Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Minimum Acceptable Diet and Associated Factors Among HIV-Exposed Children Aged 6–24 Months in Debre Tabor Town, Ethiopia
Authors Yisak H ![]() , Ambaw B, Walle Z
, Ambaw B, Walle Z ![]() , Alebachew B, Ewunetei A
, Alebachew B, Ewunetei A ![]()
Received 30 July 2020
Accepted for publication 4 October 2020
Published 28 October 2020 Volume 2020:12 Pages 639—645
DOI https://doi.org/10.2147/HIV.S274764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Hiwot Yisak,1 Birhanie Ambaw,1 Zebader Walle,2 Banchiayehu Alebachew,2 Amien Ewunetei3
1Department of Public Health Nutrition, College of Health Science, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Health Service and Management, College of Health Science, Debre Tabor University, Debre Tabor, Ethiopia; 3Department of Pharmacy, College of Health Science, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Hiwot Yisak Email [email protected]
Introduction: Minimum acceptable diet is a composite indicator of minimum dietary diversity and minimum meal frequency. World Health Organization’s newborn child feeding and HIV guidelines suggestbeginning complementary nourishments at six months, and breastfeeding for HIV-exposed children. HIV infected mothers may be more sensitive on feeding practices to protect their children from contracting the disease. On the other hand, HIV infection is associated with higher risk food insecurity which may affect feeding practices of children. But in Ethiopia, there is lack of evidence on extent of minimum acceptable diet of HIV-exposed children. Therefore, the objective of this study was to assess minimum acceptable diet and associated factors among HIV-exposed 6– 24 months aged children.
Methods: An institution-based cross-sectional study was conducted in health institutions of Debre Tabor town. The study was conducted on 287 mother-child pairs attending antiretroviral therapy (ART) and prevention of mother-to-child transmission (PMTCT) at public health facilities. Descriptive statistics like frequency, proportions, mean and standard deviation were computed. Multi-variable logistic regression was run to identify independent predictors of the outcome variable (minimum acceptable diet). A p-value < 0.05 was used to declare statistical significance.
Results: About 76% (95% CI: 70.8– 80.8) and 58.2% (95% CI: 53.0– 68.3) children were fed with appropriate meal frequency and recommended dietary diversity, respectively. One hundred (34.8%) (95% CI: 29.3– 40.4) of children were fed a minimum acceptable diet and 59.9% (95% CI: 54.0– 65.9) of children consumed iron rich or fortified food. Out of the total, 203 (71.0%) (95% CI: 66.1– 76.2) of the mothers had good knowledge on minimum dietary diversity and meal frequency feeding practices. In multi-variable logistic regression poor knowledge with AOR = 0.32, 95% CI: 0.17– 0.58, maternal workload with AOR = 0.38, 95% CI: 0.19– 0.75 and inadequate information about child feeding from health care providers with AOR = 0.46, 95% CI: 0.26– 0.81 were statistically significant predictors of minimum acceptable diet.
Conclusion: The study revealed that the proportion of children who received minimal acceptable diet was lower than that of WHO recommendation for good practice. Knowledge, maternal workload and information related to complementary feeding were associated with low minimum acceptable diet.
