Back to Journals » Journal of Asthma and Allergy » Volume 16
Multidisciplinary Discussion for Fibrotic Hypersensitivity Pneumonitis with a Positive Antigen Avoidance
Authors Okuda R ![]() , Takemura T, Misumi T, Hagiwara E, Ogura T
, Takemura T, Misumi T, Hagiwara E, Ogura T
Received 3 March 2023
Accepted for publication 29 April 2023
Published 4 May 2023 Volume 2023:16 Pages 473—479
DOI https://doi.org/10.2147/JAA.S409042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Ryo Okuda,1 Tamiko Takemura,2 Toshihiro Misumi,3 Eri Hagiwara,1 Takashi Ogura1
1Department of Respiratory Medicine, Kanagawa Cardiovascular and Respiratory Center, Yokohama, Japan; 2Department of Pathology, Kanagawa Cardiovascular and Respiratory Center, Yokohama, Japan; 3Department of Data Science, National Cancer Center Hospital East, Chiba, Japan
Correspondence: Ryo Okuda, Department of Respiratory Medicine, Kanagawa Cardiovascular and Respiratory Center, 6-16-1 Tomioka-higashi, Kanazawa-ku, Yokohama, Japan, Tel +81-45-701-9581, Email [email protected]
Background: In the two fibrotic hypersensitivity pneumonitis (fHP) diagnostic guidelines, the multidisciplinary discussion (MDD) is required to be performed in diagnosis of fHP, as in idiopathic pulmonary fibrosis (IPF) diagnostic guideline. Although some patients with fHP can improve disease condition during antigen avoidance, which can facilitate the diagnosis of fHP, it is unclear if MDD is necessary in all patients with suspected fHP who improved an antigen avoidance.
Objective: To investigate the diagnosis of fHP via MDD with positive antigen avoidance tests (AATs) and the clinical diagnosis with positive AATs.
Methods: A single-center, retrospective study was conducted. Between 2012 and 2019, patients with fHP were enrolled in the study. Patients in the MDD diagnostic group consisted of patients diagnosed with MDD, including histopathology findings and positive ATTs, and patients in the clinical diagnostic group were diagnosed by two respiratory physicians and had positive ATTs.
Results: AAT was performed on 72 of 219 patients, and 58 had positive AATs. The study included 37 patients in the MDD diagnosis group and 21 patients in the clinical diagnosis group. No significant differences in overall survival (OS) were detected between the two groups (HR: 1.99 [95% CI: 0.82‒4.83], p = 0.127). The conducting MDD was not a risk factor for OS; only < 79% forced vital capacity was a risk factor in the multivariate Cox hazard regression analysis. No significant difference in annual changes of forced vital capacity, diffusion of the lung for carbon monoxide and Krebs von den Lungen-6 between the MDD diagnostic and the clinical diagnostic groups were observed (p = 0.41, 0.79, and 0.81, respectively).
Conclusion: In patients with positive AATs, the disease progression of the MDD diagnostic and the clinical diagnostic groups were similar. Therefore, MDD could not be necessary in all patients with suspected fHP who had positive AATs.
Keywords: chronic hypersensitivity pneumonitis, diagnostic method, hypersensitivity pneumonitis, multidisciplinary team, subacute hypersensitivity pneumonitis
Introduction
No diagnostic guidelines for fibrotic hypersensitivity pneumonitis (fHP) have been available until recently. The American Thoracic Society/Japanese Respiratory Society/Asociación Latinoamericana de Tórax (ATS/JRS/ALAT) Clinical Practice Guideline and the CHEST guidelines were published in 2020 and 2021.1,2 Both guidelines recommend multidisciplinary discussion (MDD) for the diagnosis of fHP based on exposure history, chest high-resolution computed tomography (HRCT), bronchoalveolar lavage fluid, and pathological findings. The procedures for diagnosing fHP are similar to the procedures for diagnosing idiopathic pulmonary fibrosis (IPF), including HRCT pattern, pathological pattern, and an MDD.3,4 However, many institutions face difficulty in conducting high-quality MDDs due to the absence of specialists who can treat interstitial lung disease (ILD). Clinical improvement with antigen avoidance was selected as one of the important diagnostic methods for an international modified Delphi survey,5 and antigen avoidance has long been methods used to diagnose fHP and estimate the inciting antigens.6,7 However, antigen avoidance test (AAT) was not given much weight in diagnostic HP guidelines. If MDD no longer had to be conducted in every patient of suspected fHP, more facilities would be able to diagnose fHP more easily. Therefore, we investigated whether MDD has additional prognostic power in patients with positive ATTs.
