Back to Journals » Drug Design, Development and Therapy » Volume 20
Multi-Technology Empowers Dissolving Microneedles: A Novel Strategy in Rheumatoid Arthritis
Authors Wei TT, Song YM, Zhai BT, Qiao JX ![]() , Fan QQ, Cheng JX, Quan LN, Guo DY
, Fan QQ, Cheng JX, Quan LN, Guo DY ![]() , Cao W
, Cao W ![]()
Received 22 September 2025
Accepted for publication 10 February 2026
Published 4 March 2026 Volume 2026:20 569186
DOI https://doi.org/10.2147/DDDT.S569186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Georgios Panos
Tian-tian Wei,1,2 Yu-meng Song,1 Bing-tao Zhai,1 Jia-xin Qiao,1 Qiang-qiang Fan,1 Jiang-xue Cheng,1 Li-na Quan,1 Dong-yan Guo,1 Wei Cao2
1Shaanxi Province Key Laboratory of New Drugs and Chinese Medicine Foundation Research, Shaanxi University of Chinese Medicine, Xi’an, 712046, People’s Republic of China; 2Department of Rheumatology, Wang Jing Hospital, China Academy of Chinese Medicine Science, Beijing, 100102, People’s Republic of China
Correspondence: Dong-yan Guo; Wei Cao, Email [email protected]; [email protected]
Abstract: Rheumatoid arthritis (RA) is a systemic autoimmune disease associated with chronic inflammation. Current clinical management is confronted with multiple challenges, such as suboptimal drug bioavailability, insufficient joint targeting, and poor patient compliance, which critically limit therapeutic efficacy. Dissolving microneedles (DMNs) can overcome the limitations of traditional treatments through minimally invasive transdermal delivery, improve efficacy and reduce toxicity and side effects, offering an innovative solution for RA treatment. This article reviews the advantages of DMNs for RA, analyzes the advantages and limitations of their preparation methods, the physicochemical properties of DMN matrix materials and the application progress in RA treatment. The synergistic strategies of DMNs with nano-delivery systems, cell membrane bionics, stimulus response delivery systems and phototherapy are further discussed. This multi-technology integration solution solves the problems of poor targeting, low bioavailability, high toxic side effects, and poor patient compliance in RA treatment through the advantages of physical targeting, intelligent controlled release and portable drug delivery. Finally, combined with the patent landscape and clinical research progress, the existing challenges and future development prospects of DMNs in RA treatment are analyzed, hoping to provide theoretical basis and technical breakthrough direction for RA treatment.
Keywords: dissolving microneedle, rheumatoid arthritis, transdermal administration, nano-delivery, stimulus response system, cell membrane bionics, phototherapy
Introduction
Rheumatoid arthritis (RA), a systemic autoimmune disease, features chronic inflammation leading to synovitis and cartilage destruction.1 Clinical manifestations include persistent pain, stiffness and dysfunction. In severe cases, systemic complications such as cardiovascular, pulmonary and neurological lesions may occur.2 According to epidemiological research, RA affects about 1% of the world’s population. Females are more susceptible to RA infection than males, and it can appear at any age.3,4 The underlying mechanisms of RA remain incompletely understood, which may be related to many factors such as heredity, environment, immunity and infection.5 The primary objective of RA treatment is currently focused on alleviating pain and arresting or decelerating the progression of joint injury. The drugs used in clinical practice include non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticoids (GCs), disease-modifying and anti-rheumatic drugs (DMARDs), biologics, targeted preparations and traditional Chinese medicines.1,6–8 Although drug therapy, including biologics and targeted agents, has made progress. For example, the oral JAK inhibitor tofacitinib can exert anti-inflammatory effects by disrupting the cytokine cascade reaction by interfering with the signal transduction of the JAK-STAT pathway within cells.9 Intra-articular injection of biological agents can effectively delay the progression of joint injury in RA.6 However, the limitations of traditional drug delivery methods still restrict the clinical therapeutic effect for a long time. Oral administration is easy to cause gastrointestinal irritation and liver first pass effect, and injection administration has the risk of pain, discomfort and infection. Both types of administration methods are faced with common problems such as lack of joint targeting, low drug bioavailability, and poor long-term treatment compliance in patients with severe side effects.8,10–12 These challenges have prompted researchers to devote themselves to developing innovative drug delivery systems that are efficient, safe and convenient.
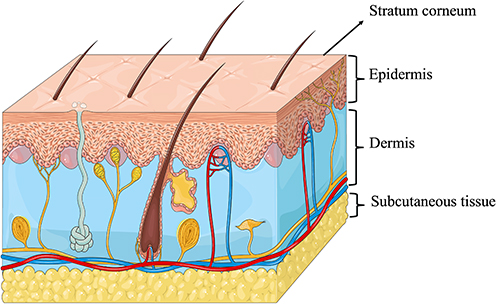 |
Figure 1 Stratified barriers of human skin. Image credit: Server Medical Art (www.smart.servier.com), modified by the authors using Microsoft PowerPoint 2025. |
The transdermal drug delivery system (TDDS) is gradually becoming an emerging strategy for RA management due to their unique advantages. Transdermal delivery of RA therapeutic drugs can avoid gastrointestinal irritation and liver first pass effect, maintain stable blood drug concentration, and provide good drug bioavailability and patient compliance.13,14 However, the physiological structure of the skin limits the application of TDDS. As shown in Figure 1, the skin consists of the stratum corneum, epidermis, dermis and subcutaneous tissue, with different physicochemical properties between layers. For RA therapeutic drugs to reach systemic circulation or deeper tissues, they must first penetrate the stratum corneum and epidermis to access dermis.15 The stratum corneum, as the outermost hydrophobic barrier, hinders the penetration of hydrophilic drugs and macromolecular drugs, such as biological agents and corticosteroids.16 Although various drug penetration promotion techniques have been reported in studies, including chemical penetration promoters,17 ion electroosmosis therapy,18 electroporation19 and ultrasound electroosmosis therapy20 to improve the transdermal delivery efficiency of drugs, their clinical transformation is hindered by complexity, skin irritation and inconsistent efficacy.21
The emergence of microneedle (MN) technology provides innovative solutions to break through the stratum corneum barrier. MNs arrays typically feature conical, pyramidal, or faceted perforated structures, with dimensional ranges of 100–1000 μm in length, 50–250 μm base width, and 1–25 μm tip diameter.22 MNs form temporary channels in the stratum corneum of the skin by mechanical puncture, which can effectively overcome the penetration problem of hydrophilic or macromolecular drugs.23 At the same time, MNs can avoid contact with nerve fibers and blood vessels in the epidermis and dermis, enabling painless drug delivery.24 Compared with traditional injections, MNs reduce the risk of invasiveness while ensuring efficient drug delivery, especially for patients with chronic diseases such as RA that require long-term treatment and those who are sensitive to pain. According to morphological characteristics and differences in drug release mechanism, MNs can be divided into five categories, with their structural characteristics illustrated in Figure 2: solid microneedles (Figure 2A), coated microneedles (Figure 2B), hollow microneedles (Figure 2C), DMNs (Figure 2D) and hydrogel microneedles (Figure 2E).25 Among them, DMNs are composed of a polymer matrix with good biocompatibility and biodegradability that achieve drug delivery through the mechanism of “poke and release”. When DMNs are inserted into the skin, the tip of the needle dissolves or degrades in the presence of interstitial fluid, allowing controlled release of the encapsulated drug to the target site.26 DMNs have the advantages of precision drug delivery and biological safety, which has become the frontier of MNs technology application.
 |
Figure 2 Schematic diagram of the classification and mechanism of microneedles: (A) Solid MNs, (B) Coated MNs, (C) Hollow MNs, (D) Dissolving MNs, (E) Hydrogel MNs. Image credit: Freepik (www.freepik.com), modified by the authors using Microsoft PowerPoint 2025. |
DMNs have shown many advantages in the treatment of RA, but the complexity of the pathological mechanism of RA and the precision of clinical treatment make it difficult for single DMN technology to meet the needs of clinical treatment. Problems such as insufficient loading efficiency of hydrophobic drugs, limited lesion targeting, and difficulty in adapting drug release to fluctuations in disease conditions have promoted the combination of DMNs with other technologies. At present, studies have reported the combination of DMNs with nano-preparations and pH/ROS-responsive systems. However, the research is mostly decentralized, and there is a lack of review of how the combined strategy can solve the problems in RA treatment. In addition, the study of DMNs for RA treatment mostly stays in preclinical studies. The key reasons for the slow clinical transformation process have not been fully analyzed. To comprehensively summarize the research progress of DMNs in the treatment of RA, relevant literatures from 2005 to 2025 were retrieved from PubMed and Web of Science in this review. The search terms mainly included “rheumatoid arthritis”, “RA”, “dissolving microneedles”, “microneedles”, “soluble microneedles” and “delivery system”. At the same time, relevant patent and clinical trial database searches are supplemented.
Based on the current research, this article will review the advantages of DMNs in RA treatment, analyze their preparation methods, physicochemical properties of matrix materials, and their application progress in RA treatment. A particular focus will be placed on the combined application of DMNs with nano-delivery systems, stimulus-responsive systems, and photodynamic/photothermal therapy in RA. In addition, the existing challenges and future development prospects of DMNs in RA treatment will be analyzed. It is hoped to provide a theoretical basis for the development of efficient drug delivery system for RA treatment and provide a technical breakthrough direction for the clinical transformation of DMNs combined technology.
Advantages of DMNs in the Treatment of RA
Improving Safety
In the treatment of RA, compared with solid MNs (Figure 2A), coated MNs (Figure 2B), and hollow MNs (Figure 2C), DMNs (Figure 2D) show excellent safety due to the biocompatibility and biodegradability of the matrix materials. Solid, coated, and hollow MNs are made from materials such as ceramics, metals, silicon, and glass. They are prone to form sharp waste residues when insufficient mechanical strength results in insertion failure or when the microneedle is partially broken after insertion into the skin.27 Hollow MNs have a cavity structure, as shown in Figure 2C. Upon insertion into the skin, MNs arrays facilitate pressure-driven infusion of drug solutions through microcavities, enabling subcutaneous delivery akin to injection. However, hollow MNs are not only complicated to prepare, but also easy to break the needle body due to improper operation, and the skin tissue is also easy to block the needle hole.25 As shown in Figure 2E, hydrogel MNs are prepared by polymer cross-linking and swelling. After insertion into the skin, the hydrogel MNs can rapidly absorb the interstitial fluid and form a hydrogel tube to deliver the drug in the hydrogel MNs to the dermis to achieve drug diffusion.28 However, due to the swelling of the hydrogel matrix, hydrogel MNs can resist the closure of micropores to a certain extent, resulting in prolonged recovery time of micropores and an increased risk of infection. In contrast, DMNs are based on biocompatible and biodegradable natural or synthetic polymers such as hyaluronic acid (HA), chondroitin sulfate (CS), and polyvinylpyrrolidone (PVP), which can be degraded by physiological metabolic pathways after drug delivery without any waste products.23 Therefore, DMNs can improve the safety of RA treatment compared with other types of MNs.
Improve the Drug Loading Capacity
Compared with other types of MNs, DMNs show differences and unique advantages in drug loading. As shown in Figure 2A, solid MNs do not inherently carry drugs and their use involves a two-step process: first, creating microchannels in the skin, followed by applying a drug solution, cream, or patch to the pretreated area to enhance permeation and absorption. Coated MNs are derived from solid MNs, as shown in Figure 2B, on which therapeutic drugs are coated on the surface of the needle tip. Upon insertion into the skin, these coatings dissolve to facilitate localized drug delivery. Although they avoid the complexity of two-step operation of solid MNs, their drug loading is very limited.29 Hollow MNs can achieve drug loading through hollow structure, which can increase the drug loading, but there are problems such as complex preparation process and high cost.25 DMNs neither rely on surface coatings nor on hollow structures but enable drugs to be uniformly dispersed within the microneedle matrix. This drug loading method not only improves the drug loading capacity but also ensures the stability of the drug and realizes the controlled release of the drug.
Controlling Drug Release
DMNs can achieve programmed drug delivery through the collaborative innovation of matrix materials and structural design. The physicochemical properties of different matrix materials directly affect the kinetics of drug release. DMNs made of hydrophilic materials such as HA and gelatin can rapidly dissolve and release drugs after contact with skin interstitial fluid, meeting the needs of diseases for rapid drug onset.30 In contrast, biodegradable polymers are barely soluble in the interstitial fluid of the skin and instead degrade slowly in the skin, and the rate of drug release from MNs preparations made from this matrix is largely dependent on the degradation of the polymers.31 Therefore, DMNs derived from biodegradable polymers can achieve long-term drug release and provide a guarantee for maintaining stable drug effect. In addition, through the optimization of multi-layer structure design, DMNs can realize the spatiotemporal regulation of drug release and effectively meet the diverse drug delivery needs in the treatment of complex diseases. Kim et al developed multilayered DMNs for delivery of hepatitis B vaccines. With the unique layered design, the rapid and sustained release of vaccine is achieved, and a single dose of vaccine can stimulate efficient and durable immune response.32 Yu et al designed a dual-layer DMNs system to encapsulate the immunosuppressive agent tacrolimus (TAC) in the middle layer of microneedles, so that it could be targeted and retained in the epidermis to effectively inhibit psoriasis plaques. The non-steroidal anti-inflammatory drug diclofenac sodium (DIC) was loaded on the tip layer of the microneedles, penetrating the dermis and penetrating the joint cavity to relieve arthritis symptoms.33 This multi-layer structure design realizes the differential release of drugs in different layers of the skin to meet the therapeutic needs.
Improved Targeting
During the treatment of RA, achieving the enrichment of drugs in inflamed joints is the key to improving the therapeutic effect and reducing systemic adverse reactions. The traditional drug administration method is difficult to ensure that the drug effectively penetrates the complex biological barrier and maintains a sufficient concentration at the lesion site, resulting in limited therapeutic effects. Although DMNs do not have active targeting capabilities, their physical targeting characteristics can deliver drugs to inflamed joints, increase local drug concentrations, and reduce systemic exposure and side effects. Wang et al studied the pharmacokinetics of brucine (Bru) in a rat model of RA. The blood and joint cavity samples of rats after Bru-DMNs administration were continuously sampled by microdialysis-based method combined with ultra-performance liquid chromatography-tandem mass spectrometry, and the concentration-time curves of brucine in these two sites were quantitatively analyzed. The results showed that Bru had higher drug concentration and longer retention time in the joint cavity after microneedle administration compared with blood.34 In addition, when DMNs are combined with delivery systems with active targeting, such as nano formulations with ligands, bionic nano formulations, and stimulation-responsive delivery systems, it can achieve both physical and active dual targeting, enhancing therapeutic efficacy and reducing side effects. These will be discussed later.
The Preparation Process and Matrix Material of DMNs
The Preparation Process of DMNs
The preparation processes of DMNs mainly include micro molding method, photopolymerization method, droplet air blowing method, stretching lithography method and 3D printing method.
In the micro molding method, the water-soluble polymer solution is poured into the mold, and then the needle cavities are filled by centrifugation or vacuum treatment. After drying and demolding, DMNs are obtained. Monkare et al used a micro molding method to prepare DMNs loaded with monoclonal IgG using HA as a matrix material and successfully achieved rapid and non-invasive subcutaneous protein delivery.35
Photopolymerization method is performed by pouring the polymer solution into a mold and initiating the polymerization process by UV light irradiation at room temperature, thereby transforming the liquid polymer into a solid state. The preparation of microneedle by photopolymerization is fast and does not require an additional drying process, but the activity and stability of the drug may be affected by external irradiation. Yu et al prepared glucose-responsive insulin microneedle patches by in situ photopolymerization at a low temperature of 4 °C using a glucose-responsive polymer loaded with insulin as a matrix.36
In the droplet air blowing method, the drug-containing polymer solution is dispersed on a plate to prepare the basic structure. The upper plate is in contact with the droplets distributed on the lower plate, and the length of the microneedle is controlled by vertical stretching at a specific speed. The elongated droplets solidified to form microneedle structure by symmetrical blowing at room temperature. The two plates are separated to form an array of DMNs on the upper and lower plates, respectively. Park et al used the droplet air blowing method to prepare a DMN patch loaded with antigen house dust mite (HDM) for transdermal immunotherapy (TDIT). This TDIT method was proved to be more effective in HDM-induced asthma mouse model.37
Stretching lithography is an innovative process to directly produce DMNs from a solid surface by stretching thermosetting polymers without the need for a mold and light irradiation. The method relies on the glass transition temperature of the polymer to produce a 3D microneedle structure through tensile deformation. The length of microneedles prepared by this method can be changed while maintaining drug activity and stability. However, this method is limited in that it relies on the glass transition temperature, limiting the types of polymer materials that can be used.38 Lee et al used stretching lithography to prepare maltose DMNs and successfully delivered two hydrophilic substances, ascorbic acid-2-glucoside and nicotinamide, to achieve transdermal delivery to inhibit cutaneous hypermelanosis.39
3D printing is an innovative technique for building three-dimensional entities that uses computer-aided design software to generate digital models and convert them into layer-by-layer physical models.40 Liu et al used 3D printing to prepare eutectic gel-soluble microneedle patches loaded with chitosan nanoparticles for diabetic wound management.41 Table 1 summarizes the advantages and limitations of different preparation methods for DMNs.
