Back to Journals » Local and Regional Anesthesia » Volume 19
Mode of Anesthesia During Cesarean Section and Neonatal Morbidity and Mortality: A Cohort Study
Authors Alhowary A, Altal O, Khasawneh W ![]() , Rawabdeh SAN
, Rawabdeh SAN ![]() , Al-Bataineh R
, Al-Bataineh R ![]() , Alrusan A
, Alrusan A ![]() , Bashaireh TK, Haddad L, Madain R
, Bashaireh TK, Haddad L, Madain R ![]() , Al Sharie AH
, Al Sharie AH ![]()
Received 19 November 2025
Accepted for publication 3 June 2026
Published 11 June 2026 Volume 2026:19 582928
DOI https://doi.org/10.2147/LRA.S582928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Stefan Wirz
Ala”a Alhowary,1 Omar Altal,2 Wasim Khasawneh,3 Saif Aldin Naif Rawabdeh,3 Rania Al-Bataineh,4 Anas Alrusan,1 Tareq Khaldoon Bashaireh,4 Lana Haddad,5 Rola Madain,2 Ahmed H Al Sharie4,6
1Department of Anesthesia and Pain Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 21110, Jordan; 2Department of Obstetrics and Gynecology, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 3Department of Pediatrics, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 4Faculty of Medicine, Jordan University of Science and Technology, Irbid, 21110, Jordan; 5Department of Pediatrics, University of Utah, Salt Lake, UT, 84112, USA; 6Department of Internal Medicine, Southeast Health, Dothan, AL, USA
Correspondence: Ala”a Alhowary, Department of Anesthesiology, Faculty of Medicine Jordan University of Science and Technology, P. O. Box: 3030, Irbid, 22110, Jordan, Tel +962791595219, Email [email protected]
Background: The influence of obstetric anesthesia on neonates is still under investigation. We aimed to investigate the influence of type of anesthesia; either general anesthesia (GA) or spinal anesthesia (SA); during elective or emergency cesarean section (CS) on neonatal outcomes.
Methods: A retrospective cohort study was conducted and all neonatal admissions to the neonatal intensive care unit for mothers who underwent elective or emergency CS as the mode of delivery during the period from 2017 to 2021 were enrolled in the study. The primary outcome of the study was to investigate the difference between SA and GA. The enrolled cohort was divided into two groups: GA and SA groups.
Results: A total of 997 patients were included in the study cohort. Among these, 628 patients underwent CS under SA. On univariate analysis, it was revealed that SA was associated with better Apgar score (8.56 ± 0.04 vs 8.16 ± 0.05, P =0.0001), less incidence of respiratory distress syndrome (RDS) (35.5% vs 42.3%, P =0.02), intraventricular hemorrhage (IVH) (0.8% vs 13.6%, P =0.0001), and neonatal thrombocytopenia (12.4% vs 17.3%, P =0.021). Moreover, GA was linked to higher mortality rates (10.8% vs 4%, P =0.0001) and more birth depression (10.6% vs 4.3%, P =0.0001). On the other hand, GA was related to less incidence of transient tachypnea of the newborn (TTN) (6.2% vs 12.6%, P =0.001). On multivariate logistic regression analysis, mode of anesthesia was related to RDS, TTN, IVH, birth depression and neonatal death.
Conclusion: GA use may be related to more adverse and worse neonatal outcomes. This is related to the utilization of GA more frequently in higher-grade emergencies and is associated with more adverse baseline predictors including lower gestational age, lower birth weight, and greater obstetric complications. SA could offer a localized effect for the anesthetic drugs. Further prospective trials are needed to justify the risk of both types of anesthesia.
Keywords: Apgar score, general anesthesia, neonatal intensive care unit, respiratory distress syndrome, spinal anesthesia
Introduction
The goal of obstetric anesthesia is to ensure the safety and well-being of the mother while delivering a healthy newborn under optimal surgical conditions. The choice of anesthesia mode depends on various factors, including the patient’s medical and antenatal history, the urgency of the cesarean section (CS), the experience of the anesthesiologist and surgeon, and the size of the hospital (larger hospitals relate to the availability of specialized anesthesia services, equipment, and trained personnel).1,2 The most commonly utilized types of anesthesia for CS are general anesthesia (GA) and regional anesthesia (ie., spinal (SA) or epidural). Each method offers distinct benefits and poses unique risks. GA is typically preferred in emergency situations due to its ability to induce maternal unconsciousness rapidly, facilitating prompt delivery and minimizing stress. Nevertheless, it carries several risks, including neonatal aspiration pneumonia, inadequate maternal anesthesia, maternal and fetal respiratory complications, failed maternal intubation, and increased maternal blood loss, particularly when halogenated agents are used.3,4 Regional anesthesia has been associated with better maternal and neonatal outcomes, as well as improved maternal-infant bonding.3 Despite these benefits, it is not entirely without risks. Both spinal and epidural anesthesia can cause significant depression in maternal blood pressure and, in rare cases, severe post-dural puncture headaches. However, the occurrence of these headaches has declined with the development of advanced needle technologies.4
In the literature, the effects of different types of anesthesia, such as general and regional anesthesia, on neonates have been primarily studied following elective cesarean sections (with the exception of certain conditions such as placenta accreta spectrum disorders, where GA is indicated regardless of preference). Of note, the time duration from skin incision to fetal delivery has not been shown to independently cause severe neonatal outcomes.5 In the literature, the effects of different types of anesthesia, such as general and regional anesthesia, on neonates have been primarily studied following elective cesarean sections.6 With many studies showing no significant differences in Apgar scores between GA and regional anesthesia.7–11 Other studies have shown an increased need for neonatal respiratory support, lower 5-minute Apgar scores (<7), and higher rates of neonatal intensive care unit (NICU) admissions following in utero exposure to anesthetics.4,12 During emergency situations, GA has rapid conduction and application, however, regional block is the most commonly utilized method for elective CS, even in certain emergency situations. SA mitigates risks linked to GA during CS, such as aspiration pneumonia and intraoperative awareness. Moreover, SA decreases respiratory complications in both mothers and neonates, fosters early mother-infant bonding, and enhances postpartum pain management.1,13,14
The main objective of this study was to evaluate the influence of types of anesthesia (either GA or SA) during a CS on neonatal morbidity and outcomes. Importantly, the study population was restricted to NICU-admitted neonates, and findings should be interpreted within this context. Prior studies have predominantly focused on elective cesarean sections in unselected populations; there remains a specific knowledge gap regarding the differential impact of anesthesia type in NICU-admitted neonates across both elective and emergency settings, particularly in regions where GA use remains relatively high. We hypothesized that SA would be associated with better neonatal outcomes compared to GA in this high-risk NICU population. In this retrospective study, we included a comprehensive chart for the perioperative, maternal and neonatal factors that may influence neonatal outcomes.
Methods
Patients and Outcomes
This single-center study was carried out at King Abdullah University Hospital, a tertiary care facility associated with the Jordan University of Science and Technology. Retrospectively, all neonatal admissions to the neonatal intensive care unit (NICU) for mothers who underwent CS as the mode of delivery during the period of 2017 to 2021 were enrolled in the study. The hospital electronic database was utilized to extract the data which underwent comprehensive review. The following information was obtained: demographics, maternal and obstetrical history, mode of anesthesia, and neonatal outcomes. The following information regarding the maternal and obstetrical history was extracted: maternal age, gestational age of delivery, number of gestations, type of delivery (either elective or emergency), maternal co-morbidities and obstetrical adverse events. Furthermore, comprehensive neonatal outcomes were allocated. This study was carried out in accordance with the ethical guidelines of the Helsinki Declaration, ensuring privacy and confidentiality of patient data.
Any women: above the age of 18 years, who underwent an emergency or elective CS were included in the study. All NICU admission of live neonates, including both inborn and out-born neonates, were included. Exclusion criteria included any women who converted from SA to GA, all stillbirths, neonates transferred to other institutions (due to lack of data), and neonates born before 24 weeks of gestation. Furthermore, all neonates with complex congenital heart disease who were transferred to other institutions within 3 days of birth were excluded.
The primary outcome of the study was to investigate the difference between SA and GA in regard. Secondary outcomes included respiratory outcomes (RDS, TTN, chronic lung disease, CPAP duration), neurological outcomes (IVH stages, EVD use, VPS placement), hematological outcomes (thrombocytopenia, PRBC transfusion, neonatal jaundice), and survival outcomes (birth depression, neonatal mortality, length of hospitalization).
Neonatal Care and Setting
The NICU at our institution is managed by neonatologist consultants who follow the same institutional guidelines. This unit accommodates all inborn neonates and the admissions that are transferred from other hospitals.15
The neonatal outcomes were categorized into respiratory, neurological, hematological, and survival outcomes. Additional neonatal outcomes were allocated: gender, gestational age, birth weight, birth weight at discharge, and length of hospitalization. Prematurity was defined as the birth of live neonates before reaching 37 completed weeks of gestation. However, we have included all NICU deliveries.
