlighted that in between RCM and histopathological examination there were some variations, including the morphological presence of wider cleft-like spaces which were not observed at RCM, thus reflecting the already emerged theory about clefting being an artifact of laboratory processing.12 Of high interest was a finding by Gill et al who reported a false-positive result on RCM-OCT, a finding which was positive only on OCT due to the fact that the image was outside the field of view of the RCM examination. The image described some angulated chords and/or nests which surrounded a very well-structured tumor nodule, the team considering these (on histopathological examination) as being peritumoral areas with fibrosis, thick collagen bundles, an increased number of blood vessels and inflammation. However, a false-negative histopathological examination cannot be excluded, the peritumoral cleft still being a questionable issue.28
Sahu et al have also used a combination of RCM and OCT in order to visualize the cellular structure and to evaluate the depth of BCCs; they have also evaluated amyloid and mucin deposits which can be found in such tumors, further correlating them histopathologically. Amyloid deposits are seen under RCM-OCT investigation as areas of amorphous, hyperreflective, homogenous material, which is placed intra- or peritumorally, while mucin is seen as hyporeflective areas (inside the tumor nodules or peritumorally), as stated before. An important aspect with prognostic significance is the fact that amyloid and/or mucin deposits have been observed in less aggressive forms of BCC, such as the nodular BCC. This raises a red flag for the physician so that such deposits be searched for, in order to establish a better further management of the patient’s case.30
Other theory concerning BCC talks about the “angiogenic switch”, meaning the predominance of pro-angiogenic factors which determine the development of new blood vessels, an important step in tumor development and progression. A higher microvascular density is correlated with higher levels of vascular endothelial growth factor (VEGF) in BCC, with a following remodeling of the extracellular matrix. BCCs have really low metastasis rates, although the vascular architecture is enriched, having increased numbers of vessels which are more dilated and irregular. Could angiogenesis be a regulating system for BCC aggressiveness? It remains a subject for further research as novel imaging tools such as RCM and OCT can ensure an in vivo examination of tumor vessels, without compression artifacts.31,32
Conclusion
RCM, OCT or both combined are new in-vivo investigating techniques for the dermatologist, with better outcomes and procedure steps concerning the patient, evaluations which can be reproduced, are cost-effective and which avoid invasiveness. At the same time, these techniques can offer a clear image of the tumor margins, prior to the surgical excision and can monitor the tumor’s response to a non-invasive treatment with vasculature observations.
Abbreviations
BCC, basal cell carcinoma; UV, ultraviolet; BCCs, basal cell carcinomas; RCM, reflectance confocal microscopy; OCT, optical coherence tomography; VEGF, vascular endothelial growth factor.
Data Sharing Statement
The information will be granted access to under reasonable request.
Acknowledgments
The authors wish to acknowledge that the present study was academically supported by the “Dunarea de Jos” University of Galati, Romania, through the research center – Multidisciplinary Integrated Center of Dermatological Interface Research MIC-DIR (Centrul Integrat Multidisciplinar de Cercetare de Interfata Dermatologica - CIM-CID).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study was supported by the “Dunărea de Jos” University of Galați.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kim HS, Kim TW, Mun JH., et al. Basal cell carcinoma-mimicking lesions in Korean clinical settings. Ann Dermatol. 2014;26(4):431–436. doi:10.5021/ad.2014.26.4.431
2. Janković S, Maksimović N, Janković J, Ražnatović M, Marinković J, Vesna T-S. Risk factors for basal cell carcinoma: results from the case-control study. Cent Eur J Med. 2010;5(6):666–673. doi:10.2478/s11536-010-0042-5
3. Naik PP, Desai MB. Basal cell carcinoma: a narrative review on contemporary diagnosis and management. Oncol Ther. 2022. doi:10.1007/s40487-022-00201-8
4. Amici JM, Dousset L, Battistella M, et al. Clinical factors predictive for histological aggressiveness of basal cell carcinoma: a prospective study of 2274 cases. Ann Dermatol Venereol. 2021;148(1):23–27. doi:10.1016/j.annder.2019.10.028
5. McDaniel B, Badri T, Steele RB. Basal cell carcinoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
6. Cives M, Mannavola F, Lospalluti L, et al. Non-melanoma skin cancers: biological and clinical features. Int J Mol Sci. 2020;21(15):5394. doi:10.3390/ijms21155394
7. Cazzato G, Cimmino A, Colagrande A, et al. The multiple faces of nodular trichoblastoma: review of the literature with case presentation. Dermatopathology. 2021;8(3):265–270. doi:10.3390/dermatopathology8030032
8. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: contemporary approaches to diagnosis, treatment, and prevention. J Am Acad Dermatol. 2019;80(2):321–339. PMID: 29782901. doi:10.1016/j.jaad.2018.02.083
9. Reiter O, Mimouni I, Gdalevich M, et al. The diagnostic accuracy of dermoscopy for basal cell carcinoma: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(5):1380–1388.
