Back to Journals » International Medical Case Reports Journal » Volume 18
Moving Through Genetic Alterations and PD-L1 Expression in High-Grade Fetal Adenocarcinoma of the Lung: A Case Report and Literature Review
Authors Xu Y ![]() , Dai K, Chen W, Wu H, Lin P
, Dai K, Chen W, Wu H, Lin P ![]()
Received 19 July 2025
Accepted for publication 13 November 2025
Published 3 December 2025 Volume 2025:18 Pages 1519—1526
DOI https://doi.org/10.2147/IMCRJ.S554848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
YunQiu Xu, KangJian Dai, Wei Chen, Haifan Wu, Peifeng Lin
Department of Cardiothoracic Surgery, Ruian People’s Hospital, The Third Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China
Correspondence: Peifeng Lin, Email [email protected]
Background: Lung cancer, the most common malignancy in humans, can be classified into a wide range of subtypes and molecular variants. Fetal adenocarcinoma of the lung (FLAC) is an infrequent subtype of lung adenocarcinoma with distinct histological characteristics. However, its incidence is extremely low (0.1– 0.5% of primary lung cancers), and its biological features remain poorly understood. In the era of immunotherapy and targeted therapy, characterizing the genetic alterations of FLAC is essential for developing personalized treatment strategies and improving patient outcomes. Here, we report the genetic alterations and PD-L1 expression in a patient with high-grade FLAC (H-FLAC) and review the relevant literature, This is one of the few reported cases describing PD-L1 expression and TP53 mutation status in H-FLAC.
Case Manifestations: A 57-year-old man with a 30-year history of smoking presented to our hospital with persistent cough, sputum, and chest tightness for 30 years, which had worsened for 1 month. Computed tomography (CT) of the chest revealed an irregular nodule in the posterior segment of the upper lobe of the left lung. The patient underwent posterior resection of the left upper lung apex, and postoperative pathology suggested H-FLAC with a tumor stage of pT1N0M0.
Conclusion: This case study provides an opportunity to better understand H-FLAC, whose genetic alterations have not been well characterized, and to identify valuable molecular markers for potential targeted therapies. We conducted gene sequencing and PD-L1 expression testing, which are helpful for H-FLAC research.
Keywords: fetal adenocarcinoma of the lung, programmed death ligand-1, genetic variant, TP53
Introduction
Lung cancers are highly heterogeneous and are usually categorized as small-cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). NSCLC accounts for approximately 85% of all lung cancer cases, making it the predominant subtype worldwide.1 The global incidence remains high and the disease remains the leading cause of cancer-related mortality.2 Established risk factors for NSCLC include tobacco smoking (the single most important factor), second-hand smoke exposure, occupational exposures (such as asbestos, arsenic, chromium), radon, air pollution, and familial/genetic susceptibility.3
Treatment of NSCLC is guided by disease stage and patient fitness. Early-stage disease is managed primarily with surgical resection, while radiotherapy, systemic chemotherapy, immunotherapy and targeted therapies play key roles in locally advanced or metastatic settings.1 The identification of actionable molecular alterations and immune checkpoint biomarkers has significantly improved survival outcomes for specific patient subgroups.
