Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Missed Appointments and Associated Factors Among Children Accessing Anti-Retroviral Therapy During the COVID-19 Pandemic in South Western Uganda
Authors Nduhukire T, Adebayo IA, Luwaga R, Mandela I ![]() , Napyo A, Ainamani H, Musiime V
, Napyo A, Ainamani H, Musiime V
Received 6 February 2025
Accepted for publication 19 June 2025
Published 28 June 2025 Volume 2025:17 Pages 175—184
DOI https://doi.org/10.2147/HIV.S520964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Timothy Nduhukire,1 Ismail Abiola Adebayo,2 Rachel Luwaga,3 Immaculate Mandela,4 Agnes Napyo,4 Herbert Ainamani,5 Victor Musiime6
1Department of Pediatrics and Child Health, Kabale University School of Medicine, Kabale, Uganda; 2Department of Microbiology, Kabale University School of Medicine, Kabale, Uganda; 3Department of Nursing Science, Mbarara University of Science and Technology, Mbarara, Uganda; 4Department of Nursing, Kabale University School of Medicine, Kabale, Uganda; 5Department of Mental Health, Kabale University School of Medicine, Kabale, Uganda; 6Department of Pediatrics and Child Health, Makerere University College of Health Science, Kampala, Uganda
Correspondence: Timothy Nduhukire, Email [email protected]
Background: Disruptions to the health sector in Uganda during the COVID 19 pandemic affected health services in the early phases of the pandemic. Not much data exists on their effect on these same services during the later stages of the pandemic especially for children. To fill this gap, we set out to study missed appointments and their associated factors during the lockdown for children receiving Anti-Retroviral Therapy (ART).
Methods: This was a retrospective cohort study from January 2022 to May 2022. We included all children aged 0– 15 and adolescents aged 15– 19 years who were on ART. Electronic Medical Records (EMR) for the participants in the last 12 months were extracted. Descriptive statistics are presented. Binary logistic regression was performed, and odds ratios were reported.
Results: Out of the 382 participants, 26 (6.8%) missed appointments during the study period. The likelihood of missing appointments was increased when drugs were given to last 4 months than when they were given to last one month (COR 3.207, P value 0.026, 95% CI 1.150– 8.943). Patients were also more likely to miss appointments if their mode of receiving drugs was Facility based group (COR 3.174, P = 0.043, 95% CI 1.037– 9.713). Not having a viral load in the last 12 months increased the likelihood of missing an appointment (COR 2.309, P = 0.049, CI 1.004– 5.306).
Conclusion: A drug refill of 4 months and being scheduled to receive drugs by Facility-based group model predisposed the participants to missing the next appointment. Home- or community-based ART delivery to clients as well as drug prescriptions for a longer period could reduce missed appointments. Timely viral load testing should be encouraged as it correlates with adherence to appointments. More research is needed on the safety, storage practices and efficacy of ART given to last more than 2 months.
Keywords: COVID 19, pandemic, anti-retroviral therapy, missed appointments, electronic medical records viral load
Introduction
The COVID-19 pandemic has been labelled the worst public health crisis in this generation.1 As of February 7, 2022, COVID-19 accounted for 396,254,535 cases and 5,759, 785 deaths globally, with Africa reporting 11,196,707 cases and 241,826 deaths.2 The pandemic-orchestrated interruption of supply chains, diversion of resources, and weakened health systems presented great challenges to public health programs, notably those dealing with HIV/AIDS.3–5
Sub-Saharan Africa and Uganda in particular had been making great strides in the fight against HIV/AIDS. AIDS-related mortality had been reduced by 58% by the end of 2019.6 Additionally, 87% of people living with HIV (PLHIV) in Uganda knew their status, with 84% receiving treatment and 75% achieving viral suppression by the end of December 2019.6 This was in tandem with the global targets of 95–95–95 which ultimately would go a long way to achieving the national goal of AIDS epidemic control by 2030.7 All this was until covid 19 struck.
