Back to Journals » International Medical Case Reports Journal » Volume 19
Mounier Kuhn Syndrome – A Case Report
Authors Mutesi J ![]() , Niwagaba P, Wanda HY, Salunkhe K
, Niwagaba P, Wanda HY, Salunkhe K ![]() , Mutesi C, Kikomeko S, Baluku JB
, Mutesi C, Kikomeko S, Baluku JB ![]()
Received 28 February 2026
Accepted for publication 21 May 2026
Published 4 June 2026 Volume 2026:19 600936
DOI https://doi.org/10.2147/IMCRJ.S600936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Judith Mutesi, Peter Niwagaba, Harriet Yvonne Wanda, Kanishka Salunkhe, Caroline Mutesi, Sharif Kikomeko, Joseph Baruch Baluku
Department of Radiology, Kiruddu National Referral Hospital, Kampala, Uganda
Correspondence: Judith Mutesi, Department of Radiology, Kiruddu National Referral Hospital, P.O Box: 6588, Kampala, Uganda, Email [email protected]
Abstract: Mounier Kuhn Syndrome (MKS) is a rare chronic condition characterized by dilatation of the trachea and the major bronchi. The clinical presentation is variable, ranging from asymptomatic mild symptoms to severe diseases that can result in death. MKS often presents with chronic cough, dyspnea, and recurrent upper respiratory tract infections. Radiological imaging is important in diagnosing the condition to identify dilatation of the trachea and major bronchi with posterior tracheal diverticuli. The HRCT scan modality clearly demonstrates these features radiologically. Bronchoscopy can be used for diagnostic and therapeutic purposes. HRCT is also used to evaluate potential complications. The treatment for symptomatic individuals is conservative management. In this report, we describe the case of a 50-year-old man who presented with a productive cough for three weeks associated with headache, vomiting, and dizziness. He was found to have a grade II digital clubbing. Chest HRCT revealed tracheobronchomegaly with posterior tracheal diverticuli and bilateral distal bronchiectasis. Diagnostic bronchoscopy revealed a widened trachea with a distorted webbed appearance of the posterior and lateral walls, and bronchial secretions in the left lower lobe. A biofire test for the pneumonia panel revealed an active Haemophilus influenzae infection. The patient also had a malarial co-infection prior to admission. The patient completed an antimalarial regimen, intravenous antibiotics, and mucolytics, and was discharged upon improvement.
Keywords: Mounier Kuhn Syndrome, MKS, tracheobronchomegaly, TBM, high resolution chest computed tomography scan, HRCT
Introduction
Mounier Kuhn Syndrome is a rare chronic disease characterized by enlargement of the trachea and bronchi1–5 There is development of diverticuli posteriorly in the trachea 2,3 Pathologically, there is atrophy of the smooth muscles and elastic tissue in the trachea and the bronchi 1–3 There is a significant male predominance of 8:12,3,6,7, and among those affected, there is a positive history of smoking.1,2,6,8: Cough is the main symptom encountered; however, recurrent upper respiratory tract infections(URTI), dyspnea, hemoptysis, and wheezing 1,2,4 Diagnosis is made radiologically by confirming the tracheobronchomegaly and diverticuli, which involve X-ray and multiplanar imaging with CT and virtual bronchoscopy 4,6,8,9 Treatment is for the symptomatic individuals and varies from conservative treatment to surgical procedures and this involves; chest physiotherapy, mucolytics, antibiotics, minimal surgical techniques involve; tracheal stent placements, tracheoplasty3,10 Here, we present a 50-year old individual who presented with symptoms of pneumonia with incidental findings on computed tomography (CT) imaging and subsequent bronchoscopy that confirmed MKS with H. influenza infection.
Case Presentation
AS, a 50-year-old male was admitted to the Kiruddu National Referral Hospital, medical ward, pulmonology unit where he presented with a productive cough for three weeks with whitish sputum and was non-blood-stained. He reported on and off fever, weight loss, and drenching night sweats. There was no difficulty in breathing or chest pain. He had been recently managed for malaria around the same time as the complaints for which he received anti-malarial treatment: artemether/lumefantrine and dihydroartemisinin/piperaquine. A review of other systems revealed episodes of vomiting, headaches, and dizziness. He had a 6 pack year smoking history of over 25 years, however, he had quit smoking. The patient had a history of painting work.