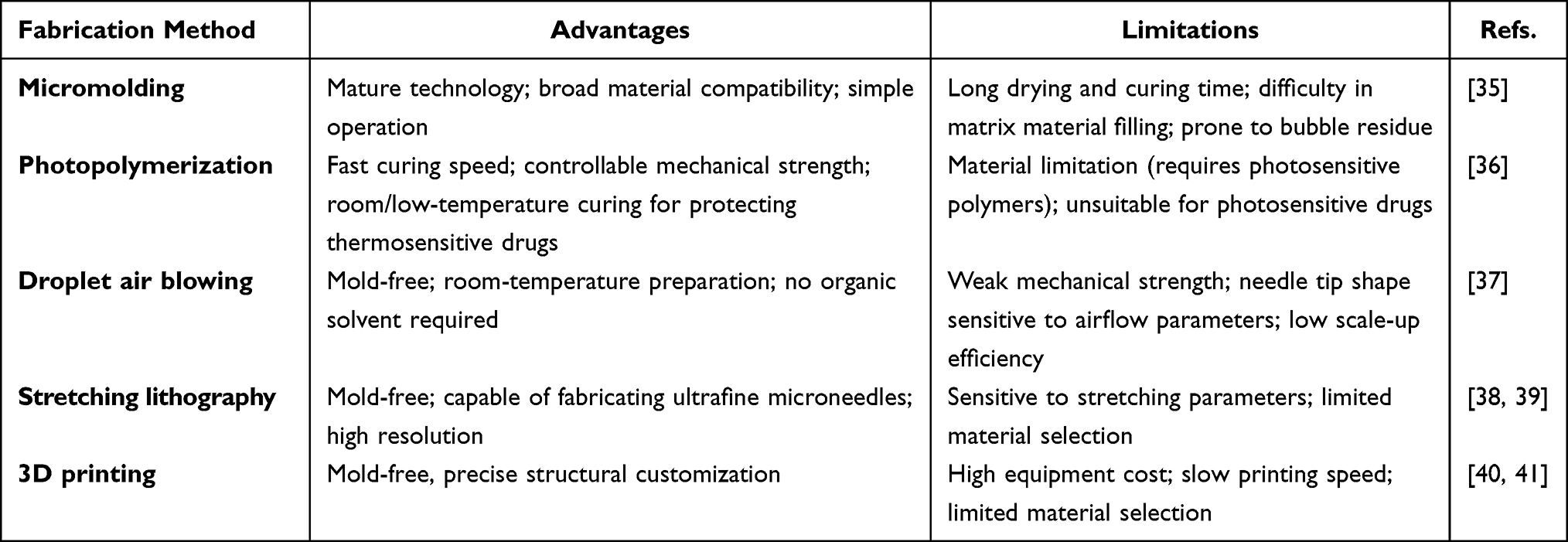 |
Table 1 Advantages and Limitations of Different Fabrication Methods for DMNs |
In current research, the preparation methods of DMNs for RA treatment include micromolding and photopolymerization. Amodwala et al used the micromolding method to prepare meloxicam dissolving microneedle patches for the treatment of RA.42 Zhao et al used the micromolding method to prepare methotrexate dissolving microneedle patches for RA treatment.30 Cao et al used UV curing technology to construct a DMNs delivery system of etanercept using HA modified with methacrylic anhydride as raw material for RA treatment.43 The droplet air blowing method, stretch lithography and 3D printing method have not been reported in the field of RA research at present. The reason may be that the microneedles prepared by droplet air blowing method have weak mechanical strength and are difficult to meet the needs of RA treatment. Stretching lithography is limited by the polymer glass transformation temperature, and it is not suitable for the common substrates of RA such as HA and CS. Due to the high cost of 3D printing, the development of basic research in the laboratory is limited.
The Matrix Material of DMNs
As an emerging drug delivery technology in the field of RA treatment, the realization of DMNs performance is highly dependent on the selection and design of matrix materials. The physicochemical properties of matrix materials, such as molecular structure, hydrophilicity and hydrophobicity, mechanical strength, and degradation rate, fundamentally determine the mechanical properties, drug loading capacity, biocompatibility, and in vivo degradation kinetics of DMNs, thereby affecting the efficiency of drug delivery and treatment safety. At present, the preparation materials of DMNs are mainly divided into two systems: natural polymer materials and synthetic polymer materials. There are differences between the two systems in molecular composition, physicochemical properties and applications. These materials can achieve the controlled release of drugs through dissolution or degradation mechanism, while avoiding the generation of residues in the body, providing key technical support for the targeted therapy of RA. In-depth exploration of the properties of different materials and their applications in DMNs is of great significance for optimizing the performance of microneedles and promoting clinical translation.
Natural Polymer Material
Natural polymer materials have shown advantages in the preparation of DMNs due to their good biocompatibility, degradability and unique biological activity. These materials are derived from organisms and have a high affinity with human tissues. They can be metabolized in vivo through enzymatic hydrolysis or hydrolysis, which reduces the risk of immune rejection and provides a safe carrier for drug delivery.
Hyaluronic Acid
Hyaluronic acid (HA), a glycosaminoglycan, consists of repeating disaccharide units formed by N-acetyl-D-glucosamine and D-glucuronic acid alternately linked via β-(1→4) and β-(1→3) glycosidic bonds.44 As a key extracellular matrix constituent, hyaluronic acid (HA) is highly concentrated in human skin, representing over 50% of the body’s total HA content.45 Its unique viscoelasticity, non-immunogenicity, and good biocompatibility and degradability make it widely used in dermatology, ophthalmology, orthopedics, and other fields.46 In DMN preparation, HA similarly showed excellent properties.26 Studies have shown that dissolving microneedle patches loaded with methotrexate (MTX) based on HA matrix have shown good application potential in the treatment of psoriasis. This microneedle patches have sufficient mechanical strength to successfully penetrate the imiquimod (IMQ)-induced thickening of the epidermis in mice, deliver the drug precisely to the lesion site, effectively suppress the inflammatory response, and reduce the symptoms of skin inflammation in mice.47 Chemical modification is an effective method to improve the processing performance of HA. The introduction of acrylate groups into the HA molecular chain enables it to have photocuring ability and simultaneously retains the inherent water solubility and biodegradability advantages of HA. Cao et al used acrylate-modified HA as the matrix and UV curing technology to prepare DMNs for the delivery of etanercept.43
Chitosan
Chitosan (CH), an N-deacetylation product derived from chitin, is formed from the polymerization of N-acetylglucosamine and D-glucosamine monomers.48 The presence of amino, acetyl amino, and hydroxyl groups in its molecular structure endows CH with a rich chemical activity, making it easy to be functionalized by modification, activation, and coupling.49 In addition, chitosan has the characteristics of non-toxicity, good biocompatibility, biodegradability, and immune stimulation activity, which make it one of the ideal choices for DMNs. However, the mechanical properties of CH are not high, and support arrays such as polylactic acid (PLA), polyvinylpyrrolidone (PVP) are usually required to enhance their mechanical strength.50 Chen et al prepared an antigen delivery microneedle system, using the structure of chitosan microneedle loaded with antigen and PVA/PVP support array. The results showed that rats immunized with low-dose microneedles maintained sustained high antibody levels for 18 weeks compared with rats immunized with high-dose microneedles, which not only achieved painless, accurate and reliable antigen delivery, but also improved vaccine efficacy and reduced antigen consumption.51
Chondroitin Sulfate
Chondroitin sulfate (CS), a glycosaminoglycan formed from β-1,4-linked D-glucuronic acid and N-acetyl galactosamine units, is a water-soluble, biodegradable natural biomacromolecule. Ubiquitous in mammalian connective tissues, it predominates within extracellular matrices—particularly in cartilage, skin, blood vessels, ligaments, and tendons—across structurally distinct variants.52 CS exhibits multiple bioactive properties, such as anti-inflammatory, antioxidant, anti-tumor, and anti-angiogenesis.53 In DMNs research, CS also shows unique advantages. Bui et al developed chondroitin sulfate C (CSC)-based DMNs for delivery of human adipose stem cell-derived extracellular vesicles (hASC-EV). They were found that the microneedles (EV@cMN) could deliver hASC-EV to inflammatory joints, effectively inhibit the polarization of M1 macrophages, reduce the release of pro-inflammatory cytokines TNF-α, IL-6 and IL-17, promote the expression of anti-inflammatory cytokine IL-10, and inhibit the migration of activated fibroblast-like synoviocytes (aFLS). In addition, EV@cMN could also promote the chondrogenic differentiation of bone marrow mesenchymal stem cells (BMSC) to achieve the repair of damaged cartilage. The synergistic inhibitory effect of CSC on the key pathological processes of RA was due to the organic combination of the anti-inflammatory properties of CSC and the immunomodulatory and regenerative functions of hASC-EV.54
Silk Protein
Silk protein is a natural polymer protein with a β-sheet structure, which gives it good mechanical properties, flexibility and stability. In vivo, silk protein is easily degraded by different enzymes and converted to amino acids, which are then absorbed by the body. Therefore, silk protein does not cause inflammatory or toxic reactions, which makes it have excellent biocompatibility and biodegradability, and has received extensive attention in the field of biology.55 For DMNs preparation, silk protein aqueous solution was mixed with macromolecular drugs at room temperature without the need for any organic solvent to form a stable microneedle structure.38 However, there are problems such as easy breakage of microneedle and burst release of drug, which often need to be optimized by modification.56 Zhu et al prepared insulin-loaded microneedle patches using silk protein as a matrix. Silk protein and insulin solution were used to prepare the needle tip, and its rapid dissolution property was used to meet the rapid release of insulin. Proline was added to prepare the base, giving it the property of expanding without dissolving and serving as a reservoir for insulin. Insulin in the base is released continuously through the micropores generated by the microneedles to achieve sustained release. Studies have shown that the microneedle patch can not only effectively reduce blood glucose but also show good slow-release effect.57
Chinese Medicine Polysaccharides
Chinese medicine polysaccharides are a class of active polysaccharide compounds extracted from Chinese herbal medicines. Due to their natural biocompatibility, biodegradability and inherent pharmacological activity, it has been gradually used as a matrix material for DMNs. Wang et al prepared dissolving microneedles with uniform structure, sufficient mechanical strength and skin penetration ability using Panax notoginseng polysaccharide (PNPS) as the needle body material. PNPS MNs can load both hydrophilic and hydrophobic drugs, and possess immune activity, achieving transdermal drug delivery and transdermal immune regulation functions.58 Liu et al used fucoidan as a matrix to prepare DMNs, which were loaded with ROS-responsive nanoparticles (FTL@SIN MNs) for the treatment of RA. The results showed that FTL @ SIN MNs could reduce macrophage inflammation, reduce key pro-inflammatory cytokines, and repolarize M1 to M2, thereby improving synovial inflammation and promoting cartilage repair. Traditional Chinese medicine polysaccharides have shown great potential in the field of dissolving microneedle matrix materials, and more exploration and innovative development are still needed in the future.59
Synthetic Polymer Material
Synthetic polymers play an important role in the preparation of DMNs due to their controllable physicochemical properties, good processing properties, and stable mechanical strength. These materials can precisely control the molecular structure and properties through chemical synthesis to meet the needs of different drug delivery. However, some materials have in vivo metabolism problems, which need to be carefully selected and optimized.
Polyvinylpyrrolidone
Polyvinylpyrrolidone (PVP) is a water-soluble polymer formed by the polymerization of N-vinylpyrrolidone. Its pharmaceutical grade is often expressed by the K value for viscosity and molecular weight.60 Polyvinylpyrrolidone (PVP) demonstrates exceptional mechanical strength and biocompatibility. Its ambient-temperature, organic solvent-free processing renders it ideal for encapsulating heat-sensitive therapeutics such as proteins and antigens.60,61 However, the in vivo metabolic characteristics of PVP limit its application. Studies indicate that renal clearance effectively eliminates PVP with molecular weights below 25 kDa—approximating the glomerular filtration threshold in rat kidneys. With the increase of the molecular weight of PVP, its elimination rate declines, leading to progressive accumulation within the reticuloendothelial system (RES). When the injection molecular weight is greater than 100 kDa, it will cause diseases.62 Therefore, when preparing DMNs using PVP as the matrix, it is necessary to comprehensively consider the drug characteristics and therapeutic requirements and reasonably select the molecular weight or add excipients to optimize the performance.
Polyvinyl Alcohol
Polyvinyl alcohol (PVA) is a water-soluble synthetic polymer with good biocompatibility, safety, water absorption, and thermal stability.63 Similar to PVP, the in vivo metabolism of PVA is closely related to its molecular weight. Low-molecular-weight PVA is eliminated by renal metabolism, whereas high-molecular-weight PVA may accumulate in the liver and spleen.62 To optimize performance, PVA is often used in combination with other polymers. Zhang et al prepared DMNs loaded with FITC-insulin using PVA and sucrose as substrates. These microneedles had a uniform appearance and sufficient mechanical strength. They could rapidly release insulin within 2 minutes after being inserted into the skin and effectively deliver it to the systemic circulation. Its hypoglycemic effect is comparable to that of subcutaneous injection.64
Carboxymethyl Cellulose
Carboxymethyl cellulose (CMC), a cellulose derivative, is an anionic, water-soluble biopolymer commonly used in drug delivery and biologic research because of its hydrophilicity, bioadhesive properties, pH sensitivity, lack of cytotoxicity, and good film-forming properties.65 In DMNs, CMC can be used either as a matrix material alone or in combination with other materials for the delivery of vaccines, hormones, or other drugs.66 Kim et al developed a DMNs system with a dual-release mode for hepatitis B vaccine delivery. The system consists of three parts: a polylactic acid (PLA) tip for slow release of hepatitis B vaccine (>55 days), a CMC coating for rapid release (20 min), and a soluble substrate composed of PVA/PVP to ensure rapid dissolution of the microneedle after insertion into the skin for drug delivery. The immunological efficacy of the DMN system was due to the rapid release of CMC microneedle to mimic the primary immunization, while the continuous release of PLA microneedle tips to mimic the booster immunization. Thus, a highly efficient and durable immune response was achieved through a single vaccination.32
Polylactic Acid (PLA)
Polylactic acid (PLA) is an aliphatic polyester synthesized from lactic acid monomer by polycondensation reaction. According to the polymerization method, PLA can be divided into poly-L-lactic acid (PLLA), poly-D-lactic acid (PDLA) and racemic poly-DL-lactic acid (PDLLA). PLA has good biocompatibility, biodegradability and excellent mechanical strength. Its stereochemical structure determines the key properties such as crystallinity and mechanical properties. PLA has defects such as brittleness and poor thermal stability, but it can be modified by plasticizing, blending, and adding fillers.67 As a matrix material for DMNs, the prominent advantage of PLA is its long-acting drug release ability, which is suitable for long-term maintenance treatment of RA. Kang et al used PLA as the matrix material to prepare microneedles by adding glucose, sucrose and trehalose. These microneedles had both the high mechanical strength of solid microneedle and the high drug release characteristics of dissolving microneedle, and the loaded hydrophobic drug retinol and hydrophilic drug vitamin E could be rapidly released within 30 minutes.68
Polylactic Acid-Glycolic Acid Copolymer (PLGA)
Polylactic acid-glycolic acid copolymer (PLGA) is a polymer composed of lactic acid (LA) and glycolic acid (GA) linked by ester bonds. It is one of the most widely used biodegradable synthetic polyesters. The physical properties of PLGA, such as solubility, mechanical strength and degradation rate, can be regulated by adjusting the ratio of the two monomers. The higher the proportion of LA, the stronger the hydrophobicity of the material and the slower the degradation rate, while the higher the proportion of GA, the faster the degradation rate. In addition, PLGA is a polymer approved by the US FDA, and its degradation mechanism in vivo is the hydrolysis reaction of ester bonds, and the final products are lactic acid and glycolic acid, with high biological safety.69 Lee et al prepared novel multi-layered dissolving microneedles using HA and PLGA as matrix materials. These microneedles had sufficient mechanical strength (0.69 N) to penetrate the porcine skin in vitro, and the model drug rhodamine was released continuously for nearly 4 weeks (90% release in 26 days). It was better than that of the traditional HA dissolving microneedle (90% release in 160 min).70
Polycaprolactone (PCL)
Polycaprolactone (PCL) is a synthetic polyester formed by ring-opening polymerization of ε-caprolactone monomer. PCL has good biocompatibility and shows low toxicity and inflammation in vitro and in vivo. PCL is degraded at a slower rate, mainly by non-enzymatic hydrolysis, and homopolymer PCL has a degradation cycle of 2–4 years. The rate of hydrolysis can be altered by copolymerization with other lactones or glycol-ides/lactides. In addition, PCL has excellent rheological properties and viscoelasticity, but the mechanical strength of pure PCL is insufficient, and it can copolymerize with PLA and PGA to improve its mechanical properties.71 Eum et al used a hot melting method to encapsulate capsaicin in PCL at 65 ° C, and a mixture of 10% (w/v) polyvinyl alcohol (PVA) and 20% (w/v) polyvinylpyrrolidone (PVP) was used as the base polymer. Separable polycaprolactone (PCL) DMNs (SPCL-DMNs) with height of 498.3±5.8 μm and encapsulated 86.66±1.13 μg capsaicin were successfully prepared. The SPCL-DMNs had sufficient mechanical strength to penetrate the porcine skin, and the base polymer could be easily peeled after insertion. The PCL was partially implanted into the skin and the drug was released continuously through biodegradation.72
As the drug delivery carrier of targeted therapy for RA, the selection and design of matrix materials of DMNs are the key factors determining the delivery efficiency, treatment safety and clinical translation potential. Natural polymer materials have the advantages of excellent biocompatibility and natural activity. Glycosaminoglycans such as HA and CS are derived from human tissues, which have non-immunogenicity and fast dissolution rate, and are suitable for rapid anti-inflammatory and local tissue repair in the acute stage of RA. Chitosan and silk protein can achieve functional expansion through structural modification to meet the needs of RA treatment. Synthetic polymer materials are characterized by highly controllable physicochemical properties. Among them, water-soluble polymers such as PVP, PVA, and CMC, which dissolve rapidly and are suitable for encapsulating heat-sensitive drugs, serve as the core matrix for fast-release DMNs. But their potential risk of long-term accumulation in vivo requires careful consideration through molecular weight control. In contrast, the degradation rate of PLGA, PLA, PCL and other polyester materials can be customized from days to months by adjusting the monomer ratio or molecular weight, which perfectly matches the long-term maintenance treatment needs in the chronic phase of RA. The characteristics of the two types of materials are complementary, providing a rich matrix material for the functional customization of DMNs. Table 2 summarizes the matrix materials for the preparation of DMNs in terms of molecular structure characteristics, biocompatibility, biodegradability, and application in RA.
 |
Table 2 Matrix Material Properties of DMNs |
Application of DMNs in the Treatment of RA
The application of DMNs in RA treatment will be introduced in this section. All the information about direct drug delivery by DMNs is summarized in Table 3. And the information on the delivery of drugs by DMNs in combination with other technologies is summarized in Table 4.
