Back to Journals » Clinical Ophthalmology » Volume 16
Modified Deep Anterior Lamellar Keratoplasty Technique to Rescue Failed Penetrating Keratoplasty
Authors Lisa C ![]() , Machado Soares R
, Machado Soares R ![]() , Fernández-Vega-Cueto L
, Fernández-Vega-Cueto L ![]() , Alfonso-Bartolozzi B, Alfonso JF
, Alfonso-Bartolozzi B, Alfonso JF ![]()
Received 19 July 2022
Accepted for publication 13 October 2022
Published 15 November 2022 Volume 2022:16 Pages 3741—3749
DOI https://doi.org/10.2147/OPTH.S382916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Modified DALK technique to rescue failed PK" [ID 382916].
Views: 948
Carlos Lisa,1,* Ricardo Machado Soares,2,* Luis Fernández-Vega-Cueto,1 Belén Alfonso-Bartolozzi,1 Jose F Alfonso1
1Cornea and Lens Department, Fernández-Vega Ophthalmological Institute, Oviedo, Spain; 2Department of Ophthalmology, Centro Hospitalar de Vila Nova de Gaia e Espinho, Porto, Portugal
*These authors contributed equally to this work
Correspondence: Ricardo Machado Soares, department of Ophthalmology, Centro Hospitalar de Vila Nova de Gaia e Espinho, Rua Conceição Fernandes, S/N, Vila Nova de Gaia, Porto, 4434-502, Portugal, Tel +35 1915045174, Email [email protected]
Purpose: To describe a modified deep anterior lamellar keratoplasty (DALK) technique to rescue failed penetrating keratoplasty (PK) grafts and report its results.
Patients and Methods: Retrospective, case-series analysis of patients who underwent modified DALK to rescue failed corneal grafts after PK was included. Every patient had corneal graft failure (GF) diagnosis due to anterior corneal (epithelium, Bowman’s, and stroma layers) or refraction disorders uncorrectable with conservative management. The main objective of the surgery and primary outcome of the study was the improvement of corrected distance visual acuity (CDVA). The study’s secondary outcome was the frequency of intra- and postoperative complications.
Results: This series included four eyes from three patients with a mean age of 57.7 years (range: 51– 63 years). Mean follow-up of patients was thirteen months (range: 12– 15 months). During follow-up, continuous improvement of corneal transparency and CDVA was observed in every patient. The only intraoperative complication reported was a peripheric DM microperforations of previous graft–host junction in two eyes. No signs of double anterior chamber, endothelial failure, GF, glaucoma, or other side effects were reported.
Conclusion: Our results suggest that modified DALK in patients with GF after PK, preserving a healthy endothelium, is surgically feasible. However, further studies are needed to compare this procedure to PK and other DALK technique variations.
Keywords: corneal transplantation, lamellar keratoplasty, graft failure, corneal diseases
Introduction
Eduard Zirm performed the first successful human penetrating keratoplasty (PK) in 1905.1 Due to remarkable improvements in surgical technique, immunology, and eye banking, PK became the standard of care for surgical treatment of corneal diseases.2 Although PK’s predominance and indications changed with the advent of lamellar keratoplasty techniques, it remains the second most performed corneal transplant technique according to the European Cornea and Cell Transplantation Registry (ECCTR) and 2019 Eye Banking Association of America (EBAA) statistical reports.3,4
Despite numerous advances in medical therapy, the increase of keratoplasties performed over the years led to a subsequent rise in graft failure (GF).5–8 In reality, GF remains the second most common indication for corneal transplantation in the ECCTR report and the most common indication for PK in ECCTR and EBAA reports.3,4 GF is defined as any irreversible central graft change preventing corneal transparency and functional vision recovery. When developed after a PK, it is primarily due to endothelial rejection or endothelial decompensation without evidence of allograft rejection.9
Management of GF after PK resides primarily in repeated PK.5,8 More recently, lamellar endothelial keratoplasty (EK) has been described and compared to PK to manage these patients.10,11 However, there are few reports regarding the use of deep anterior lamellar keratoplasty (DALK) in patients where GF after PK is due to conditions that affect anterior layers of the cornea and spare Descemet’s membrane (DM) and endothelium.12–15 In light of this, the purpose of our study is to describe a modified DALK technique to rescue failed PK grafts and report its results through a case series of patients.
