Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Moving on from CUSP to CUP: empowering multidisciplinary teams and integrating them in the management structure of hospital organization
Authors Govindarajan R ![]()
Received 17 December 2018
Accepted for publication 20 February 2019
Published 15 April 2019 Volume 2019:12 Pages 257—268
DOI https://doi.org/10.2147/JMDH.S198494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Rajaram Govindarajan.
Views: 181
Rajaram Govindarajan
Operations Management, Innovation and Data Sciences, ESADE Business School, 08001 Barcelona, Spain
Background: The functional role of Comprehensive Unit-based Safety Program (CUSP) teams was extended to empower them and make them a part of the organizational management.
Purpose: These improvements in the functional roles of CUSP were made with the objective of solving two structural issues, namely, departmentalization and compartmentalization present in health care organizations.
Methods: The following were three improved functional roles: 1) instead of just being a reactive mechanism to implement improvements based on real safety issues, they also carried out risk analysis and implemented preventive actions proactively; 2) instead of focusing only on safety, they controlled all results such as safety, quality, treatment effectiveness and timeliness of their respective process units, using a series of Key Performance Indicators; and 3) instead of being a supplementary multidisciplinary team parallel to the organization´s departmentalized management structure, they were made to participate in the decision-making structure, representing their respective process units. These teams represented different process units and were named as Comprehensive Unit-based Process (CUP) teams.
Results: The CUP structural design changed the dynamics of the organization: 1) it integrated members of different disciplines, especially physicians and nurses, and integrated them into a team with a shared goal, making internal communication and teamwork a “systemic” requirement; 2) it disabled the middle-level managers to represent the interests of specific knowledge-based groups such as physician departments or nursing areas while making decisions; and 3) it reassigned middle-level managers the task of representing different CUPs, making each manager responsible for a process unit, thus ensuring control over the results of multidisciplinary activities.
Conclusion: The new organizational structure put burden on the system, not on its people, as it made multidisciplinary communication and teamwork to be the rule of the game, allowing patient-centered health care.
Keywords: process management, CUSP, CUP, multidisciplinary teamwork, lean management, patient safety
Introduction
Multiple studies make it evident that there are major functional deficiencies in our health system.1 Let us take patient safety, first. At the policy level, health care organizations may have acquired their commitment to the Hippocrates principle of “nonmaleficence”, but in practice, systems are not well designed to ensure that.1–3 Existing evidence shows that there is a lot of maleficence done to patients, as medical error is the third biggest killer causing 250,000 deaths each year in the United States alone,4 and there is no reason to expect that the safety levels would be better in other countries. Most of these are due to “systemic” organizational deficiencies that allow involuntary errors to happen even to motivated and competent care providers.5 It is surprising to know how the errors produced by the hospital system, which has the mandate of saving human lives, can cause exactly the opposite effect in so many people. It is even more surprising to know how the matter can receive such low public and political attention, especially considering that most errors are preventable through better system design and management.1
Second, let us take morbidity. In order for 250,000 people to die by direct harm, those who are harmed, but not killed, are estimated to be millions.6 A better system should lead to the elimination of the errors that can, not only save hundreds of thousands of lives but can also reduce the morbidity in millions. Third, in addition to reducing morbimortality, a system should ensure treatment effectiveness, but studies show that it is not measured in most cases. Often efficacy is determined through clinical trials that determine whether an intervention produces the expected result under ideal circumstances, but the determination of effectiveness which measures the degree of beneficial effect under “real world” clinical settings is rather limited7 and, as a result, it is reported that only 50% of the medical practice is evidence-based.8 Govindarajan9 proposed that multidisciplinary teams take charge of measuring and improving treatment effectiveness through indicators of survival rates and toxicities in cancer patients. Fourth, among health care workers, there is a lot of stress and burnout. Employees complain about the “lack of organization” at workplace, insufficient material resources, ambiguity of roles and responsibilities, under-utilization of professional skills, low participation in decision-making, lack of training and recognition, system-induced labor disputes, and work overload.10 Health care employees are second victims of systemic errors.11,12 Finally, health care costs are higher than optimum because of morbimortality rates caused by errors. With existing disorder, it is estimated that health care costs can be reduced significantly (up to 20%) as a lot of resources is currently being spent on patients who are harmed but not killed by medical errors, through re-interventions, repeated medical treatments, prolonged hospital stays, damage claim payments, and other legal structural costs.13 If care providers inadvertently cause errors when attempting to save a life, the responsibility must lie with those who design the health system.1,14–16 Govindarajan1 pointed out that the cause of this disorder is “systemic” and is due to two structural defects of the organization: 1) departmentalization and 2) compartmentalization. By improving this structural issue, he argued, that the problems listed in this section, such as safety-related morbimortality, treatment effectiveness, treatment costs, and employee satisfaction and motivation, can all be improved.