Movement restrictions to curb the rapid spread of the corona virus were quickly instituted in line with guidance from World Health Organisation (WHO).8 These were expected to result in reduced access to medical services, including HIV services.9–11 The expected diversion of human and financial resources to manage the epidemic in the context of weak health systems would most likely curtail service delivery to persons living with HIV (PLHIV). From the PLHIV point of view, poor socioeconomic status resulting from loss of employment and loss of heads of families could increase the risk of missed appointments for medical check-ups and drug pickups.12 Studies have shown that missed medical appointments, a potential outcome of pandemic-related restrictions, have been independently associated with an increased risk of AIDS-defining illnesses and death.13,14 Interruption to anti-retroviral therapy (ART) supply has been reported as the most important determinant of HIV-related mortality.15 Further, a three-month interruption for 40% of those on ART could cause a similar number of additional deaths as those that might be saved from COVID-19 through social distancing.15 In summary, pandemic-related movement restrictions and service disruptions were likely to reduce the ease of access to HIV treatment services and psychosocial support, leading to poor adherence, mental health deterioration, and greater HIV-related morbidity and mortality in children.16
Uganda instituted a national lockdown on March 21, 2020, in response to recommendations from the WHO.8 This lockdown was characterized by several stringent restrictions such as night-time curfews, travel bans, school closure, and physical and social distancing.17 The first national lockdown stretched from March 18, 2020, to June 4, 2020. It caused severe social and economic disruptions nationwide. Within the health sector, the main disruptions included the redeployment of the existing health workforce to respond to the pandemic. There was difficult access to health facilities due to restrictions that included suspension of public transport, curfew at 7 pm and restriction on the carrying capacity of private vehicles. These disruptions were reported to have affected maternal, neonatal, child, sexual, and reproductive health services in the early phases (Mar–Apr 2020) of the pandemic response10,18 Not much data exists on their effect on these services in later stages of the pandemic, yet the lockdowns were actually instituted in these later stages. To bridge this gap, there was a need to highlight the actual burden of HIV treatment interruption due to the COVID-19 pandemic restrictions during the lockdown and beyond. Accordingly, we set out to study missed appointments and their associated factors during the covid 19 lockdown among children receiving ART from selected health facilities in south western Uganda. We envisaged that results of our study would help in policy formulation, effective planning for service delivery during future epidemics of the same nature, inform future research as well as aid in developing new innovations in combating the effects of COVID-19.
Methods
Study Design and Duration
This retrospective cohort study was conducted between January 2022 and May 2022. In this period, data from the Electronic Medical Records (EMR) of selected health facilities from April to June 2020 were collected and analyzed. Similarly, data from the EMR for participants scheduled to pick their drugs from January to March 2020 (corresponding to the quarter before the first lockdown) and from July to September 2020 (corresponding to the quarter after the first lockdown) were collected and analyzed for comparison purposes.
Study Area
The study was conducted in Kabale District, southwestern Uganda. Located 408 km from Kampala, Uganda’s capital city, Kabale district has a population of approximately 285,097 according to Uganda Bureau of statistics (UBOS). It is a predominantly rural area with a high population density. The district is predominantly occupied by Bakiga, Banyankole and Banyarwanda tribes. It is comprised of three counties: Kabale Municipality, Ndorwa County West, and Ndorwa County East. We purposively selected all Health Center (HC) Fours (IVs) and Hospitals within the three counties of Kabale District and one HC III per county. Therefore, the following Health Facilities were used in this study. Maziba HC IV and Kyanamira HC III from Ndorwa East, Rubaya HC IV and Kamuganguzi HC III from Ndorwa West, Kamukira HC IV, Rushoroza HC III and Rugarama Hospital from Kabale Municipality. Each of these study sites was selected because they have a Uganda Ministry of Health accredited HIV clinic managed by a trained HIV/ART focal person, usually a medical doctor, clinical officer, or nursing officer. The provision of HIV care at these facilities follows national HIV treatment guidelines. HIV data is captured at every clinic visit using a paper-based HIV/ART card and then entered into an electronic open medical record system/EMR. Children at these facilities receive drugs according to a differentiated service-delivery (DSDM) model. The components of DSDM include facility-based individual management, facility-based groups, and fast-track drug refills. In facility-based individual management, the clients managed are unstable (new in care, non-suppressed viral loads, or other opportunistic infections such as tuberculosis, cryptococcal meningitis, and pneumocystis pneumonia). These clients must see a clinician at every visit before they have a drug refill. In the facility-based group, clients are seen in a group before receiving the drugs. These are usually pregnant or lactating, or adolescent women. Fast drug refills are for stable clients who have their drug refills without having to see a clinician when they come to the facility.
Study Participants
All children aged 0–15 years and adolescents aged 15–19 years who were enrolled for ART services in the selected health facilities and scheduled to receive ART services from April 1, 2020, to June 30, 2020, were considered eligible for the study. In addition, all children aged 0–15 years and adolescents aged 15–19 years who were scheduled to receive ART services from January to March 2020 and July to September 2020 were included for comparison purposes. We excluded children and adolescents aged 19 years and below who had been enrolled at the selected facilities but had been transferred to other facilities because we were unable to follow them up. The Uganda Electronic Medical Records (EMR) system considers children to be individuals under the age of 15 and adolescents to be individuals aged 15–19 especially in the context of HIV care and treatment. However, in the Ugandan context, the Ministry of Health and other International Organisations like WHO and United Nations Children’s Fund (UNICEF) often focus on adolescents aged 10–19 when considering health issues like mental health, reproductive health and risky behaviour. For this reason, our study used the inclusive age group of 0–19 to cater for both children and adolescents in the Ugandan health context.
Selection of Participants
To streamline our data collection and also reduce selection bias, we selected participants by consecutive sampling. We collected and analysed the records of all children receiving ART services at the study sites that fulfilled the selection criteria.
Measurements
Routine patient monitoring raw data were extracted from the Uganda EMR version 3.3.7. Clients’ data with return visit dates between April 2020 and June 2020 were extracted with basic patient characteristics, such as age category, sex, and service delivery model. We also extracted data on the number of months of ART dispensed, viral loads performed in the previous 12 months, and detectable viral loads in the previous 12 months. Data was checked by the Principal Investigator for errors, inconsistencies and any missing values. Extracting data from the same system that all the Facilities used to report EMR data ensured that data was formatted consistently across the different health facilities in the study. Preliminary data cleaning was performed in Microsoft Excel and Microsoft Access interchangeably, and the final cleaned dataset was exported to SPSS version 16 for analysis.
