Back to Journals » Local and Regional Anesthesia » Volume 19
Modified Thoracoabdominal Nerve Block Through the Perichondrial Approach versus Thoracic Epidural Analgesia for Postoperative Analgesia in Robot-Assisted Colorectal Surgery: A Retrospective Cohort Study
Authors Yamamoto T, Yoshida Y, Ochiai Y, Hayashi M, Kawaguchi K, Michida M, Matsushima M, Katayama H ![]() , Ohashi I
, Ohashi I
Received 10 March 2026
Accepted for publication 3 June 2026
Published 9 July 2026 Volume 2026:19 608149
DOI https://doi.org/10.2147/LRA.S608149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Tatsuya Yamamoto, Yukiko Yoshida, Yoko Ochiai, Masao Hayashi, Katsuhisa Kawaguchi, Masaaki Michida, Mizuho Matsushima, Hiroshi Katayama, Ichiro Ohashi
Department of Anesthesiology and Critical Care Medicine, Kawasaki Medical School General Medical Center, Okayama, Japan
Correspondence: Tatsuya Yamamoto, Department of Anesthesiology and Critical Care Medicine, Kawasaki Medical School General Medical Center, 2-6-1 Nakasange, Kita-ku, Okayama, 700-8505, Japan, Email [email protected]
Purpose: Thoracic epidural analgesia is widely considered the gold standard for postoperative pain management in abdominal surgery; however, it is associated with workflow limitations and potential hemodynamic instability. The modified thoracoabdominal nerve block through the perichondrial approach (m-TAPA) has emerged as an alternative technique for abdominal wall analgesia. This study aimed to compare the analgesic efficacy and perioperative impact of epidural analgesia and m-TAPA in patients undergoing robot-assisted colorectal surgery.
Patients and methods: This retrospective, single-center, non-randomized cohort study included 45 adult patients who underwent robot-assisted laparoscopic colorectal resection between January and October 2024. Patients received either thoracic epidural analgesia (n = 23) or bilateral single-shot m-TAPA (n = 22), selected at the discretion of the attending anesthesiologist. The primary outcome was postoperative pain intensity assessed using the Numerical Rating Scale (NRS) at 4-hour intervals. Secondary outcomes included intraoperative and postoperative opioid consumption, time from operating room entry to surgical incision, vasopressor use, and analgesia-related complications.
Results: Postoperative NRS scores were comparable between groups up to 16 hours after surgery. At 20 and 24 hours postoperatively, pain scores were significantly lower in the epidural group. Intraoperative and postoperative fentanyl consumption was significantly higher in the m-TAPA group (p < 0.01 for both comparisons). The time from operating room entry to surgical incision was significantly shorter in the m-TAPA group (p = 0.035). Postoperative bolus vasopressor therapy was more frequently required in the epidural group (p = 0.0045). The incidence of postoperative nausea and vomiting, atelectasis, neurological complications, urinary retention, and intensive care unit length of stay did not differ significantly between groups.
Conclusion: In this small retrospective cohort, m-TAPA provided comparable early postoperative analgesia but was associated with higher opioid consumption compared with epidural analgesia. Given the non-randomized design, small sample size, and differences in analgesic duration between techniques, these findings should be interpreted with caution. m-TAPA may represent a practical alternative in selected patients; however, further prospective studies are required to confirm these findings.
Keywords: m-TAPA, thoracic epidural analgesia, robot-assisted colorectal surgery, postoperative analgesia, regional anesthesia
Introduction
Robot-assisted laparoscopic colorectal surgery has become increasingly widespread over the past decade owing to its minimally invasive nature, improved visualization, and enhanced dexterity compared with conventional laparoscopic techniques.1 These advantages have translated into reduced surgical trauma, smaller incisions, and faster postoperative recovery in many patients. Nevertheless, despite these technical improvements, postoperative pain remains a clinically relevant issue, particularly during the early postoperative period, and inadequate pain control may delay mobilization, impair respiratory function, and negatively affect overall recovery.
