Back to Journals » International Journal of Women's Health » Volume 17
Mitigating Risk of Premature Ovarian Insufficiency Using Adjunct Chinese Herbal Medicines: A Nested Patient-Control Study in Female Cancer Patients with Chemotherapy
Authors Tseng TN, Liao HH ![]() , Livneh H
, Livneh H ![]() , Lu MC
, Lu MC ![]() , Li SC, Tsai TY
, Li SC, Tsai TY ![]()
Received 6 June 2025
Accepted for publication 23 October 2025
Published 16 December 2025 Volume 2025:17 Pages 5521—5531
DOI https://doi.org/10.2147/IJWH.S541702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Tzu-Ning Tseng,1,* Hou-Hsun Liao,1– 3,* Hanoch Livneh,4,* Ming-Chi Lu,5,6 Szu-Chin Li,6,7 Tzung-Yi Tsai8,9
1Department of Chinese Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 2Department of Biochemical Science and Technology, National Chiayi University, Chiayi, 60004, Taiwan; 3Department of Nursing, Tzu Chi University of Science and Technology, Hualien, Taiwan; 4Rehabilitation Counseling Program, Portland State University, Portland, OR, USA; 5Division of Allergy, Immunology and Rheumatology, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 6School of Medicine, Tzu Chi University, Hualien, Taiwan; 7Division of Hematology and Oncology, Department of Internal Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 8Department of Environmental and Occupational Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 9Department of Medical Research, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan
*These authors contributed equally to this work
Correspondence: Szu-Chin Li, Email [email protected] Tzung-Yi Tsai, Email [email protected]
Purpose: Premature ovarian insufficiency (POI) is a common late effect of chemotherapy among survivors of adolescent and young-adult cancer (AYAC). Given on the widespread use of Chinese herbal medicine (CHM) in restoring individual health, we performed a cohort-based nested patient-control study with the aim of exploring the effect of blending CHM into routine care on the reduction of chemotherapy-induced POIrisk among females with AYAC.
Methods: Females aged 20– 39 years with a newly-diagnosed AYAC and being free of POI between 2002 and 2010 were recruited from a population-based claims data. From these enrollees, we identified those with POI occurring after AYAC onset by the end of 2013 (n = 1040). Corresponding controls were randomly selected from the remaining subjects using a pair-matched approach. We then adopted conditional logistic regression to clarify the association between CHM use and POI risk, shown as 95% confidence intervals (CI) and adjusted odds ratios (AOR).
Results: Patients who revived CHM in addition to standard treatment towards AYAC experienced a substantial lower risk of POI than did those who did not use CHM (AOR, 0.16; 95% CI, 0.13– 0.19). Importantly, initiating CHM treatment within the first three years after AYAC onset had the greatest benefit, with a lower risk of POI by 92%.
Conclusion: The present study revealed that embedding CHM into routine care of AYAC acted to prevent subsequent POI incident, implying that interdisciplinary collaboration and timely treatment planning should be emphasized to reduce the chance of POI onset.
Keywords: adolescent and young-adult cancer, premature ovarian insufficiency, Chinese herbal medicines, nested patient-control study
Introduction
Adolescent and young adult cancer (AYAC) refers to new-onset cancers in people aged 15–39 years.1 With the large increase in highly-specialized diagnostic and therapeutic approaches over past decades, the five-year survival rate of AYAC has surpassed 80%.2 Nevertheless, the extended life-span does not necessarily indicate that patients have successfully adjusted to or coped with this condition; on the other hand, some common side effects resulting from treatment-related toxicity may have serious physical and psychological consequences on patients and their families.3 Factually, the chronicity impact of AYAC in females has captured more attention than in males, involving breast cancer, thyroid cancer, melanoma, and cervical cancer.4 Worse yet, the effects of cancer-related therapies on endocrine and reproductive organ function often persist long after diagnosis and treatment, thus exerting a heavy toll on females diagnosed with AYAC.
Presently, premature ovarian insufficiency (POI) has been noticed as a relevant disease due to cancer-related therapies toexacerbate ovarian function.5 This is an imperative issue for females with AYAC since they may encounter disturbance in fertility later. POI is defined as the loss or decline of normal ovarian function before the age of 40, characterized by irregular or absent menstruation, hypoestrogenism, and elevated gonadotropin levels.5 A population-based study revealed that AYAC survivors were nearly three times more likely to suffer from POI than the cancer -free counterparts.6 Upon the onset of POI, the affected patients may face higher risks of cardiovascular disease, osteoporosis, cognitive dysfunction, and premature mortality later in life.7–9 A commonly used approach to treat ovarian dysfunction in females undergoing cytotoxic chemotherapy so far is to prescribe gonadotropin-releasing hormone agonist (GnRHa).10 Both the European Society of Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) recommend prescribing GnRHa to mitigate the risk of ovarian insufficiency.11 Despite the potential benefits of GnRHa, cancer females who received treatment-related gonadotoxicity still tend to sustain POI onset.12 On top of that, mounting evidence shows that its use had deleterious impact on bone and cardiovascular health.13,14 As a consequence, it is of great importance to broaden research and clinical horizons and explore potential adjunctive treatment methods against the onset of POI in AYAC females.