Structural defect of “departmentalization” is a system design issue
Most health care organizations are structured in unidisciplinary departments of physicians, nurses, technical staff, administrative staff, etc.1,17 In the organizational chart, the chain of command is designed in such a way that these unidisciplinary departments are managed separately by heads of the corresponding discipline (Figure 1). For example, physicians are supervised by medical department heads, who in turn are supervised by medical directors; similarly, nurses are supervised by nursing supervisors who in turn are supervised by nursing managers/directors. This “departmentalized” organizational structure is historic and is focused on managing “unidisciplinary human resource” and their “competence”, instead of focusing on whether such resource and knowledge are collectively, safely and effectively applied by multidisciplinary teams in patient care. Such departmentalized organizations are divided in “vertical” lines to control the knowledge that may be needed to carry out the task, but not to control the quality and effectiveness of the task itself.1
 | Figure 1 The Theory of the Division:1 The departmentalized structure is responsible for dividing the organization, creating gaps in multidisciplinary communication and teamwork issues among physicians, nurses, and other care providers, leading to problems of safety, effectiveness, and efficiency in health care. Abbreviation: admin, administration. |
While physicians and nurses are supervised separately by independent heads, they do work together to deliver a health service, but without a common head in the organizational structure to supervise the multidisciplinary activity.18 How can the results such as safety and treatment effectiveness of an entire team be effectively controlled, while each of its components is supervised separately by independent managers?1 One of the five key reforms proposed by the Institute of Medicine (IOM) is the provision of care as members of an interdisciplinary team.5,19 Although our discourse everywhere is asking people to work in multidisciplinary teams,20–22 the burden is placed on people to work in teams, instead of placing it on the “system” by making teamwork a systemic requirement by empowering multidisciplinary teams and making them a part of the systemic decision-making structure.1
Govindarajan1 proposed the “theory of division”, according to which the departmentalized structure is responsible for dividing the organization, creating communication gaps and teamwork issues among physicians, nurses and others, leading to problems of safety, effectiveness, and efficiency in health care (Figure 1). Systemic communication between physicians and nurses has become more and more limited, having to take up “patchwork” initiatives for compensating for this systemic deficiency using improved physician-nurse cooperation initiatives.23,24 Govindarajan1 postulated that departmentalization is the root cause of many safety and quality issues and the improvement initiatives should address this structural problem in system design. He argued that first the “departmentalization” does not structure the organization into functional multidisciplinary process units – a structure needed for controlling multidisciplinary results. Second, argued he, that each head of department, in this “representative” model, may defend the interest of their own group in top management decisions, while the interests of the patients and the multidisciplinary perspective of the organization may not be well represented. In such organizations, patient-centered care becomes difficult to implement, because being patient-centered essentially means having the vision of the “whole”. The vision of a department is “part”, and cannot be “whole” in a multidisciplinary service. This is the most serious structural defect that health care organizations historically have had to live with, while in other business sectors, department structures have transformed, at least in part, into team management structures.1
Structural defect of “compartmentalization” is another system design issue
In health care, we often are organized in “compartments” and each such compartment is an “island” within the organization, with very little communication among them.1 There are two different types of such compartments. The first type of compartments are knowledge-based groups, such as specialized medical departments. The origin of this type of “compartmentalization” may be at the clinical training level itself, as physicians are specialized by apparatus of the organism. There is very little “systemic” communication requirement between such different compartments in the organization; however, the patient´s condition in some cases may require an “integrative” perspective of a “systemic” disease, as a treatment applied in one apparatus may affect another (for example, a nephrologist treating chronic kidney failure of a heart patient may need to communicate with the patient´s cardiologist). Most organizations use interconsultation as the way of “compensating” for this compartmentalization and often specialists may have to decide between waiting for interconsultation that may take days to arrive or take the risk of treating without it. The second type of compartments are the process units (for example, a diagnostic center, a hospitalization unit, daycare hospital, radiotherapy unit, etc). Among these “compartments” often there is very little systemic communication requirement and they do not often share much information related to the same patient to be able to have a comprehensive view of the patient´s overall needs. For example, for making treatment decisions on oncology patients, a multidisciplinary combined visit of oncologists, surgeons, and radiotherapists together is reported to give much better results.25 Since such integrative physical visits may add cost to treatment and may not be economically viable in most cases, a good communication loop coupled with virtual visits, or the review of clinical questionnaires, can functionally substitute such combined visits. For example, a pathologist from pathological anatomy lab may need to communicate and obtain more information from the physician prescribing the test before doing it to avoid diagnostic errors, and similarly may need a feedback on reported test results to learn lessons when errors are detected by the prescribing physician; such communication opportunities are currently very limited.26,27 There are studies proposing better communication methods through use of checklists, protocols, or information technology, which could be essential to reduce communication failures.28