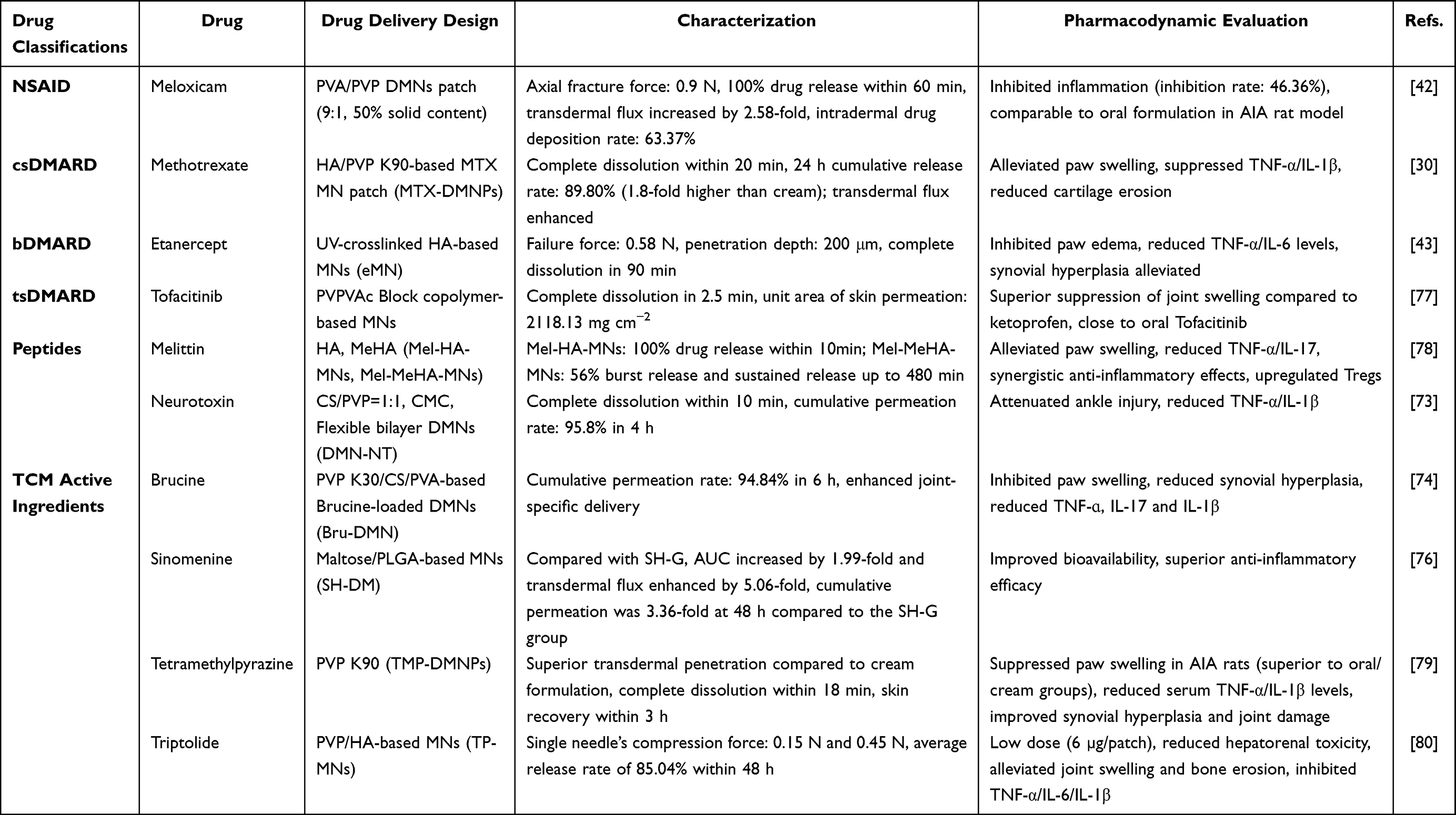 |
Table 3 DMNs Directly Deliver Drugs for the Treatment of RA |
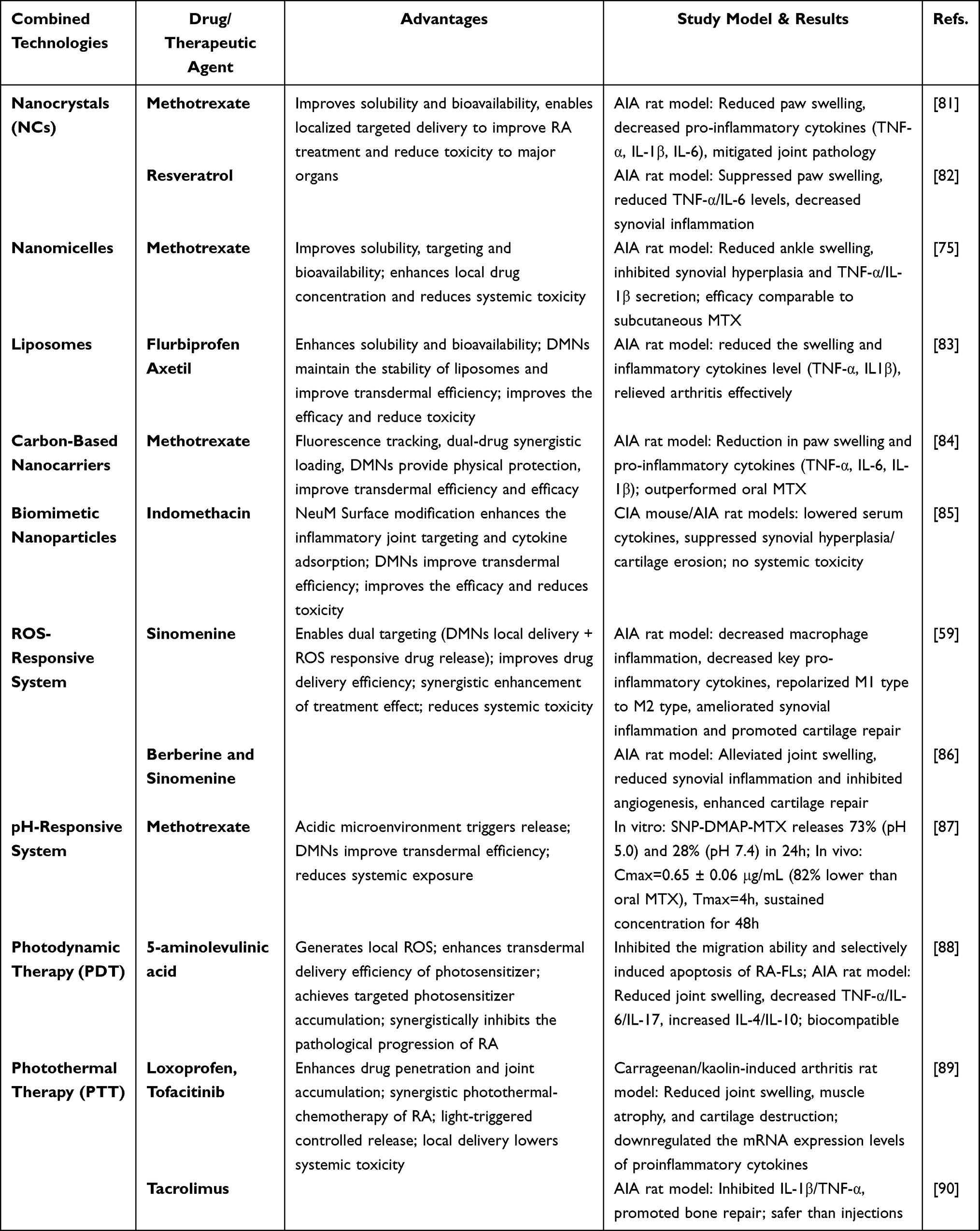 |
Table 4 DMNs Combine with Other Technologies to Deliver Drugs for the Treatment of RA |
DMNs Deliver Drugs Directly to Treat RA
In the clinical treatment of RA, effective drug delivery and precise intervention are the key to improve the prognosis of patients. DMNs provides a new delivery strategy for various RA drugs with its unique advantages to improve the efficacy and safety of drug therapy.
NSAIDs
NSAIDs are widely used in the treatment of RA because of their excellent analgesic and anti-inflammatory effects.91 NSAIDs commonly used in clinical practice, such as ibuprofen, diclofenac sodium, meloxicam, and celecoxib, exert their therapeutic effects mainly by inhibiting the activity of cyclooxygenase (COX) and blocking the synthesis of key inflammatory mediators such as prostaglandins.92 However, frequent oral administration is prone to cause serious gastrointestinal adverse reactions, including mucosal damage, ulcers, bleeding, and even threatening life.93 In order to break through this limitation, DMN technology has become a research hotspot in the delivery of NSAIDs. Amodwala et al successfully developed a microneedle patch loaded with meloxicam using PVA and PVP as substrates and optimizing the formulation by mixing D-optimal design. The results showed that when the PVA/PVP ratio was 9:1 and the solid content was 50%, the axial fracture force of the microneedle reached 0.9 N, which met the skin penetration requirements. In vitro release assays showed nearly complete drug release from the patch within 60 min. In vitro rat skin experiments showed that the transdermal flux of the solution was 2.58 times higher than that of the normal solution, and the drug deposition rate in the skin was 63.37%. Further in vivo pharmacodynamic studies showed that the anti-inflammatory effect of the microneedle patch was comparable to that of the commercial oral formulation, and histopathological analysis confirmed its good safety.42 To address the water-insoluble drug delivery challenge, Li et al developed dissolving microneedles that encapsules a composite microemulsion of celecoxib and α-linolenic acid (Cel-MEs@MNs). The experimental results showed that Cel-MEs@MNs could reduce serum inflammatory cytokines, reduce inflammatory cell infiltration, and effectively improve cartilage damage in rats, which provides an innovative idea for the delivery of hydrophobic NSAIDs.94
DMARDs
As the core drugs in the treatment of RA, DMARDs play a key role in disease remission by modulating the immune response and delaying or preventing joint degeneration.2 DMARDs are divided into conventional synthetic DMARDs (csDMARDs), biological DMARDs (bDMARDs) and targeted synthetic DMARDs (tsDMARDs). csDMARDs are usually used as the primary choice for newly diagnosed RA patients, and bDMARDs or tsDMARDs are recommended when the first-line treatment is ineffective or cannot be tolerated by patients.
csDMARD: Methotrexate
MTX, as the first-line treatment for RA, is often accompanied by severe adverse reactions, such as gastrointestinal irritation, liver and kidney damage, blood toxicity, and cancer risk,95 resulting in reduced patient compliance and limited clinical application. Currently, strategies to ameliorate these adverse effects mainly include dose optimization,96 drug substitution, and combination therapy.97 To improve this situation, researchers are actively exploring new routes of drug administration. Zhao et al used HA and PVP K90 as matrices to prepare dissolving microneedle patch (DMNP) by a two-step micro molding method for transdermal delivery of MTX to improve the therapeutic effect of RA. The patch has a uniform conical array, which can effectively penetrate the rat skin and achieve complete drug release within 20 minutes. In vitro transdermal experiments showed that DMNP increased the cumulative release rate of MTX (89.80%) within 24 hours, which was 1.8 times higher than that of the traditional cream group (49.92%). In the adjuvant arthritis rat model, MTX-DMNP treatment alleviated paw swelling compared with oral administration and cream treatment, inhibited inflammation by down-regulating the levels of TNF-α and IL-1β, and alleviated synovial destruction by reducing cartilage erosion, showing better therapeutic effects than traditional administration.30
bDMARD: Etanercept
Etanercept (EN) is a TNF-α inhibitor, which is fused by recombinant human TNF receptor p75 monomer and the Fc domain of human IgG1. It can effectively delay the progression of joint and improve joint function by blocking the TNF-α signaling pathway. However, subcutaneous administration is associated with pain, risk of infection, and poor patient adherence.98 To address these limitations, Cao et al used UV-curing technology to construct an EN microneedle system using HA modified with methacrylic anhydride as material. The microneedle array had a single needle breaking force of 0.58 N, penetrated the mouse skin to a depth of about 200 μm, and completely dissolved within 90 minutes. In the adjuvant induced arthritis mouse model, EN delivered by microneedle was as effective as subcutaneous injection in inhibiting foot swelling, reducing serum TNF-α and IL-6 levels, and reducing synovial hyperplasia and cartilage erosion. Histopathological analysis showed that mice treated with EN microneedles had improvement in joint structural damage and complete recovery at the skin puncture site within 120 minutes. This study demonstrated the feasibility and safety of DMNs for delivering macromolecular protein drugs.43
tsDMARD: Tofacitinib
As a JAK inhibitor, tofacitinib has shown efficacy in the treatment of autoimmune diseases. Currently, the commercial dosage forms of tofacitinib are limited to oral tablets and solutions, with a single route of administration. Jiang et al prepared DMNs loading tofacitinib citrate using block copolymer as a matrix and evaluated its efficacy in the treatment of RA. In vivo dissolution experiments showed that the microneedles could be completely dissolved within 2.5 minutes. In the treatment of RA rat model, the inhibition effect of tofacitinib on joint swelling was better than that of NSAIDs ketoprofen, which is close to the effect of oral tofacitinib administration. Western blot further confirmed that tofacitinib DMNs reduced the local inflammatory response caused by RA by inhibiting the phosphorylation of JAK-STAT3 pathway, which provided theoretical basis and technical support for the transdermal administration of tofacitinib for the treatment of RA.77
Peptide
Melittin (Mel), as the main bioactive component of bee venom, has immunomodulatory and anti-RA effects. However, the pain caused by intravenous injection of purified melittin, the risk of hemolysis, and the limited clinical application of live bee stings have limited its widespread use.99 Du et al solved the above problems by changing the route of administration and achieved remarkable results. The researchers prepared Mel-loaded microneedle Mel-HA-MN and Mel-MeHA-MN with sustained release using HA and HA modified by methacrylate groups as substrates, respectively. Both microneedle types have good mechanical strength for transdermal delivery of melittin. In vitro drug release results showed that Mel-HA-MN achieved drug release within 10 minutes, while Mel-MeHA-MN released 56% within 10 minutes and sustained drug release until 480 minutes. In adjuvant-induced arthritis rat and mouse models, microneedles delivery of Mel inhibited foot swelling, and the effect was comparable to that of subcutaneous injection, and the sustained release Mel-MeHA-MN was more effective. The study also compared the levels of cytokines in the joints and serum and the proportion of regulatory T cells (Tregs) in the spleen. The results showed that both Mel-HA-MN and Mel-MeHA-MN could reduce the levels of TNF-α and IL-17 in serum and joints, and up-regulate the proportion of Treg in spleen. The effect of slow-release MNs was better than that of fast-release MNs. Microneedle treatment also alleviated synovial inflammatory cell infiltration and cartilage damage without causing hematologic toxicity.78
Neurotoxin (NT), the main peptide component of cobra venom (NNAV), has been used in analgesia and arthritis treatment for a long time, but the problems of poor patient compliance and side effects need to be solved urgently. Yao et al prepared flexible bilayer dissolving microneedles loaded with NT (DMN-NT) by a two-step centrifugation method for the treatment of RA. The results showed that DMNS-NT could deliver NT through the skin, with complete dissolution within 10 minutes and a cumulative permeability of 95.8% within 4 hours. The stratum corneum could recover spontaneously after 6 hours. After 15 days of administration, there was no obvious adverse reaction in the skin, showing good biocompatibility and safety. Pharmacodynamic studies showed that DMN-NT reduced toe swelling and ankle joint injury in RA rats, and reduced serum TNF-α and IL-1β levels. DMNs technology provides a safe and effective strategy for the treatment of RA with peptide drugs.73
Active Ingredients of Traditional Chinese Medicine (TCM)
TCM and its active ingredients have attracted much attention in the treatment of RA due to their multi-target mechanism of action, safety and potential to reduce the side effects. The application of DMNs technology can effectively overcome the problems of low bioavailability and poor targeting of TCM components and improve its therapeutic effect.
