Back to Journals » Clinical Interventions in Aging » Volume 20
Multimodal Brain Monitoring-Guided Anesthesia Management Improves Functional Connectivity, Enhances Recovery and Attenuates Postoperative Pain in Elderly Surgical Patients
Authors Yang S, Feng S, Wu H, Zhong C, Zhan S, Wang C ![]() , Chen Z, Huang Y, Zhao G, Zhang Y, Wang T
, Chen Z, Huang Y, Zhao G, Zhang Y, Wang T ![]() , Xiao W
, Xiao W
Received 5 July 2025
Accepted for publication 3 October 2025
Published 15 October 2025 Volume 2025:20 Pages 1757—1771
DOI https://doi.org/10.2147/CIA.S551727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Shuyi Yang,1,* Shuai Feng,1,* Hao Wu,2,* Chonglin Zhong,1 Shubin Zhan,1 Chunxiu Wang,3 Zan Chen,2 Yaxian Huang,1 Guanxu Zhao,1 Yue Zhang,1 Tianlong Wang,1 Wei Xiao1
1Department of Anesthesiology, Xuanwu Hospital Capital Medical University, National Clinical Research Center for Geriatric, Beijing, People’s Republic of China; 2Department of Neurosurgery, Xuanwu Hospital Capital Medical University, Beijing, People’s Republic of China; 3Department of Evidence-Based Medicine, Xuanwu Hospital Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Xiao, Department of Anesthesiology, Xuanwu Hospital Capital Medical University, National Clinical Research Center for Geriatric, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +86 138 1097 1299, Email [email protected] Tianlong Wang, Department of Anesthesiology, Xuanwu Hospital Capital Medical University, National Clinical Research Center for Geriatric, No. 45 Changchun Street, Xicheng District, Beijing, 100053, People’s Republic of China, Tel +86 139 1052 5304, Email [email protected]
Purpose: Perioperative neurocognitive disorder (PND) is common in elderly surgical patients and severely affects postoperative recovery. However, effective prevention is still lacking. Potential perioperative cerebral stressors (including inappropriate sedative/analgesic depth and imbalanced cerebral oxygen supply/demand) may be important contributing factors. We developed an anesthesia management protocol based on multimodal brain monitoring to achieve standardized, individualized, and real-time regulation of sedative/analgesic depth and cerebral oxygen saturation and investigated whether it could reduce the incidence of PND and its underlying mechanisms.
Patients and Methods: Patients (aged ≥ 65 years) were randomized into Groups C (n=88) and E (n=93). Patients in Group E received multimodal brain monitoring-guided anesthesia management, and those in Group C received BIS-guided anesthesia management. The Montreal Cognitive Assessment (MoCA) was performed both before and seven days after surgery. The postoperative pain scores were recorded. Resting-state functional MRI data were analyzed to examine functional connectivity (FC).
Results: Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), but this difference was not statistically significant. Patients in Group E had increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (P < 0.05). Significantly lower pain scores were observed in Group E at rest (1h: P=0.04; 24h: P=0.04) and during movement (1h: P=0.03).
Conclusion: These results suggest that multimodal brain monitoring-guided anesthesia management may protect neurocognition by enhancing FC within cognition-associated brain regions and attenuating postoperative acute pain. And multimodal brain monitoring-guided anesthesia management may confer a clinically relevant reduction in PND incidence compared to BIS-guided management in elderly surgical patients.
Keywords: multimodal brain monitoring, elderly patients, perioperative neurocognitive disorders, functional connectivity, postoperative acute pain
Introduction
Perioperative neurocognitive disorder (PND), which refers to delirium and longer-lasting postoperative cognitive dysfunction, is characterized by memory impairment, attention deficits, diminished language processing, and reduced social adaptability, represents a significant complication in geriatric surgical populations.1,2 Epidemiological data revealed a 41.4% incidence (95% CI: 36.2–46.7%) of PND following non-cardiac surgeries at discharge, which escalates to 43% in spinal procedures.3 Neurocognitive disorders frequently persist for months or years after surgery. PND prolongs functional recovery and hospitalization owing to increased mortality and disability rates. Therefore, PND is associated with a substantial socioeconomic burden. Despite the growing aging surgical population, therapeutic strategies remain limited owing to an incomplete understanding of PND pathogenesis.
Emerging evidence indicates neuroinflammatory cascades in PND development,3 with surgical stress triggering the systemic and cerebral inflammatory responses. Key intraoperative cerebral stressors include inadequate analgesia/sedation, impaired cerebral oxygen supply-demand balance, and abnormal temperature. These cerebral stressors collectively promote neuroinflammation,4 disrupt functional brain networks,5,6 and precipitate cognitive decline.4,5,7,8 Current anesthesia practices that rely on sedation depth, such as Bispectral Index (BIS) monitoring and clinical experience, demonstrate limitations in elderly patients, particularly in nociception assessment and prevention of cerebral oxygen supply-demand imbalance.
Based on our preliminary pilot study,9 a protocol for multimodal brain monitoring-guided anesthesia management targeting cerebral stress mitigation was designed. The protocol integrated the continuous monitoring and adjustment of sedation depth (patient state index, PSI, and spectral edge frequency, SEF), analgesia depth (analgesia nociception index, ANI), cerebral oxygenation (regional cerebral oxygen saturation, rSO2), and nasopharyngeal temperature. The reason we chose lumbar fusion surgery in this study was that compared to other non-brain operations, it prominently embodies the risk factors for PND. The patient population undergoing this procedure primarily consists of elderly individuals, who are more susceptible to PND, with ageing being a well-established risk factor. Additionally, systemic inflammatory response is considered a potential mechanism underlying PND.10 Lumbar fusion surgery, in contrast to other non-brain operations, involves greater surgical trauma, longer duration, and is often accompanied by severe postoperative pain, which can further trigger inflammatory responses leading to neuroinflammation and cognitive impairment. Therefore, choosing lumbar fusion surgery enables a more effective investigation of PND.
Resting-state functional magnetic resonance imaging (rs-fMRI) provides critical insights into the functional connectivity (FC) alterations underlying PND.11 The default mode network (DMN), salience network (SN), and central executive network (CEN) are the three resting-state networks. The DMN, which is critical for memory consolidation,12 regulates the self-referential processes. Altered DMN connectivity strength predicts a decline in memory, executive function, and processing speed in elderly patients, potentially contributing to the development of PND.13 In addition, cerebral oxygen supply-demand imbalance and pain can disrupt FC. Elderly patients with a high hypoxia index exhibit reduced FC strength between the left and right parahippocampal cortices.5 Meanwhile, populations with chronic pain showed an altered FC in the prefrontal cortex.6 However, current evidence is primarily derived from patients with chronic diseases, and evidence from patients under acute surgical stress remains to be investigated.
In this study, we investigated whether multimodal brain monitoring-guided anesthesia management could effectively decrease the incidence of PND in elderly patients following spinal surgery. We also evaluated the safety and cost-effectiveness of the protocol. Furthermore, we investigated the strength of FC in cognition-associated brain regions and pain intensity to elucidate potential mechanisms mediating PND. We hypothesized that compared to conventional anesthesia management, multimodal brain monitoring-guided anesthesia management may improve postoperative cognitive outcomes by enhancing FC and attenuating pain, which may further mediate cerebral stress responses in elderly patients undergoing spinal surgery.
Materials and Methods
Study Design
This parallel-group, prospective, randomized controlled trial was conducted at a single center between April 2022 and February 2025. The study protocol was approved by the Institutional Review Board of Xuanwu Hospital, Capital Medical University (approval no. Linyanshen [2022]-021), and registered in the Chinese Clinical Trial Registry (ChiCTR2200058808). All the procedures conformed to the guidelines of the Declaration of Helsinki. Written informed consent supplemented by verbal confirmation was obtained from all participants prior to enrollment.
Patients
The inclusion criteria were age ≥65 years, American Society of Anesthesiologists (ASA) physical status I–III, scheduled for elective lumbar fusion surgery, and a minimum of six years of formal education enabling valid Montreal Cognitive Assessment (MoCA) completion. Exclusion criteria were pre-existing cognitive impairment disorders, baseline MoCA score <19, severe psychiatric conditions, contraindications to study medications, neurosurgical history, renal insufficiency, congestive heart failure, cerebrovascular events (cerebral hemorrhage and cerebral infarction) within 6 months, residual neurological deficits from prior events, persistent arrhythmia, spinal cord injury, left-handedness, alcohol or drug abuse, and refusal to participate.
The trial protocol mandated immediate discontinuation of treatment in participants who experienced serious adverse events or major protocol deviations.
Randomization and Blinding
Using a random number table (1:1 allocation) generated by validated online software (https://tools.medsci.cn/rand), participants were assigned to either multimodal brain monitoring-guided anesthesia (Group E) or BIS-guided anesthesia (Group C). Opaque sequentially numbered envelopes ensured allocation concealment until anesthesia induction. The participants, outcome assessors, and recruitment staff were blinded to the study protocol. Unblinding was performed only for acute safety concerns or trial completion.