Effective postoperative analgesia is therefore a cornerstone of perioperative management in colorectal surgery and plays a central role in enhanced recovery after surgery (ERAS) protocols.2 Traditionally, thoracic epidural analgesia has been regarded as the gold standard for postoperative pain management in major abdominal surgery because of its ability to provide excellent somatic and visceral analgesia while reducing systemic opioid requirements.3 However, epidural analgesia is not without limitations. Technical difficulty, the need for patient repositioning, and potential delays before surgical incision may compromise operating room efficiency. In addition, epidural analgesia is associated with adverse effects such as hypotension due to sympathetic blockade, urinary retention, and restrictions related to perioperative anticoagulation, which may limit its applicability in certain patient populations.2,4
These drawbacks have prompted increasing interest in peripheral truncal nerve blocks as alternatives to epidural analgesia. Among these techniques, the modified thoracoabdominal nerve block through the perichondrial approach (m-TAPA) has recently been introduced as a novel regional anesthetic technique targeting the anterior branches of the thoracic spinal nerves. In this technique, local anesthetic is injected between the internal oblique and transversus abdominis muscles caudal to the 10th costal cartilage, allowing blockade of thoracoabdominal nerves supplying the anterior abdominal wall.5,6 Anatomical studies have demonstrated that m-TAPA can achieve consistent spread across the Th7–Th11 dermatomes, which correspond to the typical incision sites in upper and midline abdominal surgery.7
Unlike epidural analgesia, however, m-TAPA primarily provides somatic abdominal wall analgesia and may provide less visceral pain control. This distinction may be particularly important in colorectal surgery, where postoperative pain includes both somatic and visceral components. Postoperative pain after colorectal surgery consists of both somatic pain arising from abdominal wall incisions and visceral pain associated with bowel manipulation and pneumoperitoneum. Because m-TAPA primarily targets thoracoabdominal nerves supplying the anterior abdominal wall, its analgesic effect is expected to predominantly reduce somatic pain rather than visceral pain.
Compared with conventional lateral transversus abdominis plane (TAP) blocks, m-TAPA is expected to provide more reliable midline analgesia because the injection point is closer to the origin of the thoracoabdominal nerves before extensive branching occurs.5 Early clinical reports and small cohort studies have suggested that m-TAPA may offer effective postoperative analgesia in various abdominal procedures, including gynecological and gastrointestinal surgery.6,8 However, the majority of available evidence remains limited to case reports or small observational studies, and direct comparisons with epidural analgesia in robot-assisted colorectal surgery are scarce.
Robot-assisted colorectal surgery represents a particularly relevant clinical setting in which the potential advantages of m-TAPA may be pronounced. Because the procedure emphasizes efficiency, minimal invasiveness, and early recovery, an analgesic technique that can be performed rapidly after induction of general anesthesia, without patient repositioning and with minimal hemodynamic disturbance, may offer practical benefits. Therefore, the present retrospective cohort study aimed to compare epidural analgesia and m-TAPA with respect to postoperative analgesic efficacy, opioid consumption, perioperative efficiency, and analgesia-related complications in patients undergoing robot-assisted colorectal surgery.
Methods
Study Design and Ethical Approval
This retrospective cohort study was conducted at Kawasaki Medical School General Medical Center. The study protocol was reviewed and approved by the Institutional Review Board of Kawasaki Medical School General Medical Center (approval number: 6510–00). Owing to the retrospective design of the study, the requirement for written informed consent was waived. This study was conducted in accordance with the Declaration of Helsinki.
Patients
Adult patients who underwent robot-assisted laparoscopic colorectal resection under general anesthesia between January 1 and October 31, 2024, were screened for eligibility. Patients were included if they received either epidural analgesia or m-TAPA as part of their perioperative analgesic management. Exclusion criteria included conversion to open surgery, incomplete medical records, or the use of alternative regional analgesic techniques.
A total of 45 patients met the inclusion criteria and were included in the final analysis. Patients were allocated to either the epidural analgesia group (Epidural group, n = 23) or the m-TAPA group (n = 22) according to the analgesic technique selected by the attending anesthesiologist. The choice of analgesic technique was based on patient characteristics, surgical factors, and anesthesiologist preference, reflecting routine clinical practice.
Anesthetic Management
General anesthesia was induced and maintained according to standardized institutional protocols in all patients. Induction agents and maintenance anesthetics were selected at the discretion of the attending anesthesiologist. Intraoperative opioid administration, including fentanyl and remifentanil, was titrated based on hemodynamic responses and surgical stimulation.
Anesthetic Management and Analgesic Techniques
The choice of analgesic technique was made at the discretion of the attending anesthesiologist based on routine clinical practice.
