Back to Journals » Clinical Ophthalmology » Volume 19
Multicenter Retrospective Analysis of Intraoperative Aberrometer Measurements and Associated Visual Outcomes with a Monofocal Aspheric Intraocular Lens
Received 9 July 2025
Accepted for publication 1 December 2025
Published 13 December 2025 Volume 2025:19 Pages 4623—4633
DOI https://doi.org/10.2147/OPTH.S542118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
William F Wiley,1 Alexis Rendon2
1Cleveland Eye Clinic, Elyria, OH, USA; 2Alcon Laboratories, Inc., Fort Worth, TX, USA
Correspondence: William F Wiley, Cleveland Eye Clinic, Brecksville, OH, USA, Email [email protected]
Purpose: To assess the real-world performance of Clareon® monofocal non-Toric and Toric intraocular lenses (IOLs) using intraoperative aberrometry (IA).
Patients and Methods: This retrospective, postmarket analysis included anonymized data from a multicenter study conducted in the US. Data were collected from patients implanted with Clareon ultraviolet-absorbing (UVA) monofocal or monofocal Toric IOL(s), utilizing the WaveTec ORA System and had available corrected distance visual acuity (CDVA) data at 28 days to 3 years postoperative. The primary endpoint was the percentage of eyes achieving monocular CDVA of 20/40 at ≥ 1 month postoperative. Secondary and exploratory endpoints included monocular uncorrected distance visual acuity (UDVA), residual refractive cylinder, stratified visual acuity (VA) thresholds, manifest refraction spherical equivalent (MRSE), and prediction error comparisons between ORA and preoperative biometry.
Results: Based on 1404 eyes, 98.4% achieved CDVA of 20/40 or better (mean logMAR 0.04 non-Toric, 0.03 Toric). Among emmetropia targeted eyes, 93.9% achieved UDVA of 20/40 or better. The mean residual refractive cylinder for Toric models was 0.40 diopters (D). The mean (standard deviation) MRSE was − 0.15 (0.45) D. The mean prediction error for emmetropia targeted eyes was − 0.10 (0.49) D. Additionally, 78.7% had prediction error differences within ± 0.25 D between ORA and preoperative biometry. In 40.8% of cases, the implanted IOLs match the preoperative selection with no clinically significant VA differences between match and unmatch eyes.
Conclusion: Most patients implanted with the Clareon UVA IOLs, using WaveTec ORA IA achieved CDVA of 20/40 or better at ≥ 1 month postoperatively, with minimal residual refractive error and enhanced target accuracy, indicating ORA may support optimize IOL power calculation and axis positioning to improve refractive outcomes.
Plain Language Summary: Clareon intraocular lenses (IOLs) are used during cataract surgery to restore clear vision and are designed to reduce visual disturbances like glare, halos, and lens-related complications such as clouding behind the lens (posterior capsule opacification). Intraoperative aberrometry (IA) is a technology that helps surgeons fine-tune lens selection during surgery, but previous studies have shown mixed results about its real-world value. This study was done to evaluate whether IA improves lens power accuracy and visual outcomes when using Clareon IOLs. We analyzed data from 1,404 eyes treated with Clareon IOLs across 87 US sites using the WaveTec AnalyzORTM system, which collects information from surgeries using IA. The study results showed that nearly 98.4% of patients achieved good distance vision (20/40 or better) one month or more after surgery. The accuracy of IA in selecting the correct lens power was found to be comparable to traditional pre-surgery measurements, suggesting that IA can be a useful tool to support clinical decision-making in everyday cataract surgery.
Keywords: Clareon IOLs, intraoperative aberrometry, prediction error, refractive outcomes, WaveTec ORA system visual outcomes
Introduction
Monofocal intraocular lenses (IOLs) are commonly implanted due to their optimal distance visual acuity (VA) outcomes, minimal photic phenomena,1 and relatively low cost. Introduced in 2018, the Clareon IOL (Alcon Vision LLC, Fort Worth, TX, USA) is a 1-piece foldable, aspheric, hydrophobic lens based on the AcrySof® IOL platform. It features a novel hydroxyethyl-methacrylate material, enhanced edge design for improved optical clarity, rotational stability, and ultraviolet (UV) absorption.2
Clareon IOLs, used in over 70 countries, have undergone extensive clinical evaluation. Research shows they reduce posterior capsule opacification (PCO), minimal axial displacement, and offer good visual outcomes with improved lens clarity, low surface haze, and glistening.3–6 While most existing data focus on blue-light filtering (BLF) models such as CNA0T03,7–9 and SY60WF10 (referred to as “natural format” lenses), data on the Clareon UVA IOLs are limited despite their widespread use in the US.
Previous studies have reported favorable visual outcomes with Clareon IOLs. For instance, Bouvarel et al observed a mean CDVA of 0.003 logMAR and UDVA of 0.075 logMAR at 3 years, with approximately 50% of eyes achieving 20/20 vision and low incidence of posterior capsular opacification.11 Similarly, Tran et al documented stable refractive outcomes and absence of glistenings up to 12 months postoperatively.12 In a multicenter trial, Lehmann et al found that 99.7% of eyes achieved CDVA of 20/40 or better and 86.8% achieved 20/20 or better at 12 months.6 While these findings indicate consistent performance of Clareon IOLs in routine cataract surgery, evidence on outcomes when implantation is guided by intraoperative aberrometry remains limited, which is important because accurate IOL power selection is critical for achieving optimal visual outcomes and patient satisfaction. This study aims to address that gap.
Achieving the predicted postoperative spherical equivalent (SE) remains challenging due to residual corneal astigmatism and biometry prediction errors.13 Besides surgeon skill, lens constant and IOL power formula selection are crucial for refractive and visual outcomes.14–16 Preoperative IOL calculations can be compromised by challenges in precisely measuring the true total corneal power, which includes both anterior and posterior corneal refractive surfaces, surgically induced astigmatism, and cataract-induced opacification, all contributing to variability in postoperative refractive outcomes. To address these challenges, intraoperative aberrometry (IA) offers real-time refractive data in both aphakic and pseudophakic states, potentially improving IOL selection and placement precision.17–19 Studies indicate that IA can result in 8%17 to 45%20 more eyes achieving ≤ 0.5 D residual refractive astigmatism compared to preoperative biometry. In one prospective study, 89.2% of eyes had ≤ 0.5 D of astigmatism 1 month post-surgery with IA, versus 76.6% (p=0.006) with preoperative methods.21 However, IA’s accuracy can be influenced by factors such as the speculum, achieving physiologic intraocular pressure (IOP), corneal surface hydration, and ophthalmic viscosurgical devices.22,23
The WaveTec OptiwaveTM Refractive Analysis (ORA) SystemTM (Alcon Vision LLC, Fort Worth, TX), introduced in 2013, is an intraoperative measurement system providing real-time data to aid precise IOL model and power selection.15,24,25 Intraoperative measurements enable surgeons to refine IOL sphere power, cylinder power, and or astigmatism axis for Toric lens placement. Furthermore, postoperative data entered the WaveTec AnalyzOR database continuously refines the ORA System’s IOL power formula, allowing individualized IOL constants and enabling surgeons to track and improve refractive outcomes.17
This multicenter, observational study explored the role of the WaveTec ORA System in evaluating the Clareon IOLs performance. Using the WaveTec AnalyzOR database data, the investigation aimed to provide real-world evidence (RWE) on the association between intraoperative measurement and postoperative visual outcomes in patients with Clareon UVA IOLs.