Keywords: minimum acceptable diet, minimum dietary diversity, meal frequency, HIV-exposed children, Ethiopia
Introduction
Minimum acceptable diet is a composite indicator of minimum dietary diversity and minimum meal frequency; it is the proportion of children 6–24 months of age who receive a minimum diversified diet and minimum meal frequency (apart from breast milk).1 Since infants and young children are in a fast growth and development stage, the World Health Organization (WHO) suggest the presentation of solid, semi-solid or delicate nourishment at six months2 and by this newborn children and small children can get the minimum meal frequency, diversified diet, adequate eating regimen, and iron rich food sources.3
Improper feeding practices and high paces of infectious diseases are the chief reasons for lack of healthy nourishment during the initial two years of life.4 Under-nourishment is responsible for over half of all youth deaths and it is high among HIV-exposed newborn children after 6 months age, which could be because of inappropriate feeding practices.5
Ideal feeding practices among HIV-exposed children in the initial 2 years of life are essential to meet nutritional necessities4 and improve physical development and intellectual advancement.5 Study outcomes indicate that improper Infant and Young Child Feeding (IYCF) practices in this window period is among the significant reasons for young children malnourishment6 bringing about changeless results of hindering, poor intellectual turn of events, and builds dangers of numerous interminable ailments.7,8 The negative effect of malnutrition and unhealthiness during this period can limit profitability during adulthood by adversely influencing the future social and financial improvement of nations and furthermore can prompt intergenerational patterns of malnutrition.9,10
HIV infection and disease is related with a danger of household-level food insecurity, which can influence the nutritional status of youngsters who need complementary food.11 HIV positive children have likewise, more unfortunate nutritional results than HIV negative children. Both HIV exposure and HIV infection worsen youth under-nutrition. Children living with HIV or born to HIV positive mothers are a high-hazard group with exceptional needs.12
The 2016 WHO general newborn child feeding and HIV guidelines suggest that extending the period of breastfeeding to 24 months or beyond is likely to improve HIV-free survival among HIV-exposed infants, especially while diarrhea and pneumonia are significant causes of infant and child mortality; this recommendation applies if the mother is receiving ART and there is no evidence of clinical, immunity or viral failure. The recommendation of breast feeding in HIV- positive mothers is different when contrasted with the general population. In such manner, HIV positive mothers may be more sensitive on feeding practices to prevent their children from HIV infection. The sensitivity of mothers on feeding practice might lead to malnourished babies with illnesses such as diarrhea.3,13 In Ethiopia, there is lack of evidence on the extent of minimum acceptable diet of HIV-exposed children. Therefore, the aim of this investigation was to evaluate the minimum acceptable diet among HIV-exposed children in Debre Tabor town, Ethiopia.
Materials and Methods
Study Area and Period
The study was conducted from March 15 to April 30,2019 in Debre Tabor town public health institutions providing ART and PMTCT services. Debre Tabor town is found in north-western Ethiopia in the Amhara regional state at 667 km distance from Addis Ababa city and is 97 km away from Bahir Dar city. In this town there are 3 governmental health centers, 1 general hospital, four health posts and five private clinics. Around 81,637 (male = 40,652 and female = 40,935) clients are expected to get health care services in these facilities. There are 18,987 households and the number of total reproductive age (15–49 years) females is estimated to be 20,000. Among the institutions, 3 governmental health centers and 1 general hospital in the town provide ART and PMTCT services. There are 4036 reproductive age mothers (15–49 years) on ART and 318 mothers getting PMTCT service during the study period.
Study Design
Institutional-based cross-sectional study was conducted.
Source Population
All HIV positive mother-child pairs in Debre Tabor town attending ART/PMTCT follow-up at public health facilities of Debre Tabor town.
Study Population
HIV positive mother-child pairs in Debre Tabor town attending ART/PMTCT follow-up at public health facilities of Debre Tabor town during the study period.
Eligibility Criteria
Inclusion Criteria
The respondents who were eligible to participate in the study included mothers who have children aged 6–24 months and were residents of Debre Tabor town for a period of not less than 6 months.
Exclusion Criteria
Respondents who were mentally or physically disabled such as mothers who are unable to speak and/or listen, mothers with serious illness at the time of data collection.
Sample Size Determination
The sample size was calculated using Epi Info software, considering 95% confidence intervals (CIs), a 5% margin of error, and a 24% proportion of exclusive breastfeeding practice among HIV-exposed infants, estimated based on a study conducted in west Shewa which gave a maximum sample size14 among different proportions of complementary feeding indicators among HIV positive mothers in Ethiopia from different literature. With the incorporation of a 7% non-response rate (found from the same study where the proportion was taken), the total sample size was 300.