Thoracic epidural analgesia was performed at a thoracic level between Th9 and L1 using a standard midline or paramedian approach. After catheter placement, correct positioning was confirmed based on clinical assessment of sensory block. A continuous postoperative epidural infusion of 0.25% levobupivacaine at 4 mL/h was administered. In cases of inadequate analgesia, additional bolus dosing or alternative analgesic management was provided at the discretion of the attending anesthesiologist.
Modified thoracoabdominal nerve block through the perichondrial approach (m-TAPA) was performed bilaterally under ultrasound guidance using 40 mL of 0.25% levobupivacaine. All m-TAPA procedures were performed by anesthesiologists with more than 3 years of experience in ultrasound-guided regional anesthesia. The block was performed using a linear ultrasound probe placed along the costal margin, with needle advancement into the appropriate fascial plane under real-time visualization.
Perioperative analgesic management, including intraoperative opioid administration and anesthetic technique, was not strictly standardized and was determined by the attending anesthesiologist.
Postoperative analgesia consisted of rescue administration of intravenous acetaminophen (Acelio®) and fentanyl upon patient request or when clinically indicated. The analgesic protocol was applied similarly in both groups.
Outcome Measures
The primary outcome was postoperative pain intensity assessed using the Numerical Rating Scale (NRS), a validated measure of pain severity.5 NRS scores were recorded every 4 hours postoperatively as part of routine nursing assessments.
Secondary outcomes included intraoperative and postoperative opioid consumption, intraoperative remifentanil requirements, and time from operating room entry to surgical incision as a measure of perioperative efficiency. Analgesia-related complications were also evaluated, including postoperative nausea and vomiting, atelectasis, neurological complications, urinary retention, and intensive care unit (ICU) length of stay.