Within this context, the subtype of high-grade fetal adenocarcinoma of the lung presents an unique molecular characteristics. Fetal adenocarcinoma of the lung (FLAC), classified as a unique subtype of adenocarcinoma, accounts for only 0.1–0.5% of lung malignancies.4,5 FLAC was initially reported and identified in 1982 because it resembles the airway epithelium of the fetal lung at 10–16 weeks.6,7 In 2011, the International Multidisciplinary Classification of Lung Adenocarcinoma (IASLC/ATS/ERS) classified FLAC as an independent variant of invasive lung adenocarcinoma. In 2015, it was further classified as a distinct entity of lung adenocarcinoma according to the World Health Organization classification of lung cancer, 4th edition.8,9
FLACs are histologically classified as low-grade (L-FLAC) or high-grade (H-FLAC) subtypes based on the differentiation and atypia of cancer cells. It should be noted that these terms refer to histological grades rather than tumor differentiation status. L-FLAC generally shows a favorable prognosis, with a 5-year survival rate exceeding 80%. In contrast, H-FLAC is often diagnosed at an advanced stage and usually requires postoperative adjuvant chemotherapy. L-FLAC usually occurs in nonsmoking women, whereas H-FLAC is more common in elderly men with a history of heavy smoking. Microscopically, L-FLAC shows low mitotic activity and slow growth, whereas H-FLAC displays marked nuclear atypia, frequent mitoses, and extensive necrosis. About 80–100% of H-FLAC cases occur in combination with conventional lung adenocarcinoma (CLA), large cell neuroendocrine carcinoma (LCNEC), or intestinal adenocarcinoma.10–12
With the rapid development of immunotherapy in recent years, identifying reliable immunotherapeutic biomarkers for individual malignancies is necessary and challenging. Tumor program death ligand-1 (PD-L1) assessment is widely used to predict the therapeutic responsiveness of immune checkpoint inhibitors (ICI). However, the molecular characteristics and immune microenvironment of H-FLAC remain poorly understood. In particular, data on PD-L1 expression and genetic alterations such as TP53 mutation are limited, yet they may have important therapeutic implications. Here, we report a case of a patient with early stage H-FLAC who underwent radical resection of the malignancy. Next-generation sequencing (NGS) and PD-L1 immunostaining assays were performed to determine the PD-L1 status and further explore other potential valuable biomarkers of H-FLAC.
Case Presentation
In November 2023, a 57-year-old man with a 30-year history of smoking (approximately 40 cigarettes/day) and never quit, was admitted to the hospital with recurrent cough, sputum, and chest tightness for 30 years, due to moderate chronic obstructive pulmonary disease (COPD), likely with long-standing chronic bronchitis. Worsening of cough persisted for one month, probably related to upper respiratory infection. The patient had no history for hypertension, diabetes mellitus, as well as no family history of malignancy. There was no history of regular home medications prior to admission. Contrast-enhanced CT of the thorax and abdomen revealed an irregular nodular focus in the posterior apical segment of the left upper lobe of the lung, with unclear borders, an area of approximately 16 mm × 11 mm (Figure 1), and clinical stage T1NM. The patient underwent single-port thoracoscopic posterior apical segmentectomy of the left upper lung, mediastinal lymph node dissection, and pleural adhesion branding procedures. The postoperative pathological report demonstrated the neoplasm as H-FLAC, without regional lymph node involvement (0/15); TNM stage was pT1N0M0. Microscopically, Hematoxylin & eosin staining revealed a complex glandular structure or solid sheet growth pattern of tumor cells (Figure 2A). Cytologically, weak eosinophilic to clear cytoplasm with sub-nuclear vacuoles was also observed. It also presented severe nuclear atypia, a high nuclear-to-cytoplasmic ratio, abundant mitotic activity (25 cells per mm2), and dramatic necrosis. The nucleoli of tumor cells were inconspicuous. Morulae formation was not observed. Immunohistochemical staining revealed TTF-1(-), Napsin-A(-), Syn(-), CgA(-), CD56(-), ALK (-), AFP (-), glypican-3 (+, focal), β-catenin (+, on membrane), Ki-67(+, 60%) (Figure 2B and C). Other positive markers included the EGFR and CDX2. Only few tumor cells expressed PD-L1 (tumor proportion score, TPS<1%), while it was moderately expressed in parts of the tumor-infiltrating immune cells, with a combined positive score (CPS) of 15 (Figure 2D). Detailed results were summarized in Table 1. Additionally, Next-generation sequencing (NGS, ZhongYou Diagnostics, Shanghai, China) was performed using a targeted 59-gene panel covering clinically relevant oncogenic mutations associated with lung cancer and drug response, including EGFR, KRAS, TP53, ALK, ROS1, RET, MET, BRAF, ERBB2, and others. The detailed gene-list and results are presented in Table 2. Only a TP53 missense mutation in exon 8 (c.808T>C, p. F270L) was identified, with a variant allele frequency (VAF) of 21.49%.
