Back to Journals » International Journal of Women's Health » Volume 18
Mindfulness Meditation Combined with eCASH-Based Nursing for Cesarean Section in Preeclampsia: A Retrospective Study on Perioperative Pain and Recovery
Authors Zhang Y, Ji Y, Zhu L, Gu X, Liu J, Zhu J, Duan J
Received 5 September 2025
Accepted for publication 20 March 2026
Published 9 June 2026 Volume 2026:18 565522
DOI https://doi.org/10.2147/IJWH.S565522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Yan Zhang,* Ye Ji,* Liyan Zhu, Xin Gu, Jinling Liu, Jinmei Zhu, Jingrui Duan
Obstetrics Department, Wuxi People’s Hospital Affiliated to Nanjing Medical University, Wuxi, 214035, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingrui Duan, Email [email protected]
Objective: To evaluate the effects of mindfulness meditation combined with eCASH-based nursing on perioperative pain and early recovery in patients with preeclampsia undergoing cesarean section.
Methods: This retrospective study included 107 patients with preeclampsia who underwent cesarean section. According to the perioperative nursing intervention received, patients were assigned to a control group (n=53, conventional nursing) or a treatment group (n=54, conventional care plus mindfulness meditation and eCASH-based nursing). Outcomes included postoperative recovery indicators (time to first flatus, first bowel movement, and lactation onset), sleep quality (PSQI), pain intensity (NRS), comfort (GCQ), anxiety and depression (HAMA, HAMD), self-management ability (GESE, AHSMSRS), complication rates, and patient satisfaction.
Results: Compared with the control group, the treatment group demonstrated shorter times to first flatus, bowel movement, and lactation (P< 0.05). Post-intervention PSQI and NRS scores decreased and GCQ scores increased in both groups, with greater improvements in the treatment group (P< 0.05). Anxiety and depression scores were significantly reduced in both groups, with larger reductions in the treatment group (P< 0.05). Self-management scores improved significantly, particularly in the treatment group (P< 0.05). The complication rate was lower in the treatment group (7.41% vs. 22.64%, P< 0.05), and patient satisfaction was higher (96.30% vs. 77.36%, P< 0.05).
Conclusion: In this retrospective study, mindfulness meditation combined with eCASH-based nursing was associated with improved perioperative pain control, psychological status, early recovery, and patient satisfaction in preeclamptic women undergoing cesarean section. These findings are exploratory and warrant prospective validation.
Keywords: mindfulness meditation, eCASH, preeclampsia, cesarean section, perioperative nursing, pain management
Introduction
Preeclampsia is a pregnancy-specific hypertensive disorder occurring after 20 weeks of gestation and is characterized by hypertension and proteinuria or other signs of end-organ dysfunction.1 It remains a major contributor to maternal and perinatal morbidity worldwide. Due to maternal and fetal risks, cesarean section is frequently performed in women with preeclampsia, particularly in cases requiring timely termination of pregnancy. However, these patients often experience heightened perioperative stress, postoperative pain, sleep disturbances, and psychological vulnerability, which may delay recovery and adversely affect maternal–infant outcomes.2,3 Effective postoperative pain control after cesarean section is essential for early mobilization, breastfeeding initiation, and psychological recovery. Current pain management strategies include multimodal analgesia, patient-controlled analgesia (PCA), neuraxial opioids, and individualized analgesic regimens.4–6 Despite pharmacological advances, non-pharmacological interventions that address emotional distress and enhance patient engagement are increasingly recognized as important adjuncts in perioperative care.
Mindfulness meditation is a psychological intervention method aimed at reducing anxiety and stress, improving emotional regulation, and enhancing patients’ self-management abilities by focusing on present-moment awareness.7,8 The concept of eCASH (early Comfort using Analgesia, minimal Sedation, and maximal Human care) emphasizes a comprehensive patient-centered model that promotes early comfort, minimizes unnecessary sedation, and enhances humanistic care during medical procedures.9
In recent years, accumulating evidence has shown that both mindfulness-based interventions and comfort-centered perioperative care strategies can alleviate negative emotions, reduce pain perception, and improve comfort and self-efficacy in surgical patients.7–9 The combination of mindfulness meditation and eCASH-based nursing may exert synergistic effects. While eCASH optimizes physiological comfort and minimizes sedation-related adverse effects, mindfulness meditation may modulate pain perception, reduce anxiety, and enhance emotional self-regulation. Together, these approaches address both physiological and psychological dimensions of perioperative stress, potentially leading to more comprehensive recovery benefits than either strategy alone.
This study specifically focused on patients with preeclampsia because this population is characterized by increased perioperative risk, heightened psychological stress, and greater vulnerability to delayed recovery due to underlying vascular dysfunction and systemic involvement. Evaluating integrative nursing strategies in this high-risk obstetric group may provide clinically meaningful insights. In this retrospective study, pain control and early postoperative recovery indicators were defined as primary endpoints, while sleep quality, emotional status, self-management ability, complication rates, and patient satisfaction were considered secondary endpoints.
