Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Mobile application intervention to promote self-management in insulin-requiring type 1 and type 2 diabetes individuals: protocol for a mixed methods study and non-blinded randomized controlled trial
Authors Adu MD ![]() , Malabu UH
, Malabu UH ![]() , Malau-Aduli AEO
, Malau-Aduli AEO ![]() , Malau-Aduli BS
, Malau-Aduli BS ![]()
Received 19 March 2019
Accepted for publication 29 April 2019
Published 24 May 2019 Volume 2019:12 Pages 789—800
DOI https://doi.org/10.2147/DMSO.S208324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Video abstract presented by Mary Adu.
Views: 286
Mary D Adu,1 Usman H Malabu,1 Aduli EO Malau-Aduli,2 Bunmi S Malau-Aduli1
1College of Medicine and Dentistry, James Cook University, Townsville, QLD 4811, Australia; 2College of Public Health, Medical and Veterinary Sciences, James Cook University, Townsville, QLD 4811, Australia
Background: Mobile applications (apps) have proven to be useful in supporting diabetes self-care, but non-consideration of users’ needs and non-inclusion of educational features are reasons for low continual use. Well-designed mobile apps that meet the needs of diabetes patients and provide ongoing self-management education and support are required. It was hypothesized that apps designed with such features can improve a range of measures including clinical outcomes, knowledge of diabetes, medication adherence, perceived ability for self-management, and quality-of-life. This may eventually facilitate a more robust and cost-effective approach for improving skills and motivation for the management of diabetes.
Methods: This project will be conducted in two phases. It will initially employ a mixed methods study design to investigate the self-management needs and perceptions of diabetes patients on the use of mobile apps to support diabetes self-management. Results of the mixed methods study will inform the content and design of an app which will be employed as an intervention tool in a 12-month parallel randomized controlled trial (RCT). The RCT will compare outcomes in relation to standard-of-care alone with standard-of-care plus a mobile phone diabetes app among 150 insulin-requiring types 1 and 2 diabetes patients. The primary outcome measures are clinical parameters such as hemoglobin A1c (HbA1c), lipids, urine albumin-to-creatinine ratio, blood pressure, frequency in events of emergency hyperglycemia and hypoglycemia. Secondary outcomes include knowledge of diabetes, medication intake and adherence, perception of self-care, and quality-of-life.
Discussion: Results from this study will provide empirical evidence on the usefulness of a mobile app developed based on self-management needs analysis of diabetic patients. The long-term goal is to harness knowledge gained from this study to provide evidenced-based data, which promote the scale-up or adoption of mobile applications that provide regular, ongoing education and self-management support to people living with diabetes.
Trial registration: Australian New Zealand Clinical Trials Registry, ACTRN12618000065291, Registered on 17 January, 2018 (prospectively registered).
Keywords: randomized controlled trial, mixed methods design, diabetes, self-management education, mobile application
Introduction
Developing knowledge and skills on targeted self-management behaviors for the prevention and early detection of diabetes complications can only occur through a process of learning known as Diabetes Self Care Education (DSCE).1,2 DSCE should go beyond the present recommendation of occurrence at diagnosis, annually, when a new complication sets in or during transition in care,3,4 to a more regular event with consistent reinforcement of educational components.5 This is essential to promote awareness of the importance of self-management, build the resilience needed to overcome barriers, cope with ongoing demands, and sustain required behaviors during the course of treatment and life transitions.6,7 Studies have shown better clinical outcomes in patients with every increment in time spent on diabetes education.8–10
In most cases, the complexity, chronic nature of diabetes, and the required daily management usually make adherence to prescribed self-management recommendations difficult for patients.11,12 Poor adherence usually results from the fact that a significant percentage of patients do not have sufficient knowledge, skills, motivation, and self-efficacy for self-management, which consequently results in complications.13,14 Insight into specific self-management areas where people with diabetes are often lacking in understanding, skills, motivation, and efficacy can inform the planning of an improved educational intervention.
With advancement in computer programming and ubiquity of mobile communication devices, it is possible to leverage on these technologies to empower patients through regular self-monitoring and disease management programs.15 Technologies in the form of websites, software applications, and mobile devices have persuasive attributes that can change users’ attitudes or behaviors in a predetermined way.16,17 The use of these technologies enables the delivery of healthcare outside the clinical environment,18 and provides ongoing self-management support and education.19,20 These technologies foster improved knowledge and promote the importance of daily self-management activities to prevent the risk of complications in patients with diabetes.21–24 However, despite the several advantages, proven effectiveness, and investments into the technological development process of apps for diabetes self-management; two major issues have limited the successful adoption of apps as a self-management tool. First, previous use of apps as interventions was characterized by high attrition rates.25–29 This low level of continuous acceptance has been attributed to insufficient consideration of users’ perceptions of its usability requirements.30–32 Second, self-management education, which is a critical component of diabetes care, has been shown to be an under-represented feature in the majority of available diabetes mobile apps.19,33–35
The reported body of evidence on significant deficits in patients’ knowledge, skills, and efficacy for diabetes self-management suggests the necessity for a participatory evaluation of the self-management education needs of patients. The needs analysis will provide insight into specific areas of reinforcement during diabetes education intervention. Additionally, high attrition rate serves as a limiting factor in the ongoing use of apps as a self-management tool. This problem is an indication of the importance of assessing the mobile app needs of patients in terms of preferred app features and exploring their recommendations on how to foster better engagement with diabetes self-management apps. Although there are many currently available diabetes self-management apps, the majority of them were not developed with users’ input, neither do they lead to long-term improved health and behavioral outcomes.36 Developing a diabetes app that best meets identified patients’ needs with the inclusion of consistent educational features could possibly provide an effective method to increase patients’ knowledge, skills, efficacy, motivation, and compliance with recommended self-management activities. Ultimately, this procedure may improve health outcomes, quality-of-life, and prevent or delay the onset of diabetes complications. Therefore, the study aims to:
- Assess the needs of patients with regards to their self-management skills and efficacy, preferred features in apps, and opinions on better engagement with mobile apps for diabetes management;
- Develop a mobile app that best meets patients’ identified needs;
- Use a randomized controlled trial to investigate the impact of the developed mobile app on hemoglobin A1c (HbA1c), albumin creatinine ratio (ACR), blood pressure (BP), lipids, anthropometric parameters, and events of hypoglycemia and hyperglycemia;
- Estimate changes in knowledge of diabetes management, medication intake and adherence, perceived efficacy in diabetes self-management, and quality-of-life pre- and post-intervention; and
- Determine the cost-effectiveness of the intervention relative to standard care.
