Back to Journals » Journal of Blood Medicine » Volume 16
Moving Toward Collecting High-Quality Umbilical Cord Blood: Application of Quality Control Circle
Authors Peng J, Shi CY ![]() , Kuang FY, Ma TB, Yu XB
, Kuang FY, Ma TB, Yu XB
Received 3 July 2025
Accepted for publication 19 November 2025
Published 6 December 2025 Volume 2025:16 Pages 589—599
DOI https://doi.org/10.2147/JBM.S550641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Jun Peng,1,2,* Cong-Ying Shi,3,* Fa-Ying Kuang,2 Tian-Bao Ma,3 Xi-Bao Yu3
1Department of Gynecology and Obstetrics, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Gynecology and Obstetrics, Zengcheng Branch of Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Guangdong Cord Blood Bank, Guangdong Women and Children Hospital, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Cong-Ying Shi, Department of Guangdong Cord Blood Bank, Guangdong Women and Children Hospital, Guangzhou, Guangdong, People’s Republic of China, Tel +86 13416131816, Email [email protected]
Purpose: All umbilical cord blood (UCB) used for hematopoietic cell transplantation (HCT) must pass through a series of strict tests, including volume, total nucleated cell count, microbial contamination, hematopoietic stem cells content, and activity. A strictly standardizing collection procedures for UCB within hospitals is a critical step in preserving hematopoietic stem cells resources.
Methods: The study included a total of 560 participants, with 337 in the control group and 223 in the observation group, collected from January 2022 to December 2024. Participants were randomly assigned to two groups. The UCB collected from newborns before the initiation of Quality Control Circle (QCC) activities served as the control group, whereas those collected after the initiation of QCC activities formed the observation group. Through the establishment of QCC nursing management, the reasons for UCB storage failures within the department were analyzed, and corresponding countermeasures were formulated. Statistical analyses were performed to compare the reasons for failure of UCB storage, success rate, and quality indicators of successfully stored UCB between the two groups.
Results: There were no statistically significant differences in the general clinical data of the newborns between the two groups. After the implementation of QCC activities, the rate of successfully stored UCB samples in the observation group was 90.6%, which was significantly higher than that of 84.3% in the control group (P=0.031). There were no statistically significant differences in the quality indicators of successfully stored UCB between the two groups.
Conclusion: The implementation of QCC in UCB collection increased the success rate by 6.3 percentage points without compromising cellular quality, supporting its application as a continuous improvement strategy in obstetric settings.
Keywords: blood banking, hematopoietic stem cells, quality improvement, umbilical cord blood
Introduction
Umbilical cord blood (UCB) contains many special types of stem cells,1 among which hematopoietic stem cells (HSCs) are more primitive and abundant than those found in the bone marrow. The advantages of UCB HSCs include wide availability and simple collection, making them an important third source of HSCs after bone marrow and peripheral blood.2,3 Allogeneic hematopoietic stem cell transplantation (HCT) is an effective and curative therapy for various types of malignancies, non-malignancies, hematological disorders, congenital conditions, and metabolic diseases.4 Unfortunately, the preferred option that a fully matched related donor is not always available for most patients (about 70%).5 In China, due to the implementation of the one-child policy in the past, such matching donors have become even scarcer. Searching for matching unrelated donors through the registration system is also very difficult and time-consuming. This has led to significant development of umbilical cord blood hematopoietic stem cell transplantation in China over the past 30 years. Research has shown that by 2018, the public bank of Guangdong Cord Blood Bank had released 1350 units of UCB for the treatment of various diseases, especially HCT.6 As of May 2024, this number has been updated to 4877 units. For the private bank, the number of umbilical cord blood applications has also reached 499 units, covering various fields such as blood diseases, cerebral palsy, diabetes, and more. These data demonstrating significant medical value of UCB.
The process of collecting and delivering UCB to the hospital involves several steps, during which there is a risk of microbial contamination and loss of activity in the HSCs. Because all UCB used for HCT must pass through a series of strict tests, including volume, microbial contamination, HSC content, and activity, UCB that do not meet the storage standards will be discarded, leading to a waste of HSCs resources.7 Therefore, strictly standardizing collection procedures for UCB within hospitals is a critical step in preserving HSCs resources.