Material and Methods
Study Design
Retrospective, case-series analysis of patients who underwent modified DALK to rescue failed corneal graft after PK. All surgeries were performed by the same surgeon (C.L.) at Fernández-Vega Ophthalmological Institute in Oviedo, Spain, from January to May of 2021. Every patient was educated about the time needed for visual rehabilitation, risks, benefits, and alternatives to DALK surgery and provided written informed consent. Written informed consent was also obtained from every patient regarding publishing their case details and images. This study was approved by Institute’s ethics committee and complied with the tenets of the Declaration of Helsinki for biomedical research.
Patient Selection and Ophthalmic Examination
Every patient included was submitted to modified DALK due to an established diagnosis of corneal graft failure (ICD10: T86.841) due to anterior corneal (epithelium, Bowman’s, and stroma layers) diseases (stromal scarring, vascularization, ectasia recurrence) or refraction disorders uncorrectable with conservative management (irregular high astigmatism due to small diameter and decentered grafts where contact lens fitting was not possible) (Figure 1). Patients selected for surgery also presented risk factors that would increase GF risk in case of repeated PK: glaucoma, history of rejection, and corneal neovascularization. Surgery exclusion criteria included endothelial immunological allograft rejection or endothelial failure (threshold established – endothelial cell density <600 cells/mm2 or corneal thickness >650 µm as evaluated by anterior segment optical coherence tomography).
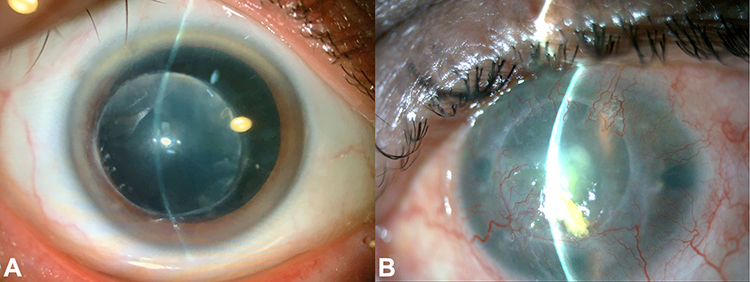 |
Figure 1 Images of patients eligible for deep anterior lamellar keratoplasty after graft failure after penetrating keratoplasty. (A) Small diameter and decentered graft with stromal opacification; (B) GF due to corneal neovascularization and stromal fibrosis. |
The main objective of the surgery and primary outcome of the study was the improvement of corrected distance visual acuity (CDVA). The study’s secondary outcome was the frequency of intra- and postoperative complications.
Patients underwent complete ophthalmological exam including CDVA (using Snellen visual acuity chart), slit-lamp examination, Goldmann applanation tonometry, manifest refraction, binocular indirect ophthalmoscopy, anterior segment optical coherence tomography (AS-OCT), corneal pachymetry (Casia SS-OCT version 2, Tomey®, Nagoya, Japan) and non-contact specular microscopy (SP-3000P, Topcon®, Japan).
Surgical Technique Description
The selected surgical technique was a modified version of Anwar’s “layer-by-layer manual dissection” technique for DALK (without small/big-bubble or intracameral air).16 Firstly, the host cornea is marked to ensure centration of trephination, paying attention to the pupil and limbus. Considering the preoperative corneal pachymetry of the patient, an 8.5 mm (outside previous PK trephination) trephine blade (Barron Radial Vacuum Trephine, Kathena®, USA) is rotated for three-quarter turns (each 60 µm deep). Afterward, approximately 1/3 of corneal stroma is dissected using a crescent blade. Subsequently, a corneal dissector and a series of curved blunt spatulas (Melles DALK spatula dissection set; DORC Instruments®, Rotterdam, Netherlands) are used to create a corneal pocket, and the stroma is smoothly dissected away from underlying DM, using curved microscissors to remove remaining stromal attachments. Corneal dissection is performed until a stromal bed of 100–120 µm in the periphery (over previous trephination) and <60 µm in the center is achieved (Figure 2). This is accomplished with the aid of real-time intraoperative optical coherence tomography (OPMI LUMERA 700, Zeiss®, Germany) and ultrasonic pachymetry (Corneo-Gage™ Plus, Sonogage®, USA).
