Back to Journals » Open Access Journal of Contraception » Volume 11
Modern Contraceptive Method Utilization and Associated Factors Among Women of Reproductive Age in Gondar City, Northwest Ethiopia
Authors Oumer M ![]() , Manaye A, Mengistu Z
, Manaye A, Mengistu Z ![]()
Received 8 March 2020
Accepted for publication 11 June 2020
Published 24 June 2020 Volume 2020:11 Pages 53—67
DOI https://doi.org/10.2147/OAJC.S252970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Mohammed Oumer,1,2 Agmas Manaye,3 Zelalem Mengistu4
1Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia; 2Department of Human Anatomy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia; 3Departments of Nursing, College of Medical Sciences, MTY Abyssinia Medical Science College, Gondar, Amhara, Ethiopia; 4Department of Gynecology and Obstetrics, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia
Correspondence: Mohammed Oumer Email [email protected]
Background: Family planning is defined as the ability of couples or individuals to attain their desired number of children, spacing, and timing of their births with the use of contraceptive methods. Ethiopia is one of the most populated countries in Africa with a high fertility rate, a highly unmet need for family planning, and low contraceptive utilization.
Objective: This study aims to assess modern contraceptive method utilization and associated factors among women of reproductive age in Gondar City, Northwest Ethiopia.
Materials and Methods: A community-based cross-sectional study design was undertaken with 708 women in the reproductive age in Gondar City, using a structured questionnaire combined with face-to-face interviews. Descriptive analysis, binary, and multivariable logistic regression analyses were applied to analyze the data.
Results: In this study, 41.2% of the respondents utilized modern contraceptive methods. Of the study participants, 52.1 % had good knowledge and 45.3% had a favorable attitude towards modern contraceptive methods. After adjusting for covariates, the odds of using modern contraceptive methods were 3.6 times, 4.7 times, 2.4 times, and 4 times higher among women of the age 20– 24, 25– 29, preparatory education, and degree holders, respectively. In addition, for the women having up to six desired children [AOR (Adjusted Odds Ratio) = 2.4 (95% CI: 1.1, 5.3)], a history of no-child death experience [AOR= 4.4 (95% CI: 1.03, 19.1)], good knowledge [AOR= 4.1 (95% CI: 2.7, 6.0)], and favorable attitude [AOR= 3.5 (95% CI: 2.4, 5.1)] were positively associated with modern contraceptive utilization.
Conclusion: The majority of participants had good knowledge about, but the unfavorable attitude towards the utilization of modern contraceptive methods. Therefore, the authors recommended that special awareness creation with the help of health education interventions should be employed in the community.
Keywords: modern contraceptive utilization, knowledge, attitude, reproductive age, Gondar City, Ethiopia
Background
Modern contraceptive use and unmet need for family planning are key to understanding profound changes in fertility and improving reproductive health worldwide.1 Although contraceptive utilization has increased in many parts of the world, especially in Asia and Latin America, it continues to be low in Sub-Saharan Africa. The global use of modern contraception has risen from 54% in 1990 to 57.4% in 2015 while it has risen from 23.6% to 28.5 % in Africa.2,3
Globally, the unmet need for contraception remains very high due to the lack of family planning services; more than 350 million couples have no access to family planning services.3–5 In Global South countries, there are 214 million women within the reproductive age group (15–49 years) who want to avoid pregnancy but have no access to use contraceptive methods. The unmet need for modern contraception among women of the reproductive age accounts for 24.2% in Africa.3 This, in turn, has a negative effect in the wider development of African countries, contraception use contributes to countries; social and economic development and it is important to achieve the Millennium Development Goals by improving child and maternal health.2
In Sub-Saharan African countries, at least thirty women die from the complications of pregnancy and delivery every hour and about 270,000 deaths occur every year. Their fertility rate (5.4 births per woman) is higher than in any other part of the world. This fertility rate doubles that of Asian countries (excluding China) and triples the fertility rate of Europe. The proper use of contraceptive methods can reduce the number of maternal morbidity and mortality by reducing the number of women who are at risk of unwanted pregnancy.2,5
In East Africa, the contraceptive use proportion among women of reproductive age is generally higher than in the Sub-Saharan region as a whole. However, there are differences when comparing individual countries (twenty-nine percent for Ethiopia and forty-six percent for Kenya in 2015, for example).2
Ethiopia is the second most populated country in Africa (more than 91.73 million); its population size multiplied by almost six times over one century, from 11.5 million in 1900 to 74 million in 2007.5–8 Currently, the government of Ethiopia is committed to improving the health status of its population and the country has prepared a national adolescent and youth health strategy 2016–2020 in line with the global strategy for Women’s, Children’s, and Adolescent’s Health.9,10 Ethiopia will continue working to improve the health status of adolescents and youth by increasing the modern contraceptive prevalence rate among women ages 15 to 19 years from thirty-two percent into forty percent and ages 20 to 24 years from thirty-eight percent to forty-three percent; reducing the unmet need for modern contraception among women ages 15 to 19 years from twenty percent to ten percent and among women ages 20 to 24 years from eighteen percent into ten percent.9,10
Even if Ethiopia set commitments to achieve a national modern contraceptive prevalence (for all women) of 55% and a total fertility rate of 3.0 in 2020, the reported (2020 projected) national modern contraceptive prevalence and the total fertility rate is at 26.2% and 3.2, respectively. In addition, there is still an unmet need (2020 unmet need for modern contraception is 23.4%) of women of reproductive age for contraception in the country, which is especially strong in rural areas of Ethiopia.5–10 However, access to the contraceptive services has been increasing due to the expansion of different health care services in the country.11,12
Regionally, the contraceptive prevalence differs in published literature depending on the region in Ethiopia.2,13-15 The prevalence rate of contraceptive methods for Addis Ababa, Amhara Region, Debat Health and Demographic Surveillance System Site, and Dembia District was 63%, 46.9%, 32.5 %, and 31.7%, respectively.14–17
As evidence from previously published studies has shown, modern contraceptive utilization is influenced by socioeconomic, demographic, geographical, cultural, and psychological factors.2,12,15,18,19 Some of these factors include the age of women, their educational status, or the educational status of their husbands, the number of children they have, the number of desired children, the number of live births, their overall attitude on family planning, and the knowledge on family planning.2,17,18,20-24
Maternal and neonatal death as consequences of pregnancy, labor, and delivery is one of the priorities of action nationally as well as internationally in recent years. Improving the usage of contraceptive methods is crucial to reduce maternal and child mortality and to improve the socio-economic development of the communities, zonal, regions, and the nation as a whole. The prevalence of modern contraceptive method utilization in different parts of the Amhara region is found to be low and it varies from place to place. Therefore, the aim of this study is to assess the knowledge and attitude towards modern contraceptive methods and the prevalence of modern contraceptive method utilization and its associated factors among women of the reproductive age in Gondar City.
Materials and Methods
Study Design and Settings
The community-based cross-sectional study design was applied. The study was performed in Gondar City, Amhara Regional State, Northwest Ethiopia from the period of 02/01/2018 to 16/04/2019. Gondar City is located 738 km Northwest of Addis Ababa and 170 km North of Bahir-Dar, the capital city of the Amhara Region. According to the national reports conducted by the Central Statistical Agency of Ethiopia, Gondar City has a total population of 360,600, of which 184,007 are women and 176,593 are men. There are 87, 682 females in the reproductive age group (the age between 15 and 49 years). The city has twenty-one Kebeles (local administrative areas) divided into six sub-cities, one comprehensive specialized hospital, and eight governmental health centers.25
Sample Size and Sampling Technique
The sample size was calculated using a single population proportion formula; by considering the P- value of 35% from a previous study,26 at 95% confidence interval (CI), 5 % margin of error and 5 % non-response rate (17.0 women). n= z(1-α/2)2 * P (1-P)/d2, (1.96)2 x 0.35 x 0.65/0.0025, (n = 349.6 = n = 349.6 +17 = 366.6, n= 367). This calculated sample size was doubled (x2) to minimize the design effect of the multistage cluster sampling technique; therefore, the final sample size was 734 women.