Materials and Methods
Study Design and Setting
This retrospective, noninterventional, nonrandomized, multicenter, unmasked, single cohort, postmarket study analyzed data from cataract patients who underwent phacoemulsification and received either the Clareon UVA monofocal IOL (models CC60WF, CCA0T0) or the Clareon UVA monofocal Toric IOL (models CCW0T3, CCW0T4, CCW0T5, CCW0T6) implanted using the WaveTec ORA System. Clareon T2 models are not available in the USA and were therefore not included in the dataset. All procedures were conducted in accordance with standard of care (SOC) clinical practices at each site, reflecting real-word variability. Pre- and postoperative data were anonymized and entered into the WaveTec AnalyzOR database. The term “model” refers to specific variants of the Clareon platform that differ in design (Toric vs non-Toric) or cylindrical power. IA could influence mode selection by identifying patients for astigmatism correction or guiding the choice among available Toric powers.
Cases were identified as consecutive entries in the AnalyzOR database from participating surgeons. Eyes were included only if IA measurements were performed intraoperatively and postoperative CDVA data were available at ≥30 days.
Inclusion criteria required eyes implanted with Clareon IOLs and with corrected distance visual acuity (CDVA) data available at 28 days to 3 years postoperative. To ensure data quality and internal consistency, eyes were included only if CDVA was not worse than the corresponding uncorrected distance visual acuity (UDVA) at the same time points. Moreover, this time range was selected to reflect typical variability in follow-up intervals observed in real-world clinical settings. While this approach enabled broad inclusion across practices, it may limit the ability to assess long-term visual or refractive stability. A minimum sample size of 300 eyes was deemed sufficient for precise CDVA estimation.
Although no formal exclusion criteria were applied for comorbidities or intraoperative complications due to the retrospective nature of the anonymized dataset, data capture predominantly reflects routine, uncomplicated cases typically entered by surgeons for outcome tracking. Eyes with prior refractive surgery (eg, LASIK, PRK, RK, ALK) were included as recorded in the AnalyzOR database. The study did not require a specific IOL power calculation formula; however, the formulas used were recorded, with Barrett, Barrett Universal II, and Holladay 2 being the most applied. IOL power selection relied on intraoperative aberrometry and surgeon judgment, consistent with standard clinical practice. Eyes with irregular or decentered ablations were not systematically flagged or excluded.
IA Procedure
IA was performed intraoperatively on aphakic eyes, following cataract removal and prior to IOL implantation, in accordance with manufacturer guidelines for achieving physiologic IOP and corneal hydration. In cases where IA and preoperative biometry predictions differed, final IOL power selection was made at the discretion of the operating surgeon. As this was a retrospective analysis of real-world cases, no formal threshold for disparity was defined or applied. IA recommendations were generally prioritized, with final IOL selection decisions made at the discretion of the operating surgeon, consistent with SOC practices across sites. Cases where IA recommendations were overridden may influence interpretation of IA-related prediction error. Challenges such as speculum positioning or corneal surface variability were inherent to routine surgical conditions and were not systematically recorded.
Postoperative Refraction and VA Measurement
Postoperative manifest refraction was recorded during routine follow-up visits at ≥30 days. VA was measured monocularly using Snellen charts or equivalent and converted to logMAR for analysis. Protocols were not standardized across sites; refraction and VA assessments were performed according to each center’s routine clinical practice.
This study adhered to the ethical principles outlined in the Declaration of Helsinki, Good Clinical Practice (GCP), and ISO 14155:2020. Approval for the study, including a waiver of informed consent and authorization for retrospective data extraction from participating centers listed in Supplementary Table 1 using the WaveTec AnalyzOR database, was granted by Sterling Institutional Review Board (Sterling Independent Services, Inc., 6300 Powers Ferry Rd, Suite 600–351, Atlanta, GA 30339, USA www.sterlingirb.com). Approval was obtained prior to study initiation and data access. Public disclosure is available on ClinicalTrials.gov (NCT05796674).
Outcome Measures
All VA outcomes were measured monocularly unless otherwise specified. The primary effectiveness endpoint was the percentage of eyes that achieved CDVA of 20/40 or better ≥ 1 month postoperative. The secondary effectiveness endpoints included the percentage of emmetropia targeted eyes achieving UDVA of 20/40 or better and the mean absolute residual refractive cylinder for Toric models. Exploratory analysis assessed VA and refractive precision metrics, including the percentage of eyes that achieved specific CDVA and UDVA levels, mean manifest refractive spherical equivalent (MRSE) for emmetropia targeted eyes, and the mean absolute residual refractive cylinder for Toric models.
Refractive precision was evaluated by calculating the ORA-prediction error as the difference between postoperative MRSE and the ORA-predicted residual spherical equivalent. When preoperative biometry data was available, biometry prediction error was calculated as the difference between postoperative MRSE and biometry predicted refraction, comparing ORA’s relative accuracy against traditional preoperative calculations. The analysis further evaluated ORA’s effect on the surgeon’s choice of IOL, including the percentage of eyes with match or modified IOL power and model, and the associated VA outcomes, providing insights into ORA’s role in enhancing refractive precision and optimizing patient vision outcomes.
Statistical Analysis
Statistical analyses were performed using SAS® software (SAS Institute Inc., Cary, NC). Statistical summaries (mean and standard deviation [SD] or percentage) were reported for all variables of interest. All analyses were descriptive in nature, no statistical hypothesis testing was conducted to compare subgroups. Analyses included “All eyes” and were stratified by non-Toric (CC60WF, CCA0T0) and Toric (CCW0T3, CCW0T4, CCW0T5, CCW0T6) IOL subgroups to account for potential differences in VA outcomes. Target dependent endpoints (UDVA and MRSE) were analyzed for emmetropia targeted eyes, defined as those with an ORA prediction refraction within ± 0.50 D of the implanted IOL. In this study, ≥ 1 month was defined as ≥ 30 days.
Results
Demographic and Other Baseline Characteristics
All data meeting the selection criteria were extracted from the WaveTec AnalyzOR database on 12 September 2023. The first recorded surgery was on 01 December 2021, and the last postoperative visit was on 08 September 2023. The study included 1090 patients (1404 eyes) across 87 sites in the US, comprising 840 patients (1084 eyes) and 250 patients (320 eyes) in the Clareon non-Toric and Clareon Toric subgroups, respectively (Figure 1). Due to anonymization in the WaveTec AnalyzOR database, demographic data such as race/ethnicity were unavailable; however, baseline and demographic characteristics were comparable across subgroups. The mean age ± SD of the cohort was 71.2 ± 7.66 years, and 675 (61.9%) were females. An anticipated difference in the baseline mean (SD) preoperative cylinder was observed, with 0.81 (0.58) D and 1.50 (0.62) D for the Clareon non-Toric group and Clareon Toric groups, respectively (Table 1). No eyes with ocular comorbidities or pre-existing eye disease were observed in the dataset.
