Back to Journals » Clinical Ophthalmology » Volume 20
Misalignment After Implantation of One-Piece Hydrophobic Toric Intraocular Lenses: Comparison Among Manufacturers and Generations
Authors Nishimura T ![]() , Minami K
, Minami K
Received 23 December 2025
Accepted for publication 23 March 2026
Published 1 April 2026 Volume 2026:20 591237
DOI https://doi.org/10.2147/OPTH.S591237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Tomohisa Nishimura,1 Keiichiro Minami2
1Mikawa Eye Clinic, Saga-city, Saga Prefecture, Japan; 2KK Evidence Slyme, Osaka City, Osaka Prefecture, Japan
Correspondence: Keiichiro Minami, KK Evidence Slyme, 1-1-1 Miyahara, Yodokaga-ku, Osaka, 532-0003, Japan, Email [email protected]
Purpose: This study aimed to retrospectively compare postoperative axial misalignment of one-piece hydrophobic toric intraocular lenses (IOLs) from three manufacturers and two different generations.
Methods: Clinical records of 420 eyes implanted with six types of toric IOLs were reviewed, including SN6AT3-T9 and CNW0T3-T9 (Alcon, groups SA and CNW, respectively); 355T3-T5 and XY1AT3-T6 (Hoya, groups 355 and XY1A); and ZCT150/225/300/375 and ZCW150/225/300/375 (Johnson & Johnson Surgical Vision, groups ZCT and ZCW, respectively), with 70 eyes in each group. All surgeries were performed using identical surgical equipment and technique, and axial marks were aligned using a surgical guidance system. The axial marker position was measured on postoperative day 1, and the absolute difference from the target position was calculated to determine the degree of misalignment. The rate of misalignment of ≥ 10 ° was also examined.
Results: The median axial misalignments were SA = 2.3 °, CNW = 1.9 °, 355 = 3.8 °, XY1A = 3.1 °, ZCT = 4.3 °, and ZCW = 2.6 °. Misalignments in the 355 and ZCT groups were significantly greater than those in the SA and CNW groups (P < 0.045). Misalignment ≥ 10 ° was observed in 9 eyes in the 355 group, 6 eyes in the XY1A group, 10 eyes in the ZCT group, and 1 eye in the ZCW group.
Conclusion: Toric IOLs from Alcon exhibited the lowest degree of misalignment. A newer-generation IOL with frost-treated haptics (ZCW group) showed reduced misalignment despite no change in material composition. This comparison suggested that IOL material and haptic properties are factors associated with misalignment.
Keywords: hydrophobic acrylic toric intraocular lens, misalignment, IOL rotation
Introduction
Toric intraocular lenses (IOLs) are widely used in cataract surgery for eyes with preexisting corneal astigmatism because they restore uncorrected distance visual acuity (UDVA) and reduce postoperative refractive astigmatism.1 To minimize postoperative refractive astigmatism, the toric model and orientation of the implanted IOL are determined on the basis of preoperative measurements of corneal astigmatism. The effectiveness of astigmatic correction with a toric IOL depends on multiple factors, including the accuracy of preoperative measurements, selection of the appropriate toric model and axis orientation, intraoperative alignment of the toric IOL, and postoperative IOL rotation. Corneal astigmatism on both the anterior and posterior corneal surfaces can now be accurately measured using three-dimensional corneal topography, while swept-source biometry provides precise measurements of axial length and anterior chamber depth. Using these measurements, advanced algorithms can determine the optimal toric model and axial orientation. Additionally, intraoperative guidance systems enable precise real-time alignment of the implanted IOL.2
Postoperative deviations from the target orientation may arise from misalignment between the intended axis and the implanted IOL orientation immediately after implantation, as well as from rotation of the implanted IOL during the postoperative period.3 Ideally, a one-piece toric IOL should unfold rapidly, allowing the haptic ends to promptly establish contact with the capsular bag. The unfolding speed of an IOL depends on its material composition and haptic design.4–6 In addition, previous studies have shown that differences in IOL orientation primarily occur between the completion of surgery and the first postoperative day,7,8 highlighting the importance of evaluating both misalignment and rotation at this early postoperative time point. Although several studies, including meta-analyses, have assessed various toric IOLs,1,3 these evaluations have been conducted using different biometry techniques, toric calculation algorithms, and axis alignment methods. Consequently, it remains challenging to directly compare axial misalignment among multiple types of toric IOLs under standardized conditions. Therefore, this retrospective study compared axial misalignment among multiple types of toric IOLs from three manufacturers and two generations using standardized protocols for preoperative examination, toric model selection, and surgery performed by a single surgeon.