Known for having minor side effect, Chinese Herbal Medicine (CHM) has been extensively used for the therapeutic and prophylactic management of human disease, including POI.15,16 Evidence suggests that CHM could exert its advantage on POI prevention through multiple signaling pathways, like caspase-mediated pathways and Nrf2 signaling pathway.17 Plant-derived compounds have been further proven to possess immunomodulatory and anti-inflammatory actions that significantly inhibit release and function of inflammatory parameters,18 which is known to severely affect ovarian function.19 Accumulating evidence has documented the beneficial effects of CHM so far, but its impact on POI prevention in females withAYAC has yet to be confirmed. This study is, therefore, geared to clarify the association between CHM use and risk of chemotherapy-induced POI among AYAC females.
Methods
Data Source
The target population for this nested patient-control study was obtained from a nationwide claims database in Taiwan that is maintained by the Bureau of National Health Insurance (NHI).20 Through random sampling of all beneficiaries under the NHI program by age and sex, this database provides researchers an opportunity to undertake population-based studies and epidemiological investigations. The database includes encrypted beneficiary information on sex, birth date, and physician billing claims for inpatient and outpatient visits covered by the NHI, allowing for the identification of all medical consultations and diagnoses. Relevant medical diagnoses are coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Since the data were anonymized before public release, individual identifying information cannot be obtained from the database. This study was conducted in accordance with the guidelines of the Helsinki Declaration. As all data were anonymized shown in this nationwide claims database, the Institutional Review Board of Buddhist Dalin Tzu Chi Hospital confirmed that this study was exempt from full review along with the need for informed consent in this study (No. B10004021-3).
Establishment of Underlying Cohort
The initial cohort included females with AYAC who were 20–39 years of age and had undergone chemotherapy for AYAC between 2002 and 2010 (ICD-9-CM code: 140–176, 185–208). To diminish misclassification bias, the lists of AYAC were further linked to the catastrophic illness card (CIR). This is because all citizens of Taiwan with autoimmune illnesses or malignancies can apply for the CIR certification to minimize the expenses of healthcare received. Prior to acquiring CIR, the experts employed in NHI would deliberately review the records of treatments received. These checks and processes are believed to ensure accurate coding to minimize ascertainment bias. Date of approval for the CIR card for AYAC was then regarded as the cohort entry date. To adhere to established research procedures, we excluded subjects who had been followed for less than one year and those with incomplete data (n = 504). Patients who underwent ovarian or uterine surgery also were deleted. Women for whose first AYAC diagnosis occurring after POI onset were removed to ensure the appropriate temporal sequence (n = 1115). The remaining patients were followed up until the earliest diagnosis of POI, death, or the end of 2013.
Patient and Control Groups
The primary outcome was the onsetof POI that occurred from 2003 to 2013. Participants were defined as having POI if they ever visited the outpatient clinic twice in one year or were hospitalized once during the study timeframe due to this condition (ICD-9-CM codes 627).21 The first medical visit for POI was viewed as the index date. Each of the POI patients was randomly matched to one control with no POI diagnosis in accordance with age, socidemographic data and comorbidities (Figure 1). An index date was assigned to each of the controls corresponding to the POI diagnosis date, which ensured the same observational frame for all enrollees.
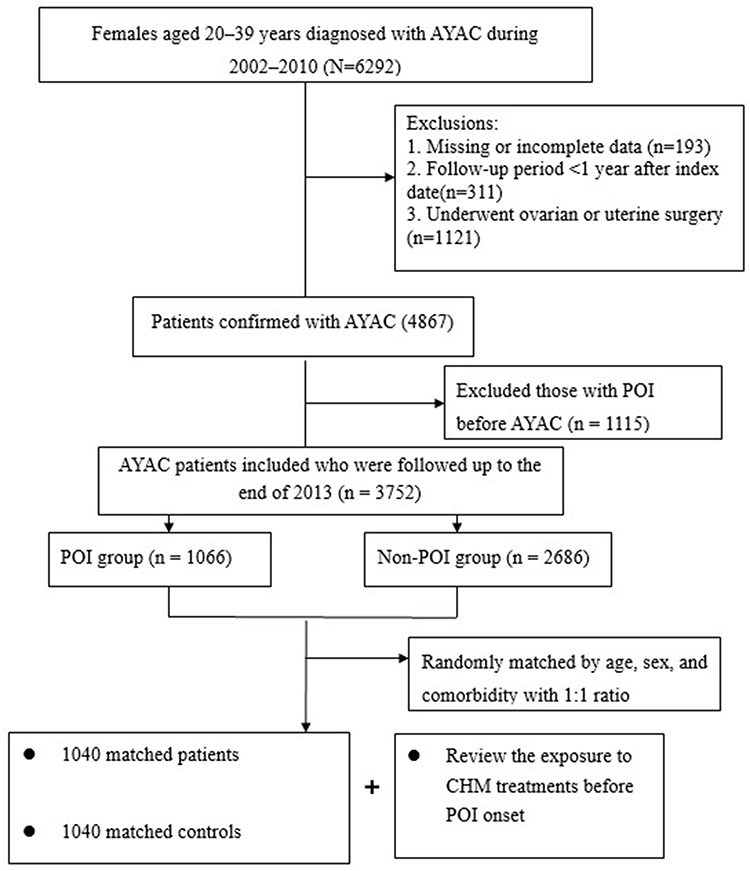 |
Figure 1 Flowchart of subject selection. |
Explication of CHM Use
The identification of CHM treatment is based on medical records indicating that visits to Chinese medicine practitioners that occurred from cohort entry date to the index date. In accordance with former method,22 the participants were then converted into CHM users and non-CHM users based on if they ever received relevant CHM treatments for AYAC or its symptomsby intervals of 30 days, made by CHM physicians. Exposure to CHM use wasfurther split into two subgroups according to individual age at baseline. This subgroup analysis allowed us to appraise if the association between adjunctive CHM treatment and subsequent POI occurred across diverse age groups.