The multistage cluster sampling technique was used to identify the sub-cities and Kebeles. Among six sub-cities (namely, Arada, Fasil, Jantekel, Zobel, Maraki, and Azezo-Tseda sub-city) found in Gondar City, three sub-cities (Arada, Jantekel, and Maraki) of them were selected randomly using the lottery method. This study also utilized the lottery method to select five Kebeles from three sub-cities (Namely, Kebele six with a proportionate sample size of 153, Kebele nine = 152, Kebele ten =130, Kebele eleven =161, and Kebele eighteen=138) and used systematic sampling methods to select the study participants. The sample size for each of the selected Kebeles was allocated proportionally to the size of the women in the reproductive age of each Kebele (ni = n/N*Ni). Besides, the Kth interval (k = 59) was calculated by using the estimated number of women of the reproductive age to the sample size. All randomly selected women of reproductive age who had lived for the last six months in the selected Kebeles of Gondar City during the data collection period were included in the study. Women who were unable to communicate, seriously ill, or had severe mental health problems during the data collection period were excluded.
Study Variables
Modern contraceptive currently using is a dependent variable.
The knowledge and attitude about modern contraceptives are the secondary outcome variables.
Independent variables include socio-demographic variables: The age of the women, religion, ethnicity, marital status, educational status of the women and their husbands, the occupation of the women and their husbands, and the monthly income of the family. And, reproductive and maternal variables: History of pregnancy, age at first pregnancy, the number of pregnancies, all live newborn deliveries, the number of children live, the number of children desired, family size, knowledge, and the attitude about modern contraceptive utilization.
Operational Definition
Women of the reproductive age group: The women’s age ranged between 15 and 49 years.
Modern contraceptive utilization: When a woman in the reproductive age reported using any method of modern family planning or contraceptives (eg injectable, regular pills, emergency pills, Implanon, intrauterine device, condom, and surgical methods).
Knowledge
When talking about “knowledge” it refers to the know-how about contraceptive methods. Women’s knowledge level about the contraceptive method was measured by using 18 knowledge-related questions (18-point scale items). All knowledge variables were computed (each correct response was given a score of 1 and a wrong response was given a score of 0) to differentiate between good and poor knowledge. A higher overall score indicated better knowledge in regards to contraceptive methods (possible scores ranged from 0 to 18). The knowledge level classification is based on previously conducted studies on related matters. The responses of those who scored the mean value and above in the knowledge-related questions were categorized into as having good knowledge and those who scored below the mean value were labeled as having poor knowledge.27,28
Good knowledge: Participants who responded to the mean (9.2) and above of the total knowledge questions had good knowledge about modern contraceptive methods.
Poor knowledge: Participants who responded below the mean (9.2) of the total knowledge questions had poor knowledge about modern contraceptive methods.
Women’s comprehensive knowledge about contraceptive methods was assessed using the main components of contraceptive methods, such as the knowledge of the respondents on the type of contraceptive methods they know, their understanding of the purpose of using contraceptive methods, and their consciousness about how and where contraceptive methods can be found.
Attitude
Under “attitude”, the research term understood women’s views and opinions towards the contraceptive methods. Women’s attitude about contraceptive methods was measured with the help of 10 attitude-related questions using a five-point Likert Scale. The questions on the Likert scale had positive and negative responses that ranged from strongly agree to, agree, neutral (neither agree nor disagree), disagree, and strongly disagree. The scoring system used with respect to the participant’s responses was as follows: strongly agree 5, agree 4, neutral 3, disagree 2, and strongly disagree 1. The order of scoring for negative statements was reversed. The attitude responses were summed-up and a total score was obtained for each respondent. The mean was calculated and those who scored the mean value and above had a favorable attitude and the ones who scored below the mean value had an unfavorable attitude towards the contraceptive method.27,28
Favorable attitude: Participants who answered higher than or equal to the mean (30.0) in the attitude questions had a favorable attitude towards modern contraceptive methods.
Unfavorable attitude: Participants who answered below the mean (30.0) in the attitude questions had an unfavorable attitude.
Women’s comprehensive attitude towards modern contraceptive methods (the women were able to rank the extent to which they agreed or disagreed with the following negative attitudes towards contraceptive methods) was assessed asking about their opinions on perception such as “short-acting contraceptives are more effective than long-acting contraceptives”, “the side effects of contraceptives are dangerous to the mother” or, “ having many children helps to improve the income of the family”, “contraceptive use causes infertility in women”, “child mortality is compensated by many births”, or “contraceptive usage decreases sexual satisfaction”. In addition, the participants were able to rank the extent to which they agreed or disagreed with the following positive attitudes towards contraceptive methods: “contraceptives help the couple to become responsible parents”, “child spacing helps to protect the health of mothers and children”, “contraceptives help a mother to regain her strength for the next baby”, and “the husband should share the responsibility of the contraceptive use”.
Data Collection Tools, Techniques, and Procedures
The data were collected through face-to-face interviews using a structured Amharic questionnaire. The questionnaire was first prepared in English, translated into Amharic (local language), and later, back to English to ensure the accuracy of the meaning. The data collection questionnaire was adapted using tools used to assess contraceptive utilization in previous studies with similar aims.2,5,7,17,18,26,29 The questionnaire was designed to have six sub-topics. Namely, socio-demographic, reproductive and maternal, source of information, knowledge, attitude, and utilization-related characteristics. Trained clinical nurses collected the data. After the data collection with each participant, health education or information was provided about modern contraceptive methods. The questionnaire was pre-tested in similar settings by the investigators before the data collection on 5 % of the total sample size.
Data Processing and Analysis
The collected data were checked for completeness, accuracy, and clarity. The collected data were analyzed by the investigators using Version 14.0 Stata Statistical Software. The coding and missing values were considered before analysis. Descriptive analysis was done to describe the frequency and percentage of dependent and independent variables. Binary logistic regression and multivariable logistic regression analysis were done to describe the association between dependent and independent variables and independent predictors of modern contraceptive utilization. The crude odds ratio and adjusted odds ratio were used for testing associations between independent and dependent variables. The variables that have a P-value less than or equal to 0.05 at bivariate analysis were included in the multivariable logistic regression to control possible confounding factors.
Ethical Consideration
This study was reviewed and approved by the ethical review board of MTY Abyssinia Medical Science College. Ethical clearance was obtained from the ethical review committee of MTY Abyssinia Medical Science College Research and the Publication Office. Besides, an official letter was sent and permission was obtained from Gondar City Administrative Health Office. The aim of this study was described to all women, and all evidence obtained from them was secured and kept confidential. To ensure confidentiality, no names were taken or written onto the questionnaires. Written informed consent was obtained from all respondents who participated in the study (participants under the age of 18 years were approved by the ethics committee to provide written informed consent on their own behalf).
Results
Socio-Demographic Characteristics of the Respondents
A total of 708 women of the reproductive age were involved in the study (response rate = 96.5 %), of whom 33.3% were between 25 and 29 years old. The mean age of the respondents was 28.3 ± (S.D. = 6.5) years ranging from 16–49 years. Of the total of the respondents, the majority identified as Amhara in their ethnicity (94.0%). Further characteristics collected showed that 69.8 % were orthodox in their religion, most of the women were married (87.7%), and 24.2% were university degree and above holders concerning their education level. About half of the respondents were homemakers in their occupation (49.9%). Among the respondent’s husbands, 31.8% were government employees in their occupation and 31.5% had a degree or above with respect to their educational qualification (Table 1).