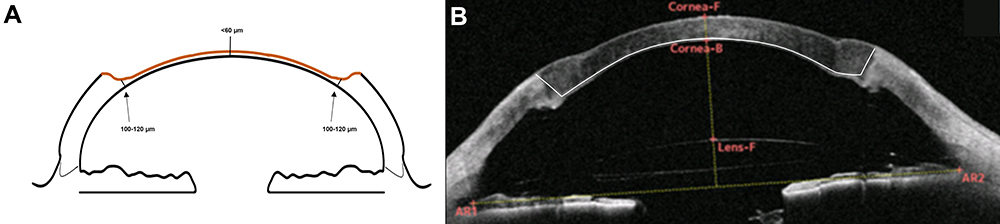 |
Figure 2 Schematic diagram of the corneal wound after stromal dissection. (A) Note the progressively thinner stromal bed towards the center of the cornea and previous penetrating keratoplasty trephination (arrow). (B) Anterior-segment optical coherence tomography showing the result of the surgery. Note the white line delineating the corneal wound configuration. |
After all corneal lamellae are removed, the donor tissue is prepared by mounting the epithelial side onto a punch block (Kathena®), and subsequent trephination (0.25- mm oversized donor button) is performed. Afterward, the donor’s cornea DM and endothelium are peeled off using a fine forceps. Finally, the lamellar donor cornea is transferred onto the host stromal bed and is sutured using interrupted 10–0 monofilament nylon sutures. Every step of the surgery is further depicted and shown in Supplementary Video.
Postoperative Care
Postoperative regimen included oral steroids for one-month, topical antibiotics, and steroids. Topical steroids were tapered by halving the dose for each time interval, and topical antibiotics were stopped after two weeks. Previous topical glaucoma agents were continued after surgery. Follow-up was assured on the first postoperative day, after one week, two weeks, and then monthly.
Results
Demographic Data
This series included four eyes from three patients with a mean age of 57.7 years (range: 51–63 years). Mean follow-up of patients was thirteen months (range: 12–15 months). During follow-up, continuous improvement of corneal transparency and CDVA was observed in every patient. The only intraoperative complication reported was a peripheric DM microperforation of previous graft–host junction. This complication happened in two eyes – one during stromal dissection and the other during suturing (vide infra). No signs of double anterior chamber, endothelial failure, GF, glaucoma, or other side effects were reported. The case series of patients included in the study is reported below. Additional clinical data pre- and post-surgery are described in Table 1.
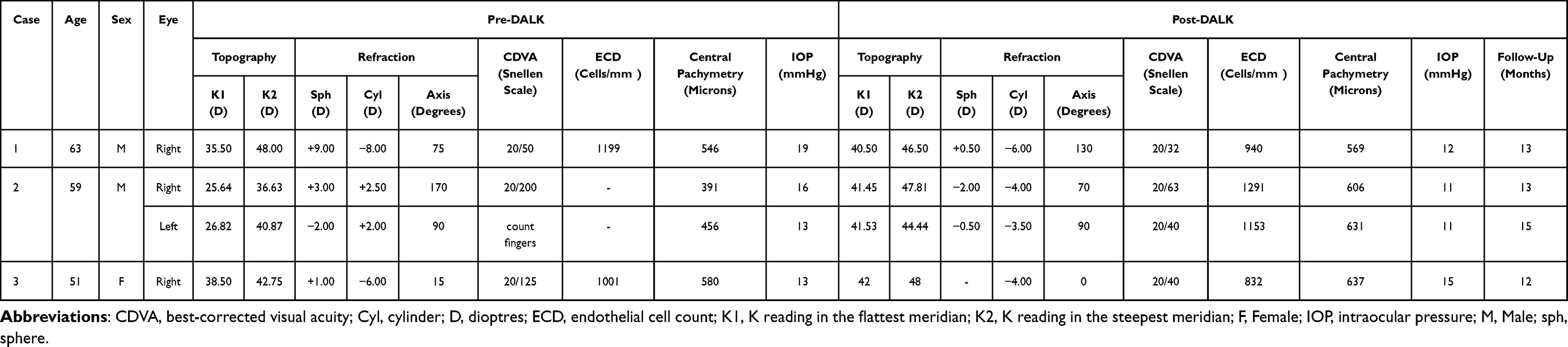 |
Table 1 Clinical Data of Patients Pre- and Postsurgery |
Case-Series Description
Case 1
A 63-year-old male, with history of PK in his right eye (OD) in 1984 due to stage 4 keratoconus (KC) and PK-induced glaucoma (under timolol and brinzolamide), presented at the ophthalmology outpatient clinic with complaints of progressively diminished visual acuity in his OD. On examination, his OD CDVA was 20/50. Biomicroscopy revealed diminished corneal transparency due to central subepithelial and stromal fibrosis, high irregular astigmatism attributable to late ectasia recurrence, and cataract (Figure 3A). A GF due to refraction disorder and subepithelial and stromal fibrosis diagnosis was made, and the patient was proposed for modified DALK triple procedure (with concomitant phacoemulsification through a 2.2 mm scleral incision after trephination and before stromal dissection). While suturing the donor graft, an opening of the donor-receptor area in the temporal side of the cornea was detected (Figure 3B). This intraoperative complication was easily solved by adding more sutures in that area (Figure 3C). Twelve months after surgery, the corneal graft remained fully transparent, perfectly positioned (Figure 3C and D), and CDVA increased to 20/32.