Materials and Methods
This retrospective study was approved by the Institutional Review Board of the Mikawa Eye Clinic (Nos. 7, 9, 11, and 12) and conducted in accordance with the Declaration of Helsinki. A waiver of informed consent was granted because of the retrospective nature of the study, which involved review of existing medical records only, while patient privacy and confidentiality were maintained according to institutional protocols. Clinical records of 70 consecutive eyes per IOL type from patients aged 65–90 years who underwent cataract surgery between January 2017 and December 2021 with implantation of a toric IOL were reviewed. Eyes with ocular pathology that could affect postoperative vision, other than cataract, or those with intraoperative complications such as failure to implant the IOL within the capsular bag were excluded.
Toric IOL Models
Table 1 lists the six types of one-piece hydrophobic toric IOLs implanted in this study, consisting of newer and predecessor models from three manufacturers.
- The Clareon® toric IOL CNW0T3-T9 (Alcon, Fort Worth, TX), included in the CNW group, was structurally similar to its predecessor, the AcrySof® toric IOL (SN6AT3-T9, Alcon), in the SA group, except that phenylethyl methacrylate was replaced with hydroxyethyl methacrylate.9 Consequently, the water content increased to 1.5%, and the glass-transition temperature decreased to 9.1 °C.
- In the toric IOLs manufactured by Hoya (Tokyo, Japan), no material modifications were made between the predecessor model 355T3-T5 (group 355) and the newer model XY1AT3-T6 (group XY1A). However, the newer model underwent oxygen processing using ultraviolet light to facilitate adhesion of capsular epithelial cells.10 Additionally, the overall length was increased from 12.5 mm to 13.0 mm together with a scuffed haptic surface.
- In the TECNIS® toric IOLs (Johnson & Johnson Surgical Vision: J&J, Santa Ana, CA, USA), the material and design did not change between the predecessor models ZCT150/225/300/375 (group ZCT) and the newer models ZCW150/225/300/375 (group ZCW), whereas the haptic surface was frosted in the newer model.
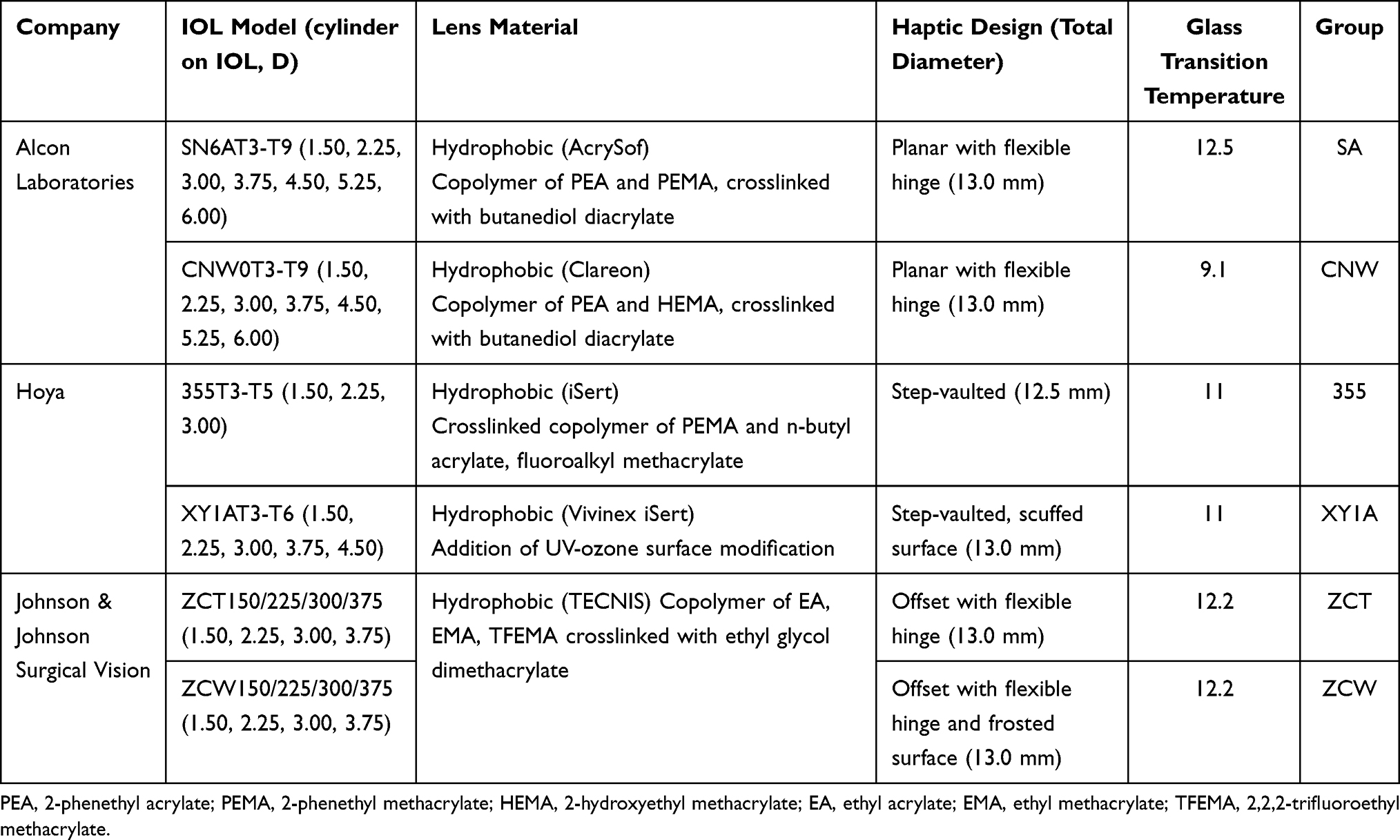 |
Table 1 Implanted One-Piece Acrylic Toric IOLs |
Surgery
