Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Multidisciplinary Management of Diabetic Foot Ulcers in Primary Cares in Quebec: Can We Do Better?
Authors Brousseau-Foley M ![]() , Blanchette V
, Blanchette V ![]()
Received 25 February 2020
Accepted for publication 27 March 2020
Published 16 April 2020 Volume 2020:13 Pages 381—385
DOI https://doi.org/10.2147/JMDH.S251236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Magali Brousseau-Foley,1,2 Virginie Blanchette2
1University Family Medicine Group, Faculty of Medicine Affiliated to Université De Montréal, Centre intégré universitaire de santé et de services sociaux de la Mauricie-et-du-Centre-du-Québec (CIUSSS-MCQ), Trois-Rivières, Québec, Canada; 2Department of Sciences of Physical Activity and Podiatric Medicine, Université du Québec à Trois-Rivières, Trois-Rivières, Québec, Canada
Correspondence: Virginie Blanchette
Department of Sciences of Physical Activity and Podiatric Medicine, Université du Québec à Trois-Rivières, 3351, Boul. Des Forges, C.P. 500, Trois-Rivières, Québec G9A 5H7 Tel +1-819-376-5011 Ext. 3756
Email [email protected]
Abstract: A growing body of evidence supports the presence of integrated foot care based on multidisciplinary and interdisciplinary teams in the management and prevention of diabetic foot ulcer (DFU) worldwide. This model of care is however rare in the clinical setting in Quebec, Canada. Many best practice gaps are identified as well as probable causal hypothesis are listed in this commentary. We support our opinions with a pilot audit conducted as part of a continuous quality improvement process in managing patients with DFU in our area and on Canadian facts and data. Our pilot study (n = 27 hospitalized patients) included a typical DFU population with neuropathy, peripheral arterial disease and previous amputation. It highlights underachievement of best practice recommendations implementation such as multidisciplinary DFU management and offloading interventions in our establishment. Due the high morbidity and mortality associated with DFU patients, four died during the studied hospitalization episode. Several barriers were encountered in the pilot audit justifying that no robust conclusion can be raised. However, our observations are concerning. Even though data accessibility was limited, our observations are sadly coherent with what is found in the literature. Economic data of what this means for our health system is put forward in the overall discussion. We are preoccupied by the trends outlined by some facts and observations, and this commentary was written with this in mind. In the face of the diabetes crisis that is arising, a plea is made to reassess care pathway for this vulnerable population as we emphasize the importance of teamwork in managing DFU.
Keywords: patient care team, teamwork, diabetes complications, foot ulcer, best practice recommendations, guidelines
Introduction
Diabetic foot publication count has increased significantly in the last decade which demonstrates the growing interest of clinicians and researchers on the topic of diabetic foot ulcer (DFU).1 This has led to the development of international and national clinical practice guidelines for the evaluation and treatment of DFU, all of them relying on a multi/interdisciplinary team approach.2,3 Indeed, it has been reported that integrated foot care based on multidisciplinary teams reduces complications such as total amputation number by 49% to 85% in the at-risk diabetic foot.2,4–6 Unfortunately, this supported model of care remains largely unachieved in many clinical practices. Even though few examples of established team approach DFU management teams can be found in Quebec, they should represent the norm not the exception.7–9 With that in mind, we need to ask ourselves if we can strive for an improved continuum of care for patients with DFU in Quebec’s and Canada’s public health systems? We firmly believe that we can do better and we should unequivocally improve our methods.10 To make a supportive argumentation about this relevant issue, with the approbation of the local director of professional services, we have conducted a pilot audit pertaining to DFU management at our general and specialized care hospital. Measurement of clinical services can be a challenge in the DFU population, but it remains essential if clinical services and patients’ outcomes are to be improved.10 We also focused on selected key indicators identified from the Canadian scientific literature to illustrate our position on this health issue in the discussion.