Anesthesia Management
All patients received a standardized anesthesia induction and maintenance protocol, and no premedication was administered. Heart rate, invasive arterial blood pressure, pulse oxygen saturation, nasopharyngeal temperature, end-tidal CO2 level, and urine output were routinely monitored. Parecoxib sodium (40 mg) and ondansetron (4 mg) were intravenously administered 30 min before skin incision. Methylprednisolone 40 mg, etomidate 0.1–0.15 mg/kg, sufentanil 0.2–0.3 μg/kg, and rocuronium 0.6–0.8 mg/kg were given intravenously for anesthesia induction. The patients were then intubated, and the ventilation parameters were as follows: FiO2 40–60%, tidal volume 6–8 mL/kg, respiratory rate 12–15 breaths/min. The partial pressure of carbon dioxide was actively regulated within the target range of 35–40 mmHg. The partial pressure of carbon dioxide was monitored using blood gas at the following time points: before induction; 5 min after intubation, and 1h, 2h, and 3h following skin incision. Anesthesia was maintained using propofol and remifentanil with dosage adjustments according to the group protocol. Goal-directed fluid therapy targeting pulse pressure variability below 13% was performed intraoperatively. The intraoperative hemoglobin level remained > 10 g/dL; otherwise, transfusion was considered. The intraoperative fluctuation range of the blood pressure and heart rate was controlled within the baseline value of ±20%. Vasoactive regimens followed standardized escalation protocols with norepinephrine titrations. Initial norepinephrine infusion was at 0.03 μg/kg/min, while an increment or decrement of 0.02 μg/kg/min adjustments was administered for >20% MAP deviations.
The postoperative analgesic regimen consisted of oxycodone 40 mg diluted in 100 mL normal saline. Postoperative analgesia was administered via patient-controlled analgesia (PCA) without a background infusion. The bolus dose was 1 mg, lockout interval was 5 min, and maximum hourly limit was 3 mg.
Intervention
Group C (BIS-Guided Anesthesia Group)
The patients underwent standard BIS-guided anesthesia management. Continuous infusion of propofol (4 mg/kg/h) and remifentanil (0.2 μg/kg/min) sustained anesthetic depth, with propofol titrated in real-time to achieve bispectral index (BIS) guidance targets (40–60 range), while remifentanil dosage was empirically adjusted within 0.2–0.4 μg/kg/min based on clinical judgment. The perioperative nasopharyngeal temperature was maintained at 36–38°C. This protocol represents conventional anesthesia management for elderly surgical patients in current clinical practice.
Group E (Multimodal Brain Monitoring-Guided Anesthesia)
Patients underwent comprehensive neuromonitoring, including sedation depth (PSI and SEF), analgesia depth (ANI), and regional cerebral oxygen saturation (rSO2).9 Continuous infusion protocols initiated with propofol (4 mg/kg/h) and remifentanil (0.2 μg/kg/min) established baseline anesthetic depth. A real-time, individualized titration protocol was implemented as follows (Figure 1A): the sedation depth index (PSI and SEF) derived from the EEG monitoring was used as the trigger, and the target range of PSI was 25–50, while SEF was maintained between 8 and 12.
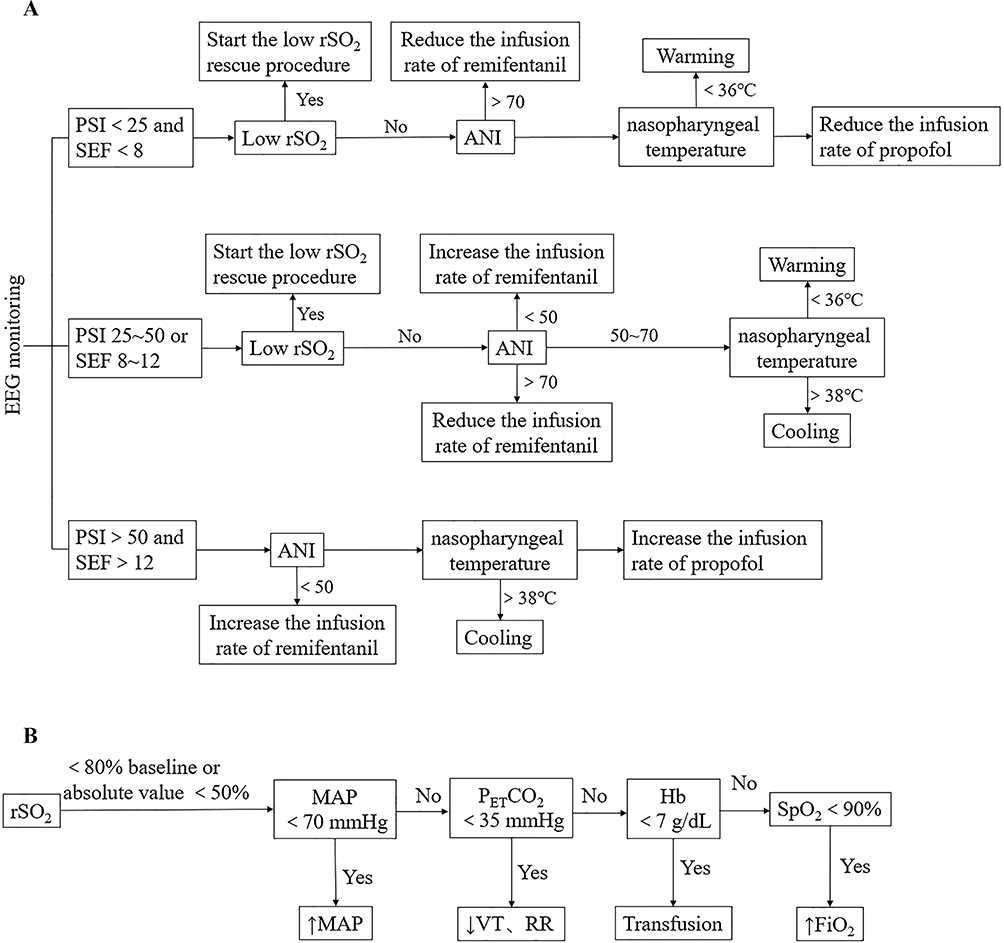 |
Figure 1 Management algorithm of Group E. (A) the algorithm of multimodal brain monitoring-guided anesthesia. The algorithm was triggered by PSI with the SEF, rSO2, ANI, and nasopharyngeal temperature observed in sequence. Low rSO2 rescue procedure, adjustment of the remifentanil or propofol infusion rate, warming or cooling were conducted according to parameters’ change. (B) Low rSO2 rescue procedure. MBP, PETCO2, Hb, and SpO2 levels were adjusted for low rSO2. (From Yang S, Xiao W, Wu H et al. Management Based on Multimodal Brain Monitoring May Improve Functional Connectivity and Post-operative Neurocognition in Elderly Patients Undergoing Spinal Surgery. Front Aging Neurosci. 2021;13:705287). Abbreviations: PSI, patient status index; SEF, spectral edge frequency; ANI, analgesia nociception index; rSO2, regional cerebral oxygen saturation; MBP, mean arterial pressure; PETCO2, partial pressure of end-tidal carbon dioxide; VT, tidal volume; RR, respiration rate; Hb, hemoglobin; SpO2, pulse oxygen saturation; FiO2, fraction of inspired oxygen. |
For low PSI/SEF (PSI <25 and SEF <8), the first step was to assess rSO2 and initiate a low rSO2 rescue procedure, if indicated (Figure 1B), until rSO2 achieved its target. The cerebral oxygenation protocol was a four-step process, including adjusting the mean arterial pressure by increasing it, increasing end-tidal carbon dioxide pressure by reducing tidal volume and respiratory rate, raising hemoglobin via blood transfusion, and improving pulse oxygen saturation by raising the fraction of inspired oxygen. The second step was to reduce the infusion rate of remifentanil in decrement of 0.02 μg/kg/min every minute until ANI normalized (50~70). The third step was warm the patients when hypothermia occurred, until the nasopharyngeal temperature was above 36 °C. If PSI/SEF remained low after cerebral oxygenation, ANI adjustment and temperature optimization, the final step was to reduce propofol infusion by 0.5 mg/kg/h every minute until the target PSI/SEF was achieved.
For normal PSI and SEF with abnormal ANI, the first step was to assess rSO2 and initiate a cerebral oxygenation protocol, if indicated (Figure 1B), until rSO2 achieved its target. Second, remifentanil was adjusted in increments or decrement of 0.02 μg/kg/min every minute until ANI normalized. The third step was to maintain the temperature within the target range via physical warming or cooling.