Methods
Study Design and Population
This was a single-center, retrospective study. Consecutive patients with fHP were enrolled in the study between January 2012 and August 2019. The MDD diagnostic group consisted of patients who underwent surgical lung biopsy or transbronchial lung cryobiopsy, had a diagnostic confidence level of fHP or probable fHP according to the ATS/JRS/ALAT guideline, and were diagnosed with HP by an MDD team. This MDD team consisted of 6 members: 2 respiratory physicians specializing in ILD, 2 thoracic radiologists specializing in ILD, 1 pathologist specializing in ILD, and 1 thoracic pathologist. Three of the six members are central MDD members in the JIPS Registry, which is an observational study of idiopathic interstitial pneumonia conducted in Japan.8 The clinical diagnostic group consisted of patients with positive AATs who did not undergo histopathological examinations and were diagnosed with fHP by the attending physician and one other respiratory physician based on medical records, chest HRCT, respiratory function tests, and blood data including specific serum IgG testing and interstitial pneumonia makers. HRCT pattern was based on the fHP pattern in the ATS/JRS/ALAT guideline. Ethical approval was obtained from the institutional review board of Kanagawa Cardiovascular and Respiratory Center (KCRC-22-0021). Because of using an opt-out consent approach and retrospective observation study, the need for patient consent was waived according to the ethical guideline of our hospital. Research participants were informed about the study details on website of our facility and their rights to withdraw from the research. All personal data were protected and de-identified. Confidentiality and compliance with the Declaration of Helsinki was maintained.
Antigen Avoidance Test
Patients were isolated from their home and work environments by hospitalization for 14 days.7 The attending physician decided to conduct the AAT in clinical practice. Patients were examined before and after antigen avoidance to determine changes during AAT. Positive criteria for the AAT were based on previous reports and included improvements in respiratory symptoms, ≥2.5% decline in white blood cell (WBC) counts, ≥0.05-mg/dL decline in C-reactive protein (CRP), ≥12% decline in Krebs von den Lungen-6 (KL-6), ≥2.5% improvement in forced vital capacity (FVC), ≥5% improvement in diffusion capacity of the lung for carbon monoxide (DLco), ≥5-mmHg improvement in alveolar–arterial oxygen difference, and improved HRCT findings for fHP, such as ground-glass opacities and reticular shadows. A patient was considered positive if at least two of the eight criteria were met.6,7
Evaluation Methods
Determining the superiority of a diagnostic method for fHP was difficult because a gold standard for the diagnosis of fHP other than MDD does not exist in current fHP guidelines. Thus, we compared disease progression between the MDD diagnosis group and clinical diagnosis group. To evaluate disease progression, we compared changes in the respiratory function test, interstitial pneumonia maker, and overall survival (OS).
Statistical Analysis
Unpaired t-tests were used to compare continuous variables. Contingency tables were used with Fisher’s exact tests and Pearson’s chi-square tests, based on the number of columns and rows. Kaplan–Meier curves were applied to analyze survival. When OS was analyzed between the MDD and clinical diagnostic groups, factors with a p value of <0.1 in baseline characteristics were adjusted using Cox hazard regression analysis. During the analysis of OS in all patients, conducting MDD and parameters with a p value of <0.1 in the univariate Cox hazard regression analysis were included in the multivariate Cox hazard regression analysis. The medians of the two groups were selected as the thresholds for continuous variables. BellCurve for Excel was used for all statistical analyses (Social Survey Research Information Co., Ltd.). All statistical methods were consulted with the co-author statistician.