Hemodynamic outcomes included postoperative use of vasopressors (norepinephrine or phenylephrine) and the need for bolus vasopressor therapy. These variables were selected to assess the impact of each analgesic technique on circulatory stability.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are presented as counts and percentages. Group comparisons were performed using Student’s t-test or nonparametric tests where appropriate.
To account for repeated measurements of postoperative pain scores, repeated-measures analysis of variance was additionally performed to evaluate trends over time.
All statistical analyses were performed using standard statistical software, and a p-value < 0.05 was considered statistically significant.
Results
Patient Characteristics and Time to Surgical Incision
A total of 45 patients were included in the analysis, comprising 23 patients in the Epidural group and 22 patients in the m-TAPA group. Baseline patient characteristics, including age, sex, and American Society of Anesthesiologists physical status classification, were comparable between groups, with no statistically significant differences observed (Table 1).
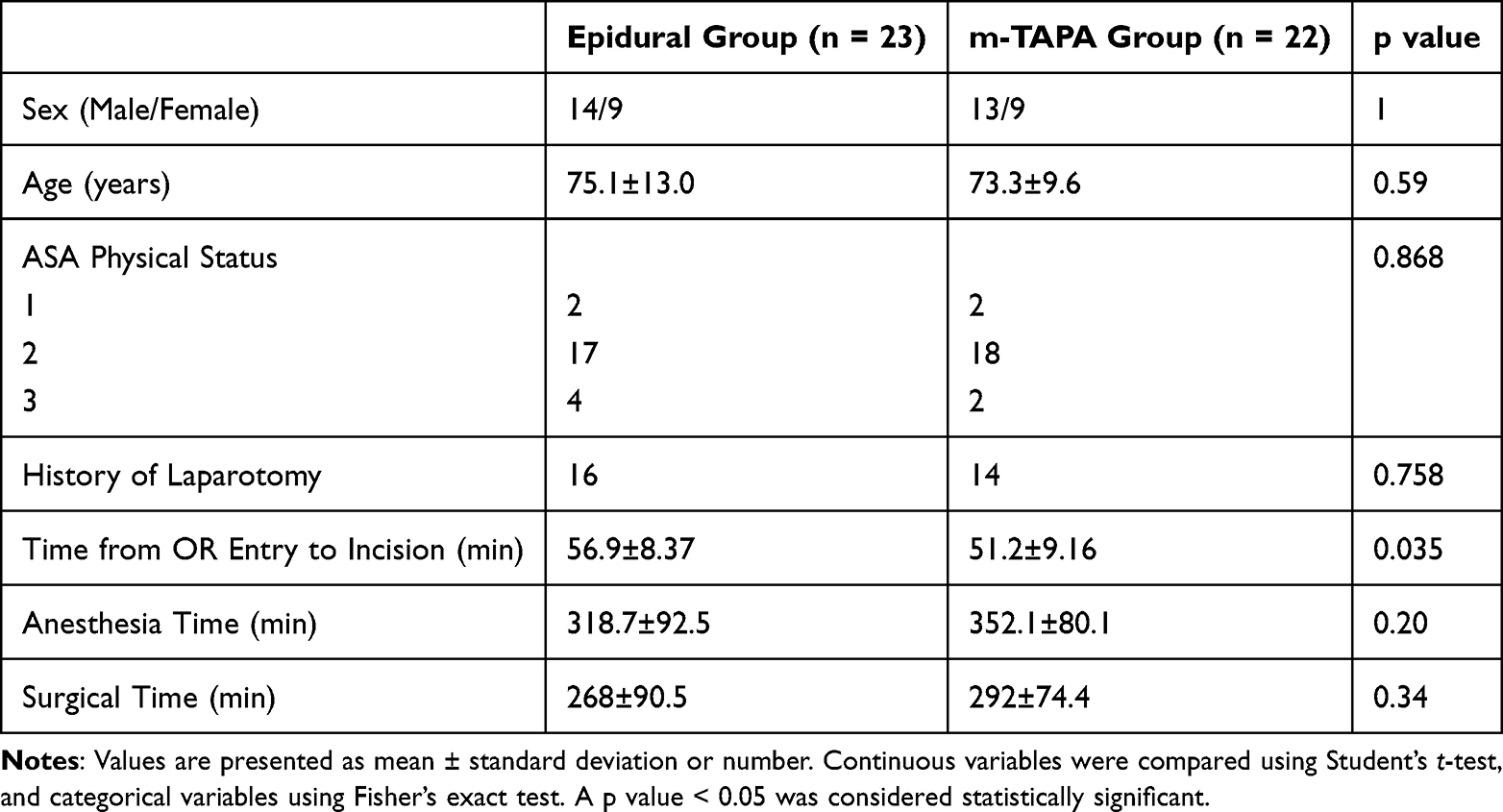 |
Table 1 Baseline Characteristics and Surgical Variables |
The time from operating room entry to surgical incision was significantly shorter in the m-TAPA group compared with the Epidural group (51.2 ± 9.16 min vs 56.9 ± 8.37 min, p = 0.035) (Table 1).
Postoperative Pain Scores and Opioid Consumption
Postoperative NRS scores at rest assessed at 4-hour intervals were comparable between groups up to 16 hours after surgery, suggesting comparable early postoperative analgesia. At 20 and 24 hours postoperatively, NRS scores were significantly lower in the Epidural group than in the m-TAPA group (p = 0.043 and p = 0.0027, respectively) (Table 2). Repeated-measures analysis of variance demonstrated a similar trend in postoperative pain scores during the early postoperative period, whereas lower pain scores were observed in the Epidural group at later time points.