For high PSI/SEF (PSI>50 and SEF>12), the first step was to increase remifentanil by 0.02 μg/kg/min every minute for concurrent ANI <50. The second step was to optimize the body temperature if the PSI and SEF remained high. For persistent high PSI/SEF, the final step was to increase propofol by 0.5 mg/kg/h every minute until the target PSI/SEF was achieved. If body movements occurred, concurrent analgesics and sedatives were administered.
Blood Sample Collection
Blood samples were obtained via venipuncture at two intervals: one day prior to surgery (POD-1) and 24 h postoperatively (POD1). Serum separation was achieved through standardized centrifugation protocols (2000 rpm, 10 min duration) to collect the supernatant, which was subsequently aliquoted and stored at −80°C until analysis. The serum concentrations of zonulin, C-reactive protein (CRP), and lipopolysaccharide (LPS) were quantified using enzyme-linked immunosorbent assay (ELISA) kits according to the manufacturer’s protocols (CRP and IL-6: R&D Systems, Minneapolis, MN, USA; zonulin and LPS: CUSABIO, Wuhan, China). All measurements were performed in duplicate at the optimal dilutions to ensure that the values were within the standard curve range.
Patient Data Collection
Demographic and baseline clinical characteristics included age, sex, body mass index (BMI), educational attainment, ASA of Anesthesiologists physical status classification, medical history (hypertension, diabetes mellitus, and coronary artery disease), surgical segments, and preoperative diagnosis. Intraoperative records included anesthetic dosage, vasoactive medication administration, surgical duration, and duration of anesthesia. Preoperative training was provided to standardize the use of an 11-point Numeric Rating Scale (NRS; 0 = no pain to 10 = worst pain imaginable) for pain assessment. Postoperative NRS scores were recorded at surgical closure and 1, 24, 48, and 72 h postoperatively. Additional postoperative outcomes included time to first oral intake (liquids/solids), time to flatus, total oxycodone consumption, adverse events, 30-day all-cause mortality, length of hospital stay, and hospitalization costs.
Neuropsychological Assessment
MoCA was administered by a trained investigator under neuropsychologist supervision 1 d before surgery (POD-1) and on postoperative day 7 (POD7). To account for practice effects, normative data from community-dwelling volunteers (mean practice effect: 1.92 ± 1.19 points) collected by our research group were utilized for PND determination.3 The formula [MoCA score at POD7 – MoCA score at POD-1 – mean practice effect]/standard deviation of practice effect was used to calculate individual Z-scores. PND was defined as a Z-score ≥1.96 (95th percentile).
Data Acquisition of rs-fMRI
A 3.0-T Siemens Verio MRI scanner (Siemens Healthineers, Erlangen, Germany) equipped with a 32-channel head coil was used to perform fMRI preoperatively (POD-1) and POD7. Motion artifacts were minimized using foam padding and noise-reducing headphones. During scanning, participants were requested to be awake, close their eyes, and avoid structured thinking. fMRI acquisition employed the following protocols: repetition time (TR)=2000ms, echo time (TE)=40ms, field of view (FOV)=240×240 mm2, flip angle (FA)=90°, section thickness = 4 mm, acquisition matrix = 64×64, and whole brain composed of 28 slices in total. Structural imaging utilized a sagittal magnetization-prepared rapid-gradient echo (MPRAGE) sequence with T1-weighting, configured with: TR=1900ms, TE=2.2ms, TI=900ms, FA=9°, FOV=256×256 mm2, voxel size= 1 mm×1 mm×1 mm, and 176 slices at 1.0 mm thickness.
Image Data Processing
Structural preprocessing pipelines were incorporated: image deobliquing followed by PRI reorientation (right-to-left, posterior-to-anterior, and inferior-to-superior); skull stripping; normalization of the brain regions based on the Montreal Neurological Institute 152 stereotactic space (1mm3 isotropic) using linear and nonlinear registrations, segmentation of the brain into gray matter, white matter, and cerebrospinal fluid (CSF); and tissue segmentation of each patient was restricted by the tissue in the standard space provided in advance by FSL.
The DPABI toolbox was utilized to preprocess functional MRI data, including converting raw DICOM data to the NIFTI format and the following steps: removal of the first 10 time points, corrections for slice timing and head motion, co-registration of each subject’s structural image to the motion-corrected functional image, spatial normalization of the data to the MNI template, and applying a 4 mm Gaussian smoothing kernel. Subsequently, linear drift removal and temporal filtering are performed.
The square root of the voxel-wise signal in the 0.01–0.1 Hz band was defined as the amplitude of low-frequency fluctuations (ALFF), and fractional ALFF (fALFF) was derived by dividing the ALFF value of each voxel by the mean amplitude across the entire frequency band. Seed-based functional connectivity (FC) analysis was performed using a 5-mm spherical seed region centered at MNI coordinates (−1, 54, 27) in the medial prefrontal cortex (mPFC), generating individual FC maps through Pearson correlation analysis.
Statistical Analysis
The sample size estimation was derived from the primary outcome of the incidence of PND. Based on our preliminary findings, assuming a 33.33% (4/12) incidence in Group C vs 14.29% (2/14) in Group E (α=0.05, power=80%, two-sided chi-square test), 85 participants per group were required. After accounting for a dropout rate of 10%, 188 participants were recruited.
All statistical analyses were performed using SPSS v19.0 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized as mean±SD (parametric) or median [IQR] (nonparametric), while categorical variables were expressed as frequencies. Normality was assessed using the Kolmogorov–Smirnov test. Parametric comparisons employed the two-sample t-test for normal distributed data, whereas the Mann–Whitney U-test was used for non-normal distributed data. Categorical analyses were performed using the chi-squared test or Fisher’s exact test, as appropriate. All tests were two-tailed, with P=0.05, defining statistical significance.
Statistical analyses for fALFF and seed-based FC were computed using two-sample t-tests implemented in DPABI. Gaussian Random Field (GRF) correction at both voxel-wise and cluster-based levels (dual P <0.05) was used for multiple comparisons.
Spearman correlation coefficient was calculated to assess the correlation between the z-transformed (z)FC and longitudinal NRS scores. Fisher’s transformation was applied to transform the t-values of FC with statistical significance into Z scores.
Results
This study enrolled 188 consecutive patients scheduled for lumbar fusion surgery, of whom 181 ultimately met the inclusion criteria and underwent randomization (Figure 2). Five patients were excluded during follow-up (two declined postoperative MRI scans, and three refused postoperative neuropsychological assessments). A total of 181 patients were included in the final analysis (88 in Group C and 93 in Group E). The baseline characteristics revealed that patients in Group E were significantly older (P=0.03) and had lower educational attainment (P=0.01) than those in Group C (Table 1).