All surgeries were performed by a single experienced surgeon with experience implanting toric IOLs in approximately 2900 eyes, using a standardized protocol. Preoperative measurement of axial length was used with the IOLMaster 700 (Carl Zeiss Meditec AG, Jena, Germany). When cataracts were too dense for measurement with the IOLMaster 700, ultrasound biometry was used instead. Corneal astigmatism was measured using the reference unit with measurement module of the surgical guidance system VERION® (Alcon). Using the axial length data, IOL power was calculated with the Barrett Universal II formula, and the target refraction was determined according to patient preferences. Subsequently, selection of the toric model and axis orientation were determined.
A 2.4-mm sclerocorneal single-plane incision was created, followed by continuous curvilinear capsulorrhexis using a 5.5-mm-diameter marker from the surgical guidance system. Cataract was removed using phacoemulsification and aspiration technique. The IOLs were implanted into the capsular bag using manufacturer-specified injectors. Eyes with capsular tears or ruptures were excluded from analysis. The IOL was aligned with the surgical guidance system, and the ophthalmic viscoelastic device was completely removed from the posterior and anterior chambers of the IOL. Then, the final IOL orientation was confirmed. Patients were advised to avoid excessive head movement or vigorous shaking until the examination next day.
Orientation Examination
As postoperative rotation of the implanted IOL most frequently occurs between the end of surgery and one day postoperatively,7,8 the IOL orientation was therefore examined on postoperative day 1. After mydriasis, retro-illumination images of the implanted toric IOL were captured using a slit-lamp microscope, and the axis marks of the toric IOL were connected (left bottom of Figure 1). This image was overlaid with an image of axis positions in the VERION image unit (left top of Figure 1), and the orientation difference between the target and postoperative positions was obtained (right of Figure 1). The difference (positive value for clock-wise direction) and the absolute value defined as the misalignment were measured. Both axial orientations were measured with the patient in a sitting position to avoid the influence of eye cyclotorsion.