An Audit as Example
This pilot audit was led by family medicine residents and conducted as part of a continuous quality improvement process in managing patients with DFU in our area. Evaluation of DFU management was the main objective of this audit. The hospital approbation of the local director of professional services was obtained and an agreement was established for the data extraction and diffusion. The audit has used secondary data. For this reason, the present research did not require the educational institution ethics committee agreement since no medical procedure has been performed for the purpose of research and there was no patient enrolment. This audit is based on the examination of medical records in different healthcare settings in Trois-Rivières’ area (Québec, Canada) such as Family Medicine Groups (GMF), Local Community Service Centers (CLSC), outpatient visits to orthopedic, vascular and infectiology clinics and hospitalization episodes. Limited resources and obstacles encountered during data collection resulted in the analysis of hospitalization episodes over a 6-month period only. Even if electronic medical records are available in our establishment, they do not represent a database as they are made of scanned copies of hand-written documents which do not allow for computer searches with use of keywords. Our efforts were therefore hampered by the lack of accessibility of available information. However, we were able to identify potential medical records from hospitalization summaries coded for billing by medical archivists. Medical records of patients with codes for both “diabetes” and “wound” or “lower extremity infection” between January and June of 2018 were included in the initial inquiry resulting in 106 identified hospitalization episodes. After manually reviewing all medical records, 29 cases in 27 patients met inclusion criteria (diabetes treated with oral medications or insulin therapy, and DFU as one of the main diagnosis). A DFU was defined as a full-thickness break in the skin occurring on the plantar surface of either foot (sole, hallux and toes).2 There were no exclusion criteria. A preplanned extraction sheet was used for demographic data (age and sex), past medical history and comorbidities related to DFU (renal function, retinopathy, neuropathy, peripheral arterial disease, heart and vascular diseases, glycemic control, dyslipidemia, smoking, history of DFU and past amputation). Treatment targets were defined according to Diabetes Canada 2018 Clinical Practice Guidelines.11 Included patients’ characteristics are available in Table 1. Results were obtained from extracted available data with descriptive statistical analysis. We also examined available data of in- and outpatient interventions for DFU and in-hospital mortality.
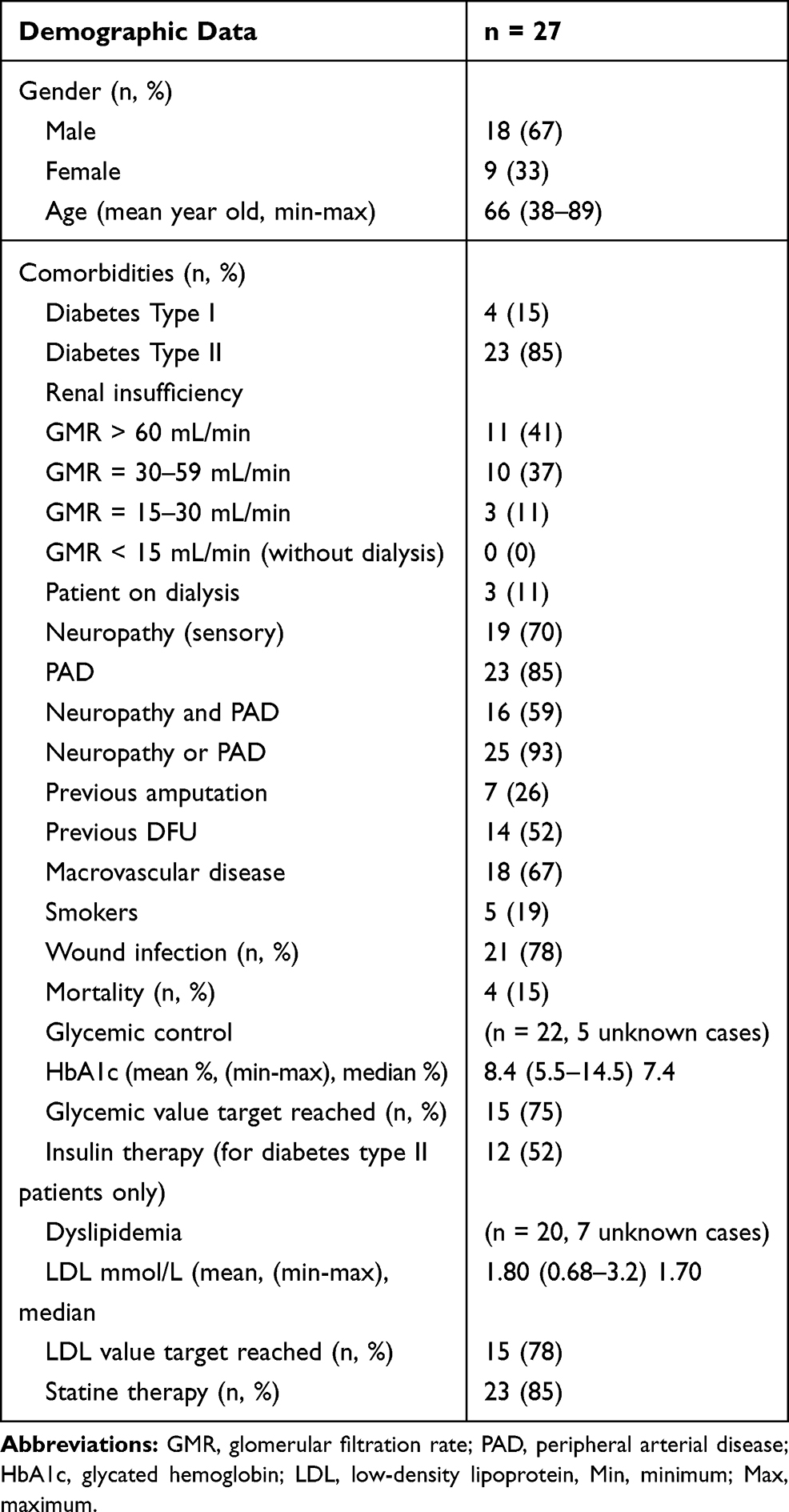 |
Table 1 Patient Characteristics Included in the Audit |