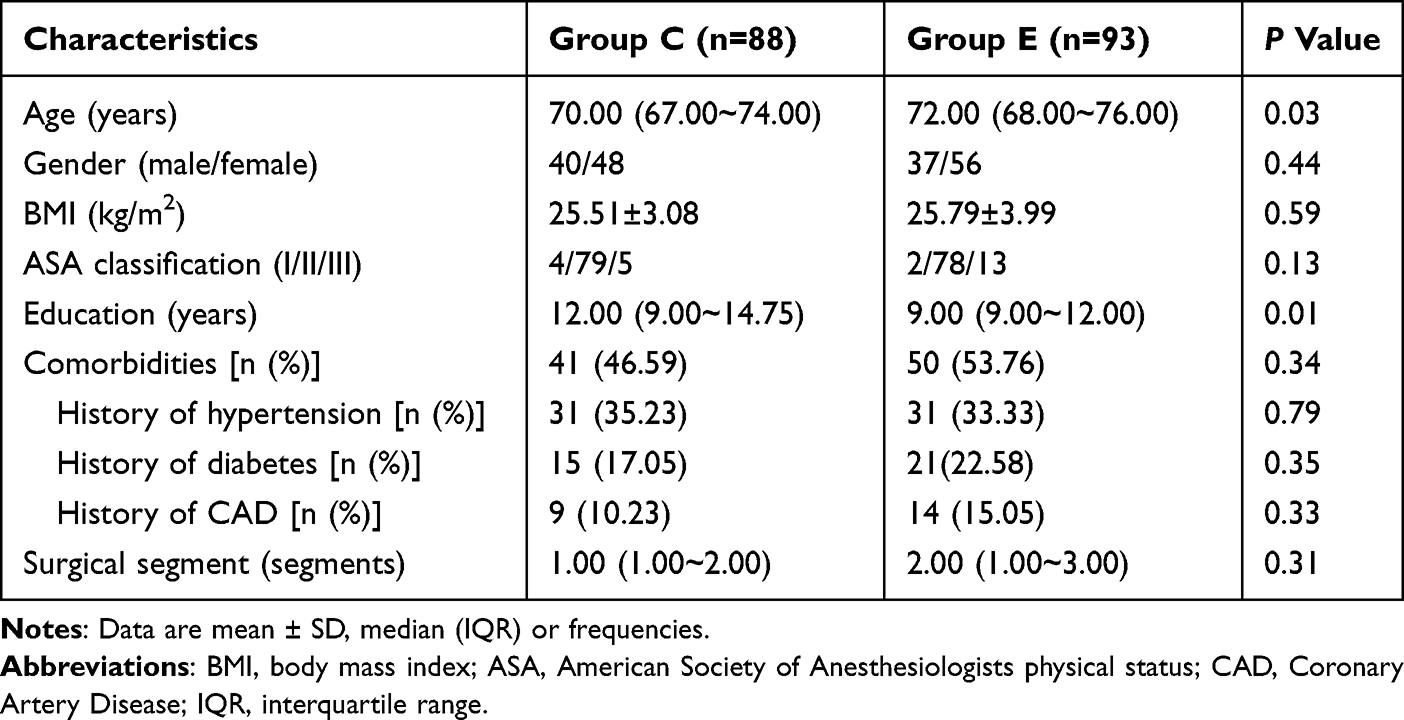 |
Table 1 Patients’ Demographic Characteristic Data |
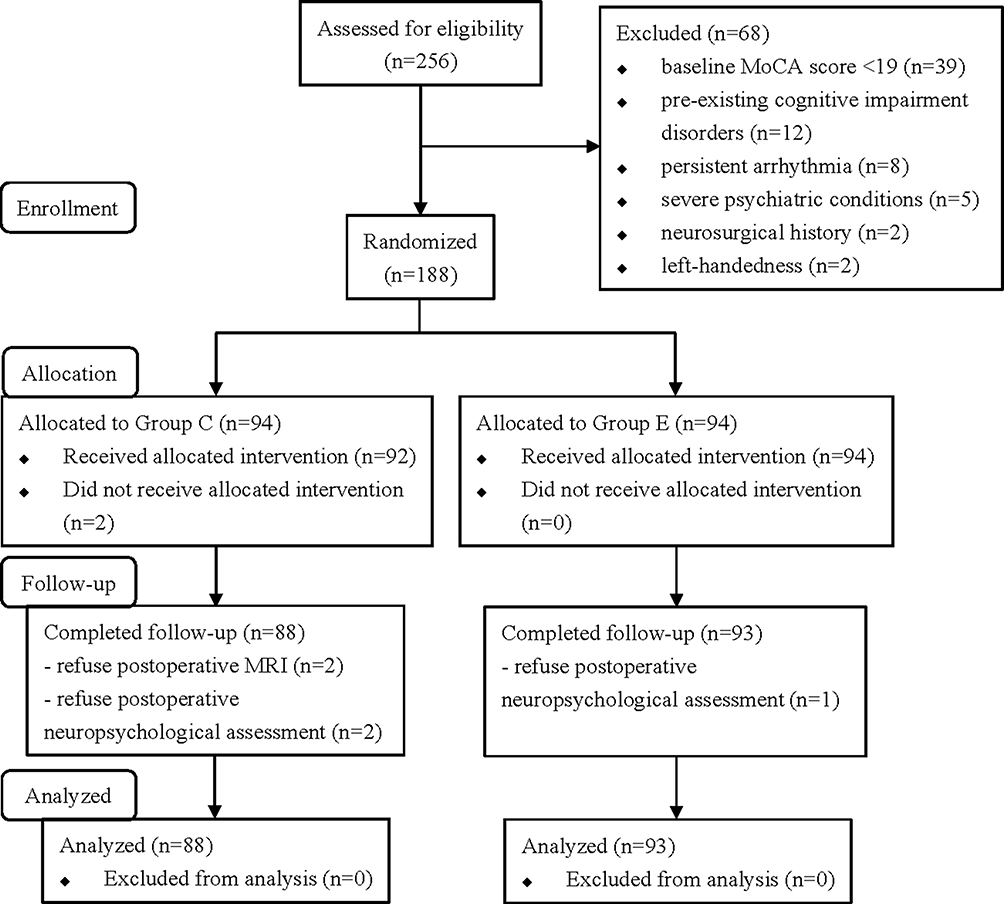 |
Figure 2 Study flow diagram. Abbreviations: MoCA, Montreal Cognitive Assessment; MRI, magnetic resonance imaging. |
Cognitive Outcomes
Preoperative (POD-1) and postoperative (POD7) MoCA scores showed no significant intergroup difference (Table 2). While Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), this difference based on Z-score analysis did not achieve statistical significance.
 |
Table 2 MoCA Scores and Incidence of PND |
Neuroimaging Findings
No baseline differences in the preoperative fALFF values were observed between the groups. At POD7, Group E exhibited a significantly increased fALFF in the left cuneus compared to Group C (GRF-corrected; Table 3 and Figure 3A).
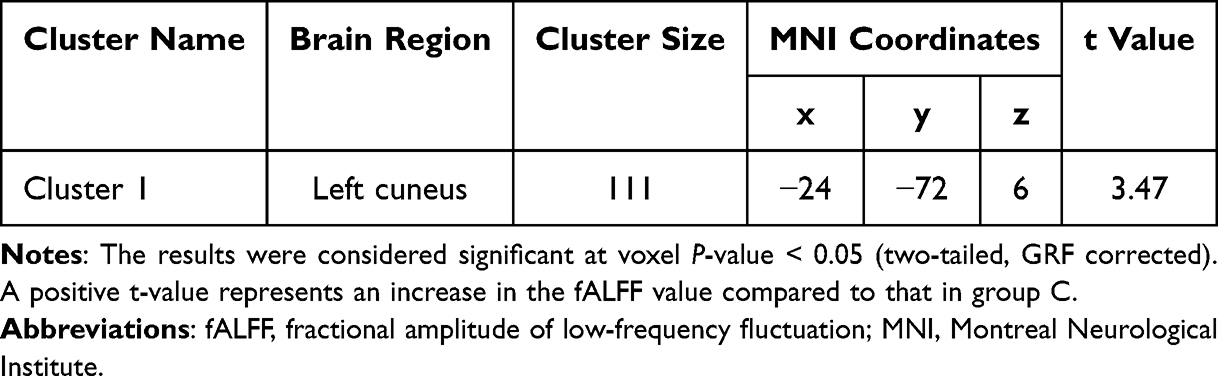 |
Table 3 Regions Showing Significant Differences in fALFF Analysis Between Group C and Group E at 7 Days After Surgery |
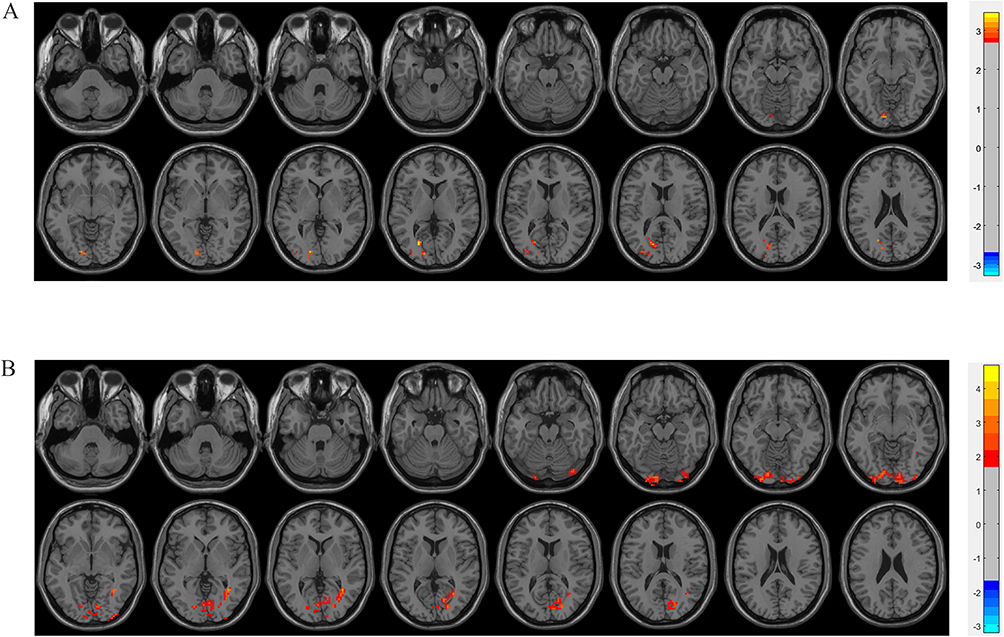 |
Figure 3 Neuroimaging Findings. (A) Significant differences of fALFF between Group E and Group C at 7 days following surgery (voxel P-value < 0.05, GRF corrected). Group E showed increased fALFF in the left cuneus compared to Group C (shown in warm colors). (B) Significant differences in FC between Group E and Group C at 7 days following surgery (voxel P-value < 0.05, GRF corrected). Group E showed increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule compared to Group C (shown in warm colors). The numerical indicators refer to t values. Abbreviations: fALFF, fractional amplitude of low-frequency fluctuations; FC, functional connectivity. |
No baseline differences in the preoperative FC values were observed between the groups. Seed-based FC analysis using the mPFC as the seed region revealed enhanced FC in Group E within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (GRF-corrected; Table 4 and Figure 3B).