Results
Figure 1 shows the enrollment of patients with fibrotic HP from January 2012 to August 2019 in the MDD and clinical diagnostic groups. A total of 219 patients with fHP were included. Of the 140 patients diagnosed with MDD, AAT was performed in 48 patients (34%), and of the 79 patients diagnosed clinically, 24 received AAT (30%). The positivity rates for AAT in the MDD and clinical diagnostic groups were 77% and 88%, respectively.
 |
Figure 1 Flowchart showing patient inclusion criteria. Abbreviations: fHP, fibrotic hypersensitivity pneumonitis; MDD, multidisciplinary discussion; AAT, antigen avoidance test. |
MDD Diagnostic and Clinical Diagnostic Groups with Positive AATs
The median baseline WBC and CRP in the clinical diagnostic group with positive AAT were significantly higher than the WBC counts and CRP in the MDD diagnostic group with positive AAT (WBC: 7730/µL vs 6200/µL, p = 0.03; CRP: 0.53 mg/dL vs 0.14 mg/dL, p = 0.047). The frequency of patients with worsening symptoms or HRCT findings during the 3 months before the AAT was significantly higher in the clinical diagnostic group compared with the frequency in the MDD diagnostic group (86% vs 46%, p = 0.005). The most frequent fHP pattern, based on the ATS/JRS/ALAT guidelines, was “compatible with fHP” in both groups, with no significant difference (Table 1).
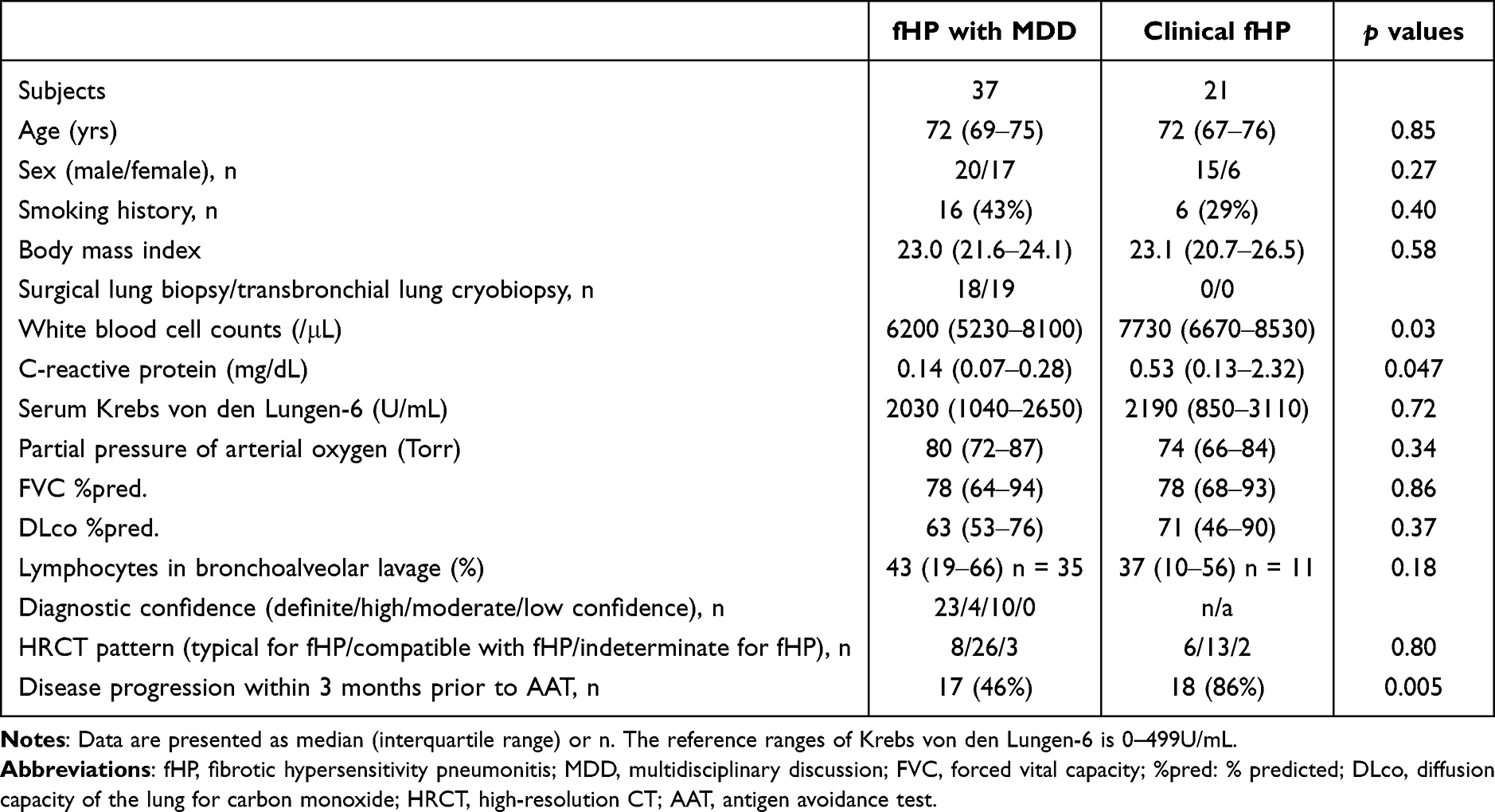 |
Table 1 Baseline Characteristics |