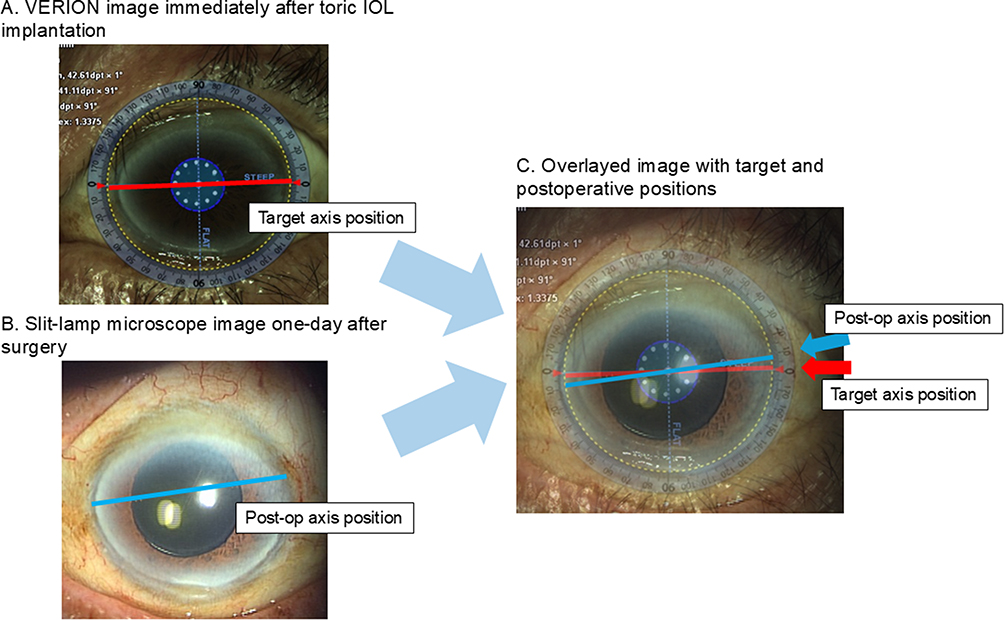 |
Figure 1 Orientation examination. Axis positions from the VERION image unit (left top in red line) and a retro-illumination image of the implanted toric-IOL with the axis mark position (left down in blue line), an overlaying an image with, the orientation difference between the two positions (right) was obtained. |
Postoperative Refraction and Vector Analysis
One month after surgery, uncorrected and corrected distance visual acuities (UDVA and CDVA, respectively) and cylindrical refraction were examined. Using preoperative cylindrical refraction values, vector analysis based on the Alpins method11 was performed using the AstigMATIC software.12 From the target-induced astigmatism vector (TIA) and surgically induced astigmatism vector (SIA) for toric IOL implantation, the difference vector (DV) was obtained. As DV corresponded to the residual astigmatism vector after treatment, the influence of misalignment can be evaluated.
Statistical Analysis
Differences in age, preoperative corneal astigmatism, and postoperative cylinder were examined using analysis of variance (ANOVA), followed by Tukey’s multiple comparison test. The means of the arithmetic and absolute differences in IOL orientation were examined using ANOVA and the Kruskal–Wallis’s test following the Steel-Dwass multiple comparison test, respectively. The rates of absolute differences of ≥5 ° and ≥10 ° were compared between groups using the chi-squared test following residual analysis. Statistical significance for the two-tailed test was set at P < 0.05.
Results
The demographic data of the groups are presented in Table 2. The mean age of the SA group was significantly higher than that of the 355 and ZCT groups (P < 0.022, Tukey’s multiple comparison test), and the mean age of the CNW group was higher than that of the ZCT group (P = 0.046). However, the mean differences in age were less than 3.6 years. In one eye each in the AT and ZCT groups and in 2 eyes in the 355T group, axial lengths were measured using ultrasound pachymetry. No significant differences in mean axial lengths were observed between the groups (P = 0.082, one-way ANOVA). Significant differences were observed in preoperative corneal astigmatism (P < 0.001, ANOVA) due to the range of cylinder powers used in the IOLs.