Descriptive statistics were presented as frequencies and percentages. At the bivariate level, Pearson’s chi-square tests were performed to test for relationships between missed appointments and different independent variables, such as sex, service point, number of months dispensed, viral load result, and detectable viral load in the previous 12 months of treatment. Statistically significant independent variables at bivariate analysis were also tested for their relationship with missed appointment using a binary logistic regression model, where unadjusted and adjusted odds ratios were reported. The statistical significance level was set at p <0.05. All variables which were statistically significant at bivariate analysis were included in the multivariate analysis to adjust for any confounders. Independent variables at multivariate analysis that had an Odds ratio of more than 1 and a P value of less than 0.05 were considered predictors of missed appointment. Those which had less than 1 were considered as those reducing the likelihood of missing appointments.
Data Management
Missed appointments were the outcome variable. A missed appointment was defined as any child in care who did not attend their scheduled appointment. This was measured on a binary scale (yes or no). A person was considered to be retained in care if they were active at the time of the study, had not missed appointments, and had their drugs. The independent variables were age category, sex, service delivery model, number of months dispensed, viral load result, and detectable viral load in the previous 12 months of treatment, as well as the quarter when the client was expected to come for drug refill. For the service delivery model, we considered the DSDM under which children were receiving care.
Ethical Considerations
Approval to conduct the study was obtained from the Research and Ethics Committee of Mbarara University of Science and Technology (MUST-2021-127). Patient and parental consent to review medical records was waived by the Research and Ethics Committee of Mbarara University of Science and Technology under the same ethical clearance for this study. We requested for this waiver of consent because we were going to review medical records and not directly interact with participants. We ensured patient data confidentiality in compliance with the Helsinki declaration.
Results
Baseline Characteristics Of The Participants