Regarding the respiratory outcomes, the following parameters were included: respiratory distress syndrome (RDS) (RDS diagnosis was established with signs of respiratory distress and typical chest X-ray findings of hyaline membrane disease including reticulgranular shadows, air bronchogram, and white-out lung fields), transient tachypnea of newborn (TTN), apnea of prematurity (a cessation of breathing for 20 seconds or longer or a shorter pause accompanied by bradycardia), chronic lung disease, pneumothorax (pneumothorax diagnosis was established with typical radiological findings or with positive transillumination sign), pulmonary hypertension (typical echocardiographic findings using the calculated tricuspid regurgitation (TR) jet as a marker), number of surfactant doses given, number of days under continuous mandatory ventilation, number of days under continuous positive airway pressure (CPAP), number of days under high flow nasal cannula, number of days on room air, the use aminophylline, and the use of inhaled steroid-.
The neurological outcomes were also investigated. The neurological parameters included intraventricular hemorrhage (IVH) (IVH was graded and diagnosed according to Papile’s classification through head ultrasonography),16 periventricular leukomalacia (PVL), the presence of myelomeningocele, the need for external ventricular drain, the need ventriculoperitoneal shunts, and the magnesium sulfate for neurological protection. Furthermore, detailed hematological outcomes were assessed and allocated. These parameters included the transfusion of blood product, neonatal jaundice, and neonatal thrombocytopenia. The diagnosis and management of hyperbilirubinemia cases were according to the American Academy of Pediatrics (AAP) guidelines.17 We reported cases of ABO incompatibility, Rh isoimmunization, duration of phototherapy, intravenous immunoglobulin administration, and exchange transfusion procedures.
Moreover, the general health and survival outcomes were investigated and comprised, birth depression (refers to neonates born flaccid with respiratory depression that requires resuscitation beyond the routine newborn care steps), Apgar score at 5 minutes, number of neonates small or large for gestational age, mortality, length of stay, weight, and corrected gestational age at discharge. Other parameters included necrotizing enterocolitis (NEC)(Bell’s classification system was applied for the diagnosis of NEC, and included typical clinical presentation associated with pneumatosis intestinalis, portal venous gas or pneumoperitoneum),18 and certain congenital anomalies.
Discharge supported and included stable vital signs for 24 hours, stable respiratory status (with no oxygen requirements), and tolerating enteral feeding.
Anesthesia Settings
The conduction of anesthesia was carried out and supervised by consultant anesthesiologists and senior residents. At the operating theater, two intravenous cannulas were inserted, and vital signs were monitored (continuous monitoring of blood pressure, oxygen saturation, and respiratory rate) and electrocardiogram were conducted.
The SA was performed after sterilization of the vertebral column at the level of L3-L4 or L4-L5. The SA was conducted using 25- or 27-gauge spinal needles with 2.3 mL of 0.5% heavy bupivacaine and 0.4 mL of 0.005% fentanyl (25 µg; 50 µg/mL). Adequate hydration and oxygenation were performed before the procedure using crystalloid solution and 100% O2 through a nasal cannula, respectively. The SA medications and guidelines were the same during the study period.
During the GA cases, rapid-sequence induction was conducted with the insertion of endotracheal tube. Propofol (2.5 mg/kg) and rocuronium (0.5 mg/kg) were administered for the induction. The maintenance was achieved by isoflurane (0.5–0.75%) in 50% oxygen and 50% air. Fentanyl was given after delivery of the baby and severing the umbilical cord, inhaled anesthetic agents were discontinued. Propofol infusion was used to maintain anesthesia. At the end of surgery, neostigmine (2.5 mg) and atropine (1 mg) were given intravenously for neuromuscular reversal; and sugammadex was used when indicated as an alternative reversal agent. The GA medications and guidelines were the same during the study period.
Obstetrical Settings
The same guidelines were used to conduct obstetric practice by consultant obstetricians. High-risk pregnancies were monitored by maternal-fetal medicine specialists. The included participants had their booking visit early in gestation and estimation of their gestational age was based on last menstrual period and/or early ultrasonography (US). Collected maternal variables include age, parity, assisted pregnancy, pregnancy complications, previous CS delivery, and antenatal steroid. Delivery related variables include gestational age, mode of delivery, induction of labor, prolonged premature rupture of membranes (PROM), and type of anesthesia. Emergency CS was defined as the CS that is performed when there is an immediate threat to the life of a fetus and/or woman. According to the Royal College of Obstetricians and Gynecologists, we have included category 1 (immediate threat to the life of the woman or fetus), and category 2 (maternal or fetal compromise that is not immediately life-threatening) as emergency CS.
Two types of steroids were utilized in our center: dexamethasone sodium phosphate and betamethasone dipropionate and betamethasone sodium phosphate. The dexamethasone is given twice as 12 mg injection, 12 hours apart. Betamethasone is formulated as a 2 mL-sterile aqueous injectable suspension of betamethasone dipropionate and betamethasone sodium phosphate equivalent to 5 and 2 mg betamethasone, respectively, in a sterile buffered and preserved vehicle. It is given twice, 24 hours apart.
Statistical Analysis
IBM SPSS statistical package for Windows v.29 (Armonk, New York, USA) was used to analyze the collected data. Nominal variables were reported as the frequency (percentage) and continuous variables as the mean ± standard error of the mean (SEM). The Kolmogorov–Smirnov test was used to test data normality. The Chi-square test for categorical variables and the Student’s t-test for continuous variables were used to determine the statistical significance between the study groups. A p < 0.05 was considered a statistically significant result. Binary logistic regression analysis was employed to assess the independent factors affecting the neonatal outcomes in order to adjust the variability of the groups. Furthermore, maternal age and number of gestations were matched between both groups (GA and SA). The matching was performed using a 1:1 nearest-neighbor propensity score matching approach based on these two covariates (maternal age and number of gestations), without replacement. As this was a retrospective cohort study, a prospective sample size calculation was not performed; the sample size was determined by the availability of all consecutive eligible records over the five-year study period (2017–2021), yielding a total of 997 patients, which provides adequate statistical power for the primary comparison between SA and GA groups. The use of SEM to express continuous variables reflects the precision of the group mean estimates used for the between-group comparisons reported in this study.
Results
General Demographics and Comparison Between SA and GA in Terms of Maternal Factors
A sum of 997 patients was included in our study cohort. Among these, 628 patients underwent CS under SA, while 369 patients received GA. The mean maternal age was 30.70 ± 0.20 years, without significant difference between the two groups. The mean gestational age at delivery was 35.15 ± 0.09 weeks, showing significant difference between the SA group and the GA group (35.46 ± 0.10 weeks vs 34.63 ± 0.20 weeks, P =0.0001). This is also reflected in the categorization of gestational age. Thrombophilias were identified in 19 patients (1.90%), with a higher prevalence in the GA group compared to the SA group (13 patients (3.50%) vs 6 patients (1.00%), P =0.005), this could be explained as thrombophilia is a relative precaution for SA. Antenatal complications included gestational diabetes mellitus (GDM), reported in 44 patients (4.40%), with higher incidence in the SA group compared to the GA group (35 patients (5.60%) vs 9 patients (2.40%), P =0.013). Preeclampsia was observed in 64 patients (6.40%), with higher incidence in the GA group compared to the SA group (35 cases (9.50%) vs 29 cases (4.60%), P =0.002). Placental abruption complicated 36 deliveries (3.60%), with higher occurrence in the GA group compared to the SA group (19 cases (5.10%) vs 17 cases (2.70%), P =0.036). PROM complicated 262 deliveries (26.30%), occurring more frequently in the SA group (185 patients (29.50%)) than in the GA group (77 patients (20.90%)) (P =0.002). The type of CS demonstrated significant differences between the two groups, with more elective CS performed in the SA group and more emergency CS in the GA group. The mean birth weight was 2364.10 ± 24.10 grams and significantly higher in the SA group than the GA group (2434.30 ± 29.70 grams vs 2244.30 ± 30.10 grams, P =0.0001). The mean APGAR score at 5 minutes was 8.41 ± 0.03, which was notably higher in the SA group compared to the GA group (8.56 ± 0.04 vs 8.16 ± 0.05, P =0.0001). Of note, male gender distribution showed a statistically significant difference between the two groups. Table 1 summarizes the general demographics and comparison between SA and GA in terms of maternal factors. Also, Table 2 summarizes the differences between elective and emergency CS.