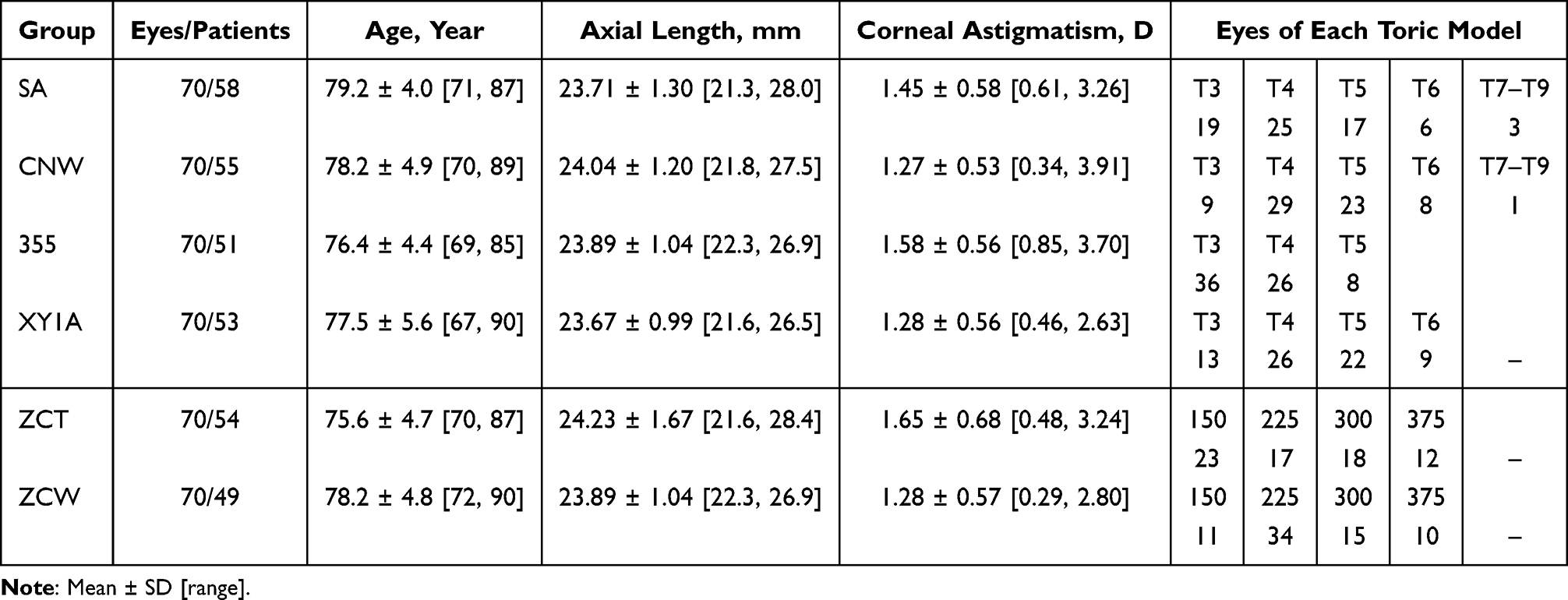 |
Table 2 Demographic and Preoperative Characteristics of Eyes Implanted with Six Types of Toric IOLs |
Table 3 presents the arithmetic mean values as well as the mean absolute values of misalignment. Although the SD values were wider in 355, XY1A, and ZCT groups for the arithmetic means, no significant difference was observed (P = 0.21, ANOVA). For the absolute values that corresponding to misalignments, the 355 and ZCT groups showed significantly larger values than the SA and CNW groups (P < 0.010, Steel-Dwass multiple comparisons). In contrast, no significant differences were observed among the SA, CNW, XY1A, and ZCW groups. Figure 2 shows box plots of the absolute misalignment values. As shown in Table 3, the rates of ≥5 °were significantly lower in the SA, CNW, and ZCW groups (P < 0.032, residual analysis), and higher in the 355 and ZCT groups (P < 0.0033). For rates of ≥10 °, the 355 and ZCT groups were higher (P < 0.011), whereas the SA and CNW groups were lower (P = 0.018).
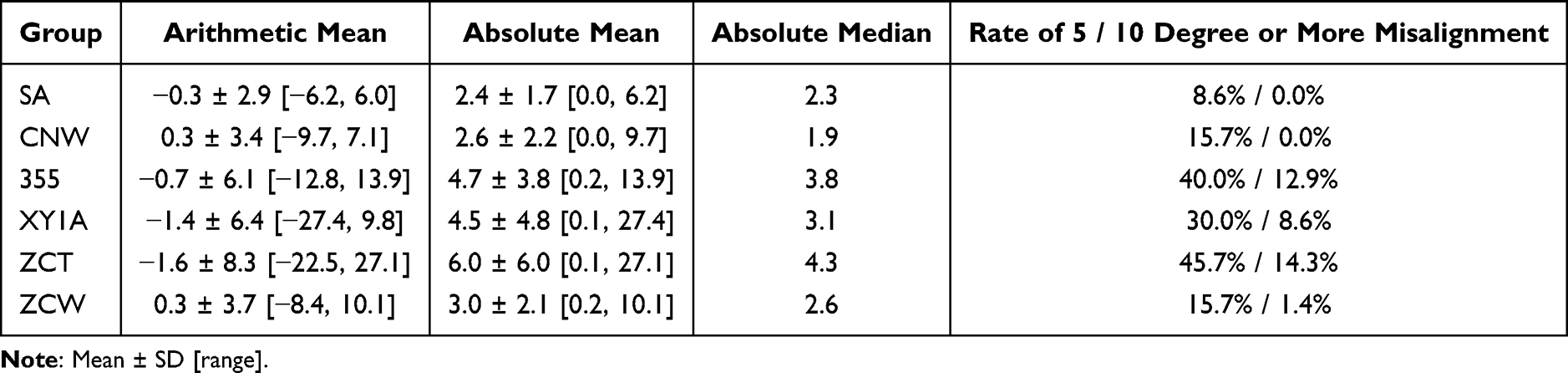 |
Table 3 Postoperative 1-Day Misalignments |
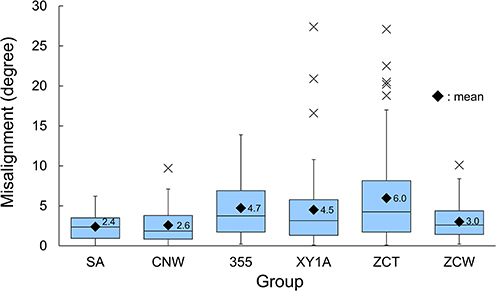 |
Figure 2 Box plots of the arithmetic (upper) and absolute (lower) differences in IOL orientation after implantation of six types of toric IOLs. Mean (upper) and median (lower) values are indicated by black ◆. |
Table 4 presents UDVA, CDVA, cylindrical refraction, and mean DV values in the six toric IOL groups at one month respectively. Significant differences were observed between the 355 and ZCT groups and the ZCW group (P < 0.027, Steel-Dwass comparison) in UDVA and between the 355 and ZCT groups (P = 0.034) in CDVA. For cylindrical refraction, the 355 group showed higher values than the CNW and ZCW groups (P<0.0064, Tukey’s multiple comparisons), whereas the mean differences were relatively small (0.20 D). No remarkable differences were observed in the arithmetic or vector means. Figure 3 shows the DVs obtained from the vector analysis. Influences of large misalignment of ≥10 ° were not identified. The impact of large misalignments 1 day postoperatively was observed in the 355 and ZCT groups for UDVA and only in the 355 group for cylindrical refractions and CDVA.