Subjects and Methods
Study Subjects
This study was designed as a retrospective observational study. A retrospective analysis was conducted on the clinical data of 107 patients with preeclampsia who underwent cesarean section in our hospital from April 2022 to April 2024. Ethical approval was obtained from the Medical Ethics Committee of our hospital (Approval No.: FCKLC-23HLBJ03). As this was a retrospective study based primarily on existing clinical records, the requirement for written informed consent was waived. However, all nursing interventions described in this study were part of routine clinical practice during the study period. For questionnaire-based assessments not routinely included in standard care, verbal informed consent was obtained from patients at the time of assessment.
Inclusion criteria: ① Meeting diagnostic criteria for preeclampsia10 and indications for cesarean section; ② Gestational age ≥37 weeks; ③ Singleton intrauterine pregnancy; ④ Complete clinical data available.
Exclusion criteria: ① Multiple pregnancies; ② Chronic hypertension diagnosed before pregnancy; ③ Severe organ dysfunction; ④ Severe immune, hematological diseases or infections; ⑤ Cognitive impairment or psychiatric disorders affecting questionnaire completion; ⑥ Incomplete data.
Patients were divided into a conventional nursing group (Control group, n=53) and a comprehensive nursing group (Observation group, n=54) according to the perioperative nursing model implemented during different clinical practice periods. The grouping was not based on individual patient selection but reflected ward-level nursing practice patterns at the time of hospitalization.
Methods
Control Group
Patients in the control group received routine perioperative nursing care according to the standard clinical protocol of our hospital. ① Health Education: Structured face-to-face health education sessions (approximately 20–30 minutes) were conducted by the responsible nurse upon admission. The content included the pathophysiology of preeclampsia, indications and necessity of cesarean section, perioperative precautions, postoperative recovery expectations, and breastfeeding guidance. Education was tailored to the patient’s educational background and cultural context. Written educational materials were provided to reinforce understanding and improve treatment adherence. ② Preoperative Preparation: Before surgery, nurses conducted a comprehensive physical and psychological assessment to ensure patients met surgical requirements. Patients were assisted with preoperative hygiene preparation and guided regarding fasting, medication adjustment, rest, and emotional stabilization to optimize surgical readiness. ③ Postoperative Care: After surgery, vital signs (blood pressure, heart rate, respiratory rate, oxygen saturation) were closely monitored. Uterine contraction, vaginal bleeding, incision status, and urine output were assessed regularly. Nurses provided dietary guidance to promote wound healing and gastrointestinal recovery and encouraged early mobilization (within 24 hours postoperatively when clinically appropriate) to reduce the risk of deep vein thrombosis and other complications. ④ Postpartum Recovery Guidance: Patients received standardized postpartum exercise instructions to promote pelvic floor muscle recovery and physical rehabilitation. Lactation guidance included demonstration of appropriate breastfeeding positions and techniques, troubleshooting of lactation difficulties, and emotional support to enhance maternal confidence and mother–infant bonding.
The duration of routine perioperative nursing care was 2 weeks.
Observation Group
In addition to routine nursing care, the observation group received mindfulness meditation combined with eCASH-based nursing interventions.
(1) Mindfulness Meditation Intervention: The mindfulness protocol was developed based on published literature and adapted to the obstetric perioperative setting.11,12 Implementation schedule: Initiated one day before cesarean section; Conducted once daily during hospitalization; Each session lasted approximately 20–30 minutes; Total intervention duration: 2 weeks. Supervision and training: The first 2–3 sessions were jointly supervised by a trained nurse and a psychologist to ensure proper technique acquisition. After demonstrating proficiency, patients were encouraged to perform guided self-practice with audio recordings provided by the clinical team. Intervention components included: ① Guided Meditation: In a quiet environment, patients lay comfortably with eyes closed and followed standardized verbal instructions. They were encouraged to focus on present-moment awareness and visualize calm and pleasant imagery. ② Progressive Muscle Relaxation: Patients sequentially tensed and relaxed major muscle groups (5–7 seconds tension followed by relaxation), proceeding from distal to proximal muscle groups to promote systemic relaxation. ③ Breathing Regulation: Patients practiced diaphragmatic and thoracic breathing exercises, maintaining a controlled respiratory rate of approximately 14–18 breaths per minute. ④ Attention Focusing: After mastering relaxation and breathing techniques, patients were instructed to focus attention on bodily sensations and breathing rhythm while reducing intrusive thoughts. ⑤ Self-Practice: Once familiar with the technique, patients were allowed to conduct independent practice sessions according to personal needs under periodic nursing supervision.