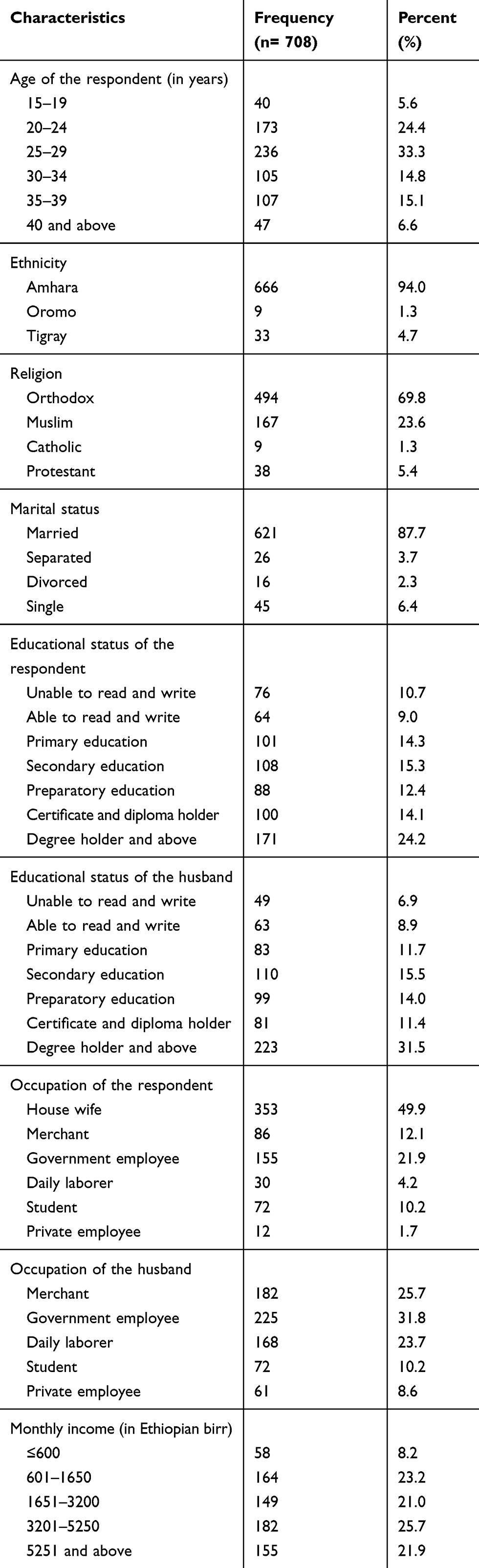 |
Table 1 Socio-Demographic Characteristics of the Reproductive Age Women in Gondar City, Northwest Ethiopia, 2019 |
Reproductive and Maternal Characteristics
The majority of the respondents had a history of previous pregnancies (88.6%) and their age at first pregnancy (40.3%) was between 20 and 24 years. Of 708 respondents, 50.8% had one up to two pregnancies, 89% had a live newborn in all deliveries, 96.5% had a history of non-child death experience, 70.2% had one up to three live children, 58.1% had four up to six desired children, and 49.6% had four up to six family sizes (Table 2).
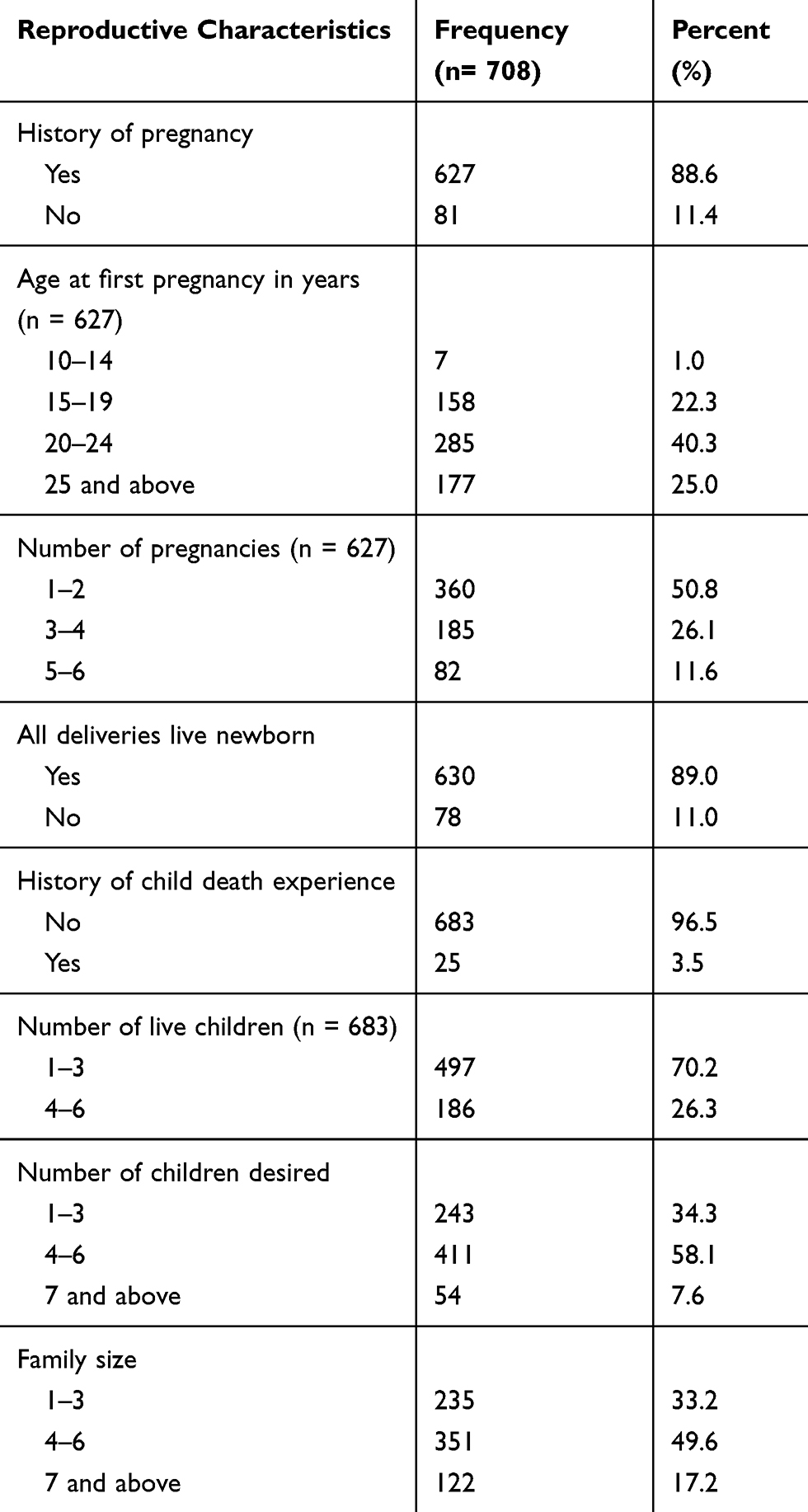 |
Table 2 Reproductive Health Characteristics of Reproductive Age Women in Gondar City, Northwest Ethiopia, 2019 |
Source of Information About Modern Contraceptive Methods
All (100%) of the women in the reproductive age group have heard about at least one modern contraceptive method. The main source of information about modern contraceptives was health care providers 460 (65%), Mass media (Radio, Television, etc.) 380 (53.7%), peers 370 (52.3%), and health extension workers 287 (40.5%). The schools 120 (17%), families 86 (12.1%), and the husband 253 (35.7%) had less contribution in disseminating information about the modern contraceptive usages.
Knowledge About Modern Contraceptive Methods
The most widely known modern contraceptive methods were injectables 603 (85.2%), regular pills 545 (77.0%), Implanon 382 (53.9%), and condom 338 (47.7%). Some of the women knew about emergency pills 197 (27.8%), the intrauterine device 268 (37.9%), and female and male surgical method 102 (14.4%).
The study respondents knew that the purpose of using modern contraceptives to different degrees. Many understood its purpose for enabling spacing of pregnancies 509 (72%) or delaying pregnancy 360 (50.8%), while less consciousness was there about its aim to limit 207 (29.2%), preventing unwanted pregnancy 176 (24.9%), for medical reason 37 (5.2%), and decreasing maternal mortality and morbidity 93 (13.1%).
The majority of the women mentioned that the modern contraceptive methods can be found in the health centers 617 (87.2%), public hospitals 381 (53.8%), and private clinics 365 (51.6%). A fewer number of women mentioned that contraceptives can be found in the pharmacy 240 (34%) and family guidance institutions 142 (20.1%).
Participant’s Attitude Towards Modern Contraceptive Methods
Forty-two percent of the women disagreed that the notion of short-acting contraceptives are more effective than long-acting contraceptives, but 36.1% believed that the contraceptives had a side effect and could be dangerous to the mother. In addition, 39.8% considered that contraceptive use could cause infertility in women (Table 3).