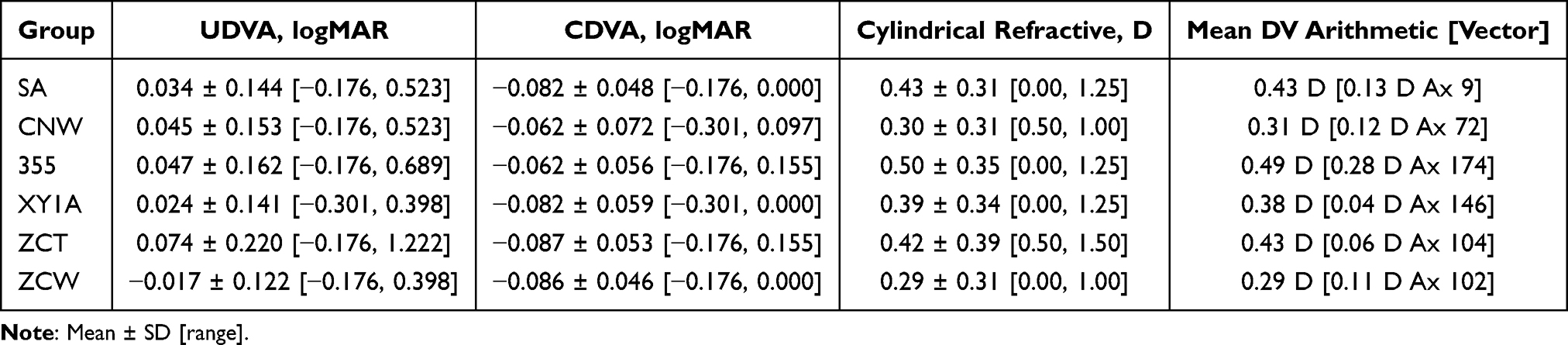 |
Table 4 Spheric and Cylindrical Refractions and Visual Acuity 1 Month Postoperatively |
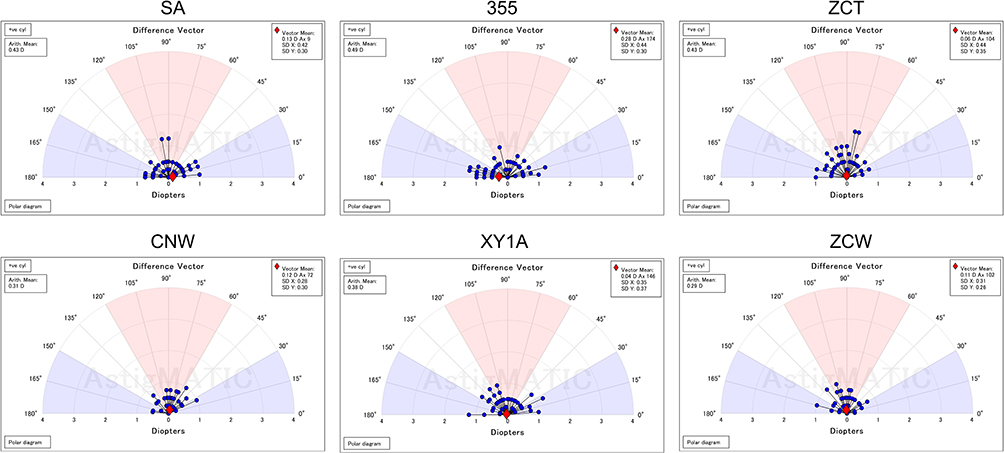 |
Figure 3 Difference vector plots for six toric IOLs. |
Discussions
Misalignment following implantation of six types of toric IOLs from three manufacturers was compared using identical procedures. The use of newer models from Hoya and J&J successfully reduced misalignment. In contrast, no significant difference was observed between the toric models from Alcon. In the evaluation by Osawa et al, misalignment of XY1A toric IOLs on postoperative day 1 (mean: 5.43 °) was significantly lower than that of 355 toric IOLs (mean: 8.78 °), and the rate of misalignment of 10 ° or more improved from 45.7% to 10.9% at 1 month postoperatively.13 In a previous comparison between ZCW and ZCV, which is a violet light-blocked version of ZCT, at 3-months postoperatively ZCW significantly reduced the mean misalignment (P = 0.018) and the rate of 10 ° or more (P = 0.04).14 In a subgroup analysis of the latest meta-analysis, newer toric models such as ZCW decreased the mean absolute rotation.3 These findings are consistent with those of the current study.
