Back to Journals » International Journal of Women's Health » Volume 18
Midwifery Research Priorities in Saudi Arabia: A Priority-Setting Partnership Approach
Authors Abdulghani N ![]()
Received 9 January 2026
Accepted for publication 30 March 2026
Published 11 April 2026 Volume 2026:18 589957
DOI https://doi.org/10.2147/IJWH.S589957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Nawal Abdulghani
College of Nursing, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nawal Abdulghani, Email [email protected]; [email protected]
Objective: Research priority-setting supports efficient use of resources and strengthens the involvement of midwifery for high-quality, equitable maternity care. In Saudi Arabia, a recent transformation has expanded the midwifery role. However, no national stakeholder-driven midwifery research agenda has been developed. Therefore, the aim of the study is to identify and set midwifery research priorities for health care services in Saudi Arabia using a modified priority-setting partnership approach.
Methods: A mixed-methods design was utilized guided by the James Lind Alliance Priority-Setting Partnership framework. A steering group comprising clinicians and mothers codesigned the process. Purposive sampling was used to recruit midwives, nurses, obstetricians, and mothers from 10 out of the 13 Saudi regions. Individual interviews generated research uncertainties, which were analyzed using conventional inductive content analysis. A long list of topics were checked against existing evidence, then refined through interim ranking by the steering group. In a consensus workshop, clinicians and mothers used a structured nominal group technique and scoring system to reach consensus on the top-10 priorities.
Results: A total of 35 (27 clinicians and eight mothers) participated in the interviews. The analysis generated 230 research uncertainties, summarized into 33 topics, which were then shortened to 19. Through interim ranking and consensus, 10 research priorities were agreed on: (1) midwifery workforce and professional recognition, (2) maternal health and care practices, (3) neonatal and newborn care, (4) midwifery education and competency development, (5) cultural and community context, (6) special populations and high-risk groups, (7) integration of technology and innovation, (8) stakeholder and patient engagement in research, (9) health system and policy, and (10) emerging research directions.
Conclusion: To our knowledge, this is the first national stakeholder-driven midwifery research priority agenda in Saudi Arabia. The identified priorities offer a comprehensive and clear road map for researchers, investors, educators, and policymakers to align future midwifery research with areas of greatest perceived need and impact.
Keywords: midwifery, midwifery research, Saudi Arabia, research priority, priority-setting partnership
Objectives and Background
The International Code of Ethics for Midwives highlights that midwives use up-to-date, evidence-based professional knowledge to ensure safe birthing practices in all environments and cultures.1 Midwives should develop and share midwifery knowledge through a variety of processes, such as peer review and research.1 Research underpins high-quality health care and clinical excellence and is encouraged as a key driver for improving health services.2 Midwifery professionals play a vital role in maternal and child health care, making research in this area crucial to improving the quality of care provided to women and newborns.3 Midwifery research can shape health care system design, enhance the delivery of care, and support the advancement of professional practice.4,5 Moreover, such research helps identify evidence-based practices and interventions that can improve the health outcomes of mothers and newborns.3,6 Research also helps midwives to evaluate the quality of care they provide and identify areas for improvement as well as helping them identify best practices, develop guidelines, and implement evidence-based protocols that can enhance the overall quality of midwifery care.7–10 By generating high-quality evidence, research helps midwives make informed decisions about their practice, ensuring that the care they provide is based on the best available evidence rather than tradition or personal beliefs.3
In Saudi Arabia, a recent health transformation linked to Vision 2030 has expanded to the midwifery role through national scope of practice standards, competency frameworks, and service models. The Saudi Commission for Health Specialties has published a national scope of practice for nursing and midwifery care and clarifies regulatory expectations for registered midwives.9 In parallel, the Ministry of Health has introduced Saudi Midwifery Clinical Standards, the Saudi Birth Centre, Home Birth Standards, the national Baby-Friendly Hospital Initiative, and the Saudi Childbirth Initiative (SCI) Mother Baby-Family Friendly Maternity Care Facility (MBFMF) Initiative Guidebook, all aiming to standardize and improve the quality of midwifery-led care and promote continuity and respect for women’s autonomy across perinatal care.11–14
Despite these advances, there is a dearth of research in midwifery in Saudi Arabia. A national report on the midwifery workforce in Saudi Arabia highlighted difficulty obtaining precise workforce numbers and workforce shortages and maldistribution, raising demand for maternity services.15 Al-Shahrani16 conducted a critical analysis of midwives’ effect on maternal and neonatal health in Saudi Arabia. The analysis emphasized limited public and professional understanding of the midwife’s role, constrained autonomy, and variability in midwifery integration into the maternity team. These gaps in recognition, role clarity, and workforce planning risk undermining the effect of the national midwifery standards on maternal and neonatal outcomes.
