Back to Journals » International Medical Case Reports Journal » Volume 15
Multidrug-Resistant Corynebacterium striatum Developed During Treatment of Ommaya Reservoir Infection
Authors Kurimoto T, Cho Y, Matsuoka T
Received 19 February 2022
Accepted for publication 27 April 2022
Published 3 May 2022 Volume 2022:15 Pages 231—234
DOI https://doi.org/10.2147/IMCRJ.S361505
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Tomonori Kurimoto, Yoshiaki Cho, Takashi Matsuoka
Department of Pediatrics, Okinawa Prefectural Nanbu Medical Center and Children’s Medical Center, Okinawa, 901-1193, Japan
Correspondence: Tomonori Kurimoto, Okinawa Prefectural Nanbu Medical Center and Children’s Medical Center, 118-1, Shinkawa, Haebaru-cho, Shimajiri-gun, Okinawa, 901-1193, Japan, Tel +81-98-888-0123, Fax +81-98-888-6400, Email [email protected]
Abstract: Corynebacterium striatum, a common component of the skin and mucosal microbiota of both immunocompetent and immunocompromised individuals, has become an emerging pathogen, colonizing indwelling medical devices and causing infections at multiple sites. A 3-year-old boy with an Ommaya reservoir in the right ventricle and a medical history of grade 3 intraventricular hemorrhage, Hirschsprung disease, catheter-related methicillin-resistant Staphylococcus aureus bacteremia, and congenital central hypoventilation syndrome was hospitalized for Ommaya reservoir infection with C. striatum. He was treated with ampicillin, to which the initial isolate was susceptible. C. striatum may have acquired multiple-drug resistance during the antibiotic treatment due to biofilm production. The Ommaya reservoir was replaced by external ventricular drainage. Cultures of the removed Ommaya reservoir, and cerebrospinal fluid samples grew C. striatum, which was susceptible to meropenem and vancomycin and resistant to other antibiotics. The antibiotic was switched to vancomycin to treat this new multidrug-resistant strain. After 8 days of vancomycin treatment, the cerebrospinal fluid culture obtained by a lumbar puncture was negative for C. striatum. In cases of device-associated infections caused by biofilm-producing bacteria, it is desirable to remove the device as soon as possible.
Keywords: coryneform bacterium, biofilm, antibiotic resistant, vancomycin
Introduction
Corynebacterium striatum is a coryneform bacterium occasionally isolated in clinical microbiology laboratories. It is a common component of the skin and mucosal microbiota of immunocompetent and immunocompromised individuals. Little is known about the pathogenic role of C. striatum as it has long been considered a skin contaminant with little or no pathogenic potential.1 Using new analytical tests such as matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS), suspicious isolates of infection, routinely isolated from patient samples of skin and mucosa and considered contaminants before, are now routinely identified to the species level. Organisms deemed clinically significant include C. striatum in multiple sites. These results portray C. striatum as an emerging pathogen in multiple infection sites and a colonizer of indwelling medical devices.2 Moreover, C. striatum strains capable of forming biofilm may be selected under antibiotic pressure and develop antibiotic resistance. Conversely, C. striatum may acquire resistance to multiple drugs within biofilm-producing populations.3 There are no international guidelines for managing infections associated with the Ommaya reservoir. To the best of our knowledge, we report the first pediatric case of multidrug-resistant C. striatum developed during the treatment of Ommaya reservoir infection.
Case Report
A 3-year-old boy with an Ommaya reservoir in his right ventricle presented to our hospital with a fever. The reservoir was used to prevent hydrocephalus after a ventriculoperitoneal (VP) shunt removal placed after a grade 3 intraventricular hemorrhage. He also had a right subclavian portal catheter placed 2 years previously due to Hirschsprung disease (entire colon type). He had a history of catheter-related methicillin-resistant Staphylococcus aureus (MRSA) bacteremia. He was mechanically ventilated through a tracheostomy because of congenital central hypoventilation syndrome. On examination, he had a fever of 38.8°C and erythema around the Ommaya reservoir. Hematology showed a white blood cell count of 9260 cells/mL with 50% neutrophils. Cerebrospinal fluid (CSF) from the Ommaya reservoir showed a leukocyte count of 6 cells/mL (40% neutrophils and 60% lymphocytes) and Gram-positive bacilli on Gram stain. Empiric intravenous treatment was initiated with 300 mg/kg/day of cefotaxime for Ommaya reservoir infection.