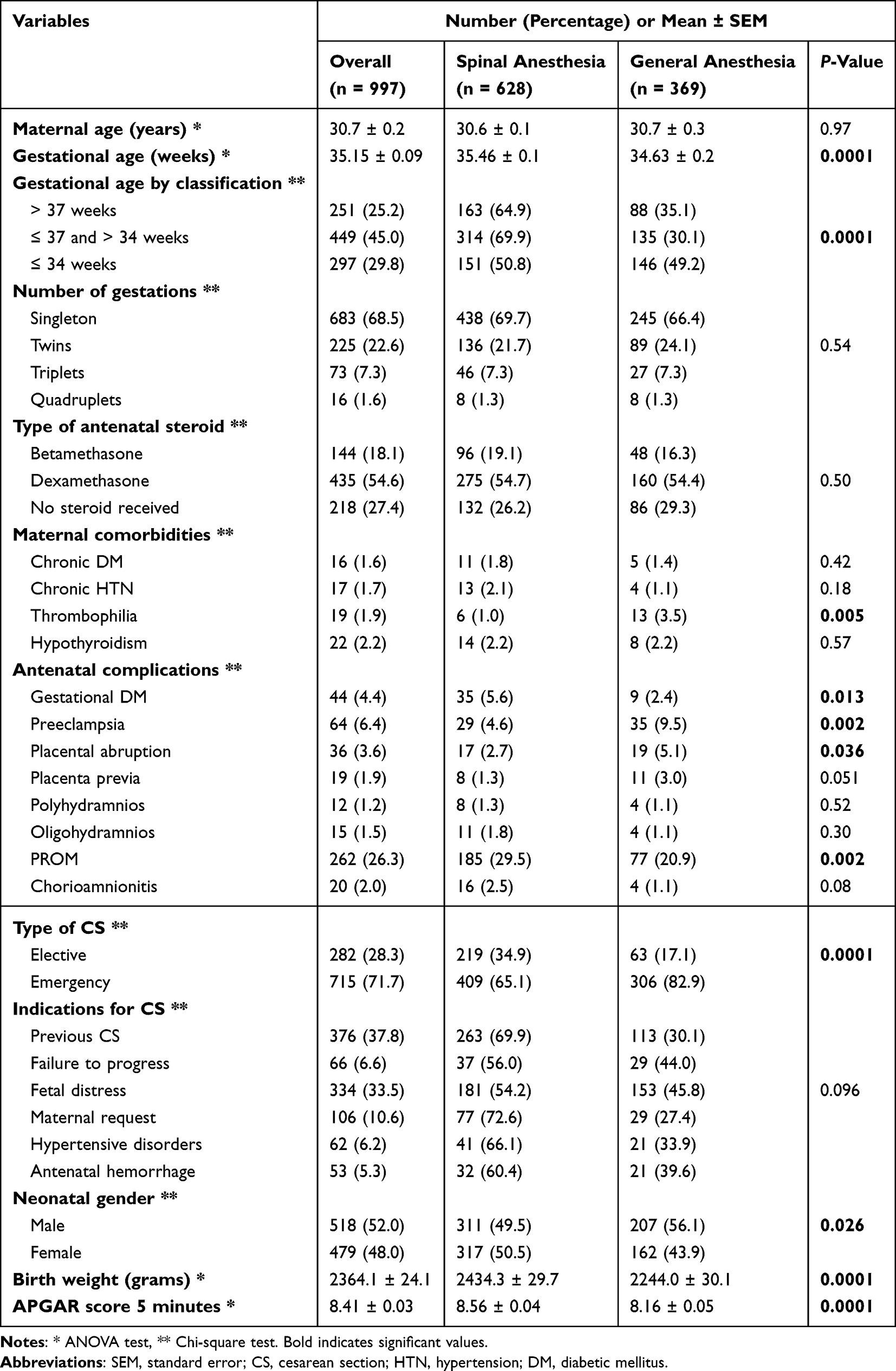 |
Table 1 General Demographics and Comparison Between Spinal and General Anesthesia in Term of Maternal Factors |
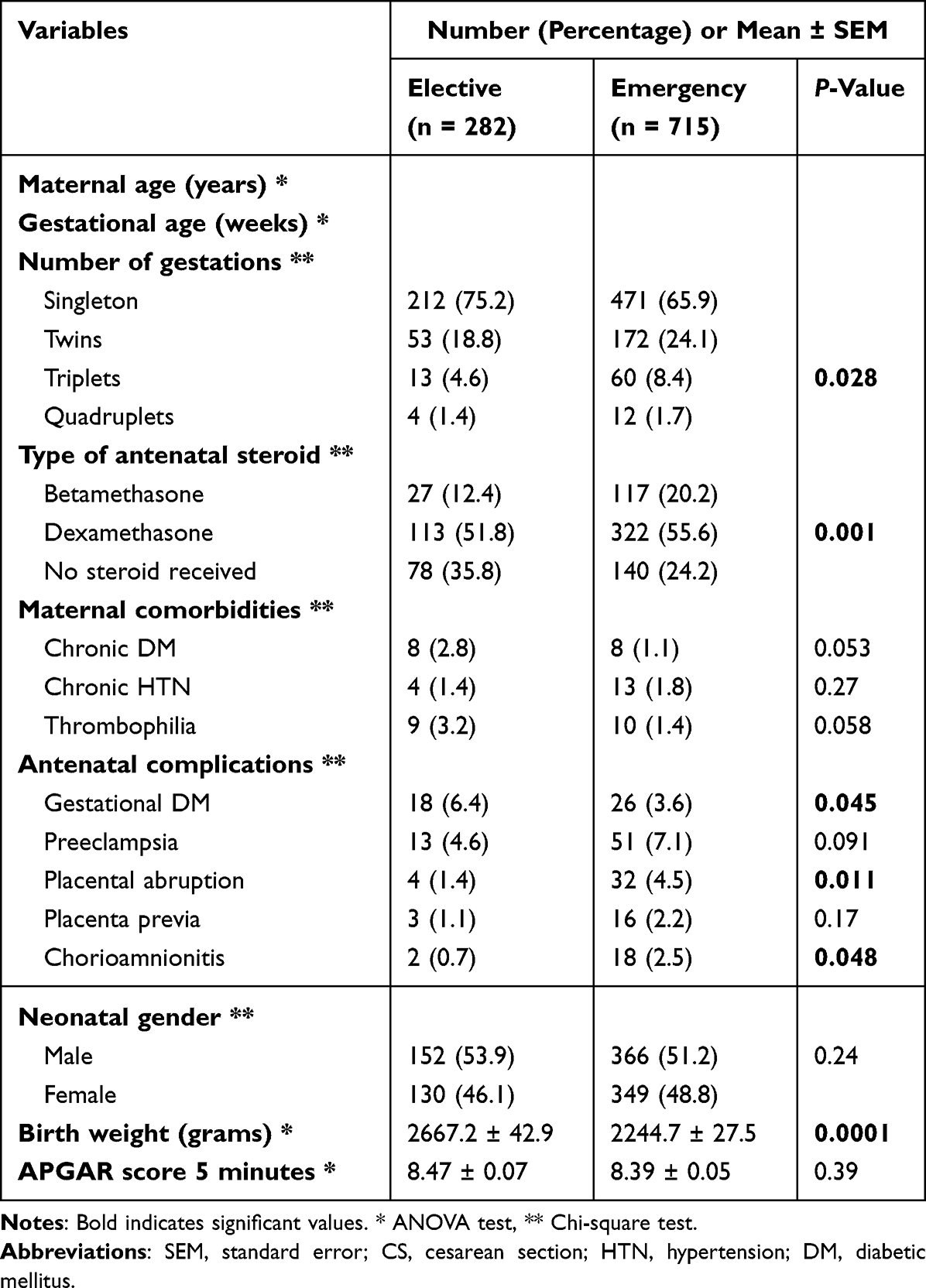 |
Table 2 Comparison Between Elective and Emergency CS |
Comparison Between SA and GA in Terms of Neonatal Respiratory Outcomes
Our univariate analysis of respiratory outcomes revealed significant differences in the incidence of RDS, TTN, chronic lung disease, the use of aminophylline and inhaled corticosteroids, and the duration of CPAP use. In contrast, no significant differences were observed in the incidence of pulmonary HTN, pneumothorax, pulmonary hemorrhage, apnea of prematurity, or the use of surfactant and sildenafil. Additionally, the duration of continuous mandatory ventilation, high-flow nasal cannula use, and time spent on room air also showed no significant differences. RDS was observed in 379 newborns (38.00%), with a higher incidence in the GA group compared to the SA group (156 affected (42.30%) vs 223 affected (35.50%), P =0.02).
Notably, TTN was identified in 102 newborns (10.20%), with a higher prevalence in the SA group compared to the GA group (79 cases (12.60%) vs 23 cases (6.20%), P =0.001). Mild, moderate, and severe lung diseases were reported in 28 newborns (2.80%), 17 newborns (1.70%), and 3 newborns (0.30%), respectively. For the mild chronic lung disease, 28 newborns (2.80%) were affected, 10 cases (1.60%) in the SA group and 18 cases (4.90%) in the GA group. In regards of moderate chronic lung disease, 17 newborns (1.70%) were affected, 10 cases (1.60%) in the SA group and 7 cases (1.90%) in the GA group. Finally, severe chronic lung disease affected 3 newborns (0.30%), 2 cases (0.30%) in the SA group and 1 case (0.03%) in the GA group. Finally, the duration of CPAP differed significantly between the two groups, with a mean duration of 4.44 ± 0.05 days (3.98 ± 0.07 days in the SA group vs 5.20 ± 0.10 in the GA group, P =0.039). Table 3 compares SA and GA in terms of respiratory outcomes.