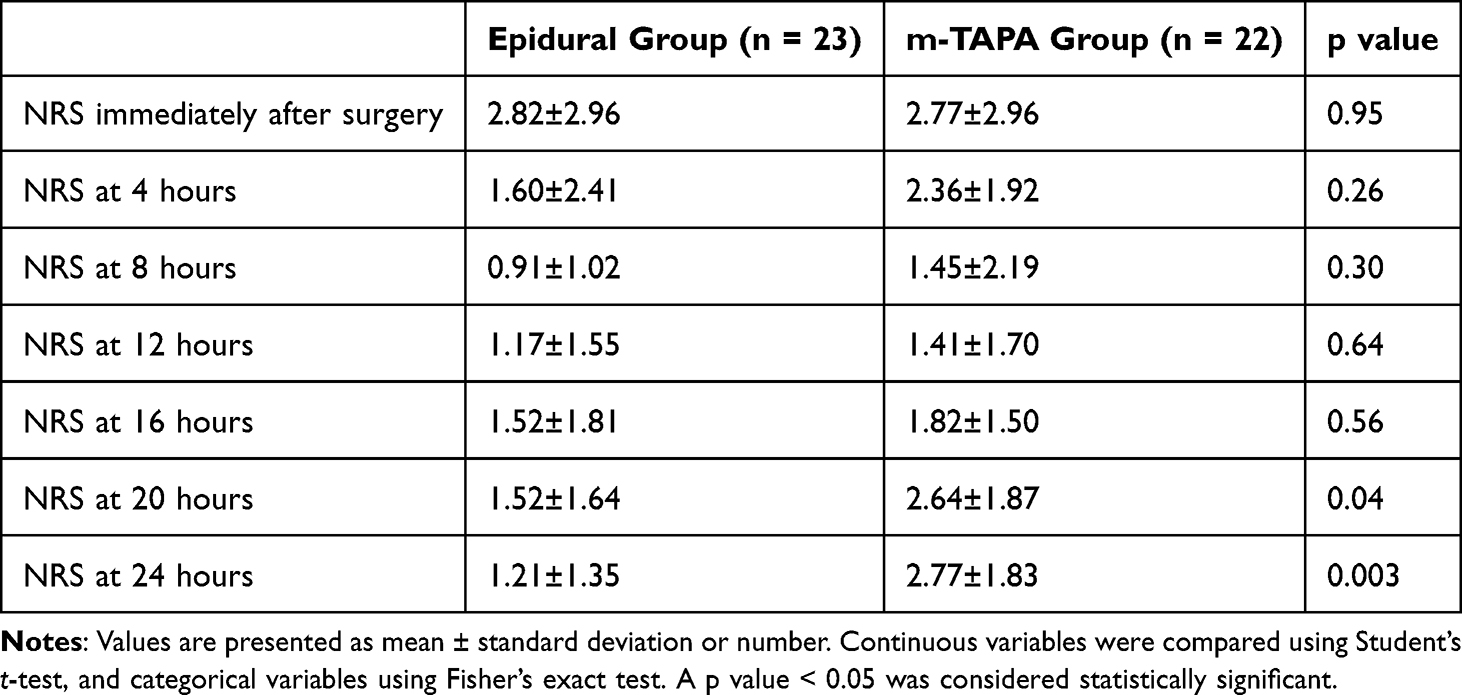 |
Table 2 Pain Scores and Opioid Consumption |
Intraoperative fentanyl consumption was higher in the m-TAPA group compared with the Epidural group (283.2 ± 97.5 μg; median 300 [IQR 200–300] μg vs 161.9 ± 88.5 μg; median 150 [IQR 100–200] μg). Similarly, postoperative fentanyl consumption was greater in the m-TAPA group (459.6 ± 157.6 μg; median 410 [IQR 394–480] μg) than in the Epidural group (98.4 ± 248.7 μg; median 0 [IQR 0–0] μg). In the Epidural group, most patients did not require additional postoperative opioid analgesia, although several patients required rescue fentanyl administration.
Hemodynamic Outcomes and Analgesia-Related Complications
Bolus vasopressor therapy was required more frequently in the Epidural group than in the m-TAPA group (13/23 vs 3/22, p = 0.0045). However, the overall use of postoperative vasopressors did not differ significantly between groups.
There were no significant differences between groups in the incidence of postoperative nausea and vomiting, atelectasis, neurological complications, urinary retention, rehabilitation progression, or intensive care unit length of stay (Table 3). No serious block-related complications were observed in either group.
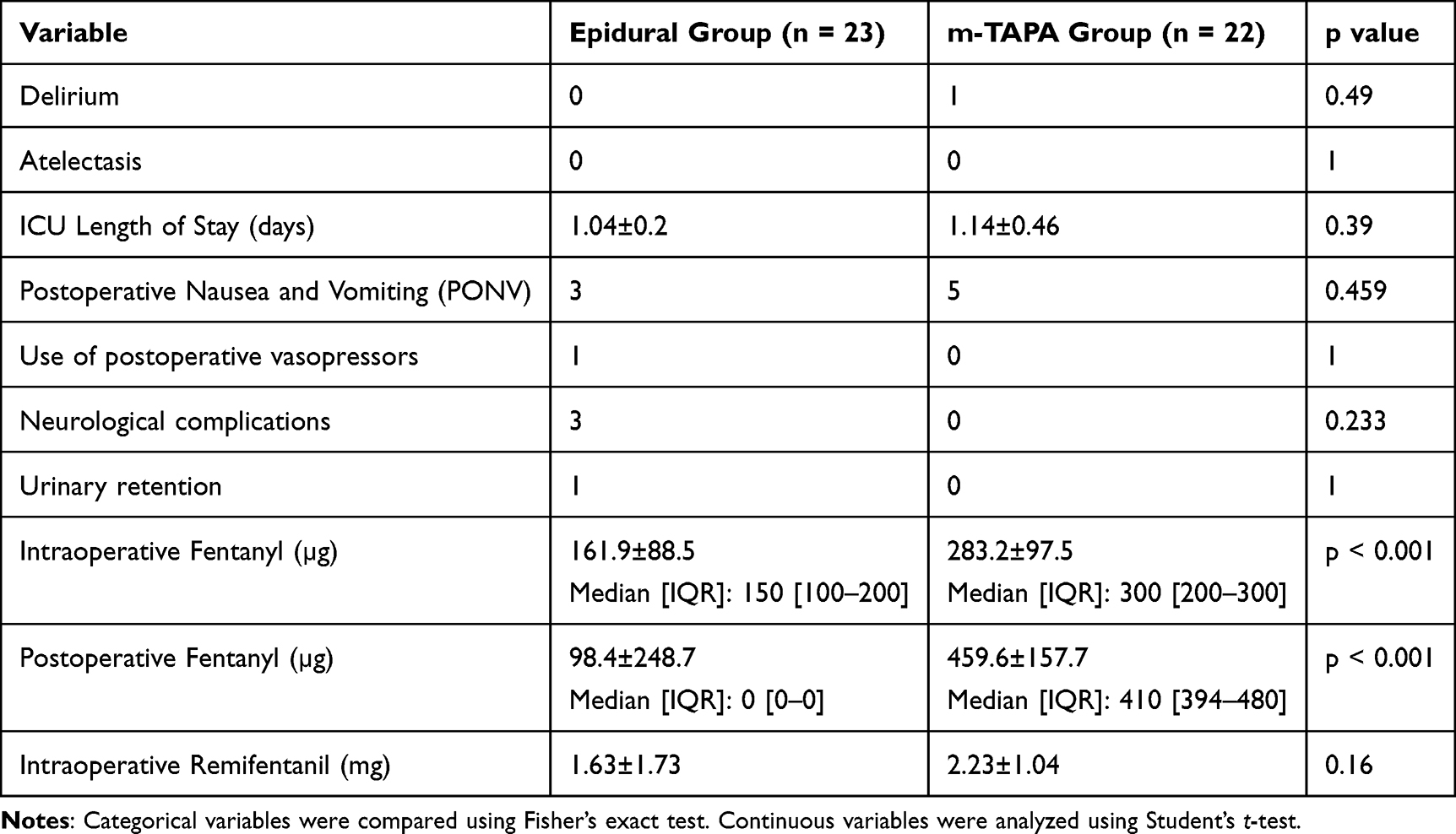 |
Table 3 Postoperative Complications |
Discussion
In this retrospective, single-center cohort study, we compared thoracic epidural analgesia and m-TAPA for postoperative pain management in robot-assisted colorectal surgery. Our results suggest that m-TAPA provides comparable early postoperative analgesia up to 16 hours after surgery, while epidural analgesia demonstrated superior pain control at later time points. In contrast, opioid consumption was higher in the m-TAPA group, indicating potential differences in analgesic efficacy.