Data from 1142 participants were reviewed. Of these, 382 (33.5%) were observed during the period of April to June 2020, corresponding to the lockdown. Of the total number of participant data reviewed, 537 (47%) were male and 605 (53%) were female. Seven hundred and thirty-one (64%) participants were aged 0–14 years with 243 (63.6%) of these being seen in the period April to June 2020. Four hundred and eleven (36.0%) participants were adolescents. In the DSMD model, the facility-based group emerged as predominantly used in all the facilities, with a total of 633 (55.4%) of participants receiving their drugs through this model. Most of the participants (49.6%) were given drugs to last them one month. Very few participants (23 in total) received drugs for six months. Almost all the participants that were examined, 1089 (95.4%) in total had a viral load performed 12 months prior to the study. Details are presented in Table 1.
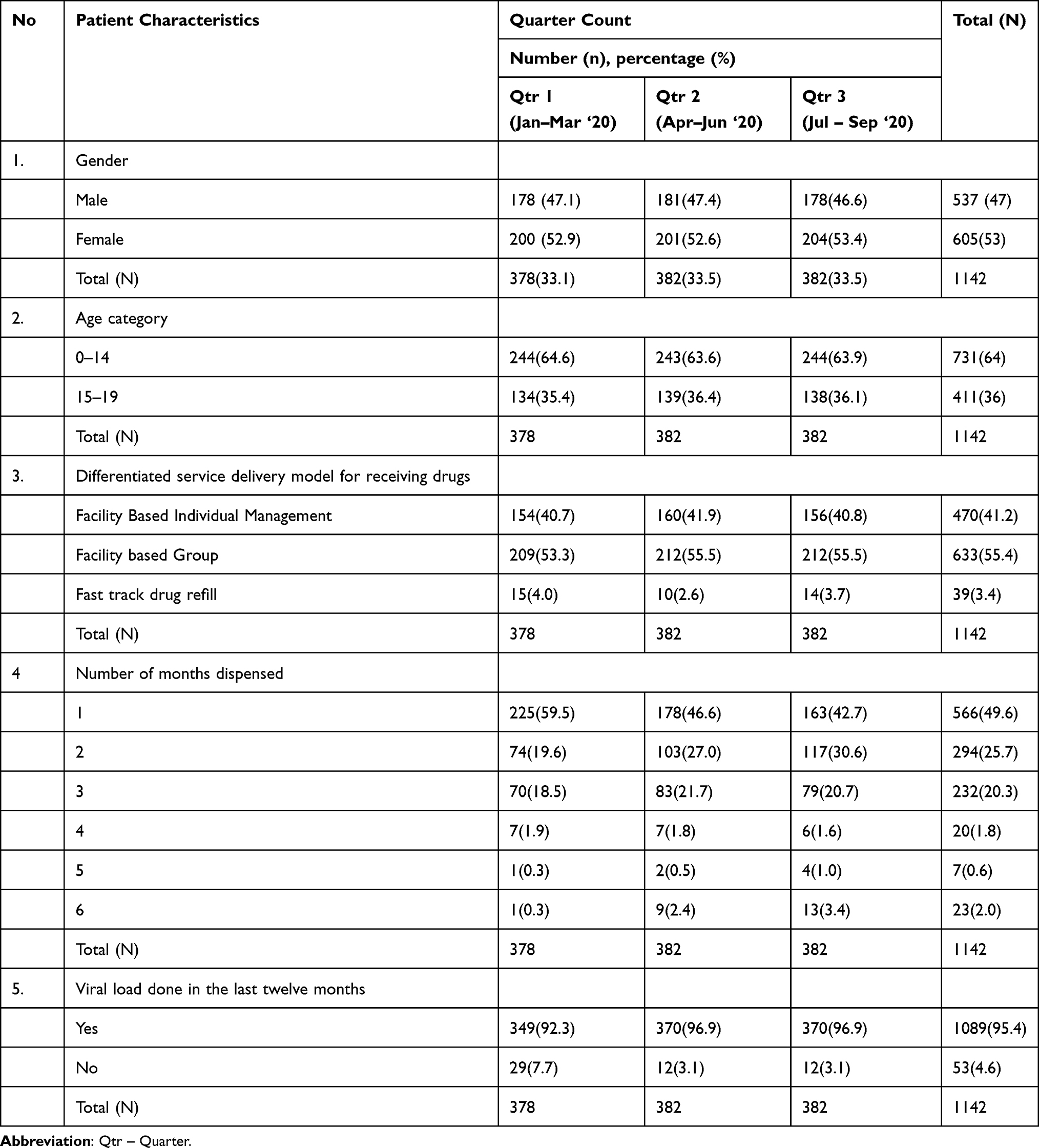 |
Table 1 Baseline Characteristics of the Participants |
Missed Appointment Among Children Receiving Anti-Rretroviral Therapy
Seventy-three (6.4%) participants missed their appointments overall across the three-quarters under study. Twenty-six (6.8%) participants missed appointments during the period of April to June 2020 (Quarter 2), (National lockdown period) compared to 18 (4.8%) in quarter 1 and 29 (7.6%) in quarter 3, although there was no statistically significant association between the quarter in which the participants were expected to receive their drugs and missed appointments.
Details are presented in Table 2.
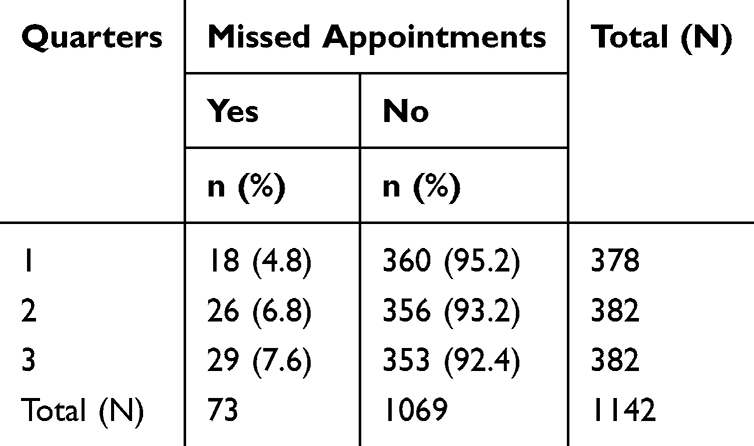 |
Table 2 Prevalence of Missed Appointments |
Factors Associated with Missed Appointment
The relationship between missed appointments and factors that were significantly associated with missed appointments was tested using binary logistic regression.
We found that the likelihood of missing appointments was increased when drugs were given for 4 months compared to when they were administered for 1 month (COR 3.207, P value 0.026 95% CI 1.150–8.943 AOR1.041, P value 0.943, 95% CI 0.352–3.078).
Additionally, patients were more likely to miss appointments if their mode of receiving drugs was Facility-based group (COR 3.174, P value 0.043 95% CI 1.037–9.713 AOR 0.377, P = 0.224, 95% CI 0.078–1.819).
Not having a viral load performed in the last 12 months increased the likelihood of missing an appointment (COR 2.309, P value 0.049 95% CI 1.004–5.306 AOR 1.408, P = 0.469, CI 0.557–3.558).