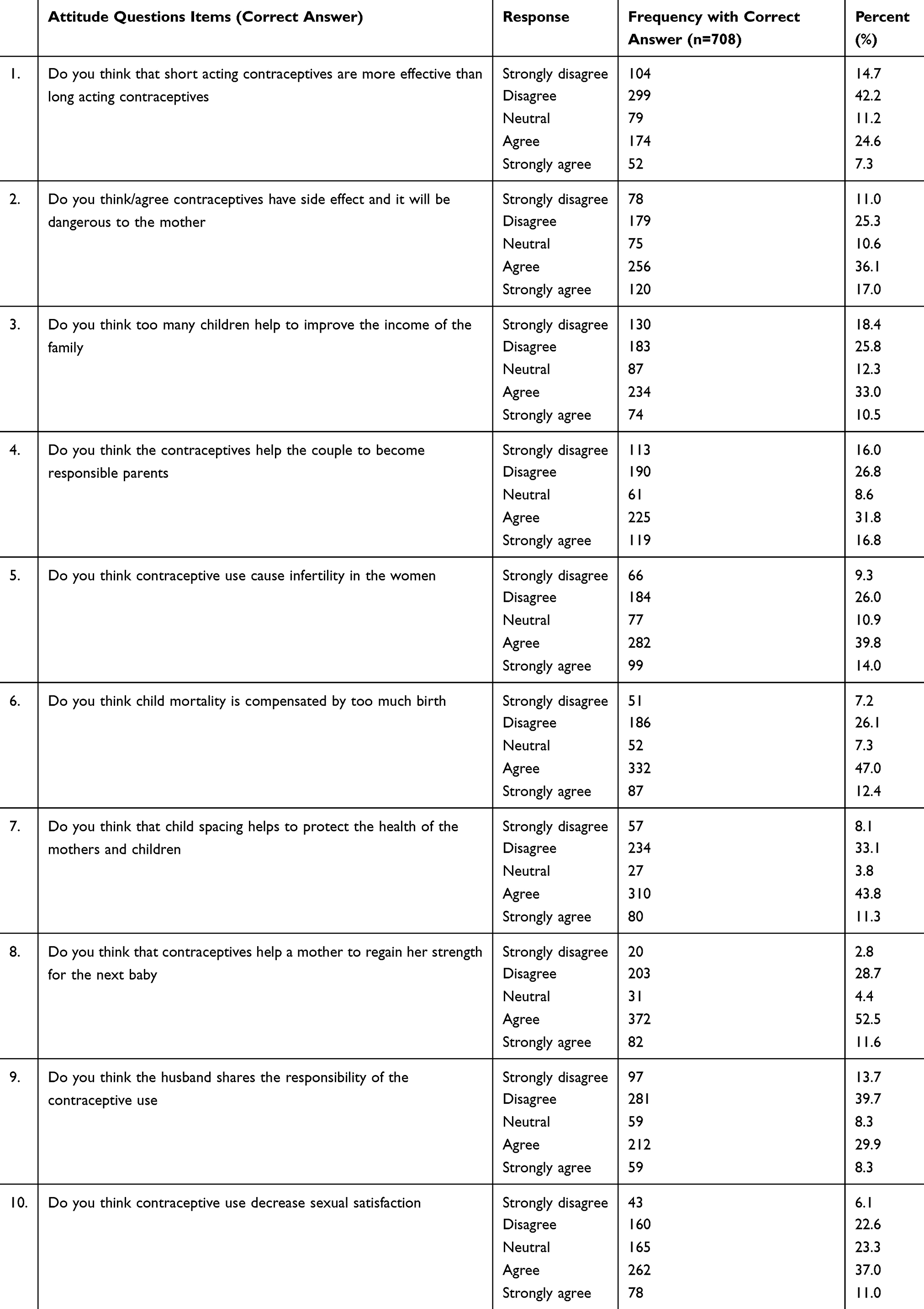 |
Table 3 Participants Attitude Towards Modern Contraceptive Methods in Gondar City, Northwest Ethiopia, 2019 |
Modern Contraceptive Utilization and Related Information
Of 708 respondents, 56.2% used modern contraceptives at some point in their lives. The prevalence of modern contraceptive use during the study period was 41.2%. Of the current users, the most preferable method was injectable 151 (51.7%). The majority of the women, 147 (50.3%), received the contraceptives from health centers. 274 (68.8%) stopped the contraceptive use, and the major factor for this pause was their wish to have another child 159 (58%). Among the current users, half of them (54.7%) reported that the decision to use contraceptive methods was made jointly with their husbands (Table 4). Most of the women mentioned that the main reason for not using contraceptives during the study period was an intention to have another child 139 (33.4%), but eight (1.9%) women were not using contraceptives for medical contraindications (Figure 1).
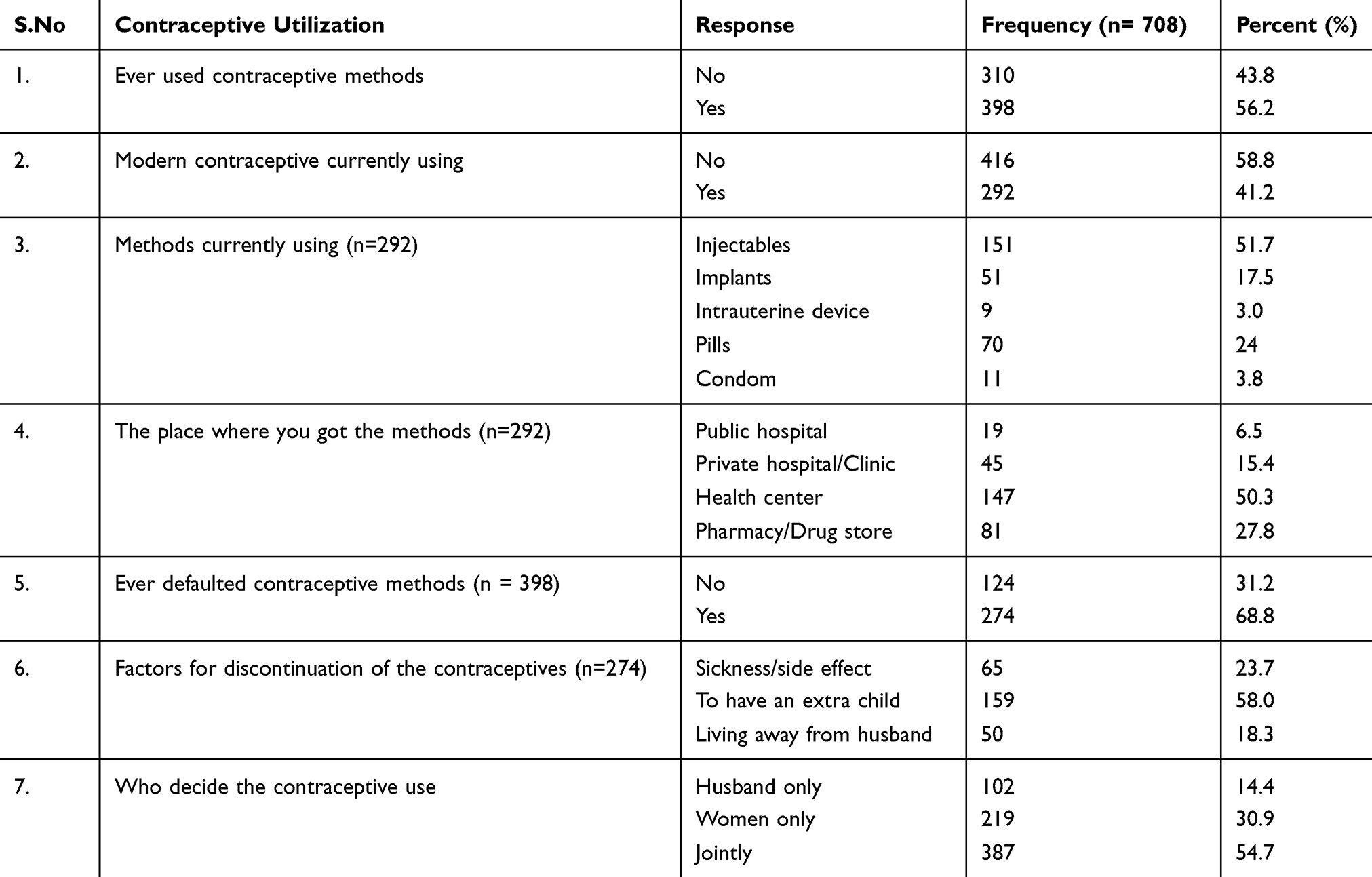 |
Table 4 Modern Contraceptive Utilization and Related Issues Among Women of Reproductive Age in Gondar City, Northwest Ethiopia, 2019 |
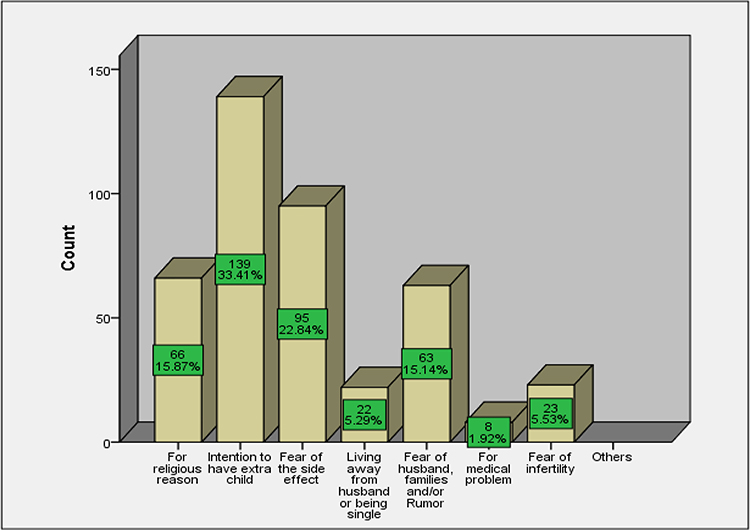 |
Figure 1 The main reasons for not using the modern contraceptive methods currently among women of reproductive age group in Gondar City, Northwest Ethiopia, 2019. |
Level of Knowledge and Attitude Towards Modern Contraceptive Methods
In this study, 369 (52.1%) of all respondents had good knowledge of modern contraceptive methods. In addition, about 321 (45.3%) respondents had a favorable attitude towards modern contraceptive methods.