The Quality Control Circle (QCC) was firstly employed in business management and company operation, refers to effective quality control and proactive activities aimed at addressing issues related to corporate strategy, policies, and problems in various positions, with the goal of improve the work flow and eventually solve the problems.8 The main feature of the QCC is the continuous improvement in quality, which targets a series of existing issues.9 With China’s rapid economic development and ongoing healthcare reforms, there is an urgent need for improvement.10 Continuous quality improvement management can be achieved through QCC. In these activities, circle members spontaneously identify weaknesses at work and implement effective countermeasures based on actual situations. All circle members must participate in specific management tasks, continuously improving overall quality management levels. QCC is increasingly being applied in nursing, with impressive results.11 After childbirth, many nursing tasks are performed in the operating room and quality management can be challenging. UCB collection requires a high level of professionalism from nurses, and post-collection assistance from mothers, obstetricians, operating room nurses, and cord blood bank staff is necessary to ensure that the collected UCB meets the storage criteria of the cord blood bank. This study hypothesized that the QCC activities implemented during the UCB collection workflow would also be beneficial in improving the success rate of high-quality UCB collection.
Materials and Methods
Setting and Sample
Pregnant women who delivered at the Obstetrics Department of Nanfang Hospital Zengcheng campus, Southern Medical University, Guangzhou, according to the inclusion and exclusion criteria. The period of data collection and analysis was from January 2022 to December 2024. The inclusion Criteria were: (1) maternal age between 18 and 45 years. (2) Signed informed consent for UCB collection. (3) Complete maternal information records. The exclusion Criteria were as follows: (1) high-risk pregnant women deemed unsuitable for UCB collection during surgery, as assessed by a doctor prenatally. Secondary exclusion criteria: (1) many or foreign objects present in the collected UCB. (2) Incomplete filling out of the cord blood collection information form. (3) Contamination with UCB during laboratory processing. No QCC activity was proceeded in the control group. The observation group conducted QCC activities with the following specific contents. Before being admitted to the hospital, the parturients were randomly assigned to these two groups according to the proportion through a software-based randomization method. Due to the UCB volume, total nucleated cell count (TNC) and CD34+ cell levels exhibit substantial inter-individual variability influenced by maternal physiological factors.12 The criteria for UCB storage success were as follows: (1) Successful collection of UCB; (2) Timely transportation of the UCB to the Guangdong Umbilical Cord Blood Bank within 24 hours; (3) The UCB was not polluted by viral or bacterial; (4) The TNC was not extremely low (TNC>1*108), meeting the minimum threshold for priviate bank storage. All data collection was conducted with the consent of the pregnant women who signed informed consent forms. General clinical data such as newborn sex, premature birth weight, blood type, and transfer to the neonatal department were recorded and organized.
An internal investigation of Guangdong Cord Blood Bank prior to this study found that the storage success rate of UCB for private bank was.83. Based on our experience, we hypothesized that QCC implementation would increase this rate to 0.93. Set a two sides Cronbach’s α =0.05, and the degree of assurance (1-β) is.9. The sample size ratio between the observation group and the control group was 1:1.5, and the Superiority Margin was 0. Using the 2-Sample Non-Inferiority or Superiority test, the sample size of the control group should be more than 291 cases and the sample size of the observation group should be more than 194 cases.
Study Design
Establishment of the QCC Group
Experienced medical personnel and laboratory technicians were selected from the obstetrics department of the Nanfang Hospital Zengcheng Campus and Guangdong Cord Blood Bank to form the QCC group. Ultimately, the QCC group consisted of 10 medical personnel, including 2 physicians, 7 nurses, and 1 staff member from the Guangdong Cord Blood Bank. The head nurse served as the mentor responsible for guiding and coordinating QCC activities. A senior nurse with strong professional skills was appointed as the circle leader, responsible for organizing group discussions, overall planning, and ensuring the quality of activities. The remaining 8 members were responsible for implementing these activities. All members worked together, following the Plan-Do-Check-Act (PDCA) cycle principle, using brainstorming methods to identify root causes and formulate implementation strategies. The slogan of the QCC group was as follows: “Improve the success rate of high-quality UCB collection”. After the group was established, a series of QCC training sessions were organized, covering basic concepts of QCC, commonly used tools, problem-solving methods, etc., to ensure that all group members acquired the necessary knowledge and skills related to QCC.