One year after the AAT, no significant differences in FVC, DLco, KL-6, or CRP changes were detected between the MDD and clinical diagnostic groups (Table 2). Antifibrotic agents were initiated during one year after diagnosis in 11 patients with MDD diagnoses and in 4 patients with clinical diagnoses (30% vs 19%, p = 0.54). Steroid therapy was also initiated in 49% and 24% of the MDD and clinical diagnostic groups, respectively (p = 0.09). OS from the date of AAT initiation was not significantly different between the two groups (HR: 1.99 [95% CI: 0.82‒4.83], p = 0.127) (Figure 2). Multivariate analysis showed that only FVC was a risk factor for OS. The incidence of events was higher when the FVC was <79% (HR: 2.55 [95% CI: 1.08‒5.99], p = 0.032). Difference in diagnostic methods between MDD and clinical diagnoses was not a risk factor for OS in the univariate and multivariate analyses (Table 3).
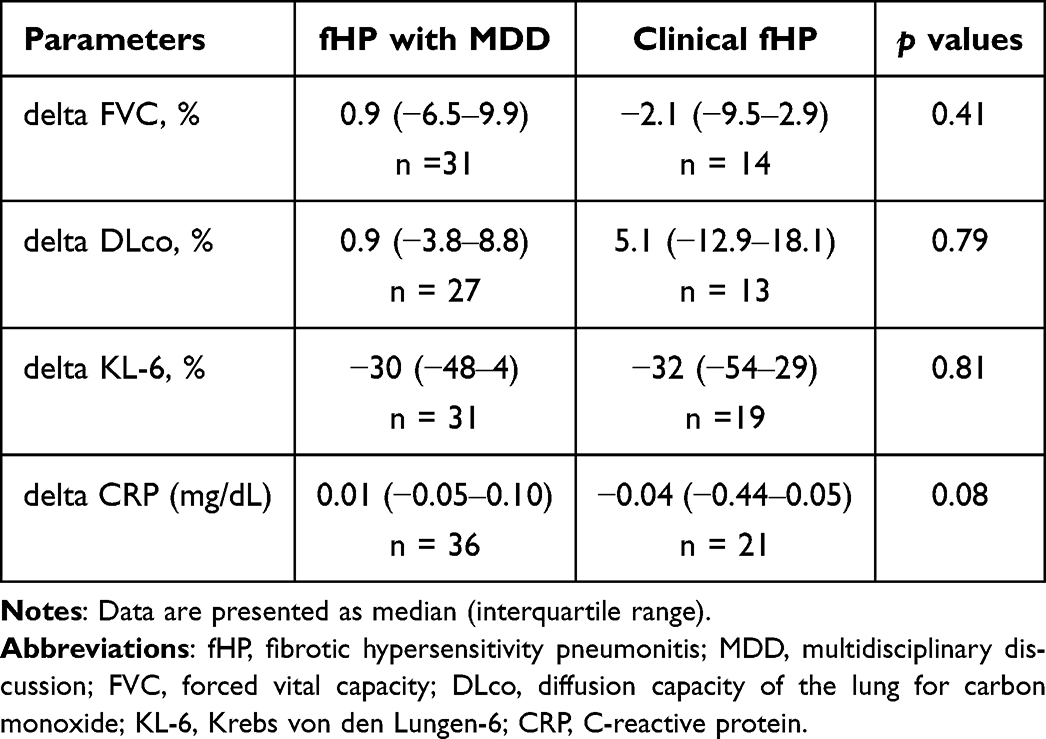 |
Table 2 Annual Changes |
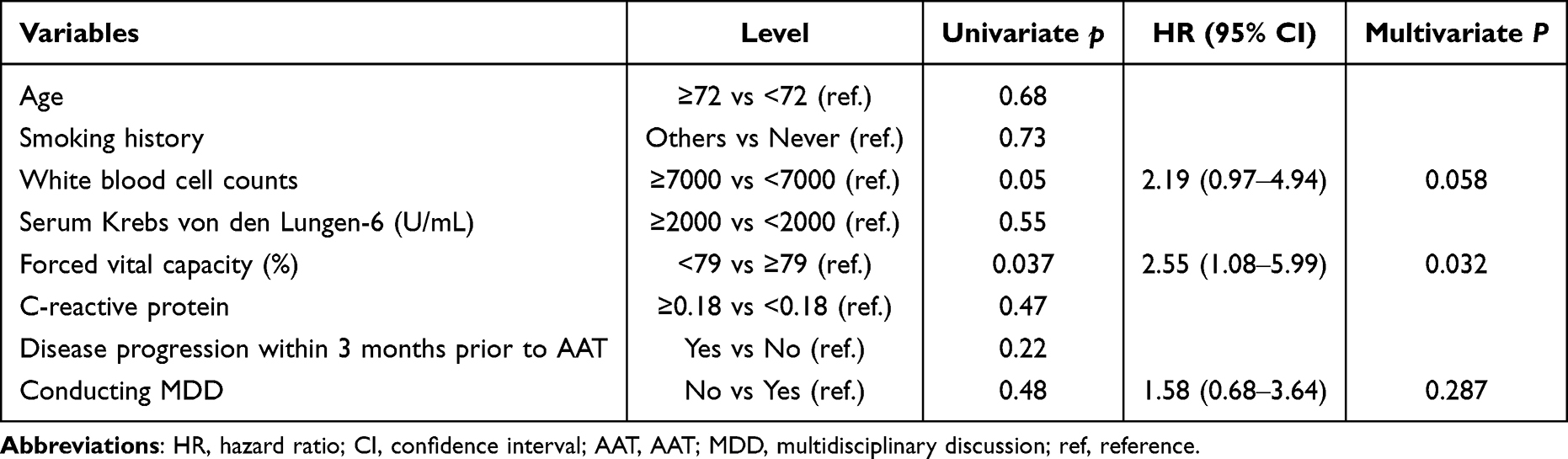 |
Table 3 Cox Hazard Regression Analysis for Overall Survival |
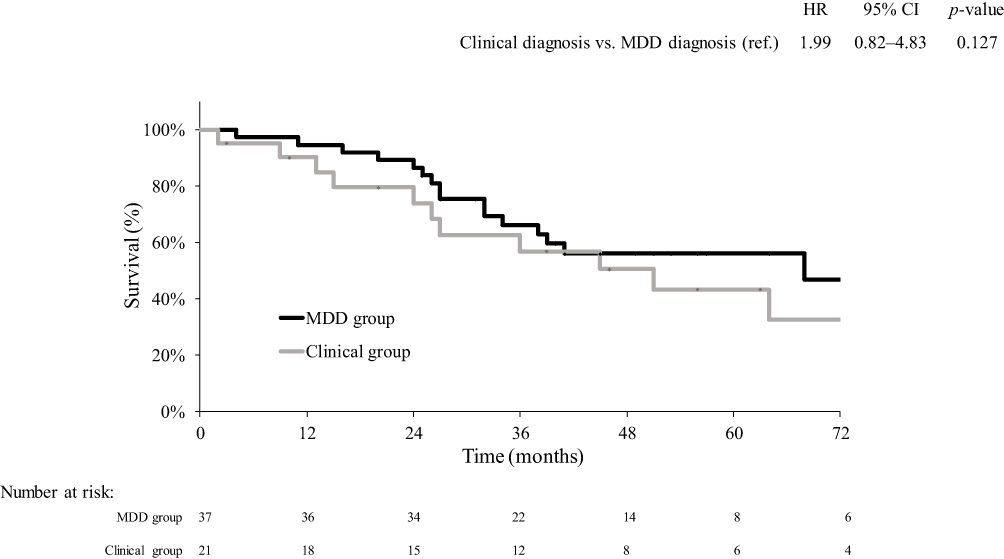 |
Figure 2 Overall survival in MDD diagnosis and clinical diagnosis groups. Abbreviations: MDD, multidisciplinary discussion; HR, hazard ratio; CI, confidence interval. |
MDD Diagnostic Group with Positive and Negative AATs