Study hypothesis
The use of a mobile app developed based on self-management education and support needs of people with diabetes will improve clinical outcomes, diabetes management knowledge, medication adherence, perceived ability to perform self-management, and quality-of-life.
Significance and innovation of research
Based on the proposed hypothesis, this project is expected to provide better health outcomes for people with diabetes through excellent and innovative provision of self-support and educational intervention. The educational delivery model is intended to utilize best practice educational methods and persuasive technologies to maximize improved health outcomes. The strength of this research lies in its targeted approach at meeting priority patient needs, connective links to health education, and fostering better health outcomes and quality-of-life for people with diabetes.
The results of this study will promote diabetes patients’ self-management via consistent and effective education and support in order to reduce their risk of developing complications. Furthermore, it is hoped that the outcome of this project will contribute to meeting one of the goals of the Australian National Diabetes Strategy 2016–2020, which is to “reduce the occurrence of diabetes-related complications and improve the quality-of-life among people with diabetes”.37
Research plans and methods
Figure 1 shows a detailed outline of the research plan. The project will be conducted in two phases using a mixed methods study design and randomized controlled trial, respectively.
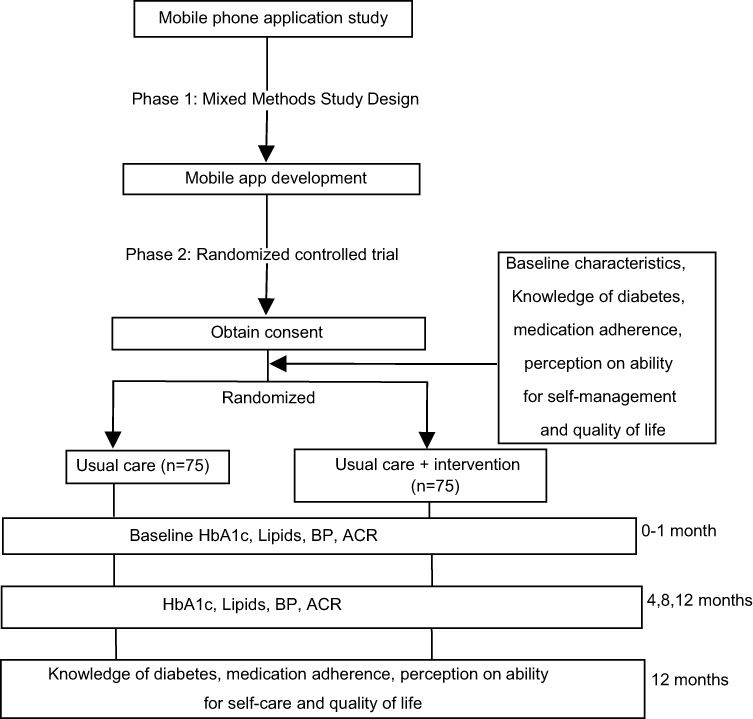 | Figure 1 Detailed outline of research plan |
Phase 1
Study design and population
This phase will utilize a mixed methods study design to identify the common self-management education needs and perceptions of the use of mobile apps for self-support among people who have diabetes. This method allows for a complete and synergistic utilization of data to validate findings from qualitative and quantitative data sources.38Any person with type 1 or type 2 diabetes and above the age of 18 years is eligible to participate in this study. This study is cross-sectional in nature and mainly aims at estimating the frequency of health behaviors and consensus on features in a mobile health technology. A priori statistical G-power analysis39 was conducted to estimate the minimum sample size required to reduce the risk of Type 1 and Type 2 errors. The analysis revealed that 128 participants are required to achieve 80% power with level of significance set at a standard of 5% in order to control for type 1 error.
Data collection
Data will be collected via online survey (designed using Survey Monkey) and individual telephone interviews. The study will be advertised widely and internationally through social media outlets, websites of diverse diabetes associations, and local newspapers. Advertisement will ensure that various demographics and international audiences are adequately represented. Participants will complete a 10–12 minute online questionnaire sub-divided into three major parts: i) demographic characteristics; ii) validated tool for assessing self-management education, skills, and self-efficacy needs;40 iii) questions developed from a review of published literature to elucidate patients’ preferred features in diabetes management apps and recommendations to foster better engagement with such apps. The main content of the questionnaire will follow an information and consent page.
Upon completion of the questionnaire, participants will be invited to participate in a 10–20 minutes telephone interview. Consenting participants to this part of the study will be asked to provide their preferred phone contact details. The interview session will provide an opportunity for data triangulation and in-depth understanding of the findings from the survey. The interview process will be ongoing until data saturation is attained enabling the research questions to be adequately answered. Data saturation is reached when incoming information results in minimal or no changes to the codebook.41
Quantitative data analysis
Data from the questionnaire will be summarized using descriptive statistics. Demographic predictors of self-management skills and efficacy as well as perceptions of preferred app features will be identified using bivariate and regression analyses.42 Significance levels will be set at a P-value less than 0.05.