Determination of the Theme
The QCC group analyzed the factors affecting the success rate of high-quality UCB collection and selected the activity theme “Improving the Success Rate of High-Quality UCB Collection”. The theme aligns with the 5M criteria for QCC topic selection, which are Manageable: Within the group’s capabilities. Measurable: Outcomes were quantified. Moderate Duration: The project can be completed within a reasonable timeframe. Management Appreciation: This theme is recognized and supported by management. Members Pride: This theme instills a sense of pride among the group members.
Cause Analysis
Using the 5W1H management tool, the QCC group conducted brainstorming meetings and mutual communication to familiarize themselves with the entire UCB collection and transportation processes. This includes signing informed consent for UCB collection before delivery, disinfection and collection of UCB after delivery, short-term storage of UCB within the hospital, and handover of UCB to the Guangdong Cord Blood Bank staff. Based on the existing workflow and actual conditions, an analysis fishbone diagram is created (Figure 1). Each cause was analyzed to exclude non-primary factors, followed by the exclusion of uncontrollable factors. Ultimately, the processes imperfection was determined as the primary influencing factor. The main reasons for the failure of high-quality UCB collection before the initiation of QCC are summarized (Figure 2).
 |
Figure 1 Fishbone diagram. |
 |
Figure 2 Quality of care deficiencies in project plato. |
Implementation of QCC Countermeasures
To enhance the comprehensive system for UCB collection and storage in clinical departments, Standard Operating Procedures were developed and integrated into training programs to standardize and refine the work process. This improves the cultural and professional competencies of the nursing staff and enhances communication with pregnant women and their families. The question “Do you wish to retain the umbilical cord blood?” is now a mandatory inquiry during patient admission, transfer to the labor room, and transfer to the operating theatre. This ensures mutual reminders and confirmation of the UCB retention at each stage. Upon admission, the patient wished to retain the UCB and the collection bag was prepared. Before entering the labor room or operating theatre for a caesarean section, proper handovers are conducted. Additionally, reminder labels are added for patients who decide to retain umbilical cord blood, with a prominent label placed on their medical records and a wristband provided to indicate UCB collection. To enhance standardized umbilical cord disinfection and comprehensive training for UCB collection, training on standardized UCB disinfection3,13 and the entire process of UCB collection is strengthened. This reinforces the sense of responsibility among the staff and regularly promotes the medical value of UCB. Training sessions were held every two weeks to ensure that all staff were familiar with the UCB collection process, standardized collection steps, and proper disinfection methods. The 5M cultural elements (manageable, measurable, moderate duration, management appreciation, and members’ pride) are integrated into training and learning to foster self-awareness, enthusiasm, and proactivity among nursing staff. To prevent collection bag quality issues, backup UCB collection bags were placed in the labor room and the operating theatre.
Regular Monitoring of Nursing Quality
Every two weeks, issues in nursing work, process improvements, service attitudes, and the application of nursing forms and procedures were summarized and discussed. Subsequently, the processes are redesigned and redefined according to the PDCA cycle. Deputy chief nurses intensify the evaluation of nursing staff, requiring them to strictly adhere to operational procedures. These requirements were incorporated into daily performance evaluation systems.
Laboratory Quality Control
Blood samples were processed in a certified laboratory (AABB, ISO9001 accredited) with a comprehensive quality control system. The laboratory maintains a robust quality management framework including: (1) daily internal quality control with at least two control rules for all equipment; (2) semi-annual internal proficiency testing for all analytical equipment; (3) biennial external proficiency testing through the National Center for Clinical Laboratory, National Health Commission of the People`s Republic of China (NCCL EQA Certificate); (4) quarterly professional maintenance of all equipment by certified engineers; and (5) annual equipment calibration with traceable standards.