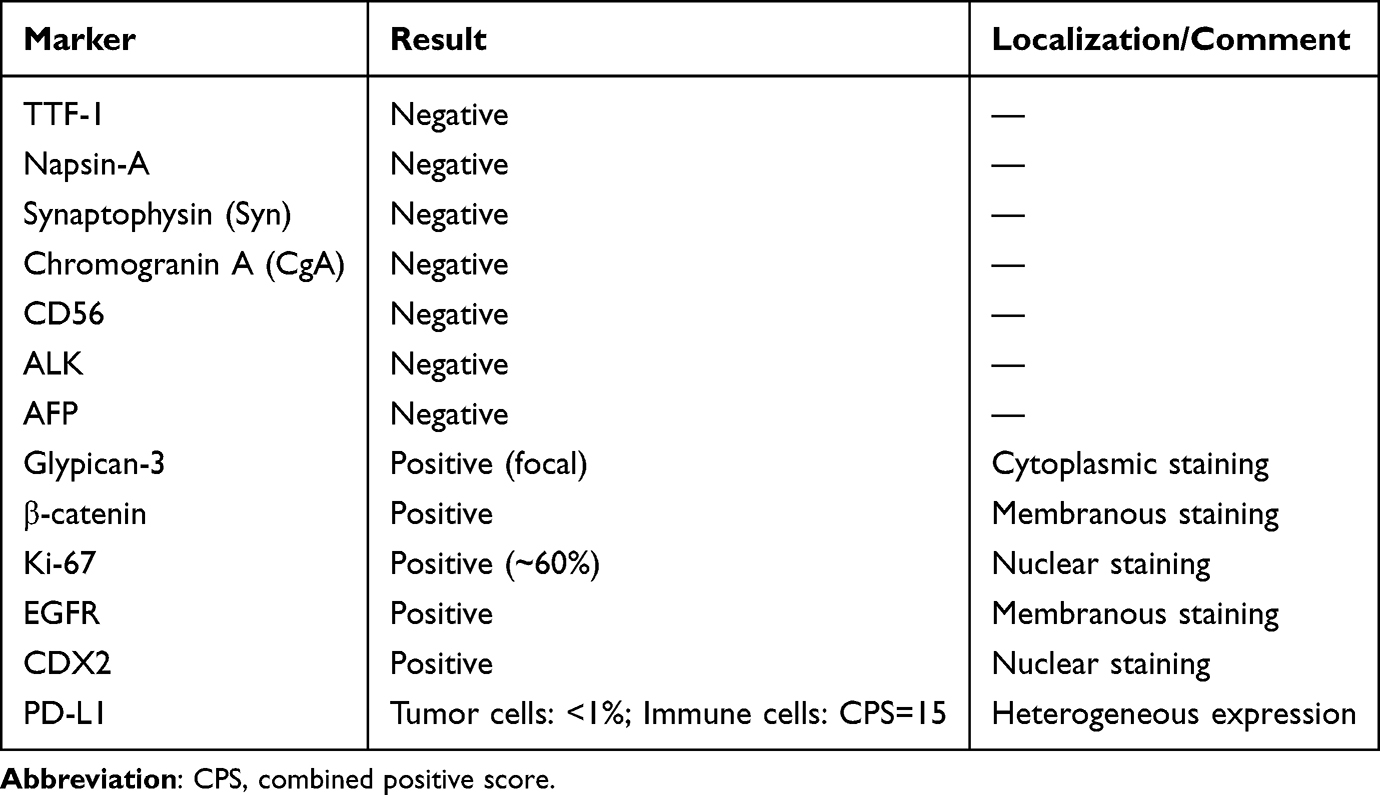 |
Table 1 Summary of Immunohistochemical Findings |
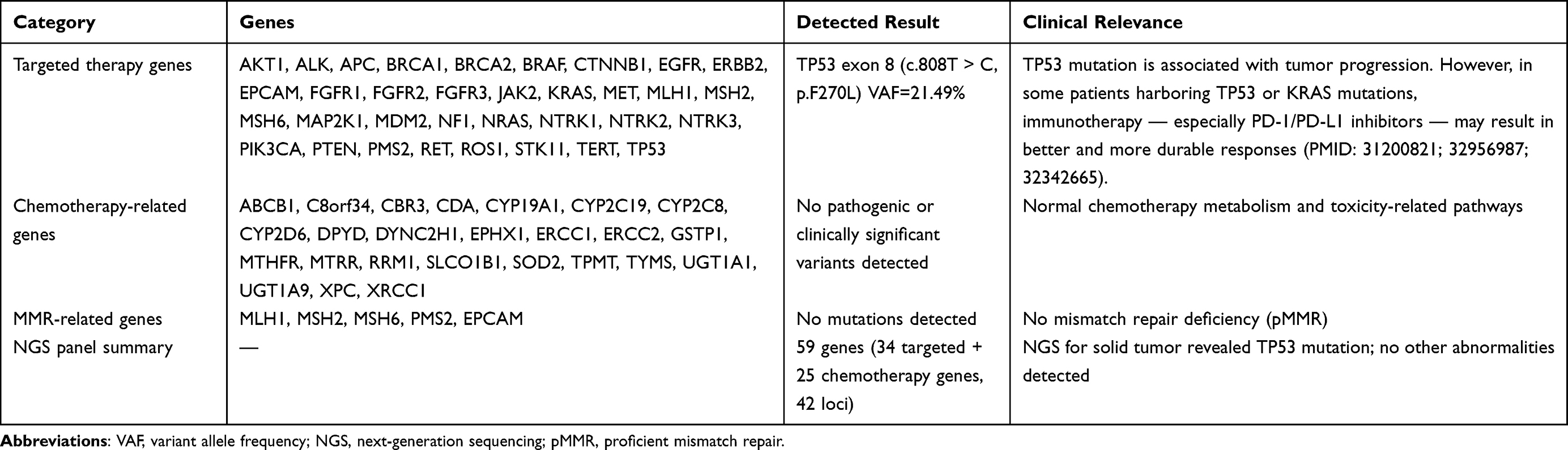 |
Table 2 Summary of Gene Panel and Detected Mutation Results |
 |
Figure 1 Contrast-enhanced computed tomography chest scan revealed an irregular lesion at (A) plain scan (indicated by red arrow), (B) arterial phase, and (C) venous phase. |
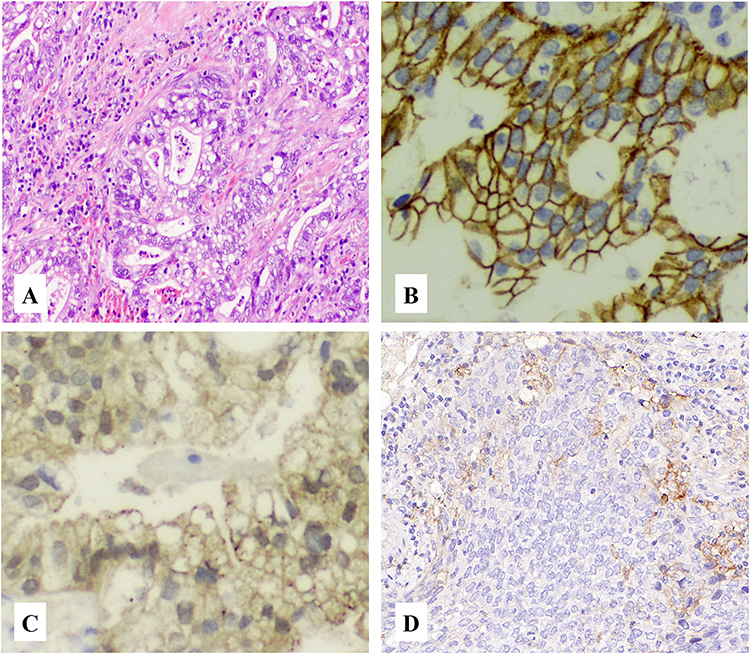 |
Figure 2 (A) Hematoxylin & eosin staining revealed fetal adenocarcinoma of the lung (×100); Immunohistochemical staining revealed (B) positive glypican-3 (×200); (C) positive membrane staining of β-catenin (×200); (D) negative programmed death ligand-1 (×100). |
Discussion
FLAC is a rare histological variant of lung adenocarcinoma. The classification of FLAC as H-FLAC or L-FLAC was proposed in 1998 and was officially determined by IASLC in 2011. In 2023, Mogavero et al discussed the molecular pathology and clinical management of special lung adenocarcinoma subtypes (colloid, fetal, enteric and NOS).13 Compared with L-FLAC, H-FLAC occurs more often in older patients with a history of heavy smoking. It is characterized by aggressive progression and poor prognosis. Here, we report a patient with H-FLAC who underwent radical resection of the malignancy, and further describe the genetic profile of the tumor, together with PD-L1 expression.