Brucine (Bru), the main active alkaloid of Strychnos nux-vomica L., has a variety of pharmacological effects such as anti-inflammatory, analgesic, immunosuppressive and anti-tumor effects.100 However, its narrow therapeutic window, oral neurotoxicity, painful swelling by injection, and easy to cause secondary inflammation and joint dysfunction have limited its clinical application.101 Song et al successfully prepared brucine dissolving microneedles (Bru-DMNs), which met the needs of RA treatment in terms of mechanical strength, biocompatibility, drug release, and safety. Microneedle administration could improve the skin permeability of Bru, and the cumulative drug permeability reached 94.84% after 6 hours of administration. In vivo studies showed that Bru-DMNs suppressed toe swelling, reduced synovial hyperplasia caused by articular cartilage erosion, and reduced swelling of the thymus and spleen in RA rats.74 Pharmacokinetic-pharmacodynamic (PK-PD) analysis showed that Bru delivered by DMNs could enhance joint specific distribution and prolong retention time compared with systemic administration, and its anti-inflammatory effect was closely related to the regulation of key inflammatory cytokines such as TNF-α, IL-1β and IL-17. Studies have also shown an indirect correlation between drug effects and local concentrations, suggesting synergism of multiple targets.34
Sinomenine (SIN) is an alkaloid extracted from Sinomenium acutum, a traditional Chinese medicine. Its hydrochloride is commonly used in clinical practice. It has anti-inflammatory and analgesic activities and has been used in the clinical treatment of RA. Currently, the common formulations of sinomenine hydrochloride (SH) on the market include tablets and injections, which have achieved good results in clinical practice.102 However, SH is limited by gastrointestinal adverse reactions, short biological half-life and unstable physicochemical properties.103 To solve these problems, Wu et al prepared SH dissolving microneedle (SH-DM) using maltose and polylactic acid-glycolic acid as raw materials by casting method, and the SH-DM had intact morphology and good mechanical strength. Compared with the traditional SH gel (SH-G), the area under the drug-time curve (AUC) of SH-DM was 1.99 times that of SH-G, and the relative bioavailability value was 199.21%.76 Shu et al fabricated SH-loaded dissolving microneedles (SH-MN) using PVP and CS. Compared to SH-G, the SH-MN formulation demonstrated markedly enhanced transdermal delivery. Permeation studies in vitro revealed cumulative permeation and permeation rates that were 5.31-fold and 5.06-fold greater, respectively. Percutaneous pharmacokinetic analysis further indicated that SH-MN achieved a 1.43-fold higher AUC in skin and a 1.63-fold higher AUC in blood. Collectively, these findings confirm that dissolving microneedles substantially improve both the bioavailability and permeability of SH, establishing them as an effective transdermal delivery strategy.104
Tetramethylpyrazine (TMP), a bioactive alkaloid derived from Ligusticum sinense, attenuates hypoxia-stimulated proliferation, migration, and inflammatory activity in fibroblast-like synoviocytes by targeting the HIF-1α-circCDC42BPB signaling axis.105 However, the clinical use of oral and injectable drugs is associated with short half-lives, high doses, low bioavailability, and poor patient adherence.106 In view of the problem of TMP, Zhao et al constructed tetramethylpyrazine-loaded dissolving microneedle patches (TMP-DMNP), which has good biocompatibility and safety. In vitro transdermal studies demonstrated enhanced TMP permeation with TMP-DMNP formulation relative to conventional TMP cream. In vivo experiments showed that TMP-DMNP reduced TNF-α and IL-1β levels, ameliorated synovial lesions, and inhibited paw swelling in adjuvant-induced RA rats. More importantly, the therapeutic effect of microneedles was superior to the same dose of TMP oral preparation or ointment.79
Triptolide (TP) is one of the main active components of Tripterygium wilfordii Hook. f. in the treatment of RA, and it is also the main toxic component, with severe liver, kidney and reproductive system toxicity, which limits its clinical application.107 Li et al used PVP and HA as matrix materials to construct a DMNs system for TP delivery. The microneedle system can rapidly release drugs after penetrating the skin barrier, reduce joint swelling and bone erosion, and reduce the expression of pro-inflammatory cytokines TNF-α, IL-6 and IL-1β in the rat model of adjuvant arthritis. Despite a low TP loading of only ~6 µg per patch in TP-MNs, this amount effectively modulated inflammation in AIA rat models. In addition, the liver and kidney toxicity of TP were reduced due to the dose reduction, and the therapeutic goal of attenuated toxicity and enhanced efficacy was achieved.80
DMNs Combined with Nano-Delivery System for the Treatment of RA
In the treatment of RA, DMNs have become a promising drug delivery method due to its advantages of painless transdermal administration, reducing the risk of infection, avoiding gastrointestinal irritation and first-pass effects in the liver, and improving drug bioavailability. However, it has inherent limitations such as rapid drug clearance, lack of active targeting ability, and low delivery efficiency of poorly soluble drugs. The development of nanotechnology provides a new direction to break through these bottlenecks, and its advantages in improving the solubility, stability, targeting and controlled release performance of drugs,27 promote the combination strategy of DMNs and nano-preparations to become a research hotspot for RA treatment. This synergistic mode integrates the characteristics of the two technologies to achieve complementary advantages, and opens a new path for the precision treatment of RA.
DMNs Combined with Nanocrystals
Nanocrystals (NC), as a special type of nano formulation, are nanoscale crystalline or amorphous particles composed of drug molecules, with particle size typically ranging from a few nanometers to 1000 nm.108 Unlike carrier-based nano formulations such as liposomes and nanoparticles, NC contains no exogenous carrier material, thereby increasing drug loading and reducing potential safety risks.109 Based on the Noyes-Whitney and Ostwald-Freundlich equations, NC improves drug solubility, dissolution rate, and bioavailability by reducing drug size and substantially increasing the specific surface area.110 However, the high surface energy of nanocrystals leads to aggregation tendency and the risk of crystal transformation, which limits their application. The combined application of DMNs and NC technology provides an innovative solution for the treatment of RA. NC can improve the solubility and dissolution rate of poorly soluble drugs by reducing drug particle size and improve the absorption performance of drugs. DMNs delivers NC directly to the inflammatory joints with the characteristics of minimally invasive transdermal drug delivery, avoiding drug dilution and nonspecific distribution caused by systemic circulation. At the same time, its matrix provides a stable physical support and protective environment for NC, which effectively improves the defects of easy aggregation and poor stability of NC. The synergy of the two not only achieves efficient drug enrichment in the lesion site, enhances the accuracy of treatment, but also reduces systemic adverse reactions such as gastrointestinal irritation, liver and kidney toxicity caused by traditional drug administration methods. The minimally invasive and painless drug administration mode meets the needs of patients’ compliance in the long-term treatment of RA, providing an innovative solution to overcome the problem of RA treatment.
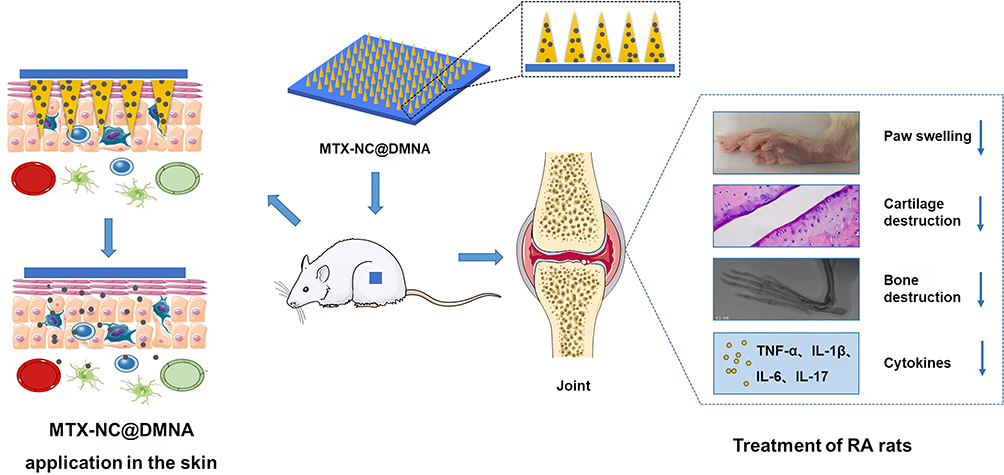 |
Figure 3 Graphical Abstract of methotrexate nanocrystals-loaded microneedles array for targeted rheumatoid arthritis therapy.81 Downward arrows (↓): Represent the reduction or inhibition of the corresponding indicators in rheumatoid arthritis (RA) treatment, including paw swelling, cartilage destruction, bone destruction, and pro-inflammatory cytokines. Copyright 2022, International Journal of Nanomedicine. |
As shown in Figure 3, Wei et al synthesized carrier/surfactant-free methotrexate nanocrystals (MTX-NC, 148.1±10.1 nm) via anti-solvent precipitation to overcome bioavailability limitations and poor drug loading problems, and then and then loaded MTX-NC into DMN to make MTX-NC@DMNA. The system had sufficient mechanical strength to penetrate the skin and deliver the drug successfully. MTX-NC@DMNA reduced foot swelling in RA rats and regulated the balance between the pro-inflammatory cytokines TNF-α, IL-1β, IL-6, IL-17 and the anti-inflammatory cytokines IL-4, IL-10. It also reduced the pathological damage of synovium, joints and cartilage, and reduce the risk of toxicity to major organs such as heart and liver, and the efficacy was better than that of oral and cream types.81
Resveratrol (Res) is a polyphenolic compound with various biological activities such as anti-inflammatory, anti-oxidation and immune regulation. Studies have found that Res can inhibit the production and release of pro-inflammatory cytokines and matrix metal enzymes by inhibiting the nuclear factor-κB (NF-κB) signaling pathway, and alleviate RA synovial inflammation, proliferation and cartilage destruction. It has potential application value in the treatment of RA.111,112 In response to the low solubility of Res and the side effects of oral injection, Diao et al constructed dissolving microneedles (Res-NC MNs) loaded with Res nanocrystals (Res-NC). Res-NC exhibited a uniform particle size of 130 nm with enhanced stability and aqueous solubility, while demonstrating negligible cytotoxicity. Res-NC-MN maintained good morphology and sufficient mechanical strength for transdermal delivery. In the AIA rat model, Res-NC MNs inhibited foot joint swelling, reduced the levels of pro-inflammatory cytokines TNF-α and IL-6, alleviated synovial inflammatory cell infiltration and cartilage damage, and the efficacy was better than that of the oral Res group. In addition, this system was safe and does not cause skin irritation and major organ toxicity, providing a new strategy for the efficient and non-invasive treatment of RA.82
DMNs Combined with Nanomicelle
Nanomicelle is a nano-scale carrier formed by the self-assembly of amphiphilic molecules such as polyethylene glycol (PEG) and polylactic acid-co-glycolic acid (PLGA), which has shown advantages in the field of drug delivery due to its unique core-shell structure. Its core is composed of hydrophobic groups, which can efficiently carry water-insoluble drugs, addressing the issue of hydrophobic anti-inflammatory drug dissolution in RA therapy. The outer hydrophilic shell can prolong the circulation time in the body, reduce the clearance of the reticuloendothelial system, and improve the stability of the drug. At the same time, the biocompatible material matrix of nanomicelles ensures in vivo safety. And the surface of nanomicelles can be modified with ligands and stimulus-response groups to achieve active targeting or controlled release functions, meeting the demand for precise drug delivery in RA treatment.113 However, nanomicelles are easily disturbed by the physiological environment in the systemic circulation, resulting in premature drug release and non-specific distribution problems, which lead to insufficient drug enrichment efficiency in lesions. The combination of DMNs with nano-micelles is one of the options to address the challenges of RA treatment. DMNs can penetrate the skin barrier and deliver the micelles directly to the inflammatory joints through minimally invasive treatment, which effectively avoids the destruction of the structure of the micelles by the systemic circulation process and avoids the premature release of drugs. At the same time, the distribution of nanomicelles in non-target tissues was reduced, so that the drug could form high concentration aggregation at the joint lesions. This synergistic strategy not only gives full play to the advantages of nanomicelles in improving drug solubility, improving stability and achieving targeted controlled release, but also effectively makes up for the defects of nanomicelles in complex in vivo environment by virtue of the physical targeting characteristics of DMNs. By reducing the systemic exposure of drugs, the risk of adverse reactions such as liver and kidney toxicity and gastrointestinal stimulation is reduced, which provides an innovative solution for the accurate and safe treatment of RA.
Liu et al developed dissolving microneedle patches (MTX@PMs MNs) based on in situ generation of nanomicelles using the amphiphilic copolymer mPEG-PLA and HA as raw materials by micromolding. After skin puncture, the nanoparticles rapidly dissolved and self-assembled to form targeted nanomicelle with a particle size of about 38 nm. Among them, HA not only enhances the mechanical strength of microneedles, but also actively targets activated macrophages in inflamed joints through CD44 receptor. In an adjuvant-induced RA rat model, MTX@PMs MNs reduced ankle swelling and clinical scores, inhibited synovial hyperplasia and the secretion of proinflammatory cytokines TNF-α and IL-1β, and reduced bone erosion. The efficacy was comparable to that of subcutaneous injection of MTX. In addition, local administration avoids the systemic toxicity of traditional oral or injection, and the analysis of serum, liver and kidney function indexes and organ pathology showed excellent safety.75 However, the skin safety assessment in this study was limited to a short period of time, and long-term adverse reactions such as fibrosis, inflammatory infiltration, and allergy were not observed after repeated administration, which could not provide long-term safety evidence. The long-term safety of DMNs is very important for the realization of clinical translation, which needs further systematic exploration and improvement.
DMNs Combined with Liposomes
As a classical nano-drug delivery carrier, liposomes are closed vesicles with bilayer structure that are spontaneously formed by phospholipids, sterols and other lipid molecules in the aqueous phase. Its unique layered structure enables it to encapsulate both hydrophilic and hydrophobic drugs. The internal aqueous phase can encapsulate water-soluble drugs, while the lipid environment of the bilayer is suitable for encapsulation of lipid-soluble components, which effectively solves the delivery challenge caused by differences in drug solubility. Because the bilayer structure of liposomes is highly similar to that of biofilms, they have excellent biocompatibility and cell affinity, which can improve the bioavailability of drugs. In addition, liposomes protect the encapsulated drug from enzymatic and chemical degradation in vivo, and structural modification of liposomes allows control of drug release behavior.114 However, the stability of liposomes limits their clinical application. During storage and circulation in vivo, liposomes are prone to aggregation, fusion, and drug leakage, affecting therapeutic efficacy and safety.115 The combined application of DMNs and liposomes provides a new solution to solve the above problems. DMNs uses biocompatible polymer as a matrix to stably encapsulate liposomes in the microneedle structure, forming a physical barrier to effectively inhibit the aggregation and leakage of liposomes and improve their stability during storage and drug delivery. At the same time, DMNs can deliver liposomes directly to the inflammatory joints of RA patients with minimally invasive, realizing the physical targeted delivery of drugs, and avoiding the non-specific distribution and premature release of liposomes in the systemic circulation. This synergistic delivery system not only retains the advantages of liposomes as drug carriers, but also overcomes the inherent defects of liposomes through the structural support and targeted delivery of DMNs, providing a safe and efficient new drug delivery scheme for local precision treatment of RA.
Xie et al prepared liposomes loaded with flurbiprofen axetil (FA) by thin-film hydration ultrasound (FA@Lipo), with an encapsulation efficiency of 75% and particle size of 146.4±2.801 nm. FA@Lipo was pH responsive and released drugs faster under acidic conditions. The dissolving microneedle patch (FA@Lipo-DMNs) loaded with FA@Lipo was prepared by mixing it with HA. Its mechanical strength was sufficient to penetrate the stratum corneum of the skin for drug delivery. In vitro experiment indicated that under the acidic conditions (pH=5.0) of the simulated inflammatory site, the drug release rate within 48 hours was 91%, while under the neutral conditions (pH=7.0) of the physiological environment, the drug release rate was only 53%. Animal experiments showed that FA@Lipo-DMNs had the same effect as subcutaneous injection, which could reduce the swelling of the plantar and ankle joints of rats, inhibit the expression of inflammatory cytokines TNF-α and IL-1β, relieve joint inflammation and cartilage damage, and the compliance of patients was better. However, this study did not carry out the in vivo pharmacokinetic study which needs to be further supplemented.83
To overcome the problems of pain, allergic reactions, low oral bioavailability and systemic toxicity in the clinical application of Melittin, Xiong et al developed a soluble microneedle patch loaded with melittin liposomes (Mel-Lip-MN) based on the transdermal delivery technology of microneedle. This system enhanced the stability of Melittin and reduced its hemolytic toxicity through liposome encapsulation. The particle size of Mel-Lip was about 126 nm, and the encapsulation efficiency was more than 80%. In the AIA rat model, Mel-Lip-MN could reduce joint swelling, reduce serum IL-6 and TNF-α levels, improve cartilage damage and bone mineral density, and its high dose group had similar efficacy to methotrexate.116
DMNs Combined with Carbon-Based Nanocarriers
Carbon dots (CDs) are carbon-based nanomaterials with a particle size of less than 10 nm.117 The surface of CDs is characterized by a high concentration of carboxyl, hydroxyl and other functional groups, collectively referred to as the “carbon core” with surface functional groups. They have good biocompatibility, chemical stability, low cytotoxicity, and fluorescence properties, making it suitable for drug delivery and in vivo tracking.118 CDs have been used in the delivery of anti-cancer, anti-inflammatory, antibacterial and other drugs. However, their circulation time in the body is short and they are easily cleared, which shortens the action time of the drug and reduces the therapeutic effect.119 In the treatment of RA, drugs mainly act on inflamed joints. DMNs combined with CDs can achieve local targeted delivery of drugs and avoid premature clearance of drugs in the body circulation.