The problem of “compartmentalization” may also lead to issues in care continuum, making patient flow and treatment speed non-optimal. Patients of compartmentalized organizations may need multiple appointments and tests, and the selected treatment option may not be the most indicated. Such patients may find themselves signing on to various independent waiting lists with little coordinated communication between care units, leading to increased lead times. This is why internal communication is one of the most important systemic problems in the health sector. In many such organizations, their top managers are found to be managing “islands of compartments” instead of aligning and managing them as a system.1,29 Therefore, there are often risks of failure due to a lack of complete perspective of a patient’s problems. In other words, by design, the healthcare system cannot possibly focus on patient-centered care, if the problem of compartmentalization is not eliminated.1
In the literature, the use of multidisciplinary teams of front-line providers for safety improvement has been experimented and reported to be useful.30–33 Pronovost et al30 used Comprehensive Unit-based Safety Program (CUSP) methodology to introduce multidisciplinary teamworking climate for learning lessons and improving safety in large number of intensive care units (ICU) in Michigan. Wick et al31 demonstrated the usefulness of formation of small CUSP teams to address Surgical Site Infections (SSI). Khan et al32 evaluated the CUSP approach to improve the care of mechanically ventilated patients and reported less ICU mortality rate.
In this study the idea of CUSP was taken a step further to integrate the teams in the decision-making structure of the organization so that such benefits could materialize, focusing on qualitative benefits for the patients, employees and the organization in diverse management aspects. For that purpose, the functional roles of the multidisciplinary groups were expanded in three different dimensions: 1) be proactive not just reactive, 2) deal with all process variables, not just safety, and 3) be part of the decision-making management structure, not as a supplementary team.
Methods
Learning from the functional design aspects of biological systems such as the human organism itself, just as the physiology is based on transforming the anatomic structure into structural process units (circulation, respiration, etc.) and integrating them to create the system, known as the organism, in this study the hospital organization´s departmental structure was transformed into functional process units and were named as Comprehensive Unit-based Processes (CUP). The CUPs were aligned and inter-connected to form a system, the organization. Just as when one of the processes of the organism does not function correctly, it sends out feedback “signals” to achieve “homeostasis” to maximize survival and longevity, when a CUP of the organization was not functioning correctly, as it would no longer be compartmentalized, it would send out communication signals, through the introduction of a series of Key Performance Indicators (KPIs). This feedback from one CUP team would make other related CUP teams to react and compensate for it, in order to optimize the overall results of the organization (For example, diagnostic errors and delays would be detected and fed back by a “hospitalization CUP” to the “diagnostic CUP” for correcting errors and delays).
CUPs were created by dividing the organization along “horizontal” lines in multidisciplinary process units, instead of dividing it in vertical departmental lines, to strengthen multidisciplinary communication and teamwork, and to set common goals for different members of the multidisciplinary knowledge workers (Figure 2). Each CUP was managed by a multidisciplinary team comprising relevant medical department heads, nursing supervisors, senior physicians, nursing team leaders, among others (between 7 and 10 members). These CUP teams had the same multidisciplinary structure as CUSP teams that have been tested elsewhere.30–33 Some of the medical department heads and other middle-level managers had a new task of representing a CUP and ensuring control over the results of multidisciplinary activities. CUP teams were made to be a part of the organizational structure, and were made to take charge of all their collective professional activities through the following improved functional roles: 1) instead of just being a reactive mechanism to implement improvements based on real safety issues that have already occurred, they also carried out risk analyses and implemented preventive actions proactively; 2) instead of focusing only on safety, they took charge of the results of all multidisciplinary activities of their respective process units such as quality, treatment effectiveness, resource use efficiency, and treatment delays, among others, so that the teams can take control of the consequence of their collective clinical activities and become accountable; and 3) instead of being a supplementary multidisciplinary team parallel to the existing departmental organizational structure, they were given a mechanism to participate in the decision-making structure of the organization. The improvements made in the functional role were to resolve the structural issue of “departmentalization” and “compartmentalization” present in health care organizations.1 In this organization, as CUSP teams did not exist previously, CUPs were created directly but with the same structure as CUSP.