On examination, he was sick looking, afebrile, and had grade 2 digital clubbing. Vitals were as follows: heart rate, 92bpm; 110/71 mmHg; oxygen saturation, 98% on room air; respiratory rate, 20bpm. The diagnostic workups are presented in Table 1.
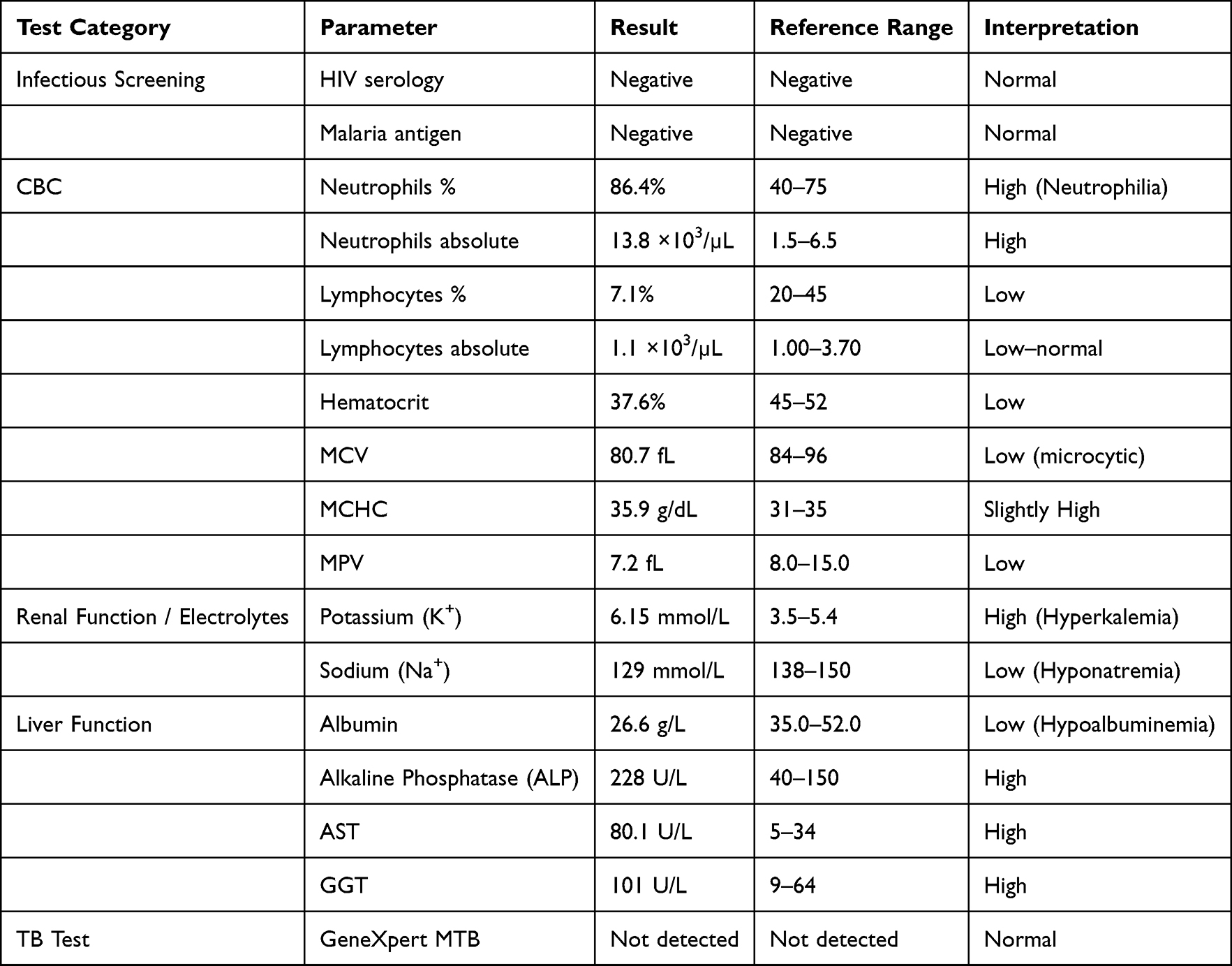 |
Table 1 Diagnostic Work up in a Patient with MKS |
Bronchoscopy performed during the current admission revealed a widened trachea with a distorted webbed appearance in the posterior and lateral walls. Webbing was also observed in bronchioles of the right lower, middle, upper, and upper lobes. Thick off-white secretions were observed in the left lower lobe, from which bronchial washings were aspirated, as well as in the left main bronchus- as shown in Figure 1.