Covariates Definition
Covariates in the statistical model included sex, age, previous medical comorbidities, individual monthly salary, and urbanization level of residence. Health insurance premiums, used as a substitute for monthly salary, wereseparated into three quartile values, where level one stood for the lowest monthly salary group. As to the enrollees’ residential district, it was subdivided into three groups in accordance with the established method that took into account several factors, like population density per square kilometer, the proportion of individuals with a bachelor’s degree or higher, the ratio of residents aged 65 years or older, the percentage of the labor force employed in agriculture, and the number of clinicians per 100,000 inhabitants.23 This indicator enables researchers to consider the enrollee’s healthcare accessibility. Medical comorbidities were defined as conditions that occurred at least once in inpatient, or twice in outpatient, claims one year prior to cohort entry. The Charlson–Deyo comorbidity index (CCI), a method that ranks the number and severity of 17 pre-defined comorbid conditions by assigning a weighted scale of 1 to 6, was adopted to categorize the baseline comorbidity burden for each patient.24
Data Analysis
Statistical analyses were conducted using SAS for Windows, Version 9.4. Descriptive statistics, including the mean, standard deviation (SD), frequency, and percentages, were used to assess the baseline patients’ characteristics. Baseline data were compared for treated and control groups using Student’s t-test test for continuous variables or chi-square test for categorical variables, as appropriate. Conditional logistic regression was used to estimate odds ratios (OR) with 95% confidence intervals (CI) for the relationship between CHM use and the subsequent incidence of POI. The adjusted OR (AOR) was also used to determine whether the adjustments shown in Table 1 would affect the results of CHM treatment. In all statistical tests, p ≤ 0.05 was considered significant.
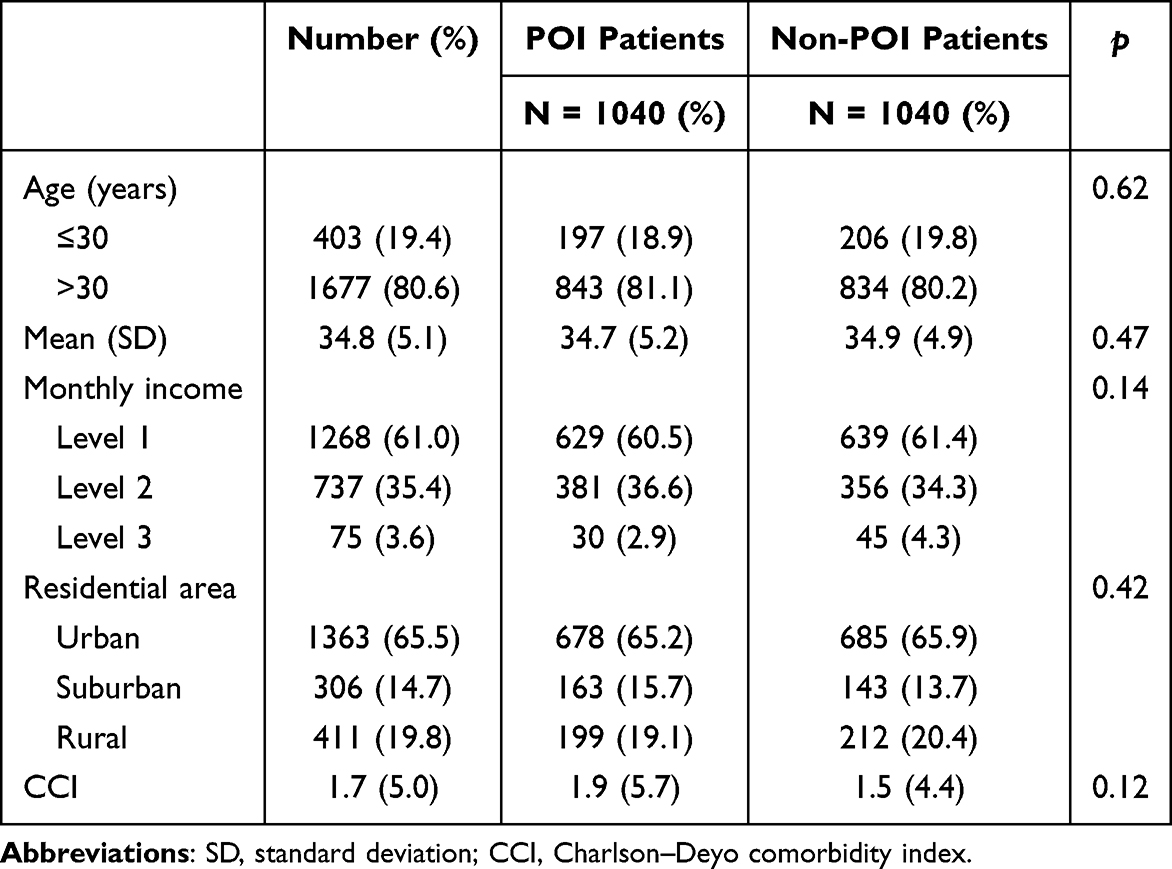 |
Table 1 Comparison of Demographic Data and Selected Comorbidities for AYAC Females with and without POI |
Results
Among the recruited subjects, matching those with POI to those without POI resulted in 1040 cases in each group. Descriptive statistics showed no remarkable differences in demographic or clinical features between patients with and with no POI after random matching procedure (Table 1). The mean age for enrollees was 34.8 years (SD= 5.1 years). Over 60% of participants resided in an urban area and had a low-level income.