Qualitative data analysis
Data from telephone interviews will be audiotaped, transcribed, and analyzed in N-Vivo using in-depth thematic analysis for identifying, analyzing, reporting patterns within the data, organizing (minimally) and describing the data in rich detail.43 The data will be subjected to inductive, bottom-up analysis to elicit emerging themes that are directly linked to the study.43
Outcomes
The major outcomes of interest for this phase of the study include common self-management education needs of patients identified through knowledge gaps in specific diabetes management skills and self-efficacy; preferred features in mobile diabetes app and approaches to foster consistent engagement with self-management diabetes apps. These findings will inform the development of a new mobile app and self-management educational intervention. This phase is geared towards achieving the first and second aims of the project.
Development, usability and pilot testing of mobile app
We hypothesized that participants’ preferences will be influenced by their educational status, age, country of residence, level of familiarity with modern technologies, and the type of diabetes they have. Therefore, the results emanating from this phase of the project will be thoughtfully considered and prioritized in the development of the app. Priority will be given to nominated app features with empirical evidence on the management of diabetes and best interventional techniques likely to promote health behavioral change. Features and ideas that maximize usability and engagement with the app will also be considered. Overall, the app will be designed based on the identified needs of the users.
The newly-developed mobile app will be validated in two stages. In the first stage, usability testing of the user interface, app design elements, and satisfaction with the app will be done using an adapted version of the Mobile App Rating Scale (MARS).44 MARS is a useful tool which could provide essential information for the design and development of new apps in terms of assessing an apps’ esthetics, functionality, and information quality. The tool has been found to be simple, objective, and reliable for assessing the quality of a broad spectrum of user interfaces.44 A mix of participants including a minimum of 10 members of the public and people who have type 1 or type 2 diabetes will be asked to use the app and provide feedback using the adapted tool. This strategy is essential for ascertaining the technical performance of the app and navigation issues (if any) when downloaded on various mobile phones. Necessary improvement to the app will be made according to results from the usability testing. The second stage will involve pilot testing of the app in order to assess its’ acceptability and feasibility and preliminary efficacy for wider implementation in the randomized controlled trial.
Phase 2
Study design
This phase will be a parallel randomized controlled trial (RCT) comparing patient outcomes for standard-of-care alone vs standard-of-care plus a mobile diabetes app intervention (newly-developed app). RCT allows for rigorous research to determine cause–effect relationships between intervention and outcomes and ensure that there are no systemic differences between both groups that may affect results.45
Setting
The research will be conducted in the diabetes centers of a tertiary hospital and a community health campus in North Queensland, Australia. Both centers are operated by the Townsville Hospital and Health Service. This service serves a socially and ethnically diverse group of people with diabetes.46
Most public hospital services in Australia are financed by the state, territory, and the Australian Commonwealth Governments. Australia’s health funding, referred to as Medicare, largely covers the necessary healthcare cost that patients require, including medical services, allied health services, and pharmaceuticals.47 In addition to Medicare, the National Diabetes Service Scheme (NDSS) provides a range of support services to Australians diagnosed with diabetes. Part of the services includes payment for accessing diabetes self-management education (DSME) from a Credentialed Diabetes Educator. The focus of DSME is the provision of support which may be educational, psychosocial, or clinically guided by evidence-based standards.48,49
Eligibility
Eligibility criteria include i) Adults above 18 years of age; ii) Diagnosed with type 1 or 2 diabetes; iii) Using insulin therapy with or without oral antidiabetic agents; iv) Using a smart phone; and v) Willing to return for follow-up at 4, 8, and 12 months. Inclusion of only insulin-requiring type 1 and type 2 diabetes patients was based on the fact that diabetes patients with these characteristics have the highest likelihood to regularly monitor their blood glucose levels, since it is a standard pre-requisite prior to insulin dose administration. Additionally, there is a high probability that the new app will include a blood glucose tracking feature because regular blood glucose monitoring is an important self-management activity for diabetes patients (especially those requiring insulin administration as part of their treatment regimen). Inclusion of type 2 diabetes patients who do not use insulin will be an additional burden to their self-management, since such patients will have to regularly monitor their blood glucose in order to use the blood glucose tracking feature of the app. Studies have reported reduced acceptability and engagement with health technologies that are perceived by patients to be burdensome.50
Type 1 and 2 diabetes patients with major diabetes complications (such as kidney failure and lower limb amputation), pregnancy, and psychiatric co-morbidity will not be eligible to participate in the study. This exclusion is based on the fact that this set of medical conditions requires close medical monitoring and unique self-management needs, which the intervention is not likely to address.
Recruitment
A trial nurse will screen for eligible potential participants. The nurse will work in collaboration with the booking officer to obtain patients’ mailing addresses. A detailed information sheet explaining the goal and conduct of the study will be mailed to eligible participants 2 weeks ahead of their clinic appointments. This is to give them prior information about the study and allow eligible participants ample time to make a decision on whether they wish to participate or not. The email address and phone number of the principal investigator will also be provided in the event that prospective participants require some clarification about the study. Initial contact will be on the clinic day when the principal investigator describes the study and offers participants time to ask any study-related questions. Participants interested in the study will then be presented with the informed consent form to sign.
Allocation, blinding, and orientation
The principal investigator will assign enrolled participants study numbers to aid de-identification, and the numbers will be used for random allocation into one of the groups using optimal multivariate matching.51 Participants will be matched based on HbA1c, type of diabetes, and duration of diagnosis. Those in the control group will continue with their standard care, while those in the experimental group will receive the intervention in addition to their regular care. Blinding of participants is not possible due to the nature of intervention involved. However, initial contact and orientation (on app use) for intervention participants will take place on aone-on-one basis. Therefore, participants may not be aware of others in similar or different groups. Technical support for app use will be offered to those in the intervention group by giving them a phone call at least twice during the first 2 months of the study.