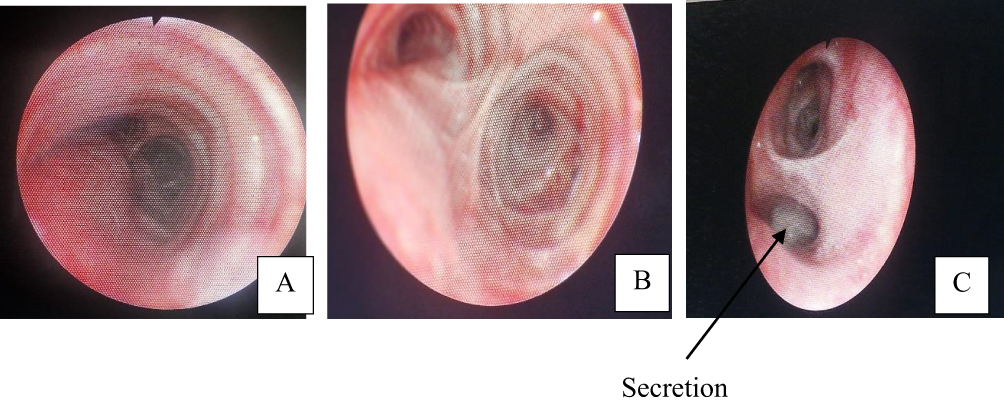 |
Figure 1 Shows images from bronchoscopy done; (A and B) show enlarged trachea and major bronchi with webbings in the walls. (C) shows an enlarged left bronchiole with a thick off white secretion as shown by the arrow. |
A high resolution chest CT was done as shown in Figures 2 and 3 featuring dilated trachea and bronchi, branching bronchioles and distal bronchioles with thickened walls. There were multiple posterior tracheal diverticuli seen.
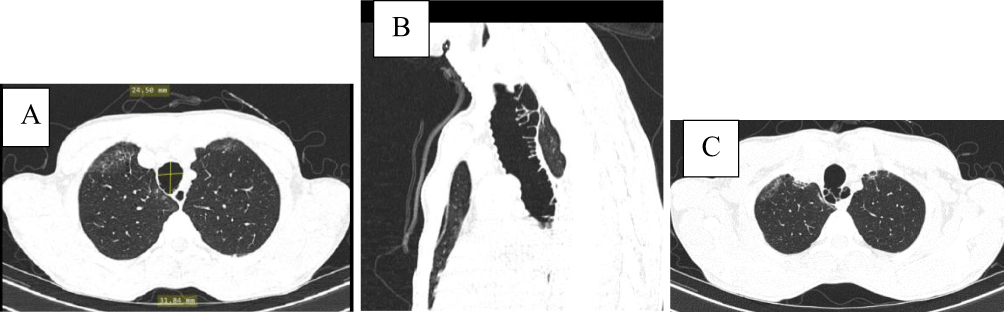 |
Figure 2 (A) (axial lung window) shows increased tracheal diameter (AP diameter-3.2cm and tranverse diameter-2.5cm), dilated bronchioles and mild subpleural septal interlobular thickening in right apical segment. (B and C) (sagittal and axial lung windows) show dilated trachea with multiple posterior diverticuli. |
 |
Figure 3 (A–C) show dilated branching bronchioles, bilateral dilated distal bronchioles in the lower lobe bases with thickening of the walls in a varicose bronchiectasis pattern. |
Diagnosis: In view of tracheobronchomegaly with posterior tracheal diverticuli and bilateral distal bronchiectasis, this was a case of Mounier–Kuhn Syndrome.
A bio-fire test was performed, which showed Hemophilus influenza infection with ≥ 107 copies/mL.
Treatment: The patient was managed for hyperkalemia with 50% dextrose, soluble insulin 10IU STAT and calcium gluconate-10 mls of 10% calcium gluconate.