Several barriers were encountered in conducting this pilot audit which prevented a stronger methodological framework. Even though no robust conclusions could be made, we were able to establish that our sample was typical of a DFU population with neuropathy and peripheral arterial disease.12 DFU infection and past history of DFU and/or amputation were present in almost 80% of the analyzed cases. According to our preliminary results, additional efforts in our establishment appeared to be necessary in order to reach glycated hemoglobin target value (HbA1c) equal or inferior to 7% for most patients and between 7.1% and 8.5% for the 5 identified aged, frail, dependent or prone to hypoglycemia patients, and cholesterol-LDL target value inferior to 2.0 mmol/L, respectively, reached for only 75% and 78% of our sample.13,14 Standard cares were oral medication or insulin therapy for diabetes and statin administration for dyslipidemia.13,14 Pressure offloading, a key standard intervention in managing DFU, was identified in only 7 cases and unknown for the others, no matter which type offloading device was used.2–4 Moreover, coordination and provision of DFU care before and after hospitalization episodes seemed to be a major issue. Standard DFU care should at least include foot care and wound care based on multidisciplinary team approach interventions.2–4 From the 27 included cases, 5 wounds were not taken care of by a health professional before hospitalization, while it was impossible to retrieve information for 4 patients. Among the 13 patients for whom DFU management was noted, it was not multidisciplinary because only one professional (a nurse) intervened. Nevertheless, it is impossible to evaluate quality of care as in many cases wound evolution was undocumented. Lastly, only 5 patients had a multidisciplinary DFU management. It is noteworthy to mention that 4 patients died during the hospitalization episode, one death being directly related to DFU, 2 from cardiovascular diseases and one from an unrelated condition. In addition, analysis was limited pertaining to patient’s education, nutritional interventions and smoking cessation counselling, yielding no conclusions on these parameters. Moreover, as in any retrospective chart-based study, we cannot consider that the collected data corresponded to all care provided for these patients without any doubt. This is a major limitation of this type of design using secondary data. Also, there is no guarantee that all eligible cases during the pilot audit period have been identified considering initial keyword coding research process. Even if no formal research conclusions can be made, this pilot audit revealed in-practice trends coherent with what was obtained in a similar study.15 According to our pilot audit experience, evaluation of DFU clinical services and patients’ outcomes are challenging in our public health system. Improved methods and novel resources are needed to be able to obtain a clear portrait of DFU management and its outcomes.