Intervention
Intervention will entail the use of the newly-developed mobile phone app, which focuses on self-management education and support, for 12 months.
Mobile application
The mobile app will contain essential diabetes management features for tracking blood glucose, physical exercise, diet, in addition to other preferred features that may be identified from the mixed methods study. Furthermore, the app will have personalized educational features that provide computed algorithm feedback messages in response to reported blood glucose measurements. Several separate feedback messages will be developed and input into the app to be controlled by a decision-based system. Rules will be set, stipulating requirements for messages to be delivered to patients. These requirements will be specific to the indicated type of diabetes, value of blood glucose (whether within or beyond the standard recommended range), and the period of blood glucose measurement (either fasting or 2 hours post-prandial). In addition, regular randomization to guard against unnecessary repetition of the same message will be integrated into the decision-based system. These messages are evidence-based, motivational, health promotional, and behavioral skills information aimed at supporting self-management practices. For example, where a type 1 DM participant logged a fasting BG of 6 mmol/L, feedback message may include “Excellent: BG appears within recommended target range, continue your medication as prescribed“, or “Excellent … keeping BG levels within target range reduces the risk of complications”. In situations where the inputted BG value is in the range of emergency hyperglycemia (≥14 mmol/L) consistently, an immediate contact with the patient’s health provider will be recommended. The intervention group will be instructed to log their blood glucose measurements into the app twice weekly at a minimum. Data logged into the app will be automatically transferred to a secured, password protected cloud storage accessible by the principal investigator only. Participants will be informed about the automatic transfer of the logged data into a cloud storage and consent will be obtained to access the information.
Given that the app will be used by both type 1 and type 2 diabetes patients who have different care guidelines with regards to recommended blood glucose values, it is important to ensure that the app is suitable for both groups of patients. Furthermore, although recommendations for diet, exercise, and associated education are different for both groups of patients, they have the common characteristic of developing hypoglycemia when exercise, food, and insulin are not balanced. Hence, we aim to provide educational messages in the app that include information on strategies to balance exercise (especially long duration) and diet with blood glucose levels and insulin.
Self-management education
Through the mobile app, general messages will be provided, in addition to personalized automated messages. Messages will reinforce information on the seven essential diabetes self-management behaviors that predict good outcomes, namely: lifestyle modifications (healthy eating and improved physical activity), monitoring of blood sugar, complying with medications, good problem-solving skills, healthy coping skills, and risk-reduction behaviors (such as smoking cessation and reduction in alcohol intake).7 Essentially, there will be emphasis on the indicated common educational needs for self-management deduced from the results of the mixed methods study. Educational information will be prepared by MDA, who is a diabetes educator, based on guidance and advice from UM, who is an Endocrinologist. The frequency of delivery of general education via the app will be twice a week. Conciseness and simple formatting of messages will be ensured so that the provided education can benefit all participants, regardless of literacy level.
Standard care
Participants in the control group will receive standard care only. Standard care for diabetes in Australian Hospitals comprises consultation with a physician diabetes specialist at 3–4 month intervals. During this period, depending on individual healthcare needs, patients will be managed in a collaborative care arrangement between the specialist and other allied health professionals such as diabetes educators. The key areas of education include, but are not limited to, healthy eating, physical activity, reducing the risk of complications, monitoring blood glucose, and using results to improve diabetes management.52
Data collection at different time points
Pre-intervention
After initial contact and enrolment, patients will complete a questionnaire about their baseline information on socio-demographics, medical, and family history of disease. The questionnaire was developed for the study based on a review of published literature.
Additionally, information on diabetes management knowledge, medication adherence, perceived ability for self-management, and quality-of-life will be elucidated using self-administered validated questionnaires. Please see Table 1 for an outline of the validated questionnaires.
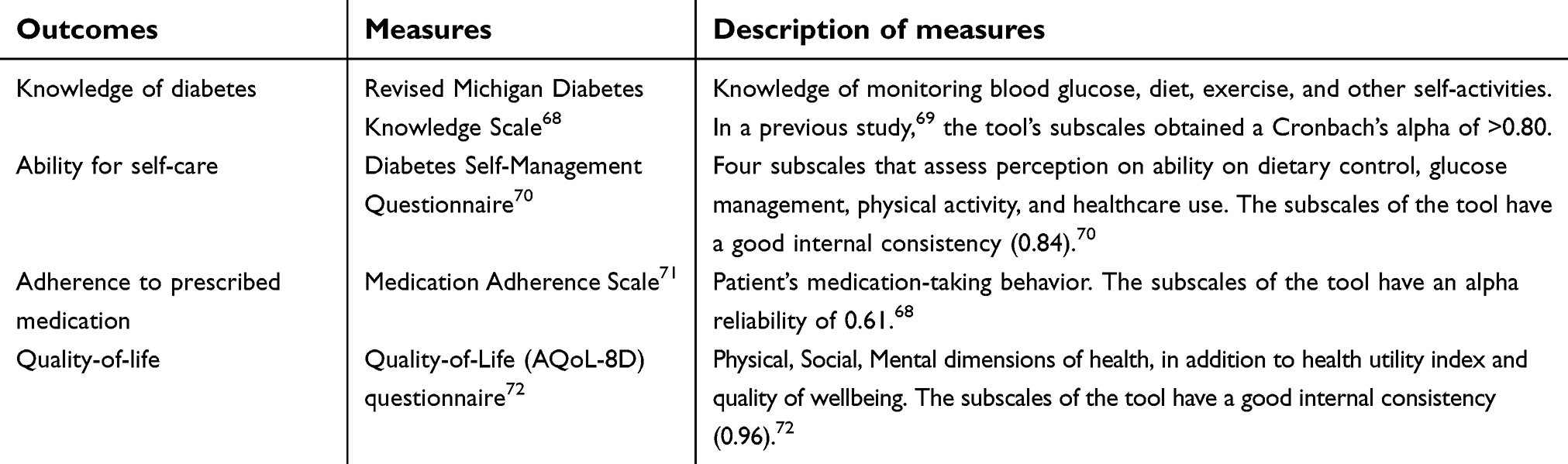 | Table 1 Measures of secondary outcomes |
Baseline, 4, 8, and 12 months during intervention
The primary outcomes of interest are the clinical data which will be assessed at four different time points (intake, 4, 8, and 12 months). Relevant clinical outcomes include HbA1c, BP, lipids, ACR, weight, height, waist circumference, events of emergency hypoglycemia, and hyperglycemia. These parameters are requested by the patient’s doctor as part of routine care, hence there will be retrospective collection of these measures from each participant’s hospital record at each data collection time point. At the time of enrolment, patients will be asked to provide consent to retrieve these data from their clinical records.