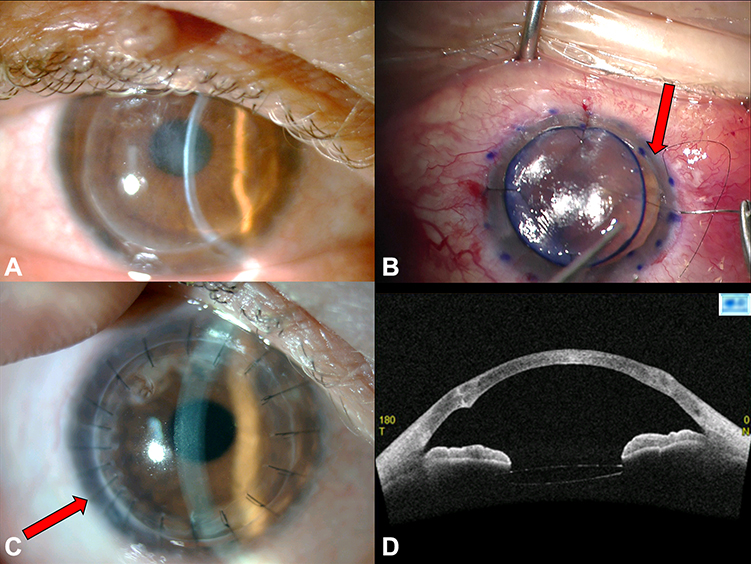 |
Figure 3 Case 1 (A) Anterior segment photograph of the right eye revealing diminished corneal transparency due to central subepithelial and stromal fibrosis; (B) Linear microperforation in the donor-receptor area in the temporal side of the cornea noted during suturing (red arrow); (C) Postoperative status of the right eye – note the increased number of sutures around the donor-receptor opening (red arrow); (D) Anterior-segment optical coherence tomography showing a perfect apposition of the corneal graft. |
Case 2
A 59-year-old male, already followed in the Institute, presented at the ophthalmology outpatient clinic with complaints of progressively diminished visual acuity in both eyes. He underwent PK in his OD (in 2004) and two PKs in his left eye (OS) (in 2005 and 2016) due to repeated corneal ulcers owing to an undetermined autoimmune disease. Additionally, the patient had history of cataract surgery in both eyes (angle supported intraocular lens) and PK-induced glaucoma (under timolol). Biomicroscopy revealed diminished corneal transparency due to long-standing lipid keratopathy (with subepithelial and stromal fibrosis) and corneal neovascularization in the OD and stromal fibrosis and corneal neovascularization in the OS (Figure 4A and B, respectively). CDVA was 20/200 in the OD and counting fingers in the OS. Endothelial function was accessed through corneal thickness (specular microscopy was not possible) measured by AS-OCT (391 µm in OD and 456 µm in OS), and the patient was proposed for bilateral modified DALK. During the OS surgery, a linear peripheric microperforation in the donor-receptor area during stromal dissection was observed and easily controlled with viscoelastic (Figure 4C). Due to his autoimmune background and inflammatory response, an amniotic membrane was applied to both anterior surfaces. At the twelfth-month appointment of OD and OS, both corneas were transparent, the grafts were perfectly positioned (Figure 4D–F), and the patient presented a CDVA of 20/63 in his OD and 20/40 in his OS.