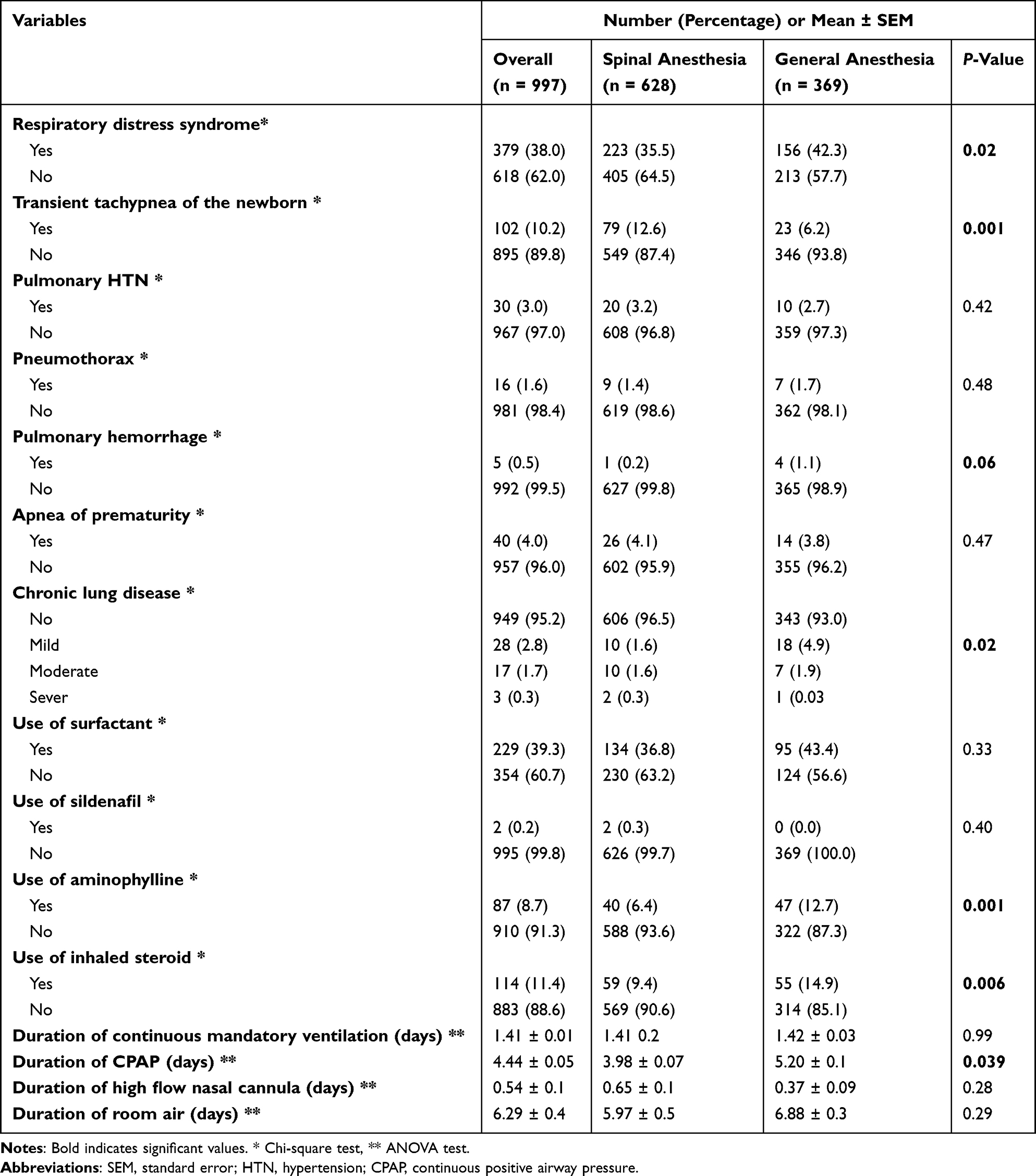 |
Table 3 Comparison Between Spinal and General Anesthesia in Term of Respiratory Outcomes |
Binary logistic regression analysis was conducted to adjust the independent factors affecting the respiratory outcomes; RDS, TTN, duration on CPAP, and utilization of inhaled steroid and aminophylline. The development of RDS was found to be affected independently by less birth weight, earlier gestational age, the presence of PET, and by GA. It was revealed that GA cases were at 1.8-fold risk for RDS than SA (Table 4). Moreover, the independent factors affecting the development of TTN were SA and gestational age. SA cases were associated with 1.9-fold risk of TTN than GA. The other respiratory parameters were not associated with the mode of anesthesia on the binary logistic regression analysis.
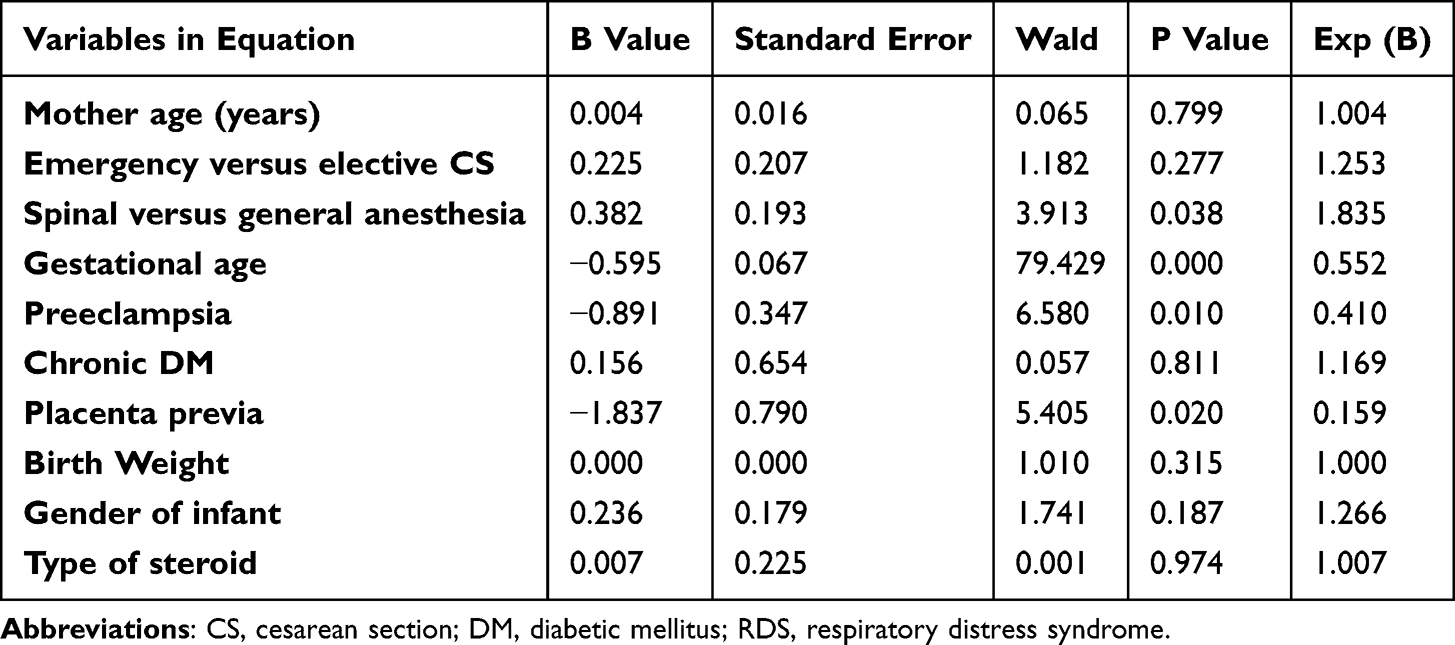 |
Table 4 Regression Analysis Regarding Factors Affecting RDS |
Comparison Between SA and GA in Terms of Neurological Outcome
Multiple neurological manifestations were observed in our study, with significant associations noted between the presence and absence of IVH and its stages, the use of external ventricular drainage (EVD), and the need for ventriculoperitoneal shunting (VPS). In contrast, no significant associations were found with PVL, myelomeningocele, or the use of magnesium sulfate. 55 newborns (5.50%) in our study were diagnosed with IVH, with significantly higher incidence in the GA group (P =0.0001). Among these, 40 newborns (4.00%) had stage 1 IVH, 8 (0.80%) had stage 2, 5 (0.50%) had stage 3, and 2 (0.20%) had stage 4. Of the 55 newborns with IVH, 5 (0.80%) were in the SA group and had stage 1 IVH, while the remaining 50 newborns (13.60%) were in the GA group: 35 (9.50%) had stage 1 IVH, 8 (2.20%) had stage 2, 5 (1.40%) had stage 3, and 2 (0.50%) had stage 4. Table 5 compares SA and GA in terms of neurological outcomes.