 | Figure 2 Moving on from anatomy to physiology: The CUP model converted departmental structure into various multidisciplinary processes and made them a part of the systemic decision-making structure, which made multidisciplinary communication and teamwork a “systemic” activity. |
The CUP implementation was made in the pilot area of hospitalization in a 400-bed public hospital in Barcelona area (Hospital del Mar) for a period of 2 years, within the framework of the Lean Management project. In this project, after plotting a process map of different CUPs (Figure 3), the pilot area of hospitalization was divided into 5 CUPs, namely Critical Care Hospitalization, Maternity Hospitalization, Psychiatry Hospitalization, Medical Hospitalization, and Surgical Hospitalization. All 5 CUP team members, and the top management (CEO, Medical Director, Nursing Director, etc.), went through a 24 hr training program before starting the implementation of CUP. There were also internal-supplier CUPs, such as Diagnostic Centers, Hospital Pharmacy, Surgical Wards, to name a few.
 | Figure 3 An example of the process map to create the system by integrating different CUPs in a hospital organization.Abbreviations: CUP, Comprehensive Unit-based Process. |
The proactive function of the CUP teams consisted of risk management and prevention through risk analysis and by managing all results of their process units. They received methodological support from the Lean Management project team to do the risk analysis and implement preventive systemic improvement actions, using Failure Mode and Effects Analysis.34 CUP teams managed their process results by monitoring its output such as safety, treatment effectiveness, errors, nosocomial infections, speed of services, and resource use efficiency (Table 2) in a monthly meeting using their respective KPIs. Of course, they also played the complementary reactive role of root cause analysis and implemented corrective actions when adverse events did happen, but they used the philosophy of “prevention is better than correction” and worked principally on harm prevention and result optimization of the entire process. The method was to try to change the non-functional, departmentalized, compartmentalized, unidisciplinary organizational structure into multidisciplinary team-based structure for hospital management.
 | Table 1 Major improvements achieved during risk analysis |
 | Table 2 Example of key performance indicators (KPI) of surgical hospitalization CUP analyzed in a monthly meeting |
Results
The most important and common KPI of all 5 hospitalization CUPs was the average hospital stay duration, which was identified to be the consequence of many safety and quality issues in the risk analysis and was the most difficult one to improve because of the following multi-factorial systemic organizational issues: 1) hospitalized patients were admitted a day before surgery for “just in case” reasons because the system did not ensure their preparedness for the surgery or sometimes some major ambulatory surgeries were performed by hospitalizing patients unnecessarily, 2) patients waited for diagnostic testing despite being hospitalized (up to 1 week in case of Magnetic Resonance Imaging) because they had to compete with outpatients for a slot in the same diagnostic center located in the hospital premises, 3) interconsultation delays were systemic (specialist medical departments needed 2 days on an average) causing systematic delays for diagnosis and treatment, 4) additional hospital stays occurred due to adverse events in hospitalized patients that included medication errors, patients falling out of beds, pressure ulcers, nosocomial infections, among other hospital acquired conditions, and 5) patients who had been “clinically” discharged were waiting hospitalized for days before being “administratively” discharged mainly due to internal communication delays and due to unresolved social issues that could have been detected and resolved earlier (for example, no elevator in the residential building of the discharged patient who could not climb stairs or a discharged patient needing a social assistant at home for personal care that had not yet arrived). It was understood that, if the safety and quality were managed well, the service would flow without delays and the hospitalized patients should get cured and discharged sooner, without readmissions. On the other hand, as average hospital stay costs 375$/night/patient, the top management´s lean initiative of this methodology was to save money on hospital stays by improving safety and quality, as judged and managed by the clinical teams themselves. With the help of the Lean Management team, different CUP teams had collectively identified specific actions to save 7000 nights of hospitalization leading to 2.6Million$ of annual savings for the hospital. This was the central objective of the CUP teams.
After training, CUP teams participated in risk analysis and implemented a series of improvement actions (Table 1). For example, the Surgical Hospitalization CUP identified some major surgical operations that could be safely carried out without the need for hospitalization and made them ambulatory, proposed that interconsultation response be given on the same day as requested, requested 100% quality checks on unit-dose medication preparations by a second person, suggested that dangerous medication be identified with red stickers, created a “daily quota” for conducting magnetic resonance imaging or endoscopes on hospitalized patients so that they do not have to wait hospitalized for days, introduced a “social condition” checklist for all patients on day 1 of their admission to avoid discharge delays through early involvement of social workers, introduced a protocol for nursing staff to accompany vulnerable post-surgery patients to toilet to avoid falling, and demanded timely rehabilitation for indicated patients.