When the AAT-positive and AAT-negative groups were compared in patients diagnosed by MDD team, no single antigen was identifitied in any patients among both groups from the clinical history taking and specific serum immunoglobulin (Ig) G testing. In the MDD diagnostic group, 26 of 48 patients with the AAT-positive and 7 of 11 patients with the AAT-negative had (typical) fHP patterns in the histopathological criteria in the ATS/JRS/ALAT guideline, and no association was found between AAT results and pathological patterns (p = 0.72). In the AAT-positive MDD group, 26 of 37 patients had compatible HRCT patterns; in the AAT-negative, 6 of 11 patients had a compatible HRCT pattern, with no significant difference (p = 0.24).
Discussion
No significant differences were detected in annual changes, OS, or treatment between AAT-positive patients diagnosed by an MDD team and those clinically diagnosed by the attending physician.
In total, AAT was performed in only 33% of the patients with fHP, and 66% of patients with conducting AAT experienced disease progression in the 3 months before the AATs. The ATS/JRS/ALAT and CHEST guidelines divided HP into nonfibrotic and fibrotic HPs; however, HP is also conventionally classified based on the clinical course into acute, subacute, and chronic disease.9,10 Many of the patients had so-called subacute disease condition with fibrotic changes and obvious disease progression over a 3-month period. The AATs shows fewer changes than the inhalation challenge test because the AATs only involves 14 days of isolation from the living environment.7 It is often experienced that antigen avoidance in stable patients with fHP does not change in any parameters. Patients with rapid disease progression in the last month, such as acute exacerbation of IPF, could be better treated with medications such as intravenous methyl prednisolone pulse therapy than with antigen avoidance. Patients with mild exacerbations over several months could be good candidates for AATs.
From pathological diagnosis, MDD diagnosis is becoming the gold standard for ILD diagnosis. With the exception of a few facilities, high-quality MDD diagnosis is more difficult to conduct than pathological diagnosis due to lack of ILD specialists. Meanwhile, the concept of progressive fibrosing interstitial lung disease (PF-ILD) and progressive pulmonary fibrosis (PPF) consider patients with progressive disease as having the similar or same disease.11,12 Therefore, we investigated the validity of the MDD diagnosis by using disease progression, such as FVC changes and OS. In AAT-positive patients with fHP, no significant differences in OS and annual changes in FVC and KL-6 were detected between the MDD diagnostic and clinical diagnostic groups in the current study. Among the AAT-positive patients in both groups, a lower FVC at the time of AAT was more predictive of OS than performing MDD. Based on the results of the current study, additional MDD did not improve prognostic discrimination in fHP patients with positive AATs. Thus, a diagnosis based on the AAT is worth considering, especially when the disease condition is subacute or in situations where ILD specialists cannot available.