Identifying a national research priorities assists health professionals to focus resources and efforts on addressing the most pressing issues for their consumers. The World Heath Organization recommends a transparent, participatory research priority–setting process as good practice, through systematic steps of planning, implementation, and evaluation, leading to legitimate and equitable health system requirements.17 Recently, the Saudi National Institute of Health published its Health Research Priorities Report, in which 17 areas are prioritized according to disease burden, health economics, innovative approaches for prevention, and early detection and diagnosis.18 However, there has been no national midwifery-specific research agenda developed using participatory methods in Saudi Arabia, highlighting the need to address this gap to support the implementation and evaluation of midwifery-led care.
The resulting priorities are intended to support decision-making by research funders and health authorities, inform policy and workforce planning, guide curriculum and clinical training reform, and assist maternity services translate midwifery-led models of care into measurable quality-improvement and evaluation programs.
The James Lind Alliance (JLA) Priority Setting Partnership (PSP) approach offers a robust framework to address this gap. The JLA is an initiative designed to unite health care professionals, patients, and caregivers in identifying and ranking key research questions.19 It describes a structure comprising seven steps, which include forming a steering group composed of both patient and clinician representatives. The process follows several stages to collect and refine research uncertainties, such as topics, questions, or focus areas, and ultimately establishes a list of the top-10 research priorities. The Priority Setting Partnership framework has been used in the nursing and midwifery fields, such as a study done in Australia that looked at nursing and midwifery research priorities for an Australian health service Janerka, Mellan.20 Another study done in the United Kingdom researched the top-10 priorities for diabetes in pregnancy according to women, support network, and health care professionals.21
In this study, the JLA PSP was adapted for feasibility and national reach in Saudi Arabia by using individual interviews to generate research uncertainties and a structured scoring process within a facilitated nominal group consensus workshop (rather than an open national survey). This modification was intended to maximize depth of insight, include bilingual participations and support engagement across geographically dispersed regions while maintaining the core PSP principals of transparency, clinicians and mothers partnership and explicit prioritization.
Given the rapid evolution of midwifery policy, persistent workforce, and role recognition challenges, it is crucial to determine midwifery research priorities for health care services in Saudi Arabia using a priority-setting partnership approach in conjunction with midwives, nurses, obstetricians, and mothers. This approach aligns with national and international standards for stakeholder involvement in research.17,22
The findings of this research will contribute to evidence-based practice and policy development in Saudi Arabia. To support a strong research agenda, health care services should identify priorities for midwifery research. Determining research priorities can assist in designing a clear road map to understand health service needs, direct resources, and support legitimate and translational research.23,24
The study aims to identify and set midwifery research priorities for health care services in Saudi Arabia. The research questions are as follows:
- What are the key gaps in midwifery practices in Saudi Arabia that require further research to improve service delivery?
- What research is needed to enhance culturally competent practices?
- Which specific maternal health outcomes in Saudi Arabia necessitate urgent midwifery research to reduce morbidity and mortality rates?
- What are the top-10 research priorities for midwifery in Saudi Arabia?
Methods
A mixed-methods designed was utilized in this study guided by a modified JLA PSP19 approach to determine the top-10 research priorities. This approach involved (1) formation of a steering group (consumers and clinicians); (2) an individual and group discussion with midwives, obstetricians, nurses, and mothers to identify research topics; (3, 4) summarizing and checking of research topics; (5) interim priority-setting; (6) a consensus workshop for final priority-setting using a modified nominal group technique; and (7) reporting, as shown in Figure 1.
 |
Figure 1 Study phases in accordance with the James Lind Alliance Priority Setting Partnership process. *Phase 2 has been modified according the nature of study. |
A purposive sampling method was used to ensure representation of diverse professions. The sample size was determined based on the saturation point in qualitative data collection and statistical power in quantitative analysis. The study participants were academics from different universities; clinicians in various health care settings (midwives, nurses, and obstetricians), including hospitals, clinics, and community health centers; and mothers from different regions in Saudi Arabia. The participants were from the following 10 regions in Saudi Arabia (in alphabetical order): Asir, Baha, Eastern Province, Jizan, Madinah, Makkah, Najran, Northern Border, Riyadh, and Tabuk.