H-FLAC accounts for approximately 0.1–0.5% of primary lung cancers. The main clinical symptoms are non-specific cough, hemoptysis, and sputum.10 Patients with H-FLAC are usually in the end stages of the disease once they are diagnosed.14,15 The definitive diagnosis of H-FLAC is based on pathological examination. Histologically, FLAC is characterized by an irregular and complex glandular structure resembling the epithelium of the fetal lung.16 Compared with L-FLAC, H-FLAC exhibits more advanced histological features, including pronounced nuclear atypia and abundant mitotic activity. In addition, H-FLAC may be mixed with components of other types of adenocarcinomas, such as enteric, hepatic, or conventional lung adenocarcinoma, and occasionally, with neuroendocrine cancer.10,11 However, none of these components were observed in the present study. Immunochemically, membrane staining of beta-catenin is a feature of H-FLAC, in contrast to the nuclear or cytoplasmic staining pattern of L-FLAC.8 Other positive IHC markers in this case included glypican-3, CDX2, and EGFR. Similar results have been reported in other H-FLAC cases.17–19 In addition, neuroendocrine markers (CgA, CD56, and Syn) were negative in this case. Alpha-fetoprotein (AFP) expression has been identified in H- FLAC according to other previous reports; however, in our case, the IHC analysis of AFP presented a negative result.7,14,17
The optimal adjuvant approach for high-grade fetal lung adenocarcinoma (H-FLAC) remains undefined due to its rarity. However, a few case reports and reviews have described the use of adjuvant platinum-based chemotherapy following surgical resection. Xiao-Feng et al reported an H-FLAC patient who underwent adjuvant chemotherapy with pemetrexed and cisplatin, achieving disease-free survival after four cycles.20 Similarly, Ricaurte et al reviewed previously published cases and suggested that adjuvant chemotherapy and radiotherapy may be considered in selected patients, especially those with advanced stages or incomplete resection.15 Postoperative chemotherapy may be a reasonable option for resected H-FLAC, but larger multi-institutional studies are needed to define optimal therapy. In conclusion, Radical excision of the tumor remains the best choice so far, for patients who are not in the advanced stage. Additional adjuvant chemotherapy and radiotherapy are needed post operation for better survival.