10. Reiter O, Mimouni I, Dusza S, Halpern AC, Leshem YA, Marghoob AA. Dermoscopic features of basal cell carcinoma and its subtypes: a systematic review. J Am Acad Dermatol. 2019. doi:10.1016/j.jaad.2018.12.026
11. Álvarez-Salafranca M, Ara M, Zaballos P. Dermoscopy in basal cell carcinoma: an updated review. Actas Dermosifiliogr. 2021;112(4):330–338. doi:10.1016/j.ad.2020.11.011
12. Ulrich M, Roewert-Huber J, González S, Rius-Diaz F, Stockfleth E, Kanitakis J. Peritumoral clefting in basal cell carcinoma: correlation of in vivo reflectance confocal microscopy and routine histology. J Cutan Pathol. 2011;38(2):190–195. doi:10.1111/j.1600-0560.2010.01632.x
13. Fania L, Didona D, Morese R, et al. Basal cell carcinoma: from pathophysiology to novel therapeutic approaches. Biomedicines. 2020;8(11):449. doi:10.3390/biomedicines8110449
14. Niculet E, Craescu M, Rebegea L, et al. Basal cell carcinoma: comprehensive clinical and histopathological aspects, novel imaging tools and therapeutic approaches (Review). Exp Ther Med. 2022;23:60. doi:10.3892/etm.2021.10982
15. Tsubura A, Oyaizu T, Fujita Y, Asada M, Hilgers J, Morii S. Keratin phenotypes in Basal-cell carcinomas of the skin. Int J Oncol. 1993;2(3):431–435. doi:10.3892/ijo.2.3.431
16. Fernández-Figueras MT, Malvehi J, Tschandl P, et al. Position paper on a simplified histopathological classification of basal cell carcinoma: results of the European Consensus Project. J Eur Acad Dermatol Venereol. 2021;36:351–359.
17. Cameron MC, Lee E, Hibler BP, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303–317. doi:10.1016/j.jaad.2018.03.060
18. Messina J, Epstein EH Jr, Kossard S, et al. Chapter 1 – keratinocytic/epidermal tumors. Basal cell carcinoma. In: Elder DE, Massi D, Scolyer RA, Willemze R, editors. WHO Classification of Skin Tumors.
19. Căruntu C, Boda D, Guţu DE, Căruntu A. In vivo reflectance confocal microscopy of basal cell carcinoma with cystic degeneration. Rom J Morphol Embryol. 2014;55(4):1437–1441.
20. Hasan A, Rabie A, Elhussiny M, et al. Recurrent cutaneous basal cell carcinoma after surgical excision: a retrospective clinicopathological study. Ann Med Surg. 2022;78:103877. doi:10.1016/j.amsu.2022.103877
21. Mackiewicz-Wysocka M, Bowszyc-Dmochowska M, Strzelecka-Węklar D, Dańczak-Pazdrowska A, Adamski Z. Basal cell carcinoma - diagnosis. Contemp Oncol. 2013;17(4):337–342. doi:10.5114/wo.2013.35684
22. Tosca A, Varelzidis A, Nicolis G, Hadzis J, Stratigos J, Capetanakis J. Antigenic alterations in tumors of epidermal origin. Cancer. 1980;45(9):2284–2290. doi:10.1002/1097-0142(19800501)45:9<2284::AID-CNCR2820450911>3.0.CO;2-S
23. Hirakawa Y, Futaki S, Tanizaki H, et al. Enhanced expression of nidogen 1 around the nest of basal cell carcinoma compared with that around squamous cell carcinoma. Med Mol Morphol. 2019;52(2):99–105. doi:10.1007/s00795-018-0207-x
24. Stanley JR, Beckwith JB, Fuller RP, Katz SI. A specific antigenic defect of the basement membrane is found in basal cell carcinoma but not in other epidermal tumors. Cancer. 1982;50(8):1486–1490. PMID: 6288214. doi:10.1002/1097-0142(19821015)50:8<1486::aid-cncr2820500807>3.0.co;2-f
25. Mérot Y, Faucher F, Didierjean L, Saurat JH. Loss of bullous pemphigoid antigen in peritumoral lacunas of basal cell carcinomas. Acta Derm Venereol. 1984;64(3):209–213.
26. Basset-Séguin N, Uhle P, Emanuel D, Henry P, Yancey KB. Defective expression of basement membrane-associated C3d,g in papulonodular basal cell carcinomas. J Invest Dermatol. 1989;92(5):734–738. PMID: 2654297. doi:10.1111/1523-1747.ep12721747
27. Puizina-Ivić N, Sapunar D, Marasović D, Mirić L. An overview of Bcl-2 expression in histopathological variants of basal cell carcinoma, squamous cell carcinoma, actinic keratosis and seborrheic keratosis. Coll Antropol. 2008;32(Suppl 2):61–65.
28. Gill M, Sahu A, Alessi-Fox C, et al. Angulated small nests and cords: key diagnostic histopathologic features of infiltrative basal cell carcinoma can be identified using integrated reflectance confocal microscopy-optical coherence tomography. J Cutan Pathol. 2021;48(1):53–65. doi:10.1111/cup.13871
29. Ghita MA, Caruntu C, Rosca AE, et al. Reflectance confocal microscopy and dermoscopy for in vivo, non-invasive skin imaging of superficial basal cell carcinoma. Oncol Lett. 2016;11(5):3019–3024. doi:10.3892/ol.2016.4354
30. Sahu A, Cordova M, Gill M, et al. In vivo identification of amyloid and mucin in basal cell carcinoma (BCC) with combined reflectance confocal microscopy (RCM) - optical coherence tomography (OCT) device and direct histopathological correlation. JAAD. 2020;83(2):619–622. doi:10.1016/j.jaad.2019.08.063
31. Lupu M, Caruntu C, Popa MI, Voiculescu VM, Zurac S, Boda D. Vascular patterns in basal cell carcinoma: dermoscopic, confocal and histopathological perspectives. Oncol Lett. 2019;17(5):4112–4125. doi:10.3892/ol.2019.10070
32. Niculet E, Tatu AL. Comment on Correlation of basal cell carcinoma subtype with histologically confirmed subclinical extension during Mohs micrographic surgery: a prospective multicenter study. JAAD. 2022;87(1):e49–50. doi:10.1016/j.jaad.2022.03.060
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Syringocystadenoma Papilliferum and Basal Cell Carcinoma Arising in Nevus Sebaceous
Jiang J, Chen Y, He Q, Yang J, Zhang Z, Yang H, Zhang H, Yang C
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2021-2026
Published Date: 23 September 2022