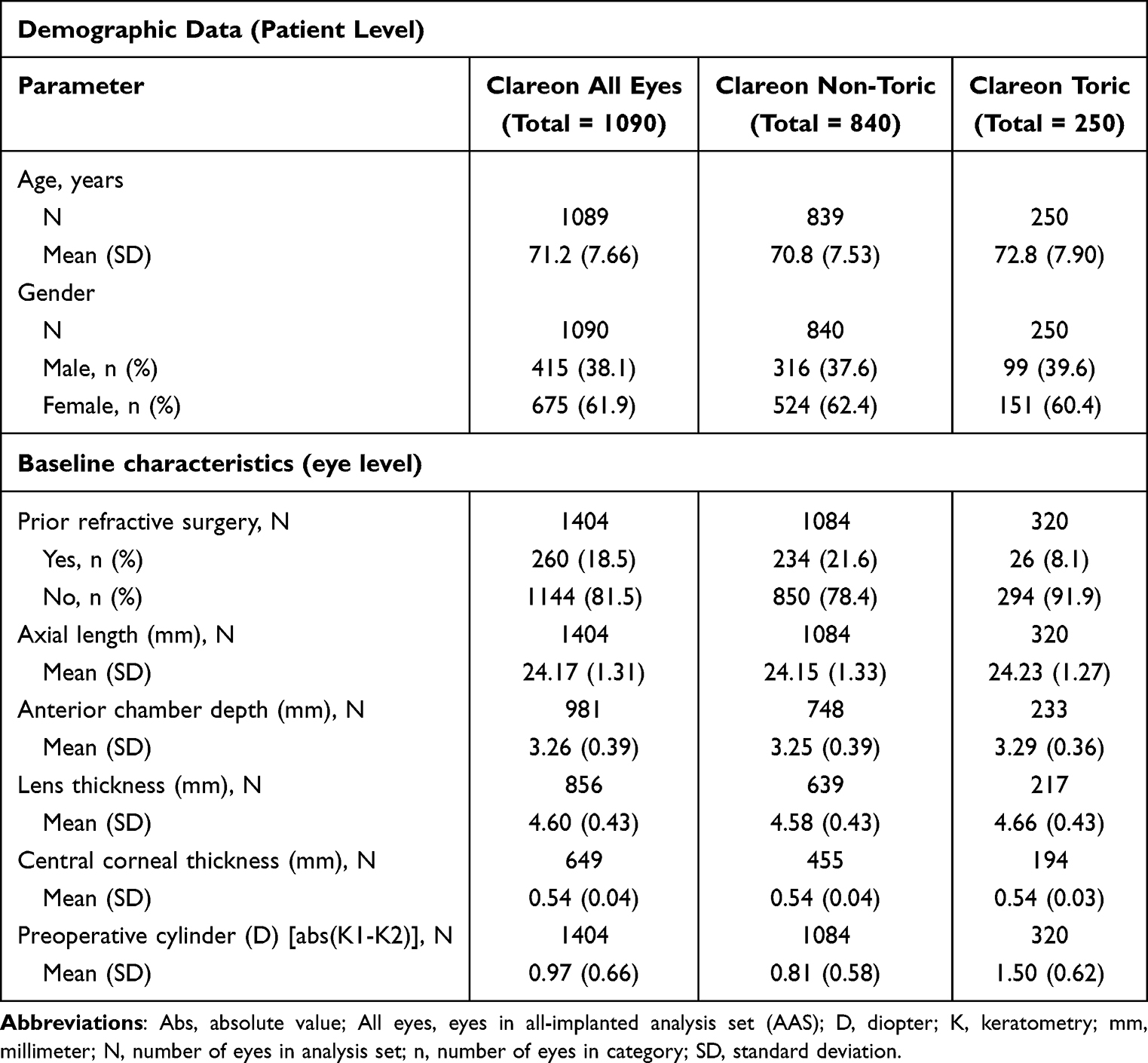 |
Table 1 Patient Demographic and Baseline Characteristics (All-Implanted Analysis Set) |
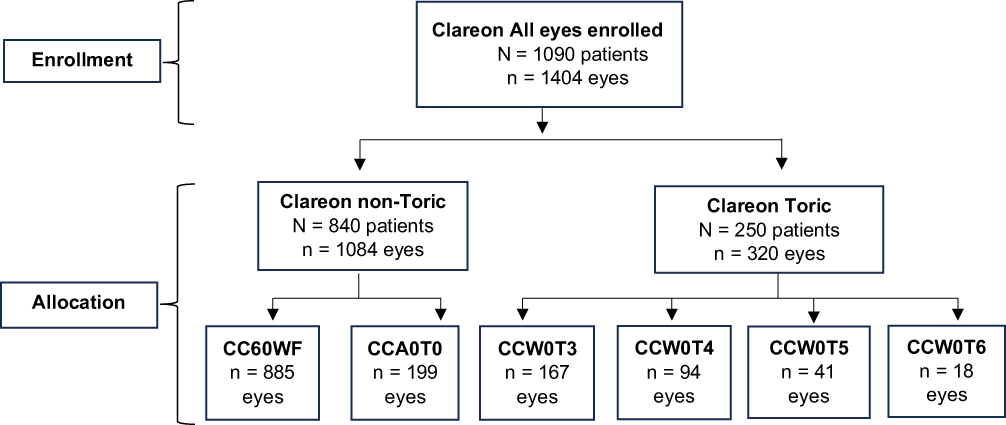 |
Figure 1 Patient disposition. CC60WF and CCA0T0 are identical non-toric Clareon IOLs differing only by delivery system. CCW0T3, CW0T4, CCW0T5, and CCW0T6 are Clareon toric IOLs with identical optical properties, differing in toric power: 1.50 D, 2.25 D, 3.00 D, and 3.75 D at the IOL plane, respectively, for astigmatism correction. Abbreviations: All eyes, eyes in all-implanted analysis set (AAS); N, number of eyes in analysis set; n, number of eyes in category. |
Subgroup analysis focused on lens type (Toric vs non-Toric), prior refractive surgery status, and the match status between preoperative and intraoperative IOL selection. Where feasible, emmetropia targeted eyes were isolated for refractive precision evaluation, defined as those in which the ORA-predicted refraction for the implanted IOL was within ± 0.50 D. Eyes outside this range, including monovision targeting, were categorized as non-emmetropia targeted. Prior refractive surgery included radial keratotomy (RK), photorefractive keratectomy (PRK), automated lamellar keratoplasty (ALK), or laser-assisted in situ keratomileusis (LASIK). Non-emmetropia targeted eyes were retained in broader VA analysis but were not further stratified due to dataset limitations regarding exact intended target refraction.
Visual Acuity Outcomes
The VA outcomes for the Clareon IOL subgroups are shown in Table 2. 98.4% of eyes (1220/1240; 95% confidence interval (CI) [97.5, 99.0]) achieved CDVA of 20/40 or better ≥ 1 month postoperatively. Specifically, 98.1% (948 eyes; 95% CI [97.1, 98.8]) of the Clareon non-Toric and 99.3% (272 eyes; 95% CI [97.1, 99.8]) of the Clareon Toric subgroups achieved these outcomes (Table 2). The mean (SD) CDVA was 0.04 (0.11) logMAR with similar results observed across both subgroups.