For patients in the advanced stages of the disease, platinum-based chemotherapy and radiotherapy may be their only options.11,15 In the era of personalized therapy, detailed genetic analysis may be helpful in determining more precise therapeutic strategies for individual patients. However, further research is necessary to identify the essential biological processes involved in tumor progression and the key molecular markers with potential therapeutic value. Unlike lung adenocarcinoma, which is usually driven by specific oncogenes such as EGFR, the tumorigenesis of H-FLAC may be more complex, and no important oncogenes have been identified yet. The most frequent genetic mutations occur in TP53 (44%), KRAS (11–25%), and KMT2C (38.8%); therefore, WEE1 and KRAS G12C inhibitors are potential therapeutic options.17,21,22
KRAS G12C inhibitors have emerged as promising targeted agents for non-small cell lung cancer (NSCLC) harboring KRAS G12C mutations. The first-in-class inhibitor sotorasib (AMG 510) was evaluated in the CodeBreaK 100 clinical trial, which demonstrated an objective response rate (ORR) of 37% and a median progression-free survival (PFS) of 6.8 months in previously treated KRAS G12C-mutant NSCLC patients.23 Another inhibitor, adagrasib (MRTX849), showed comparable efficacy in the KRYSTAL-1 trial, achieving an ORR of 43% and median PFS of 6.5 months.24 Although no data is available specifically for fetal-type adenocarcinoma, H-FLAC harboring KRAS G12C mutation may still be benefit from KRAS G12C inhibitor. Further investigation into H-FLAC is warranted.
TP53 mutations have been reported in fetal-type lung adenocarcinomas25 and in lung adenocarcinomas with isolated TP53 alterations and fetal-like morphology,26 suggesting that TP53 may contribute to the aggressive behavior and potential immunogenicity of these tumors, although large‐scale data on TP53 mutated H-FLAC are still lacking. In our current study, we performed gene-sequencing analysis of 59 genes related to drug response and TP53 mutation was identified, that may indicate potential sensitivity to DNA damage response–targeted agents, such as WEE1 inhibitors, which are currently under clinical investigation for TP53-mutated tumors. Nevertheless, using a targeted 59-gene panel may not capture other rare or novel genomic alterations that could have therapeutic relevance. Therefore, comprehensive genomic profiling (eg, whole-exome or RNA sequencing) may provide deeper insights into the molecular landscape of H-FLAC and uncover actionable targets for precision therapy.
In addition, H-FLAC exhibits a heterogeneous immune microenvironment characterized by variable PD-L1 and TIL expression patterns.19 Recent studies have shown that PD-L1 expression on tumor-infiltrating immune cells, even when absent on tumor cells, can still contribute to local immune modulation and may be associated with responsiveness to immune checkpoint inhibitors in certain contexts.27 Our data also suggest similar results for PD-L1 expression in H-FLAC (TPS<1, CPS=15), indicating that its responsiveness to immunotherapy with programmed death receptor/ligand-1 inhibitors may be limited, but evaluation of detailed therapeutic effect should dependent on further well-designed clinical trials. In rare lung cancer subtypes, other potential bio-markers, such as tumor mutational burden (TMB) and microsatellite instability (MSI) could also inform immunotherapeutic responses,28 although the mismatch repair-related genes were wild-type in our case. Consistent with previous reports, our targeted NGS analysis did not detect common driver mutations such as EGFR, KRAS, ALK, or BRAF, suggesting that H-FLAC may follow a distinct molecular pathway of tumorigenesis compared with conventional lung adenocarcinoma.
Conclusion
Recent genomic and immunologic studies have highlighted the heterogeneity and potential therapeutic vulnerability of rare lung cancer subtypes.28,29 Here we reported a case of H-FLAC with a TP53 mutation and its PD-L1 expression was negative in tumor cells but mild in some immune cells in the tumor microenvironment. Our findings suggest that H-FLAC may have limited intrinsic immune evasion capacity. The weak PD-L1 expression on immune cells indicates a partially activated yet insufficient antitumor response. Additional cases and more detailed gene-panels are needed to identify novel therapeutic targets and to guide personalized treatment strategies, including immunotherapy in the era of precision oncology.
Abbreviations
AFP, Alpha-fetoprotein; CPS, Combined positive score; FLAC, Fetal adenocarcinoma of the lung; H-FLAC, High-grade fetal adenocarcinoma of the lung; CT, Computed tomography; IALSC, The International Association for the Study of Lung Cancer; L-FLAC, Low-grade fetal adenocarcinoma of the lung; NGS, Next-generation sequencing; PD-L1, Programmed death ligand-1; TPS, Tumor proportion score.
Data Sharing Statement
No datasets were generated or analyzed during the current study. The data are available from the corresponding author, Peifeng Lin, upon reasonable request.