Data Collection
The reasons for failure and success rates in the collection of high-quality UCB by the nursing staff before and after implementation were compared. The quality indicators of successfully collected and stored UCB before and after implementation were compared, including UCB volume, TNC, and CD34+ content. In this study, all collected UCB were transported to the Guangdong Cord Blood Bank for quality testing and subsequent processing.
UCB Volume and TNC: Upon arrival at the Guangdong Cord Blood Bank, paper records were double-checked, and the blood bags were weighed to determine the cord blood volume. One milliliter of UCB was analyzed using an automatic blood cell analyzer (Sysmex XE-5000, Japan) to calculate TNC.
Bacterial Contamination: In a Class 10,000 cleanroom, 10 mL of plasma separated from UCB via centrifugation was inoculated into both aerobic and anaerobic blood culture bottles. These were then incubated for seven days using an automated bacterial culture system to detect any aerobic or anaerobic bacterial contamination.
CD34+ Cell Content: CD34 is a transmembrane glycoprotein that is specifically expressed on immature hematopoietic stem and progenitor cells, but not in mature blood cells. It serves as a critical marker for assessing the transplantation potential of UCB HSCs.13 In this study, a flow cytometer (FACSCalibur, BD Biosciences) was used to quantify the CD34+ cells in the UCB samples. This was achieved using monoclonal antibodies directed against the common leukocyte antigens, CD45 and CD34.
Data Analysis
Statistical analyses were performed using SPSS version 26.0. Categorical data are presented as n (%) and were analyzed using the chi-square test for two independent samples. Continuous variables are expressed as mean ± standard deviation ( ±s) and were compared between the two groups using an independent samples t-test. Multivariate logistic regression was used to assess the risk factors for the primary outcome. The continuous variables were determined to follow a normal distribution through the histogram analysis. Confidence intervals were set at 95.0%. Statistical significance was set P <0.05.
±s) and were compared between the two groups using an independent samples t-test. Multivariate logistic regression was used to assess the risk factors for the primary outcome. The continuous variables were determined to follow a normal distribution through the histogram analysis. Confidence intervals were set at 95.0%. Statistical significance was set P <0.05.
Ethical Consideration
The ethics committee of GDCBB approved this study (Ethical number: IRB-2024001). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised most recently in 2013. All participants had provided their written informed consent to this study. The study data did not involve information that could identify individual participants.
Results
General Clinical Data of Newborns Between Two Groups
A total of 590 parturients were recruited, and 560 parturients were finally analysed because of partial data loss. A total of 337 parturients were included in the control group and 223 parturients were included in the observation group. Flow diagram is shown in Figure 3. The general clinical data of the newborns in the two groups are shown in Table 1. There were no statistically significant differences between the two groups in terms of sex, prematurity, transfer to the neonatology department, or birth weight (P >0.05).