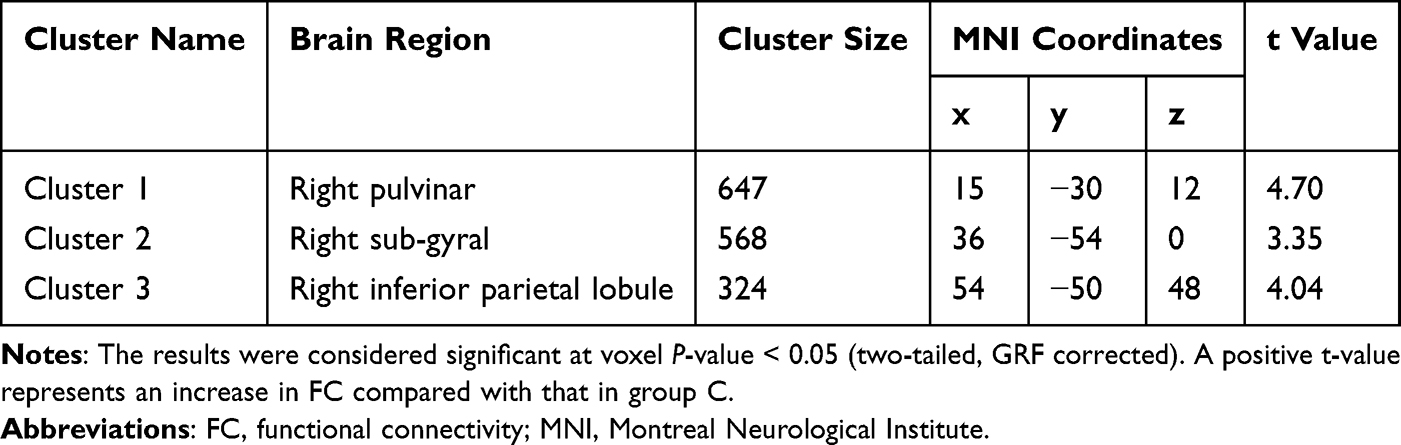 |
Table 4 Regions Showing Significant Difference in FC Analysis Between Group C and Group E at 7 Days After Surgery |
Inflammatory Markers
Quantitative analysis of serum CRP, LPS, and ZO-1 revealed no statistically significant intergroup differences at the preoperative and postoperative time points (Table 5). ΔCRP, ΔLPS, and ΔZO-1 (calculated as CRP [POD-1] − CRP [POD1], LPS [POD-1] − LPS [POD1], and ZO-1 [POD-1] − ZO-1 [POD1], respectively) did not differ between the groups. Notably, the postoperative CRP levels increased from baseline in Group E (P<0.001) but decreased in Group C (P<0.001). No significant perioperative changes were observed in the LPS or ZO-1 levels.
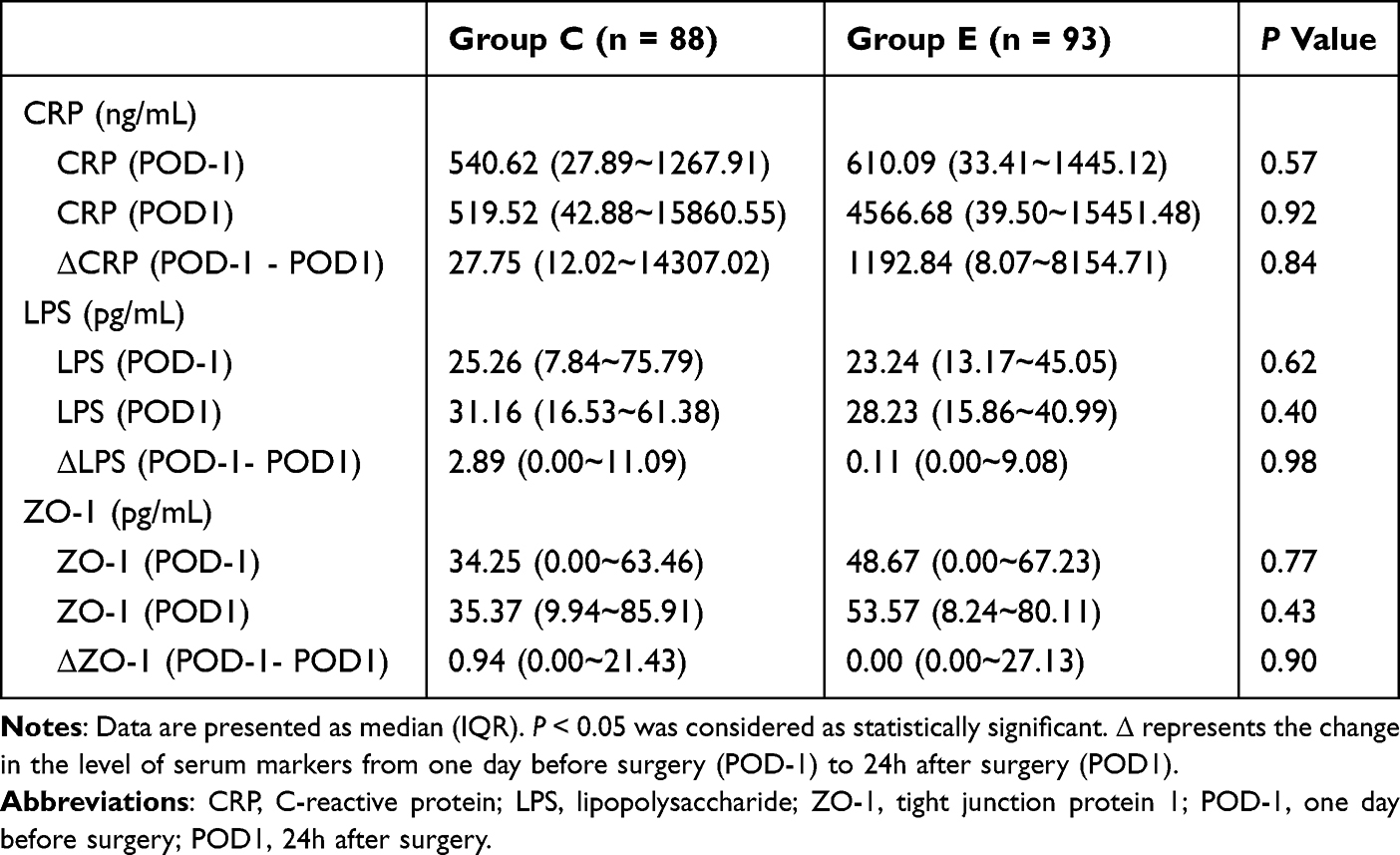 |
Table 5 Serum Markers in Two Groups |
Surgical Parameters and Postoperative Recovery
Intraoperative variables, including surgical/anesthesia duration, fluid balance, blood loss, and anesthetic agent consumption, were comparable between the groups (Table 6).
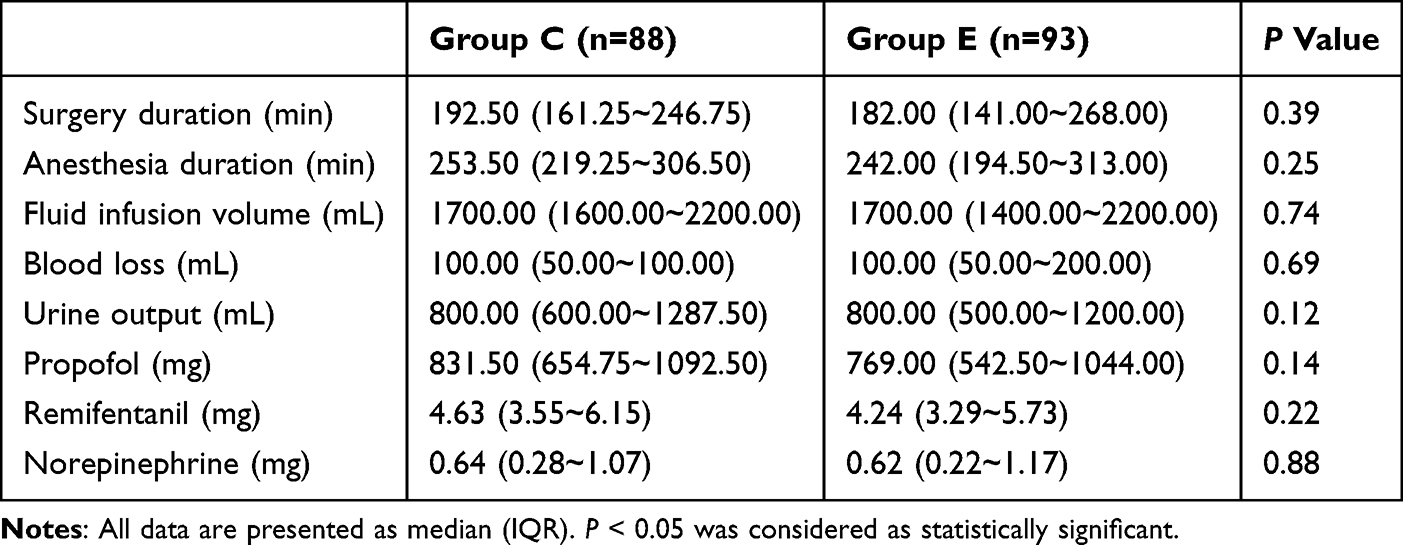 |
Table 6 Intraoperative Data in Two Groups |
Pain assessment demonstrated significantly lower NRS scores in Group E at rest (1h: P=0.04; 24h: P=0.04) and during movement (1h: P=0.03) postoperatively (Figure 4A and B). Correlation analysis revealed positive associations between z-transformed FC in cluster 3 and 1h postoperative pain scores (at rest: R=0.64, P=0.01; during movement: R=0.58, P=0.02; Table 7).