Post-intervention
At the end of 12 months, intervention will stop and all participants will be invited to a final visit to enable them to fill out the post-intervention questionnaires to assess the secondary outcomes. These will be the same validated questionnaires administered at the start of the pre-intervention study.
Additionally, at this final visit, a questionnaire developed for the study will be used to assess participants’ level of acceptability of the app. The questionnaire will consist of items pertaining to satisfaction, usability, functionality, and willingness to use the app in the future and/or recommend to other patients.
Furthermore, data on direct and indirect healthcare costs will be collated to determine the cost-effectiveness of the intervention. Direct costs of implementing the intervention are costs associated with personnel, operating, maintenance, utilities, and capital. Hospital visit costs due to emergency complications (if any) as well as predicted long-term healthcare costs incurred in relation to chronic complication development (if any), will also be determined. Indirect health costs will entail transportation to clinic appointments due to emergency complications and loss of productivity from being absent from work or usual activity due to such complications. Cost of standard care will also be factored in.
App utilization will be tracked directly from the number of data logged into the app and extracted from cloud storage at the end of the study.
Sample size calculation
A priori statistical power analysis was computed using G-power.39 Estimation of sample size was done using expected change in HbA1c as the primary outcome. A 0.4% reduction in HbA1c level in the intervention group was expected with a statistical criterion level of 0.05 (two-tailed). This analysis also indicated that 68 participants per control and intervention group will be required to achieve 80% power for detecting differences in the outcomes of interest between both groups. The total sample size was increased to 150 to allow for drop out, which is peculiar to longitudinal studies.53 The chosen effect size, significance level, and statistical power were derived from inspecting previous similar trials.54,55
Statistical analysis
Analysis of this RCT will be performed by intent-to-treat (ITT) principle, including all randomized participants.56
Primary outcome variables (clinical parameters) will be analyzed as continuous variables and dichotomized. Randomization is expected to produce similar groups; therefore, baseline demographics and clinical variables will be compared using two sample t-tests for continuous variables and chi-square test or Analysis of Variance (ANOVA) for categorical variables. Furthermore, adjusted group comparisons using multilinear and logistic regressions will be carried out. Covariates will include clinically relevant baseline characteristics such as age, duration of diagnosis, HbA1c, and co-morbidities.
To determine the effect of the intervention on clinical parameters, Bonferroni pair-wise comparison tests for multivariate analysis and/or mixed effects regression modeling will be used to compare mean changes between the two groups. The extent to which improvement in clinical parameters mediate reduction in complication development will be assessed by fitting two linear/logistic regression models, one including only group characteristics (such as age, sex, baseline HbA1c level) and the other incorporating both group effect and the intervention as covariates. The degree to which group characteristics are abated after adding the intervention into the model provides an indication of the mediating effect.57
Secondary outcomes will be reported using descriptive statistics. Any statistically significant difference in these outcomes (pre- and post-intervention) between the intervention and control groups will be assessed using appropriate parametric and non-parametric statistics.
Economic evaluation will entail the cost-effectiveness and cost of implementing the intervention. Cost-effectiveness will be expressed as an Incremental Cost-Effectiveness Ratio (ICER),58 while direct and indirect costs will be computed to determine the cost consequences of the intervention.
Data on app utilization and acceptability will be analyzed descriptively. All statistical analyses for this phase of the study will be performed using SPSS software and a P-value<0.05 will be considered to be statistically significant.
Study approval and consent to participate
The Phase 1 study procedure received approval from the James Cook University Human Research Ethics Committee (Permit number H707). The Phase 2 (RCT) protocol was approved by the Human Research Ethics Committee of the Townsville Hospital and Health Service (Permit Number HREC/17/QTHS/148). Electronic and audio consents will be obtained from participants in phase 1 as deemed appropriate. All participants for phase 2 will be required to provide written informed consent. The trial has been registered on Australian New Zealand Clinical Trials Registry, ACTRN12618000065291.
Data storage/confidentiality
All data from this study will be stored in accordance with the Australian Code for the Responsible Conduct of Research.59 All data will be treated as confidential. Any data stored on an electronic device will be de-identified. All completed questionnaires and consent forms will be securely stored in a locked file cabinet. Only members of the research team will have access to the final data set.
Dissemination of research findings
The knowledge gained from this study will be disseminated through publications in peer reviewed journals and presentations at academic conferences.