Sampling Procedure
Since the source population was nearly the same as the calculated sample size, the research was conducted on all source population.
Study Variables
Dependent Variable
Minimum acceptable diet
Independent Variables
- Socio-demographic and socio-economic factors (age, marital status, family size, level of education, occupation, and income level)
- Maternal knowledge on recommended child feeding
- Maternal and child related factors (maternal and childhood illness, maternal workload)
- Cultural norms and beliefs (presence of prohibited foods for infants, familial and cultural acceptance)
- Obstetric factors (ANC, PNC, birth order, parity, place of delivery)
Data Collection Procedure and Measurement
After written informed consent was obtained, the data on both child feeding practice and associated factors were taken using a pre-tested structured interviewer administered questionnaire. Data were collected from all eligible mothers as they attended the institution for follow-up. Recommended child feeding practice was assessed based on compliance to WHO recommended practices for timely initiation (introduce complementary feeding at six months), minimum meal frequency (fed minimum of three meals/day and four times/day for children aged 6–8 months and 9 months and above, respectively) and minimum meal diversity (fed four or more foods within 24 hours)15 using 24 hours dietary recall method. Complementary feeding practice was appropriate if all the three indicators mentioned above were fulfilled otherwise it was considered as inappropriate.
Operational Definitions
HIV-Exposed Infant or Child
An infant or child born to a mother living with HIV until the infant or child is reliably excluded from being HIV infected.
Complementary Foods
Any solid or semi-solid or soft foods which are given to the child.
Minimum Dietary Diversity
Children 6–24 months of age who consume from 4 or more of the 7 food groups (grains/tubers/roots, legumes/nuts, milk/diary product, eggs vitamin A rich, flesh foods and other fruits and vegetables) with 24 hours dietary recall.
Minimum Meal Frequency
Children of age 6–8 months fed a minimum of three meals per day and children aged 9 months and above fed four times per day within a 24-hourdietary recall period.
Minimum Acceptable Diet
A composite indicator of minimum dietary diversity and minimum meal frequency. Proportion of children 6–24 months of age who received a minimum diversified diet and minimum meal frequency (apart from breast milk).
Good Knowledge of Child Feeding
When the respondents correctly answer 60% or above out of 10 questions about MTCT and child feeding knowledge questions.
Poor Knowledge of Child Feeding
When the respondents correctly answer below 60% of questions about MTCT and child feeding knowledge questions (24).
Young Child
Child less than 24 months of age.
Infant
Child less than 12 months of age.
Maternal Workload
Perceived presence of work load by mothers.
Data Quality Control
The questionnaire was adapted first in English by the investigators and then translated to Amharic by another individual who is native to Amharic and has experience in translation. The questionnaire was translated back to English by another individual in order to maintain its conceptual equivalence. Two days training was given to the data collectors on how to collect the data and keep confidentiality of the respondents. Moreover, during data collection the principal investigator was closely supervising the activity on a daily basis. At the end of each data collection day the principal investigator checked the completeness of filled questionnaires and whether recorded information makes sense or not to ensure the quality of data collected.
Data Analysis
After data were collected, entering into Epi Info software version 3.1 (Lauritsen JM and Bruus M., Odense, Denmark, 2003–2005) was done and then exported to SPSS version 23 (IBM® SPSS® Statistics, Armonk, NY: IBM Corp) software for data processing and analysis. Descriptive statistics like frequency, proportions, mean and standard deviation was computed accordingly. The results were described using table, chart, graph and narration. Bi-variable logistic regression was carried out to screen candidate variables for the multiple logistic regression analysis and p-value ≤0.25 was taken as a cut-off point. Then multi-variable logistic regression was computed to identify independent predictors of inappropriate minimum dietary diversity and meal frequency feeding practices. A p-value <0.05 was used to declare statistical significance.