(2) eCASH-Based Nursing Intervention: The eCASH (early Comfort using Analgesia, minimal Sedation, and maximal Human care) approach was implemented as follows: ① Early Intervention and Self-Management Enhancement: Health education was reinforced throughout hospitalization to enhance disease understanding and coping ability. Preoperative pain tolerance and anxiety levels were assessed to facilitate individualized postoperative pain management. Early postoperative mobilization and functional exercises were encouraged. ② Minimal Sedation and Optimized Analgesia:Postoperative pain management followed a standardized multimodal analgesia protocol. Neuraxial opioid administration was used intraoperatively when indicated. Postoperatively, non-steroidal anti-inflammatory drugs (eg., flurbiprofen axetil 50–100 mg/day) and/or acetaminophen were administered as first-line agents. Additional rescue analgesics were provided when NRS ≥4. Sedative medications were minimized unless clinically necessary. Analgesic dosing was adjusted according to patient-reported pain intensity and clinical status. ③ Comfort Promotion: Psychological counseling was provided to reduce anxiety and sleep disturbance. Individualized dietary guidance was offered to support immune function and gastrointestinal recovery. Position adjustment, incision support, and gentle massage were applied when appropriate to alleviate discomfort. ④ Humanistic Care: Personalized care plans were developed based on individual patient characteristics. Non-verbal communication (therapeutic touch, eye contact, encouraging gestures) was used to enhance emotional support. Soothing music was provided before sleep when desired. Patient privacy and autonomy were respected throughout hospitalization.
Both groups received interventions for 2 weeks. After discharge, structured follow-up was conducted for 1 month via telephone or WeChat to reinforce healthy behaviors and monitor recovery progress.
Observation Indicators
(1) Postoperative Recovery: Including the time to first flatus (defined as the interval from completion of surgery to first passage of gas per rectum, reflecting gastrointestinal recovery), first defecation, and lactation. These indicators were uniformly recorded by the hospital’s medical staff.
(2) Sleep Quality: Assessed using the Pittsburgh Sleep Quality Index (PSQI)13 before and 2 weeks after the intervention (post-intervention). PSQI scores range from 0 to 21, with higher scores indicating poorer sleep quality.
(3) Pain: Assessed using the Numeric Rating Scale (NRS)14 before and 2 weeks after the intervention (post-intervention). NRS scores range from 0 to 10, with higher scores indicating greater pain intensity.
(4) Comfort Level: Assessed using the General Comfort Questionnaire (GCQ)15 before and 2 weeks after the intervention (post-intervention). GCQ scores range from 0 to 100, with higher scores indicating greater comfort.
(5) Negative Emotions: Assessed using the Hamilton Anxiety Scale (HAMA) and Hamilton Depression Scale (HAMD) before and 2 weeks after the intervention (post-intervention).16 HAMA scores range from 0 to 56, and HAMD scores range from 0 to 76, with higher scores indicating greater negative emotions.
(6) Self-Management Ability: Assessed using the General Self-Efficacy Scale (GSES)17 and the Adult Health Self-Management Scale (AHSMSRS)18 before and 2 weeks after the intervention (post-intervention). GSES scores range from 10 to 40, with higher scores indicating greater self-efficacy. AHSMSRS scores range from 38 to 190, with higher scores indicating greater self-management ability.
(7) Complication Incidence: This includes surgery-related complications (bleeding), anesthesia-related complications (nausea and vomiting, dizziness and headache, blood pressure abnormalities), postpartum complications (uterine atony, difficulties in lactation), and self-management deficiencies (poor compliance, cognitive and/or behavioral deficiencies in self-management). The incidence of these complications was uniformly recorded by the relevant medical staff at our hospital.
(8) Satisfaction: Assessed before discharge using a hospital-developed 19-item Satisfaction Evaluation Scale scored on a 5-point Likert scale. The internal consistency reliability of this scale in our institution demonstrated acceptable reliability (Cronbach’s α = 0.82). Total satisfaction rate was calculated as: (number of very satisfied + satisfied cases)/total cases × 100%.
Statistical Analysis
Graphs were plotted using GraphPad Prism 8 software, and data were processed using SPSS 22.0 software. Categorical data were expressed as percentages (%), analyzed using the chi-square test; continuous data were expressed as ( ), with independent sample t-tests used for between-group comparisons and paired t-tests for within-group comparisons. Given the retrospective observational design, multivariable linear regression (for continuous outcomes) and logistic regression (for binary outcomes such as complications) were conducted to adjust for potential confounders, including age, gestational age, parity, and baseline values of corresponding outcome measures. Confounders were selected based on clinical relevance. A two-sided P < 0.05 was considered statistically significant. Given the modest sample size and retrospective nature of the study, findings are interpreted as exploratory and hypothesis-generating rather than confirmatory.
), with independent sample t-tests used for between-group comparisons and paired t-tests for within-group comparisons. Given the retrospective observational design, multivariable linear regression (for continuous outcomes) and logistic regression (for binary outcomes such as complications) were conducted to adjust for potential confounders, including age, gestational age, parity, and baseline values of corresponding outcome measures. Confounders were selected based on clinical relevance. A two-sided P < 0.05 was considered statistically significant. Given the modest sample size and retrospective nature of the study, findings are interpreted as exploratory and hypothesis-generating rather than confirmatory.