Factors Associated with Modern Contraceptive Utilization
Binary logistic regression analysis showed that the age of the respondents, educational status of the respondent, educational status of the husband, the numbers of children who were born live, numbers of desired children, no history of child-death experience, all live newborn deliveries, good knowledge, and positive attitude were factors associated with their contraceptive utilization. All variables that show statistically significant association in binary logistic regression were entered into a multivariable logistic regression to rule out confounders. Accordingly, respondents aged between 15 and 19 years were found to be 5 times [AOR =5.4 (95% CI: 1.6, 18.8)] more likely to utilize modern contraceptives as compared to those aged above 40 years. Being in the age group from 20–24 years made them 4 times [AOR =3.6 (95% CI: 1.3, 9.5)] more likely to utilize modern contraceptives as compared to being in the age of above 40 years; and being in the age group from 25–29 years women were 5 times [AOR = 4.7 (95% CI: 1.8, 12.3)] more likely to utilize modern contraceptives as compared to that of above 40 years of age. Respondents who completed preparatory education were 2 times [AOR=2.4 (95% CI: 1.02, 5.6)] more likely to utilize modern contraceptives as compared to those respondents who were unable to read and write. Respondents who completed their certificate and diploma education were 2 times [AOR= 2.3 (95% CI: 1.01, 5.3)] more likely to utilize modern contraceptives as compared to women unable to read and write. Respondents with completed their degrees and above educational status were 4 times [AOR= 4.0 (95% CI: 1.8, 8.9)] more likely to utilize modern contraceptives as compared to respondents unable to read and write. Women with husbands who completed their primary, preparatory, diploma, and degree and above education were 5 times, 4 times, 5 times, and 3 times, respectively, more likely to utilize modern contraceptives as compared to those with husbands unable to read and write (Table 5).
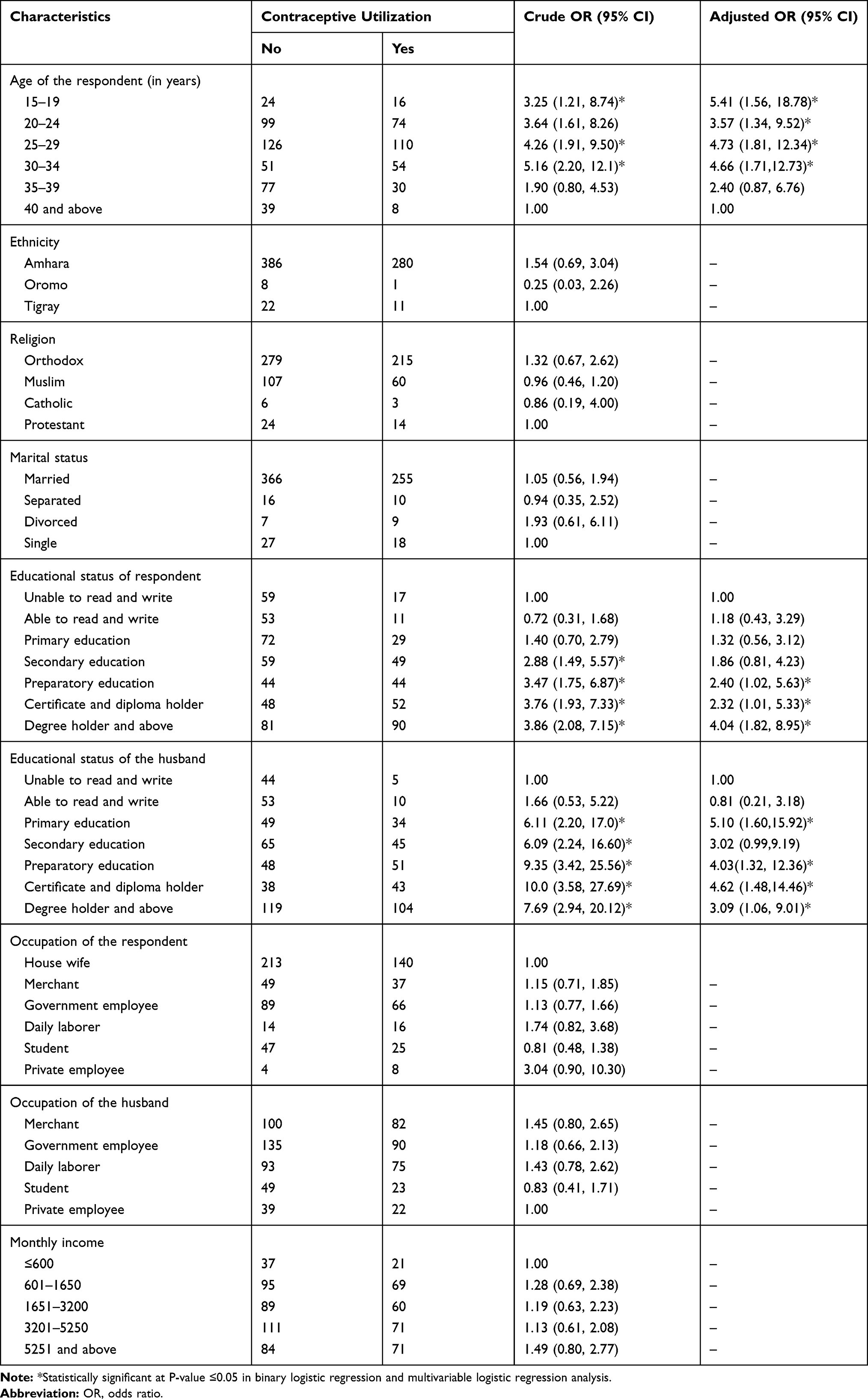 |
Table 5 Multivariable Logistic Regression Analysis on Factors Associated with Modern Contraceptive Utilization Among Women of Reproductive Age in Gondar City, Northwest Ethiopia, 2019 |
Participants having below six desired children were 2 times [AOR= 2.4 (95% CI: 1.1, 5.3)] more likely to utilize modern contraceptives as compared to those having above seven desired children. Respondents who did not have a child death experience were 4 times [AOR= 4.4 (95% CI: 1.03, 19.1)] more likely to utilize modern contraceptives as compared to respondents who had child death experiences. Those having all their deliveries with live newborns were 2 times [AOR=2.3 (95% CI: 1.2, 4.6)] more likely to utilize modern contraceptives as compared to those without having all their deliveries been completed with live newborns. Respondents with a good knowledge about family planning options were 4 times [AOR= 4.1 (95% CI: 2.7, 6.0)] more likely to utilize modern contraceptives as compared to those who have poor knowledge. Those having a positive attitude were 4 times [AOR= 3.5 (95% CI: 2.4, 5.1)] more likely to utilize modern contraceptives as compared to those who had a negative attitude (Table 6).