One important consideration in interpreting these findings is the fundamental difference between the two techniques. Epidural analgesia provides continuous neuraxial blockade, including both somatic and visceral analgesia, whereas m-TAPA primarily provides somatic abdominal wall analgesia and was administered as a single-shot technique in this study. Therefore, the observed differences in pain scores at later time points and higher opioid consumption in the m-TAPA group may reflect differences in duration and coverage of analgesia rather than inherent superiority of one technique over the other.
Additionally, the increased opioid requirement observed in the m-TAPA group, despite similar early pain scores, suggests that visceral pain may not have been adequately controlled by the fascial plane block alone. This finding highlights the importance of multimodal analgesic strategies when using m-TAPA, particularly for procedures involving significant visceral components.
The comparable early postoperative analgesia observed with m-TAPA can be explained by its ability to block the anterior branches of the thoracic spinal nerves over the Th7–Th11 dermatomes, which correspond to the primary incision sites in colorectal surgery.5,7 Cadaveric studies using Thiel-fixed specimens have demonstrated consistent dye spread within this dermatomal range, supporting the anatomical basis for effective midline abdominal analgesia with m-TAPA.7 These findings align with early clinical reports describing satisfactory pain control with m-TAPA in abdominal surgery.6,8
The diminished analgesic efficacy of m-TAPA after approximately 20 hours likely reflects the inherent limitation of a single-shot fascial plane block. Previous studies have reported that the duration of analgesia with levobupivacaine-based m-TAPA is generally limited to 9–18 hours,8 which is consistent with the temporal pattern observed in the present study. From a clinical perspective, this finding highlights the importance of incorporating m-TAPA into a multimodal analgesic regimen rather than relying on it as a stand-alone technique.