Discussion
Many discrepancies from best practices can be identified from our observational pilot audit: nonexistent DFU team in our establishment, absent coordination of care, silo work from health professionals leading to inefficient communication between all people involved, lack of knowledge about roles and scope of practice of disciplines involved in DFU management, lack of training and the inability to prioritize concurrent needs in patients with chronic diseases, etc.3 These examples highlight the necessity to make changes for evidence-based DFU care in Quebec, especially to introduce a culture of teamwork. For example, in order to improve patient' cares, systematic use of standardized tools and resources would help enhance coordination of care and outcomes both for patients and organizations. Also, use of electronic medical records allowing more comprehensive data analysis, from diagnosis to interventions’ tracking from multiple professionals, need to be made available in clinical settings so DFU care trajectories could be better evaluated and subsequently improved. Other strategies can be implemented based on recommendations of care provided from a Canadian guidance document on optimal management of DFU care for patients in all settings.16 Best practices implementation for DFU management in team approach has already demonstrated positive DFU outcomes in Canada.7,8,17,18
Disparities in diabetes care are reported by the Canadian Institute for Health Information (CIHI). Indeed, discrepancies between recommended DFU care and care as it is delivered result in acknowledged quality gaps, unnecessary costs and negative outcomes for patients.19 In addition, CIHI has recommended providing better healthcare services and increasing preventative interventions to avoid DFU occurrence. DFU should be identified as a health system’s priority and a number of pan-Canadian, provincial and regional initiatives need to be established to improve prevention and management interventions.20 Knowing the number of Canadians living with diabetes is increasing, DFU are bound to be more prevalent in the future. Diabetes affects at least 2.7 million Canadians and up to 25% of people will develop a DFU at some point during their lifetime.21,22 In Canada, 65% of all amputations are caused by diabetes and approximately 70% of them are major amputations. Moreover, it is estimated that around 9% of these patients will not survive past amputation and around 6% to 10%, will die within 30 days post-surgery.23,24 The 5-year mortality rate is between 43% and 55% following DFU diagnosis and up to 74% after an amputation.4 Data from the province of Quebec are often absent from Canadian studies mainly because of the late and incomplete transition from manuscript charting to electronic medical records. A study about Quebec amputation rate has demonstrated that it was similar during a 9-year period with standard care.25 This same study also established that average hospitalization length of stay after amputation was 32 days, which could reach more than 35 days when concomitant peripheric arterial disease was present.25 We are concerned about these numbers considering the heavy hospitalization burden they represent for the health system, more evidently when these numbers are compared to the average of 23 hospitalization days for a stroke.26 It is estimated that by 2020 diabetes care costs will reach 16.9 billion Canadian dollars per year.27,28 At present, the average cost for a single DFU episode not requiring hospitalization is approximated at 21,371 Canadian dollars, and this amount does not include indirect health costs.29 A microeconomic study of severe DFU conducted in Quebec demonstrated that hospitalization increases costs of 70,000 Canadian dollars per hospitalization episode.28,30 Another study from Ontario demonstrated that excess costs incurred by a person with diabetes in the health system are mainly attributable to complications related to DFU, followed by nephropathy, micro- and macrovascular problems, retinopathy and metabolic complication.31 It is therefore expected that diabetes-related health expenses will keep increasing at the same rate as DFU related deaths, amputations, and other complications if nothing is done to close practice gaps in the context of a rising diabetes crisis.