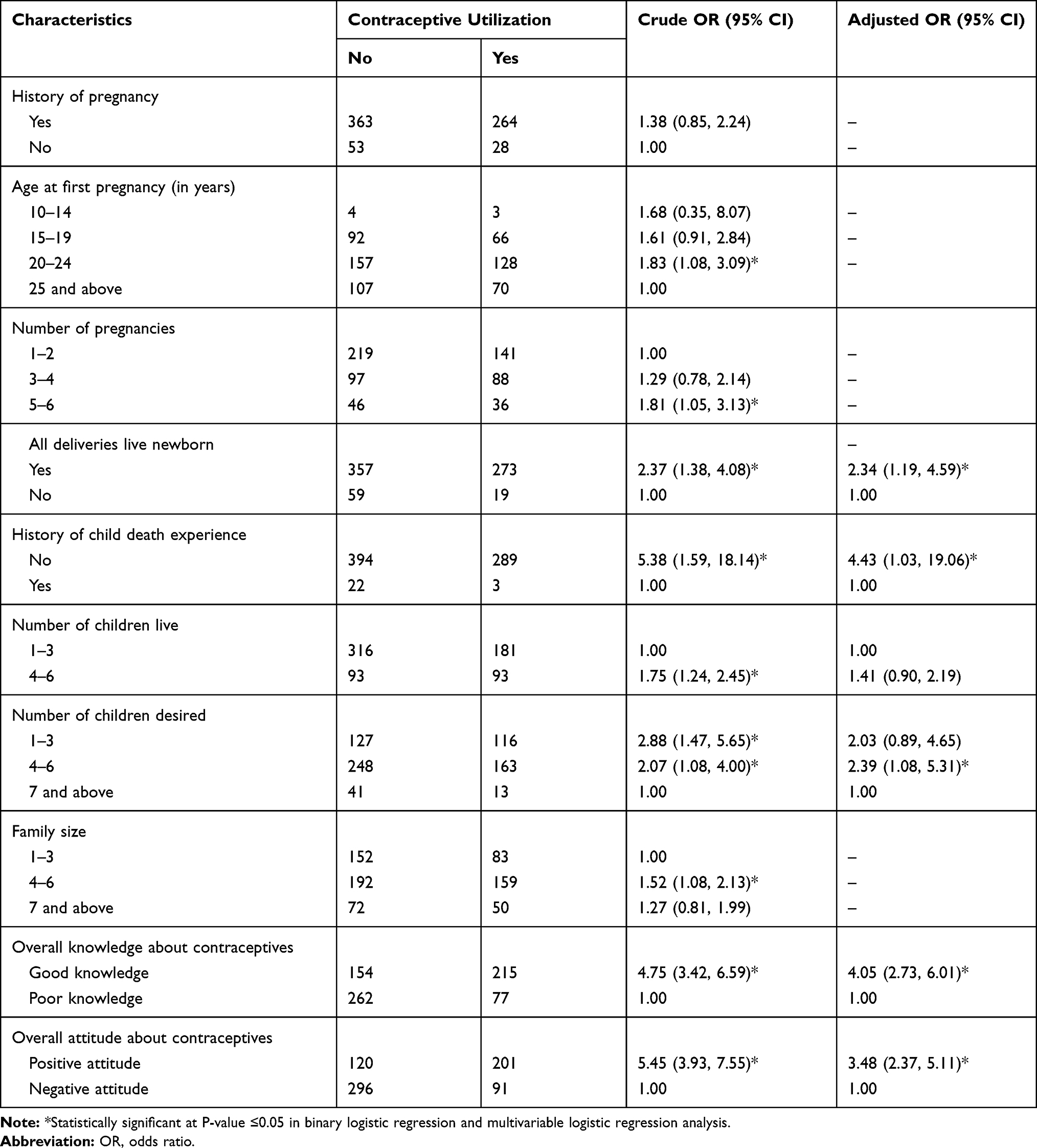 |
Table 6 Multivariable Logistic Regression Analysis on Factors That Associated with Modern Contraceptive Utilization Among Women of Reproductive Age in Gondar City, Northwest Ethiopia, 2019 |
Discussion
This community-based study was employed to determine the prevalence of and to identify factors associated with modern contraceptive utilization in Gondar City. Accordingly, the age of the women, the educational status of the respondent, the educational status of the husband, the history of non-child death experience, the number of desired children, all live newborn deliveries, their knowledge, and their attitude level, were significantly associated with modern contraceptive utilization.
In this study, the overall prevalence of modern contraceptive utilization was 41.2%. This finding is almost in line with the findings from the DHSAR and compares to the Ethiopian national level, Mojo Town, Debre-Brahhan (urban vs rural), Boditi Town, and Gondar hospital. The observed small variation may be due to the difference in study setting (urban vs rural), and study design (institution vs community-based).
Though one may find the rising trend prevalence of modern contraceptive methods in Gondar city promising, the numbers still compare poorly on an international scope.31 The variation may be due to the presence of different population characteristics, and the difference in countries’ health policy.15 Similarly, it is lower than in comparison with the study results from Addis Ababa City, Arba-Minch Town, Farta District, Arsi Zone, and SNNPR (Table 7).