In the study by Chen et al, glycyrrhizic acid (GA) was modified on carbon dots (CDs) by amide reaction and then MTX was loaded onto the system to create a nano-drug delivery system that exhibited both fluorescent properties and dual anti-inflammatory effects. Then HA was combined with nano-drug delivery system to prepare biodegradable dissolving microneedles for transdermal drug delivery of rheumatoid arthritis. In vitro cell experiments showed that the system could inhibit the secretion of TNF-α, IL-6 and IL-1β induced by lipopolysaccharide (LPS) in RAW264.7 macrophages, and the process of drug delivery could be monitored by fluorescence imaging in real time. In animal experiments, the drug-loaded microneedle showed excellent skin penetration and slow-release properties. In RA rats induced by Freund’s complete adjuvant, the drug-loaded microneedle reduced foot swelling and serum inflammatory cytokines, and the therapeutic effect was better than that of oral MTX and MTX microneedle. This study provides a novel transdermal strategy for RA treatment that combines targeted delivery, synergistic anti-inflammation, and patient compliance.84
DMNs Combined with Cell Membrane Biomimetic Technology for the Treatment of RA
In the clinical treatment of RA, the traditional treatment method not only leads to insufficient local drug concentration and limited efficacy due to the non-specific distribution of drugs, but also may cause systemic toxic and side effects, which brings risks to the health of patients. The nano delivery system can achieve passive targeting by means of the enhanced permeability and retention (EPR) effect, which reduces the systemic toxicity to a certain extent. However, the recognition and clearance effect of the immune system on nanomaterials limits their targeting efficiency and is difficult to meet the requirements of precise treatment for RA.120 In recent years, cell membrane biomimetic technology has made breakthroughs, which opens up a new way for the construction of active targeted drug delivery system. Different cell membranes confer specific biological functions on nano formulations. For example, macrophage membranes possess specific antigens and retain the ability to bind proinflammatory cytokines, allowing active enrichment of drug-loaded nano formulations into inflammatory regions.121 However, biomimetic nano formulations still face the problem of how to cope with the complex physiological environment and penetrate the skin barrier efficiently. DMNs technology provides strong support for solving this problem. DMNs can deliver biomimetic nano formulations to inflamed joints in a minimally invasive manner, reducing the loss and non-specific distribution of drugs in the systemic circulation. The physical penetration characteristics of DMNs and the biological targeting function of bionic technology complement each other, forming a dual strategy of physical penetration and biological targeting. This combination method not only solves the problem that drugs are difficult to penetrate the skin barrier in traditional transdermal drug delivery but also gives the drug delivery system the ability to actively target, which can accurately deliver drugs to the inflamed joints of RA, effectively improve the therapeutic effect of drugs, and reduce systemic toxic side effects. It provides an innovative and promising solution for the treatment of RA.
Neutrophils originate from the bone marrow, circulate in the blood without inflammatory stimuli, and migrate to sites of inflammation in response to IL-8 stimulation. Neutrophils are an important cell population in the synovial fluid of RA patients.122,123 Therefore, the combination of NeuM and nanoparticles can achieve the targeting of RA treatment. Lin et al reported HA microneedle patches loaded with NeuM-coated indomethacin-loaded PLGA nanoparticles (NeuM-Ind@PLGA NPs). This system combines the transdermal advantages of microneedle patch, the targeting function of cell membrane biomimetic technology and the anti-inflammatory effect of non-steroidal anti-inflammatory drugs. The microneedles can painlessly penetrate the corneum of the skin and gradually dissolve to achieve the release of nanoparticles. Coating of neutrophil membrane provides the nanosized NSAIDs with the capability of cytokine binding and inflammatory joint tropism. And PLGA nanoparticles loaded with indomethacin exert local anti-inflammatory effect by inhibiting COX-2 activity. Its efficacy was validated in a collagen-induced arthritis (CIA) mouse model and an adjuvant-induced arthritis (AIA) rat model. The results showed that the NeuM-modified co-delivery system reduced serum inflammatory cytokine levels and inhibited synovial hyperplasia, cartilage erosion and bone destruction compared with oral administration and unmodified nanoparticles. Histological and Micro-CT analysis further confirmed that it could synergistically alleviate joint damage, and no obvious systemic toxicity was observed.85
DMNs Combined with Stimulus-Response Delivery System for the Treatment of RA
DMNs Combined with ROS Response Delivery System
As a complex autoimmune disease, the pathogenesis of RA has not been fully elucidated, but sufficient evidence has shown that oxidative stress plays a key regulatory role in its pathological process.124,125 In the synovial microenvironment of RA patients, the level of reactive oxygen species (ROS) is increased compared with the normal physiological state. Excessive accumulation of ROS can trigger a series of cascade reactions. Oxidative damage can inactivate biological molecules, interfere with the normal physiological function of cells, and trigger the release of pro-inflammatory mediators. These proinflammatory mediators will induce the polarization of macrophages to M1 type with pro-inflammatory properties, forming a vicious cycle of pro-inflammation and pro-osteoclast, and ultimately aggravating joint destruction. Based on the central role of ROS in RA pathology, the development of antioxidant therapeutic strategies with ROS scavenging functions has become an important research direction.126 In addition, efforts are being made to develop smart drug delivery systems with ROS-responsive properties that can trigger precise drug release through the pathological microenvironment to improve therapeutic efficacy and reduce systemic toxicity.127,128 However, traditional oral or injectable administration has limitations such as gastrointestinal irritation, first-pass liver effect, and low patient compliance. DMNs technology combined with ROS response delivery system can achieve targeted therapy through transdermal drug delivery, which provides an innovative solution to break through the bottleneck of existing treatment.
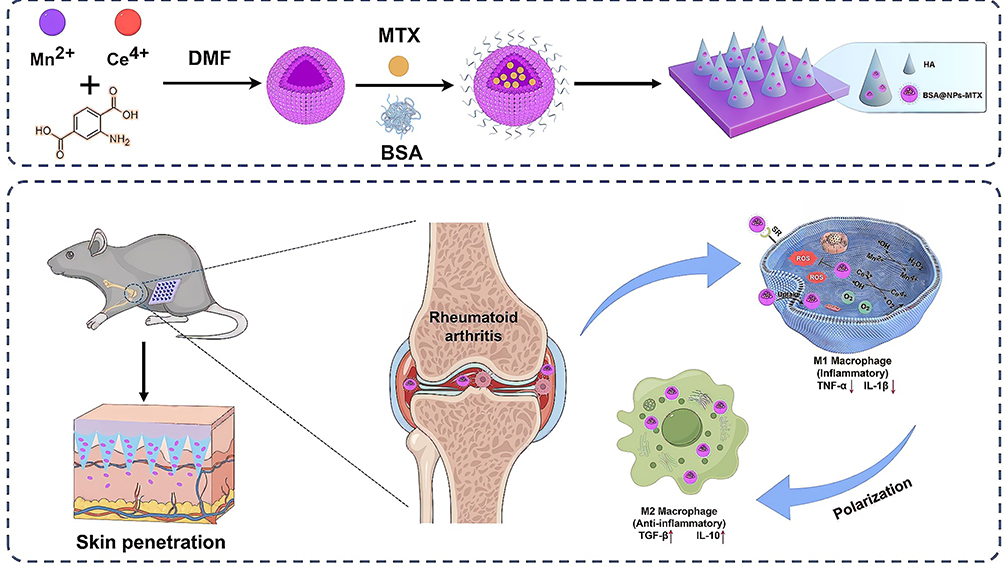 |
Figure 4 Schematic illustration of BSA@NPs-MTX preparation and corresponding therapeutic mechanism in RA treatment. Figure was created by Figdraw.129 Copyright 2024, Journal of Nanobiotechnology. |
Xia et al developed a HA-based DMNs loaded with cerium manganese oxide nanoparticles (NPs) for targeted therapy of RA, as shown in Figure 4. Aiming at the imbalance of inflammatory microenvironment caused by the increase of ROS in RA, MTX was loaded into cerium manganese NPs with antioxidant and catalytic functions and then integrated into MNs after modification by bovine serum albumin (BSA) to achieve transdermal delivery. In vitro experiments showed that BSA@NPs-MTX could clear ROS, promote the polarization of macrophages from pro-inflammatory M1 to anti-inflammatory M2, and reduce the secretion of TNF-α and other inflammatory cytokines. In vivo experiments in CIA mouse model confirmed that the MNs system was effective in reducing joint swelling, bone erosion and synovial inflammation, and improving cartilage damage, which was superior to MTX or NPs treatment alone.129
 |
Figure 5 Schematic of FTL@SIN MNs for rheumatoid arthritis treatment: (a) Preparation of FTL@SIN nanoparticles via self-assembly of FTL and SIN; (b) Fabrication process of ROS-responsive microneedles using HA as the matrix material; (c) In vivo immune response and anti-inflammatory mechanism of FTL@SIN MNs in RA treatment.59 Downward arrows (↓): Indicate the decrease of pro-inflammatory cytokines/cells (IL-6, TNF-α, M1 macrophages) in RA microenvironment. Upward arrows (↑): Denote the increase of anti-inflammatory cells (M2 macrophages) in RA treatment. Copyright 2024, International Journal of Biological Macromolecules. |
Liu et al developed a DMNs-mediated ROS-responsive drug delivery system for the treatment of RA. In this system, amphiphilic nanoparticles (FTL) were constructed by connecting fucoidan (Fuc) with luteolin (Lut) through ROS-responsive bond thioketal, and SIN was loaded to form ROS-responsive FTL@SIN nanocomposites, which were then loaded into Fuc-based DMNs by vacuum casting (Figure 5). This microneedle achieves local drug delivery with its efficient transdermal property and triggers drug release in the joint cavity where ROS is highly expressed. It has been shown that FTL@SIN responds to the high reactive oxygen environment of inflamed tissues, which in turn releases SIN. In addition, FTL@SIN could be taken up by inflammatory cells, inducing the transformation of macrophages from M1 to M2 phenotype, and reducing the content of inflammatory cytokines such as NO, TNF-α, IL-6. In the rat model of AIA, the microneedle system could effectively relieve joint swelling, reduce synovial inflammatory cell infiltration, and promote cartilage repair.59 However, this study was only limited to the rat model of AIA for efficacy and safety evaluation, and a variety of RA related animal models were not combined for comparative studies, making the results difficult to exclude the bias caused by model specificity.
 |
Figure 6 Schematic illustration of (A) the fabrication procedures of the HA-based microneedle encapsulated with dual HSA-contained nanocomplexes (TPH/CH MN) and (B) the RA therapeutic mechanism through inducing RA FLS apoptosis and regulating inflammatory macrophages.130 Copyright 2024, Bioactive Materials. |
Peng et al prepared HA-based DMN patches for transdermal co-delivery of two human serum albumin (HSA) -modified nanocomposites for synergistic treatment of RA, as shown in Figure 6. Thioketal-crosslinked fluorinated polyethyleneimine 1.8 K (TKPF) was engineered to complex with the pro-apoptotic gene PUMA-encoding plasmid. This complex was then coated with human serum albumin (HSA) to form TKPF/pPUMA@HSA (TPH) nanoparticles. TPH could up-regulate PUMA expression and induce apoptosis of FLS cells by responding to the release of genes in the high ROS environment in RA joints. HSA nanocomplex encapsulating the anti-inflammatory ingredient triptolide (CH) inhibited inflammation by NF-κB pathway. Animal experiments showed that TPH/CH MN combined treatment alleviated joint swelling, synovial hyperplasia and bone erosion in CIA mice, reduced serum levels of TNF-α, IL-6 and IL-1β, and promoted the polarization of macrophages from M1 to M2 phenotype.130
Synovitis and angiogenesis are two fundamental pathological factors that synergically exacerbate RA. Hua et al developed a DMNs patch integrating natural products (B/S-TM@MN) for the anti-inflammatory and anti-angiogenic combination therapy of RA. These microneedles were based on carboxymethyl cellulose and loaded with ROS-responsive micelles (B/S-TM), in which berberine (Ber) and sinomenine (Sin) were encapsulated. In vitro experiments had shown that B/S-TM can promote the polarization of macrophages from M1 type to M2 type, reduce the secretion of pro-inflammatory cytokines such as TNF-α and IL-6, and inhibit the migration and tube formation of vascular endothelial cells. In vivo in a mouse model of CIA, B/S-TM@MN was targeted and accumulated in the inflamed joint through the ELVIS effect, and the drug was released triggered by ROS, reducing CD68-positive macrophages and CD31-labeled vessel density, and alleviating joint swelling, bone erosion and cartilage damage.86
DMNs Combined with pH-Responsive Delivery System
Although the therapeutic drugs for RA have efficacy, the systemic side effects caused by them cannot be ignored. Fundamentally, the untargeted distribution of drugs is the key factor for adverse reactions. Notably, the articular cavity microenvironment showed acidic characteristics during the pathological process of RA. The pH of joint synovial fluid is about 6.0, and the pH in endosomes/lysosomes is even lower, about 4.5–5.5.131 Based on this, a pH-responsive nano-delivery system was designed to achieve precise controlled drug release at the target site. It maintains structural stability in the physiological environment to reduce systemic exposure, and triggers drug release in the acidic microenvironment to achieve the therapeutic goal of synergistic efficacy and attenuated toxicity. In addition, to enhance the targeting efficiency, DMNs technology was combined with pH-responsive system to form a dual targeting strategy. This innovative protocol has dual advantages. First, transdermal administration of microneedles can avoid the first-pass effect and improve drug bioavailability. Second, the pH-responsive nano-formulation released by the microneedle after dissolution in the dermis can achieve primary targeting by means of the EPR effect and trigger the precise release of the drug through the pH response of the microenvironment. This dual regulation mechanism not only reduces the drug loss in the systemic circulation, but also maximizes the therapeutic index through in situ drug release at the lesion site, providing a new technical path for the precise treatment of RA.
Febrianti et al developed a pH-responsive smart nanoparticle system (SNPs-MTX) by combining PEG-PCL copolymer with MTX. To avoid the side effects of MTX administration, the system was transdermally delivered by DMNs patch (SNP-DMAP-MTX). The in vitro drug release study showed that the drug release ability of SNP-DMAP-MTX in PBS medium at pH 5.0 was higher than that in PBS medium at pH 7.4. The amount of drug released in the first half hour was 1.23±0.14, which was about 0.4% of the prescribed amount. Then the drug was released slowly and reached 103.23±11.36 after 8 hours, which was about 41% of the prescribed amount. After 24 hours, the amount of release was 183.88±20.23, about 73% of the prescribed amount. However, the release amount of SNP-DMAP-MTX in PBS medium was 69.54±7.65 after 24 h, which was about 28% of the specified amount. The drug release rate of this system in inflamed tissues was higher than that in normal tissues, and it had pH-responsive targeting ability to inflamed tissues. In vivo pharmacokinetic studies showed that compared with oral administration, this delivery system reduced the peak plasma concentration (Cmax 0.65 vs 3.63 μg/mL) and prolonged the time to peak (Tmax 4 h vs 2 h), which could effectively reduce systemic side effects.87
DMNs Combined with Phototherapy for RA
Photodynamic therapy (PDT) and photothermal therapy (PTT) are both light-mediated treatment modalities, which have become promising alternative therapies for a variety of diseases due to their advantages of precise targeting, minimal invasiveness and low systemic toxicity. PDT is a targeted therapy technology based on photochemical reaction. The mechanism of action of PDT is that under light irradiation of a specific wavelength, the enriched photosensitizer molecules in the target area can activate oxygen molecules to generate ROS, and then induce cell apoptosis or death.132,133 Compared with conventional therapies, PDT has distinct advantages. On the one hand, photosensitizers enriched in the target area by local illumination can selectively kill diseased tissues or cells and protect normal cells to the greatest extent.88 On the other hand, PDT therapy is less invasive and less toxic, especially suitable for the treatment of superficial lesions.134 PDT has been used to treat cancer,132,135 and infectious diseases.136,137
Organisms are highly sensitive to temperature changes, and sudden increases in temperature can disrupt important cellular structures and interfere with essential functions.138 When the local temperature is increased to 41°C, the heat shock response is activated to combat heat-induced injury through the production of heat shock proteins. Irreversible tissue damage will occur when the temperature reaches 42°C. Exposure to temperatures between 42°C and 46°C for 10 minutes results in cell necrosis. Between 46 and 52°C, cells die rapidly due to microvascular thrombosis and ischemia. If the tissue temperature is higher than 60°C, protein denaturation and plasma membrane damage will immediately lead to cell death.139,140 This temperature-dependent biological effect provides the rationale for PTT, a non-invasive therapeutic technique based on photothermal conversion materials with photothermal agents (PAs) at its core, such as carbon nanomaterials, gold nanomaterials, silver nanomaterials, and germanium nanocrystals. PAs can effectively absorb light at specific wavelengths, convert light energy into heat energy, and locally generate high temperatures to eliminate diseased cells or regulate biological processes.141 PTT has a wide range of applications, covering tumor therapy,142 anti-infection,143 and inflammatory diseases.144 Notable advancements have been made in the domain of MN-assisted PDT and PTT, particularly in the formulation of synergistic therapeutic strategies. Figure 7 provides a schematic representation of MNs in combination with PTT and PDT for the treatment of diseases.
 |
Figure 7 Schematic illustration of MNs combined with PTT and PDT for the treatment of skin diseases. (A) Precursors or PSs or PAs are conjugated with nano-materials including polymers, gene, antigen or drug for the fabrication of MNs. (B) The insertion of MN arrays into the skin allows the precursors or PSs or PAs to penetrate into the disease site. (C) Precursors or PSs or PAs are photo-excited using NIR radiation, and produced cytotoxic ROS to induce cell death or generated heat to ablatedisease cells or release chemical drugs to kill abnormal cells for therapeutic purposes.141 Copyright 2020, Journal of Controlled Release. |
DMNs Combined with PDT
Since the first report of PDT for RA treatment in 1995, the application of PDT in RA has received increasing attention. The photosensitizers are specifically accumulated in the inflamed parts of the synovial membrane of the joint, and they are irradiated with specific wavelengths of light to produce ROS that effectively eliminate infiltrating macrophages, synovial fibroblasts and other inflammatory cells, thereby reducing the concentration of related inflammatory cytokines IL-17, TNF-α, IL-1β and IL-6.145 As PS evolves from the first to the third generation, its targeting, photochemical properties, and safety continue to increase.146 However, conventional systemic administration, such as oral administration or injection, leads to severe photosensitivity, which limits its application. For this bottleneck, DMNs show unique advantages. DMNs can painlessly penetrate the cuticle of the skin, deliver the photosensitizer accurately to the inflamed sites around the joint, increase its concentration in the target tissue, reduce normal tissue distribution, and maximize efficacy and minimize toxicity.. Therefore, the combination of DMNs and PDT provides new ideas for the treatment of RA.