Results
Socio-Demographic Characteristics
A total of 287 mother–child pairs were included in the study with a response rate of 95.7%. The mean (± SD) age of the mothers was 31.5 m (±4.99) years. The mean (±SD) family size of the households was 4.42 (±1.52), and about 81.5% of households had ≤5 family members. Most of the mothers had primary education (34.8%), married (67.9%) and housewife (32.4%). Regarding to economic status based on average monthly income, about more than half of respondents (57.3%) earn USD111.1 and higher monthly, whereas 11.3% respondents earn 37.0 and lesser USD (Table 1). About 245 (85.4%) of mothers have disclosed their HIV status to their families. About 10 (3.3%) of mothers reported that they were having breast infection and 73 (24.3%) of mothers reported to have work load. Two hundred fifty one (83.7%) of mothers were having ANC follow up.
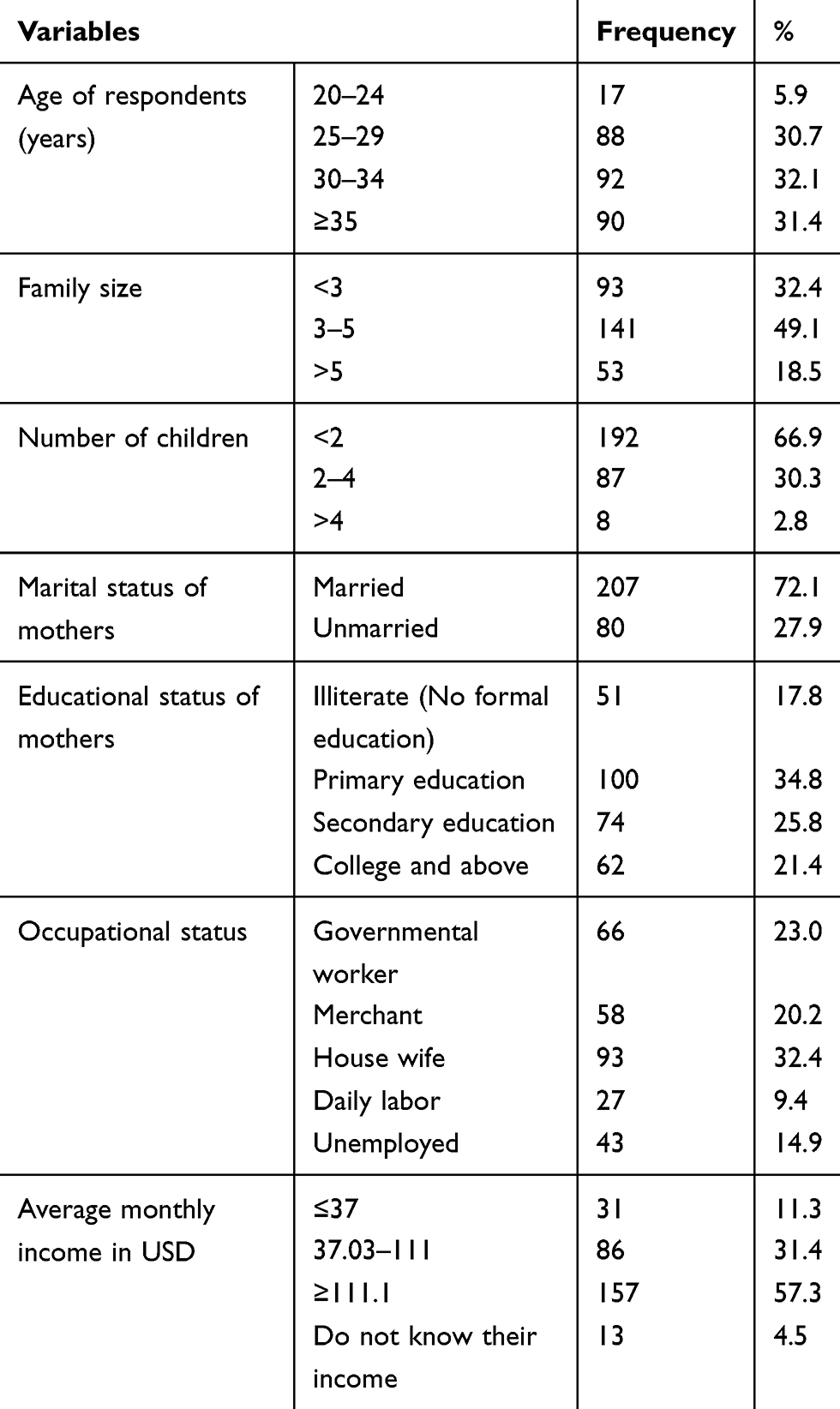 |