Within the study period, 17.6% of POI patients and 56.1% of non-POI patients received adjunctive CHM treatment after AYAC. Multivariate conditional logistic regression analysis showed that those with a history of CHM use were 84% less likely to have POI than those not receiving CHM treatment. The positive effect of CHM treatment on the prevention of POI risk was predominant among patients ≤ 30 years of age (Table 2). CHM use provided the greatest therapeutic benefit when it was initiated within the first 3 years after AYAC onset (AOR, 0.08; 95% CI, 0.03–0.17). The association between CHM use and absence of POI gradually decreased with the delay of CHM initiation (Table 3).
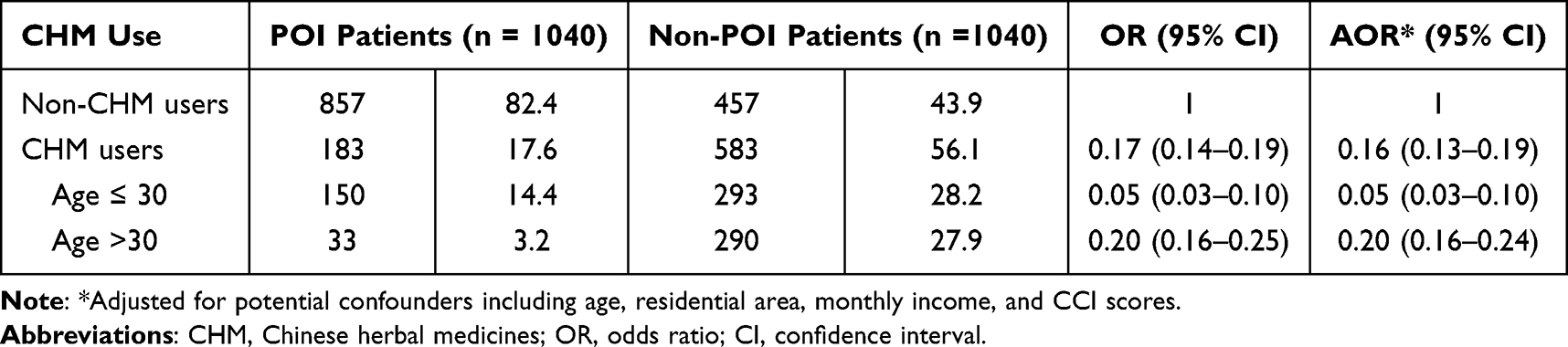 |
Table 2 Association Between POI Onset and CHM Use by Age Group |
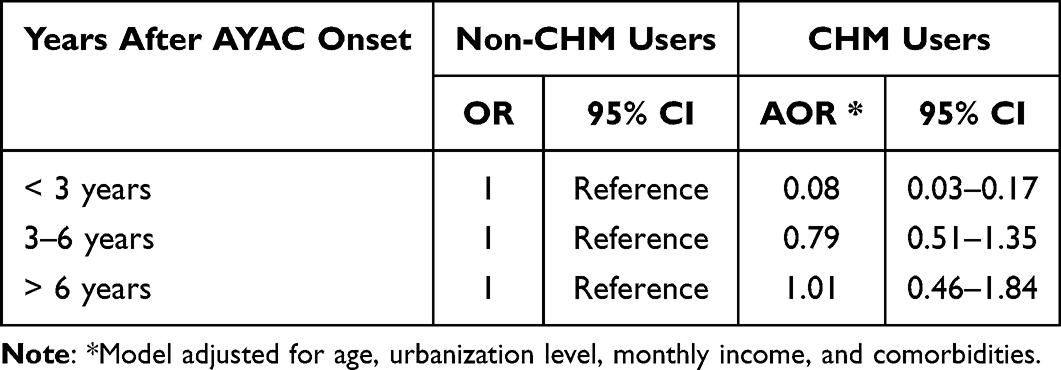 |
Table 3 Risk of POI in AYAC Females with and without Receiving CHM Stratified by Time of CHM Commencement |
Table 4 displayed the top ten most commonly prescribed single-herb and multi-herb formulae for the treatment of AYAC (). From them, we identifiedseveral potential agents that were correlated with a lower risk of POI, which included Da-Huang, Xiang-Fu, Ping-Wei-San, Ge-Gen-Tang, Xin-Yi-Qing-Fei-Tang, Jia-Wei-Xaio-Yao-San, and Shao-Yao-Gan-Cao-Tang (Figure 2).