Higher intraoperative and postoperative opioid requirements in the m-TAPA group may be attributable to limited visceral analgesic coverage and incomplete blockade of lower abdominal incisions below the umbilicus. Similar limitations have been reported with other truncal blocks, including TAP and quadratus lumborum blocks.9,10 Nevertheless, with appropriate opioid supplementation, m-TAPA achieved acceptable early postoperative pain control, suggesting that it can be effectively integrated into multimodal analgesia strategies.
From a perioperative workflow perspective, m-TAPA was associated with a shorter time from operating room entry to surgical incision, suggesting a potential advantage in efficiency. Furthermore, the lower requirement for vasopressor support in the m-TAPA group may reflect reduced hemodynamic instability compared with epidural analgesia.
However, several important limitations must be acknowledged. First, this was a retrospective, non-randomized study, and the choice of analgesic technique was based on anesthesiologist preference, introducing potential selection bias and confounding. Second, the sample size was small, limiting statistical power and generalizability. Third, perioperative anesthetic and analgesic management were not strictly standardized, which may have influenced pain scores and opioid consumption. Fourth, pain scores were measured repeatedly over time, and despite the use of repeated-measures analysis of variance, more advanced statistical models may still better account for within-patient correlations.
Finally, because this study compared a continuous epidural technique with a single-shot peripheral nerve block, differences in analgesic duration must be carefully considered when interpreting the results. Future prospective, randomized studies with standardized analgesic protocols and appropriate statistical modeling are needed to more definitively compare these techniques.
Conclusion
In this retrospective cohort study, m-TAPA provided comparable early postoperative analgesia but was associated with higher opioid consumption compared with epidural analgesia. Given the limitations of the study design and differences in analgesic mechanisms, these findings should be interpreted with caution. m-TAPA may be a practical alternative in selected patients; however, further prospective studies are required to confirm these findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Keller DS, Senagore AJ, Lawrence JK, Delaney CP. Comparative effectiveness of laparoscopic versus robot-assisted colorectal surgery. Ann Surg. 2014;259(4):670–7.
2. Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS). World J Surg. 2019;43(3):659–695. doi:10.1007/s00268-018-4844-y
3. Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet. 2003;362(9399):1921–1928. doi:10.1016/S0140-6736(03)14966-5
4. Liu SS, Carpenter RL, Neal JM. Epidural anesthesia and analgesia: their role in postoperative outcome. Anesthesiology. 2001;95(2):452–456. doi:10.1097/00000542-200108000-00030
5. Ohgoshi Y, Fujii Y, Kiyama S, et al. Novel external oblique muscle plane block for blockade of the lateral abdominal wall: a pilot study on volunteers. Can J Anaesth. 2022;69(10):1203–1210. doi:10.1007/s12630-022-02310-4
6. Ohgoshi Y, Fujii Y, Kiyama S, et al. External oblique muscle plane blocks in combination with modified thoracoabdominal nerves block through the perichondrial approach for analgesia in abdominal surgery: a case report. Saudi J Anaesth. 2023;17(3):413–415. doi:10.4103/sja.sja_807_22
7. Sawada A, Koyanagi T, Shigematsu-Locatelli M, et al. Modified thoracoabdominal nerve block through the perichondrial approach: an anatomical study using Thiel cadavers. Reg Anesth Pain Med. 2023;48(8):403–407. doi:10.1136/rapm-2022-104275
8. Tanaka N, Ueshima H, Otake H, et al. Efficacy of modified thoracoabdominal nerves block through the perichondrial approach in open gynecological surgery. BMC Anesthesiol. 2022;22(1):107. doi:10.1186/s12871-022-01652-2
9. Abdallah FW, Laffey JG, Halpern SH, et al. Transversus abdominis plane block: a systematic review. Anesth Analg. 2015;121(2):521–536.
10. Elsharkawy H, El-Boghdadly K, Barrington M. Truncal fascial plane blocks: clinical applications and future directions. Reg Anesth Pain Med. 2022;47(5):299–310.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.