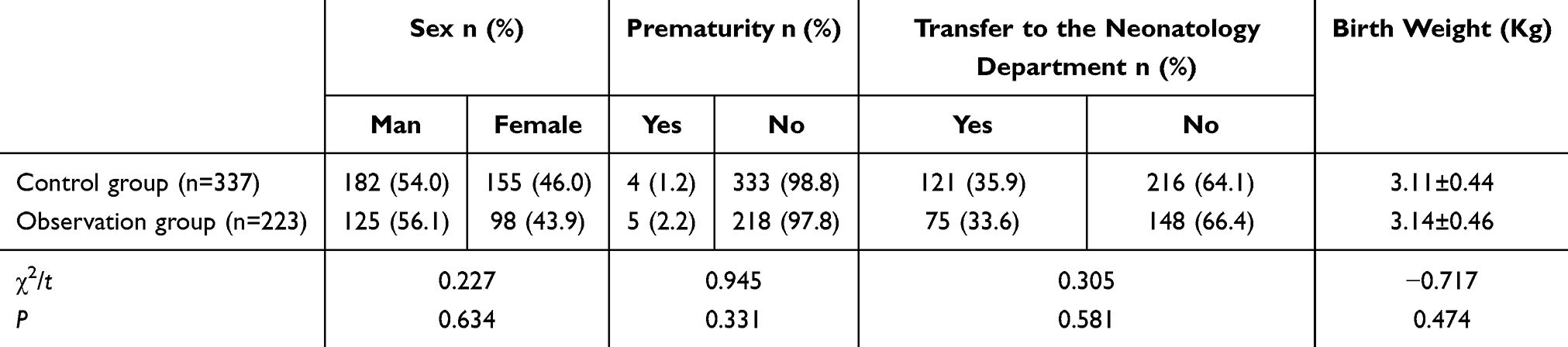 |
Table 1 General Clinical Data of Newborns Between Two Groups |
 |
Figure 3 Flow diagram. |
Comparison of UCB Storage Between the Two Groups
The comparison of UCB storage for these two groups are shown in Table 2. The reasons for storage failure of Control group were: 34 cases of collection failure in 53 cases (64.2%), low cell count 5 cases (9.4%), and viral or bacterial pollution 14 cases (26.4%). The reasons for storage failure of observation group were: 17 cases of collection failure in 21 cases (81.0%), low cell count 1 case (4.8%), and viral or bacterial pollution 3 cases (14.3%). After the implementation of QCC, the storage failure rate decreased to 9.4%. The storage success rate was significantly higher in the QCC group (90.6% vs 84.3%, RR=0.091, 95% CI: 0.035-0.043, P =0.031). We also employed multivariate logistic regression to assess the risk factors influencing the success of UCB storage. UCB storage success was regarded as the dependent variable, while whether QCC implementation was considered as the main exposure. All confounding factors were input as continuous or categorical predictors. After adjusting for all confounders, the QCC intervention remains significantly associated with increased UCB storage success (OR=2.091, 95% CI: 1.172–3.732, P =0.013).
 |
Table 2 Comparison of Umbilical Cord Blood Storage Between the Two Groups |
Comparison of Quality Indicators of Successfully Stored UCB Between the Two Groups
A comparison of the quality indicators for successfully stored UCB between the two groups is presented in Table 3. There were no statistically significant differences in the UCB volume, TNC, or CD34+ cell content between the two groups (Control group vs Observation group: UCB volume 95% Cl: 51.33–56.51 vs 52.03–59.22, P >0.05; TNC 95 Cl: 6.21–7.02 vs 6.03–6.93, P >0.05; CD34+ cell content 95% Cl: 0.28-0.33 vs. 0.28-0.33, P >0.05).
 |
Table 3 The Comparison of Quality Indicators for Successfully Stored Umbilical Cord Blood Between the Two Groups |
Discussion
In this study, UCB samples were prepared and tested by the Guangdong Cord Blood Bank, which has a cleanroom facility compliant with the College of American Pathologists interlaboratory quality assessment standards, is accredited by the Association for the Advancement of Blood & Biotherapies, and is certified under the ISO9001 quality management system. Cord blood was collected using a triple-bag system to ensure that it remained isolated from the external environment during processing. Cord blood samples were prepared and separated under sterile conditions. The results of our research showed that, after implementing QCC activities, the success rate of UCB collection in our department statistically increased from 84.3% to 90.6% (P =0.031). There was no statistically significant difference in the general clinical data of the newborns between the two groups (P >0.05). There was also no statistically significant difference (P >0.05) when comparing the quality indicators of the UCB that was successfully stored between the two groups. This suggests that implementing QCC activities can increase the success rate of high-quality UCB collection without affecting the quality of UCB, making it suitable for application in clinical work.