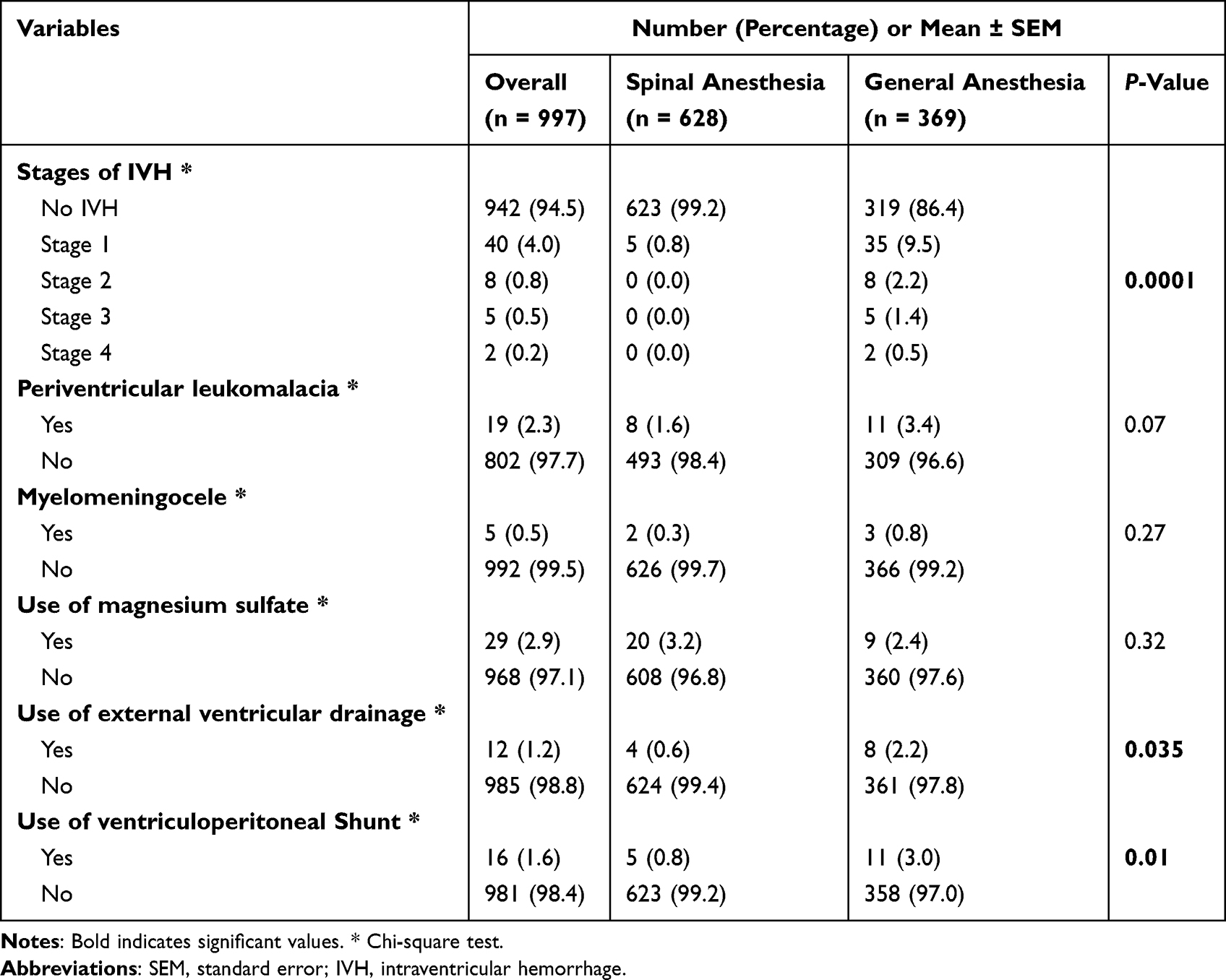 |
Table 5 Comparison Between Spinal and General Anesthesia in Term of Neurological Outcome |
Logistic regression analysis was run to adjust different factors affecting the stages of IVH, the use of external ventricular drainage device, and the use of ventriculoperitoneal shunt. Independently, earlier gestational age, and GA were associated with more advanced stages of IVH. Furthermore, GA was associated independently with the need for ventriculoperitoneal shunt.
Comparison Between SA and GA in Terms of Hematological Outcomes
Our analysis of the difference between SA and GA in terms of hematological outcomes revealed several significant differences. Thrombocytopenia, the need for packed red blood cell (PRBC) transfusion, erythropoietin administration, platelet transfusion, and phototherapy for neonatal jaundice, as well as the duration of phototherapy, all showed significant differences. However, the need for exchange transfusion and intravenous immunoglobulin did not show significant differences. The number of neonates who developed thrombocytopenia was 142 newborns (14.20%). Among these, 78 newborns (12.40%) were in the SA group whereas 64 newborns (17.30%) were in the GA group. Thrombocytopenia was significantly more common in the GA group (P =0.021). Table 6 compares SA and GA in terms of hematological outcomes.
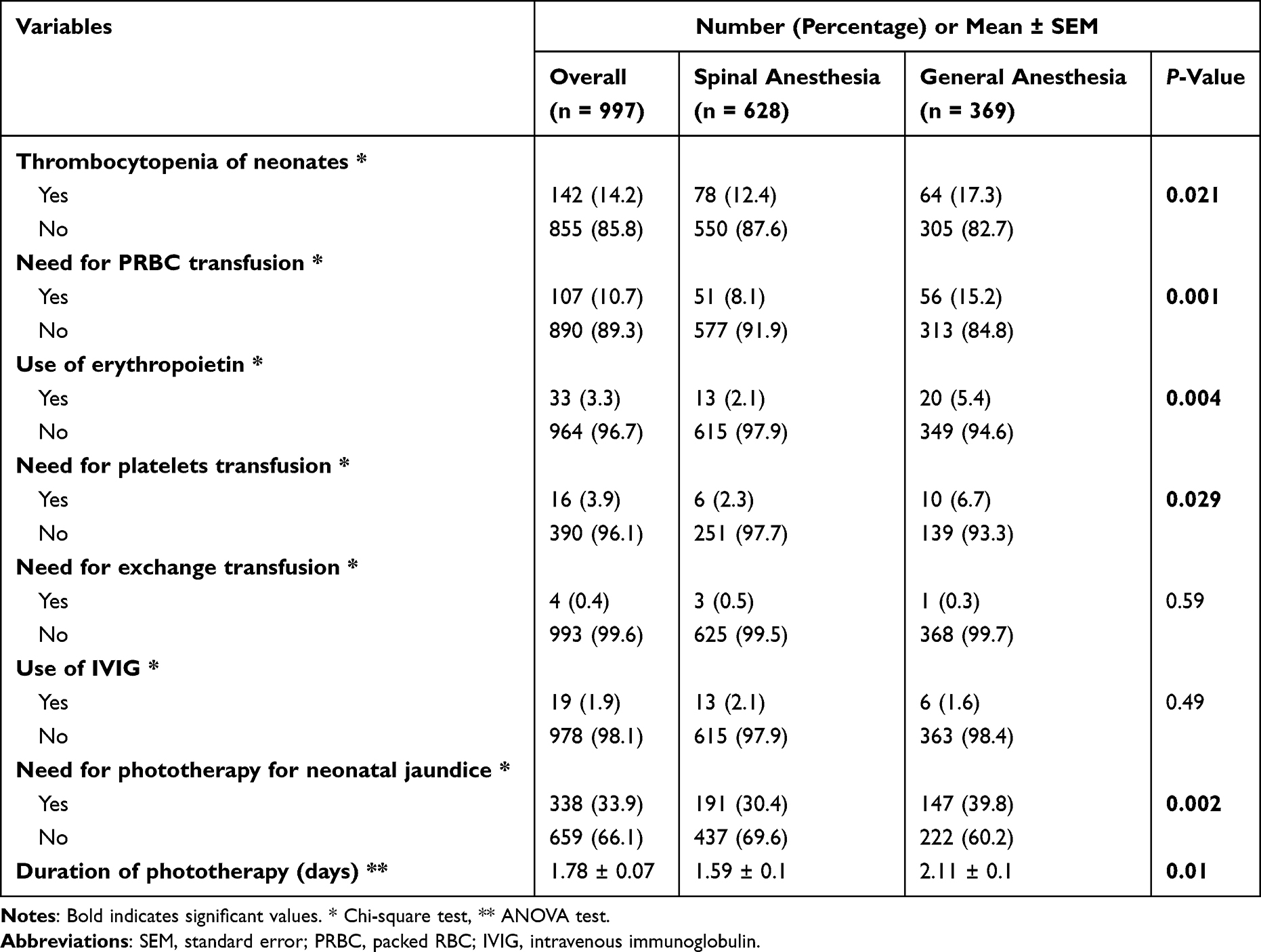 |
Table 6 Comparison Between Spinal and General Anesthesia in Term of Hematological Outcome |
On logistic regression analysis, the mode of anesthesia was not associated with the hematological outcomes.
Comparison Between SA and GA in Terms of Neonatal Death and Other Anomalies
Our analysis revealed significant difference in terms of birth depression, neonatal death, length of hospitalization, and neonatal weight at discharge. Whereas, the development of necrotizing enterocolitis, omphalocele, gastroschisis, diaphragmatic hernia, arrythmias, small for gestational age, and large for gestational age showed no significance between the two groups. A total of 66 neonates (6.60%) experienced birth depression, with 27 (4.30%) in the SA group and 39 (10.60%) in the GA group. The incidence of birth depression was significantly higher in the GA group (P =0.0001). Overall, there were 65 neonatal deaths (6.50%), 25 of which (4.00%) were in the SA group and 40 (10.80%) were in the GA group. Neonatal death rates were significantly higher with the GA group (P =0.0001). The mean length of hospitalization was 11.72 ± 0.50 days, with the GA group showing a significantly longer hospitalization compared to the SA group (13.37 ± 0.90 days vs 10.76 ± 0.60 days, P =0.017). Table 7 compares SA and GA in terms of neonatal death and other anomalies.