Table 1 Socio-Demographic Characteristics of Respondents in Debre Tabor Town, Ethiopia, 2019 |
Child Feeding Practices
During the survey mothers with children aged 6–24 months were also asked retrospectively about child feeding practices. From the total interviewed mothers, about 76% and 58.2% of children were fed with appropriate meal frequency and recommended dietary diversity, respectively. One hundred (34.8%) children were fed minimum acceptable diet and 59.9% of children consumed iron rich or fortified food (Table 2).
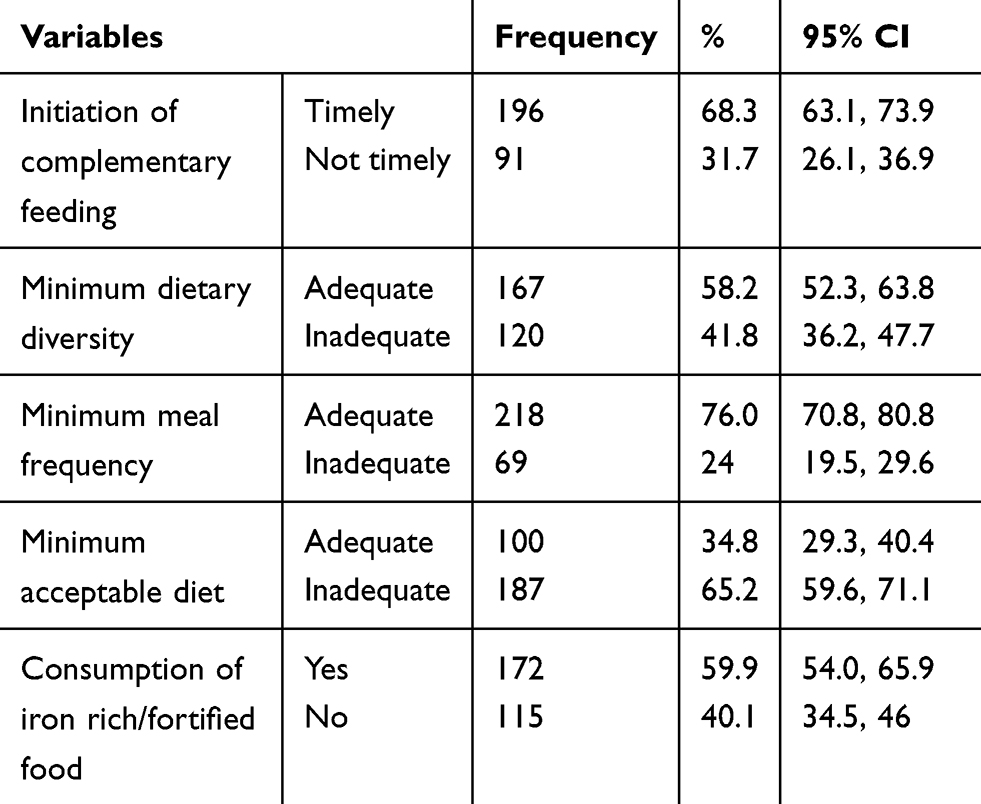 |
Table 2 Child Feeding Practices of HIV Positive Mothers in DebreTabor Town, Ethiopia, 2019 |
Mothers’ Infant and Young Child Feeding Knowledge
A total of ten questions were included to assess the knowledge status about complementary feeding (CF) practices. Out of the total 203 (71.0%), 95% CI (66.1, 76.2) of the respondents had good knowledge on CF practices and 83 (29.0%), 95% CI (23.8, 33.9) of respondents had poor knowledge.