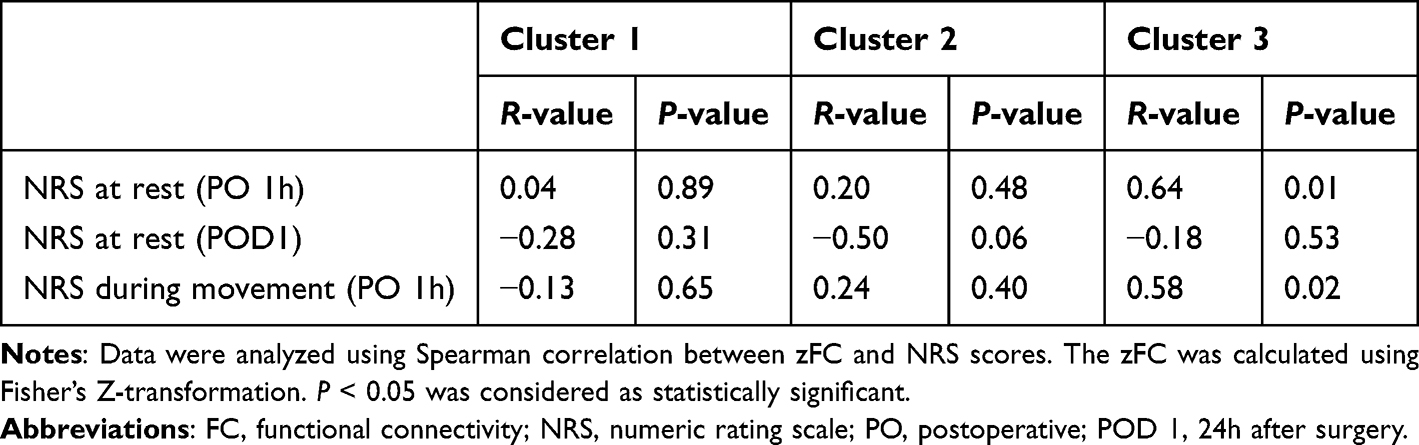 |
Table 7 Correlation Between FC and NRS Scores |
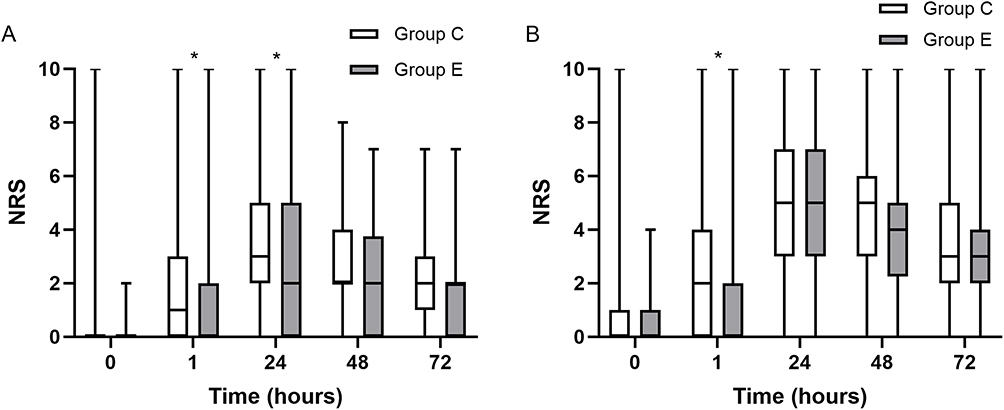 |
Figure 4 NRS scores following surgery. (A) NRS scores at rest following surgery. (B) NRS scores during movement following surgery. Asterisks represented statistically significant difference between Group E and Group C: *P < 0.05. |
No significant differences were observed in opioid consumption, gastrointestinal recovery, length of hospital stay, cost, or incidence of complications (wound infection, emergence delirium, and renal failure) between the groups (Table 8). None of the patients in either group died within 30 days postoperatively.
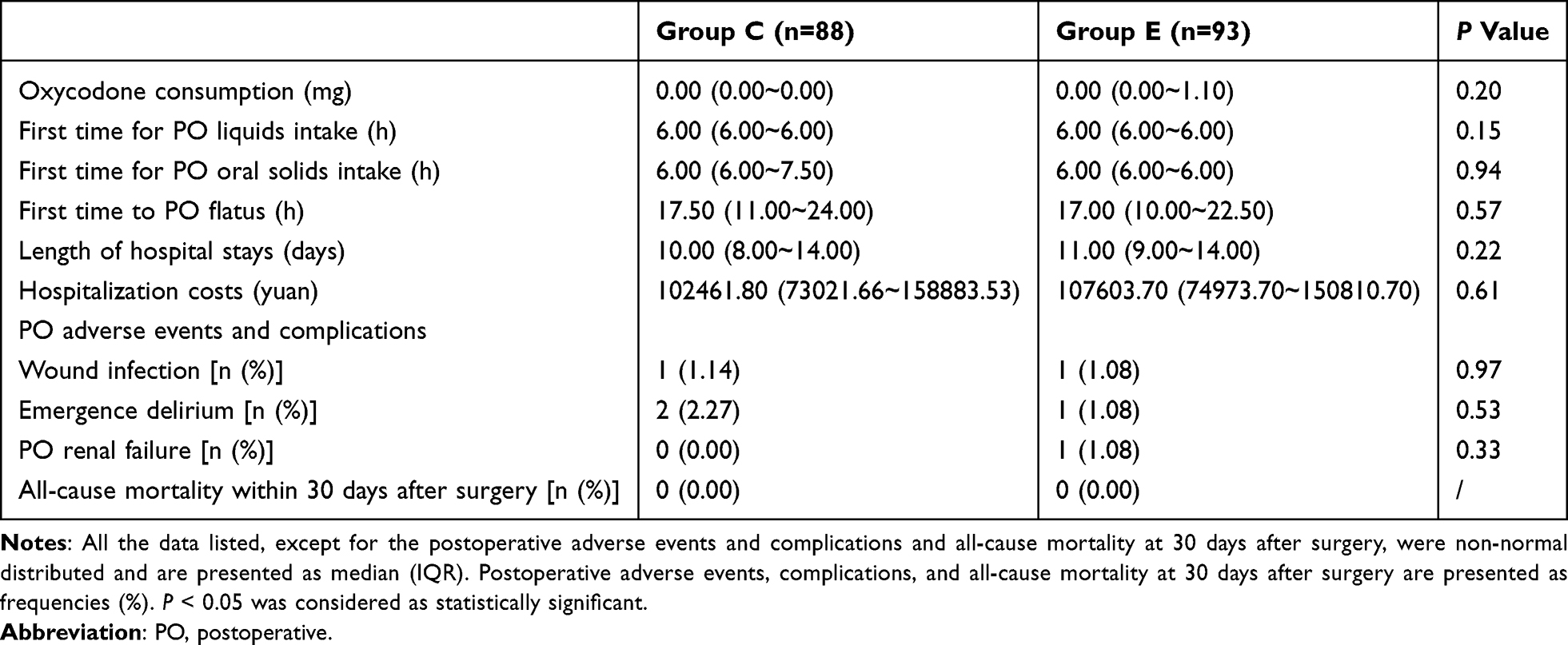 |
Table 8 Postoperative Rehabilitation Indicators in Two Groups |
Discussion
In the present study, anesthesia management guided by multimodal brain monitoring was demonstrated to enhance cerebral FC in cognition-related regions and mitigate surgical/anesthetic-induced disruptions to neural networks compared with conventional BIS-guided anesthesia in elderly patients undergoing lumbar fusion surgery. The observed intergroup differences may be attributed to the reduced postoperative pain-mediated cerebral stress in the intervention group.