Although misalignments of ≥10 ° occurred in 9, 6, and 10 eyes in the 355, XY1A, and ZCT groups, respectively, no impact was observed in the DV results across the six groups. Misalignment creates differences between SIA and TIA and increases DV.11 Specific groups exhibited large misalignments, yet the mean DV values were not different from those of the other groups with few or no such cases. Further investigation remains necessary.
SA and CNW groups showed comparable misalignment. The toric IOL platform of SN6AT3-T9 consists of a material suitable for faster unfolding4,5 and a haptic with a flexible hinge to ensure contact between the haptic end and the capsule. The toric IOL of CNW0T3-T9 contains slightly softer material, with a lower glass-transition temperature and higher water content.9 Therefore, detecting a significant difference in misalignment between these models may be challenging.
Among TECNIS toric IOLs, the ZCW group demonstrated notably reduced misalignment. Experimental evaluations of IOL unfolding and clinical comparisons between ZCT and ZCW IOLs indicated that faster unfolding and a frosted IOL contribute to reduced misalignment.14 In addition, a meta-analysis3 concluded that haptic design is effective in improving rotational stability. Frosted haptic arms improve rotational stability by increasing friction between the haptic arm and the capsular bag.15 Although the unfolding speed was slower than that of the SN6AT3-T9 IOLs platform,5 the misalignment of the ZCW group was comparable to that of the SA and CNW groups. Because the hinge design of the haptics was similar to that of the Alcon toric IOL, it was speculated that increasing friction between the haptic arm and the capsular bag would have a greater impact. In XY1A IOLs, the haptic surface was scuffed, and misalignment was slightly greater than that in the ZCW group, suggesting that differences in haptic surface properties may contribute to this outcome. Further investigation is warranted.
In Hoya toric IOLs, improvements in the total IOL length and the haptic surface were designed to reduce misalignment. Compared with a toric IOL with an overall length of 12.5 mm, a toric IOL with an overall length of 13.0 mm decreases misalignment.13 However, the XY1A group exhibited a slightly greater misalignment than the SA, CNW, and ZCW groups. Differences in IOL material and haptic design, as well as slow unfolding16 should be investigated.
This study has some limitations. First, owing to its retrospective design, IOL orientation could not be examined immediately after surgery. This factor should be examined to evaluate the exact difference between misalignment and IOL rotation.3 Previous findings have indicated that the greatest difference in IOL orientation was observed one day postoperativelu.7,8 Current measurements therefore remain adequate for evaluating material and haptic design effects. Further evaluation requires experiments at physiological ocular temperature17 and prospective comparisons. Next, bilateral cases occurred in groups. To maintain the privacy and confidentiality of patient privacy-related data, patient identification was completely masked. Ideal analysis would include one eye from each patient; however, there was a slight risk owing to the small number of bilateral cases. Lastly, the implantation period varied among the toric models. Newer models were implanted sequentially after their predecessors rather than in parallel. Owing to longer experience with identical procedures, surgeons and examiners became accustomed to implanting new toric models. This proficiency was minimally influenced by the use of established examination and surgical guidance systems.
Conclusions
Alcon toric IOLs exhibited the least misalignment, with no significant differences between the material generations (AcrySof and Clareon). Newer generations of the XY1A and ZCW groups reduced misalignment by changing the design and overall length of the haptics. This comparison performed under the same procedure demonstrated the influence of IOL material and haptic properties on misalignment.