After 3 days of cefotaxime treatment, his fever persisted. Therefore, considering the patient’s history of catheter-associated MRSA bacteremia, two sets of blood cultures were drawn, one from a peripheral site and another from the indwelling vascular catheter. A second CSF sample from the Ommaya reservoir was obtained, and antibiotic treatment was switched from cefotaxime to vancomycin (20 mg/kg/day) and meropenem (120 mg/kg/day). The CSF from the Ommaya reservoir showed the following features: glucose concentration, 55 mg/dL with blood glucose of 101 mg/dL; protein concentration, 40 mg/dL; and leukocyte count, 194/mL (81% neutrophils and 19% lymphocytes). Three days later, C. striatum was identified in CSF cultures. Antibiotic susceptibility testing (BD Phoenix automated microbiology systems) revealed that the strain was susceptible to penicillin, amino benzylpenicillin, cefotaxime, cefepime, sulbactam/ampicillin, imipenem/cilastatin, meropenem, erythromycin, clindamycin, levofloxacin, and vancomycin and was resistant to sulfamethoxazole/trimethoprim.
Thus, vancomycin and meropenem were de-escalated to 400 mg/kg/day of ampicillin.
Ampicillin treatment was continued for 2 weeks. A CSF culture obtained on day 6 of ampicillin treatment was negative for C. striatum; thus, the Ommaya reservoir was removed and replaced by external ventricular drainage. However, cultures of the removed Ommaya reservoir, and CSF samples grew C. striatum, which was susceptible to meropenem and vancomycin and resistant to the other antibiotics tested (Table 1). Vancomycin was initiated to treat this new