Each CUP team identified a series of KPIs to monitor their process results, along with target values for each indicator, which was based on historical data and benchmarks. KPI results were reviewed monthly by the corresponding CUP teams. For example, Table 2 shows the KPI monitored by the Surgical Hospitalization CUP. Their KPIs were: Number of discharges, % of patients discharged before 12 noon on the same day they were “clinically discharged”, Average hospital stay (days), Mortality rate (%), Number of patients readmitted in 30 days, Interconsultations rate (%), Pre-surgical waiting in programmed interventions (days), Diagnostic testing (%), Nosocomial bacteremia (%), Falling of the bed (%), and Pressure ulcers (%). Lean Management project team obtained objective data for all KPIs through the information system of the hospital and facilitated monthly review meetings of CUP teams in the project office. For each indicator result, the CUP team did a Pareto analysis, identified the factors on which to act and improve, and planned the corresponding improvement actions; different team members shared the responsibility to execute the planned actions with a committed deadline for each. In the following monthly meeting, the progress on those actions was tracked and new improvement actions based on new data analyses were added. The teams thus entered into the dynamics of a 3-step methodology for continuous improvement: measurement, analysis, and improvement.
CUP teams collectively planned and executed treatment plans. Customer preferences and needs were shared among team members and were collectively executed. They focused on collective tasks and their effect on patient outcome: whether or not patients were safe and got cured. The decision-making was taken over by multidisciplinary team heads with the understanding of how such decisions affected all team members, including the patient outcome. Physicians and nurses integrated in one single group because of their shared destiny. They improved social interaction as members of single group, with increased communication opportunities during breaks. CUP teams took up collective responsibility for their clinical activity. The Lean Management project team that coordinated the CUP teams, as well as the top management committee that oversaw the Lean Management project team, observed the benefits of the multidisciplinary CUP intervention methodology described in Table 3.
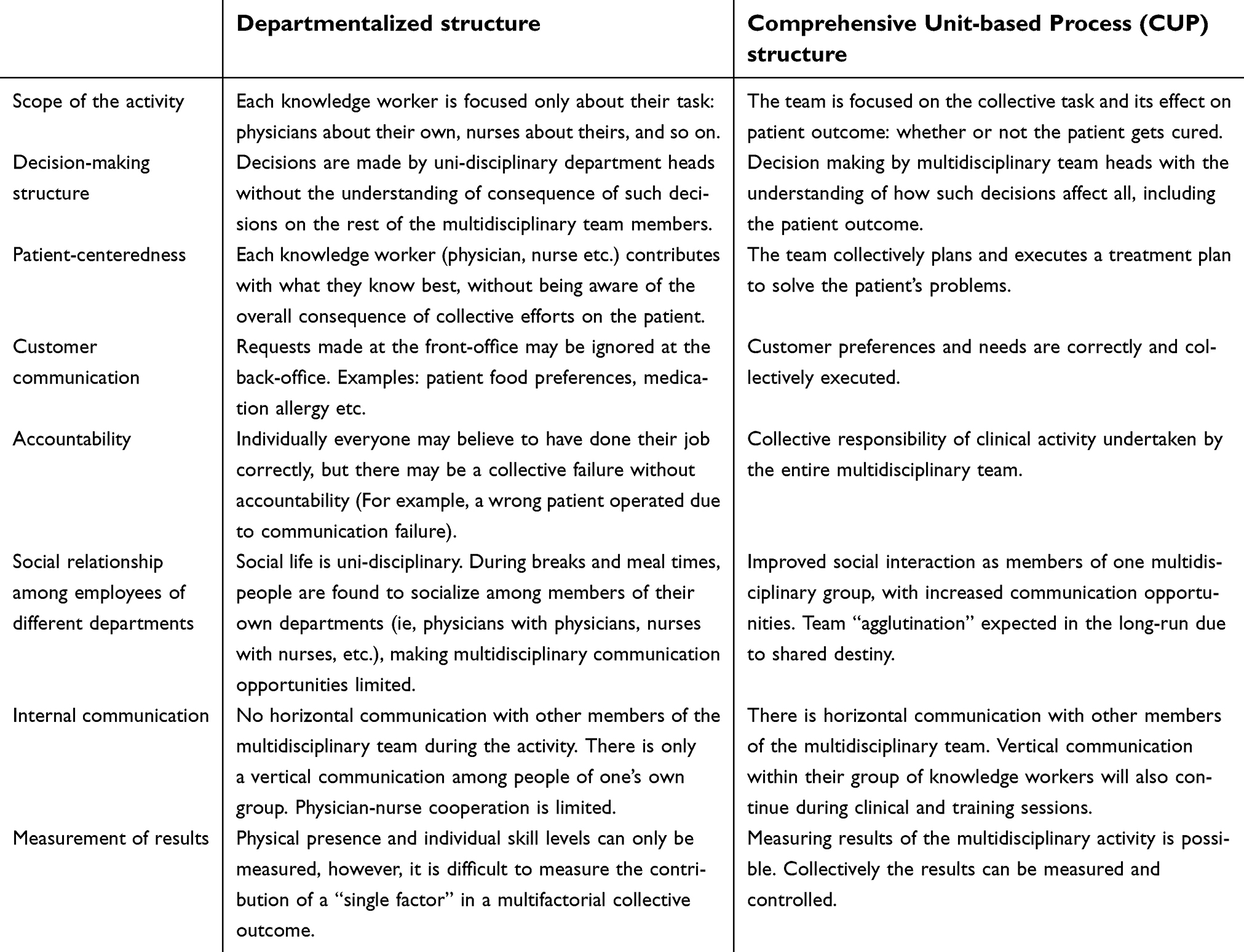 | Table 3 Compared to the “departmentalized” structure, the benefits of the CUP structure observed |
The CUP structure was found to change the dynamics of the organization: 1) it integrated members of different disciplines, especially physicians and nurses, and integrated them into a team, making teamwork a “systemic” requirement; 2) it disabled the middle-level managers to represent the interests of specific knowledge-based groups such as physicians or nurses while making decisions; and 3) it reassigned middle-level managers the task of representing different CUPs, making each manager responsible for a functional unit, thus ensuring control over the results of multidisciplinary activities. In this way, the middle manager’s job became process-oriented and result-oriented.