Abbreviations
ANOVA, analysis of variance; CDVA, corrected distance visual acuity; DV, difference vector; IOL, intraocular lens; SIA, surgically induced astigmatism vector; TIA, target-induced astigmatism vector; UDVA, uncorrected distance visual acuity.
Data Sharing Statement
The data from this study are available from the corresponding author upon reasonable request.
Acknowledgments
This paper was previously presented at the 39th Asia-Pacific Academy of Ophthalmology Congress, Bali, Indonesia, February 2024.
Disclosure
Mr Keiichiro Minami reports a patent issued to Tomey corporation. No other potential conflict of interest was reported by the authors.
References
1. Al-Mohtaseb Z, Steigleman WA, Pantanelli SM, et al. Toric monofocal intraocular lenses for the correction of astigmatism during cataract surgery: a report by the american academy of ophthalmology. Ophthalmology. 2024;131(3):383–8. doi:10.1016/j.ophtha.2023.10.010
2. Zhou F, Jiang W, Lin Z, et al. Comparative meta-analysis of toric intraocular lens alignment accuracy in cataract patients: image-guided system versus manual marking. J Cataract Refract Surg. 2019;45(9):1340–1345. doi:10.1016/j.jcrs.2019.03.030
3. Li ES, Vanderford EK, Xu Y, Kang PC. Rotational stability of toric intraocular lenses by lens model and haptic design: systematic review and single-arm meta-analysis. J Cataract Refract Surg. 2024;50(9):976–984. doi:10.1097/j.jcrs.0000000000001486
4. Iwase T, Tanaka N. Unfolding characteristics of a new hydrophobic acrylic intraocular lens, and possible association with complications in triple procedures. Clin Experiment Ophthalmol. 2007;35(7):635–639. doi:10.1111/j.1442-9071.2007.01565.x
5. Eom Y, Lee JS, Rhim JW, Kang SY, Song JS, Kim HY. A simple method to shorten the unfolding time of prehydrated hydrophobic intraocular lens. Can J Ophthalmol. 2014;49(4):382–387. doi:10.1016/j.jcjo.2014.06.002
6. Borkenstein AF, Borkenstein EM. Geometry of acrylic, hydrophobic IOLs and changes in haptic-capsular bag relationship according to compression and different well diameters: a bench study using computed tomography. Ophthalmol Ther. 2022;11(2):711–727. doi:10.1007/s40123-022-00469-z
7. Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38(1):54–59. doi:10.1016/j.jcrs.2011.08.028
8. Inoue Y, Takehara H, Oshika T. Axis misalignment of toric intraocular lens: placement error and postoperative rotation. Ophthalmology. 2017;124(9):1424–1425. doi:10.1016/j.ophtha.2017.05.025
9. Werner L, Thatthamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490–1497. doi:10.1016/j.jcrs.2019.05.017
10. Matsushima H, Iwamoto H, Mukai K, Obara Y. Active oxygen processing for acrylic intraocular lenses to prevent posterior capsule opacification. J Cataract Refract Surg. 2006;32(6):1035–1040. doi:10.1016/j.jcrs.2006.02.042
11. Alpins N. Astigmatism analysis by the Alpins method. J Cataract Refr Surg. 2001;27(1):31–49. doi:10.1016/S0886-3350(00)00798-7
12. Gauvin M, Wallerstein A. AstigMATIC: an automatic tool for standard astigmatism vector analysis. BMC Ophthalmol. 2018;18(1):255. doi:10.1186/s12886-018-0920-1
13. Osawa R, Oshika T, Sano M, Yuguchi T, Kaiya T. Rotational stability of modified toric intraocular lens. PLoS One. 2021;16(3):e0247844. doi:10.1371/journal.pone.0247844
14. Takaku R, Nakano S, Iida M, Oshika T. Influence of frosted haptics on rotational stability of toric intraocular lenses. Sci Rep. 2021;11(1):15099. doi:10.1038/s41598-021-94293-3
15. Vukich JA, Ang RE, Straker BJK, et al. Evaluation of intraocular lens rotational stability in a multicenter clinical trial. Clin Ophthalmol. 2021;15:3001–3016. doi:10.2147/OPTH.S309214
16. Ota Y, Minami K, Oki S, Tanaka M, Bissen-Miyajima H. Early Outcomes and axial alignment after implantation of the HOYA toric intraocular lens. Jpn J. Ophthalmic. Surg. 2018;31:138–141. in Japanese.
17. Minami K, Yaguchi S, Bissen-Miyajima H. Temperature-controlled porcine eye holder for observing intraocular temperature during cataract surgery. Sci Rep. 2023;13(1):4331. doi:10.1038/s41598-023-31070-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.