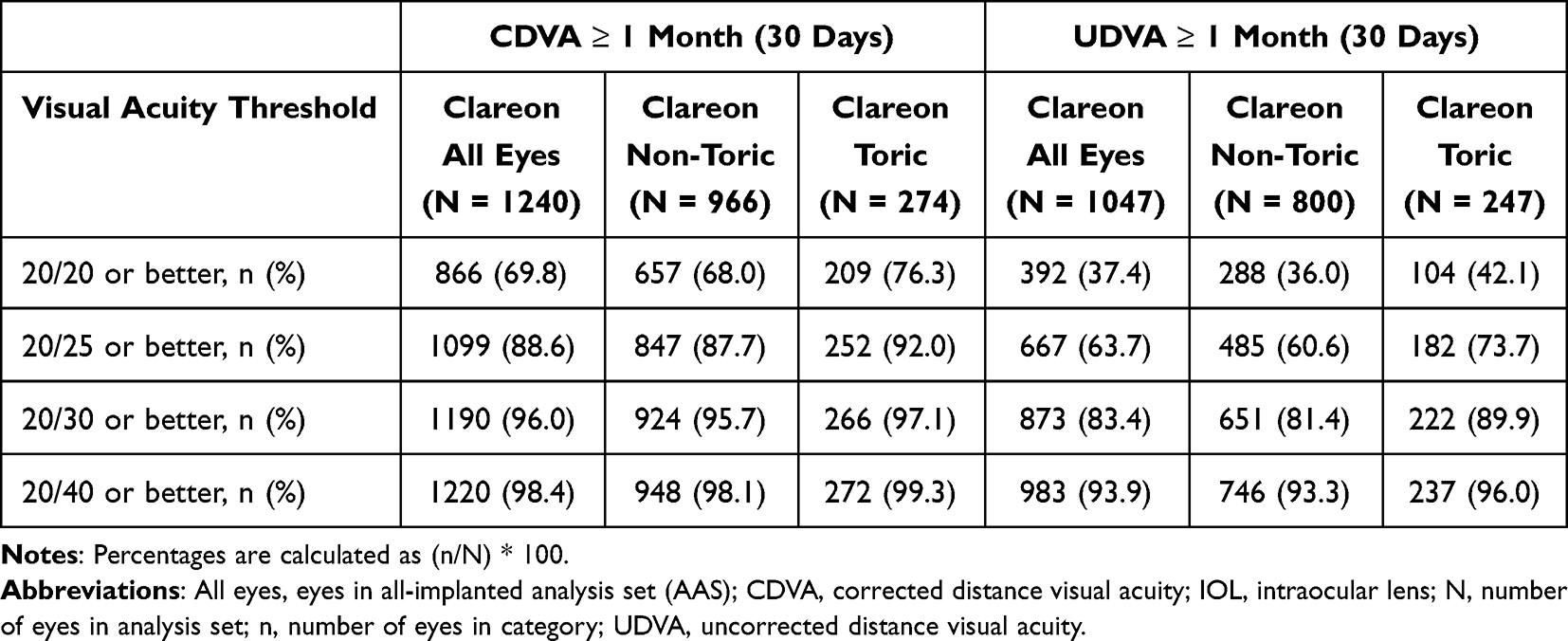 |
Table 2 Percentage of Eyes with CDVA and Emmetropia Targeted Eyes with UDVA of 20/20 or Better, 20/25 or Better, 20/30 or Better, and 20/40 or Better by Clareon IOL Subgroups at ≥ 1 Month Postoperative |
In addition, > 90% of emmetropia targeted eyes achieved UDVA of 20/40 or better across all subgroups. Among 1047 emmetropia targeted eyes, 93.9% (983 eyes; 95% CI [92.4, 95.3]) achieved UDVA of 20/40 or better, including 93.3% (746 eyes; 95% CI [91.5, 95.0]) and 96.0% (237 eyes; 95% CI [92.6, 97.8]) in the non-Toric and Toric subgroups, respectively (Table 2). The mean (SD) UDVA for the 1046 emmetropia targeted eyes in the “All eyes” group was 0.12 (0.15) logMAR, with 0.13 (0.16) logMAR and 0.10 (0.12) logMAR for the Clareon non-Toric (799 eyes) and Clareon Toric subgroup (247 eyes), respectively.
Refractive Outcomes
The mean (SD) MRSE for 1047 emmetropia targeted eyes in the “All eyes” group was −0.15 (0.45) D with subgroup values shown in Figure 2. The mean (SD) absolute residual refractive cylinder for the Clareon Toric models for 274 eyes was 0.40 (0.35) D. Notably, 49.6% (136 eyes) had an absolute residual refractive cylinder of ≤ 0.25 D, 72.6% (199 eyes) had ≤ 0.50 D, and 98.2% (269 eyes) had ≤ 1.00 D.
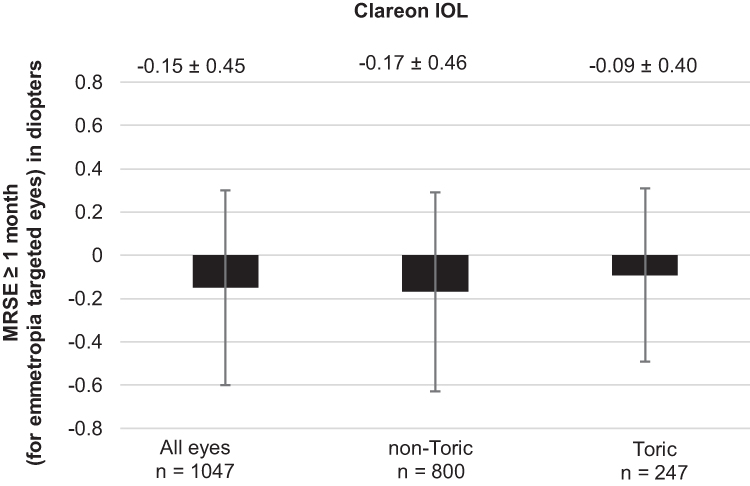 |
Figure 2 Mean MRSE at ≥ 1 month postoperative (emmetropia targeted eyes). Abbreviations: All eyes, eyes in all-implanted analysis set (AAS); IOL, intraocular lens; MRSE, manifest refraction spherical equivalent; n, number of eyes with data. |
Prediction Error
The mean (SD) prediction error was −0.10 (0.49) D in the “All eyes” group, −0.12 (0.49) D in the non-Toric, and −0.05 (0.46) D in the Toric subgroups. Among the 1240 eyes in the “All eyes” group, the mean (SD) absolute prediction error based on ORA predicted vs achieved refractive spherical equivalent was 0.36 (0.35) D.
In 619 eyes where planned and implanted IOL powers match, the mean (SD) difference between absolute ORA prediction error (0.33 [0.32])) and absolute preoperative biometry prediction error (0.32 [0.30]) was 0.01 (0.22) D. For 78.7% of all Clareon IOLs, the difference between the two prediction errors was within ± 0.25 D, with similar results for non-Toric (76.5%) and Toric (86.2%) subgroups (Supplementary Table 2). This analysis specifically focuses on cases with matching planned and implanted IOL powers to ensure consistency and reduce variability in prediction error comparison, as shown in Supplementary Table 2.