Ethical Approval and Consent to Participate
Ethics approval for case reports is not required at our institute.
Consent for Publication
Written informed consent for publication was obtained from the patient.
Author Contributions
Yunqin Xu collected the data, prepared the figures, and drafted the manuscript. Kangjian Dai, Wei Chen, and Haifan Wu contributed to data collection and figure preparation. Peifeng Lin conceptualized the work, supervised the study, collected the data, and served as the corresponding author. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Alduais Y, Zhang H, Fan F, Chen J, Chen B. Non-small cell lung cancer (NSCLC): a review of risk factors, diagnosis, and treatment. Medicine. 2023;102(8):e32899. doi:10.1097/MD.0000000000032899
2. Smolarz B, Lukasiewicz H, Samulak D, Piekarska E, Kolacinski R, Romanowicz H. Lung cancer-epidemiology, pathogenesis, treatment and molecular aspect (Review of Literature). Int J Mol Sci. 2025;26(5):2049. doi:10.3390/ijms26052049
3. Laguna JC, Tagliamento M, Lambertini M, Hiznay J, Mezquita L. Tackling non-small cell lung cancer in young adults: from risk factors and genetic susceptibility to lung cancer profile and outcomes. Am Soc Clin Oncol Educ Book. 2024;44(3):e432488. doi:10.1200/EDBK_432488
4. Patnayak R, Jena A, Rukmangadha N, Lakshmi AY, Chandra A. Well-differentiated fetal adenocarcinoma of the lung in an adult male: report of an unusual tumor with a brief review of literature. J Cancer Res Ther. 2014;10(2):419–421. doi:10.4103/0973-1482.136677
5. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
6. Kradin RL, Young RH, Dickersin GR, Kirkham SE, Mark EJ. Pulmonary blastoma with argyrophil cells and lacking sarcomatous features (pulmonary endodermal tumor resembling fetal lung). Am J Surg Pathol. 1982;6(2):165–172. doi:10.1097/00000478-198203000-00009
7. Nakatani Y, Kitamura H, Inayama Y, et al. Pulmonary adenocarcinomas of the fetal lung type: a clinicopathologic study indicating differences in histology, epidemiology, and natural history of low-grade and high-grade forms. Am J Surg Pathol. 1998;22(4):399–411. doi:10.1097/00000478-199804000-00003
8. Travis WD, Brambilla E, Noguchi M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society: international multidisciplinary classification of lung adenocarcinoma: executive summary. Proc Am Thorac Soc. 2011;8(5):381–385. doi:10.1513/pats.201107-042ST
9. Travis WD, Brambilla E, Nicholson AG, et al. The 2015 world health organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243–1260. doi:10.1097/JTO.0000000000000630
10. Li Y, Xi SY, Yong JJ, Wu XY, Yang XH, Morphologic WF. Immunohistochemical, and genetic differences between high-grade and low-grade fetal adenocarcinomas of the lung. Am J Surg Pathol. 2021;45(11):1464–1475. doi:10.1097/PAS.0000000000001744
11. Kubouchi Y, Matsuoka Y, Araki K, et al. Pure high-grade fetal adenocarcinoma of the lung: a case report. Surg Case Rep. 2018;4(1):70. doi:10.1186/s40792-018-0478-4
12. Luo Z, Cao C, Xu N, Ying K. Classic biphasic pulmonary blastoma: a case report and review of the literature. J Int Med Res. 2020;48(10):300060520962394. doi:10.1177/0300060520962394
13. Mogavero A, Bironzo P, Righi L, et al. Deciphering lung adenocarcinoma heterogeneity: an overview of pathological and clinical features of rare subtypes. Life. 2023;13(6):1291. doi:10.3390/life13061291