Results of binary logistic Regression are showed in Table 3
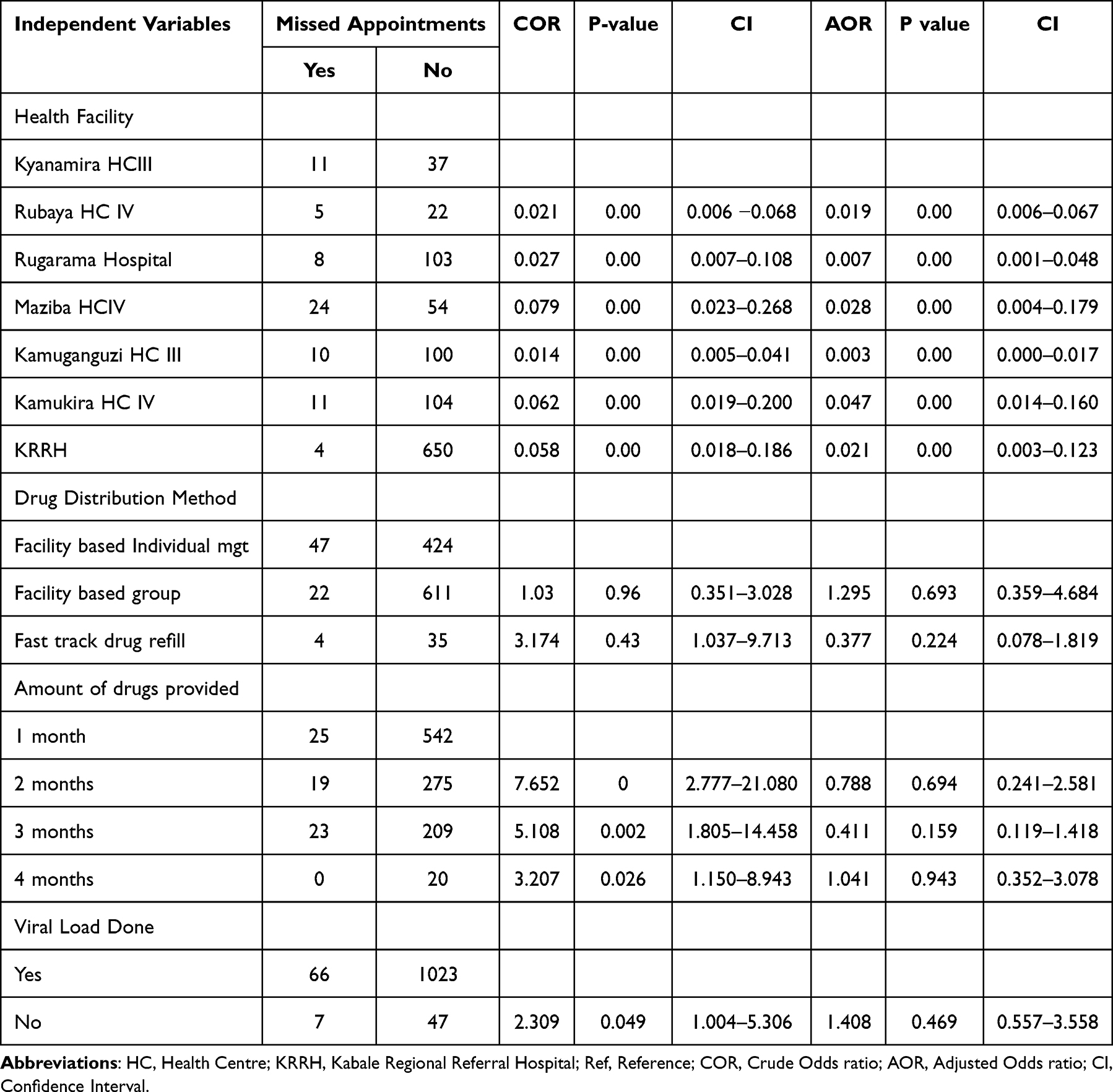 |
Table 3 Binary Logistic Regression for Factors Associated with Missed Appointment |
Discussion
Our study investigated missed appointments and factors associated with missed appointments among children 0–15 years and adolescents 15–19 years receiving anti-retroviral therapy in selected health facilities in Kabale District, south-western Uganda.
In this study, we found that 73 (6.4%) participants missed their appointments overall across the three-quarters under study, with 26 (6.8%) participants missing appointments during the period of April to June 2020 (Quarter 2), (National lockdown period) compared to 18 (4.8%) in quarter 1 and 29 (7.6%) in quarter 3. The participants who were most likely to miss their appointment were those whose mode of receiving drugs was Facility-based group. The likelihood of missing appointments was increased when drugs were given for 4 months compared to when they were administered for 1 month. Not having a viral load performed in the last 12 months increased participants’ likelihood of missing an appointment.
Our study, though in tandem with a number of studies from South Africa in reporting challenges by patients in honoring appointments during covid 1919–22 found a lower overall number of children who missed their appointments compared to what has previously been reported in Uganda.6 That said, the higher number of participants who missed their appointments in the second quarter compared to the preceding quarter could be attributed to challenges in accessing HIV treatment services, such as increased transport costs and lockdown restrictions. In addition, fear of COVID-19 exposure from health facilities could have led to a higher number of missed appointments in the second quarter, especially considering that most of the participants who missed their appointment were likely to be those who were receiving their drugs by the facility-based group model, which could enhance their risk of catching covid 19. These lockdown restrictions and the likelihood of fear of catching covid 19 during the covid 19 lockdown have been previously reported in studies conducted in peri-urban settings in Uganda.23,24 The high number of missed appointments in the Quarter after the Lockdown could be due to the fact that Uganda as a whole, especially the economy, took long to recover from the effects of the lockdown, and therefore, most participants were still unable to travel to the Facilities to receive drugs. It is also possible that fear of catching covid 19 at the Facilities was still real considering that the pandemic had not yet been declared to be over. Although our study did not explore why children had a low number missing their appointments during the covid 19 lockdown, our findings resonate with those of other studies. Studies from Kenya and Thailand reported low numbers of missed appointment in young adolescents.25,26 Another study involving children on ART aged 10 years or older in Kenya, Mozambique, Rwanda, and Tanzania reported low rates of missed appointments in young adolescents compared to youth. It is also worth mentioning that the study by Oryokot et al in Mbale, Eastern Uganda, had a higher number of child participants than this study, which could explain the relatively low number of children who missed their appointment in this study.