Although vertical intra-disciplinary communication within their respective group of physicians or nurses continued, there was more horizontal communication with other members of the multidisciplinary team. The measurement of results of the multidisciplinary activity became possible. Collectively the results could be measured and controlled.
In previous studies,30–33 the benefit of working in multidisciplinary teams for improving safety, using a single variable such as mortality rate or Surgical Site Infection, had been demonstrated using statistical analysis. As there were dozens of variables related to safety, quality, treatment effectiveness, and timeliness, demonstrating through statistical analysis the benefit of teamwork in so many different and diverse variables in a real-life setting for five different CUP teams was beyond the scope of this management initiative. In fact, the teams were given a mechanism and authority through which they themselves “optimized” their own results, using their own collective judgment. That was the empowerment sought in this initiative.
Conclusions
As compared to the CUSP model, the proposed CUP model added a proactive, risk-analysis component to patient safety management, and expanded its scope into managing all process variables that affected safety, quality, treatment effectiveness, and speed of service. The new structure empowered the multidisciplinary teams to participate in the management structure of the organization.
First, multidisciplinary CUP teams identified proactively different risks for their patients and implemented preventive actions. Then, for their respective process units, the CUP teams became aware of the consequences of what they did and did not, through a monthly review of objective data in the form of KPIs; they analyzed those results and implemented corrective actions. Instead of addressing a single safety variable such as Surgical Site Infections31 that surgical area CUSP teams would, the Surgical Hospitalization CUP team addressed all KPIs related to safety of their patients (mortality rate, nosocomial bacteremia, falling of the bed and pressure ulcer rates), their collective work load (number of discharges, interconsultations rates), quality issues and treatment effectiveness (average hospital stay in days of their patients, number of discharged patients readmitted in 30 days) and timeliness (% of “clinically discharged” being discharged “administratively” before 12 noon on the same day, pre-surgical waiting time in days for patients programmed for surgery). Similarly, other remaining 4 hospitalization CUPs (Critical Care Hospitalization, Maternity Hospitalization, Psychiatry Hospitalization, and Medical Hospitalization) had their own respective KPIs relevant to their clinical activity, which were measured, analyzed, and improved in their respective monthly multidisciplinary meetings.
With this methodology, multidisciplinary communication and teamwork were made a systemic requirement. This methodology provided physicians and nurses an internal communication forum and made them work in multidisciplinary teams to improve results that affected them and their patients, through the participatory mechanism in management decisions of the organization. The organizational structure became process-unit based and multidisciplinary-team based, eliminating in part the problem of departmentalization. CUP teams became a part of the new management structure. On one hand, the model provided CUP teams with a mechanism to participate in all management decisions in their respective clinical processes, and on the other, it made them become accountable for the results that they themselves monitored, analyzed, and improved.
There was also systemic communication between different CUP teams, as seen in the process map (Figure 3) of the hospital, which was structured as a network of CUPs; a KPI of one CUP sometimes is the consequence of the performance of another (for example, in Medical Hospitalization CUP, the Waiting Time in days for Magnetic Resonance Imaging or Endoscopy was measured and fed back to the diagnostic process unit, seeking explanations and corrective actions). This type of systemic communication between process units eliminated at least in part the problem of compartmentalization. With this methodology, the focus was shifted to patients and the results that affected them, making the organization more patient-centered by system design, as compared to the existing departmentalized and compartmentalized structure.