In the current study, no difference in the frequency of pathological and radiological patterns defined by the ATS/JRS/ALAT guideline between patients diagnosed with MDD that had positive and negative AATs was observed. Therefore, the results of AATs could not be predicted from pathological and HRCT patterns. Different results might be obtained if pathological and radiological findings were examined instead of pattern classification.
In all patients by MDD diagnostic group, no single inciting antigen could be identified by clinical history taking and specific serum IgG testing in the current study. ATS/JRS/ALAT HP Clinical Practice Guideline suggested emphasized the importance of clinical history taking and specific serum IgG testing in identifying the inciting antigen. With the exception of humidifier lung and acute HP, identifying a single inciting antigen from a clinical history taking and specific IgG testing can occasionally lack objectivity. A history of bird keeping and positive bird IgG antibodies can lead to a diagnosis of bird-related fHP.13 However, regardless of the fHP onset, anti-bird antibodies will rise if birds are kept. Identification of the inciting antigen by clinical history taking and IgG antibody is highly dependent on the discretion and conscience of the attending physicians or researchers. AAT cannot identify a single inciting antigen; however, it can estimate inciting antigens in the area around the patient’s home or workplace with a little objectivity.
Our study had several limitations. First, this was a single-center retrospective study, and all patients underwent AAT. Thus, patient selection for the study was biased. Second, 46% of the patients diagnosed with MDD and positive AAT experienced disease progression 3 months before the AAT, suggesting that a relatively large number of patients with acute on fHP or subacute fHP were included in the current study. The inclusion of only fHP patients in the stable phase could have different results. Third, although no differences in annual FVC changes or OS were detected between the MDD and clinical diagnostic groups, the small number of patients can have resulted in insufficient statistical power. However, FVC was a risk factor for OS in patients with fHP as in a previous article,14 and there were a number of patients with fHP in which FVC was a detectable risk factor for OS in the current study. Fourth, the MDD diagnostic group had a pathological examination, while the clinical diagnostic group had no pathological examination, which was a significant bias. Because previous reports on the usefulness of MDD have been conducted in patients with pathological examination, the MDD diagnostic group in the current study included only patients with pathological investigations.15–17 Under clinical practice, it is ethically impossible to make a diagnosis of fHP solely by an attending physician without performing an MDD diagnosis in the patients for whom the pathological examinations were performed. In addition, even if an attending physician diagnosis is made after a pathological examination for research, the subsequent treatment is affected by the results of the MDD diagnosis in real-world research; therefore, it is not possible to genuinely compare the disease progression of the two groups, the attending physician diagnosis and the MDD diagnosis. Finally, the validity of the MDD in current study needs to be discussed. The diagnosis of fHP only by the attending physicians was not considered to guarantee high accuracy; therefore, the patients were judged to have fHP based on the attending physician’s diagnosis and a positive AAT in current study. Since MDD is the gold standard for fHP diagnosis in current guidelines, the diagnostic accuracy of MDD cannot be verified. Therefore, the diagnostic accuracy of the diagnosis was examined in the disease progression.
In conclusions, no significant differences were detected in disease progression between patients with positive AATs diagnosed with fHP via MDD and patients with positive AATs diagnosed by an attending physician. MDD could not be necessary in all patients of suspected fHP.
Date Sharing Statement
The datasets analyzed during the study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Nao Onishi, Keiko Teramura and Yukiko Ogasawara, who work at our hospital for the assistance in data accumulation and Enago (www.enago.jp) for the professional English language review.
Funding
There is no funding to report.
Disclosure
Dr Takashi Ogura reports grants, personal fees from Nippon Boehringer Ingelheim Gmb, personal fees from Taiho Pharmaceutical Co, personal fees from Shionogi & Co. LTD, personal fees from Bristol Myers Squibb Co, personal fees from Astellas Co, personal fees from AstraZaneca KK, personal fees from Eizai Inc, outside the submitted work. The authors declare no other competing interests.