This study revealed that patients are more likely to miss appointments if their mode of receiving drugs is facility-based. This is not surprising considering that the risk of catching covid 19 at the Facility during the Lockdown was real,23 especially if you were expected to receive your drugs in a group. It is likely that many participants chose to stay away or perhaps receive drugs from lower health facilities closer to them. The transport restrictions coupled with the reduced economic activity during the lockdown, and hence the inability to meet the already high transport costs, could have also contributed to the likelihood of missing one’s appointment. It is also important to note that the differentiated service delivery model implemented by the facilities that participated in the study did not have a community component, unlike what was reportedly implemented at a Facility in Eastern Uganda6 where the DSD model in addition to what was implemented in facilities in our study included Community-client-led ART delivery (CCLAD) and community drug delivery points (CDDPs). All participants in our study had all been predetermined to receive drugs at the facilities and then covid 19 struck. Had there been a community component, it could have been easier to disburse treatments from selected locations in the community because health units had logistics to travel to the communities during the lockdown. The COvid 19 pandemic has indeed restarted conversations about community ART delivery models in Uganda.27 Zakamumpa et al in their study vouch for modifications to traditional community drug delivery models such as home-based ART delivery, drug pick-up at Community Drug Distribution Points (CDDPs), and provision of longer treatment refills27 It is not surprising that many HIV programs in Western Kenya have adopted a community approach to HIV care to reduce pressure on the health system and the waiting time for clients seeking HIV treatment services.28 This is something that facilities in southwestern Uganda could adopt to improve the robustness of HIV services in dealing with future pandemics.
In this study, participants who received drugs to last for 4 months were less likely to miss appointments compared to those who had received drugs for 1 month. Clients who received fewer drug refills were expected to visit the facilities more frequently which put great economic stress on them. Further, considering that during the COVID-19 pandemic, transport costs were much higher than before, it is plausible that clients opted to receive drugs from Facilities nearer to them or not receive drugs altogether. Our findings resonate with those of a study conducted in Eastern Uganda which also reported that clients who had been administered drugs to last 3 to 6 months were less likely to miss their appointment.6 Indeed, many policymakers have recommended the use of Multi Month Dispensing Model (MMD) as an antidote to increased missed appointments among PLHIV. MMD ART refills form a critical component of PLHIV-centered care, so much so that the President’s Emergency Plan for AIDS Relief (PEPFAR) had been at the forefront of recommending its increased uptake to mitigate the potentially dire consequences of missed appointments during the COVID-19 pandemic on client retention.29 Facilities in southwestern Uganda need to start implementing the recommendation of the National ART guidelines of November 2022 of giving clients six-month ART refills. This will go a long way in reducing missed appointment schedules among the PLHIV thereby improving their readiness to deal with any pandemic associated challenges in future.
Finally, our study found that having a viral load performed in the last 12 months was protective against missing appointments. A similar finding was reported in a study conducted in Eastern Uganda.6 Not many other studies have reported on this. However, it is plausible that clients who regularly pick their drugs are also likely to be disciplined with having their viral loads done. Based on our findings and those of other studies, we can postulate that encouraging health workers to be keen on ensuring that clients have their viral load done at the right time will ultimately improve their retention in care.
Strengths of the Study
We used routine program data for our study, which reflect the actual situation on the ground.
Limitation of the Study
We missed actual patient experiences regarding what could have deterred them from coming to their drug refill. Future studies could consider the qualitative aspect of gathering patients’ and health workers’ experiences. Using data from EMR meant that we were limited to only variables that are catered for in the EMR. This limited the number of factors we studied. However, our study lays a ground work for more research in this area. The smaller number of participants in our study compared to other studies could have impacted the power of our study. Larger studies on the same subject considering more observations than we did need to be carried out in similar settings.
Conclusion
In this study, the number of children who missed their appointments during the national lockdown was higher than that of those who missed their appointments in the previous quarter (before the lockdown). Children were most likely to miss appointments if they were scheduled to receive drugs from the health facility. On the other hand, participants who were given drugs for four months were less likely to miss their appointments as opposed to participants who received drugs for one month. Our study also found that participants who had their viral loads done in a timely manner were likely not to miss their appointments for receiving treatment.
Recommendations
- In Uganda, clients receive free ART and also have free Laboratory tests like viral load monitoring courtesy of the support of developing partners like PEPFAR and United States Agency for International Development (USAID). We have demonstrated that clients who receive drugs for a longer period of time tend not to miss their appointments which improves their adherence and ultimately reduces the morbidity and mortality from HIV AIDS. Additionally, we have demonstrated that clients who have their viral loads done in time will also most likely keep their appointments for receiving treatments. Our study recommends continued, if not improved funding to the HIV AIDS programs.