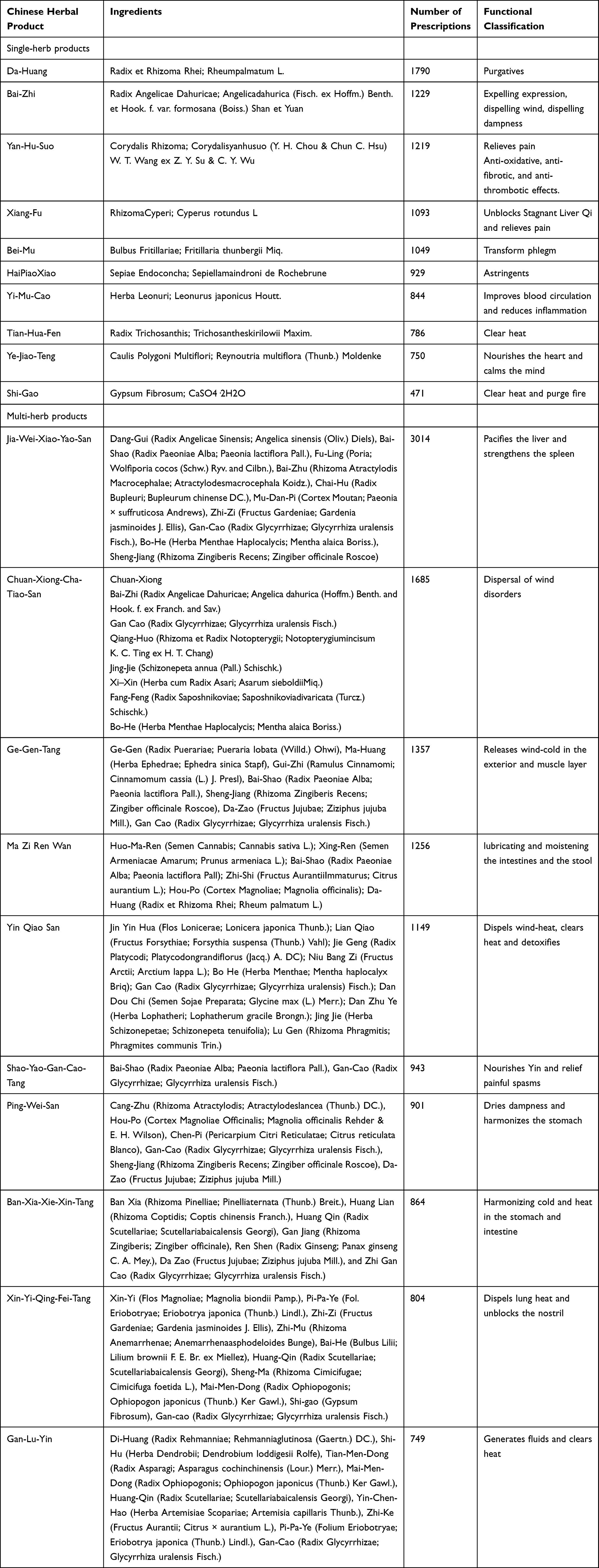 |
Table 4 The Ingredient Herbs Contained in the Most-Used Single-Herb and Multi-Herb Products Among Participants |
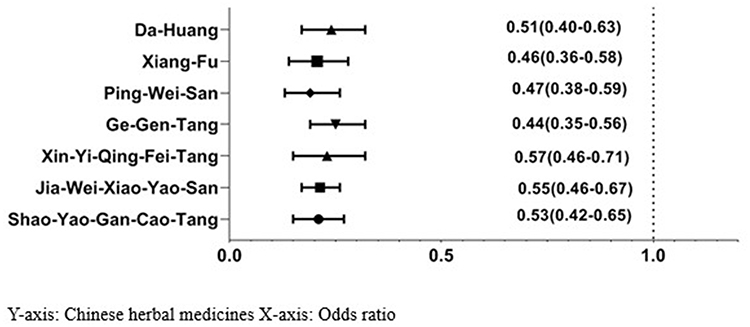 |
Figure 2 Risk of POI in females with AYAC as determined by multivariate conditional logistic regression analysis. |
Discussion
To the best of our knowledge, this study is the first to utilize the electronic health records to delineate the association between adjunctive CHM use and subsequent risk of POI among AYAC females undergoing chemotherapy-related treatments. We observed that CHM use correlated with a lower risk of POI. Furthermore, CHM users under the age of 30 experienced a significantly lower incidence of POI by over 90%, suggesting that the benefit of CHM for POI treatment is more pronounced in younger individuals. Importantly, the commencement of CHM treatment within three years after AYAC onset correlated with a notably lower risk of POI. The association between CHM use and lower POI risk reported herein were in accord with published data and extend our understanding of these medical conditions.15–17 Several explanations underlay the protective effects of CHM for the prevention of POI, which may include modulation of apoptosis, immune response regulation, enhancement of antioxidant capacity, and estrogen-like activity.16
One major breakthrough yielded by the findings of this study is the identification of specific CHM herbs that may act to prevent POI in females with AYAC. Several are single herbs, such as Da-Huang and Xiang-Fu, while others are multi-herb formulae that include Ge-Gen-Tang, Xin-Yi-Qing-Fei-Tang, Jia-Wei-Xaio-Yao-San, and Shao-Yao-Gan-Cao-Tang. We observed that Da-Huang use significantly decreased risk of POI. In clinical practice, Da-Huang has long been used for its diverse pharmacological properties, especially its ability to regulate ovarian function and influence fertility. Li et al found that aloe-emodin, one of the main pharmacodynamic ingredients of Da-Huang, inhibited growth and induced apoptosis of squamous cell carcinoma by regulating caspase-9 and caspase-3 levels.25 In addition, Da-Huang has been shown to improve reproductive health by contributing to estrogen balance and supporting ovarian function.26
We also observed that Xiang-Fu use was associated with a reduced risk of POI. The biological mechanism by which this herb could decrease the risk of POI may be related to its striking effect on hormone regulation. One recent in-vitro study demonstrated that Cyperus rotundos (Xiang-Fu) inhibits the mRNA expression of NF-kB through the Akt pathway.27 The PI3K/Akt pathway is well known to regulate a variety of cellular events, including cell proliferation, apoptosis, immune response, and the oxidative stress response by regulating various intra- and extra-cellular signaling molecules.28 This phenomenon may underlie the effects of this medication in females with AYAC.
This study shows that females with AYAC who took Ge-Gen-Tang were at lower chance of having POI. Pueraria, the primary component of Ge-Gen-Tang, is renowned for its reduced age-related vascular stiffening and improves endothelial-dependent vasodilation, Several scholars found that pueraria isoflavones, active compounds in Gegan, can balance estrogen levels, neutralize free radicals, and improve immune function.29 A recent review article further elucidated that by modulating T-lymphocyte activity, reducing B-lymphocyte proliferation, and diminishing associated autoantibodies, the pueraria isoflavones can efficiently alleviate menopausal symptoms and improve ovarian function in POI patients.16 Similarly, a positive correlation was observed between Xin-Yi-Qing-Fei-Tang use and a decreased risk of POI. Magnolin (Xin-Yi), a major constituent of Xin-Yi-Qing-Fei-Tang, has been traditionally prescribed for anti-inflammatory conditions.30 By targeting ERK1/2 activity, Lee and coworkers observed that magnolin greatly suppressed RSK2 phosphorylation and downstream proteins, including ATF1, c-Jun, and AP-1, thus abating neoplastic cell transformation and its relevant late effects.30 These underlying mechanisms may, therefore, account for the advantages of Ge-Gen-Tang and Xin-Yi-Qing-Fei-Tang reported in the current study.