Conclusion
In conclusion, we believe there is an urgent need to reassess care pathways pertaining to DFU management in Quebec’s and Canada’s health systems, as we sense the overall gravity of this diagnosis is underestimated. It has to be kept in mind that an unremarkable plantar callus or a seemingly benign nail problem can lead the way toward the development of a DFU and its potential negative outcomes. The concomitant lack of prevention, insufficient early detection and often inadequate management often lead to uncomplicated skin conditions eventually evolving into a chronic DFU. Why should we wait for unfavorable outcomes before working together in a team approach? It is time for a collective wake-up call, especially in Quebec. As already stated, tools and resources to help coordination of care and to track interventions and diagnosis urge to be implemented. These are the first steps in addressing significant care disparities with otherwise well-documented best practice guidelines. The whole community of practice on DFU management, including healthcare professionals, patients and caregivers, policymakers and administrators, should rally and take actions to address significant practice gaps.
Acknowledgments
Special thanks to Alexandre Champagne and Amélie Bellavance, doctors in family medicine, for their valuable work and collaboration for the audit. It was performed in a clinical erudition project for family physician residents and not as formal research project and for this reason, data were not published as an original research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zha M-L, Cai J-Y, Chen H-L. A bibliometric analysis of global research production pertaining to diabetic foot ulcers in the past ten years. J Foot Ankle Surg. 2019;58(2):253–259. doi:10.1053/j.jfas.2018.08.052
2. Schaper N, Van Netten J, Apelqvist J, Lipsky B, Bakker K. Foot IWGotD. Prevention and management of foot problems in diabetes: a summary guidance for daily practice 2015, based on the IWGDF guidance documents. Diabetes Res Clin Pract. 2017;124:84–92. doi:10.1016/j.diabres.2016.12.007
3. Botros M, Kuhnke J, Embil J, et al. Prevention and Management of Diabetic Foot Ulcers. Canadian Association of Wound Care (Wounds Canada):2019.
4. Van Netten J, Price PE, Lavery L, et al. Prevention of foot ulcers in the at‐risk patient with diabetes: a systematic review. Diabetes Metab Res Rev. 2016;32:84–98. doi:10.1002/dmrr.2701
5. van Acker K, Léger P, Hartemann A, Chawla A, Siddiqui MK. Burden of diabetic foot disorders, guidelines for management and disparities in implementation in Europe: a systematic literature review. Diabetes Metab Res Rev. 2014;30(8):635–645. doi:10.1002/dmrr.2523
6. Buggy A, Moore Z. The impact of the multidisciplinary team in the management of individuals with diabetic foot ulcers: a systematic review. J Wound Care. 2017;26(6):324–339. doi:10.12968/jowc.2017.26.6.324
7. Ogrin R, Houghton PE, Thompson GW. Effective management of patients with diabetes foot ulcers: outcomes of an interprofessional diabetes foot ulcer team. Int Wound J. 2015;12(4):377–386. doi:10.1111/iwj.12119
8. Blanchette V, Hains S, Cloutier L. Establishing a multidisciplinary partnership integrating podiatric care into the Quebec public health-care system to improve diabetic foot outcomes: a retrospective cohort. Foot. 2018;38:54–60.
9. Basiri R, Haverstock BD, Petrasek PF, Manji K. Reduction in diabetes-related major amputation rates after implementation of a multidisciplinary model: an evaluation in Alberta, Canada. J Am Podiatr Med Assoc. 2019. doi:10.7547/19-137
10. Leese GP, Stang D. When and how to audit a diabetic foot service. Diabetes Metab Res Rev. 2016;32:311–317. doi:10.1002/dmrr.2749
11. Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes Canada 2018 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes. 2018;42(Suppl 1):S1–S325. doi:10.1016/j.jcjd.2017.10.001
12. Monteiro‐Soares M, Boyko E, Ribeiro J, Ribeiro I, Dinis‐Ribeiro M. Predictive factors for diabetic foot ulceration: a systematic review. Diabetes Metab Res Rev. 2012;28(7):574–600. doi:10.1002/dmrr.2319
13. Institut national d’excellence en santé et services sociaux. Diabète type 2: autosurveillance glycémique chez les adultes non traités par l’insuline; 2013. Available from:https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/MaladiesChroniques/INESSS_Guide_usage_ASG.pdf.