Li et al developed a dissolving microneedle array (5-ALA@DMNA) loaded with 5-aminolevulinic acid (5-ALA) to treat RA by photodynamic therapy. 5-ALA@DMNA efficiently penetrated the stratum corneum of the skin to deliver 5-ALA topically, and was selectively metabolized to the photosensitizer protoporphyrin IX (PpIX) in fibroblast-like synoviocytes of RA. In vitro experiments showed that 5-ALA-mediated PDT inhibited the migration and selectively induced apoptosis of RA-FLS by inducing the generation of reactive oxygen species under 635 nm light. In a rat model of adjuvant-induced arthritis, the results showed that 5-ALA@DMNA mediated PDT showed a good therapeutic effect on RA, which could effectively reduce joint swelling and inflammation, reduce the levels of pro-inflammatory cytokines TNF-α, IL-6 and IL-17, and increase the levels of anti-inflammatory cytokines IL-4 and IL-10. In addition, the microneedle array has good biocompatibility, and the skin puncture holes can heal within 24 hours. Therefore, the combination of DMNs and PDT may be a potential treatment for RA.88
DMNs Combined with PTT
In the treatment of RA, the targeting of PTT stems from the similar pathological characteristics of inflammatory tissues and tumors. Inflamed tissues are rich in blood vessels and heat is not easy to lose, so their heat resistance is lower than that of normal tissues.89 PA can increase local tissue temperature under near infrared (NIR) irradiation. An increase in temperature to 41 to 47°C produces a hyperthermic effect that inhibits the growth of inflammatory tissue and the formation of vascular opacities, and cause damage ablation through irreversible protein denaturation, nucleic acid damage and cytoplasmic evaporation, leading to inflammatory cell apoptosis.145,147 Therefore, PTT can alleviate RA by local clearance of inflammatory cells by hyperthermic effects. To improve efficacy, investigators have developed an innovative delivery system that combines DMNs with PTT. The system effectively penetrates the stratum corneum and enables painless and accurate delivery of PA and anti-inflammatory drugs to joint lesions. The photothermal effect not only promotes drug release to enhance anti-inflammatory efficacy, but also controls the area and timing of light exposure to ensure the clearance of inflammatory cells while minimizing systemic toxicity.148 The combined strategy of DMNs and PTT integrates multiple mechanisms, including physical permeation, photoactivated drug release, and selective cellular targeting, to provide a novel treatment for RA with high efficiency and low toxicity.
Lu et al prepared a DMNs system (Lox + Tof NPs@MN) with photothermal (PT) properties based on polydopamine (PDA) to co-deliver the nonsteroidal anti-inflammatory drug loxoprofen (Lox) and the JAK inhibitor tofacitinib (Tof) for the synergistic treatment of RA. The study showed that under 808 nm near-infrared light irradiation, the PDA within the microneedles produced a photothermal effect, and the local temperature rose to 40 °C, which promoted the penetration and retention of drugs in the skin and joint cavity. In the carrageenan/kaolin-induced arthritis rat model, 808+Lox+Tof NPs @ MN showed efficacy, and the joint swelling degree was reduced to 3.1% compared with 31.1% of the control group. The effect of improving calf muscle atrophy was the most obvious. The proportion of calf muscle was restored to 103.5%, and the expression of TNF-α, IL-1β, iNOS and JAK\/STAT pathway-related genes in articular cartilage was down-regulated. Importantly, the efficacy of the microneedle system is superior to traditional intra-articular injection, and it has good safety and patient compliance.89
Considering the unique characteristics of joints, precise coordination between MN and skin is required to accommodate joint motion and ensure drug delivery efficiency.149 Shen et al combined gold nanorods (AuNRs) and tacrolimus (TAC) to develop a flexible photothermal DMNs patch (AuNRs/TAC-FMNs). In this study, the conical MN arrays were fabricated using gelatin as a flexible substrate, which was mechanically strong enough to penetrate the skin, while the gelatin substrate exhibited excellent flexibility and bending recovery. The near-infrared photothermal response characteristics of gold nanorods combined with the chemical anti-inflammatory effect of TAC realized the synergistic effect of photothermal-chemotherapy. In the AIA rat model, AuNRs/TAC-FMNs could reduce joint swelling, inhibit the expression of inflammatory cytokines such as IL-1β and TNF-α, and promote bone repair through nano-hydroxyapatite. In addition, this method also reduces the liver and kidney toxicity of TAC, providing an efficient and safe synergistic strategy for RA treatment.90
Patents and Clinical Trials of DMNs in RA
As an emerging transdermal drug delivery platform, DMNs have shown great potential in the treatment of RA. In recent years, the patents of dissolving microneedles technology for RA treatment have shown explosive growth. These patents have not only continuously expanded the types of drug delivery but also made progress in the accuracy and intelligence of the delivery system. Patent CN119280137A develops a dissolving microneedle based on metal-drug coordination nanoparticles. In this technology, Zn2⁺ was used as the central ion to form coordination nanoparticles with the targeting peptide (Fmoc-HTKPR) and methotrexate (MTX), which were loaded into the MNS. Nanoparticles released after dissolution of microneedles in vivo can actively target the inflammatory site and release drugs in response to the high level of reactive oxygen species (ROS) in the lesion, achieving precise drug delivery and synergistic treatment.150 CN120053685A encapsulated Kartogenin (KGN) in mesenchymal stem cell membrane-derived nano vesicular vesicles (KGN@NVs), which were then incorporated into a dissolving microneedle. This design combines the innate immunomodulatory function of MSCS vesicles with the efficient transdermal delivery ability of microneedles, which promotes cartilage repair while reducing the expression of inflammatory cytokines such as IL-1β and TNF-α.151 Patent CN116831975A proposes an immune tolerogenic microneedle patch co-loaded with a self-antigenic peptide and an immunomodulator. The microneedles can deliver drugs through the skin to the dermis with dense immune cells, induce the generation of tolerogenic dendritic cells, and then activate regulatory T cells (Treg) to restore the immune balance of RA patients, demonstrating the unique value of microneedles in disease modification therapy.152 Patent CN117224467A designed a ROS-responsive Platycodon grandiflorum extracellular vesicles, which was prepared by co-incubation of Platycodon grandiflorum extracellular vesicles with nanocarriers constructed by fucoidan, thioketal and luteolin. The carrier was further loaded in dissolving microneedles, which provided a new drug delivery system for targeted therapy of rheumatoid arthritis.153 Another patent, CN115154405A, discloses a luteolin dissolving microneedle and its preparation method. The prepared microneedle not only has the mechanical strength suitable for skin administration, but also has excellent skin adhesion, which can achieve effective treatment of rheumatoid arthritis by percutaneous delivery of luteolin.154
Although dissolving microneedles are very active in the patent field of RA treatment, their clinical transformation is still in the early stage. Through a comprehensive search of international clinical trial databases such as clinicaltrials.gov, we found that there is no clinical trial registration of dissolving microneedles targeting RA. The existing relevant clinical trials mainly focus on diabetes, vaccine delivery, skin diseases and other indications, but it also provides important safety and feasibility reference for the application of RA. A clinical trial (ID NCT04936984) evaluated and compared the bioequivalence of two Abaloparatide-sMTS treatments in healthy women.155 In another clinical trial (ID NCT01674621), the therapeutic effect of Abaloparatide transdermal microneedle patch on postmenopausal osteoporosis was evaluated.156 The skin safety of denosumab dissolving microneedle patch was also studied (ID NCT07085520).157 Among them, a clinical trial (ID NCT03607903) carried out by the Netherlands human drug research center is particularly noteworthy. Adalimumab is an effective biological agent for the treatment of autoimmune diseases such as RA, but traditional subcutaneous injection has pain and patient compliance problems. A randomized double-blind placebo-controlled trial was conducted to compare the pain perception, acceptability, and local tolerance of 40 mg adalimumab via microneedle intradermal injection (ID) with traditional subcutaneous injection (SC) in healthy adult volunteers. The safety, pharmacokinetics, pharmacodynamics, and immunogenicity of both administration methods were also evaluated. It provided an important clinical basis for the delivery of biological agents through microneedle technology.158 It is worth mentioning that the dissolving microneedle patch (MICROEPAD™) developed by Advaccine Biopharmaceuticals Suzhou Co., Ltd had been approved by FDA for listing OTC category.159 This indicates that the dissolving microneedle as a drug delivery technology platform has been recognized by regulatory authorities. It laid an important foundation for the clinical development of dissolving microneedles for RA treatment in the future.
Conclusion and Prospect
As an autoimmune disease characterized by chronic synovitis and joint destruction, RA is difficult to cure and seriously affects the quality of life of patients. At present, clinical treatment mainly uses oral or injection therapeutic drugs to relieve pain and delay the development of the disease. However, such drug delivery methods have problems such as poor targeting, low bioavailability, strong toxic side effects, and poor patient compliance, which seriously affect the treatment effect. As a minimally invasive percutaneous delivery technology, DMNs have shown unique advantages in the treatment of RA. First, DMNs have the advantage of physical targeting, which can directly deliver drugs to the inflamed joint, reducing systemic drug exposure and systemic side effects. Second, DMNs is minimally invasive and painless drug administration, and the puncture process does not touch the nerves and blood vessels, which avoids the pain and infection risk caused by traditional injection, and avoids gastrointestinal stimulation caused by oral administration, and improves the medication compliance of RA patients who need long-term treatment. Third, the matrix materials of DMNs include natural and synthetic polymers, and the balance between the mechanical strength of DMNs and the drug release performance can be achieved by rational compatibility. Fourth, DMNs have a wide range of drug loading capacity, which can load a variety of RA treatment drugs such as non-steroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs, peptide drugs, and active ingredients of traditional Chinese medicine. At the same time, DMNs can break through the cuticle barrier of the skin and solve the penetration problem of traditional transdermal drug delivery. In addition, the synergistic integration of DMNs and multiple technologies can achieve the improvement of drug delivery efficiency and efficacy in RA treatment. The combination of DMNs and nano-delivery system can improve drug solubility and targeted enrichment ability. The combination of DMNs and cell membrane biomimetic technology can give the system the function of actively targeting the inflammatory site. DMNs combined with photodynamic/photothermal therapy can enhance the efficacy through the dual effects of inflammatory cell killing and drug osmosis.
Although DMNs have shown potential application in the field of RA, there are still many challenges in clinical translation. Firstly, the current research mostly stays in the preclinical stage, most experiments are based on animal models, and there are great differences between humans and animals. Secondly, the long-term safety of DMNs is critical for their successful clinical translation. Current studies have evaluated the skin irritation of DMNs through experimental animal models, but the experimental period is short, which is not enough to illustrate the long-term safety of DMNs. Thirdly, despite the increasing research on DMNs, stability studies are rarely reported in the literature. In addition, the drug release rate of DMNs is mainly in vitro, and the drug release rate of DMNs in vivo needs to be further verified. At the same time, the current pharmacokinetic study of DMNs is insufficient, and the absorption, distribution, metabolism and excretion of drugs in the body are lacking, which is difficult to support clinical medication guidance. Finally, the performance evaluation system of DMNs has not been established, which also brings obstacles to its clinical translation. Therefore, future research should focus on solving these key problems to promote DMNs to clinical practice.
In summary, DMNs as a minimally invasive percutaneous drug delivery technology provides a new strategy for the treatment of RA. DMNs have the characteristics of physical targeting, minimally invasive and painless, and integration with other technical platforms, which is helpful to solve the problems of poor targeting, substantial side effects and low patient compliance in traditional drug delivery methods. However, the clinical translation of DMNs still faces several challenges. Future research should focus on advancing validation using translational models, conducting long-term safety evaluations and formulation stability studies, elucidating the in vivo processes in greater depth, and establishing standardized evaluation systems. Additionally, the integration of DMNs with various technologies represents an important direction for future development. By combining ligand-receptor mediated nanoformulations or matrix metalloproteinase-responsive drug release systems, it is possible to achieve precise drug delivery and intelligent release. Furthermore, DMNs serving as delivery carriers for cell therapy and gene therapy are expected to enhance local targeting and therapeutic efficacy. Moreover, integrating DMNs with wearable devices holds the potential to achieve real-time monitoring and dynamic administration, thereby advancing RA treatment toward personalization and diagnosis and treatment integration. In summary, with the continuous advancement of science and technology, DMNs are expected to play an important role in the treatment of RA.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Consent for Publication
All authors have reviewed the final version of the manuscript and approved it for publication.
Acknowledgments
The authors thank for grants from General Project of Shaanxi Provincial Department of Science and Technology, Qinchuangyuan Traditional Chinese Medicine Industry Innovation Aggregation Zone Project, Capital’s Funds for Health Improvement and Research and General Project of Shaanxi Provincial Department of Science and Technology.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by grants from General Project of Shaanxi Provincial Department of Science and Technology (grant No. 2024SF-YBXM-496), Qinchuangyuan Traditional Chinese Medicine Industry Innovation Aggregation Zone Project (Traditional Chinese Medicine University, Medical Institutions), (grant No. L2024-QCY-ZYYJJQ-X27), Capital’s Funds for Health Improvement and Research (grant No. 2024-1-4162), General Project of Shaanxi Provincial Department of Science and Technology (grant No. 2025JC-YBMS-1033).
Disclosure
The authors declare no competing interests in this work.