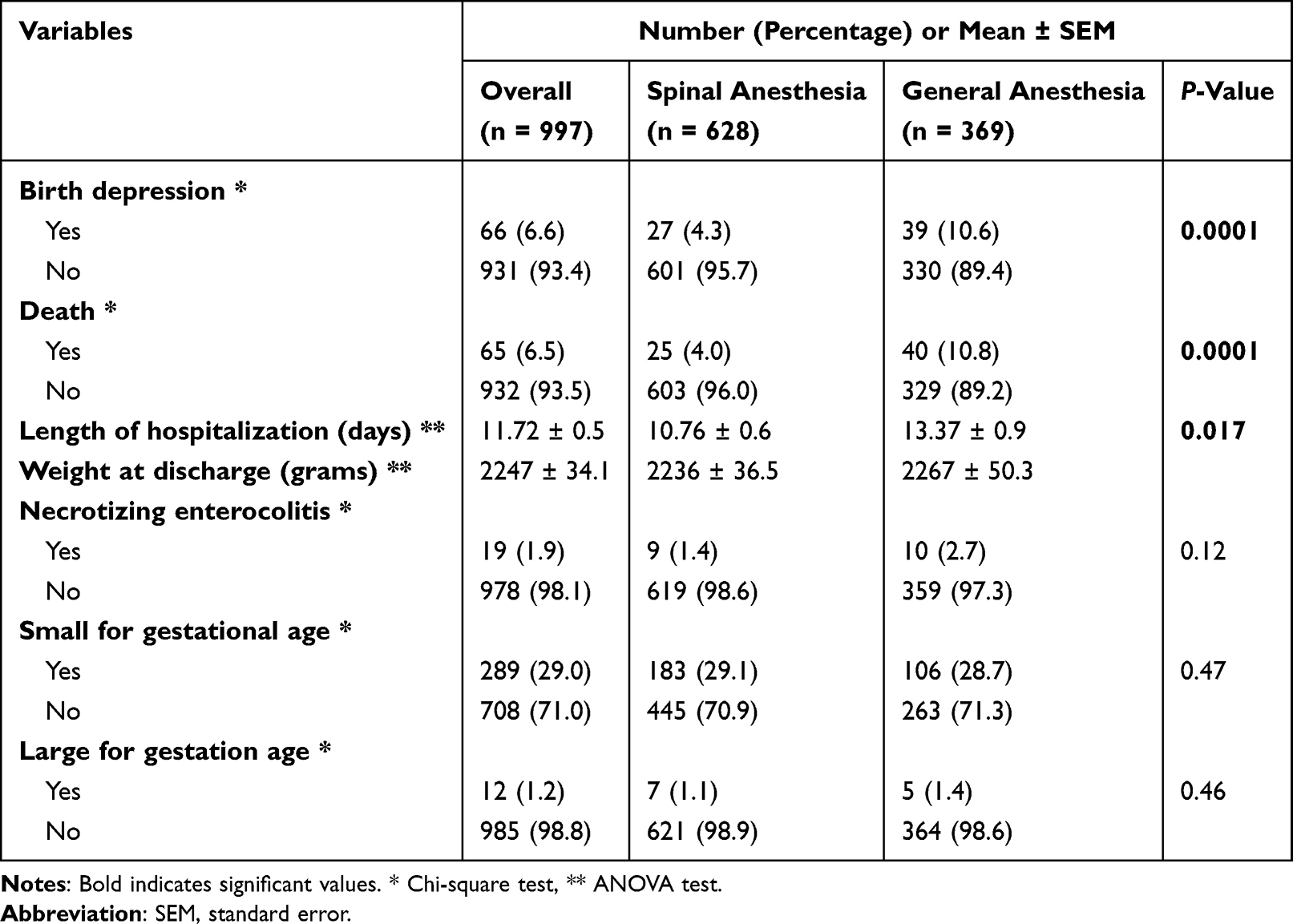 |
Table 7 Comparison Between Spinal and General Anesthesia in Term of Neonatal Death and Other Anomalies |
On logistic regression analysis, it was revealed that earlier gestational age and GA were independent factors affecting the death. Moreover, GA was the independent factor affecting birth depression. The length of hospitalization was not associated independently with the mode of anesthesia.
Discussion
This study compared neonatal outcomes of this magnitude between regional anesthesia (ie., SA) and GA in patients undergoing CS, both elective and emergency. Overall, our findings may indicate SA was associated with better maternal and neonatal outcomes. However, it is important to acknowledge that the majority of patients receiving GA underwent emergency CS. Maternal comorbidities were comparable between the two groups (ie., chronic diabetes mellitus, chronic hypertension, and hypothyroidism), with the exception of thrombophilia, which was more prevalent in the GA group. This finding may suggest an association, as thrombophilia is implicated with adverse pregnancy outcomes such as late pregnancy losses, placental abruption, and preeclampsia,19 potentially increasing the risk of emergency CS. Conversely, Arodi et al concluded in their study that CS was indicated due to obstetrical causes, rather than thrombophilia-related factors, when the condition was properly diagnosed and managed.20 Therefore, it is equally plausible that the observed association may be coincidental. Further research, controlling potential confounding factors, is needed to delineate the effect of thrombophilia on pregnancy and type of delivery. Moreover, several antenatal complications analyzed in this study, including GDM, preeclampsia, placental abruption, and PROM, demonstrated significant differences. Notably, GDM was more frequently reported in the SA group. Several factors may explain this finding. According to the National Institute for Health and Care Excellence (NICE) guidelines, women with GDM should be advised to deliver by induction of labor or CS (if indicated) no later than 40 weeks plus 6 days of gestation.21 This underscores the management of GDM in a controlled setting, where elective CS are often planned in advance. In such cases, patients may opt for the anesthesia type perceived to be least complicated or recommended by their healthcare providers. It is noteworthy that SA was significantly more common in elective CS. Furthermore, preeclampsia and placental abruption were more frequently observed in the GA group, both of which fall under the category of abnormal placentation. These complications are not uncommon in pregnancy and have been increasingly linked to defective utero-placental remodeling and the emergence of placental vascular pathologies in previous years.22,23 Pregnant ladies with such conditions are considered to have high-risk pregnancies. It is possible that these conditions, especially if underdiagnosed, elevate the risk of pregnancy complications,22–24 thereby contributing to the significantly higher incidence in GA use in this group. However, confounding factors, such as pre-existing vascular diseases, use of vasoconstrictive agents, family history, obesity, and other risk factors for abnormal placentation should be controlled to better delineate the association. Further studies are warranted to control these variables and provide a more comprehensive understanding of the underlying relationships. It is also critical to acknowledge that maternal comorbidities (including thrombophilia, preeclampsia, placental abruption, and gestational diabetes mellitus) and obstetric complications represent important alternative explanations for adverse neonatal outcomes, independent of the anesthetic modality chosen. These confounders should be carefully considered when interpreting the associations reported in this study, as they may largely account for the observed outcome differences between groups. On the other hand, PROM was more prevalent in the SA group. One possible explanation is that women undergoing elective CS, which was more commonly performed under SA, had more risk factors for PROM, such as higher gestational age (which was significantly higher is the SA group compared to the GA group in our cohort), infection, or prior history of PROM. Alternatively, PROM itself could serve as a risk factor necessitating an elective CS, either due to complications in pregnancy management or as a result of failed induction of labor. PROM is often managed expectantly if no contraindications arise, which can lengthen the duration of pregnancy and increase the likelihood of elective CS.25 In our study, neonates born to mothers under GA had significantly lower birth weights and Apgar scores compared to those in the SA group. However, a study by Kavak et al found comparable mean birth weights and Apgar scores between GA and SA groups in patients randomly allocated for elective repeat CS.26 This indicates that the observed difference in these parameters in our study may be attributed to the type of CS (emergency vs elective) rather than the choice of anesthesia. This also could be highlighted as the gestational age of delivery of GA women were lower than SA.
From our study, it was evident that the incidence of RDS and TTN differed significantly between the two groups. RDS was more common among newborns delivered under GA, whereas TTN was more common among those delivered under SA. It is important to note that these two conditions showed opposite trends between the two anesthesia groups; therefore, it would be an oversimplification to conclude broadly that GA is associated with uniformly worse respiratory outcomes. The higher RDS rate with GA likely reflects the lower gestational age and emergency status in this group, while the higher TTN rate with SA may relate to the higher proportion of elective term deliveries in the SA group. CS itself is associated with an increased risk of adverse neonatal respiratory outcomes CS itself is associated with an increased risk of adverse neonatal respiratory outcomes, especially when delivery occurs before the onset of labor. Gestational age is a known risk factor for developing RDS, with decreasing incidence as gestational age increases.27 This aligns with our results, as newborns delivered under GA had a lower gestational age and developed RDS more.28 In contrast, TTN is more commonly seen in term or near-term deliveries. However, the literature on this topic is inconsistent. Some studies recommend SA to avoid TTN,29 which contrasts our findings, while others have linked TTN to CS regardless of anesthesia type.30 Other neonatal respiratory parameters in our cohort showed significant differences between the two groups, including the incidence of chronic lung disease, the need for aminophylline, the need for inhaled steroids, and the duration of CPAP.
In our study, we explored neonatal neurological sequelae and their association with each type of anesthesia. Our findings revealed significant differences between the two groups in the incidence of IVH, the need for EVD, and the placement of VPS. IVH is a common neurological complication in preterm neonates, correlating directly to their birth weight and gestational age. It is primarily caused by cerebral ischemia-reperfusion injury.31 Interestingly, low umbilical cord arterial pH has been linked to neonatal mortality, hypoxic ischemic encephalopathy, cerebral palsy, periventricular leukomalacia, and IVH.32 Given this, we propose that low umbilical cord arterial pH may directly contribute to the development of IVH. Supporting this hypothesis, a study by Ozden et al found that neonate delivered under GA exhibited lower pH,33 aligning with our results.