C. striatum meningitis strain, and after 8 days of treatment, the CSF culture from lumbar puncture was negative for C. striatum. External ventricular drainage was removed after confirmation that the ventricular enlargement had not progressed.
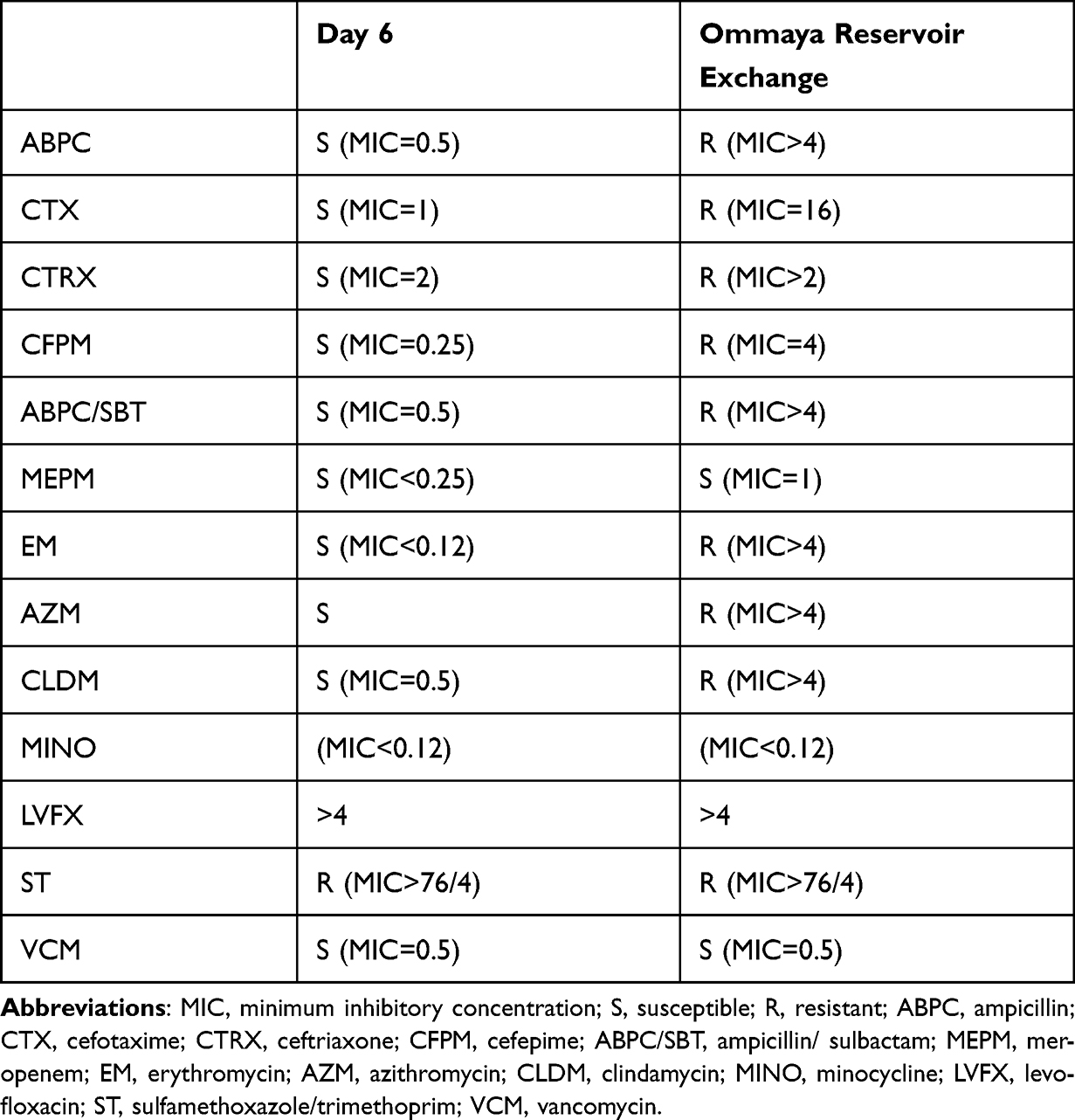 |
Table 1 Antibiotic Sensitivity of C. striatum |
The patient was discharged from the hospital after confirming that there was no residual infection or ventricular enlargement.
Discussion
Historically, C. striatum has been shown to be uniformly susceptible to vancomycin and other antibiotics with a wide range of Gram-positive activity. Resistance to penicillin, ciprofloxacin, erythromycin, clindamycin, and tetracycline has been demonstrated, and oral antibiotic options for treatment are limited.4 In this case, Ommaya reservoir infection was treated with ampicillin following the microbial susceptibility findings, at a dose appropriate for CNS penetration.5 No abscess was found on an MRI examination.
CSF cultures are the gold standard for diagnosing bacterial meningitis and are positive in 80–90% of the patients with acute community-acquired bacterial meningitis before the start of treatment.6 The CSF culture from the Ommaya reservoir was negative on day 6 of ampicillin treatment and remained negative on day 14. On day 15, the Ommaya reservoir was removed, and a new VP shunt was inserted. However, the Ommaya reservoir and CSF cultures were positive for C. striatum at removal. The newly identified strain had developed resistance to additional antibiotics but remained sensitive to meropenem and vancomycin.