Results
Comparison of General Data
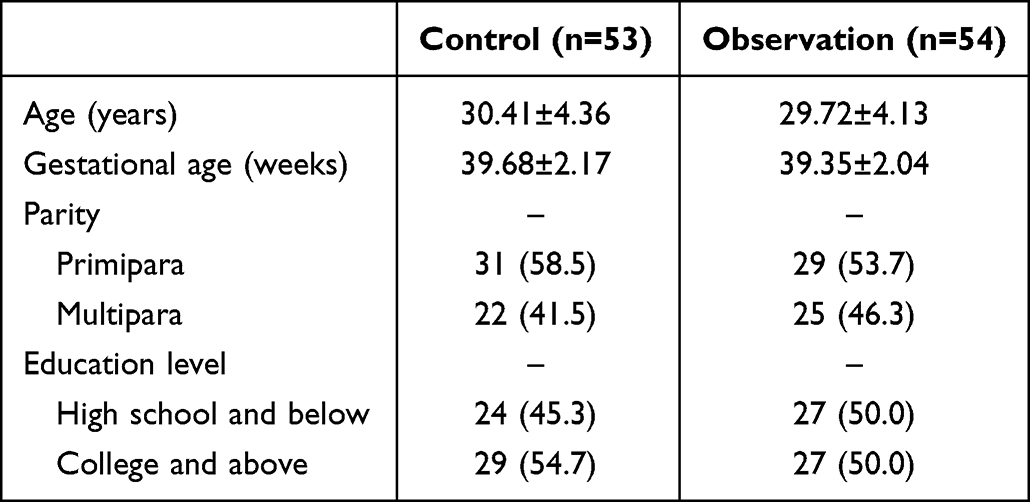
A total of 107 patients with preeclampsia undergoing cesarean section were included in the final analysis, including 53 patients in the control group and 54 patients in the observation group. The baseline characteristics of the two groups were generally comparable. The mean age was 30.41 ± 4.36 years in the control group and 29.72 ± 4.13 years in the observation group. The mean gestational age was 39.68 ± 2.17 weeks and 39.35 ± 2.04 weeks, respectively. In the control group, 58.5% were primiparas and 41.5% were multiparas, whereas in the observation group, 53.7% were primiparas and 46.3% were multiparas. Educational level distribution was also similar between groups. In accordance with reporting recommendations for observational studies, no statistical significance testing was performed for baseline characteristics. As shown in Table 1.
 |

Comparison of Postoperative Recovery
Postoperative recovery indicators, including time to first flatus, time to first defecation, and time to lactation onset, were compared between the two groups. The mean time to first flatus was 27.96 ± 5.31 h in the control group and 21.37 ± 4.45 h in the observation group, representing a mean difference of −6.59 h (95% CI: −8.46 to −4.72; P < 0.001). The mean time to first defecation was 45.47 ± 6.64 h in the control group and 34.16 ± 5.12 h in the observation group, corresponding to a mean difference of −11.31 h (95% CI: −13.42 to −9.20; P < 0.001). Similarly, the mean time to lactation onset was 26.49 ± 4.08 h in the control group compared with 18.27 ± 3.51 h in the observation group, yielding a mean difference of −8.22 h (95% CI: −9.73 to −6.71; P < 0.001). These findings indicate that patients receiving mindfulness meditation combined with eCASH-based nursing experienced significantly accelerated gastrointestinal recovery and earlier lactation initiation. As shown in Table 2.
 |

Comparison of Sleep Quality, Pain, and Comfort
Sleep quality, pain intensity, and comfort level were assessed before the intervention and 2 weeks after intervention. Both groups demonstrated improvement compared with baseline; however, improvements were more pronounced in the observation group. At 2 weeks post-intervention: The PSQI score decreased to a greater extent in the observation group compared with the control group, with a between-group mean difference of −2.14 points (95% CI: −3.02 to −1.26; P < 0.001), indicating better sleep quality. The NRS score was also significantly lower in the observation group, with a mean difference of −1.37 points (95% CI: −1.92 to −0.82; P < 0.001), reflecting improved pain control. In contrast, the GCQ score increased more substantially in the observation group, with a mean difference of 8.46 points (95% CI: 5.12 to 11.80; P < 0.001), suggesting enhanced overall comfort. These results suggest that the combined intervention not only improved physical recovery but also contributed to better subjective comfort and symptom control. As shown in Figure 1.
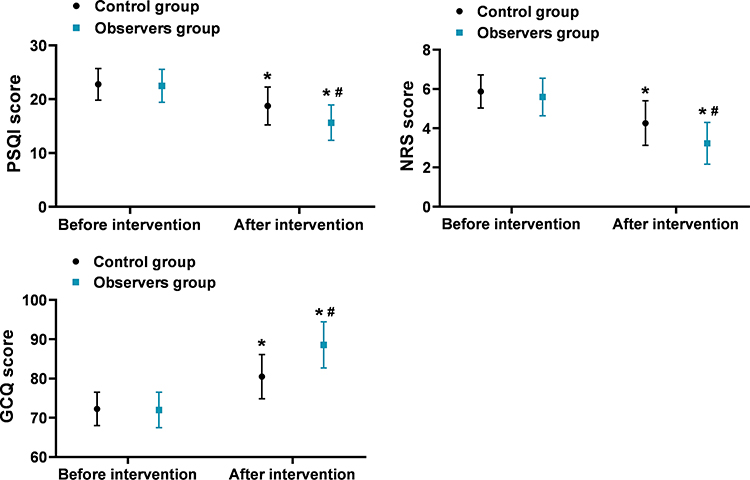 |
Figure 1 Comparison of Sleep Quality, Pain, and Comfort ( Note: Compared with before the intervention, *P<0.05; Comparison between groups, #P<0.05. |

Comparison of Negative Emotions
Anxiety and depressive symptoms were evaluated using the HAMA and HAMD scales. After 2 weeks of intervention, both groups showed reductions in HAMA and HAMD scores; however, reductions were significantly greater in the observation group. The mean between-group difference in HAMA score was −3.85 (95% CI: −5.12 to −2.58; P < 0.001). For HAMD, the mean difference was −4.11 (95% CI: −5.70 to −2.52; P < 0.001). These findings indicate that mindfulness meditation combined with eCASH-based nursing was associated with improved emotional regulation and reduced psychological distress during the perioperative period. As shown in Figure 2.