QCC are activities that require full participation from all members, where brainstorming is used to propose high-quality work methods from each individual’s perspective on their job, aiming to solve difficulties encountered in the workplace.14 The QCC reduces human error through two interconnected mechanisms: (1) fostering a proactive safety culture that transforms error reporting from punitive to preventive, and (2) bringing in standardized workflow with real-time feedback. First, QCC reduce individual subjective errors through established procedures and systems. Second, during the QCC process, the workflow is dynamically adjusted through real-time group meetings for discussion. To be specific, after a series of QCC group activities within the gynecology and obstetrics departments, several issues in the UCB collection process were identified. ① There is a lack of effective management of surgical instruments such as UCB collection bags and disposable needles, and items are not properly placed in designated locations.10 Effective management of medical supplies is crucial for successful collection of high-quality UCB. ② Refrigerators storing UCB lack labels, leading to the incorrect placement of collected samples or forgetting to return them to a designated refrigerator. ③ UCB collection procedures are incomplete and there is a lack of training in these procedures. ④ The skill levels of nursing staff in the UCB collection varied widely. ⑤ Disinfection procedures for the umbilical cord before collection are not standardized,11 and a standardized operating procedure must be established. ⑥There is a lack of verification steps to ensure that the UCB must be collected or that the collected samples are returned to the designated location. ⑦There is insufficient communication and coordination among departments and institutions, and staff members lack clear awareness of responsibility. During the UCB collection process, they completed the assigned tasks without showing any initiative or teamwork. ⑧Effective communication and handover processes are lacking between healthcare providers and Guangdong Cord Blood Bank staff before and after the collection. To address these issues, the QCC group members took a series of measures and conducted timely reflections. This effectively enhances every nursing staff member’s sense of involvement in the activity, while respecting everyone is viewpoints throughout the process.15 All participating nurses felt a sense of satisfaction and accomplishment from managing their work environment in an enjoyable manner. Nurses at all levels were included in the discussions, forming an interactive model that fosters vertical collaboration. This allows all nursing staff to see different hierarchical views on the same problems and measures taken to resolve them, stimulating their initiative to participate and actively share. It also enables nursing management to understand the thoughts of nursing staff and to guide and invigorate them, thereby strengthening the cooperative spirit among all members of the department, improving work efficiency, and enhancing overall management capabilities. After implementing the QCC activities in this research, we identified issues in the collection of UCB and used brainstorming to develop detailed measures for UCB collection. We refined the process from UCB collection to handover to the Guangdong Cord Blood Bank and incorporated this process into the standardization. The head nurse supervised, evaluated, and continuously improved the UCB collection work based on these standards. Nurses in the QCC group inspired each other and reflected on the issues present in the UCB collection. Under the leadership of the team leader, solutions were developed to address the problems that arose, thereby significantly improving work efficiency. While reducing overall oversights in the UCB collection process,16 the team’s collaborative abilities also improved.
Since the first transplantations of UCB in 1988, over 40000 UCB transplantations has been performed, and over half of the patients have been cured with this technique.17 Allogeneic HCT is of vital importance in the treatment of hematological malignancies. These tumors may also cause some complications, such as infections and endothelial injury syndrome.18 Therefore, a high-quality umbilical cord blood hematopoietic stem cell is extremely important. With the advancement of regenerative medicine, UCB is not only applicable for HCT but also for the regeneration and repair of damaged nerves.19 With the declining birth rate in China, UCB has become a valuable therapeutic resource. The collection of UCB from consenting mothers has become a routine part of obstetric research. The quality of UCB is directly influenced by the effectiveness of the UCB collection technique, which in turn affects the potential clinical application of HSCs therapy. The TNC count and CD34+ cell content in UCB represent critical parameters prioritized by clinicians for HCT and regenerative medicine applications.20,21 However, these metrics are based on the premise that all UCB units of the banks must first meet strict entry criteria. Both TNC and CD34+ cell levels exhibit substantial inter-individual variability influenced by maternal physiological factors.12 Some studies have indicated that the total bacterial pollution rate in cord blood ranges from 6% to 10.3%, and contamination is primarily associated with poor collection techniques, inadequate staff training, and vaginal delivery, leading to exposure to the gut and vaginal microbiota.22–24 Therefore, in UCB collection protocols, obstetricians and midwives primarily focus on standardizing procedural practices to maintain TNC and CD34+ cell concentrations within acceptable ranges around population means while simultaneously minimizing the risk of storage failure caused by various reasons. A few studies have explored the factors influencing the quality of UCB25 and methods for improving the collection of umbilical cord blood.26 However, very few studies have focused on how to enhance the success rate of umbilical cord blood storage from the perspective of healthcare administrators. To the best of our knowledge, this study demonstrated the first implementation QCC methodology in UCB collection workflows, significantly increased the success rate of Storage.