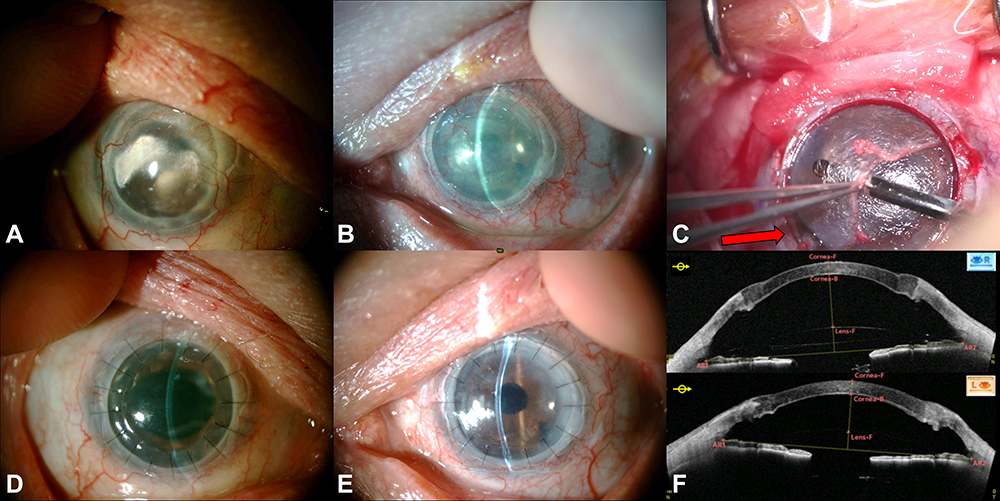 |
Figure 4 Case 2 (A) Anterior segment photography of right eye displaying lipid keratopathy (with subepithelial and stromal fibrosis) and corneal neovascularization; (B) Preoperative anterior segment photography of the left eye revealing stromal fibrosis and corneal neovascularization; (C) Intraoperative complication during left eye surgery - linear peripheric microperforation between I and II hours in the previous donor-host region (red arrow); (D and E) Postoperative anterior segment photographs of the right and left eye, respectively. (F) Anterior-segment optical coherence tomography of both eyes – note the perfect apposition of the corneal graft. AS-OCT. |
Case 3
A 51-year-old female previously followed in another center following penetrating trauma in 2014 in her OD. Due to this injury, the patient underwent corneal reconstruction, cataract phacoemulsification, and PK in the OD. This graft developed GF, and she was submitted to a second PK in 2017. In the same eye, the patient also developed PK-induced glaucoma (under timolol and dorzolamide). At the first appointment in the Institute, biomicroscopy showed some clusters of stromal fibrosis, a displaced intraocular lens (IOL), which was causing uveitis-glaucoma-hyphaema syndrome and GF due to endothelial failure. She was submitted to IOL replacement surgery (single-piece IOL to optic captured three-piece IOL) and subsequent Descemet membrane endothelial keratoplasty (DMEK). After six months of DMEK surgery, the patient presented with progressively diminished visual acuity in her OD - 20/125 - due to central stromal fibrosis (Figure 5A) despite functional endothelium (1001 cells/mm2). She was submitted to modified DALK in her OD, and surgery was uneventful. At the twelfth month postoperative appointment, CDVA increased to 20/40 in her OD, and the cornea was transparent (Figure 5B and C).
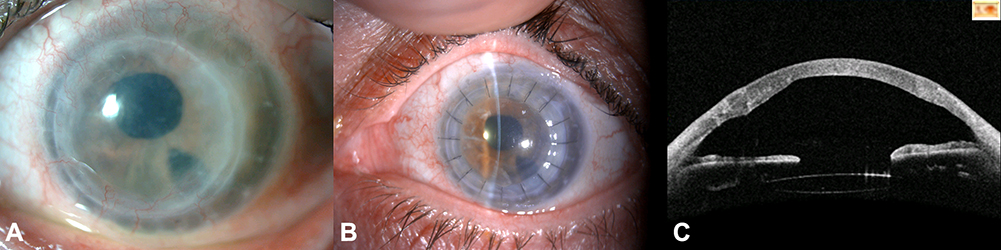 |
Figure 5 Case 3 (A) Preoperative anterior segment photo with diminished corneal transparency due to stromal fibrosis; (B) Graft after twelve months of surgery; (C) anterior-segment optical coherence tomography shows a perfect apposition between layers. |
Discussion
Anterior corneal diseases are a significant cause of GF. Al-Mezaine et al reported that corneal scars (second most common cause of GF in the study – 25.2%), KC recurrence (7.6%), and stromal dystrophies (5.7%) represented 38.5% of all GF.6 However, even in the presence of functional endothelium, repeated PK is the mainstay of treatment when GF after PK is concerned. This is particularly important as there is a significant diminish in 5-year survival between the first and second PK grafts (91.9% and 79.1%, respectively), and prognosis and overall graft survival worsen with each subsequent PK.6–8,17,18 It is hypothesized that this is due to GF turning low-risk transplants into a much higher risk category due to the greater prevalence of risk factors, namely glaucoma and use of glaucoma medication, corneal neovascularization, active ocular inflammation, anterior synechiae, and other complications related to open-sky segment surgery.8,19 PK-induced glaucoma, in particular, is considered an important cause of GF. It has an overall incidence of 21.5% (95% CI 17.8–25.7%)20 and occurs more frequently in eyes with a history of failed PK.5,6,9,19 Surgery trauma (angle distortion and collapse of trabecular meshwork, iridocorneal synechiae, and vitreous prolapse) and steroid-induced IOP elevation are some of the proposed mechanisms for this type of glaucoma.21
DALK provides advantages over PK, which are particularly important in GF patients. Firstly, DALK is an extraocular surgery without replacement of corneal endothelium, making immunological rejection negligible. This is particularly important in these patients, in whom a large-diameter PK graft (8.5 mm in our series) would lead to a greater risk of endothelial rejection. Avoiding anterior chamber’s breach could also prove beneficial in avoiding the increase of antigenic load, especially in this setting where all patients were young and may need additional transplants. Regarding glaucoma incidence, DALK does not induce PK’s angle morphological alterations, and topical corticosteroids can be discontinued earlier when compared to PK, which theoretically leads to a lower incidence of post-surgery glaucoma (<5% in 5 years).22,23 This is particularly important as glaucoma is one of the main factors that lead to GF in subsequent transplants and is present in every patient in this study. Other advantages of DALK include an earlier removal of corneal sutures and complete avoidance of other open-sky procedure-related complications.24