Time frame for the study
At the time of submission of this manuscript, data collection for Phase 1 (mixed methods study) had been completed with 217 and 16 participants in the survey and telephone interviews, respectively. The results of the analysis will inform the content and design of the intervention app. The app will be developed with the assistance of software developers who will work in collaboration with the authors of this study. As at the submission of this work for publication, several meetings have been held between the authors and the software developers on the app development. It is anticipated that the mobile app design, usability, and pilot testing will be completed in 2019, and the randomized control trial of its efficacy will commence in 2020.
Discussion
The strength of this research lies in the use of mixed methods study design to seek information from a multinational audience (Phase1) in order to address knowledge gaps in patients’ preferences for apps features as well as their self-management skills and efficacy, and perceptions on how to foster better engagement with diabetes self-management mobile apps. This approach is hypothesized to increase the opportunity for maximizing patients’ engagement with the app because it emphasizes shared decision-making and ensures input from end-users.60,61
The objective of the international study is to identify global patient preferences for essential features in diabetes apps, common gaps in skills and self-efficacy for diabetes management, and recommendations on motivators to foster long-term engagement with apps. We believe these objectives will be relevant in any app development because, regardless of location/setting, recommended standard of care and therapeutic management of diabetes is regulated. Nevertheless, in the event that results from phase 1 reveal the need for country-specific requirements for app features and functionalities, such information will be utilized in the development of an app that is adequate and suitable for use in an Australian context. The intervention will be designed to use mobile app technology and provide self-management and educational support to Australians who have insulin-requiring type 1 or type 2 diabetes.
Mobile apps have the potential to motivate and support healthy lifestyle decisions in patients with chronic diseases, such as diabetes.62–64Additionally, mobile apps can be used to provide regular diabetes self-management information.65,66 Availability of the support and education on an ongoing basis will enable improved management and reduced morbidity and mortality.9,67 Results from these studies will provide the much-needed information on patients’ self-management education needs, their preferred app features, and opinions on how to foster engagement with diabetes apps in order to improve health outcomes for diabetes patients. The benefits expected from the studies include:
- Identification of the needs of patients with regards to self-management skills and efficacy, preferred features in apps, and opinions on better engagement with a mobile app for diabetes management;
- Promotion of diabetes self-management;
- Improvement of clinical outcomes, knowledge, self-care abilities, medication adherence, and quality-of-life;
- Reduction of the huge burden of diabetes on the healthcare system; and
- Meeting one of the goals of the Australian National Diabetes Strategy 2016–2020 to reduce the occurrence of diabetes-related complications and improve the quality-of-life among people with diabetes.
Limitations of this project include the use of self-reported measures in Phase 1 and secondary outcomes for Phase 2. Compared to objective measures, self-reported measures are liable to recall bias and social desirability. Nevertheless, self-reported measures are brief and less expensive to administer. Additionally, we aim to use validated tools to strengthen the study. Another limitation is that, because the RCT is powered to examine the effectiveness of the mobile app on HbA1c, therefore, analysis examining the effect of the secondary outcomes may be underpowered. However, this does not deter the results of the outcomes from being informative.
Overall, we anticipate that this research project will be able to meet priority patient needs, have connective links to health education, and foster better health outcomes and quality-of-life for people with diabetes.
Acknowledgments
This study is part of the requirements for a PhD (Health) research degree at the James Cook University, Queensland, Australia by the corresponding author (MDA) who is supported by the Australian Government International Research Training Program Scholarship, James Cook University, Queensland, Australia. The funding body is not involved in the study design, collection, analysis, or interpretation of data.
Author contributions
MDA is the principal investigator and wrote the original draft of the manuscript. The study was designed by all authors (BMA, UHM, AEOMA, MDA) and they all contributed to the study plan and manuscript development. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Clark M. Diabetes self-management education: a review of published studies. Prim Care Diabetes. 2008;2(3):113–120. doi:10.1016/j.pcd.2008.04.004
2. Renders CM, Valk GD, Griffin SJ, Wagner EH, van JT E, Assendelft WJJ. Interventions to improve the management of diabetes in primary care, outpatient, and community settings: a systematic review. Diabetes Care. 2001;24(10):1821–1833.
3. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American association of diabetes educators, and the academy of nutrition and dietetics. J Acad Nutr Diet. 2015;115(8):1323–1334. doi:10.1016/j.jand.2015.05.012
4.
5. Colagiuri R, Girgis S, Eigenmann C, Gomez M, Griffiths R. National Evidenced Based Guideline for Patient Education in Type 2 Diabetes. Canberra:Diabetes Australia and the NHMRC;2009. Available from::
6. Coyle ME, Francis K, Chapman Y. Self-management activities in diabetes care: a systematic review. Aust Health Rev. 2013;37(4):513–522. doi:10.1071/AH13060
7. Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(1):14. doi:10.1186/2251-6581-12-14
8. Duncan I, Birkmeyer C, Coughlin S, Qijuan L, Sheer D, Boren S. Assessing the value of diabetes education. Diabetes Educ. 2009;35(5):752–760. doi:10.1177/0145721709343609
9. Norris SL, Lau J, Smith SJ, Schmid C, Engelgau MM. Self-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care. 2002;25(7):1159–1171.