 |
Figure 2 Comparison of Negative Emotions ( Note: Compared with before the intervention, *P<0.05; Comparison between groups, #P<0.05. |

Comparison of Self-Management Ability
Self-management ability was evaluated using the GSES and AHSMSRS scales. At 2 weeks post-intervention, the observation group demonstrated significantly greater improvement. The mean difference in GSES score between groups was 4.32 points (95% CI: 2.91 to 5.73; P < 0.001), indicating enhanced self-efficacy. For AHSMSRS, the mean difference was 9.47 points (95% CI: 6.02 to 12.92; P < 0.001), suggesting improved health self-management capacity. These results indicate that the combined intervention may enhance patients’ confidence and active engagement in postoperative recovery. As shown in Figure 3.
 |
Figure 3 Comparison of Self-Management Ability ( Note: Compared with before the intervention, *P<0.05; Comparison between groups, #P<0.05. |

Comparison of Complication Incidence
During the observation period, patients could experience more than one type of complication; however, prevalence was defined as the proportion of patients experiencing at least one complication. In the control group, 12 of 53 patients (22.6%) experienced one or more complications. These included surgical complications (hemorrhage), anesthesia-related complications (nausea, vomiting, blood pressure abnormalities), postpartum complications (uterine atony, lactation difficulties), and self-management-related issues. In the observation group, 4 of 54 patients (7.4%) experienced at least one complication. The risk difference between groups was −15.2% (95% CI: −28.3% to −2.1%; P = 0.027), indicating a significantly lower complication prevalence in the observation group. As shown in Table 3.
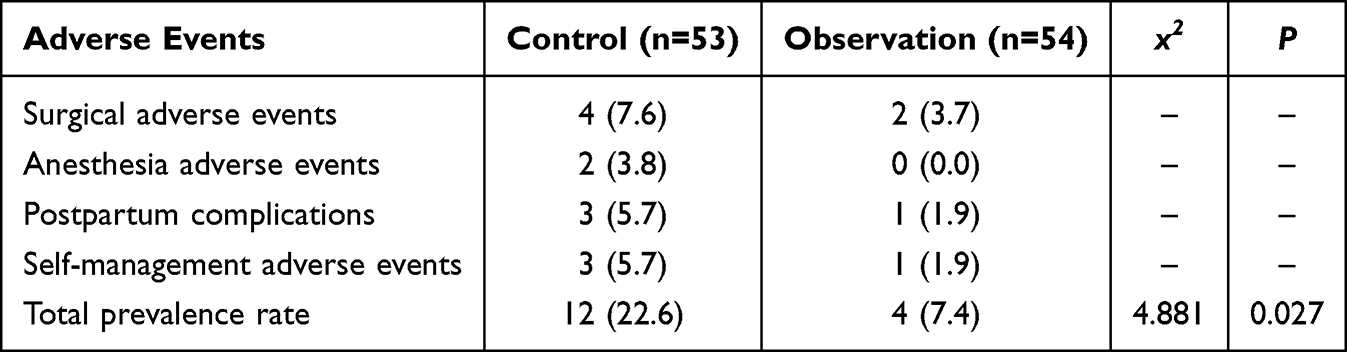 |
Table 3 Comparison of Complication Incidence [n(%)] |
Comparison of Satisfaction
Patient satisfaction was evaluated before discharge. In the control group, 41 of 53 patients were categorized as satisfied or very satisfied, yielding a total satisfaction rate of 77.4%. In the observation group, 52 of 54 patients were satisfied or very satisfied, corresponding to a total satisfaction rate of 96.3%. The between-group risk difference was 18.9% (95% CI: 6.2% to 31.6%; P = 0.003), indicating significantly higher satisfaction among patients receiving the combined intervention. As shown in Table 4.