This investigation focused on elderly patients requiring lumbar fusion procedures, a population particularly susceptible to PND as evidenced by our previous research documenting significant cognitive decline following spinal surgeries.3 The intervention we used in this study was multimodal brain monitoring-guided anesthesia management, which including the continuous monitoring and adjustment of sedation depth, analgesia depth, cerebral oxygenation and nasopharyngeal temperature. This intervention can regulate cerebral stress caused by inappropriate sedation depth, pain, and cerebral oxygen supply-demand imbalance during surgery under general anesthesia—all of which could impair cognitive function. Compared with BIS-guided anesthesia management, which focuses solely on the patient’s intraoperative sedation depth, multimodal brain monitoring-guided anesthesia management enables procedural, individualized, and real-time regulation during surgery and holds promise for improving patients’ postoperative cognitive function. Building upon preliminary findings from our pilot study suggesting potentially enhanced FC in cognition-related brain regions by multimodal brain monitoring,9 the current work extends these observations while acknowledging the need for further mechanistic clarifications.
Optimization of the depth of anesthesia is crucial for elderly patients. In elderly patients undergoing major noncardiac surgery, deep sedation increases the risk of postoperative delirium and PND by three months postoperatively compared with light sedation.14 Age-related decline in brain function and heightened anesthetic sensitivity predispose elderly patients to electroencephalographic burst suppression during excessive sedation, which is a known risk factor for PND.15 Conventional BIS monitoring demonstrates reduced reliability in geriatric populations due to characteristic electroencephalogram (EEG) alterations, particularly diminished alpha-band power.16
Cerebral oxygen supply and demand imbalance as well as pain can lead to brain stress, affecting EEG patterns and postoperative cognitive function. Insufficient oxygen delivery may impair postoperative cognitive function. A previous study demonstrated that elderly patients with a high oxygen desaturation index exhibit poorer working memory and visual memory recall in neuropsychological assessments.7 Additionally, anesthesia management guided by rSO2 could improve memory scores at 6 months postoperatively.5
Pain can influence EEG activity and lead to cognitive dysfunction. Preclinical evidence has revealed that unmanaged perioperative pain induces postoperative deficits in trace and contextual memory, whereas adequate analgesia mitigates surgery-induced memory impairments in rat model.4 Clinical research has also indicated that even during interictal periods, migraine sufferers exhibit specific cognitive impairments.8 Pain can also lead to changes in the brain networks. In the population of chronic pain patients, it was found that the activation of brain network connections in PFC (especially in the dorsolateral and ventral prefrontal cortex) increased.6 Recently, a meta-analysis17 revealed that postoperative pain intensity was associated with the occurrence and risk of developing postoperative delirium, which was defined as PND in our study. As revealed by our results, multimodal brain monitoring-guided anesthesia management has achieved a trend toward reducing PND occurrence by mitigating postoperative acute pain.
Considering the limitations of conventional anesthesia management that relies solely on BIS monitoring, we developed a multimodal brain monitoring-guided anesthesia management protocol.9 The results of our study indicated that Group E comprised older individuals with a lower education level. Although the primary outcome of this study, which is the difference of PND incidence between groups, did not reach statistical significance, we observed a numerical reduction in the incidence in the intervention group. While the current data are insufficient to draw definitive conclusions, they suggest that multimodal brain monitoring-guided anesthesia management may offer clinically relevant benefits in reducing the incidence of PND among elderly patients with low educational levels.
Fractional ALFF, a normalized index derived from ALFF, is a stable and reliable indicator.18,19 This metric reflects neural activity through the lens of brain energy metabolism, and thereby, fALFF enhances the sensitivity and specificity in the detection of spontaneous brain activity compared to conventional ALFF measures.20 The identification of regional abnormalities has significant clinical value with potential applications extending from research settings to real-world clinical practice. Notably, brain regions with elevated fALFF values concurrently exhibited increased network centrality, which is a graph-theoretical measure of node importance. fALFF may contribute to the functional integration of brain networks.21,22
The left cuneus, a critical neural substrate for cognitive processing, is specifically implicated in working memory. Neurogenetic studies have revealed that the morphological characteristics of this region mediate the genetic influences on working memory performance.23 The left cuneus plays an essential role in human cognition through its dual capacity to temporarily store and operationally process information, facilitating essential mental activities including reasoning, comprehension, and learning.24 Previous studies have demonstrated that the fALFF values in the cuneus exhibit a decreasing trend, corresponding to cognitive function decline.25,26 Our findings, which revealed that management guided by multimodal brain monitoring may effectively modulate regional neural activity in cognition-related brain regions, are consistent with those of previous studies.
From a whole-brain perspective, interdependent fluctuations in blood oxygenation level-dependent (BOLD) signals across distinct brain regions were quantified using FC. FC has been widely used to investigate functional alterations in patients with cognitive dysfunction.27 FC analysis frequently detects functional reorganization patterns and elucidates whether interregional connectivity demonstrates pathological disruption or adaptive compensation.28
Given our hypothesis that multimodal brain monitoring-guided management may enhance patients’ FC through attenuation of pain-induced cerebral stress, and considering the established dual role of the medial prefrontal cortex (mPFC) in both pain processing and cognitive regulation,29,30 we selected the mPFC as the seed region for analysis. Our findings revealed enhanced FC between the mPFC and three right-hemisphere regions: the pulvinar nucleus, subgyral area, and inferior parietal lobule (IPL) in patients undergoing multimodal brain monitoring.
Consistent with its anatomical connectivity patterns, the pulvinar is widely regarded as a thalamic structure that specializes in the broad dissemination of information throughout the cerebral cortex.31 The pulvinar plays an important role in visual attention; in patients with pulvinar lesions, attentional deficits can be severe.32 Regarding the subgyral region, prior neuroimaging evidence indicated its hypoactivation during working memory impairments while paradoxically demonstrating negative correlations between FC strength (subgyral-declive connectivity) and cognitive performance.33 This evidence suggests a regulatory role for the sub-gyral region in cognitive networks. The functional profile of the IPL encompasses attentional reorientation and memory retrieval processes.34 Another age-related study demonstrated that the mPFC-IPL FC can be enhanced through cognitive training interventions.35
Collectively, our results demonstrated FC augmentation between the mPFC and these cognition-associated regions, thereby providing preliminary neurophysiological evidence that multimodal monitoring-based management may optimize cerebral network integration through mPFC-mediated pathways.
Yang et al36 demonstrated dynamic alterations in the brain functional network activity and clinical manifestations in patients with acute ocular pain. Their findings revealed elevated degree centrality (DC) values in the inferior parietal lobule (IPL). Their findings also demonstrated that visual analog scale (VAS) scores were significantly positively correlated with the left IPL signal intensity in the affected cohort. DC, a graph-theoretical metric, quantifies the total number of direct connections between a given voxel and all other cerebral voxels, without requiring predefined nodes or regions of interest.37 Expanding on this methodological framework, our investigation employed FC analysis, a distinct whole-brain network assessment approach. Consistent findings were observed in our study, and we identified a positive association between right IPL FC strength and postoperative NRS scores, which objectively quantified acute pain intensity. However, because the FC-enhancing effect of multimodal brain monitoring-guided anesthesia management masked the FC-reducing effect of low pain scores in this group, the FC strength in Group E ultimately appeared higher than that in Group C.
This study had several limitations. First, preoperative NRS scores were not systematically recorded in our dataset. Candidates for lumbar fusion surgery typically exhibit varying severities of chronic pain syndrome, which may substantially modulate individual pain-perception thresholds. Such pre-existing neurological sensitization could potentially confound the interpretation of the postoperative pain assessments. Second, the single-center design, with participants recruited exclusively from one tertiary care institution, introduces a potential selection bias and limits the generalizability of the findings to broader populations. Regional practice patterns and institutional-specific surgical protocols may influence patient selection and outcomes. Third, we only assessed the incidence of PND at 7 days after surgery, therefore, our study cannot reveal the long-term evolutionary trends, duration, or impact of PND on patients’ long-term quality of life and recovery. Future research should include longer follow-up periods to comprehensively evaluate the long-term neurocognitive functional outcomes.
Conclusion
In conclusion, multimodal brain monitoring-guided anesthesia management demonstrated dual neuroprotective effects by enhancing functional connectivity within cognition-associated cerebral networks and attenuating postoperative acute pain. The observed trend toward reduced PND occurrence may be partially mediated by postoperative pain mitigation pathways. Our findings provide a clinical framework for optimizing perioperative cognitive protection strategies through simultaneous modulation of cerebral network dynamics and nociceptive processing. Implementation of this approach is expected to establish a scalable standard protocol for the prevention and management of postoperative neurocognitive disorders in the future and may substantially improve neurocognitive outcomes in geriatric surgical patients while advancing precision anesthesia paradigms.
Data Sharing Statement
The datasets of this study are available from the corresponding author (Wei Xiao) on reasonable request.
Acknowledgments
We extend our sincere gratitude to the participating physicians, research assistants from Xuanwu Hospital’s Department of Neurosurgery, and operating room nurses for their invaluable contribution and collaborative support.