Intraoperative IOL Refinement and Match/Change Analysis
Overall, the IOLs match the preoperatively selected sphere power and cylinder/model in 40.8% of cases, with differences observed between the Clareon Toric and non-Toric subgroups (29.9% vs 43.9%, respectively; Table 3). In the non-Toric subset, 82.8% of cases involved either a match (no change) or only a power change, whereas the Toric subgroup exhibited a more even distribution across change types, with 60.2% representing a match or power change. This variability underscores the broader range of adjustments available for the Toric subgroup. Notably, mean CDVA and UDVA outcomes were generally less favorable in eyes with power changes than those with match, cylinder/model changes, or combined power and cylinder/model changes (Table 4). For UDVA, the power change group showed a four-letter difference compared to the cylinder/model change group (logMAR 0.22 vs logMAR 0.14) and was two letters worse than the match and power + cylinder/model change groups. CDVA differences were subtler, with the power change group being approximately one letter worse (0.05 logMAR vs 0.02 logMAR). These findings emphasize the need for further investigation into surgeon decision-making and reliance on preoperative biometry or ORA predictions during IOL selection.
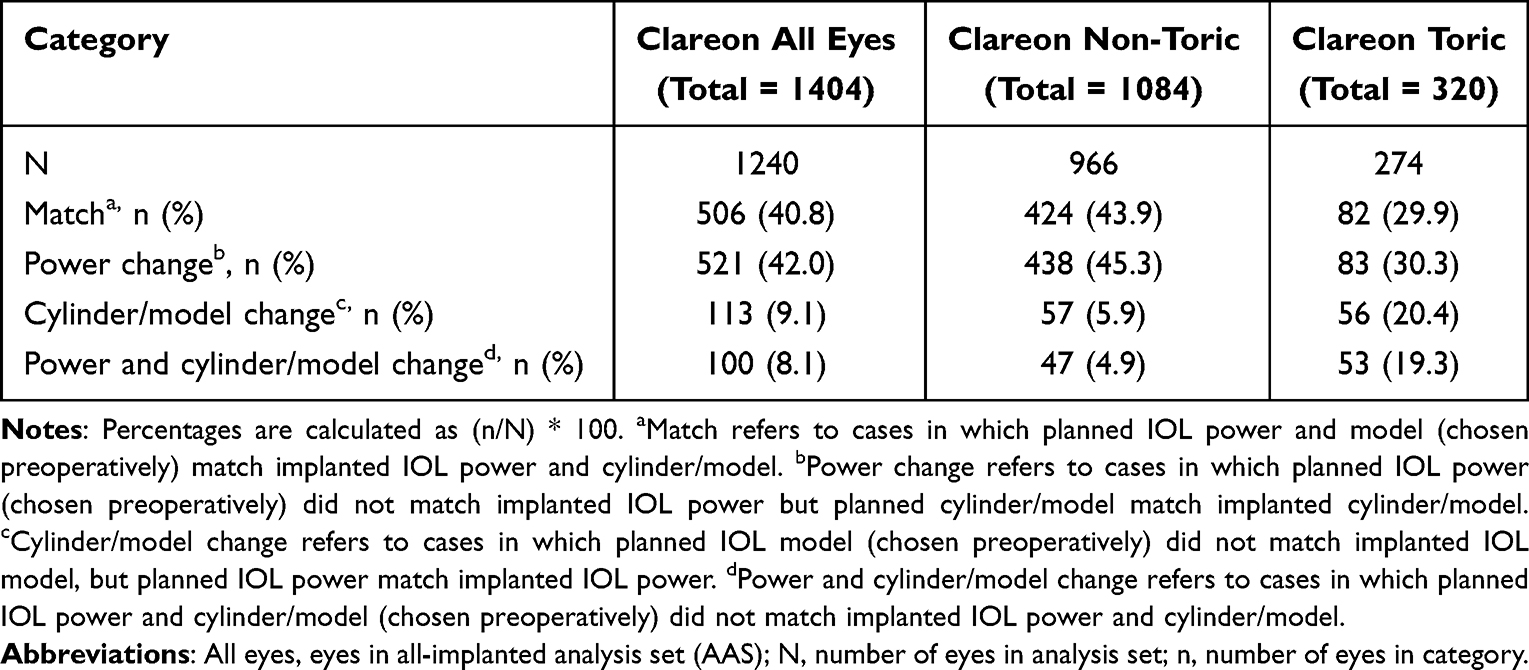 |
Table 3 Percentage of Eyes with Match or Change of Planned IOL Power or Cylinder/Model |
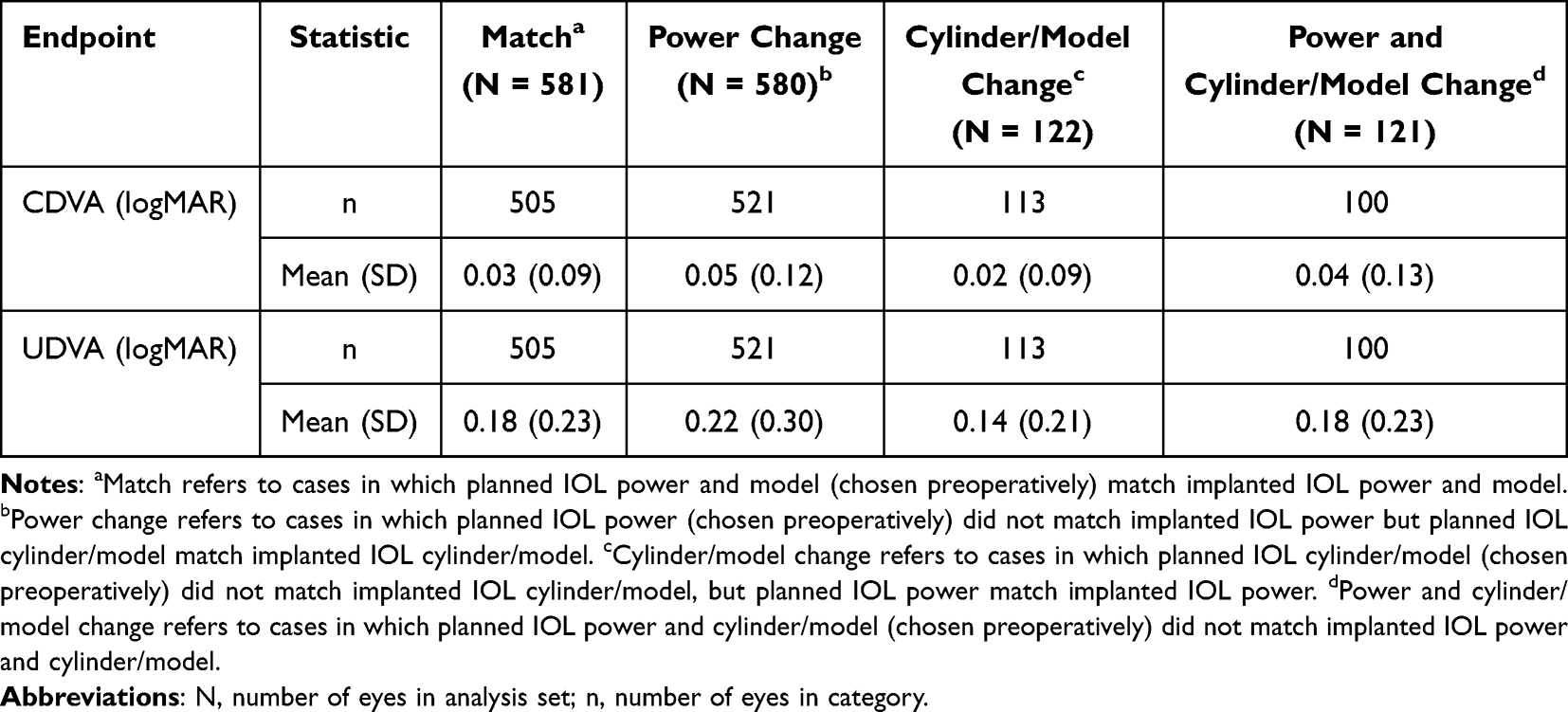 |
Table 4 Monocular Visual Acuity ≥ 1 Month Postoperative, Classified by Match Categories |
ORA played a critical role in refining intraoperative IOL power selection, with 49.9% of cases involving changes to the preoperatively planned IOL power, cylinder, or both. Among matched eyes, 29.1% reflected agreement between ORA suggestions and preoperative calculations, while 20.9% observed the surgeon’s preoperative selection overrode ORA recommendations (Supplementary Table 3). Differences between Clareon Toric and non-Toric subgroups further highlighted ORA’s role in astigmatic correction, with fewer matches (29.9%) in the Clareon Toric group (Table 3). Though ORA influenced nearly half of all cases by fine-tuning IOL selection through real-time measurements, it complemented, rather than replaced, preoperative planning, improving the accuracy of IOL power selection and aligning final outcomes more closely with patients’ anatomical and refractive needs, particularly in astigmatic correction (Supplementary Table 3). Percentages in Table 3 reflect the type of change relative to the preoperative plan, whereas Supplementary Table 3 reflects decision influence (preoperative calculation chosen, ORA match, or ORA influenced). As these categories reflect different aspects of IOL selection, they are not directly comparable across tables.
Discussion
The main objective of this study was to generate RWE to enhance understanding of Clareon UVA IOL performance using WaveTec AnalyzOR data. To our knowledge, this is the largest and most comprehensive multicenter study to evaluate both Clareon UVA non-Toric and Toric IOLs using multicenter postoperative data stored in ORA, filling the research gap. While the literature discusses the ORA System extensively,26 studies focusing on the performance of Clareon and Clareon Toric IOLs using ORA remain limited. Spekreijse et al27 explored Clareon outcomes with ORA, but their study was limited to 100 eyes. In contrast, our study investigates Clareon IOL performance using postoperative data stored in ORA from 1404 eyes across 87 sites in the US, providing robust evidence on Clareon IOL effectiveness guided by ORA in a real-world clinical setting. This distinction underscores the significance of our findings in advancing the understanding of Clareon IOL performance in a real-world setting.