10. Steinsbekk A, Rygg L, Lisulo M, Rise MB, Fretheim A. Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Serv Res. 2012;12(1):213. doi:10.1186/1472-6963-12-213
11. Peyrot M, Rubin RR, Funnell MM, Siminerio LM. Access to diabetes self-management education. Diabetes Educ. 2009;35(2):246–263. doi:10.1177/0145721708329546
12. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. 2009;32(Suppl 1):S87–94. doi:10.2337/dc09-S087
13. Nagelkerk J, Reick K, Meengs L. Perceived barriers and effective strategies to diabetes self‐management. J Adv Nurs. 2006;54(2):151–158. doi:10.1111/j.1365-2648.2006.03799.x
14. Clement S. Diabetes self-management education. Diabetes Care. 1995;18(8):1204–1214.
15. Mickan S, Tilson JK, Atherton H, Roberts NW, Heneghan C. Evidence of effectiveness of health care professionals using handheld computers: a scoping review of systematic reviews. J Med Internet Res. 2013;15(10). doi:10.2196/jmir.2530
16. Fogg B. Persuasive Technology: Using Computers to Change What We Think and Do.
17. Matthews J, Win KT, Oinas-Kukkonen H, Freeman M. Persuasive technology in mobile applications promoting physical activity: a systematic review. J Med Syst. 2016;40(3):72. doi:10.1007/s10916-015-0425-x
18. Goyal S, Cafazzo JA. Mobile phone health apps for diabetes management: current evidence and future developments. Qjm. 2013;106(12):1067–1069. doi:10.1093/qjmed/hct203
19. Chomutare T, Fernadez-Luque L, Arsand E, Hartvigsen G. Features of mobile diabetes applications: review of the literature and analysis of current applications compared against evidence-based guidelines. J Med Internet Res. 2011;13(3). doi:10.2196/jmir.1874
20. Martínez-Pérez B, De La Torre-Díez I, López-Coronado M. Mobile health applications for the most prevalent conditions by the World Health Organization: review and analysis. J Med Internet Res. 2013;15(6). doi:10.2196/jmir.2600
21. Boren SA, Leo GD, Chanetsa F, Donaldson J, Krishna S, Balas EA. Evaluation of a diabetes education call center intervention. Telemed J E Health. 2006;12(4):457–465. doi:10.1089/tmj.2006.12.457
22. Déglise C, Suggs LS, Odermatt P. Short message service (SMS) applications for disease prevention in developing countries. J Med Internet Res. 2012;14(1). doi:10.2196/jmir.1823
23. Vervloet M, Linn AJ, van Weert JCM, de Bakke DH, Bouvy ML, van Dijk L. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. J Am Med Inform Assoc. 2012;19(5):696–704. doi:10.1136/amiajnl-2011-000748
24. Bonoto BC, de Araujo VE, Godoi IP, et al. Efficacy of mobile apps to support the care of patients with diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. JMIR Mhealth Uhealth. 2017;5(3). doi:10.2196/mhealth.6309
25. Catherine HY, Parsons JA, Mamdani M, et al. A web-based intervention to support self-management of patients with type 2 diabetes mellitus: effect on self-efficacy, self-care and diabetes distress. BMC Med Inform Decis Mak. 2014;14:117. doi:10.1186/s12911-014-0117-3
26. Steele R, Amanda LO, Secombe C, Wong YK. Elderly persons’ perception and acceptance of using wireless sensor networks to assist healthcare. Int J Med Inform. 2009;78(12):788–801. doi:10.1016/j.ijmedinf.2009.08.001
27. Istepanian RS, Zitouni K, Harry D, et al. Evaluation of a mobile phone telemonitoring system for glycaemic control in patients with diabetes. J Telemed Telecare. 2009;15(3):125–128. doi:10.1258/jtt.2009.003006
28. Holmen H, Torbornsen A, Wahl AK, et al. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: one-year results from the Norwegian randomized controlled trial RENEWING HEALTH. JMIR Mhealth Uhealth. 2014;2:4. doi:10.2196/mhealth.3882
29. Kirwan M, Vandelanotte C, Fenning A, Duncan MJ. Diabetes self-management smartphone application for adults with type 1 diabetes: randomized controlled trial. J Med Internet Res. 2013;15:11. doi:10.2196/jmir.2588
30. Demidowich AP, Lu K, Tamier R, Bloomgarden Z. An evaluation of diabetes self-management applications for Android smartphones. J Telemed Telecare. 2012;18(4):235–238. doi:10.1258/jtt.2012.111002
31. Mallenius S, Rossi M, Tuunainen VK. Factors affecting the adoption and use of mobile devices and services by elderly people–results from a pilot study. 6th Annu Global Mobility Roundtable. 2007;31:12. Available from:
32. Holzinger A, Searle G, Nischelwitzer A On some aspects of improving mobile applications for the elderly. Universal access in human-computer interaction. Coping with diversity.
33. Jahns R Today’s diabetes apps are far away from meeting the seven best practice standard. research2guidance; 2014. Available from:
34. Holmen H, Whal AK, Smastuen MC, Ribu L. Tailored communication within mobile apps for diabetes self-management: A systematic review. J Med Internet Res. 2017;19(6). doi:10.2196/jmir.7045
35. Izahar S, Lean Q, AbdulHameed M, et al. Content analysis of mobile health applications on diabetes mellitus. Fron Endocrinol. 2017;8:318. doi:10.3389/fendo.2017.00318
36. El-Gayar O, Timsina P, Nawar N,Eid W.Mobile applications for diabetes self-management: status and potential. J Diabetes Sci Technol. 2013;7(1):247–262. doi:10.1177/193229681300700130
37.
38. Wisdom J, Creswell J. Mixed Methods: Integrating Quantitative and Qualitative Data Collection and Analysis while Studying Patient-Centered Medical Home Models. Rockville, MD: Agency for Healthcare Research and Quality; 2013.