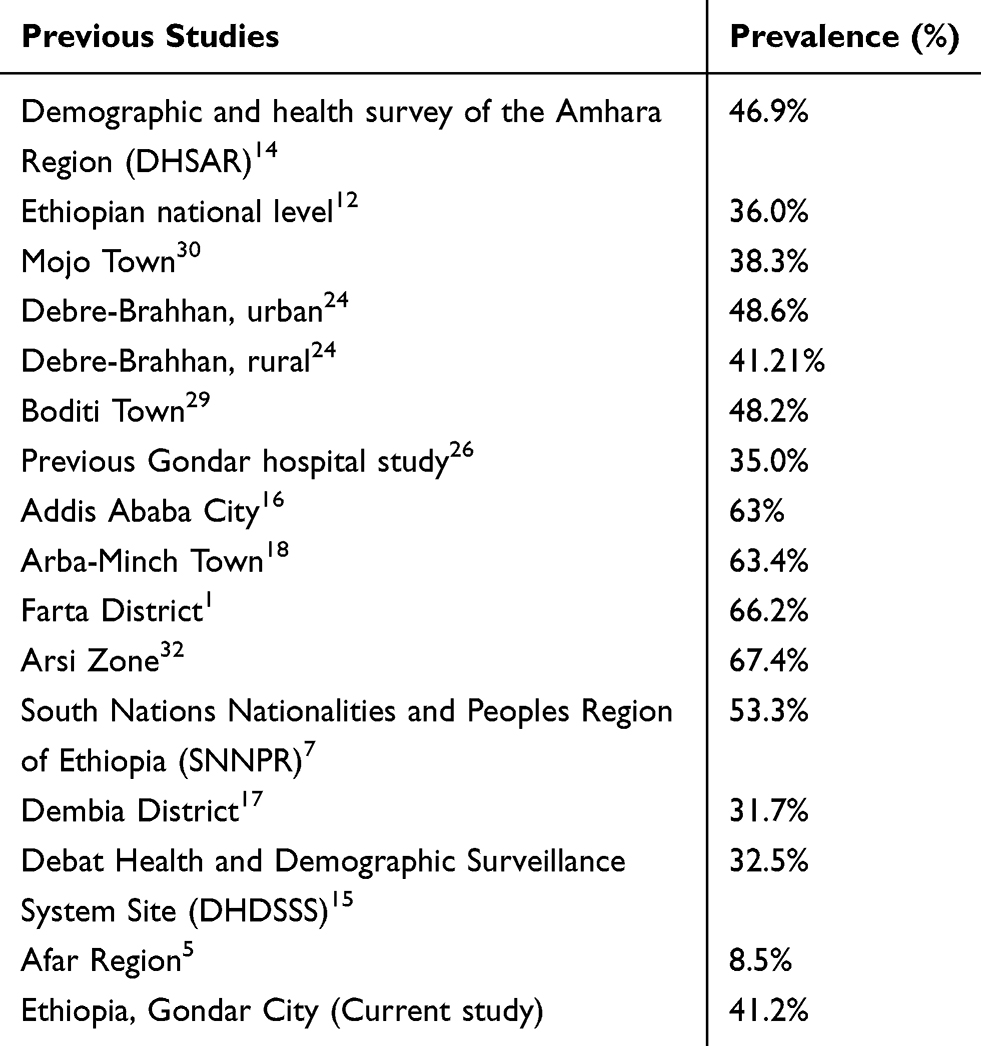 |
Table 7 Comparison of the Prevalence of Modern Contraceptive Utilization with Various Previous Studies |
Gondar’s contraceptive usage seems, however, higher than what the findings from studies conducted in Dembia District, DHDSSS, and Afar Region indicate. The reason for this could be the fact that the study participants of our research were from urban areas, while, for instance, the participants from the pastoralist community were recruited for the study in the Afar Region. The differences in the place of residency, religion, year of the study, and community literacy affect modern contraceptive utilization.5,12,15 According to studies, there is regional variation in modern contraceptive utilization in Ethiopia.2,12-15
Regarding modern contraceptive methods, 51.7% of respondents were users of injectable types of contraceptive methods. This finding is in agreement with other previous studies in Ethiopia.2,7,15,17,18 The reason may be due to its convenience and availability. Next to the injectable method, widely used contraceptive methods were pills, implants, and intrauterine devices. This finding is similar to the findings from Arba-Minch Town, Farta District, and Gondar hospital.
In this study, socio-demographic and reproductive variables were assessed for its correlation with modern contraceptive utilization. Being above the age of forty was negatively correlated with contraceptive utilization. This finding is supported by the study conducted in the Debre-Brahhan, Arba-Minch Town, Dembia District, Shire-Endaslasie Town,33 SNNPR, and DHDSSS. This is related to the fact that older women may be in less need of contraceptive methods.7,15,18
The higher educational status of the respondents and their husbands was significantly and positively associated with modern contraceptive utilization. This finding is supported by the study conducted among the Dembia District, Arba-Minch Town, Boditi Town, DHDSSS, Mojo Town, Afar Region, Shire-Endaslasie Town, and Gondar hospital. This can be explained with the idea that women with better educational levels have better access to health care information, have greater independence to make their own and informed decisions, and greater ability to use health care services. The positive effect of education helps women to increase their understanding of reproductive health issues and to understand and use the different contraceptive methods that suit their health condition best. It also increases the overall status of women in knowledge, attitude, and health-seeking behavior.15,18,30
Women whose deliveries were all live newborns were more likely to use the contraceptive methods as compared to their counterparts. Similar correlations have been found in previously conducted studies in the Shire-Endaslasie Town, Debre-Brahhan, and SNNPR. Because of contraceptive usage (and thus, spacing, etc.), the likelihood of healthy newborns increases. The experience of delivering at health institutions will allow women to get more family planning-related information at the time of antenatal, delivery, and postnatal care visits.7,24,33
Women with smaller numbers of desired children were more likely to utilize contraceptive methods as compared to those who have more desired children. This finding is supported by the study conducted in the Debre-Brahhan and SNNPR. One may assume that once the respondent decided to have fewer children, they will use contraceptive methods to limit their births. It might be due to the fact that globally, one can see that the more educated people are, the smaller the amount of the desired children is.
Those who had child death experience were less likely to utilize contraceptive methods as compared to those women with non-child death experience. This finding is supported by some studies.7,33 This could be due to an intention to replace the lost ones and the need to have more children.7 In the social perspective, communities that are less educated and thus, rely on their children to ensure their care when old.
In this study, women having good knowledge of contraceptive methods were more likely to use modern contraceptives as compared to those who had poor knowledge. This is in line with the findings from Arba-Minch Town, Farta District, and SNNPR. The lack of awareness about contraceptive methods was a key factor that preventing women in the reproductive age from using contraceptives.2,18 The women who had a positive attitude had higher odds of using contraceptives. This is in line with findings from the Afar Region and SNNPR. This implies that having a positive attitude is an important factor for promoting contraceptive utilization, and it creates a favorable environment to accept informed consent to health care providers who offer contraceptive methods.5 According to the participants of this study, their negative attitude comes from the rumor that the modern contraceptives contain an ingredient that may lead to infertility, as well as the perception change due to the previous political situations in Ethiopia.
As migraine prevalence is high in women of reproductive age, it is common to face the issue of migraine and hormonal contraceptive use in clinical practice. Menarche, menstruation, pregnancy, and menopause, and the use of hormonal contraceptives may influence migraine occurrence.34–36 Truly speaking, migraine with aura is a risk factor for ischemic stroke, cardiac disease, and vascular mortality.36 Systematic reviews have shown that administration of combined oral contraceptives to migraineurs may further increase the risk for ischemic stroke.34–39 In order to avoid the risks, migraine with aura, hereditary thrombophilia, and epileptic patients should take non-hormonal forms of the contraception.36,37,40 However, in migraine without aura patients, the use of combined oral contraceptives may not be contraindicated, but their intake must be suspended if aura symptoms appear. Moreover, other risk factors for stroke must be carefully considered when prescribing it (smoking, hypertension, diabetes, hyperlipidemia, thrombophilia, obesity, age over 35 years (a very important factor), for example).38,39
Strength and Limitations of the Study
This is a community-based study, performed based on a random sampling method and it has a high sample size to increase the precision. The study has assessed the overall knowledge and attitude towards modern contraceptives, which can function as a barrier to contraceptive utilization.15 The cross-sectional nature of the study does not allow making assumptions surrounding causal effects between the relationships.
Conclusion
The majority of the participants had good knowledge and an unfavorable attitude towards modern contraceptive utilization.
Factors like the age of the women, the educational status of the respondent, the educational status of their husband, the history of non-child death experience, the number of children desired, all deliveries live newborns, good knowledge, and favorable attitude were independently associated with the modern contraceptive utilization.
Therefore, the authors recommend that special awareness creation through the means of health education should be given to the community. This will help them to develop appropriate knowledge and attitude towards modern contraceptive utilization. Further, women’s educational levels should be improved by applying continuous efforts in order to increase their understanding of reproductive and family planning issues. It is also important to give special emphasis for those aged between fifteen and thirty-five years and for those having many desired children.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We would like also to thank the data collectors, the study participants, and our friends for their valuable contribution in this study. Our appreciation also goes to Dr. Olga Yegorova (Ph.D., School of Media, Communication and Sociology, University of Leicester, Bankfield House, 132 New Walk, Leicester, LE1 7JA, United Kingdom) for her valuable comments on reviewing, and editing this manuscript to meet the journals manuscript writing criteria.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization: Sexual and Reproductive Health program. WHO; 2020. Available from: https://www.who.int/reproductivehealtth/en/.
2. Tigabu K, Getu D, Zelalem B. Assessment of modern contraceptive practice and associated factors among currently married women age 15–49 years in Farta District, South Gondar Zone, Northwest Ethiopia. Sci J Public Health. 2014;2(6):507–512. doi:10.11648/j.sjph.20140206.11
3. World Health Organization: family planning and Contraception. WHO; 2018. Available from: https://www.who.int.news-room/factsheets/detail/familyplanning-contraception.
4. Jacob SR, Bakamjian L, Pile JM. Threatened and Still Greatly Needed Family Planning Programs in Sub-Saharan Africa. New York: The acquire Project. Gender Health; 2008:2.