Using the analogy of human organism and comparing it with organizations, it became clear that, just as an understanding of the anatomical structure was not enough to understand the physiopathology and treat a disease, the “departmental” structure was not considered to be enough to understand and treat safety and quality issues in health care; it was necessary to understand how multidisciplinary teams worked together and, what exactly they, as a group, did and did not, to understand and resolve issues related to patient safety and treatment effectiveness. CUP structure allowed physicians and nurses to collectively understand and manage the results of their process units. The benefits of CUP model included sensitized employees becoming aware of the risks for their patients, working in team with increased multidisciplinary communication, and making decisions that affected their patients and becoming accountable. As a consequence, patients faced less risk and enjoyed better quality service as safety and treatment quality indicators were monitored and improved by their own clinical teams. With all these, the organization enjoyed more satisfied employees, and higher efficiency as hospital stay duration for patients was optimized by their providers.
The CUP structure mitigated the problems of “departmentalization” and “compartmentalization” present in existing organizational structure. By integrating these CUPs, a hospital system was created. The model allowed us to manage healthcare in a network of processes (functional units) in which multiple health care providers were involved to ensure the focus on the optimal flow of patients so that safety and treatment effectiveness could be ensured, and the waiting times could be kept minimal for patients, with optimal health care costs. CUP, when defined and managed well, provided a necessary overview of the “whole”, enabling multidisciplinary communication, teamwork, internal communication, and care continuum. In summary, safer system created safer rules. Safer rules permitted safer practices. Safer practices potentially led to safety and quality.
Ethics committee exemption
This project was a management change initiative to structure the organization in multidisciplinary groups and empower them, and as it does not affect the clinical decisions of care providers, ethics committee review and approval was not needed.
Acknowledgments
The author thanks all those mentioned here, and others omitted unintentionally, for their kind participation in this project: Aguilar BM, Aljama LY, Alvarez LA, Amaya GL, Ballano CC, Barranco L, Bastida GA, Blat FMR, Bory F, Bricios AE, Brunat E, Castellano DO, Castells A, Civit CA, Claret M, Colomar PG, Cots F, Diaz NA, Escudero MM, Escribano J, Estevez RJ, Ferrand ME, Ferro FM, Garcia P, Garcia Zaldívar L, Gimeno VE, Gomar P, Grande L, Herranz CA, Lafuente CE, Lopez CMJº, Lopez MS, Martinez S, Merino A, Nebreda DMªJ, Nogues X, Orejuela GD, Pastor P, Perez M, Planas I, Pons VF, Ravantós J, Rincon RA, Riquelme GA, Rodriguez A, Salcedo AG, Sanchez M, Servitja TS, Termes E, Torrenueva P, Torres JE, Trabado M, Varverdu AL, and Vilar MJ. The author also thanks Dr Olga Pane and her clinical management team, Dr Julio Pascual, Mrs Lourdes Garcia and Dr Xavier Castells.
Disclosure
The author declares that there was no conflict of interest in carrying out this project.
References
1. Govindarajan R. Healthcare Disorder Is Curable (In Spanish). Barcelona: Marge Medica Books; 2011.
2. Grober ED, Bohnen JM. Defining medical error. Can J Surg. 2005;48(1):39–44.
3. La Pietra L, Calligaris L, Molendini L, Quattrin R, Brusaferro S. Medical errors and clinical risk management: state of the art. Acta Otorhinolaryngol Ital. 2015;25(6):339–346.
4. Makary MA, Daniel M. Medical error – the third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2996.
5.
6. Phillips DP, Bredder CC. Morbidity and mortality from medical errors: an increasingly serious public health problem. Annu Rev Public Health. 2002;23:135–150. doi:10.1146/annurev.publhealth.23.100201.133505.
7. Gartlehner G, Hansen RA, Nissman D, Lohr KN, Carey TS Criteria for distinguishing effectiveness from efficacy trials in systematic reviews. Agency for Healthcare Research and Quality Technical Reviews No. 12 and Report No. 06-0046. Rockville (MD); 2006.
8. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–2645. doi:10.1056/NEJMsa022615.
9. Govindarajan R. The Excellence in Health Sector Using ISO9001 (In Spanish). Madrid: McGraw Hill Interamericana; 2007.
10. Govindarajan R. An organizational improvement model for preventing burnout of healthcare employees. JHRSS. 2018;6:306–317. doi:10.4236/jhrss.2018.64044.
11. Mira JJ, Carrillo I, Guilabert M, et al. The second victim phenomenon after a clinical error: the design and evaluation of a website to reduce caregivers’ emotional responses after a clinical error. J Med Internet Res. 2017;19(6):e203. doi:10.2196/jmir.7840.