39. Faul F, Erdgfelder E, Lang A, Buchner AG. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191.
40. Mbuagbaw L, Aronson R, Walker A, Brown RE, Orzech N. The LMC Skills, Confidence & Preparedness Index (SCPI): development and evaluation of a novel tool for assessing self-management in patients with diabetes. Health Qual Life Outcomes. 2017;15(1):27. doi:10.1186/s12955-017-0606-z
41. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
42. Pallant J. SPSS Survival Manual: A Step by Tep Guide to Data Analysis Using IBM SPSS.
43. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
44. Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M. Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth. 2015;3(1):e27. doi:10.2196/mhealth.3949
45. Sibbald B, Roland M. Understanding controlled trials. Why are randomised controlled trials important? BMJ: Br Med J. 1998;316(7126):201. doi:10.1136/bmj.316.7126.201
46. Crowther CA, Hiller JE, Moss JR, McPhee AJ, Jeffries WS, Robinson JS. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med. 2005;352(24):2477–2486. doi:10.1056/NEJMoa042973
47.
48.
49.
50. Stiles-Shields C., Montague E, Lattie EG, Kwasny MJ, Mohr DC. What might get in the way: barriers to the use of apps for depression. Digit Health. 2017;3:2055207617713827. doi:10.1177/2055207617729937
51. Greevy R, Lu B, Silber JH, Rosenbaum P. Optimal multivariate matching before randomization. Biostatistics. 2004;5(2):263–275. doi:10.1093/biostatistics/5.2.263
52. Haas L, Maryniuk M, Beck J, et al. National standards for diabetes self-management education and support. Diabetes Educ. 2012;38(5):619–629. doi:10.1177/0145721712455997
53. Friedman L, Furberg C, DeMets D. Fundamentals of Clinical Trials.
54. Rossi MC, Nicolucci A, Lucisano G, et al. Impact of the “Diabetes Interactive Diary” telemedicine system on metabolic control, risk of hypoglycemia, and quality of life: a randomized clinical trial in type 1 diabetes. Diabetes Technol Ther. 2013;15(8):670–679. doi:10.1089/dia.2013.0021
55. Ribu L, Olmen H, Torbjornsen A, et al. Low-intensity self-management intervention for persons with type 2 diabetes using a mobile phone-based diabetes diary, with and without health counseling and motivational interviewing: protocol for a randomized controlled trial. JMIR Res Protoc. 2013;2(2). doi:10.2196/resprot.2768
56. McCoy CE. Understanding the intention-to-treat principle in randomized controlled trials. West J Emerg Med. 2017;18(6):1075. doi:10.5811/westjem.2016.10.32233
57. Lin D, Fleming T, De Gruttola V. Estimating the proportion of treatment effect explained by a surrogate marker. Stat Med. 1997;16(13):1515–1527.
58. Drummond MF, Sculpher MJ, Claxto K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes.
59.
60. Årsand E, Demiris G. User-centered methods for designing patient-centric self-help tools. Inform Health Soc Care. 2008;33(3):158–169. doi:10.1080/17538150802457562
61. McCurdie T, Taneva S, Casselman M, Yeung M, McDaniel C, Ho W, Cafazzo J. mHealth consumer apps: the case for user-centered design. Biomed Instrum Technol. 2012;46(s2):49–56. doi:10.2345/0899-8205-46.1.49
62. Whitehead L, Seaton P. The effectiveness of self-management mobile phone and tablet apps in long-term condition management: a systematic review. J Med Internet Res. 2016;18(5). doi:10.2196/jmir.4883
63. Goyal S, Morita P, Lewis GF, Yu C, Seto E, Cefazzo JA. The systematic design of a behavioural mobile health application for the self-management of type 2 diabetes. Can J Diabetes. 2016;40(1):95–104. doi:10.1016/j.jcjd.2015.06.007
64. Torbjørnsen A, Jenum AK, Smastuen MC, et al. A low-intensity mobile health intervention with and without health counseling for persons with type 2 diabetes, part 1: baseline and short-term results from a randomized controlled trial in the Norwegian part of RENEWING HEALTH. JMIR Mhealth Uhealth. 2014;2(4). doi:10.2196/mhealth.3535
65. Pereira K, Beth P, Constance J, Allison V. Internet delivered diabetes self-management education: a review. Diabetes Technol Ther. 2015;17(1):55–63. doi:10.1089/dia.2014.0155
66. Greenwood DA, Gee PM, Fatkin KJ, Peeples M. A systematic review of reviews evaluating technology-enabled diabetes self-management education and support. J Diabetes Sci Technol. 2017;11(5):1015–1027. doi:10.1177/1932296817713506
67. Kitsiou S, Pare G, Jaana M, Gerber B. Effectiveness of mHealth interventions for patients with diabetes: an overview of systematic reviews. PLoS One. 2017;12(3):e0173160. doi:10.1371/journal.pone.0173160
68. Collins G, Mughal S, Barnett AH, Fitzgerald J, Lioyd CE. Modification and validation of the revised diabetes knowledge scale. Diabet Med. 2011;28(3):306–310. doi:10.1111/j.1464-5491.2010.03190.x
69. Al-Qazaz H, Hassali MA, Shafie AA, Sulaiman SA, Sundram S. The 14-item michigan diabetes knowledge test: translation and validation study of the Malaysian version. Practical Diabetes Int. 2010;27(6):238–241a. doi:10.1002/pdi.1495
70. Schmitt A, Gahr A, Hermanns N, Kulzer B, Huber J, Haak T. The Diabetes Self-Management Questionnaire (DSMQ): development and evaluation of an instrument to assess diabetes self-care activities associated with glycaemic control. Health Qual Life Outcome. 2013;11(1):138. doi:10.1186/1477-7525-11-138
71. Culig J, Leppée M. from morisky to hill-bone; self-reports scales for measuring adherence to medication. Coll Antropol. 2014;38(1):55–62.
72. Richardson J, Iezzi A, Khan MA et al. Validity and reliability of the Assessment of Quality of Life (AQoL-8D) multi-attribute utility instrument. Patient. 2014;7(1):85–96. doi:10.1007/s40271-013-0036-x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.