References
1. Jakobsson P, Robertson L, Welzel J, et al. Where traditional Chinese medicine meets Western medicine in the prevention of rheumatoid arthritis. J Intern Med. 2022;292(5):745–34. doi:10.1111/joim.13537
2. Radu AF, Bungau SG. Management of Rheumatoid Arthritis: an Overview. Cells. 2021;10(11):2857. doi:10.3390/cells10112857
3. Gorantla S, Batra U, Samshritha R, et al. Emerging trends in microneedle-based drug delivery strategies for the treatment of rheumatoid arthritis. Expert Opin Drug Delivery. 2022;19(4):395–407. doi:10.1080/17425247.2022.2053674
4. McInnes IB, Schett G. Pathogenetic insights from the treatment of rheumatoid arthritis. Lancet. 2017;389(10086):2328–2337. doi:10.1016/S0140-6736(17)31472-1
5. Scherer HU, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. 2020;110:102400. doi:10.1016/j.jaut.2019.102400
6. Bullock J, Rizvi SAA, Saleh AM, et al. Rheumatoid Arthritis: a Brief Overview of the Treatment. Med Princ Pract. 2018;27(6):501–507. doi:10.1159/000493390
7. Hua C, Buttgereit F, Combe B. Glucocorticoids in rheumatoid arthritis: current status and future studies. RMD Open. 2020;6(1):e000536. doi:10.1136/rmdopen-2017-000536
8. Cutolo M, Paolino S, Gotelli E. Glucocorticoids in rheumatoid arthritis still on first line: the reasons. Expert Review of Clinical Immunology. 2021;17(5):417–420. doi:10.1080/1744666X.2021.1903319
9. Benucci M, Damiani A, Infantino M, et al. Cardiovascular safety, cancer and Jak-inhibitors: differences to be highlighted. Pharmacol Res. 2022;183:106359. doi:10.1016/j.phrs.2022.106359
10. He Y, Majid K, Maqbool M, et al. Formulation and characterization of lornoxicam-loaded cellulosic-microsponge gel for possible applications in arthritis. Saudi Pharm J. 2020;28(8):994–1003. doi:10.1016/j.jsps.2020.06.021
11. Watanabe T, Fujiwara Y, Chan FKL. Current knowledge on non-steroidal anti-inflammatory drug-induced small-bowel damage: a comprehensive review. J Gastroenterol. 2020;55(5):481–495. doi:10.1007/s00535-019-01657-8
12. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N Engl J Med. 2022;386(4):316–326. doi:10.1056/NEJMoa2109927
13. He J, Zhang Y, Yu X, Xu C. Wearable patches for transdermal drug delivery. Acta Pharmaceutica Sinica B. 2023;13(6):2298–2309. doi:10.1016/j.apsb.2023.05.009
14. Liu XY, Pei WJ, Wu YZ, Ren FL, Yang SY, Wang X. Transdermal delivery of triptolide–phospholipid complex to treat rheumatoid arthritis. Drug Delivery. 2021;28(1):2127–2136. doi:10.1080/10717544.2021.1986603
15. Shang H, Younas A, Zhang N. Recent advances on transdermal delivery systems for the treatment of arthritic injuries: from classical treatment to nanomedicines. WIREs Nanomed Nanobiotechnol. 2022;14(3):e1778. doi:10.1002/wnan.1778
16. Wang FY, Chen Y, Huang YY, Cheng CM. Transdermal drug delivery systems for fighting common viral infectious diseases. Drug Deliv Transl Res. 2021;11(4):1498–1508. doi:10.1007/s13346-021-01004-6
17. Karande P, Jain A, Ergun K, Kispersky V, Mitragotri S. Design principles of chemical penetration enhancers for transdermal drug delivery. Proc Natl Acad Sci USA. 2005;102(13):4688–4693. doi:10.1073/pnas.0501176102
18. Kim TH, Kim NY, Lee HU, Choi JW, Kang T, Chung BG. Smartphone-based iontophoresis transdermal drug delivery system for cancer treatment. J Control Release. 2023;364:383–392. doi:10.1016/j.jconrel.2023.10.046
19. Tokumoto S, Higo N, Sugibayashi K. Effect of electroporation and pH on the iontophoretic transdermal delivery of human insulin. Int J Pharm. 2006;326(1–2):13–19. doi:10.1016/j.ijpharm.2006.07.002
20. Gupta J, Prausnitz MR. Recovery of Skin Barrier Properties after Sonication in Human Subjects. Ultrasound Med Biol. 2009;35(8):1405–1408. doi:10.1016/j.ultrasmedbio.2009.04.001
21. Lin Z, Zheng K, Zhong J, Zheng X. Advances in microneedle-based therapy for bone disorders. Biomed Pharmacother. 2023;165:115013. doi:10.1016/j.biopha.2023.115013
22. Xu C, Wu Y, Zhao L, et al. Transdermal hormone delivery: strategies, application and modality selection. J Drug Delivery Sci Technol. 2023;86:104730. doi:10.1016/j.jddst.2023.104730
23. Sartawi Z, Blackshields C, Faisal W. Dissolving microneedles: applications and growing therapeutic potential. J Control Release. 2022;348:186–205. doi:10.1016/j.jconrel.2022.05.045
24. Ai X, Yang J, Liu Z, Guo T, Feng N. Recent progress of microneedles in transdermal immunotherapy: a review. Int J Pharm. 2024;662:124481. doi:10.1016/j.ijpharm.2024.124481
25. Guo P, Huang C, Yang Q, et al. Advances in Formulations of Microneedle System for Rheumatoid Arthritis Treatment. Int J Nanomed. 2023;18:7759–7784. doi:10.2147/IJN.S435251
26. Zhang L, Guo R, Wang S, Yang X, Ling G, Zhang P. Fabrication, evaluation and applications of dissolving microneedles. Int J Pharm. 2021;604:120749. doi:10.1016/j.ijpharm.2021.120749
27. Wendong Y, Xingxing Y, Xianze X, et al. Nanoformulation-assisted microneedle transdermal drug delivery system: an innovative platform enhancing rheumatoid arthritis treatment. Biomed Pharmacother. 2024;178:117219. doi:10.1016/j.biopha.2024.117219
28. Hou X, Li J, Hong Y, et al. Advances and Prospects for Hydrogel-Forming Microneedles in Transdermal Drug Delivery. Biomedicines. 2023;11(8):2119. doi:10.3390/biomedicines11082119
29. Ma G, Wu C. Microneedle, bio-microneedle and bio-inspired microneedle: a review. J Control Release. 2017;251:11–23. doi:10.1016/j.jconrel.2017.02.011
30. Zhao W, Zheng L, Yang J, Ma Z, Tao X, Wang Q. Dissolving microneedle patch-assisted transdermal delivery of methotrexate improve the therapeutic efficacy of rheumatoid arthritis. Drug Delivery. 2023;30(1):121–132. doi:10.1080/10717544.2022.2157518
31. Chudzińska J, Wawrzyńczak A, Feliczak-Guzik A. Microneedles Based on a Biodegradable Polymer—Hyaluronic Acid. Polymers. 2024;16(10):1396. doi:10.3390/polym16101396
32. Kim JS, Ah CJ, Kim JC, et al. Microneedles with dual release pattern for improved immunological efficacy of Hepatitis B vaccine. Int J Pharm. 2020;591:119928. doi:10.1016/j.ijpharm.2020.119928
33. Yu K, Yu X, Cao S, et al. Layered dissolving microneedles as a need-based delivery system to simultaneously alleviate skin and joint lesions in psoriatic arthritis. Acta Pharmaceutica Sinica B. 2021;11(2):505–519. doi:10.1016/j.apsb.2020.08.008
34. Wang Y, Yang C, Liu W, et al. Enhanced efficacy of brucine dissolving-microneedles as a targeted delivery system in rheumatoid arthritis treatment: a comprehensive pharmacokinetic-pharmacodynamic analysis. Drug Deliv Transl Res. 2024. doi:10.1007/s13346-024-01606-w
35. Mönkäre J, Reza Nejadnik M, Baccouche K, Romeijn S, Jiskoot W, Bouwstra JA. IgG-loaded hyaluronan-based dissolving microneedles for intradermal protein delivery. J Control Release. 2015;218:53–62. doi:10.1016/j.jconrel.2015.10.002
36. Yu J, Wang J, Zhang Y, et al. Glucose-responsive insulin patch for the regulation of blood glucose in mice and minipigs. Nat Biomed Eng. 2020;4(5):499–506. doi:10.1038/s41551-019-0508-y
37. Park KH, Oh EY, Han H, et al. Efficacy of transdermal immunotherapy with biodegradable microneedle patches in a murine asthma model. Clin Experimental Allergy. 2020;50(9):1084–1092. doi:10.1111/cea.13688
38. Wang X, Yue J, Guo S, et al. Dissolving microneedles: a transdermal drug delivery system for the treatment of rheumatoid arthritis. Int J Pharm. 2025;671:125206. doi:10.1016/j.ijpharm.2025.125206
39. Lee K, Lee CY, Jung H. Dissolving microneedles for transdermal drug administration prepared by stepwise controlled drawing of maltose. Biomaterials. 2011;32(11):3134–3140. doi:10.1016/j.biomaterials.2011.01.014
40. Li R, Zhang L, Jiang X, et al. 3D-printed microneedle arrays for drug delivery. J Control Release. 2022;350:933–948. doi:10.1016/j.jconrel.2022.08.022
41. Liu H, Nail A, Meng D, et al. 3D printed eutectogel dissolving microneedles patch loaded with chitosan-based nanoparticles for diabetic wound management. Int J Biol Macromol. 2025;307:142018. doi:10.1016/j.ijbiomac.2025.142018
42. Amodwala S, Kumar P, Thakkar HP. Statistically optimized fast dissolving microneedle transdermal patch of meloxicam: a patient friendly approach to manage arthritis. Eur J Pharm Sci. 2017;104:114–123. doi:10.1016/j.ejps.2017.04.001
43. Cao J, Zhang N, Wang Z, et al. Microneedle-Assisted Transdermal Delivery of Etanercept for Rheumatoid Arthritis Treatment. Pharmaceutics. 2019;11(5):235. doi:10.3390/pharmaceutics11050235
44. Yasin A, Ren Y, Li J, Sheng Y, Cao C, Zhang K. Advances in Hyaluronic Acid for Biomedical Applications. Front Bioeng Biotechnol. 2022;10:910290. doi:10.3389/fbioe.2022.910290
45. Zhu J, Tang X, Jia Y, Ho CT, Huang Q. Applications and delivery mechanisms of hyaluronic acid used for topical/transdermal delivery – a review. Int J Pharm. 2020;578:119127. doi:10.1016/j.ijpharm.2020.119127
46. Huang G, Huang H. Application of hyaluronic acid as carriers in drug delivery. Drug Delivery. 2018;25(1):766–772. doi:10.1080/10717544.2018.1450910
47. Du H, Liu P, Zhu J, et al. Hyaluronic Acid-Based Dissolving Microneedle Patch Loaded with Methotrexate for Improved Treatment of Psoriasis. ACS Appl Mater Interfaces. 2019;11(46):43588–43598. doi:10.1021/acsami.9b15668
48. Confederat LG, Tuchilus CG, Dragan M, Sha’at M, Dragostin OM. Preparation and Antimicrobial Activity of Chitosan and Its Derivatives: a Concise Review. Molecules. 2021;26(12):3694. doi:10.3390/molecules26123694
49. Li H, Cui J, Zhang T, Lin F, Zhang G, Feng Z. Research Progress on Chitosan Microneedle Arrays in Transdermal Drug Delivery. IJN. 2024;19:12957–12973. doi:10.2147/IJN.S487313
50. Fonseca DFS, Vilela C, Silvestre AJD, Freire CSR. A compendium of current developments on polysaccharide and protein-based microneedles. Int J Biol Macromol. 2019;136:704–728. doi:10.1016/j.ijbiomac.2019.04.163
51. Chen MC, Lai KY, Ling MH, Lin CW. Enhancing immunogenicity of antigens through sustained intradermal delivery using chitosan microneedles with a patch-dissolvable design. Acta Biomater. 2018;65:66–75. doi:10.1016/j.actbio.2017.11.004
52. Volpi N. Chondroitin Sulfate Safety and Quality. Molecules. 2019;24(8):1447. doi:10.3390/molecules24081447
53. Abourehab MAS, Baisakhiya S, Aggarwal A, et al. Chondroitin sulfate-based composites: a tour d’horizon of their biomedical applications. J Mater Chem B. 2022;10(44):9125–9178. doi:10.1039/D2TB01514E
54. Bui VD, Jeon J, Duong VH, et al. Chondroitin sulfate-based microneedles for transdermal delivery of stem cell-derived extracellular vesicles to treat rheumatoid arthritis. J Control Release. 2024;375:105–115. doi:10.1016/j.jconrel.2024.08.050
55. Lu H, Wang J, Li J, Gao B, He B. Advanced Silk Fibroin Biomaterials‐Based Microneedles for Healthcare. Macromol biosci. 2023;23(11):2300141. doi:10.1002/mabi.202300141
56. Yin Z, Kuang D, Wang S, Zheng Z, Yadavalli VK, Lu S. Swellable silk fibroin microneedles for transdermal drug delivery. Int J Biol Macromol. 2018;106:48–56. doi:10.1016/j.ijbiomac.2017.07.178
57. Zhu M, Liu Y, Jiang F, Cao J, Kundu SC, Lu S. Combined Silk Fibroin Microneedles for Insulin Delivery. ACS Biomater Sci Eng. 2020;6(6):3422–3429. doi:10.1021/acsbiomaterials.0c00273
58. Wang C, Liu S, Xu J, et al. Dissolvable microneedles based on Panax notoginseng polysaccharide for transdermal drug delivery and skin dendritic cell activation. Carbohydr Polym. 2021;268:118211. doi:10.1016/j.carbpol.2021.118211
59. Liu X, Diao N, Song S, et al. Inflammatory macrophage reprogramming strategy of fucoidan microneedles-mediated ROS-responsive polymers for rheumatoid arthritis. Int J Biol Macromol. 2024;271:132442. doi:10.1016/j.ijbiomac.2024.132442
60. RK A, Anjani QK, Hartrianti P, Donnelly RF, Ramadon D. Fabrication of dissolving microneedles for transdermal delivery of protein and peptide drugs: polymer materials and solvent casting micromoulding method. Pharmal Develop Technol. 2023;28(10):1016–1031. doi:10.1080/10837450.2023.2285498
61. Li Y, Hu X, Dong Z, et al. Dissolving Microneedle Arrays with Optimized Needle Geometry for Transcutaneous Immunization. Eur J Pharm Sci. 2020;151:105361. doi:10.1016/j.ejps.2020.105361
62. Cole G, McCaffrey J, Ali AA, et al. Dissolving microneedles for DNA vaccination: improving functionality via polymer characterization and RALA complexation. Hum Vaccines Immunother. 2017;13(1):50–62. doi:10.1080/21645515.2016.1248008
63. Aung NN, Ngawhirunpat T, Rojanarata T, Patrojanasophon P, Pamornpathomkul B, Opanasopit P. Fabrication, characterization and comparison of α-arbutin loaded dissolving and hydrogel forming microneedles. Int J Pharm. 2020;586:119508. doi:10.1016/j.ijpharm.2020.119508
64. Zhang N, Zhou X, Liu L, Zhao L, Xie H, Yang Z. Dissolving Polymer Microneedles for Transdermal Delivery of Insulin. Front Pharmacol. 2021;12:719905. doi:10.3389/fphar.2021.719905
65. Javanbakht S, Shaabani A. Carboxymethyl cellulose-based oral delivery systems. Int J Biol Macromol. 2019;133:21–29. doi:10.1016/j.ijbiomac.2019.04.079
66. Silva ACQ, Pereira B, Lameirinhas NS, et al. Dissolvable Carboxymethylcellulose Microneedles for Noninvasive and Rapid Administration of Diclofenac Sodium. Macromol biosci. 2023;23(1):2200323. doi:10.1002/mabi.202200323
67. Chen Y, Geever LM, Killion JA, Lyons JG, Higginbotham CL, Devine DM. Review of Multifarious Applications of Poly (Lactic Acid). Polym Plast Technol Eng. 2016;55(10):1057–1075. doi:10.1080/03602559.2015.1132465
68. Kang S, Song JE, Jun SH, Park SG, Kang NG. Sugar-Triggered Burst Drug Releasing Poly-Lactic Acid (PLA) Microneedles and Its Fabrication Based on Solvent-Casting Approach. Pharmaceutics. 2022;14(9):1758. doi:10.3390/pharmaceutics14091758
69. Marquina S, Ozgul M, Robertson-Brown K, Kenney MC. A review on PLGA particles as a sustained drug-delivery system and its effect on the retina. Exp Eye Res. 2023;235:109626. doi:10.1016/j.exer.2023.109626
70. Lee C, Kim J, Um DJ, et al. Optimization of Layered Dissolving Microneedle for Sustained Drug Delivery Using Heat-Melted Poly(Lactic-Co-glycolic Acid). Pharmaceutics. 2021;13(7):1058. doi:10.3390/pharmaceutics13071058
71. Woodruff MA, Hutmacher DW. The return of a forgotten polymer—Polycaprolactone in the 21st century. Prog Polym Sci. 2010;35(10):1217–1256. doi:10.1016/j.progpolymsci.2010.04.002
72. Eum J, Kim Y, Um D, Shin J, Yang H, Jung H. Solvent-Free Polycaprolactone Dissolving Microneedles Generated via the Thermal Melting Method for the Sustained Release of Capsaicin. Micromachines. 2021;12(2):167. doi:10.3390/mi12020167
73. Yao W, Tao C, Zou J, et al. Flexible two-layer dissolving and safing microneedle transdermal of neurotoxin: a biocomfortable attempt to treat Rheumatoid Arthritis. Int J Pharm. 2019;563:91–100. doi:10.1016/j.ijpharm.2019.03.033
74. Song X, Wang Y, Chen H, et al. Dosage-efficacy relationship and pharmacodynamics validation of brucine dissolving microneedles against rheumatoid arthritis. J Drug Delivery Sci Technol. 2021;63:102537. doi:10.1016/j.jddst.2021.102537
75. Liu T, Fu J, Chen M, et al. In situ polymeric nanomicelle-generating dissolving microneedle patch for enhanced transdermal methotrexate delivery in rheumatoid arthritis treatment. Eur Polym J. 2024;210:113008. doi:10.1016/j.eurpolymj.2024.113008
76. Wu X, Chen Y, Gui S, et al. Sinomenine hydrochloride-loaded dissolving microneedles enhanced its absorption in rabbits. Pharmal Develop Technol. 2015;2015:1–7. doi:10.3109/10837450.2015.1055766
77. Jiang X, Chen P, Niu W, et al. Preparation and evaluation of dissolving tofacitinib microneedles for effective management of rheumatoid arthritis. Eur J Pharm Sci. 2023;188:106518. doi:10.1016/j.ejps.2023.106518
78. Du G, He P, Zhao J, et al. Polymeric microneedle-mediated transdermal delivery of melittin for rheumatoid arthritis treatment. J Control Release. 2021;336:537–548. doi:10.1016/j.jconrel.2021.07.005
79. Zhao W, Zheng L, Yang J, et al. Dissolving microneedle patches-mediated percutaneous delivery of tetramethylpyrazine for rheumatoid arthritis treatment. Eur J Pharm Sci. 2023;184:106409. doi:10.1016/j.ejps.2023.106409
80. Li S, Chen Q, Zhang Y, et al. Hyaluronic acid dissolving microneedle patch-assisted acupoint transdermal delivery of triptolide for effective rheumatoid arthritis treatment. Sci Rep. 2024;14(1):25256. doi:10.1038/s41598-024-76341-w
81. Wei F, Wang Q, Liu H, et al. High Efficacy Combined Microneedles Array with Methotrexate Nanocrystals for Effective Anti-Rheumatoid Arthritis. Int J Nanomed. 2022;17:2397–2412. doi:10.2147/IJN.S365523
82. Diao N, Liu Y, Wang W, et al. Resveratrol nanocrystals based dissolving microneedles with highly efficient for rheumatoid arthritis. Drug Delivery and Translational Research. 2025;15(1):203–215. doi:10.1007/s13346-024-01581-2