He received the intravenous antibiotics-amoxicillin-clavulinic acid 1.2 g twice daily for 5 days, ceftriaxone (2 g) once daily for 5 days, and expectorant ascoril.
The patient improved with the above treatment and was discharged on the 6th day after admission.
Discussion
Mounier Kuhn Syndrome is a rare chronic condition characterized by dilatation of the trachea and major bronchi 1–5 The bronchioles are also eventually affected. Though not clearly understood, the underlying pathophysiology has been observed to be atrophy of the smooth muscles and elastic tissue in the trachea and the main bronchi 3–6 The condition is associated with recurrent upper respiratory infections, considerable morbidity and mortality.1,2,4–6,10
It has been described as congenital; however, some studies state that there are acquired cases, and it is almost always diagnosed in adults. Less than 500 cases have been reported11 and with a 0.5–1.6% prevalence.6 Studies have shown there is inheritance through an autosomal recessive gene4,10 Familial susceptibility has also been observed in siblings and cousins to those affected have also been diagnosed7 There have been acquired cases with association to connective tissue diseases including Ehlers-Danlos syndrome, Marfan Syndrome, Cutis laxa, ankylosing spondylitis, and ataxia telangiectasia 8,10,11 There is a male predominance of 8:12,3,6,7, which is commonly observed among middle-aged men and smokers2,6,8 A few cases have been reported in infants, children and elderly1 Cases have been reported among nonsmokers.8 There was no correlation between age and the degree of tracheal dilatation. Although it is commonly referred to as a congenital condition, there is literature that reports cases are acquired because they are frequently reported in adults. Acquired cases have also been observed among those with neonatal ventilation and barotrauma.7 The patient was a middle-aged man with a history of smoking; however, he had no family history of this condition.
Clinical presentations vary from asymptomatic to minor, with preserved respiratory function, severe disease, and life-threatening symptoms 9 Common clinical presentations include cough, dyspnea, and recurrent URTI 2,6,10 Wheezing and hemoptysis have also been reported1,4,8 Pathological dilatation and impaired mucociliary activity in the trachea and bronchi result in ineffective cough, increased tidal volume, and dead space with recurrent infections 6,10 On examination, these patients typically have digital clubbing, bronchial rales have also been described8 The patient in this case presented with chronic productive cough and was found to have grade II digital clubbing on examination.
The diagnosis is typically made based on radiological investigations and bronchoscopy. Often over looked on x-rays, the dilated trachea can be clearly seen on HRCT scans1, and superior multiplanar imaging on CT scans and virtual bronchoscopy can also be employed4,6,9 Diagnostic criteria measurements suggest > 3 cm for the trachea or >3SD from the mean tracheal diameter6,10, >2 cm and >1.8 cm for the right and left main bronchi 10 Tracheobronchomegaly can be classified as Type I, II and III, based on the extent of enlargement of the trachea, bronchi, and distal bronchioles. Type I involves symmetrical enlargement of the trachea and bronchi, whereas Type II involves additional diverticuli that are distinct. Type III involves dilatation of the trachea and bronchi, diverticulosis, and dilated distal bronchioles dilated7,11 Diagnostic work up is important to differentiate MKS from acquired TBM and other differential diagnoses that include; laryngocele, pharyngocele, Zenkers diverticulum9,11 CT scan imaging also assesses for any complications; emphysema, atelectasis, fibrosis, pneumothorax 8 Pulmonary function tests also have a role to play in the diagnosis of MKS and evaluating for treatment options2,10 Diagnostic bronchoscopy is used to assess the structural integrity of the trachea and bronchi. Visualization of dilated trachea and bronchi during inspiration and collapse during expiration.4,6,8,10
The diagnosis for this patient was made using chest HRCT, which revealed tracheobronchomegaly with posterior tracheal diverticuli and distal bronchiectasis, which was also confirmed and correlated with similar findings on diagnostic bronchoscopy.