- We recommend that facilities in south western Uganda consider increased use of community approaches like Community-client-led ART delivery (CCLAD) and community drug delivery points (CDDPs) to issue drugs to clients on chronic care. With these approaches, ART is delivered to the community by both health workers and peers through outreach sites. The Consolidated guidelines for the prevention and treatment of HIV AIDS in Uganda (2022 edition) have further subdivided CCDPs into Drop in centers, Community Retail Pharmacy drug distribution point, Client led drug distribution points and home delivery. We recommend that Facilities set up Drop in centers and also start home delivery for distribution of ART to children in care. Emphasising a community approach to drug distribution will help mitigate future transport restriction challenges in the event of another pandemic. It will also deal with the accessibility to health facility problem that may arise from Kabale district being a mostly hilly district with roads that may be impassable especially in the rainy season.
- Facilities in south western Uganda need to align with the recommendation of the 2022 national guidelines for the prevention and treatment of HIV AIDS in Uganda to introduce 6-month refill prescription to all eligible clients. This, coupled with introduction of community approaches to drug distribution, will increase the robustness of health facilities in dealing with any restrictions that may hinder clients from keeping their treatment appointments.
- Larger studies need to be carried out to detail children and caretakers’ reasons and experiences that cause them to miss their appointments. The safety, storage practices and economic implications among clients who receive drug refills for a longer period of time need to be studied further.
Acknowledgment
Research reported in this publication was supported by the Fogarty International Center of the National Institutes of Health, US Department of State’s Office of the US Global AIDS Coordinator and Health Diplomacy (S/GAC), and the President’s Emergency Plan for AIDS Relief (PEPFAR) under Award Number 1R25TW011213. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We would also like to acknowledge the contribution of the following Research Assistants in carrying out the study; Lydia Tushabe, Isaac Atungisa, Ndyagumanawe Sarah, Kiconco Praise, Kashemeire Quinn, Ayebare Prima, Kambendiho Whycliffe, Tusiime Irene and Nomwesigwa Viola. We also appreciate Dr Gilbert Mateeka, the District Health officer, Kabale, Mr Alfred Besigensi, the District Health Educator, Kabale and Ms Sarah Beinomugisha, the District Biostatistician, Kabale, for their support during the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chandir S, Siddiqi DA, Mehmood M. et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: an analysis of provincial electronic immunization registry data. Vaccine. 2020;38(45):7146–7155. doi:10.1016/j.vaccine.2020.08.019
2. Chanda-Kapata P, Ntoumi F, Kapata N, et al. Tuberculosis, HIV/AIDS and malaria health services in sub-Saharan Africa–a situation analysis of the disruptions and impact of the COVID-19 pandemic. Inter J Infect Dis. 2022;124:S41–S6. doi:10.1016/j.ijid.2022.03.033
3. Cash R, Patel V. Has COVID-19 subverted global health? Lancet. 2020;395(10238):1687–1688. doi:10.1016/S0140-6736(20)31089-8
4. Divala T, Burke RM, Ndeketa L, Corbett EL, MacPherson P. Africa faces difficult choices in responding to COVID-19. Lancet. 2020;395(10237):1611. doi:10.1016/S0140-6736(20)31056-4
5. Nachega JB, Grimwood A, Mahomed H, et al. From easing lockdowns to scaling up community-based coronavirus disease 2019 screening, testing, and contact tracing in Africa—shared approaches, innovations, and challenges to minimize morbidity and mortality. Clinl Infect Dis. 2021;72(2):327–331. doi:10.1093/cid/ciaa695
6. Oryokot B, Kazibwe A, Oluka AI, Miya Y, Etukoit MB. COVID-19 and HIV treatment interruption: a case study of the AIDS Support Organization (TASO) Mbale clinic. World J AIDS. 2021;11(4):199–215. doi:10.4236/wja.2021.114015
7. Walker J-A. Achieving Health SDG 3 in Africa through NGO capacity building-insights from the Gates Foundation investment in Partnership in Advocacy for Child and Family Health (PACFaH) Project. Afr J Reproduct Health. 2016;20(3):55–61. doi:10.29063/ajrh2016/v20i3.10