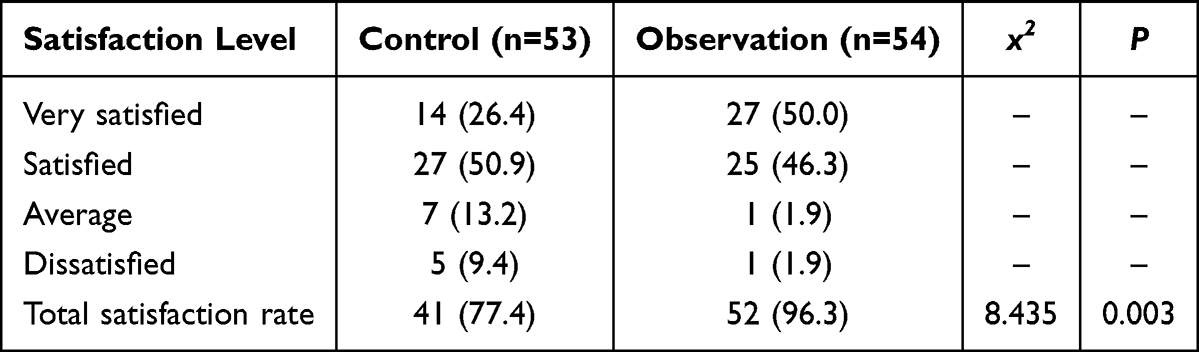 |
Table 4 Comparison of Satisfaction [n (%)] |
Discussion
Preeclampsia is a serious pregnancy-specific complication that not only threatens the life safety of pregnant women but also significantly impacts the growth and development of the fetus.19 According to global epidemiological data, the incidence of preeclampsia is approximately 2–8%, making it one of the leading causes of maternal and infant mortality during pregnancy.20 Although the exact etiology of preeclampsia is not fully understood, studies21 suggest that it may be related to various factors such as genetic predisposition, immune abnormalities, and endothelial dysfunction. Cesarean section is one of the common methods to manage preeclampsia, especially when the condition is severe or poses risks to the mother and baby. However, cesarean section is not without risks, and perioperative management is equally critical.22 Perioperative management includes interventions before, during, and after surgery, aiming to reduce the stress response induced by surgery, promote rapid recovery, and lower the incidence of complications. Traditional perioperative care models mainly focus on monitoring and maintaining physiological indicators, often neglecting the psychological needs and overall comfort of the patients. During postoperative recovery, pain management, sleep quality, and psychological state are crucial factors affecting the quality of patient recovery. Postoperative pain not only increases the physical burden on patients but can also lead to anxiety, depression, and other negative emotions, thereby affecting sleep quality and the speed of postoperative recovery.23 Studies24 indicate a significant correlation between postoperative pain and negative emotions, with severe pain associated with higher levels of anxiety and depression. Conversely, good sleep quality and a positive psychological state help alleviate postoperative pain, enhance patient comfort, and improve recovery outcomes. Against this backdrop, mindfulness meditation, as an effective psychological intervention method, guides patients to focus on the present and accept their emotions and feelings, effectively alleviating anxiety and depression, improving sleep quality, and aiding in pain management.25 Mindfulness meditation emphasizes non-judgmental attention to current experiences, helping patients cultivate a calm and accepting mindset, thereby reducing the impact of negative emotions. In recent years, accumulating evidence suggests that mindfulness-based interventions may also influence central pain processing pathways and autonomic nervous system activity, thereby reducing physiological stress responses and enhancing emotional regulation capacity.26 The eCASH concept, which stands for “early comfort and health recovery,” is a new nursing model emphasizing early intervention, comprehensive management, and personalized care.27 This concept advocates for early identification and intervention of potential issues, providing comprehensive comfort care to promote overall patient recovery. It highlights optimized analgesia, minimal sedation, early mobilization, and enhanced humanistic care, which together aim to improve both physiological recovery and patient experience. Although mindfulness meditation and the eCASH concept have been applied and studied in other medical fields,28–30 their specific effects in the perioperative care of cesarean section patients with preeclampsia have not been fully explored. Previous related studies31–33 have demonstrated that psychological interventions and structured comfort-based nursing can significantly improve perioperative outcomes, which is consistent with the findings of the present study.