Regarding hematological neonatal outcomes, several significant differences were observed between the two groups in our cohort. Neonates delivered under GA more frequently developed thrombocytopenia, required PRBC transfusion, required platelet transfusion, needed erythropoietin, required phototherapy for neonatal jaundice, and had longer durations of phototherapy. Neonatal thrombocytopenia can be classified into early (<72hr after delivery) and late (>72hr after delivery) onset. Early onset is commonly attributed to placental insufficiency, whereas late onset is often caused by sepsis and NEC. It is important to note that maternal preeclampsia and intrauterine growth restriction are known risk factors for placental insufficiency, which can result in neonatal thrombocytopenia.34 In our cohort, a higher incidence of preeclampsia was observed in the GA group, which may account for the increased risk of thrombocytopenia in this group. However, there were no significant differences in the development of NEC between the two groups, and other potential risk factors (eg., congenital infections, perinatal infections, autoimmune diseases, bone marrow disorders) were not evaluated in our study.34 The increased need for platelet transfusion in the GA group is likely attributable to the higher incidence of neonatal thrombocytopenia. Moreover, many medical conditions may necessitate the use of PRBC, erythropoietin, and phototherapy in neonates. PRBC transfusion is most commonly indicated for the acute treatment of perinatal hemorrhagic shock and correction of anemia of prematurity.35 Erythropoietin can be used to treat anemia of prematurity and hemolytic anemia, though clear guidelines regarding its administration remain lacking.36 On the other hand, conflicting findings are evident in literature regarding neonatal jaundice and the need for phototherapy. A study by Ozcakir et al revealed no significant difference in bilirubin levels between neonates delivered under GA and those delivered under epidural anesthesia during elective CS.37 Similarly, Eskicioğlu et al studied the effects of various anesthetic techniques during CS and vaginal deliveries on neonatal bilirubin levels. While they found no significant difference in bilirubin levels between neonates delivered by CS under GA versus SA, they observed significantly higher bilirubin levels in neonates delivered by CS compared to those delivered vaginally.38 In contrast, a study by Alkan et al reported higher bilirubin levels in neonates delivered under GA and epidural anesthesia compared to those delivered under SA.39 These discrepancies in literature underscore the need for further research to understand the impact of anesthesia type on neonatal bilirubin levels, with consideration of relevant risk factors.
Our study also investigated neonatal mortality and other anomalies. In our cohort, birth depression, neonatal mortality, length of hospitalization, and discharge weight were significantly higher in the GA group. Birth depression, defined as a 5-minute Apgar score of 0–3, is considered as a strong indicator of 1-year mortality in newborns.40 Similar to our findings, Joo et al reported that neonates delivered under GA had significantly lower Apgar scores at both 1 and 5 minutes, required resuscitation more frequently, had higher rates of intensive care unit admissions, and needed respiratory support more often compared to those delivered under SA.41 On the contrary to our findings, studies by Ong et al6 and Ozden et al33 both found no significant differences in neonatal mortality in their cohort between neonates delivered under GA and those delivered under SA. Regarding the length of hospitalization, neonates in the GA group in our cohort experienced an increased rate of complications, including RDS, IVH, neonatal thrombocytopenia, and the need for phototherapy. These complications likely lead to an extended hospital stay as they required additional time for recovery. Lastly, weight at discharge was higher in the GA group. We hypothesize that the lower gestational age and longer hospital stay may have contributed to this result, which allowed for additional gains of weight during their extended stay; however, confounding factors were not accounted for, and further research is needed to explain such findings and their potential implications.
Regarding medications used in GA, induction of GA is conducted by a rapid-acting intravenous agent (thiopental, methohexital, ketamine, propofol, or midazolam), supported with a neuromuscular blocking agent (rocuronium, atracurium, or succinylcholine), and maintained with an inhalational agent (desflurane, enflurane, isoflurane, halothane, sevoflurane, or nitrous oxide).42 Hodgkinson reported that infants of mothers who had received thiopentone demonstrated more pronounced neurophysiological disturbances than after ketamine.43 Moreover, high doses of ketamine may cause a marked decrease in placental blood flow and arterial hypertension. Surgical concentrations of inhalation medications may cause time and dose-related neonatal depression.44 Accordingly, the global trend is toward SA.45
Regarding post-operative complications, venous thromboembolism (VTE) is an important risk in the perioperative period following cesarean section, particularly in patients with pre-existing thrombophilia or those undergoing emergency procedures. The mode of anesthesia may influence VTE risk indirectly through its effect on mobility, hemodynamic status, and surgical duration; however, dedicated marker detection for VTE was not performed in our study.46
Our study is not without limitations. First, the retrospective nature of the study limits its generalizability (eg. missing important parameters such as Lucas’s classification, APGAR score at 1 minute, detailed laboratory parameters such as hemoglobin level, and umbilical cord analysis data, and possible selection bias). Second, multiple co-founders were assessed during the analysis which may reduce the power of conclusions. The variability between the anesthesia groups limits the generalizability of results. The inclusion of elective and emergency CS is the most crucial and possible misleading and may limit the validity of the conclusions. The issue lies in the fact that neonatal outcomes largely depend on the reason for which the cesarean section was performed. To solve this partially, regression analyses were performed for most variables. Third, many intraoperative and maternal factors were not studied. Fourth, scoring certain factors such as birth depression were not performed. Fifth, the exclusion of cases converted from SA to GA may be considered as bias. Sixth, the study population was restricted to NICU-admitted neonates, which may introduce selection bias and limit generalizability to the broader cesarean section population. Finally, long-term neurodevelopmental and respiratory outcomes of the two anesthesia modalities could not be assessed in this retrospective study and warrant future prospective investigation.
Conclusions
Although the GA was utilized more in emergency cases and extreme premature neonates, its use may be utilized with cautions. It is critical to underscore that GA is preferentially employed in higher-grade emergencies and is associated with more adverse baseline predictors, including lower gestational age, lower birth weight, and greater obstetric complications. Therefore, the observed association between GA and worse neonatal outcomes should be interpreted with caution, as these outcomes may reflect the underlying emergency conditions rather than the anesthetic modality per se. However, GA independently, may be associated with worse respiratory (especially RDS), neurological, and survival neonatal outcomes. SA may offer a localized effect for the anesthetic drugs. This study investigates critical practice in one of the regions where the trends toward SA are still slow and the rates of GA are still high. The results of this retrospective study cannot be generalized, so further prospective trials are needed to justify the risk of both types of anesthesia.
Abbreviations
GA, general anesthesia; SA, spinal anesthesia; CS, cesarean section; NICU, neonatal intensive care unit; RDS, respiratory distress syndrome; TTN, transient tachypnea of newborn; CPAP, continuous positive airway pressure; IVH, intraventricular hemorrhage; PVL, periventricular leukomalacia; NEC, necrotizing enterocolitis; EVD, external ventricular drainage; VPS, ventriculoperitoneal shunting; GDM, gestational diabetes mellitus; PROM, premature rupture of membrane; PRBC, packed red blood cell; HTN, hypertension.
Data Sharing Statement
Data is available upon request from the corresponding author.
Ethics Approval and Consent to Participate
The Institutional Review Board (IRB) at KAUH and JUST approved the study’s ethical conduct under the approval number (5/170/2024). Due to the retrospective nature of the study, the need for the consent form was waived, as per our IRB guidelines. The study is carried out in compliance with the ethical guidelines in place at our institute, taking the Helsinki Declaration as an ethical guideline for research involving human subjects. We confirm that the privacy of the participants was saved, and the data was anonymized and maintained with confidentiality.
Funding
This research received no funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Taşgöz FN, Kılıçarslan N. Effect of anesthesia type on outcome measures in cesarean section in the presence of fetal macrosomia. Revista da Associacao Medica Brasileira (1992). 2022;68(10):1410–16. doi:10.1590/1806-9282.20220382
2. Park JI, Park SH, Kang MS, Kang GW, Kim ST. Evaluation of changes in anesthetic methods for cesarean delivery: an analysis for 5 years using the big data of the Korean Health Insurance Review and Assessment Service. Anesthesia and Pain Medicine. 2020;15(3):305–313. doi:10.17085/apm.20021
3. Sung T-Y, Jee YS, You H-J, Cho CK. Comparison of the effect of general and spinal anesthesia for elective cesarean section on maternal and fetal outcomes: a retrospective cohort study. Anesthesia and Pain Medicine. 2021;16(1):49–55. doi:10.17085/apm.20072
4. Afolabi BB, Lesi AF. Regional versus general anaesthesia for caesarean section. Cochrane Database of Systematic Reviews. 2012;2012(10). doi:10.1002/14651858.CD004350.pub3
5. Nguyen PN, Vuong ADB, Pham XTT. Neonatal outcomes in the surgical management of placenta accreta spectrum disorders: a retrospective single-center observational study from 468 Vietnamese pregnancies beyond 28 weeks of gestation. BMC Pregnancy Childbirth. 2024;24(1):228. doi:10.1186/s12884-024-06349-7
6. Ong B, Cohen MM, Palahniuk RJ. Anesthesia for cesarean section—effects on neonates. Anesthesia Analgesia. 1989;68(3):270–275. doi:10.1213/00000539-198903000-00015
7. Zagorzycki MT, Brinkman III CR. The effect of general and epidural anesthesia upon neonatal Apgar scores in repeat cesarean section. Surgery, Gynecology & Obstetrics. 1982;155(5):641–645.