14. Mancini GJ, Hegele RA, Leiter LA. Dyslipidémie. Can j Diabetes. 2013;1(37):S484–S491. doi:10.1016/j.jcjd.2013.07.015
15. Claveau C. Évaluation des retombées cliniques et économiques du suivi des pratiques exemplaires pour l’ulcère du pied diabétique: Une étude descriptive. Master thesis. Université de Sherbrooke. 2018.
16. Health Quality Ontario. Quality standards for diabetic doot ulcer: care for patients in all settings; 2016. Available from:http://www.hqontario.ca/portals/0/documents/evidence/quality-standards/foot-ulcers-clinical-guide-1611-en.pdf.
17. Roth-Albin I, Mai SHC, Ahmed Z, et al. Outcomes following advanced wound care for diabetic foot ulcers: a Canadian study. Can J Diabetes. 2017;41(1):26–32. doi:10.1016/j.jcjd.2016.06.007
18. Prentice D, Ritchie, L, Crandall J, et al. Implementation of a diabetic foot management best practice guideline (BPG) in hemodialysis units. CANNT J/J ACITN. 2009;16(4):20
19. Institut Canadien d’information sur la santé. Lacunes et disparités en matière de soins aux personnes diabétiques au Canada; 2009. 24. Available from:https://secure.cihi.ca/free_products/Diabetes_care_gaps_disparities_aib_f.pdf.
20. Institut canadien d’information sur la santé. Les plaies difficiles au Canada. ICIS2013.
21. Gouvernement du Canada. Le diabète au Canada: Perspectives de santé publique sur les faits et les chiffres; 2011.
22. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. J Am Med Assoc. 2005;293(2):217–228. doi:10.1001/jama.293.2.217
23. Kayssi A, de Mestral C, Forbes TL, Roche-Nagle G. A Canadian population-based description of the indications for lower-extremity amputations and outcomes. Can J Surg. 2016;59(2):99. doi:10.1503/cjs.013115
24. Imam B, Miller WC, Finlayson HC, Eng JJ, Jarus T. Incidence of lower limb amputation in Canada. Can J Public Health. 2017;108(4):374–380. doi:10.17269/CJPH.108.6093
25. Dawes D, Iqbal S, Steinmetz OK, Mayo N. The evolution of amputation in the province of Quebec. Can J Diabetes. 2010;34(1):58–66. doi:10.1016/S1499-2671(10)41011-4
26. Mayo NE, Nadeau L, Daskalopoulou SS, Côté R. The evolution of stroke in Quebec: a 15-year perspective. Neurology. 2007;68(14):1122–1127. doi:10.1212/01.wnl.0000258664.12423.4c
27. Rosella L, Lebenbaum M, Fitzpatrick T, et al. Impact of diabetes on healthcare costs in a population‐based cohort: a cost analysis. Diabetic Med. 2016;33(3):395–403. doi:10.1111/dme.12858
28. Pelletier C, Dai S, Roberts K, Bienek A. Report summary Diabetes in Canada: facts and figures from a public health perspective. Chronic Dis Inj Can. 2012;33(1).
29. Hopkins RB, Burke N, Harlock J, Jegathisawaran J, Goeree R. Economic burden of illness associated with diabetic foot ulcers in Canada. BMC Health Serv Res. 2015;15(1):13. doi:10.1186/s12913-015-0687-5
30. Bissonnette V Évaluation des coûts et éléments d’efficacité du traitement d’un ulcère du pied diabétique. Université de Sherbrooke. 2011.
31. Goeree R, Lim ME, Hopkins R, et al. Prevalence, total and excess costs of diabetes and related complications in Ontario, Canada. Can J Diabetes. 2009;33(1):35–45. doi:10.1016/S1499-2671(09)31007-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.