In our study, 98.4% of implanted eyes achieved CDVA of 20/40 (0.3 logMAR) or better, and 93.9% of emmetropia targeted eyes achieved a UDVA of 20/40 (0.3 logMAR) or better at ≥ 1 month postoperative. These findings highlight the Clareon IOL’s effectiveness in clinical settings. Notably, our results align with prospective studies, highlighting the reliability of Clareon IOL’s performance. For instance, Agarwal et al observed comparable high visual outcomes with Clareon and AcrySof IQ lenses,28 while Blehm et al reported stable refractive results and good VA in a prospective cohort.29 Additionally, Bouvarel et al’s long-term data support our findings, demonstrating sustained high VA and stability over time.11 This alignment with prospective research demonstrates the Clareon IOL’s consistent performance across various study designs, supporting the validity of our real-world outcomes. Furthermore, the mean residual cylinder in 274 eyes implanted with Clareon Toric IOLs was 0.40 D at ≥ 1 month postoperative, aligning with the typical range (0.30 D to 0.76 D) reported in the literature.29–32 Additionally, 49.6% and 72.6% of Toric eyes had residual refractive cylinders of ≤ 0.25 D and ≤ 0.50 D, respectively, and 98.2% had a residual cylinder of ≤ 1.00 D. While specific cutoff distributions vary across studies, these outcomes fall within the range of results observed in prior clinical evaluations of Toric IOLs in both prospective and real-world settings.29–32 These results support the favorable refractive performance observed in this cohort and may serve as a reference point for future comparative or long-term evaluations.
Refractive outcomes after cataract surgery significantly impact patient satisfaction, including visual clarity, functional vision, and overall quality of life.33,34 Despite advancements in IOL calculation formulas, some patients still experience unwanted refractive errors. One approach to reducing these errors associated with preoperative IOL calculations is applying an intraoperative measurement system after removing the crystalline lens. This ensures an accurate measurement of aphakic refraction, which infers refractive corneal power and axial length. These two key variables determine aphakic refraction value and total, leading to a more precise IOL selection and improved visual outcome. However, evidence of improving IOL power calculation using IA remains mixed.27 Cionni et al’s analysis of a multicenter dataset of over 30,000 eyes found IA outperforming preoperative calculations in eyes with no history of refractive surgery.17 In contrast, other single site studies18,35 concluded that IA did not improve refractive outcomes. In our multicenter study, eyes with similar planned and implanted IOL power showed minimal difference between ORA and preoperative biometry prediction error, with 78.7% of cases within ± 0.25 D. This indicates that, in a diverse dataset of real-world instances, IA provided results comparable to preoperative biometry. The surgeon’s experience, patient population, and surgical environment may influence mixed results on IA efficacy. Our study did not investigate prediction error differences at the surgeon or site level, as this was not the focus of our research. Further studies are warranted to understand IA’s role in enhancing refractive outcomes across different clinical settings.
Prior refractive surgery may confound IOL power selection.36 Intraoperative wavefront aberrometry, such as ORA, has been suggested to reduce IOL power calculation error in such eyes.37 While studies have demonstrated potential benefits, the evidence remains mixed, and further research is warranted.36 A recent systematic review and network analysis on IOL power calculations in eyes post myopic laser surgery identified ORA as highly effective, providing the highest proportion of eyes achieving postoperative refractive error within ± 0.50 and ± 1.00 D, with the lowest mean and median absolute errors.38 In our study, although 83% of eyes with prior refractive surgery required power changes per ORA, the absolute prediction error was still >1 D, suggesting prior refractive surgery may impact postoperative refraction predictability even when using IA.35,39 While this study did not primarily focus on differences in IA effectiveness by the surgeon or site, multicenter studies or detailed subgroup analyses could provide insights into IA’s impact on refractive outcomes across clinical settings.