8. Moisa RC, Negrut N, Macovei IC, et al. The Impact of Maternal Spinal Anesthesia on Newborn Out-Comes: a Clinical Perspective. Children. 2025;12(4):450. doi:10.3390/children12040450
9. Uram-Benka A, Fabri-Galambos I, Pandurov-Brlić M, et al. Optimizing Newborn Outcomes in Cesarean Sections: a Comparative Analysis of Stress Indicators under General and Spinal Anesthesia. Children. 2024;11(7):783. doi:10.3390/children11070783
10. Cocchi E, Pini R, Gallipoli A, et al. Impact of general vs. neuraxial anesthesia on neonatal outcomes in non-elective cesarean sections. Frontiers in Pediatrics. 2025;13. doi:10.3389/fped.2025.1518456
11. Gwanzura C, Gavi S, Mangiza M, et al. Effect of anesthesia administration method on apgar scores of infants born to women undergoing elective cesarean section. BMC Anesthesiology. 2023;23(1):142. doi:10.1186/s12871-023-02098-w
12. Datta S, Ostheimer GW, Weiss JB, Brown Jr WU, Alper MH. Neonatal effect of prolonged anesthetic induction for cesarean section. Obstet Gynecol. 1981;58(3):331–335.
13. Hawkins JL, Chang J, Palmer SK, Gibbs CP, Callaghan WM. Anesthesia-related maternal mortality in the United States: 1979–2002. Obstet Gynecol. 2011;117(1):69–74. doi:10.1097/AOG.0b013e31820093a9
14. Fernandes NL, Dyer RA. Anesthesia for Urgent Cesarean Section. Clinics in Perinatology. 2019;46(4):785–799. doi:10.1016/j.clp.2019.08.010
15. Khasawneh W, Sindiani A, Rawabdeh SA, Aleshawi A, Kanaan D. Indications and Clinical Profile of Neonatal Admissions: a Cross-Sectional Descriptive Analysis from a Single Academic Center in Jordan. Journal of Multidisciplinary Healthcare. 2020;13:997–1006. doi:10.2147/JMDH.S275267
16. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. The Journal of Pediatrics. 1978;92(4):529–534. doi:10.1016/S0022-3476(78)80282-0
17. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114(1):297–316. doi:10.1542/peds.114.1.297
18. Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Annals of Surgery. 1978;187(1):1–7. doi:10.1097/00000658-197801000-00001
19. Battinelli EM, Marshall A, Connors JM. The role of thrombophilia in pregnancy. Thrombosis. 2013;2013(1):516420. doi:10.1155/2013/516420
20. Arodi A, Mazor M, Friger M, Smolin A, Bashiri A. Independent risk factors for cesarean section among women with thrombophilia. The Journal of Maternal-Fetal & Neonatal Medicine. 2009;22(9):770–775. doi:10.3109/14767050902926939
21. NICE. National Institute for Health and Care Excellence: guidelines. In: Diabetes in Pregnancy: Management From Preconception to the Postnatal Period. London: National Institute for Health and Care Excellence (NICE); 2020.
22. Kovo M, Schreiber L, bar J. Placental vascular pathology as a mechanism of disease in pregnancy complications. Thrombosis Research. 2013;131:S18–S21. doi:10.1016/S0049-3848(13)70013-6
23. Romero R, Kusanovic JP, Chaiworapongsa T, Hassan SS. Placental bed disorders in preterm labor, preterm PROM, spontaneous abortion and abruptio placentae. Best Pract Res Clin Obst Gynaecol. 2011;25(3):313–327. doi:10.1016/j.bpobgyn.2011.02.006
24. English FA, Kenny LC, McCarthy FP. Risk factors and effective management of preeclampsia. Integrated Blood Pressure Control. 2015;8:7–12. doi:10.2147/IBPC.S50641
25. Garg A, Jaiswal A. Evaluation and management of premature rupture of membranes: a review article. Cureus. 2023;15(3):1.
26. Kavak ZN, Başgül A, Ceyhan N. Short-term outcome of newborn infants: spinal versus general anesthesia for elective cesarean section: a prospective randomized study. Eur J Obstet Gynecol Reproduct Biol. 2001;100(1):50–54. doi:10.1016/S0301-2115(01)00417-1
27. Yeganegi M, Bahrami R, Azizi S, et al. Caesarean section and respiratory system disorders in newborns. Eur J Obstet Gynecol Reproduct Biol. 2024;2024:100336.
28. Shi X, Xu C, Wen Y, et al. Perinatal outcome of emergency cesarean section under neuraxial anesthesia versus general anesthesia: a seven-year retrospective analysis. BMC Anesthesiology. 2024;24(1):33. doi:10.1186/s12871-024-02412-0
29. Ozden Omaygenc D, Dogu T, Omaygenc MO, et al. Type of anesthesia affects neonatal wellbeing and frequency of transient tachypnea in elective cesarean sections. The Journal of Maternal-Fetal & Neonatal Medicine. 2015;28(5):568–572. doi:10.3109/14767058.2014.926328
30. Keleş E, Yazgan H, Gebeşçe A, Pakır E. The type of anesthesia used during cesarean section is related to the transient tachypnea of the newborn. International Scholarly Research Notices. 2013;2013(1):264340.
31. McCann ME, Lee JK, Inder T.Beyond Anesthesia Toxicity: anesthetic Considerations to Lessen the Risk of Neonatal Neurological Injury. Anesthesia and Analgesia. 2019;129(5):1354–1364. doi:10.1213/ANE.0000000000004271
32. Malin GL, Morris RK, Khan KS. Strength of association between umbilical cord pH and perinatal and long term outcomes: systematic review and meta-analysis. BMJ. 2010;340(may13 1):c1471–c1471. doi:10.1136/bmj.c1471
33. Ozden MGN, Koruk S, Collak Z, Panik N. Comparison of the effects of general and spinal anesthesia for cesarean delivery on maternal and fetal outcomes: a retrospective analysis of data. Northern Clinics of Istanbul. 2023;10(5):575–582. doi:10.14744/nci.2023.25593
34. Roberts I, Murray NA. Neonatal thrombocytopenia: causes and management. Archives of Disease in Childhood-Fetal and Neonatal Edition. 2003;88(5):F359–F364. doi:10.1136/fn.88.5.F359
35. Whyte RK, Jefferies AL. Red blood cell transfusion in newborn infants. Paediatrics Child Health. 2014;19(4):213–217. doi:10.1093/pch/19.4.213
36. Donato H. Erythropoietin: an update on the therapeutic use in newborn infants and children. Expert Opinion on Pharmacotherapy. 2005;6(5):723–734. doi:10.1517/14656566.6.5.723
37. Ozcakir HT, Lacin S, Baytur YB, Lüleci N. Different anesthesiologic strategies have no effect on neonatal jaundice. Eur J Obstet Gynecol Reproduct Biol. 2004;270:179–181.
38. Eskicioğlu F, Ozlem S, Bilgili G, Baytur Y, Sciences R. Evaluation of the effects of different anesthetic techniques on neonatal bilirubin levels. International Journal of Women’s Health and Reproduction Science. 2014;2(1):10–16. doi:10.15296/ijwhr.2014.02
39. Alkan S, Tıraş Ü, Dallar Y, Sunay D. Effect of anaesthetic agents administered to the mothers on transcutaneous bilirubin levels in the neonates. Acta Pædiatrica. 2010;99(7):993–996. doi:10.1111/j.1651-2227.2010.01761.x
40. Miles KG, Liu J, Tseng SY, et al. Neonatal Depression Is Associated With 1-Year Mortality in Critical Congenital Heart Disease. Journal of the American Heart Association. 2023;12(11):e028774. doi:10.1161/JAHA.122.028774
41. Joo YJ, Jeon GW, Lee J, Jun YH. Comparison of Neonatal Outcomes among Patients Undergoing Cesarean Delivery under General or Spinal Anesthesia. Perinatology. 2023;34(3):128–134. doi:10.14734/PN.2023.34.3.128
42. Petropoulos G, Siristatidis C, Salamalekis E, Creatsas G. Spinal and epidural versus general anesthesia for elective cesarean section at term: effect on the acid-base status of the mother and newborn. Journal of Maternal-Fetal & Neonatal Medicine. 2003;13(4):260–266.
43. Hodgkinson R, Marx GF, Kim SS, Miclat NM. Neonatal neurobehabioral tests following vaginal delivery under ketamine, thiopental, and extradural anesthesia. Anesthesia and Analgesia. 1977;56(4):548a. doi:10.1213/00000539-197707000-00018
44. Dick WF. Anaesthesia for caesarean section (epidural and general): effects on the neonate. Eur J Obstet Gynecol Reproduct Biol. 1995;59:S61–S67. doi:10.1016/0028-2243(95)02075-4
45. Juang J, Gabriel RA, Dutton RP, Palanisamy A, Urman RD. Choice of Anesthesia for Cesarean Delivery: an Analysis of the National Anesthesia Clinical Outcomes Registry. Anesthesia and Analgesia. 2017;124(6):1914–1917. doi:10.1213/ANE.0000000000001677
46. Vuong ADB, Tran NH, Pham TH, Ham L, Nguyen PN. Soluble Fibrin Monomer Complex and D-Dimer Concentrations Between Patients at Low and High Risk of Venous Thromboembolism Before Delivery According to RCOG Score Assessment: an Observational Study Among 100 Third-Trimester Vietnamese Pregnancies. J Clin Med. 2025;14(5):1399. doi:10.3390/jcm14051399
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.