In this study, we described the results of modified DALK in patients with GF due to PK. All patients were young, had functional endothelium, and had a high-risk profile for GF after repeated PK. The primary outcome of improved CDVA was obtained in every patient. Regarding intraoperative complications, two peripheric DM microperforations of the previous graft–host junction were observed and easily managed. No signs of GF, endothelial failure, aggravated glaucoma, or anterior double-chamber were reported during follow-up. Regarding surgical technique, it was decided to use a modified version of Anwar’s manual DALK technique (without small/big-bubble or intracameral air). We believe that using intracameral air could lead to an increase in intraoperative complications as patients who underwent previous PK are theoretically more prone to major donor-receptor DM ruptures and wound dehiscence. Additionally, some endothelial cell loss during DALK is attributable to trauma induced by big-bubble procedure or intracameral air.24 Moreover, we further tried to avoid large donor-receptor DM ruptures by constructing a progressively thicker wound towards the periphery. This peripheral stromal crown over previous trephination provides additional tectonic support in peripheral thinning. Finally, we intentionally sparred a fine central lamella of stroma. According to several reports, visual acuities obtained by preserving this structure are not inferior to bare-Descemetic surgery after one year of follow-up.25–28 By avoiding deeper dissection, we decrease the central DM micro/macro-perforation rate and conversion to PK and double anterior chamber events.29
To our knowledge, Lake et al were the first to describe the results of manual bare-Descemet DALK in patients with previous PK due to KC. In this study, DALK was performed in seven eyes with marked ectasia in the graft–host interface. Every patient achieved an increase in visual acuity post-surgery. Regarding surgery complications, they reported four DM microperforations, two cases of dehiscence of graft–donor interface and three events of double anterior chamber.12 In 2014, Scorzia and Busin reported the results of small-bubble DALK in nine patients with GF due to previous PK. Despite the increased CDVA and low number of complications, they later reported that preventing the bubble from expanding into the PK wound was not always possible, requiring conversion to PK.13,14 When we compare our results to these studies, we also report good visual outcomes, a more controlled corneal dissection and wound construction, and absence of double anterior chamber or conversion to PK events.
More recently, Bovone et al and Busin et al published two studies describing an interesting new technique of stromal peeling in patients with GF due to previous PK. Despite the excellent results, this technique was not possible to perform in every patient: 85.7% of success (18/21 eyes) in Bovone et al study and 87.5% (84/91 eyes) in Busin et al study. In these cases, conversion to mushroom PK was necessary due to macroperforation. The DM-endothelium complex observed after stromal peeling appears to be a weak cleavage plane, making Descemet membrane perforations more challenging to manage. We hypothesize that the 50–60 microns (pre-Descemetic) residual bed obtained after our layer-by-layer manual dissection may be of added value in cases where stromal peeling is not obtainable or where perforations are expected. However, further studies are needed to confirm this. They also reported a relatively high number of double anterior chamber events – 44% (8/21 eyes) and 22% (22/91 eyes) – which were solved by injecting intracameral air during postoperative follow-up.14,15 Additionally, as reported in other studies, we believe that the stepped stromal wound of this surgical technique could affect the posterior curvature regularity and cause a curvature disparity.30,31 For this reason, attaching the residual bed could fail despite the absence of micro-perforations and a future DMEK procedure could also be affected by this posterior irregularity.32 Nevertheless, this is an exciting technique that can prove helpful in the future.