Funding
This work was supported by the National Natural Science Foundation of China [grant number 82301440]; Capital’s Funds for Health Improvement and Research [grant number 2022-2-1032].
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could influence the work reported in this study.
References
1. Subramaniyan S, Terrando N. Neuroinflammation and perioperative neurocognitive disorders. Anesth Analg. 2019;128(4):781–788. doi:10.1213/ane.0000000000004053
2. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br J Anaesth. 2018;121(5):1005–1012. doi:10.1016/j.bja.2017.11.087
3. Zhang M, Zhang YH, Fu HQ, et al. Ulinastatin may significantly improve postoperative cognitive function of elderly patients undergoing spinal surgery by reducing the translocation of Lipopolysaccharide and systemic inflammation. Front Pharmacol. 2018;9:1007. doi:10.3389/fphar.2018.01007
4. Koyama T, Kawano T, Iwata H, et al. Acute postoperative pain exacerbates neuroinflammation and related delirium-like cognitive dysfunction in rats. J Anesth. 2019;33(3):482–486. doi:10.1007/s00540-019-02635-3
5. Uysal S, Lin HM, Trinh M, et al. Optimizing cerebral oxygenation in cardiac surgery: a randomized controlled trial examining neurocognitive and perioperative outcomes. J Thorac Cardiovasc Surg. 2020;159(3):943–953.e943. doi:10.1016/j.jtcvs.2019.03.036
6. Nascimento SS, Oliveira LR, DeSantana JM. Correlations between brain changes and pain management after cognitive and meditative therapies: a systematic review of neuroimaging studies. Complement Ther Med. 2018;39:137–145. doi:10.1016/j.ctim.2018.06.006
7. Naismith SL, Duffy SL, Cross N, et al. Nocturnal hypoxemia is associated with altered Parahippocampal functional brain connectivity in older adults at risk for Dementia. J Alzheimers Dis. 2020;73(2):571–584. doi:10.3233/jad-190747
8. Lo Buono V, Bonanno L, Corallo F, et al. Cognitive functions and psychological symptoms in migraine: a study on patients with and without aura. Int J Neurosci. 2019;129(6):588–592. doi:10.1080/00207454.2018.1554658
9. Yang S, Xiao W, Wu H, et al. Management based on multimodal brain monitoring may improve functional connectivity and post-operative neurocognition in elderly patients undergoing spinal surgery. Front Aging Neurosci. 2021;13:705287. doi:10.3389/fnagi.2021.705287
10. Fu HQ, Yang T, Xiao W, et al. Prolonged neuroinflammation after lipopolysaccharide exposure in aged rats. PLoS One. 2014;9(8):e106331. doi:10.1371/journal.pone.0106331
11. Biswal B, Yetkin FZ, Haughton VM, et al. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med. 1995;34(4):537–541. doi:10.1002/mrm.1910340409
12. Huang H, Tanner J, Parvataneni H, et al. Impact of total knee arthroplasty with general anesthesia on brain networks: cognitive efficiency and ventricular volume predict functional connectivity decline in older adults. J Alzheimers Dis. 2018;62(1):319–333. doi:10.3233/jad-170496
13. Persson J, Pudas S, Nilsson LG, et al. Longitudinal assessment of default-mode brain function in aging. Neurobiol Aging. 2014;35(9):2107–2117. doi:10.1016/j.neurobiolaging.2014.03.012
14. Cottrell JE, Hartung J. Anesthesia and cognitive outcome in elderly patients: a narrative viewpoint. J Neurosurg Anesthesiol. 2020;32(1):9–17. doi:10.1097/ana.0000000000000640
15. Momeni M, Meyer S, Docquier MA, et al. Predicting postoperative delirium and postoperative cognitive decline with combined intraoperative electroencephalogram monitoring and cerebral near-infrared spectroscopy in patients undergoing cardiac interventions. J Clin Monit Comput. 2019;33(6):999–1009. doi:10.1007/s10877-019-00253-8
16. Purdon PL, Pavone KJ, Akeju O, et al. The ageing brain: age-dependent changes in the electroencephalogram during propofol and sevoflurane general anaesthesia. Br J Anaesth. 2015;115(Suppl 1):i46–i57. doi:10.1093/bja/aev213
17. Khaled M, Sabac D, Fuda M, et al. Postoperative pain and neurocognitive outcomes after noncardiac surgery: a systematic review and dose-response meta-analysis. Br J Anaesth. 2025;134(1):89–101. doi:10.1016/j.bja.2024.08.032
18. Küblböck M, Woletz M, Höflich A, et al. Stability of low-frequency fluctuation amplitudes in prolonged resting-state fMRI. Neuroimage. 2014;103:249–257. doi:10.1016/j.neuroimage.2014.09.038
19. Zuo XN, Di Martino A, Kelly C, et al. The oscillating brain: complex and reliable. Neuroimage. 2010;49(2):1432–1445. doi:10.1016/j.neuroimage.2009.09.037
20. Zou QH, Zhu CZ, Yang Y, et al. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J Neurosci Methods. 2008;172(1):137–141. doi:10.1016/j.jneumeth.2008.04.012
21. Sato JR, Biazoli CE, Moura LM, et al. Association between fractional amplitude of low-frequency spontaneous fluctuation and degree centrality in children and adolescents. Brain Connect. 2019;9(5):379–387. doi:10.1089/brain.2018.0628
22. Di X, Kim EH, Huang CC, et al. The influence of the amplitude of low-frequency fluctuations on resting-state functional connectivity. Front Hum Neurosci. 2013;7:118. doi:10.3389/fnhum.2013.00118
23. He X, Li X, Fu J, et al. The morphometry of left cuneus mediating the genetic regulation on working memory. Hum Brain Mapp. 2021;42(11):3470–3480. doi:10.1002/hbm.25446
24. Baddeley A. Working memory. Curr Biol. 2010;20(4):R136–140. doi:10.1016/j.cub.2009.12.014
25. Yang L, Yan Y, Li Y, et al. Frequency-dependent changes in fractional amplitude of low-frequency oscillations in Alzheimer’s disease: a resting-state fMRI study. Brain Imaging Behav. 2020;14(6):2187–2201. doi:10.1007/s11682-019-00169-6
26. Wang X, Wei W, Bai Y, et al. Intrinsic brain activity alterations in patients with Parkinson’s disease. Neurosci Lett. 2023;809:137298. doi:10.1016/j.neulet.2023.137298
27. Cha J, Hwang JM, Jo HJ, et al. Assessment of functional characteristics of Amnestic mild cognitive impairment and Alzheimer’s disease using various methods of resting-state FMRI analysis. Biomed Res Int. 2015;2015:907464. doi:10.1155/2015/907464
28. Liu Y, Chen Y, Liang X, et al. Altered resting-state functional connectivity of multiple networks and disrupted correlation with executive function in major depressive disorder. Front Neurol. 2020;11:272. doi:10.3389/fneur.2020.00272
29. Ong WY, Stohler CS, Herr DR. Role of the prefrontal cortex in pain processing. Mol Neurobiol. 2019;56(2):1137–1166. doi:10.1007/s12035-018-1130-9
30. Jahn A, Nee DE, Alexander WH, et al. Distinct regions within medial prefrontal cortex process pain and cognition. J Neurosci. 2016;36(49):12385–12392. doi:10.1523/jneurosci.2180-16.2016
31. Bridge H, Leopold DA, Bourne JA. Adaptive pulvinar circuitry supports visual cognition. Trends Cognit Sci. 2016;20(2):146–157. doi:10.1016/j.tics.2015.10.003
32. Karnath HO, Himmelbach M, Rorden C. The subcortical anatomy of human spatial neglect: putamen, caudate nucleus and pulvinar. Brain. 2002;125(Pt 2):350–360. doi:10.1093/brain/awf032
33. Feng S, Yao H, Zheng S, et al. Altered functional connectivity in working memory network after acute sleep deprivation. Neuroscience. 2023;535:158–167. doi:10.1016/j.neuroscience.2023.11.003
34. Kizilirmak JM, Rösler F, Bien S, et al. Inferior parietal and right frontal contributions to trial-by-trial adaptations of attention to memory. Brain Res. 2015;1614:14–27. doi:10.1016/j.brainres.2015.04.012
35. Lee ATC, Luo Y, Huo Z, et al. Effect of increasing cognitive activity participation on default mode network in older adults with subjective cognitive decline: a randomised controlled trial. EBioMedicine. 2024;102:105082. doi:10.1016/j.ebiom.2024.105082
36. Yang YC, Cai GQ, Yang QC, et al. Brain functional connectivity changes in patients with acute eye pain: a resting-state functional magnetic resonance imaging (fMRI) study. Med Sci Monit. 2021;27:e930588. doi:10.12659/msm.930588
37. Zuo XN, Ehmke R, Mennes M, et al. Network centrality in the human functional connectome. Cereb Cortex. 2012;22(8):1862–1875. doi:10.1093/cercor/bhr269
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.