Based on the above reasons, this study attempted to apply a combined nursing intervention of mindfulness meditation and the eCASH concept to the perioperative period of cesarean section for patients with preeclampsia. The results showed that the observation group had shorter times to first exhaust, first defecation, and lactation compared to the control group (P<0.05), suggesting accelerated gastrointestinal function recovery and earlier initiation of breastfeeding. Post-intervention scores for PSQI, NRS, HAMA, and HAMD were lower in the observation group than in the control group, while GCQ, GESE, and AHSMSRS scores were higher (P<0.05). These findings indicate that the combined intervention was associated with improvements in sleep quality, pain intensity, emotional status, comfort, and self-management ability. The prevalence of complications in the observation group (7.4%) was lower than that in the control group (22.6%) (P<0.05), and the nursing satisfaction rate was higher (96.3% vs. 77.4%) (P<0.05). It should be clarified that “promotion of recovery” in the present study specifically refers to earlier gastrointestinal recovery, earlier lactation onset, better pain control, improved psychological status, enhanced comfort, and strengthened self-management ability. From a clinical perspective, faster bowel recovery facilitates nutritional intake and mobilization, while improved emotional stability and pain control may enhance patient participation in rehabilitation. Although the differences observed were statistically significant, statistical significance does not necessarily equate to clinical significance. For example, a reduction of approximately one point on the NRS pain scale is generally considered clinically meaningful in postoperative care settings; therefore, the observed magnitude of pain reduction suggests potential practical relevance. Nevertheless, the minimal clinically important difference was not predefined in this study and warrants further investigation. The reasons for these findings may be analyzed as follows: (1) Mindfulness Meditation: ① Mindfulness meditation guides patients to focus on present experiences without judgment, accepting reality with a calm mindset, which may reduce maladaptive cognitive responses to pain and stress and alleviate anxiety and depression. ② The intervention emphasizes breathing regulation and body awareness, which may improve autonomic balance, reduce sympathetic overactivation, and attenuate the physiological stress response associated with surgery. ③ By enhancing emotional regulation and self-efficacy, mindfulness may indirectly promote adherence to postoperative rehabilitation and self-management behaviors. (2) eCASH Concept Nursing: ① eCASH emphasizes adequate analgesia with minimal sedation, which may reduce pain-related stress while avoiding excessive sedative effects. Through early comfort-oriented management, patients may experience reduced fear and improved cooperation. ② eCASH nursing promotes early postoperative mobilization and feeding based on patient condition, which may accelerate gastrointestinal recovery and reduce postoperative complications. ③ The strong humanistic component of eCASH enhances trust between patients and healthcare providers, increases satisfaction, and may improve compliance with medical advice.
However, several limitations should be acknowledged. First, this study adopted a retrospective and non-randomized design, which limits causal inference and may introduce information bias and selection bias. Second, subjective outcomes such as pain, sleep quality, emotional status, and satisfaction are susceptible to reporting bias, particularly in the absence of blinding. Third, the satisfaction scale was institution-developed and lacks external validation, which may influence the magnitude of observed differences. Fourth, multiple comparisons were conducted, which may increase the risk of type I error. Fifth, this was a single-center study with a relatively small sample size, and the population consisted of term preeclamptic patients undergoing cesarean section; therefore, the generalizability of the findings to other populations or healthcare settings may be limited. Cultural and institutional factors may also influence satisfaction and compliance.
Overall, the findings of this study reinforce the concept that psychological and comfort-oriented perioperative interventions may positively influence both psychological well-being and physical recovery. Although such integrative strategies are increasingly recognized in perioperative medicine, evidence in obstetric populations—especially among women with preeclampsia—remains relatively limited. Therefore, prospective, multicenter, randomized controlled trials are warranted to further validate these findings and explore long-term outcomes.
Conclusions
In conclusion, the combined application of mindfulness meditation and eCASH-based nursing in the perioperative management of cesarean section for patients with preeclampsia was associated with faster gastrointestinal recovery, earlier lactation initiation, improved pain control, better emotional status, enhanced self-management ability, lower complication prevalence, and higher patient satisfaction.
Given the retrospective observational design and modest sample size, these findings should be interpreted as exploratory and hypothesis-generating rather than definitive evidence of causality. Further prospective and randomized studies are needed to confirm the clinical effectiveness and broader applicability of this integrative nursing approach.
Funding
Soft Project of Wuxi Association for Science and Technology (KX-24-C158).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rana S, Lemoine E, Granger JP, et al. Preeclampsia: pathophysiology, challenges, and perspectives. Circ Res. 2019;124(7):1094–10. doi:10.1161/CIRCRESAHA.118.313276
2. Jung E, et al. The etiology of preeclampsia. Am J Obstet Gynecol. 2022;226(2s):S844–s866.
3. Sakowicz A, Bralewska M, Rybak-Krzyszkowska M, et al. New ideas for the prevention and treatment of preeclampsia and their molecular inspirations. Int J Mol Sci. 2023;24(15):12100. doi:10.3390/ijms241512100
4. Mostafa M, Hasanin A, Elsayad M. Post-cesarean delivery pain management. Pain Manag. 2021;11(3):243–254.
5. Bollag L, Lim G, Sultan P, et al. Society for Obstetric Anesthesia and Perinatology (SOAP) consensus statement on enhanced recovery after cesarean. Anesth Analg. 2021;132(5):1362–1377. doi:10.1213/ANE.0000000000005257
6. Lv S, Sun N, Hao C, et al. Development and validation of machine learning models for predicting post-cesarean pain and individualized pain management strategies: a multicenter study. BMC Anesthesiol. 2023;23:170. doi:10.1186/s12871-023-02143-8
7. Ngampramuan S, Cabanban R, Wang SS. The impact of mindfulness-based interventions on surgical patients: a systematic review. J Clin Med. 2022;11(9):2524. doi:10.3390/jcm11092524
8. Wielgosz J, Goldberg SB, Kral TRA, et al. Mindfulness meditation and psychopathology. Annu Rev Clin Psychol. 2019;15:285–316. doi:10.1146/annurev-clinpsy-021815-093423
9. Vincent JL, Shehabi Y, Walsh TS, et al. Comfort and patient-centred care without excessive sedation: the eCASH concept. Intensive Care Med. 2020;46(5):962–965.
10. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020;135(6):e237–e260.