Additionally, careful monitoring of these patients is essential since they may need a future EK due to their relatively low endothelial cell density.
Over the years, the increasing number of corneal transplantation surgeries led to an increase in GF, which will only grow in the foreseeable future. Envisioning this increase, an adequate standard of care for these cases is paramount. Notwithstanding its steeper learning curve compared to PK, DALK surgery has many advantages that should be considered when the appropriate patient presents. Our results suggest that modified DALK to rescue failed PKs could be an effective option in patients with GF due to anterior corneal diseases. However, further studies are needed to compare this procedure to PK and other DALK technique variations.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work. The authors do not have any financial disclosures or conflicts of interest to disclose. The authors alone are responsible for the writing and content of the article.
References
1. Zirm EK. Eine erfolgreiche totale Keratoplastik (A successful total keratoplasty). 1906. Refract Corneal Surg. 1989;5(4):258–261. doi:10.3928/1081-597X-19890701-12
2. Crawford AZ, Patel DV, McGhee CN. A brief history of corneal transplantation: from ancient to modern. Oman J Ophthalmol. 2013;6(Suppl 1):S12. doi:10.4103/0974-620X.122289
3. Dunker SL, Armitage WJ, Armitage M, et al. Practice patterns of corneal transplantation in Europe: first report by the European cornea and cell transplantation registry. J Cataract Refract Surg. 2021;47(7):865–869. doi:10.1097/J.JCRS.0000000000000574
4. EBAA Eye banking statistical report 2019. Eye Bank Association America; 2020:1–110. Available from: www.restoresight.org.
5. Patel NP, Kim T, Rapuano CJ, Cohen EJ, Laibson PR. Indications for and outcomes of repeat penetrating keratoplasty, 1989–1995. Ophthalmology. 2000;107(4):719–724. doi:10.1016/S0161-6420(00)00003-8
6. Al-Mezaine H, Wagoner MD. Repeat penetrating keratoplasty: indications, graft survival, and visual outcome. Br J Ophthalmol. 2006;90(3):324. doi:10.1136/BJO.2005.079624
7. Aboshiha J, Jones MNA, Hopkinson CL, Larkin DFP. Differential survival of penetrating and lamellar transplants in management of failed corneal grafts. JAMA Ophthalmol. 2018;136(8):859. doi:10.1001/JAMAOPHTHALMOL.2018.1515
8. Claesson M, Armitage WJ. Clinical outcome of repeat penetrating keratoplasty. Cornea. 2013;32(7):1026–1030. doi:10.1097/ICO.0B013E31828A2810
9. Alio JL, Montesel A, Sayyad F, Barraquer RI, Arnalich-Montiel F, Barrio JLA. Corneal graft failure: an update. Br J Ophthalmol. 2021;105(8):1049–1058. doi:10.1136/BJOPHTHALMOL-2020-316705
10. Wang F, Zhang T, Kang YW, He JL, Li SM, Li SW. Endothelial keratoplasty versus repeat penetrating keratoplasty after failed penetrating keratoplasty: a systematic review and meta-analysis. PLoS One. 2017;12:7. doi:10.1371/JOURNAL.PONE.0180468
11. Ang M, Ho H, Wong C, Htoon HM, Mehta JS, Tan D. Endothelial keratoplasty after failed penetrating keratoplasty: an alternative to repeat penetrating keratoplasty. Am J Ophthalmol. 2014;158(6):1221–1227.e1. doi:10.1016/J.AJO.2014.08.024
12. Lake D, Hamada S, Khan S, Daya SM. Deep anterior lamellar keratoplasty over penetrating keratoplasty for host rim thinning and ectasia. Cornea. 2009;28(5):489–492. doi:10.1097/ICO.0B013E31818D3B3C
13. Scorcia V, Beltz J, Busin M. Small-bubble deep anterior lamellar keratoplasty technique. JAMA Ophthalmol. 2014;132(11):1369–1371. doi:10.1001/JAMAOPHTHALMOL.2014.2756
14. Bovone C, Nahum Y, Scorcia V, et al. Stromal peeling for deep anterior lamellar keratoplasty in post-penetrating keratoplasty eyes. Br J Ophthalmol. 2022;106(3):336–340. doi:10.1136/BJOPHTHALMOL-2020-316653
15. Busin M, Bovone C, Scorcia V, et al. Ultrastructural alterations of grafted corneal buttons: the anatomic basis for stromal peeling along a natural plane of separation. Am J Ophthalmol. 2021;231:144–153. doi:10.1016/J.AJO.2021.06.005
16. Anwar M. Dissection technique in lamellar keratoplasty. Br J Ophthalmol. 1972;56(9):711–713. doi:10.1136/BJO.56.9.711
17. Tan DTH, Janardhanan P, Zhou H, et al. Penetrating keratoplasty in Asian eyes: the Singapore corneal transplant study. Ophthalmology. 2008;115:6. doi:10.1016/J.OPHTHA.2007.08.049
18. Williams KA, Keane MC, Coffey NE, Jones VJ, Mills RA, Coster DJ The Australian corneal graft registry 2018 report; 2018. Available from: https://dspace.flinders.edu.au/xmlui/handle/2328/37917.