Minimum Acceptable Diet and Associated Factors
Assessment of association between child feeding practices and respondents’ socio-demographic and economic status, knowledge, and other maternal and child characteristics was made by employing bi-variable logistic regression to screen candidate variables and multi-variable binary logistic regression model to get independent association.
The bi-variable logistic regression analysis showed that knowledge, breast infection/problem, ANC follow-up, disclosure of HIV status, child feeding difficulties, information about child feeding, maternal workload, income, and fear of transmission were found to have association (P< 0.25) with inappropriate meal diversity and meal frequency feeding. In multi-variable logistic regression poor knowledge with AOR = 0.32, 95% CI (0.17–0.58), maternal workload with AOR = 0.38, 95% CI (0.19–0.75) and adequate information about child feeding from health care providers with AOR = 0.46, 95% CI (0.26–0.81) were statistically significant predictors of minimum acceptable diet of HIV-exposed children in the study area (Table 3).
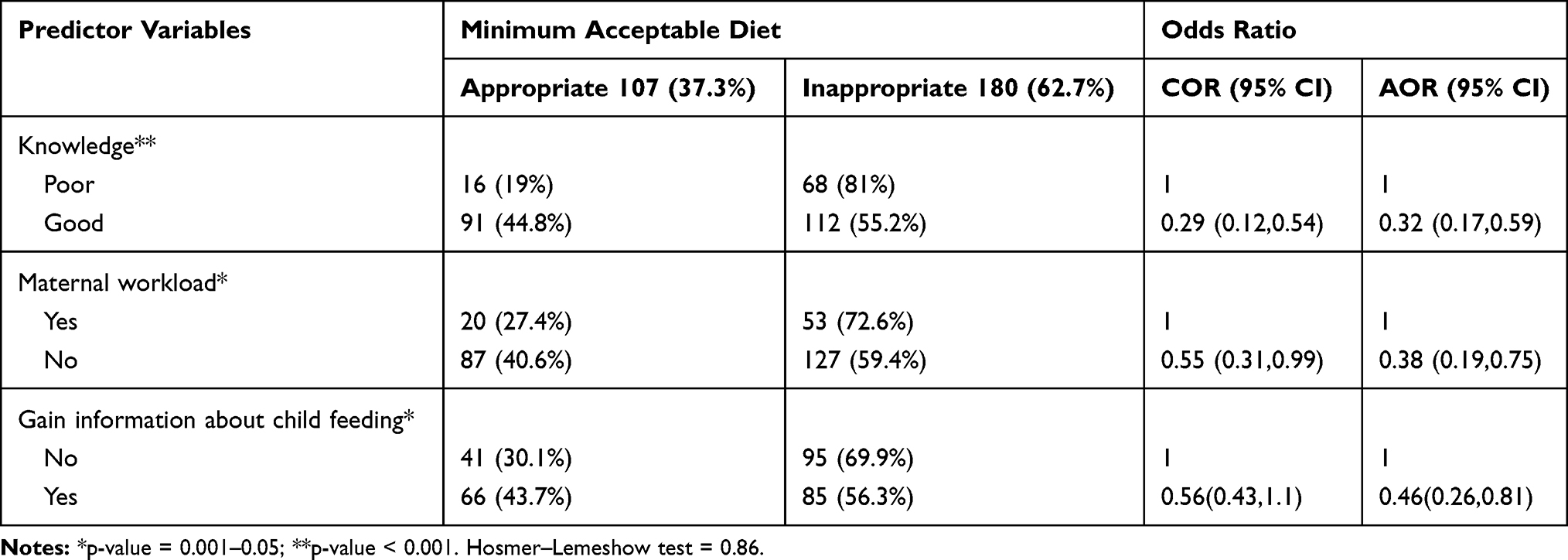 |
Table 3 Multi-Variable Logistic Regression Showing Associated Factors of Minimum Acceptable Diet in Debre Tabor Town, Ethiopia, 2019 |
Discussion
In this study the prevalence of MDD and MMF was 58.2%, and 76% respectively which was higher than the findings from southern Ethiopia (MDD=34.4% and MMF=42.7%).16 The discrepancy might be due to the time between studies and could be due to higher maternal literacy rate (43.03% of mothers were illiterate in the study done in southern Ethiopia; whereas in this study illiterate mothers were only 17.8%) and utilization of institutional delivery in the latter study areas which may increase exposure of health information and improved mothers’ knowledge about infant and young child feeding.