Data were collected through individual interviews, surveys, and app usage analytics. Qualitative data were analyzed using inductive content analysis,25,26 and quantitative data were analyzed using descriptive statistics. In this paper, the quantitative data will be presented.
The study was guided by the JLA PSP framework as follows:
Phase 1: Formation of the Steering Group and Planning
A steering group was formed comprising two senior nurses and two senior midwives, all with expertise in both practice and academia, and two mothers who represented all the priority issues related to the priority-setting partnership. Participation in the steering group was voluntary. The steering group members agreed on the terms of reference, privacy, and interest statements and met to plan the research.
To support meaningful consumer involvement, steering group discussions used plain language summaries of each topic, equal speaking time, and facilitated clarification of technical terms. The consumers (mothers) were encouraged to challenge, merge, or rephrase topics to reflect lived experience. During prioritization, mothers votes carried the same weight as professional votes.
Phase 2: Gather Research Uncertainties (Interviews)
Phase 2 in this study has been modified according to the Saudi Arabian context and methods that are appropriate to obtain the required information. A decision was made in between the primary researcher and steering group to conduct individual interviews using open-ended questions to attain a comprehensive view of the midwifery research priorities in Saudi Arabia. The development of the interview questions was guided by JLA methods and those in similar studies.19,27 The semi-structured interview questions were designed to explore the research priority areas perceived by clinicians and consumers (Refer to Supplementary 1). The interview guide encompasses seven sections as follows: Section 1, background and experience, aims to capture the participants’ experience and role in maternal and neonatal services, duration of working experience, and area of practice and expertise. Section 2, identifying research gaps and needs, aims to detect the challenges facing the midwifery profession, practice, and education in Saudi Arabia and determine areas in maternal or neonatal care where more research is urgently needed. Section 3, cultural and contextual considerations, addresses research needed to improve culturally competent midwifery care in Saudi Arabia. Section 4, research outcomes and impacts, aims to identify maternal or neonatal health outcomes that require immediate research attention to reduce morbidity and mortality and which specific populations should be prioritized in midwifery research. Section 5, research prioritization, aims to identify crucial research topics by asking participants to identify and rank five topics for research perceived to have the greatest impact on the health system. Section 6, stakeholder engagement, explains strategies to ensure that research findings are translated into practice. Section 7 summarizes the final thoughts on midwifery research needs and gaps in Saudi Arabia.
The interview questions were reviewed by the steering group for face validity and iteratively amended, then pilot-tested for clearness and ease of understanding by the group before distribution. Following piloting, no substantial changes were required, and the same guide was used for all interviews.
The participants were recruited based on their experience and expertise. They agreed to participate in the study, and Participants Information Statement and consent forms were read and approved before they were interviewed. Participants were approached via Email and messaging applications through professional networks and social media, and those who expressed interest were contacted to schedule an interview. An online interview using the Microsoft Teams Insider program was conducted to obtain a wide distribution and convenience for participants. Interviews were conducted in English and Arabic (according to the participants’ preferences). The interviews were audio recorded with participants’ permission and then transcribed verbatim. Brief notes were taken during and after each interview to capture contextual information and initial impressions. Each interview lasted approximately 45 to 60 minutes. Recruitment and data collection continued until no new themes or topics were identified and the researcher agreed that data saturation had been reached. The data were collected during August and November 2025.
For interviews conducted in Arabic, transcripts were translated into English for synthesis. A bilingual reviewer checked translations for conceptual equivalence and a subset underwent back-translation to confirm accuracy of meaning for priority statement used in ranking.
The inclusion criteria for participants were clinicians who were registered nurses, midwives, or obstetricians and worked at the health service. Consumers (mothers) were eligible to participate if they were 18 years old, able to communicate in English and Arabic, and had been to the health service in the past 2 years. Two clinicians decided not to participate before being interviewed because they were not interested in midwifery research.