Our results also show that uses of both Jia-Wei-Xaio-Yao-San and Shao-Yao-Gan-Cao-Tang positively correlated with a lower risk of POI. Jia-Wei-Xaio-Yao-San is the most frequently used CHM decoction for co-treatment with Tamoxifen in breast cancer patients undergoing hormone therapy.31 Using a breast-cancer mouse model, a previous study found that this herb inhibited tumor growth in 4T1-tumor–induced mice via regulation of the Bcl-2/Bax/TP53 signaling pathway.32 Jia-Wei-Xaio-Yao-San was found to exhibit dose-dependent antioxidative effects by inhibiting xanthine oxidase, an enzyme that converts xanthine to uric acid while producing superoxide anions as a byproduct.33 Excessive immune and inflammatory responses in ovaries are well known to impair ovarian function by disrupting T cell subsets and stimulating B cells to produce anti-oocyte and anti-ovarian antibodies.19 As to Shao-Yao-Gan-Cao-Tang, this herb has been traditionally used in the treatment of various gynecological disorders, including dysmenorrhea, polycystic ovary syndrome, endometriosis, and adenomyosis. Recent studies have shown that this formula exerts dose-dependent reductions in body weight and chronic inflammation by inhibiting the Toll-like receptor 4 /NF-κB signaling pathway.34,35 Suppression of this inflammation-linked pathway has been shown to eliminate endogenous peroxidases and inflammation, thus likely decreasing the risk of POI.
Despite the important public health implications of this study, it has several limitations and raises questions that are not fully resolved by this study. First, the claims-based database that we used lacks some pertinent information, such as physical activity, psychosocial variables, dietary intake and biomedical data. Future studies should further aim to overcome these drawbacks to validate the accuracy of our findings, especially indiverse AYAC types. Nonetheless, given the magnitude and statistical significance of the observed effect in this large-scale survey, these limitations are unlikely to affect our findings. Second, the use of secondary healthcare databases may have resulted in the accidental inclusion of miscoded patients, thereby introducing misclassification bias. To minimize this drawback, we only included individuals with new-onset AYAC or POI, and only after they had at least two outpatient visits reporting consistent diagnoses or at least one inpatient admission. It should also be acknowledged that the NHI of Taiwan randomly reviews charts and audits medical charges to assure the authenticity of claims files. Furthermore, since the coding approach and data availability were similar for the two groups, any misclassification bias would likely have been nondifferential, thus biased towards demonstrating no relationships between CHM use and POI risk. Third, despite the substantial correlation between CHM use and the subsequent lower risk of POI in females with AYAC, caution must be exerted in interpreting the results since participants were not randomly categorized into treated and control groups at the beginning of the study. For the sake of these reasons, the well-controlled, randomized, prospective, multicenter large clinical explorations are required to further validate the evidence shown herein. Not only is this manner imperative for elucidating the potential mechanism of action of CHM herbs, it also makes interpretation of the findings more straightforward and clinically robust.