In this study the proportion of mothers timely introduced complementary feeding for their children was 68.3% which is slightly consistent with a study conducted from Kenya (70%).17 But the finding was lower than the report from Debre Markos (84.7%)18 and it was higher than the report from southern Ethiopia (42%).16 This difference could be explained by better maternal education in which 82.2% of mothers in the current study versus 52.5% in the study from southern Ethiopia had formal education, and utilization of institutional delivery and improved living style depends on educational status.
As the logistic regression illustrated that the inappropriate MDD and MMF feeding was more likely practiced by respondents who did not know about MTCT of HIV, benefit of breast feeding and appropriate MDD and MMF feeding compared to mothers who had good knowledge. Many studies conducted in different countries revealed that mothers who had knowledge on optimal IYCF and prevention of mother-to-child transmission of HIV were more likely to feed their children appropriately than those who did not have knowledge.8,12,17
Minimum acceptable diet was negatively influenced by maternal workload. Mothers who had no workload are 62% less likely to practice inappropriate complementary feeding than those mothers who had a workload. This could be due to quality of the alternative child care or a relationship between poverty and the necessity of working much.
In addition, inappropriate MDD and MMF feeding was 54% less likely practiced among mothers who gain information about child feeding recommendations from health care providers as compared with those who did not gain the information. This is because mothers who had exposure to health information from health care providers and educational materials that might lead to avoiding inappropriate feeding practices. Complementary feeding counseling during critical periods of pregnancy, including antenatal care visits discourages inappropriate MDD and MMF and promotes appropriate and optimal child feeding practices. It may improve mothers’ knowledge and change negative culture which is the main fertile grounds to increase mothers’ confidence in challenging the community attitude towards inappropriate feeding practices which ultimately improves the likelihood of mothers’ adherence to optimal IYCF recommendations.
Conclusion
In conclusion, this study revealed that minimum acceptable diet (minimum dietary diversity and minimum meal frequency) were lower than the WHO recommendation for good practice of complementary feeding. Knowledge, maternal workload and information related to complementary feeding were associated factors with minimum acceptable diet of HIV-exposed children.
Limitations of the Study
The 24-h recall method may cause over-estimation of the proportion of complementary feeding practices due to recall and social desirability biases. In addition, respondents were asked retrospectively about breastfeeding practices so there may be recall bias which may affect the result. Even though we had sampled almost all HIV positive mother-child pairs in Debre Tabor town attending ART/PMTCT follow-up at public health facilities of Debre Tabor town, the study was underpowered with 287 participants interviewed.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; ART, antiretroviral therapy; CF, complementary feeding; CI, confidence interval; COR, crude odds ratio; HIV, Human Immunodeficiency Virus; IYCF, Infant and Young Child Feeding; MTCT, mother-to-child Transmission; PMTCT, prevention of mother-to -child Transmission; SPSS, Statistical Package for Social Science; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. The ethical approval and clearance for this study was obtained from Debre Tabor University College of Health Sciences Institutional Research Ethics Review Committee (IRERC). Support letter was written by IRERC with reference number of CHS/857/2019. A permission letter was received from the respective health facilities. Written informed consent was obtained from each study participant after explaining the purpose of the study. The right of a participant to withdraw from the study at any time, without any precondition was disclosed unequivocally. Moreover, the confidentiality of information obtained was guaranteed by all data collectors and investigators using code numbers and by keeping the questionnaire locked. Nutrition education and counseling were provided to all study participants after the data collection process is completed.