Bacteria in biofilms are relatively resistant to antibiotic concentrations that would normally kill bacteria in free suspension; however, they are susceptible to supratherapeutic concentrations of antibiotics (approximately 100-fold higher than therapeutic plasma concentrations).7
Early removal of the Ommaya reservoir after diagnosis of device-associated infection shortens the length of hospital stay and duration of antibiotic use and enables early escape from life-threatening situations. Therefore, in this case, it was desired to remove the device as soon as possible after diagnosis.8,9
Comparing the susceptibility patterns of the two isolates (day 3 and day 9) did not demonstrate whether the two isolates have the same gene sequence. Therefore, the possibility that they were not the same strain cannot be denied. However, this pediatric case report adds a rare species to the list of possible pathogens in Ommaya reservoir infection.
Conclusion
In this case, the biofilm-producing C. striatum coated the inner lumen of the Ommaya reservoir. Moreover, it was unreachable by the antibiotic treatment, leading to the development of drug resistance. In cases of device-associated infections by biofilm-producing bacteria, it is desirable to remove the device as soon as possible.
Data Sharing Statement
Data ownership to support the results reported in the manuscript is owned by the institution and controlled by the research representative.
Statement of Ethics
This case study was conducted in accordance with the provisions of the Declaration of Helsinki, as revised in Tokyo in 2004, and was approved by the Ethics Committee of Okinawa Prefectural Nanbu Medical Center and Children’s Medical Center.
Patient Consent
Written informed consent was obtained from the patient’s parent to publish this report in accordance with the journal’s patient consent policy.
Acknowledgments
We would like to thank the pediatricians at Okinawa Prefectural Nanbu Medical Center and Children’s Medical Center for their valuable discussion contribution to the topic presented in this study and the hospital staff for taking care of the children in the hospital.
Author Contributions
T.K., Y.C. and T.M. conceptualized the study. T.K. and T.M. designed and executed the study and acquired, analyzed and interpreted the data. T.K. wrote and edited the manuscript. All authors took part in drafting, revising or critically reviewing the article and approved of the final manuscript to be published and agreed on the journal to which the article has been submitted and have agreed to be accountable for all aspects of this work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Funke G, von Graevenitz A, Clarridge JE, et al. Clinical microbiology of coryneform bacteria. Clin Microbiol Rev. 1997;10:125–159. doi:10.1128/CMR.10.1.125
2. Leal SM, Jones M, Gilligan PH. Clinical significance of commensal Gram-positive rods routinely isolated from patient samples. J Clin Microbiol. 2016;54(12):2928–2936. doi:10.1128/JCM.01393-16
3. Souza C, Faria YV, Sant’Anna Lde O, et al. Biofilm production by multiresistant Corynebacterium striatum associated with nosocomial outbreak. Mem Inst Oswaldo Cruz. 2015;110(2):242–248. doi:10.1590/0074-02760140373
4. Hahn WO, Werth BJ, Butler-Wu SM, Rakita RM. Multidrug-resistant Corynebacterium striatum associated with increased use of parenteral antimicrobial drugs. Emerg Infect Dis. 2016;22(11):1908–1914. doi:10.3201/eid2211.160141
5. van de Beek D, Brouwer MC, Thwaites GE, Tunkel AR. Advances in treatment of bacterial meningitis. Lancet. 2012;380(9854):1693–1702. doi:10.1016/S0140-6736(12)61186-6
6. Brouwer MC, Thwaites GE, Tunkel AR, van de Beek D. Dilemmas in the diagnosis of acute community-acquired bacterial meningitis. Lancet. 2012;380(9854):1684–1692. doi:10.1016/S0140-6736(12)61185-4
7. Allon M. Saving infected catheters: why and how. Blood Purif. 2005;23(1):23–28. doi:10.1159/000082007
8. Szvalb AD, Raad II, Weinberg JS, et al. Ommaya reservoir-related infections: clinical manifestations and treatment outcomes. J Infect. 2014;68(3):216–224.
9. Hosoda T, Katayama M. Epidemiology and prognosis of ommaya reservoir-related bacterial meningitis in adult patients with leptomeningeal metastases from solid tumors: a 10-year retrospective single-center study in Japan. J Infect Chemother. 2021;27(3):486–491. doi:10.1016/j.jiac.2020.10.025
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.