Asymptomatic individuals do not require treatment, however may benefit from preventative pneumococcal and influenza vaccinations6,7,9 Symptomatic individuals can be managed by using surgical techniques. Conservative management involves chest physiotherapy, antibiotics, and mucolytics 1,4–6,10 Cessation of smoking is beneficial and minimal exposure to pollutants and irritants6,7,9 Therapeutic bronchoscopy is essential in achieving mucociliary clearance and pulmonary toilet 6 Patients with TBM may benefit from long-term continuous positive airway pressure, airway stenting, and surgical tracheoplasty. Surgical treatment modalities can be used depending on the degree of viscosity and refractoriness of secretions. Minimally invasive techniques involve airway stenting to achieve physiomechanical stabilization. Laser treatment has been employed in some patients 1,5,6,10 The patient was managed conservatively with intravenous antibiotics and mucolytics for the H.influenza infection.
Study Limitations
The diagnosis of Mounier Kuhn Syndrome in this patient is limited by the absence of dynamic chest CT imaging to confirm the tracheobronchomegaly. Additionally, comprehensive pulmonary function tests were not available, which could have provided further supportive and functional assessment.
Conclusion
Mounier Kuhn Syndrome is a rare chronic condition that commonly affects middle-aged males. It is often missed on radiography and is diagnosed using computed tomography (CT) and bronchoscopy. Morbidity is characterized by recurrent upper respiratory tract infections, recurrent hospitalizations, and eventual death in severe cases; therefore, it is important to evaluate it among patients with recurrent infections and diagnose it to enable preventative actions in asymptomatic individuals. Clinicians should maintain a high index of suspicion for MKS among adult males presenting with recurrent respiratory infections, pursue appropriate investigations to facilitate early diagnosis and help prevent associated complications. Radiological imaging is also used to evaluate complications that can be managed further.
Data Sharing Statement
All data are provided in this manuscript.
Consent for Publish
The patient described in the case report provided written informed consent to share his medical history, diagnostic workup and accompanying images. Institutional approval to publish the case details was also obtained from the Kiruddu National Referral Hospital administration.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Krustins E, Kravale Z, Buls A. Mounier-Kuhn syndrome or congenital tracheobronchomegaly: a literature review. Respir Med. 2013;107(12):1822–6. doi:10.1016/j.rmed.2013.08.042
2. Krustins E. Mounier-Kuhn syndrome: a systematic analysis of 128 cases published within last 25 years. Clin Respir J. 2016;10(1):3–10. doi:10.1111/crj.12192
3. Simon M, Vremaroiu P, Andrei F. Mounier-Kuhn syndrome. J Bronchology Interv Pulmonol. 2014;21(2):145–149. doi:10.1097/LBR.0000000000000068
4. Babirye D, Walubembe J, Babirye JA, et al. Tracheobronchomegaly (Mounier-Kuhn Syndrome) in a 43-year-old male: a case report. Int Med Case Rep J. 2022;15:631–637. doi:10.2147/IMCRJ.S386083
5. Akgedik R, Karamanli H, Kizilirmak D, et al. Mounier-Kuhn syndrome (tracheobronchomegaly): an analysis of eleven cases. Clin Respir J. 2018;12(3):885–889. doi:10.1111/crj.12600
6. Sharma S, Kuperberg SJ. State-of-the-art narrative review: mounier-Kuhn syndrome and tracheobronchomegaly. Respir Med. 2025;237:107914. doi:10.1016/j.rmed.2024.107914
7. Rjimati M, Serraj M, Elbiaze M, et al. Mounier-Kuhn syndrome (Tracheobronchomegaly): radiological diagnosis. Radiol Case Rep. 2021;16(9):2546–2550. doi:10.1016/j.radcr.2021.06.021
8. El Oualladi F, Labied M, Bouzid I, et al. A rare cause of dyspnea: Mounier Kuhn syndrome. Radiol Case Rep. 2025;20(2):1268–1272. doi:10.1016/j.radcr.2024.11.015
9. Loued L, Migaou A, Achour A, et al. Mounier-Kuhn syndrome: a variable course disease. Respir Med Case Rep. 2020;31:101238. doi:10.1016/j.rmcr.2020.101238
10. Celik B, Bilgin S, Yuksel C. Mounier-Kuhn syndrome: a rare cause of bronchial dilation. Tex Heart Inst J. 2011;38(2):194–196.
11. Wang Y, Wang L, Zhang H, et al. Mounier-Kuhn syndrome: a tripartite analysis bridging clinical epidemiology, imaging evolution, and global research landscapes. Orphanet J Rare Dis. 2025;20(1):238. doi:10.1186/s13023-025-03745-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.