83. Xie J, Zhu X, Wang M, Liu C, Ling G, Zhang P. Dissolving microneedle-mediated transdermal delivery of flurbiprofen axetil-loaded pH-responsive liposomes for arthritis treatment. Chem Eng J. 2024;482:148840. doi:10.1016/j.cej.2024.148840
84. Chen Q, Wu C, Wang S, et al. Glycyrrhizic acid modified Poria cocos polyscaccharide carbon dots dissolving microneedles for methotrexate delivery to treat rheumatoid arthritis. Front Chem. 2023;11:1181159. doi:10.3389/fchem.2023.1181159
85. Lin Y, Chen Y, Deng R, et al. Delivery of neutrophil membrane encapsulated non-steroidal anti-inflammatory drugs by degradable biopolymer microneedle patch for rheumatoid arthritis therapy. Nano Today. 2023;49:101791. doi:10.1016/j.nantod.2023.101791
86. Hua P, Yang S, Yu L, Huang Y, Chen M. Natural product-integrated microneedle patch for rheumatoid arthritis treatment through anti-inflammation and angiogenesis suppression. Biomater Sci. 2025;13(9):2462–2474. doi:10.1039/D5BM00036J
87. Febrianti NQ, Tunggeng MGR, Ramadhany ID, Asri RM, Djabir YY, Permana AD. Validation of UV–Vis spectrophotometric and colorimetric methods to quantify methotrexate in plasma and rat skin tissue: application to in vitro release, ex vivo and in vivo studies from dissolving microarray patch loaded pH-sensitive nanoparticle. Spectrochimica Acta Part a Molecular and Biomolecular Spectroscopy. 2024;315:124258. doi:10.1016/j.saa.2024.124258
88. Li Y, Zheng L, Cao W, et al. 5-aminolevulinic acid-loaded dissolving microneedle array for photodynamic therapy of rheumatoid arthritis on rats. Biomed Pharmacother. 2023;162:114684. doi:10.1016/j.biopha.2023.114684
89. Lu Y, Xiao T, Lai R, et al. Co-Delivery of Loxoprofen and Tofacitinib by Photothermal Microneedles for Rheumatoid Arthritis Treatment. Pharmaceutics. 2023;15(5):1500. doi:10.3390/pharmaceutics15051500
90. Shen S, Wan A, Wang Y, et al. Flexible microneedles incorporating gold nanorods and tacrolimus for effective synergistic photothermal-chemotherapy of rheumatoid arthritis. Int J Biol Macromol. 2024;276:133797. doi:10.1016/j.ijbiomac.2024.133797
91. Thakur S, Riyaz B, Patil A, Kaur A, Kapoor B, Mishra V. Novel drug delivery systems for NSAIDs in management of rheumatoid arthritis: an overview. Biomed Pharmacother. 2018;106:1011–1023. doi:10.1016/j.biopha.2018.07.027
92. Chapa-Villarreal FA, Stephens M, Pavlicin R, Beussman M, Peppas NA. Therapeutic delivery systems for rheumatoid arthritis based on hydrogel carriers. Adv Drug Delivery Rev. 2024;208:115300. doi:10.1016/j.addr.2024.115300
93. Moore RA, Derry S, Simon LS, Emery P. Nonsteroidal Anti‐Inflammatory Drugs, Gastroprotection, and Benefit–Risk. Pain Pract. 2014;14(4):378–395. doi:10.1111/papr.12100
94. Li J, Tian X, Wang K, Jia Y, Ma F. Transdermal delivery of celecoxib and α-linolenic acid from microemulsion-incorporated dissolving microneedles for enhanced osteoarthritis therapy. J Drug Targeting. 2023;31(2):206–216. doi:10.1080/1061186X.2022.2123492
95. Wang W, Zhou H, Liu L. Side effects of methotrexate therapy for rheumatoid arthritis: a systematic review. Eur J Med Chem. 2018;158:502–516. doi:10.1016/j.ejmech.2018.09.027
96. Visser K, Van Der Heijde D. Optimal dosage and route of administration of methotrexate in rheumatoid arthritis: a systematic review of the literature. Ann Rheumatic Dis. 2009;68(7):1094–1099. doi:10.1136/ard.2008.092668
97. Fraenkel L, Bathon JM, England BR, et al. American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care & Research. 2021;73(7):924–939. doi:10.1002/acr.24596
98. Burmester GR, Pope JE. Novel treatment strategies in rheumatoid arthritis. Lancet. 2017;389(10086):2338–2348. doi:10.1016/S0140-6736(17)31491-5
99. DeGrado WF, Musso GF, Lieber M, Kaiser ET, Kézdy FJ. Kinetics and mechanism of hemolysis induced by melittin and by a synthetic melittin analogue. Biophys J. 1982;37(1):329–338. doi:10.1016/S0006-3495(82)84681-X
100. Wu P, Liang Q, Feng P, et al. A Novel Brucine Gel Transdermal Delivery System Designed for Anti-Inflammatory and Analgesic Activities. IJMS. 2017;18(4):757. doi:10.3390/ijms18040757
101. Lu L, Huang R, Wu Y, et al. Brucine: a Review of Phytochemistry, Pharmacology, and Toxicology. Front Pharmacol. 2020;11:377. doi:10.3389/fphar.2020.00377
102. Liu WW, Qian X, Ji W, Lu Y, Wei G, Wang Y. Effects and safety of Sinomenine in treatment of rheumatoid arthritis contrast to methotrexate: a systematic review and Meta-analysis. J Tradit Chin Med. 2016;36(5):564–577. doi:10.1016/S0254-6272(16)30075-9
103. Zheng X, Li W, Xu H, et al. Sinomenine ester derivative inhibits glioblastoma by inducing mitochondria-dependent apoptosis and autophagy by PI3K/AKT/mTOR and AMPK/mTOR pathway. Acta Pharmaceutica Sinica B. 2021;11(11):3465–3480. doi:10.1016/j.apsb.2021.05.027
104. Shu Z, Cao Y, Tao Y, et al. Polyvinylpyrrolidone microneedles for localized delivery of sinomenine hydrochloride: preparation, release behavior of in vitro & in vivo, and penetration mechanism. Drug Delivery. 2020;27(1):642–651. doi:10.1080/10717544.2020.1754524
105. Zhang Y, Chen L, Li X, Chen J, Tan Z. Tetramethylpyrazine alleviates hypoxia-induced proliferation, migration, and inflammatory response of fibroblast-like synoviocytes via inhibiting the HIF-1α- circCDC42BPB pathway. Adv Rheumatol. 2024;64(1):19. doi:10.1186/s42358-024-00355-1
106. Mei D, Mao S, Sun W, Wang Y, Kissel T. Effect of chitosan structure properties and molecular weight on the intranasal absorption of tetramethylpyrazine phosphate in rats. Eur J Pharm Biopharm. 2008;70(3):874–881. doi:10.1016/j.ejpb.2008.06.031
107. Jiang S, Wan F, Lian H, et al. Friend or foe? The dual role of triptolide in the liver, kidney, and heart. Biomed Pharmacother. 2023;161:114470. doi:10.1016/j.biopha.2023.114470
108. Junghanns J, Müller R. Nanocrystal technology, drug delivery and clinical applications. Int J Nanomed. 2008; 3 (3);295. doi:10.2147/IJN.S595
109. Li J, Wang Z, Zhang H, Gao J, Zheng A. Progress in the development of stabilization strategies for nanocrystal preparations. Drug Delivery. 2021;28(1):19–36. doi:10.1080/10717544.2020.1856224
110. Bonhoeffer B, Kordikowski A, John E, Juhnke M. Numerical modelling of the dissolution of drug nanocrystals and its application to industrial product development. ADMET DMPK. 2022. doi:10.5599/admet.1437
111. Sheng S, Wang X, Liu X, et al. The role of resveratrol on rheumatoid arthritis: from bench to bedside. Front Pharmacol. 2022;13:829677. doi:10.3389/fphar.2022.829677
112. Yang G, Chang -C-C, Yang Y, et al. Resveratrol Alleviates Rheumatoid Arthritis via Reducing ROS and Inflammation, Inhibiting MAPK Signaling Pathways, and Suppressing Angiogenesis. J Agric Food Chem. 2018;66(49):12953–12960. doi:10.1021/acs.jafc.8b05047
113. Bose A, Roy Burman D, Sikdar B, Patra P. Nanomicelles: types, properties and applications in drug delivery. IET Nanobiotechnol. 2021;15(1):19–27. doi:10.1049/nbt2.12018
114. Shah S, Dhawan V, Holm R, Nagarsenker MS, Perrie Y. Liposomes: advancements and innovation in the manufacturing process. Adv Drug Delivery Rev. 2020;154–155:102–122. doi:10.1016/j.addr.2020.07.002
115. Guimarães D, Cavaco-Paulo A, Nogueira E. Design of liposomes as drug delivery system for therapeutic applications. Int J Pharm. 2021;601:120571. doi:10.1016/j.ijpharm.2021.120571
116. Xiong T, Li D, Ren J, et al. Soluble microneedle acupuncture patches containing melittin liposomes for the percutaneous treatment of rheumatoid arthritis. Nanomed Nanotechnol Biol Med. 2025;64:102806. doi:10.1016/j.nano.2025.102806
117. Ansari L, Hallaj S, Hallaj T, Amjadi M. Doped-carbon dots: recent advances in their biosensing, bioimaging and therapy applications. Colloids Surf B. 2021;203:111743. doi:10.1016/j.colsurfb.2021.111743
118. Kaurav H, Verma D, Bansal A, Kapoor DN, Sheth S. Progress in drug delivery and diagnostic applications of carbon dots: a systematic review. Front Chem. 2023;11:1227843. doi:10.3389/fchem.2023.1227843
119. Qi J, Zhang R, Liu X, et al. Carbon Dots as Advanced Drug-Delivery Nanoplatforms for Antiinflammatory, Antibacterial, and Anticancer Applications: a Review. ACS Appl Nano Mater. 2023;6(11):9071–9084. doi:10.1021/acsanm.3c01207
120. Vallorz EL, Janda J, Mansour HM, Schnellmann RG. Kidney targeting of formoterol containing polymeric nanoparticles improves recovery from ischemia reperfusion-induced acute kidney injury in mice. Kidney Int. 2022;102(5):1073–1089. doi:10.1016/j.kint.2022.05.032
121. Thamphiwatana S, Angsantikul P, Escajadillo T, et al. Macrophage-like nanoparticles concurrently absorbing endotoxins and proinflammatory cytokines for sepsis management. Proc Natl Acad Sci USA. 2017;114(43):11488–11493. doi:10.1073/pnas.1714267114
122. Nourshargh S, Alon R. Leukocyte Migration into Inflamed Tissues. Immunity. 2014;41(5):694–707. doi:10.1016/j.immuni.2014.10.008
123. Ma L, Jiang X, Gao J. Revolutionizing rheumatoid arthritis therapy: harnessing cytomembrane biomimetic nanoparticles for novel treatment strategies. Drug Deliv Transl Res. 2025;15(1):66–83. doi:10.1007/s13346-024-01605-x
124. Wang X, Fan D, Cao X, et al. The Role of Reactive Oxygen Species in the Rheumatoid Arthritis-Associated Synovial Microenvironment. Antioxidants. 2022;11(6):1153. doi:10.3390/antiox11061153
125. Kondo N, Kanai T, Okada M. Rheumatoid Arthritis and Reactive Oxygen Species: a Review. CIMB. 2023;45(4):3000–3015. doi:10.3390/cimb45040197
126. Han Z, Gao X, Wang Y, et al. Ultrasmall iron-quercetin metal natural product nanocomplex with antioxidant and macrophage regulation in rheumatoid arthritis. Acta Pharmaceutica Sinica B. 2023;13(4):1726–1739. doi:10.1016/j.apsb.2022.11.020
127. Wang Y, Guo R, Zou M, et al. Combined ROS Sensitive Folate Receptor Targeted Micellar Formulations of Curcumin Effective Against Rheumatoid Arthritis in Rat Model. Int J Nanomed. 2024;19:4217–4234. doi:10.2147/IJN.S458957
128. Chen G, Deng S, Liu S, et al. pH and ROS Dual‐Sensitive Nanocarriers for the Targeted Co‐Delivery and On‐Demand Sequential Release of Tofacitinib and Glucosamine for Synergistic Rheumatoid Arthritis Treatment. Small. 2024;20(24):2308520. doi:10.1002/smll.202308520
129. Xia T, Zhu Y, Li K, et al. Microneedles loaded with cerium-manganese oxide nanoparticles for targeting macrophages in the treatment of rheumatoid arthritis. J Nanobiotechnol. 2024;22(1):103. doi:10.1186/s12951-024-02374-y
130. Hua P, Liang R, Yang S, Tu Y, Chen M. Microneedle-assisted dual delivery of PUMA gene and celastrol for synergistic therapy of rheumatoid arthritis through restoring synovial homeostasis. Bioact Mater. 2024;36:83–95. doi:10.1016/j.bioactmat.2024.02.030
131. Wang X, Cao W, Sun C, Wang Y, Wang M, Wu J. Development of pH-sensitive dextran-based methotrexate nanodrug for rheumatoid arthritis therapy through inhibition of JAK-STAT pathways. Int J Pharm. 2022;622:121874. doi:10.1016/j.ijpharm.2022.121874
132. Agostinis P, Berg K, Cengel KA, et al. Photodynamic therapy of cancer: an update. Ca a Cancer J Clinicians. 2011;61(4):250–281. doi:10.3322/caac.20114
133. Kwiatkowski S, Knap B, Przystupski D, et al. Photodynamic therapy – mechanisms, photosensitizers and combinations. Biomed Pharmacother. 2018;106:1098–1107. doi:10.1016/j.biopha.2018.07.049
134. Yang D, Lei S, Pan K, et al. Application of photodynamic therapy in immune-related diseases. Photodiagn Photodyn Ther. 2021;34:102318. doi:10.1016/j.pdpdt.2021.102318
135. Jo C, Ahn H, Kim JH, et al. Cancer therapy by antibody-targeted Cerenkov light and metabolism-selective photosensitization. J Control Release. 2022;352:25–34. doi:10.1016/j.jconrel.2022.10.014
136. Shi X, Zhang CY, Gao J, Wang Z. Recent advances in photodynamic therapy for cancer and infectious diseases. WIREs Nanomed Nanobiotechnol. 2019;11(5):e1560. doi:10.1002/wnan.1560
137. Sun L, Zhao Y, Peng H, et al. Carbon dots as a novel photosensitizer for photodynamic therapy of cancer and bacterial infectious diseases: recent advances. J Nanobiotechnol. 2024;22(1):210. doi:10.1186/s12951-024-02479-4
138. Richter K, Haslbeck M, Buchner J. The Heat Shock Response: life on the Verge of Death. Molecular Cell. 2010;40(2):253–266. doi:10.1016/j.molcel.2010.10.006
139. Knavel EM, Brace CL. Tumor Ablation: common Modalities and General Practices. Techniques in Vascular and Interventional Radiology. 2013;16(4):192–200. doi:10.1053/j.tvir.2013.08.002
140. Li X, Lovell JF, Yoon J, Chen X. Clinical development and potential of photothermal and photodynamic therapies for cancer. Nat Rev Clin Oncol. 2020;17(11):657–674. doi:10.1038/s41571-020-0410-2
141. Zhi D, Yang T, O’Hagan J, Zhang S, Donnelly RF. Photothermal therapy. J Control Release. 2020;325:52–71. doi:10.1016/j.jconrel.2020.06.032
142. Zhao L, Zhang X, Wang X, Guan X, Zhang W, Ma J. Recent advances in selective photothermal therapy of tumor. J Nanobiotechnol. 2021;19(1):335. doi:10.1186/s12951-021-01080-3
143. Obeng E, Feng J, Wang D, Zheng D, Xiang B, Shen J. Multifunctional phototheranostic agent ZnO@Ag for anti-infection through photothermal/photodynamic therapy. Front Chem. 2022;10:1054739. doi:10.3389/fchem.2022.1054739
144. Wu M, Liu H, Li D, et al. Smart‐Responsive Multifunctional Therapeutic System for Improved Regenerative Microenvironment and Accelerated Bone Regeneration via Mild Photothermal Therapy. Adv Sci. 2024;11(2):2304641. doi:10.1002/advs.202304641
145. Dong Y, Cao W, Cao J. Treatment of rheumatoid arthritis by phototherapy: advances and perspectives. Nanoscale. 2021;13(35):14591–14608. doi:10.1039/D1NR03623H
146. Gallardo-Villagrán M, Leger DY, Liagre B, Therrien B. Photosensitizers Used in the Photodynamic Therapy of Rheumatoid Arthritis. IJMS. 2019;20(13):3339. doi:10.3390/ijms20133339
147. Gadeval A, Chaudhari S, Bollampally SP, et al. Integrated nanomaterials for non-invasive photothermal therapy of rheumatoid arthritis. Drug Discovery Today. 2021;26(10):2315–2328. doi:10.1016/j.drudis.2021.04.026
148. Costa Lima SA, Reis S. Temperature-responsive polymeric nanospheres containing methotrexate and gold nanoparticles: a multi-drug system for theranostic in rheumatoid arthritis. Colloids Surf B. 2015;133:378–387. doi:10.1016/j.colsurfb.2015.04.048
149. Zeng Z, Jiang G, Sun Y, et al. Rational design of flexible microneedles coupled with CaO2 @PDA-loaded nanofiber films for skin wound healing on diabetic rats. Biomater Sci. 2022;10(18):5326–5339. doi:10.1039/D2BM00861K
150. Ding Y, Hong J, Zhang J. A Dissolving microneedle based on metal amino acid/peptide/drug coordination nanoparticles and its preparation method and Application. Chinese Patent, CN119280137A. 2025.
151. Chen PX, Hu ZQ, Jiang XY, Zhu YL, Zhang ML, Yang S. Kgn loaded Nanovesicles, dissolving microneedles and their preparation methods and Applications. Chinese Patent, CN120053685A. 2025.
152. Sun X, Du GS, Zhao YH, Xiong K. A microneedle patch for inducing immune tolerance in the treatment of rheumatoid arthritis. Chinese Patent, CN202310668315. 2023.
153. Chen DQ, Diao NN, Guo CJ, et al. Preparation method of composite microneedle patch for extracellular vesicles of Platycodon grandiflorum. Chinese Patent, CN117224467A. 2023.
154. Wu YM, Chen L, Xiong YA, Zhang YD, Qin Y, Li LC. A dissolving microneedle of magnolol and its preparation method. Chinese Patent, CN115154405A. 2022.
155. Radius Health, Inc. A Study to Evaluate and Compare the Bioequivalence of Two Abaloparatide-sMTS Treatments in Healthy Women. Available from: https://clinicaltrials.gov/study/nct04936984.
156. Radius Health, Inc. Phase 2 Study of BA058 (Abaloparatide) Transdermal Delivery in Postmenopausal Women with Osteoporosis. Available from: https://clinicaltrials.gov/study/nct01674621.
157. Union Hospital, Tongji Medical College. Huazhong University of Science and Technology. A Clinical Study Evaluating the Dermal Safety of Soluble Denosumab Microneedle Patches. Available from: https://clinicaltrials.gov/study/nct07085520.
158. Centre for Human Drug Research, Netherlands. Adalimumab Microneedles in Healthy Volunteers. Available from: https://clinicaltrials.gov/study/nct03607903.
159. Advaccine Biopharmaceuticals Suzhou Co. Ltd. Dissolvable Microneedle Blemish Patches (Salicylic Acid 5 Mg/1000 Mg). U.S. FDA National Drug Code Directory. NDC Package Code: 84895-102-06. Start Marketing Date: 2025 Oct 16. Available from: https://www.accessdata.fda.gov/scripts/cder/ndc/dsp_searchresult.cfm.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Multifunctional Nano-Delivery System Against Rheumatoid Arthritis by Combined Phototherapy, Hypoxia-Activated Chemotherapy, and RNA Interference

Li X, Zhang S, Zhang M, Li G, Yang B, Lu X, Teng L, Li Y, Sun F
International Journal of Nanomedicine 2022, 17:6257-6273
Published Date: 10 December 2022