8. WHO. Responding to community spread of COVID-19. Interim Guidance. 2020;7:1–6.
9. Kabagenyi A, Kyaddondo B, Nyachwo EB, et al. Disruption in essential health service delivery: a qualitative study on access to family planning information and service utilization during the first wave of COVID-19 pandemic in Uganda. Open Access J Contracept. 2022;Volume 13:75–82. doi:10.2147/OAJC.S360408
10. Burt JF, Ouma J, Lubyayi L, et al. Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda. BMJ Global Health. 2021;6(8):e006102. doi:10.1136/bmjgh-2021-006102
11. Atim MG, Kajogoo VD, Amare D, et al. COVID-19 and health sector development plans in Africa: the impact on maternal and child health outcomes in Uganda. Risk Management Healthcare Policy. 2021;Volume 14:4353–4360. doi:10.2147/RMHP.S328004
12. Pinto RM, Park S. COVID-19 pandemic disrupts HIV continuum of care and prevention: implications for research and practice concerning community-based organizations and frontline providers. AIDS & Behav. 2020;24(9):2486–2489. doi:10.1007/s10461-020-02893-3
13. Park W, Choe P, Kim SH, et al. One‐year adherence to clinic visits after highly active antiretroviral therapy: a predictor of clinical progress in HIV patients. J Internal Med. 2007;261(3):268–275. doi:10.1111/j.1365-2796.2006.01762.x
14. Mugavero MJ, Lin H-Y, Willig JH, et al. Missed visits and mortality among patients establishing initial outpatient HIV treatment. Clinl Infect Dis. 2009;48(2):248–256. doi:10.1086/595705
15. Jewell BL, Mudimu E, Stover J, et al. Potential effects of disruption to HIV programmes in sub-Saharan Africa caused by COVID-19: results from multiple mathematical models. Lancet HIV. 2020;7(9):e629–e40. doi:10.1016/S2352-3018(20)30211-3
16. Coker M, Folayan MO, Michelow IC, Oladokun RE, Torbunde N, Sam-Agudu NA. Things must not fall apart: the ripple effects of the COVID-19 pandemic on children in sub-Saharan Africa. Pediatr Res. 2020;2020:1–9.
17. Izudi J, Kiragga AN, Kalyesubula P, Okoboi S, Castelnuovo B. Effect of the COVID-19 pandemic restrictions on outcomes of HIV care among adults in Uganda. Medicine. 2022;101(36):e30282. doi:10.1097/MD.0000000000030282
18. Tumwesigye NM, Denis O, Kaakyo M, Biribawa C. Effects of the COVID-19 Pandemic on Health Services and Mitigation Measures in Uganda: Center for Global Development Washington. 2021.
19. Siewe Fodjo JN, Faria de Moura Villela E, Van Hees S, Vanholder P, Reyntiens P, Colebunders R. Follow-up survey of the impact of covid-19 on people living with hiv during the second semester of the pandemic. Int J Environ Res Public Health. 2021;18(9):4635. doi:10.3390/ijerph18094635
20. Hochstatter KR, Akhtar WZ, Dietz S, et al. Potential influences of the COVID-19 pandemic on drug use and HIV care among people living with HIV and substance use disorders: experience from a pilot mHealth intervention. AIDS & Behav. 2021;25(2):354–359. doi:10.1007/s10461-020-02976-1
21. Wagner Z, Mukasa B, Nakakande J, Stecher C, Saya U, Linnemayr S. Impact of the COVID-19 pandemic on use of HIV care, antiretroviral therapy adherence, and viral suppression: an observational cohort study from Uganda. J Acquired Immune Deficiency Syndromes. 2021;88(5):448. doi:10.1097/QAI.0000000000002811
22. Ahmed A, Dujaili JA, Jabeen M, et al. Barriers and enablers for adherence to antiretroviral therapy among people living with HIV/AIDS in the era of COVID-19: a qualitative study from Pakistan. Front Pharmacol. 2022;12:807446. doi:10.3389/fphar.2021.807446
23. Nalubega S, Kyenkya J, Bagaya I, et al. COVID-19 may exacerbate the clinical, structural and psychological barriers to retention in care among women living with HIV in rural and peri-urban settings in Uganda. BMC Infect Dis. 2021;21(1):1–10. doi:10.1186/s12879-021-06684-6
24. Linnemayr S, Jennings Mayo-Wilson L, Saya U, et al. HIV care experiences during the COVID-19 pandemic: mixed-methods telephone interviews with clinic-enrolled HIV-infected adults in Uganda. AIDS & Behav. 2021;25(1):28–39. doi:10.1007/s10461-020-03032-8
25. Koech E, Teasdale CA, Wang C, et al. Characteristics and outcomes of HIV-infected youth and young adolescents enrolled in HIV care in Kenya. Aids. 2014;28(18):2729–2738. doi:10.1097/QAD.0000000000000473
26. Teeraananchai S, Puthanakit T, Kerr SJ, et al. Attrition and treatment outcomes among adolescents and youths living with HIV in the Thai National AIDS Program. J Virus Eradication. 2019;5(1):33–40. doi:10.1016/S2055-6640(20)30276-4
27. Zakumumpa H, Tumwine C, Milliam K, Spicer N. Dispensing antiretrovirals during Covid-19 lockdown: re-discovering community-based ART delivery models in Uganda. BMC Health Serv Res. 2021;21(1):1–11. doi:10.1186/s12913-021-06607-w
28. Lagat H, Sharma M, Kariithi E, et al. Impact of the COVID-19 pandemic on HIV testing and assisted partner notification services, Western Kenya. AIDS & Behav. 2020;24(11):3010–3013. doi:10.1007/s10461-020-02938-7
29. PEPFAR. PEPFAR 2020 Country Operational Plan Guidance for All PEPFAR Countries. 2020.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.