The QCC workflow of the research exhibits a certain degree of operability and influence. Nationally, it adheres to the technical guidelines for UCB banks in China. Internationally, it also complies with the AABB’s technical guidelines. On this basis, the research further refines the work within two time - windows: one is the period after the parturient is admitted to the hospital’s obstetrics department but before delivery, and the other is the period after UCB collection but before it is transported to the UCB bank. Based on the QCC management system, it can be replicated and implemented at a relatively low cost in an environment with limited resources, which is conducive to increasing the global cord blood inventory.
This study has certain limitations. First, it was conducted in a single hospital, and future research could expand to include more hospitals to enhance generalizability. Second, several confounding factors, such as mode of delivery and the clamping timing of UCB collection, were not included in the analysis. These factors may influence the quality of UCB and the success rate of collection. Third, while the study mentions that strict disinfection and procedural protocols reduced the risk of microbial contamination, UCB contamination could still occur from either intrauterine or extrauterine infections. Futhur study can focus on the potential operational variations in different country, to discuss a suitable workflow to improve UCB collection of their own region.
Conclusion
The implementation of QCC in UCB collection increased the success rate by 6.3 percentage points without compromising cellular quality, supporting its application as a continuous improvement strategy in obstetric settings. Given the potential variations in operational challenges faced by healthcare institutions across different regions, future research could prioritize investigating these contextual disparities to develop targeted quality improvement frameworks.
Data Sharing Statement
The data generated and analyzed in this study are not publicly available but may be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the Guangdong Cord Blood Bank, Guangzhou, Guangdong (Ethical number: IRB-2024001).
Acknowledgments
We would like to thank all the doctors and nurses of the Nanfang Hospital Zengcheng Campus Obstetrics Department who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research is supported by Guangzhou Science and Technology Program Projects (ID: 202103000002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. American College of Nurse-Midwives, Cord blood banking. J Midwifery Womens Health. 2022;67(5):673–674. doi:10.1111/jmwh.13345
2. Zhu X, Tang B, Sun Z. Umbilical cord blood transplantation: still growing and improving. Stem Cells Transl Med. 2021;10 Suppl 2(S2):S62–S74. doi:10.1002/sctm.20-0495
3. Devi S, Bongale AM, Tefera MA, Dixit P, Bhanap P. Fresh umbilical cord blood-A source of multipotent stem cells, collection, banking, cryopreservation, and ethical concerns. Life. 2023;13(9). doi:10.3390/life13091794
4. Passweg JR, Baldomero H, Bader P, et al. Hematopoietic stem cell transplantation in Europe 2014: more than 40 000 transplants annually. Bone Marrow Transplant. 2016;51(6):786–792. doi:10.1038/bmt.2016.20
5. Gragert L, Eapen M, Williams E, et al. HLA match likelihoods for hematopoietic stem-cell grafts in the US registry. N Engl J Med. 2014;371(4):339–348. doi:10.1056/NEJMsa1311707
6. Shi CY, Wei W, Lyu LJ, Wang Q. Umbilical cord blood application analysis of Guangdong cord blood bank. Chin Med J. 2020;133(16):1997–1998. doi:10.1097/CM9.0000000000000924
7. Navarrete C, Contreras M. Cord blood banking: a historical perspective. Br J Haematol. 2009;147(2):236–245. doi:10.1111/j.1365-2141.2009.07827.x
8. Zhu YT, Jiang YX, Pei L, Zhu WC, Jin XG. Application of quality control circle in the management of early ambulation after cesarean section: an observational study. Medicine. 2024;103(14):e37633. doi:10.1097/MD.0000000000037633
9. Lake S, Kerr T, Buxton J, et al. Does cannabis use modify the effect of post-traumatic stress disorder on severe depression and suicidal ideation? Evidence from a population-based cross-sectional study of Canadians. J Psychopharmacol. 2020;34(2):181–188. doi:10.1177/0269881119882806
10. Yu J, Qi R, Wang W, Jiang G, Liu Y, Zhang W. Effect of quality control circle on nursing in orthopaedic trauma surgery. Am J Transl Res. 2022;14(6):4380–4387.