References
1. Raghu G, Remy-Jardin M, Ryerson CJ, et al. Diagnosis of hypersensitivity pneumonitis in adults. An official ATS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2020;202:e36–e69. doi:10.1164/rccm.202005-2032ST
2. Fernandez Perez ER, Travis WD, Lynch DA, et al. Diagnosis and evaluation of hypersensitivity pneumonitis: CHEST Guideline and expert panel report. Chest. 2021;160:e97–e156. doi:10.1016/j.chest.2021.03.066
3. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183:788–824. doi:10.1164/rccm.2009-040GL
4. Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An Official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198:e44–e68. doi:10.1164/rccm.201807-1255ST
5. Morisset J, Johannson KA, Jones KD, et al. Identification of diagnostic criteria for chronic hypersensitivity pneumonitis: an international modified delphi survey. Am J Respir Crit Care Med. 2018;197:1036–1044. doi:10.1164/rccm.201710-1986OC
6. Tsutsui T, Miyazaki Y, Okamoto T, et al. Antigen avoidance tests for diagnosis of chronic hypersensitivity pneumonitis. Respir Investig. 2015;53:217–224. doi:10.1016/j.resinv.2015.04.003
7. Okuda R, Takemura T, Iwasawa T, et al. Impact of antigen avoidance test for fibrotic hypersensitivity pneumonitis in stable phase. Allergy Asthma Clin Immunol. 2022;18:104. doi:10.1186/s13223-022-00748-1
8. Okuda R, Ogura T, Hisata S, et al. Design and rationale of the Japanese Idiopathic Interstitial Pneumonias (JIPS) Registry. Respir Investig. 2023;61:95–102. doi:10.1016/j.resinv.2022.08.009
9. Bank L, Benatar SR. Subacute cor pulmonale in hypersensitivity pneumonitis. A case report. S Afr Med J. 1982;62:768–769.
10. Remy-Jardin M, Remy J, Wallaert B, Muller NL. Subacute and chronic bird breeder hypersensitivity pneumonitis: sequential evaluation with CT and correlation with lung function tests and bronchoalveolar lavage. Radiology. 1993;189:111–118. doi:10.1148/radiology.189.1.8372179
11. Raghu G, Remy-Jardin M, Richeldi L, et al. Idiopathic pulmonary fibrosis (an Update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2022;205:e18–e47. doi:10.1164/rccm.202202-0399ST
12. Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in progressive fibrosing interstitial lung diseases. N Engl J Med. 2019;381:1718–1727. doi:10.1056/NEJMoa1908681
13. Morell F, Roger A, Reyes L, Cruz MJ, Murio C, Munoz X. Bird fancier’s lung: a series of 86 patients. Medicine. 2008;87:110–130. doi:10.1097/MD.0b013e31816d1dda
14. Gimenez A, Storrer K, Kuranishi L, Soares MR, Ferreira RG, Pereira CAC. Change in FVC and survival in chronic fibrotic hypersensitivity pneumonitis. Thorax. 2018;73:391–392. doi:10.1136/thoraxjnl-2017-210035
15. Walsh SLF, Wells AU, Desai SR, et al. Multicentre evaluation of multidisciplinary team meeting agreement on diagnosis in diffuse parenchymal lung disease: a case-cohort study. Lancet Respir Med. 2016;4:557–565.
16. De Sadeleer LJ, Meert C, Yserbyt J, et al. Diagnostic ability of a dynamic multidisciplinary discussion in interstitial lung diseases: a retrospective observational study of 938 cases. Chest. 2018;153:1416–1423. doi:10.1016/j.chest.2018.03.026
17. Fujisawa T, Mori K, Mikamo M, et al. Nationwide cloud-based integrated database of idiopathic interstitial pneumonias for multidisciplinary discussion. Eur Respir J. 2019;53:1802243. doi:10.1183/13993003.02243-2018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.