Conclusions
Given the serious consequences of POI in females with AYAC, improvements in available therapeutic modalities to minimize this condition are needed. Findings of the present study shed light on the beneficial addition of CHM treatment to standard cancer therapies, by demonstrating its association with a reduced risk of chemotherapy-induced POI, particularly for AYAC patients under the age of 30. Early initiation of CHM, especially within three years of AYAC onset, further decreased POI risk, indicating its potential benefit in the prevention of chemotherapy-induced gonadotoxicity. In addition to providing preliminary evidence of the beneficial effects of CHM in arresting the development of POI, this study paves the way for further in vivo studies of specific herbal prescriptions to explore their potential for treating POI. In clinical practice, healthcare practitioners should initiate monitoring of patients’ ovarian function on a regular basis. Last but not least, it is very important for health care professionals to recognize that aspects of cancer survivorship continue to require attention and possible follow-up care via the interdisciplinary caring strategies.
Acknowledgments
This study used data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institutes, Taiwan. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or the National Health Research Institutes. We also thank for the suggestions from Dr. Tzu-Ning Tseng, Dr. Hou-Hsun Liao, and Professor Hanoch Livneh equally contributed to this work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ferrari A, Stark D, Peccatori FA, et al. Adolescents and young adults (AYA) with cancer: a position paper from the AYA Working Group of the European Society for Medical Oncology (ESMO) and the European Society for Paediatric Oncology (SIOPE). ESMO Open. 2021;6(2):100096. doi:10.1016/j.esmoop.2021.100096
2. Miller KD, Fidler-Benaoudia M, Keegan TH, et al. Cancer statistics for adolescents and young adults, 2020. CA Cancer J Clin. 2020;70(6):443–459. doi:10.3322/caac.21637
3. Lustberg MB, Kuderer NM, Desai A, et al. Mitigating long-term and delayed adverse events associated with cancer treatment: implications for survivorship. Nat Rev Clin Oncol. 2023;20(8):527–542. doi:10.1038/s41571-023-00776-9
4. Li W, Liang H, Wang W, et al. Global cancer statistics for adolescents and young adults: population based study. J Hematol Oncol. 2024;17(1):99. doi:10.1186/s13045-024-01623-9
5. Benmachiche A, Debbih AD. Premature ovarian insufficiency. In: Lutsenko OI, editor. Menstrual Cycle. London, UK: IntechOpen; 2018:97–209.
6. Baillargeon A, Pudwell J, McClintock C, et al. Premature ovarian insufficiency in female adolescent and young adult survivors of cancer: a population-based cohort study. J Obstet Gynaecology Canada. 2021;43(5):658. doi:10.1016/j.jogc.2021.02.033
7. Gallagher JC. Effect of early menopause on bone mineral density and fractures. Menopause. 2007;14(3 Pt 2):567–571. doi:10.1097/gme.0b013e31804c793d
8. Atsma F, Bartelink ML, Grobbee DE, et al. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: a meta-analysis. Menopause. 2006;13(2):265–279. doi:10.1097/01.gme.0000218683.97338.ea
9. van der Stege JG, Groen H, van Zadelhoff SJ, et al. Decreased androgen concentrations and diminished general and sexual well-being in women with premature ovarian failure. Menopause. 2008;15(1):23–31. doi:10.1097/gme.0b013e3180f6108c
10. Arecco L, Ruelle T, Martelli V, et al. How to protect ovarian function before and during chemotherapy? J Clin Med. 2021;10(18):4192. doi:10.3390/jcm10184192
11. Valsamakis G, Valtetsiotis K, Charmandari E, et al. GnRH analogues as a co-treatment to therapy in women of reproductive age with cancer and fertility preservation. Int J Mol Sci. 2022;23(4):2287. doi:10.3390/ijms23042287
12. Lee CJ, Lee MH, Yoo SM, et al. Magnolin inhibits cell migration and invasion by targeting the ERKs/RSK2 signaling pathway. BMC Cancer. 2015;15:576. doi:10.1186/s12885-015-1580-7
13. Chan JSK, Lee YHA, Hui JMH, et al. Long-term cardiovascular risks of gonadotropin-releasing hormone agonists and antagonists: a population-based cohort study. Clin Oncol. 2023;35(6):e376–e83. doi:10.1016/j.clon.2023.03.014
14. Mohamad NV, Ima-Nirwana S, Chin KY. The skeletal effects of gonadotropin-releasing hormone antagonists: a concise review. Endocr Metab Immune Disord Drug Targets. 2021;21(10):1713–1720. doi:10.2174/1871530321666201216164410
15. Fu Y, Ding DN, Shen Y, et al. Complementary and alternative medicine for premature ovarian insufficiency: a review of utilization and mechanisms. Evid Based Complement Alternat Med. 2022;2022:9053930. doi:10.1155/2022/9053930
16. Xueling L, Kun MA, Wenhua T, et al. Natural products for treatment of premature ovarian failure: a narrative review. J Tradit Chin Med. 2023;43(3):606–617. doi:10.19852/j.cnki.jtcm.20230227.002
17. Li M, Xiao YB, Wei L, et al. Beneficial effects of traditional Chinese medicine in the treatment of premature ovarian failure. Evid Based Complement Alternat Med. 2022;2022:5413504. doi:10.1155/2022/5413504
18. Siyu Y, Shixiao Z, Congying S, et al. Advances in cytokine-based herbal medicine against premature ovarian insufficiency: a review. J Ethnopharmacol. 2024;333:118477. doi:10.1016/j.jep.2024.118477
19. Kang MH, Kim YJ, Cho MJ, et al. Mitigating age-related ovarian dysfunction with the anti-inflammatory agent MIT-001. Int J Mol Sci. 2023;24(20):15158. doi:10.3390/ijms242015158
20. National Health Insurance Database, Taiwan. LHID 2000–2012. Available from: https://nhird.nhri.edu.tw//en/index.html.