11. Zhao H, Hu M, Cao Y, Wu X, Zhu F. Study on the application of quality control circle activity in postoperative nursing of elderly dental implants. Medicine. 2024;103(2):e36894. doi:10.1097/MD.0000000000036894
12. Faivre L, Couzin C, Boucher H, et al. Associated factors of umbilical cord blood collection quality. Transfusion. 2018;58(2):520–531. doi:10.1111/trf.14447
13. Mousavi SH, Zarrabi M, Abroun S, Ahmadipanah M, Abbaspanah B. Umbilical cord blood quality and quantity: collection up to transplantation. Asian J Transfus Sci. 2019;13(2):79–89. doi:10.4103/ajts.AJTS_124_18
14. Wang Y, Lai Y, Du L, Shen W. Impact of quality control circle on patient outcomes after hepatocellular carcinoma intervention: a meta-analysis. Expert Rev Anticancer Ther. 2023;23(8):875–882. doi:10.1080/14737140.2023.2219899
15. Liu W, Guo J, Jiang Q, et al. Quality control circle practices to improve mask-wearing compliance by patients diagnosed with tuberculosis during external examinations. Patient Prefer Adherence. 2024;18:227–237. doi:10.2147/PPA.S445632
16. Wang H, Zhou XM, Xu WD, et al. Inhibition of elevated hippocampal CD24 reduces neurogenesis in mice with traumatic brain injury. J Surg Res. 2020;245:321–329. doi:10.1016/j.jss.2019.07.082
17. Ballen K. Update on umbilical cord blood transplantation. F1000Res. 2017;6:1556. doi:10.12688/f1000research.11952.1
18. Paschalis Evangelidis EG, Tsakiris DA, Tsakiris DA. Thrombotic complications after hematopoietic stem cell transplantation and other cellular therapies. Thrombosis Update. 2024;16:100186. doi:10.1016/j.tru.2024.100186
19. Paton MCB, Wall DA, Elwood N, et al. Safety of allogeneic umbilical cord blood infusions for the treatment of neurological conditions: a systematic review of clinical studies. Cytotherapy. 2022;24(1):2–9. doi:10.1016/j.jcyt.2021.07.001
20. Sanchez-Petitto G, Rezvani K, Daher M, et al. Umbilical cord blood transplantation: connecting its origin to its future. Stem Cells Transl Med. 2023;12(2):55–71. doi:10.1093/stcltm/szac086
21. Sun Z, Hu Y, Ji Y, et al. Refining eligibility criteria of unit selection for myeloablative cord blood transplantation in acute leukemia: real-world experience of a referral center. EJHaem. 2023;4(2):470–475. doi:10.1002/jha2.703
22. Bianchi M, Orlando N, Barbagallo O, et al. Allogeneic cord blood red blood cells: assessing cord blood unit fractionation and validation. Blood Transfus. 2021;19(5):435–444. doi:10.2450/2020.0138-20
23. Bello-Lopez JM, Nogueron-Silva J, Castaneda-Sanchez JI, Rojo-Medina J. Molecular characterization of microbial contaminants isolated from umbilical cord blood units for transplant. Braz J Infect Dis. 2015;19(6):571–577. doi:10.1016/j.bjid.2015.07.005
24. Cundell T, Atkins JW, Lau AF. Sterility testing for hematopoietic stem cells. J Clin Microbiol. 2023;61(3):e0165422. doi:10.1128/jcm.01654-22
25. Jawdat D, Arab S, Thahery H, Almashaqbeh W, Alaskar A, Hajeer AH. Improving cord blood unit quantity and quality at King Abdullah international medical research center cord blood bank. Transfusion. 2014;54(12):3127–3130. doi:10.1111/trf.12746
26. Shi C, Rao W, Huang W, Ma T, Wei W. Effect of cord blood double collection method on cord blood hematopoietic stem cell transplantation-related indices and blood gas analysis. Medicine. 2023;102(47):e36227. doi:10.1097/MD.0000000000036227
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.