5. Alemayehu M, Lemma H, Abrha K, et al. Family Planning Use and Associated factors among pastoralist community of Afar region, Eastern Ethiopia. BMC Womens Health. 2016;16:39. doi:10.1186/s12905-016-0321-7
6. National Guideline for Family Planning Services in Ethiopia. Federal Democratic Republic of Ethiopia, Ministry of Health; 2011:1–69
7. Endriyas M, Eshete A, Mekonnen E, Misganaw T, Shiferaw M, Ayele S. Contraceptive utilization and associated-factors among women of reproductive age group in Southern Nations Nationalities and Peoples’ Region, Ethiopia: cross-sectional survey, mixed-methods. Contracept Reprod Med. 2017;2:10. doi:10.1186/s40834-016-0036-z
8. Central Statistical Agency, Ethiopia and ORC Macro. Ethiopia Demographic and Health Survey 2007. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ORC Macro; 2011.
9. An Ethiopian FP2020-2019 core indicators 1-9 country fact sheet/handout, 2020. Available from: https://www.Familyplanning2020.Org/Ethiopia.
10. Family Planning 2020 Commitment Govt. of Ethiopia. Available from: https://www.Familyplanning2020.Org/Ethiopia.
11. Central Statistical Agency [Ethiopia]. Ethiopia Mini Demographic and Health Survey 2014. Addis Ababa: Central Statistical Agency [Ethiopia]; 2014.
12. Worku AG, Tessema GA, Zeleke AA. Trends of Modern Contraceptive Use among Young Married Women Based on the 2000, 2005, and 2011 Ethiopian Demographic and Health Surveys: a Multivariate Decomposition Analysis. PLoS One. 2015;10(1):e0116525. doi:10.1371/journal.pone
13. Lakew Y, Reda A, Tamene H, Benedict S, Deribe K. Geographical variation and factors influencing modern contraceptive use among married women in Ethiopia: evidence from a national population based survey. Reprod Health. 2013;10(1):52. doi:10.1186/1742-4755-10-52
14. Central Statistical Agency [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2016. Addis Ababa: Central Statistical Agency [Ethiopia]; 2016.
15. Asrade GA, Fekadu A, Yitayal M, et al. Prevalence and determinants of contraceptive utilization among married women at Debat Health and Demographic surveillance system site, Northwest Ethiopia. BMC Womens Health. 2018;18(118):2–7.
16. Tsigereda G. Barriers to Use Contraceptive Methods Among Adolescents in Addis Ababa City. Addis Ababa University; 2004.
17. Debebe S, Limenih M, Biadgo B. Modern contraceptive methods utilization among reproductive aged women in Rural Dembia District, North-West Ethiopia. Int J Reprod Biomed. 2017;15(6):367–374.
18. Samuel A, Uliso A, Olle B, Dambe D, Nigatu M, Sorato M. Assessment of Modern Contraceptive Method Utilization and Associated Factors Among Women of Reproductive Age Group in Arba-Minch Town, SNNPR, Ethiopia. EC Gynaecol. 2017;6.2:36–53.
19. The Last Ten Kilometers Project. Community-Based Family Planning, Including Long-Acting Contraceptive Services at Selected Health Centers and Their Health Posts in Four Regions of Ethiopia: A Situational Analysis. Addis Ababa: JSI Research and Training Institute; 2015.
20. John H. Contraceptive knowledge, perceptions and use among adolescents. Journal of Socioll Res. 2012;3(2):170–180.
21. Oluwasanmi L, Akintade M. Awareness, use of and barriers to family planning services among University Students in Lesotho. Hum Sci Res Counc. 2011;17(3):73–77.
22. Stephenson R, Baschieri A, Clements S, Hennink M, Madise N. Contextual Influences on modern contraceptive use in Sub-Saharan Africa. Am J Public Health. 2007;97(7):1233–1240. doi:10.2105/AJPH.2005.071522
23. Ankomah A, Anyanti O. Myths, mis-information, and communication about family planning and contraceptive use in Nigeria. J Contracept. 2011;2:95–105.
24. Mohammed A, Woldeyohannes D, Feleke A, Megabiaw B. Determinants of modern contraceptive utilization among married women of reproductive age group in North Shoa Zone, Amhara Region, Ethiopia. Reprod Health. 2014;11(1):13. doi:10.1186/1742-4755-11-13
25. Oumer M. Prevalence and associated factors of induced abortion among women of reproductive age group in Gondar Town, Northwest Ethiopia. Sci J Public Health. 2019;7(3):66–73. doi:10.11648/j.sjph.20190703.11
26. Chernet B, Mulat A, Melaku K, Yalemzewod A. Factors associated with utilization of long-acting and permanent contraceptive methods among women who have decided not to have more children in Gondar city. BMC Womens Health. 2017;17(75):2–7.
27. Desalegn A, Tsegaw A, Shiferaw D, Woretaw H. Knowledge, attitude, practice and associated factors towards spectacles use among adults in Gondar Town, Northwest Ethiopia. BMC Ophthalmol. 2016;16:184. doi:10.1186/s12886-016-0357-3
28. Alemayehu AM, Belete GT, Adimassu NF. Knowledge, attitude and associated factors among primary school teachers regarding refractive error in schoolchildren in Gondar City, Northwest Ethiopia. PLoS One. 2018;13:2. doi:10.1371/journal.pone.0191199
29. Gebremeskel F, Getahun D, Kanko T, et al. Prevalence of modern contraceptive utilization and associated factors among women of reproductive age group at Boditi Town, Wolayita Zone, SNNPR, Ethiopia. Am J Nurs Sci. 2017;6(6):447–453. doi:10.11648/j.ajns.20170606.12
30. Gizaw A, Regassa N. Family planning service utilization in Mojo town, Ethiopia: a population based study. J Geogr Reg Plan. 2011;4:355–363.
31. Department of Economic and Social Affairs. Population Division. Trends in Contraceptive Use Worldwide; 2015.United Nations.
32. Koi S, Youm A, Kime S. Family planning practice and related factors of married women in Hetosa Woreda, Arsi Zone, Ethiopia. Int Nurs Rev. 2010;57:377–382. doi:10.1111/j.1466-7657.2010.00805.x
33. Tsehaye TW, Mengistu D, Berhe K. Assessment of modern contraceptive methods utilization and its determinant factors among women of reproductive age groups at Shire-Endaslasie Town, Tigray, Northern Ethiopia. J Bio Innov. 2014;3(3):144–169.
34. Sacco S, Gabriele SM, Karen LA, et al. Hormonal contraceptives and risk of ischemic stroke in women with migraine: a consensus statement from the European Headache Federation and the European Society of Contraception and Reproductive Health. J Headache Pain. 2017;18:108. doi:10.1186/s10194-017-0815-1
35. Lee SY, Lim JS, Oh DJ, et al. Risk of ischaemic stroke in patients with migraine: a longitudinal follow-up study using a national sample cohort in South Korea. BMJ Open. 2019;9:e027701. doi:10.1136/bmjopen-2018-027701
36. Sacco S, Ricci S, Degan D, Carolei A. Migraine in women: the role of hormones and their impact on vascular diseases. J Headache Pain. 2012;13(3):177–189. doi:10.1007/s10194-012-0424-y
37. Faubion SS, Casey PM, Shuster LT. Hormonal contraception and migraine: clinical considerations. Curr Pain Headache Rep. 2012;16(5):461–466. doi:10.1007/s11916-012-0278-7
38. Allais G, Castagnoli IG, De-Lorenzo C, et al. Oral contraceptives in migrane. Expert Rev Neurother. 2009;9(3):381–393. doi:10.1586/14737175.9.3.381
39. Nappi RE, Merki-Feld GS, Terreno E, Pellegrinelli A, Viana M. Hormonal contraception in women with migraine: is progestogen-only contraception a better choice? J Headache Pain. 2013;14(1):66. doi:10.1186/1129-2377-14-66
40. Reddy DS. Do oral contraceptives increase epileptic seizures? Expert Rev Neurother. 2017;17(2):129–134. doi:10.1080/14737175.2016.1243472
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.