21. Huang SC, Gau SY, Huang JY, et al. Increased risk of hypothyroidism in people with asthma: evidence from a real-world population-based study. J Clin Med. 2022;11(10):2776. doi:10.3390/jcm11102776
22. Liao -H-H, Livneh H, Huang H-L, et al. Reduced risk of dementia in patients with type 2 diabetes mellitus using Chinese herbal medicine: a nested case-control study. World J Diabetes. 2023;14(11):1632–1642. doi:10.4239/wjd.v14.i11.1632
23. Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag. 2006;4(1):1–22. doi:10.29805/JHM.200606.0001
24. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619. doi:10.1016/0895-4356(92)90133-8
25. Li Q, Wen J, Yu K, et al. Aloe-emodin induces apoptosis in human oral squamous cell carcinoma SCC15 cells. BMC Complement Altern Med. 2018;18(1):296. doi:10.1186/s12906-018-2353-z
26. Wen Y, Yan PJ, Fan PX, et al. The application of rhubarb concoctions in traditional Chinese medicine and its compounds, processing methods, pharmacology, toxicology and clinical research. Front Pharmacol. 2024;15:1442297. doi:10.3389/fphar.2024.1442297
27. Ahn JH, Choi JM, Kang ES, et al. The anti-endometriotic effect of cyperi rhizoma extract, inhibiting cell adhesion and the expression of pain-related factors through Akt and NF-kB pathways. Medicina. 2022;58(3):335. doi:10.3390/medicina58030335
28. Shi X, Wang J, Lei Y, et al. Research progress on the PI3K/AKT signaling pathway in gynecological cancer (Review). Mol Med Rep. 2019;19(6):4529–4535. doi:10.3892/mmr.2019.10121
29. Chen YWJ, Xie XF. Research progress on the chemical composition and pharmacological action of Radix Puerariae. Zhong Yao Yu Lin Chuang. 2021;2021(12):53–60.
30. Lee CJ, Lee HS, Ryu HW, et al. Targeting of magnolin on ERKs inhibits Ras/ERKs/RSK2-signaling-mediated neoplastic cell transformation. Carcinogenesis. 2014;35(2):432–441. doi:10.1093/carcin/bgt306
31. Wang BR, Chang YL, Chen TJ, et al. Coprescription of Chinese herbal medicine and Western medication among female patients with breast cancer in Taiwan: analysis of national insurance claims. Patient Prefer Adherence. 2014;8:671–682. doi:10.2147/PPA.S61280
32. Chen WF, Xu L, Yu CH, et al. The in vivo therapeutic effect of free wanderer powder (xiao yao san, Xiaoyaosan) on mice with 4T1 cell induced breast cancer model. J Tradit Complement Med. 2012;2(1):67–75. doi:10.1016/s2225-4110(16)30073-6
33. Chien SC, Chang WC, Lin PH, et al. A Chinese herbal medicine, jia-wei-xiao-yao-san, prevents dimethylnitrosamine-induced hepatic fibrosis in rats. Sci World J. 2014;2014:217525. doi:10.1155/2014/217525
34. Chang ZP, Deng GF, Shao YY, et al. Shaoyao-Gancao decoction ameliorates the inflammation state in polycystic ovary syndrome rats via remodeling gut microbiota and suppressing the TLR4/NF-κB pathway. Front Pharmacol. 2021;12:670054. doi:10.3389/fphar.2021.670054
35. Shao YY, Chang ZP, Cheng Y, et al. Shaoyao-Gancao Decoction alleviated hyperandrogenism in a letrozole-induced rat model of polycystic ovary syndrome by inhibition of NF-κB activation. Biosci Rep. 2019;39(1):BSR20181877. doi:10.1042/bsr20181877
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.