Acknowledgment
The authors would like to acknowledge, Debre Tabor Town Health office, data collectors and the respondents.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There was no financial support for this study.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Onyango AW, Borghi E, de Onis M, et al. Complementary feeding and attained linear growth among 6–23-month-old children. Public Health Nutr. 2014;17(9):1975–1983. doi:10.1017/S1368980013002401
2. MoHFDRo E. Infant and Young Child Feeding Quick Reference Book (0–24 Months). WHO. 2010.
3. Organization WH. Guideline Updates on HIV and Infant Feeding. WHO. 2016.
4. Organization WH. Guiding Principles for Feeding Non-Breastfed Children 6–24 Months of Age. World Health Organization; 2005.
5. UNICEF. Infant and Young Child Feeding, Nutrition Section Program. New York: UNICEF; 2012.
6. lexicon M. What is Malnutrition? What Causes Malnutrition, in Medical News Today. MNT. 2014.
7. Blössner M. Malnutrition: Quantifyingthe Impact at National and Local Leveles. Geneva: World health Organization; 2005:12.
8. Saha KK, Frongillo EA, Alam DS, et al. Appropriate infant feeding practices result in better growth of infants and young children in rural Bangladesh. Am J Clin Nutr. 2008;87(6):1852–1859. doi:10.1093/ajcn/87.6.1852
9. Behrman J, Alderman H, Hoddinott J. Hunger and malnutrition. Global Crises, Global Solutions. 2004:420.
10. Maluccio J, Moore C, Glassman A, et al. Breaking the Cycle of Poverty: Nicaraguan red de Protección Social. International Food Policy Research Institute brief (also available in Spanish); 2005.
11. Alemu A, Bezabih T. The Impacts of HIV/AIDS on Livelihoods and Food Security in Rural Ethiopia: Results from Household Survey in Four Regions. United Nations World Food Program (WFP; 2008.
12. Kimani-Murage EW, Norris SA, Pettifor JM, et al. Nutritional status and HIV in rural South African children. BMC Pediatr. 2011;11(1):23. doi:10.1186/1471-2431-11-23
13. Organization WH. Guidelines for an Integrated Approach to the Nutritional Care of HIV-Infected Children (6 Months–14 Years): Handbook, Chart Booklet and Guideline for Country Adaptation. Geneva: WHO; 2009.
14. Bayissa Z. Exclusive breast feeding status and its determinant among HIV positive women in West showa zone Oromia region Ethiopia. J AIDS Clin Res. 2017;8(1).
15. Organization WH. Strengthening Action to Improve Feeding of Infants and Young Children 6–23 Months of Age in Nutrition and Child Health Programmes: Report of Proceedings. Geneva: WHO. 2008.
16. Haile D, Belachew T, Berhanu G, et al. Complementary feeding practices and associated factors among HIV positive mothers in Southern Ethiopia. J Health Popul Nutr. 2015;34(1):5. doi:10.1186/s41043-015-0006-0
17. Wapang’ana G, Assessment of factors influencing infant feeding practices among HIV positive mothers in Rongo District, Western Kenya. MPH Thesis School of Public Health. Kenyatta University. 2013.
18. Wakwoya EB, Zewudie TA, Gebresilasie KZ. Infant feeding practice and associated factors among HIV positive mothers in Debre Markos Referral Hospital East Gojam zone, North West Ethiopia. Pan Afr Med J. 2016;24.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.