In our study, about 60% of eyes received a Clareon IOL different from the preoperatively selected IOL in power, model/cylinder, or both. Notably, the ORA dataset was limited to eyes implanted with Clareon IOLs but did not restrict the planned IOL type, explaining the 6% of non-Toric cases. A 4-letter difference in UDVA between eyes with power changes and those with confirmed IOL powers suggests confounding factors affecting IOL power selection. Variations in corneal curvature, posterior corneal power, anterior chamber depth, and residual refractive errors may affect IOL power selection beyond preoperative formula predictions. These findings underscore the practical implications of using ORA in IOL power selection. While ORA demonstrates significant accuracy and benefits, particularly in post-myopic laser surgery eyes in other studies, its performance varies by the IOL type and surgical history.38 This study provides real-world data on ORA use with Clareon IOLs, strengthening our comprehensive understanding of Clareon IOL performance and its potential to improve postoperative refractive outcomes.
The WaveTec AnalyzOR system, with its broad inclusion of preoperative, intraoperative, and postoperative data across multiple US surgical centers, supports large-scale, real-world IOL evaluation but also introduces certain limitations. The retrospective design is subject to reporting bias, as surgeons might selectively enter data for eyes that achieved desired outcomes to optimize surgeon-related factors. Consequently, the dataset likely underrepresents eyes with comorbidities or surgical complications, limiting the findings’ applicability to a broader patient population. As with most retrospective real-world datasets, potential selection bias may exist, with surgeons more likely to enter outcomes from routine or uncomplicated cases. Although no exclusion criteria were applied due to this design, the WaveTec AnalyzOR system, typically employed for accuracy and performance tracking, suggests that the cohort predominately includes eyes that underwent uncomplicated cataract surgery. Despite being a RWE study, the data reflect cases that surgeons chose to enter for postoperative review, rather than all treated eyes. This limitation also restricted data on certain subgroups. Eyes with prior refractive surgery were included; however, no dedicated subgroup analysis was performed as the study aimed to evaluate Clareon IOL performance in a real-world context, and inclusion of post-refractive cases could introduce negative bias in accuracy outcomes. The role of IA in these eyes warrants further investigation in prospective studies.
Comparisons between Toric and non-Toric were based on implanted lens type, but potential crossover effects were not accounted for, where ORA might have influenced the lens selection. The single-arm design also precluded direct comparisons with other IOL platforms. Future studies should include head-to-head comparisons between IOL platforms and assess a broader range of clinical outcomes. Additionally, anonymizing patient information limits access to demographic details like race and ethnicity, which may affect the interpretation of specific outcomes. Another limitation is the use of logMAR equivalents. The dataset did not capture additional letters read or missed during VA assessments, which may have impacted the accuracy of the logMAR conversions and, consequently, the mean VA outcomes.
Despite these limitations, the multicenter design, with data from diverse practices, enhances the overall applicability of these findings to real-world clinical settings. Including diverse surgical environments provides valuable insights into postoperative outcomes across various practice types, strengthening the study’s contribution to the growing body of RWE in ophthalmology.
Conclusion
This large-scale real-world study provides compelling evidence of the visual performance of both non-Toric and Toric Clareon models, consistent with outcomes from prospective Clareon studies,6,8 when guided by ORA IA. The study showed that most eyes achieved UDVA and CDVA of 20/40 or better with minimal residual refractive error at ≥ 1 month postoperative, indicating that the ORA system may be useful in cataract surgery for IOL power calculation and axis positioning to enhance refractive target accuracy in clinical practice.
Data Sharing Statement
The primary study data are available at (Identifier: NCT05796674), which includes registration details and summary results. Additional individual-level data can be requested from the corresponding author, subject to privacy and ethical restrictions.
Acknowledgments
The article writing and editorial services were provided by Yugandhar Vudhya Gowrisankar, PhD and Hanieh Mirhajianmoghadam, PhD (employed by Alcon). The authors extend their special thanks to Hanieh Mirhajianmoghadam for her valuable contributions to the execution of the study and the preparation of this article.
Funding
This study was funded by Alcon Research, LLC. Fort Worth, TX, USA.
Disclosure
W. F. Wiley is a consultant for Alcon Vision, LLC., Carl Zeiss Meditec AG., Johnson & Johnson Vision., and Bausch & Lomb, Inc. A. Rendon is an employee of Alcon Laboratories, Inc. The authors report no other conflicts of interest in this work.
References
1. Mencucci R, Cennamo M, Venturi D, Vignapiano R, Favuzza E. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J Cataract Refract Surg. 2020;46(3):378–387. doi:10.1097/j.jcrs.0000000000000061
2. Oshika T, Fujita Y, Inamura M, Miyata K. Mid-term, and long-term clinical assessments of a new 1-piece hydrophobic acrylic IOL with hydroxyethyl methacrylate. J Cataract Refract Surg. 2020;46(5):682–687. doi:10.1097/j.jcrs.0000000000000142
3. Werner L, Thatthamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490–1497. doi:10.1016/j.jcrs.2019.05.017
4. Das KK, Werner L, Collins S, Hong X. In vitro and schematic model eye assessment of glare or positive dysphotopsia-type photic phenomena: comparison of a new material IOL to other monofocal IOLs. J Cataract Refract Surg. 2019;45(2):219–227. doi:10.1016/j.jcrs.2018.09.017
5. De Giacinto C, Porrelli D, Turco G, Pastore MR, D’Aloisio R, Tognetto D. Surface properties of commercially available hydrophobic acrylic intraocular lenses: comparative study. J Cataract Refract Surg. 2019;45(9):1330–1334. doi:10.1016/j.jcrs.2019.04.011
6. Lehmann R, Maxwell A, Lubeck DM, Fong R, Walters TR, Fakadej A. Effectiveness and safety of the clareon monofocal intraocular lens: outcomes from a 12-month single-arm clinical study in a large sample. Clin Ophthalmol. 2021;15:1647–1657. doi:10.2147/OPTH.S295008
7. Kim HK, Seo KY, Yoon KC, et al. Clinical evaluation of a hydrophobic intraocular lens using a preloaded automated injector in a Korean population. Clin Ophthalmol. 2023;17:3353–3363. doi:10.2147/OPTH.S421864
8. Oshika T, Sasaki N, Clinical Study Group on New Intraocular Lens and Delivery System. One-year multicenter evaluation of a new hydrophobic acrylic intraocular lens with hydroxyethyl methacrylate in an automated preloaded delivery system. J Cataract Refract Surg. 2022;48(3):275–279. doi:10.1097/j.jcrs.0000000000000746
9. Titiyal JS, Basak SK, Shetty N, et al. Twelve-months follow-up postmarket study of a hydrophobic intraocular lens using a preloaded automated injector in an Indian population. Clin Ophthalmol. 2022;16:4215–4225. doi:10.2147/OPTH.S379054
10. Tsuji A, Kawai K. Long-term stability of new acrylic intraocular lens materials by accelerated severe aging test. Tokai J Exp Clin Med. 2022;47(1):9–12.