14. Morita S, Yoshida A, Goto A, et al. High-grade lung adenocarcinoma with fetal lung-like morphology: clinicopathologic, immunohistochemical, and molecular analyses of 17 cases. Am J Surg Pathol. 2013;37(6):924–932. doi:10.1097/PAS.0b013e31827e1e83
15. Ricaurte LM, Arrieta O, Zatarain-Barron ZL, Cardona AF. Comprehensive review of fetal adenocarcinoma of the lung. Lung Cancer. 2018;9:57–63. doi:10.2147/LCTT.S137410
16. Takahashi Y, Takashima S, Watanabe S, et al. F18-FDG PET-CT analyses of small peripheral adenocarcinoma of the lung. Acta Radiol. 2013;54(2):164–168. doi:10.1258/ar.2012.120138
17. Suzuki M, Yazawa T, Ota S, et al. High-grade fetal adenocarcinoma of the lung is a tumour with a fetal phenotype that shows diverse differentiation, including high-grade neuroendocrine carcinoma: a clinicopathological, immunohistochemical and mutational study of 20 cases. Histopathology. 2015;67(6):806–816. doi:10.1111/his.12711
18. Zhang J, Sun J, Liang XL, Lu JL, Luo YF, Liang ZY. Differences between low and high grade fetal adenocarcinoma of the lung: a clinicopathological and molecular study. J Thorac Dis. 2017;9(7):2071–2078. doi:10.21037/jtd.2017.07.14
19. Gu Y, Zhang S, Liang X, Zhao H, Li X, Lu J. Clinical and pathological characteristics and prognosis of lung adenocarcinoma with high-grade fetal features: a retrospective analysis. Int J Surg Pathol. 2024;32(4):667–678. doi:10.1177/10668969231188890
20. Xiao-Feng L, Guo-Qi Z, Wei H, et al. High-grade fetal adenocarcinoma of the lung with abnormal expression of alpha-fetoprotein in a female patient: case report. Medicine. 2021;100(7):e24634. doi:10.1097/MD.0000000000024634
21. Suzuki M, Kasajima R, Yokose T, et al. Comprehensive molecular analysis of genomic profiles and PD-L1 expression in lung adenocarcinoma with a high-grade fetal adenocarcinoma component. Transl Lung Cancer Res. 2021;10(3):1292–1304. doi:10.21037/tlcr-20-1158
22. Kong A, Mehanna H. WEE1 Inhibitor: clinical development. Curr Oncol Rep. 2021;23(9):107. doi:10.1007/s11912-021-01098-8
23. Skoulidis F, Li BT, Dy GK, et al. Sotorasib for lung cancers with KRAS p.G12C mutation. N Engl J Med. 2021;384(25):2371–2381. doi:10.1056/NEJMoa2103695
24. Janne PA, Riely GJ, Gadgeel SM, et al. Adagrasib in non-small-cell lung cancer harboring a KRAS(G12C) mutation. N Engl J Med. 2022;387(2):120–131. doi:10.1056/NEJMoa2204619
25. Wang B, Jin H. A case report of low grade fetal lung adenocarcinoma with TP53 mutation. Medicine. 2022;101(11). doi:10.1097/MD.0000000000029047
26. Mendoza RP, Chen-Yost HI, Wanjari P, et al. Lung adenocarcinomas with isolated TP53 mutation: a comprehensive clinical, cytopathologic and molecular characterization. Cancer Med. 2024;13(1):e6873. doi:10.1002/cam4.6873
27. Gureviciene G, Matulione J, Poskiene L, Miliauskas S, Zemaitis M. PD-L1 expression and tumour microenvironment patterns in resected non-small-cell lung cancer. Medicina. 2024;60(3):482. doi:10.3390/medicina60030482
28. Harada G, Yang SR, Cocco E, Drilon A. Rare molecular subtypes of lung cancer. Nat Rev Clin Oncol. 2023;20(4):229–249. doi:10.1038/s41571-023-00733-6
29. Huang N, Qu T, Zhang C, Li J. Case report: successful treatment of advanced pulmonary sarcomatoid carcinoma with BUBIB-ALK rearrangement and KRAS G12C mutation by sintilimab combined with anlotinib. Front Oncol. 2024;14:1269148. doi:10.3389/fonc.2024.1269148
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.