11. Zollars I, Poirier TI, Pailden J. Effects of mindfulness meditation on mindfulness, mental well-being, and perceived stress. Curr Pharm Teach Learn. 2019;11(10):1022–1028.
12. Valluri J, Gorton K, Schmer C. Global Meditation Practices: a Literature Review. Holist Nurs Pract. 2024;38(1):32–40.
13. Zitser J, Allen IE, Falgàs N, et al. Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PLoS One. 2022;17(6):e0270095.
14. Shafshak TS, Elnemr R. The visual analogue scale versus numerical rating scale in measuring pain severity and predicting disability in low back pain. J Clin Rheumatol. 2021;27(7):282–285. doi:10.1097/RHU.0000000000001320
15. Li A, Du F, Jin Y, et al. Clinical evaluation of comfort nursing in gynecological patients undergoing laparoscopic surgery. Altern Ther Health Med. 2023;29(6):311–315.
16. Meng J, Du J, Diao X, et al. Effects of an evidence-based nursing intervention on prevention of anxiety and depression in the postpartum period. Stress Health. 2022;38(3):435–442. doi:10.1002/smi.3104
17. Poortaghi S, Baghernia A, Golzari SE, et al. The effect of home-based cardiac rehabilitation program on self efficacy of patients referred to cardiac rehabilitation center. BMC Res Notes. 2013;6:287. doi:10.1186/1756-0500-6-287
18. Ridosh MM, Stiles-Shields C, Stern A, et al. The adolescent/young adult self-management and independence scale (AMIS-II): expanding evidence for validity and reliability. J Pediatr Rehabil Med. 2021;14(4):583–596. doi:10.3233/PRM-200679
19. Ma’ayeh M, Costantine MM. Prevention of preeclampsia. Semin Fetal Neonatal Med. 2020;25(5):101123
20. Filipek A, Jurewicz E. [Preeclampsia - a disease of pregnant women]. Postepy Biochem. 2018;64(4) Danish
21. Overton E, Tobes D, Lee A. Preeclampsia diagnosis and management. Best Pract Res Clin Anaesthesiol. 2022;36(1):107–121.
22. Omani-Samani R, Ranjbaran M, Amini P, et al. Adverse maternal and neonatal outcomes in women with preeclampsia in Iran. J Matern Fetal Neonatal Med. 2019;32(2):212–216. doi:10.1080/14767058.2017.1376643
23. Sorabella LL, Bauchat JR. Enhanced Recovery after Surgery: cesarean Delivery. Anesthesiol Clin. 2021;39(4):743–760. doi:10.1016/j.anclin.2021.08.012
24. Veef E, Van de Velde M. Post-cesarean section analgesia. Best Pract Res Clin Anaesthesiol. 2022;36(1):83–88. doi:10.1016/j.bpa.2022.02.006
25. Schmidt H, Pilat C. Effects of Meditation on Pain Intensity, Physical Function, Quality of Life and Depression in Adults with Low Back Pain - a Systematic Review with Meta-Analysis. Vol. 72. Complement Ther Med; 2023:102924.
26. Paschali M, Lazaridou A, Sadora J, et al. Mindfulness-based interventions for chronic low back pain: a systematic review and meta-analysis. Clin J Pain. 2024;40(2):105–113. doi:10.1097/AJP.0000000000001173
27. Fu Q, Qiu Y, Xu Q, et al. eCASH concept-based care for patients with small-area burns: a pilot randomized controlled trial. Wounds. 2023;35(12):E439–e447. doi:10.25270/wnds/23058
28. Shi S, Wei J, Lyu G, et al. Application of comfort therapy under eCASH concept in acute and chronic wound treatment. Dermatol Ther. 2023;13(1):299–314. doi:10.1007/s13555-022-00852-5
29. Kral TRA, Schuyler BS, Mumford JA, et al. Impact of short- and long-term mindfulness meditation training on amygdala reactivity to emotional stimuli. Neuroimage. 2018;181:301–313. doi:10.1016/j.neuroimage.2018.07.013
30. Liang J, Tian XF, Yang W. Psychological care can reduce pain intensity, relieve negative emotions, and improve the quality of life of patients with advanced gastrointestinal cancer. J Mod Nurs Pract Res. 2021;1(1):6. doi:10.53964/jmnpr.2021006
31. Finan PH, Hunt C, Keaser ML, et al. Effects of savoring meditation on positive emotions and pain-related brain function: a mechanistic randomized controlled trial in people with rheumatoid arthritis. J Pain. 2024;25(7):104478. doi:10.1016/j.jpain.2024.01.343
32. Acevedo-Nuevo M, González-Gil MT, Romera-Ortega MÁ, et al. The early diagnosis and management of mixed delirium in a patient placed on ECMO and with difficult sedation: a case report. Intensive Crit Care Nurs. 2018;44:110–114. doi:10.1016/j.iccn.2017.07.013
33. Tan H, Ma X, Wang M. Effect of targeted nursing combined with psychological intervention on perioperative anxiety and postoperative complications in elderly cataract patients. J Mod Nurs Pract Res. 2021;1(2):7. doi:10.53964/jmnpr.2021007
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.