19. Kitazawa K, Wakimasu K, Kayukawa K, et al. Moderately long-term safety and efficacy of repeat penetrating keratoplasty. Cornea. 2018;37(10):255–259. doi:10.1097/ICO.0000000000001694
20. Wu S, Xu J. Incidence and risk factors for post-penetrating keratoplasty glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12:4. doi:10.1371/JOURNAL.PONE.0176261
21. Dada T, Aggarwal A, Minudath K, et al. Post-penetrating keratoplasty glaucoma. Indian J Ophthalmol. 2008;56(4):269. doi:10.4103/0301-4738.41410
22. Huang OS, Mehta JS, Htoon HM, Tan DT, Wong TT. Incidence and risk factors of elevated intraocular pressure following deep anterior lamellar keratoplasty. Am J Ophthalmol. 2016;170:153–160. doi:10.1016/J.AJO.2016.07.025
23. Liu H, Chen Y, Wang P, et al. Efficacy and safety of deep anterior lamellar keratoplasty vs. penetrating keratoplasty for keratoconus: a meta-analysis. PLoS One. 2015;10(1). doi:10.1371/JOURNAL.PONE.0113332
24. Reinhart WJ, Musch DC, Jacobs DS, Lee WB, Kaufman SC, Shtein RM. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty a report by the American academy of ophthalmology. Ophthalmology. 2011;118(1):209–218. doi:10.1016/J.OPHTHA.2010.11.002
25. Mohammadpour M, Maleki S, Hashemi H, Beheshtnejad AH. Recurrent corneal perforation due to chronic graft versus host disease; a clinicopathologic report. J Ophthalmic Vis Res. 2016;11(1):108–111. doi:10.4103/2008-322X.180705
26. Feizi S, Javadi MA, Rastegarpour A. Visual acuity and refraction after deep anterior lamellar keratoplasty with and without successful big-bubble formation. Cornea. 2010;29(11):1252–1255. doi:10.1097/ICO.0b013e3181d83710
27. Knutsson KA, Rama P, Paganoni G. Modified big-bubble technique compared to manual dissection deep anterior lamellar keratoplasty in the treatment of keratoconus. Acta Ophthalmol. 2015;93(5):431–438. doi:10.1111/aos.12705
28. Hashish AM, El-Awady HE, Sabry DM, Awad EA. Assessment of corneal densitometry in big-bubble dissection versus manual dissection deep anterior lamellar keratoplasty. Cornea. 2022;41(5):593–597. doi:10.1097/ICO.0000000000002815
29. Elbaz U, Kirwan C, Shen C, Ali A. Avoiding big bubble complications: outcomes of layer-by-layer deep anterior lamellar keratoplasty in children. Br J Ophthalmol. 2018;102(8):1103–1108. doi:10.1136/BJOPHTHALMOL-2017-310962
30. Sarnicola V, Sarnicola E, Sarnicola C. Recovery techniques in DALK. In Holland E, editor. Cornea.
31. Sarnicola E, Sarnicola C, Sarnicola V. Deep anterior lamellar keratoplasty: surgical technique, indications, clinical results and complications. InCornea. 2015;6:81–101. doi:10.1159/000381495
32. Einan-Lifshitz A, Belkin A, Sorkin N, et al. Descemet membrane endothelial keratoplasty after penetrating keratoplasty: features for success. Cornea. 2018;37(9):1093–1097. doi:10.1097/ICO.0000000000001628
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Changing Strategies in Keratoplasty After Corneal Hydrops: From Penetrating to Lamellar Approaches – A Narrative Review
Fairaq R, Kirat O, AlMutlak M, Ahad MA, Khan O, AlDayel A, Khan SA, Alshareef M, Alghamdi WS, Bin Helayel H
Clinical Ophthalmology 2026, 20:568953
Published Date: 13 February 2026