11. Bouvarel H, Agard E, Billant J, et al. Long-term real-life outcomes of the Clareon® hydrophobic intraocular lens: the Clarte study in 191 eyes: 3-years real-life outcomes of the Clareon® intraocular lens. BMC Ophthalmol. 2024;24(1):133. doi:10.1186/s12886-024-03393-x
12. Tran E, Shah N, Caballero Ortiz S, et al. Visual performance and refractive stability of clareon® monofocal intraocular lens implanted with an automated delivery system. Clin Ophthalmol. 2025;19:3933–3939. doi:10.2147/OPTH.S545977
13. Koch DD. The enigmatic cornea and intraocular lens calculations: the LXXIII edward jackson memorial lecture. Am J Ophthalmol. 2016;171:xv–xxx. doi:10.1016/j.ajo.2016.08.020
14. Petermeier K, Gekeler F, Messias A, Spitzer MS, Haigis W, Szurman P. Intraocular lens power calculation and optimized constants for highly myopic eyes. J Cataract Refract Surg. 2009;35(9):1575–1581. doi:10.1016/j.jcrs.2009.04.028
15. Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. Intraocular lens formula constant optimization and partial coherence interferometry biometry: refractive outcomes in 8108 eyes after cataract surgery. J Cataract Refract Surg. 2011;37(1):50–62. doi:10.1016/j.jcrs.2010.07.037
16. Cooke DL, Cooke TL. Comparison of 9 intraocular lens power calculation formulas. J Cataract Refract Surg. 2016;42(8):1157–1164. doi:10.1016/j.jcrs.2016.06.029
17. Cionni RJ, Dimalanta R, Breen M, Hamilton C. A large retrospective database analysis comparing outcomes of intraoperative aberrometry with conventional preoperative planning. J Cataract Refract Surg. 2018;44(10):1230–1235. doi:10.1016/j.jcrs.2018.07.016
18. Solomon KD, Sandoval HP, Potvin R. Evaluating the relative value of intraoperative aberrometry versus current formulas for toric IOL sphere, cylinder, and orientation planning. J Cataract Refract Surg. 2019;45(10):1430–1435. doi:10.1016/j.jcrs.2019.05.023
19. Ianchulev S. Intraoperative Aberrometry. In: Aramberri J, Hoffer KJ, Olsen T, Savini G, Shammas HJ editors. Intraocular Lens Calculations. Springer International Publishing; 2024:673–687. doi:10.1007/978-3-031-50666-6_45
20. Hatch KM, Woodcock EC, Talamo JH. Intraocular lens power selection and positioning with and without intraoperative aberrometry. J Refract Surg. 2015;31(4):237–242. doi:10.3928/1081597X-20150319-03
21. Woodcock MG, Lehmann R, Cionni RJ, Breen M, Scott MC. Intraoperative aberrometry versus standard preoperative biometry and a toric IOL calculator for bilateral toric IOL implantation with a femtosecond laser: one-month results. J Cataract Refract Surg. 2016;42(6):817–825. doi:10.1016/j.jcrs.2016.02.048
22. Stringham J, Pettey J, Olson RJ. Evaluation of variables affecting intraoperative aberrometry. J Cataract Refract Surg. 2012;38(3):470–474. doi:10.1016/j.jcrs.2011.09.039
23. Masket S, Fram NR, Holladay JT. Influence of ophthalmic viscosurgical devices on intraoperative aberrometry. J Cataract Refract Surg. 2016;42(7):990–994. doi:10.1016/j.jcrs.2016.04.022
24. Watanabe K. Evaluation of refractive accuracy of ORA and the factors impacting residual astigmatism in patients implanted with trifocal IOLs during cataract surgery: a retrospective observational study. Clin Ophthalmol. 2022;16:2491–2503. doi:10.2147/OPTH.S371555
25. Davidson J, Gu X, Breen M, Babu RJ. Impact of global optimization of lens constants on absolute prediction error for final IOL power selection when using intraoperative aberrometry. Clin Ophthalmol. 2022;16:3155–3164. doi:10.2147/OPTH.S369797
26. Kaufman AR, Pineda R. Intraoperative aberrometry: an update on applications and outcomes. Curr Opin Ophthalmol. 2023;34(1):48–57. doi:10.1097/ICU.0000000000000915
27. Spekreijse LS, Bauer NJC, van den Biggelaar FJHM, et al. Predictive accuracy of an intraoperative aberrometry device for a new monofocal intraocular lens. J Cataract Refract Surg. 2022;48(5):542–548. doi:10.1097/j.jcrs.0000000000000791
28. Agarwal S, Thornell E. Comparison of visual outcomes and patient satisfaction following cataract surgery with two monofocal intraocular lenses: clareon® AcrySof® IQ monofocal. Open Ophthalmol J. 2021;15:144–150. doi:10.2174/1874364102115010144
29. Blehm C, Hall B. Evaluation of visual outcomes and 3-month refractive stability of a new hydrophobic acrylic intraocular lens. Clin Ophthalmol. 2023;17:1859–1864. doi:10.2147/OPTH.S415400
30. Emesz M, Dexl AK, Krall EM, et al. Randomized controlled clinical trial to evaluate different intraocular lenses for the surgical compensation of low to moderate-to-high regular corneal astigmatism during cataract surgery. J Cataract Refract Surg. 2015;41(12):2683–2694. doi:10.1016/j.jcrs.2015.07.036
31. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40(10):1654–1660. doi:10.1016/j.jcrs.2014.01.044
32. Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof Toric intraocular lenses. Br J Ophthalmol. 2016;100(2):263–268. doi:10.1136/bjophthalmol-2015-306656
33. Conner-Spady BL, Sanmugasunderam S, Courtright P, McGurran JJ, Noseworthy TW. Steering committee of the Western Canada waiting list project. determinants of patient satisfaction with cataract surgery and length of time on the waiting list. Br J Ophthalmol. 2004;88(10):1305–1309. doi:10.1136/bjo.2003.037721
34. Hawker MJ, Madge SN, Baddeley PA, Perry SR. Refractive expectations of patients having cataract surgery. J Cataract Refract Surg. 2005;31(10):1970–1975. doi:10.1016/j.jcrs.2005.03.065
35. Raufi N, James C, Kuo A, Vann R. Intraoperative aberrometry vs modern preoperative formulas in predicting intraocular lens power. J Cataract Refract Surg. 2020;46(6):857–861. doi:10.1097/j.jcrs.0000000000000173
36. Wang L, Koch DD. Intraocular lens power calculations in eyes with previous corneal refractive surgery: review and expert opinion. Ophthalmology. 2021;128(11):e121–e131. doi:10.1016/j.ophtha.2020.06.054
37. Christopher KL, Patnaik JL, Ifantides C, et al. Time utilization and refractive prediction enhancement associated with intraoperative aberrometry use during cataract surgery. Clin Ophthalmol. 2021;15:531–539. doi:10.2147/OPTH.S287573
38. Wen D, Yu J, Zeng Z, et al. Network meta-analysis of no-history methods to calculate intraocular lens power in eyes with previous myopic laser refractive surgery. J Refract Surg. 2020;36(7):481–490. doi:10.3928/1081597X-20200519-04
39. Gasparian SA, Nassiri S, You H, Vercio A, Hwang FS. Intraoperative aberrometry compared to preoperative Barrett True-K formula for intraocular lens power selection in eyes with prior refractive surgery. Sci Rep. 2022;12(1):7357. doi:10.1038/s41598-022-11462-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.