12. Wu Albert W. Medical error: the second victim: the doctor who makes the mistake needs help too. BMJ. 2000;320:726–727. doi:10.1136/bmj.320.7237.726.
13. Andel C, Davidow SL, Hollander M, Moreno DA. The economics of heath care quality and medical errors. J Health Care Finance. 2012;39(1):39–50.
14. Reason J. Human error: models and management. BMJ. 2000;320(7237):768–770.
15. Pierluissi E, Fischer AM, Campbell AR, Landefeld S. Discussion of medical errors in morbidity and mortility conferences. JAMA. 2003;290(21):2838–2842. doi:10.1001/jama.290.21.2838.
16. Van Den Bos J, Rustagi K, Gray T, Halford M, Ziemkiewicz E, Shreve J. The $17.1B problem: the annual cost of measurable medication errors. Health Aff (Milwood). 2011;30(4):596–603. doi:10.1377/hlthaff.2011.0084.
17. Mosadeghrad AM. Factors affecting medical service quality. Iran J Public Health. 2014;43(2):210–220.
18. Parker A, Rakes L, Arndt K. Departmentalized, self-contained, or somewhere in between: understanding elementary grade-level organizational decision-making. Educ Forum. 2017;81(3):236–255. doi:10.1080/00131725.2017.1314569.
19. Hurtado M, Swift E, Corrigan J. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press; 2001.
20. Hackman JR. Leading Teams: Setting the Stage for Great Performances. Boston: Harvard Business Press; 2002.
21. Künzle B, Kolbe M, Grote G. Ensuring patient safety through effective leadership behavior: a literature review. Saf Sci. 2010;48(1):1–17.
22. Weaver SJ, Dy SM, Rosen MA. Team training in healthcare: a narrative synthesis of the literature. BMJ Qual Saf. 2014;23(5):359–372. doi:10.1136/bmjqs-2013-001848.
23. Sommers LS, Marton KI, Barbaccia JC, Randolph J. Physician, nurse, and social worker collaboration in primary care for chronically ill seniors. Arch Intern Med. 2000;160(12):1825–1833.
24. Henkin S, Chon T, Christopherson M, Halvorsen A, Worden L, Ratelle J. Improving nurse-physician teamwork through interprofessional bedside rounding. J Multidiscip Healthc. 2016;9:201–205. doi:10.2147/JMDH.S106644.
25. Germa L. Onclogic functopnal units. Medicina Clínica. 2016;135(13):581–630. doi:10.1016/j.medcli.2010.03.017.
26. Moorman D. Communication, teams, and medical mistakes. Ann Surg. 2007;245(2):173–175. doi:10.1097/01.sla.0000254060.41574.a2.
27. Williams RG, Silverman R, Schwind C, et al. Surgeon information transfer and communication: factors affecting quality and efficiency of inpatient care. Ann Surg. 2007;245(2):159–169. doi:10.1097/01.sla.0000242709.28760.56.
28. Nagpal K, Vats A, Ahmed K, Vincent C, Moorthy K. An evaluation of information transfer through the continuum of surgical care: a feasibility study. Ann Surg. 2010;252(2):407. doi:10.1097/SLA.0b013e3181e986df.
29. Ambrosini V, Jenkins M, Mowbray N. Advanced Strategic Management, A Multi-Perspective Approach. London: Palgrave Macmillan; 2015.
30. Pj P, Sm B, Goeschel C, et al. Improving patiente safety in intensive care units in Michigan. J Crit Care. 2008;23(2):207–221. doi:10.1016/j.jcrc.2007.09.002.
31. Wick EC, Hobson DB, Bennett JL, et al. Implementation of a surgical comprehensive unit-based safety program to reduce surgical site infections. J Am Coll Surg. 2012;215(2):193–200. doi:10.1016/j.jamcollsurg.2012.03.017. Epub 2012 May 24.
32. Khan RM, Al-Juaaid M, Al-Mutairi H, et al. Implementing the comprehensive unit-based safety program model to improve the management of mechanically ventilated patients in Saudi Arabia. Am J Infect Control. 2018; pii: S0196-6553(18)30740-5. doi:10.1016/j.ajic.2018.06.022.
33. Timmel J, Kent PS, Holzmueller CG, Paine L, Schulick RD, Pronovost PJ. Impact of the Comprehensive Unit-based Safety Program (CUSP) on safety culture in a surgical inpatient unit. Jt Comm J Qual Patient Saf. 2010;36(6):252–260.
34. Govindarajan R. Failure Mode and Effects Analysis (FMEA) helps improve safety in radiation therapy. Rev Calid Asist. 2007;22(6):299–309. doi:10.1016/S1134-282X(07)71238-1.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.