Phase 3: Summarize Research Uncertainties
The qualitative data from the interviews were analyzed and summarized using a conventional, inductive content analysis technique25,26 to identify research uncertainties (topics). The researcher coded the interviews, and an independent transcriber reviewed the codes against raw data and agreed on the framework stages, with any disagreement resolved through discussion.
A systematic method was undertaken to analyze the data. First, the interviews were transcribed according to the language that was used in the interview. Second, the interviews were read several times to get a general sense of the content, and transcripts were coded to capture key thoughts and concepts related to crucial midwifery research topics in Saudi Arabia. Third, all codes were translated to English and checked by an independent transcriber. Fourth, codes with shared conceptual content were sorted into a long list of broad content areas and subsequently abstracted into categories of themes, starting with the most frequently occurring codes. A coding tree was developed to document the relation between codes, subcategories, and overarching themes and was iteratively refined throughout the analysis. Fifth, definitions for each theme were created with exemplar codes. The final themes were reviewed for clarification by an independent transcriber. Sixth, the content of each category was checked and validated against the original data by the independent transcriber. Qualitative data were organized and managed using Excel spreadsheets and coded manually to support systematic retrieval.
Phase 4: Check Research Uncertainties
The research steering group compared the long list of topics against existing literature and ongoing studies at the health service and removed any that were no longer valid. This step was carried out in parallel with the interim priority-setting (Phase 5).
Phase 5: Interim Priority-Setting
The long list of research topics with exemplar codes was circulated to the steering group for the interim priority-setting process. Steering group members were requested to (1) review the topics and comments for clarity and relevance to the health service and (2) select and rank their top-10 topics. Ranking data were entered and analyzed in an Excel spreadsheet; topics ranked number 1 received the highest score (10), and those ranked number 10 scored the lowest (1). Overall scores were then summed for each topic, which were then ordered according to their total scores. Based on the steering group’s feedback, ranking, and the validation steps from Phase 4, some topics were refined or removed. A final short list of topics was then agreed upon for progression to the next phase.
A 10–1 weighting was selected to provide a simple, transparent ranked-choice scoring approach that preserves ordinal preference while allowing aggregation across participants. Given the consensus-oriented aim, small score differences were interpreted cautiously and final ordering was confirmed through workshop discussions.
Phase 6: Final Priority-Setting (Consensus Workshop)
The short list of research topics, together with their interim ranking, number of survey responses, and exemplar codes, was presented at a consensus workshop. A random sample of mothers and clinicians were recruited from participants of the interview (Phase 2) and the steering group. During the workshop, participants engaged in structured group discussion to review, debate, and re-rank the topics. The results of Phases 5 and 6 were then combined, scores were calculated, and topics were re-ordered according to the highest score. The final ranking was agreed on, and the top-10 research priorities were identified.
To reduce the risk of dominance effects, the workshop used trained facilitation, structured turn-taking and small-group discussion before plenary re-ranking. All participants were invited to comment on each topic, and agreement was checked before finalizing the ranked list.
Phase 7: Dissemination of Results
Reports and presentations will be used to disseminate the findings of the study to the designated authorities responsible for midwifery in Saudi Arabia. The dissemination of the findings will be achieved through journal publication and conference presentations and posters. The identified priorities are intended to be embedded into strategic planning for midwifery research across the health service, guiding the alignment of existing projects and incentivizing future work. They will also serve as the basis for formulating specific research questions in partnership with researchers and funding bodies. The progress and relevance of these priorities will be reviewed in 5 years.
Ethical Considerations
Ethical approval for the study was granted by the Biomedical Research Ethics Committee at Umm Al-Qura University (HAPO-02-K-012-2025-06-2849). Participants were provided with a participant information sheet and gave informed consent prior to the interview. The data collected were nonidentifiable. Participation as a steering group member or workshop participant was voluntary. Participants were informed that they could withdraw at any time without consequence and that all data would be anonymized during transcription and analysis to protect confidentiality. All the data collected and transcripts were stored in electronic files protected by passcodes to ensure the privacy and confidentiality of the data.
Rigor and Trustworthiness
The rigor and trustworthiness of the qualitative component were enhanced through multiple, complementary strategies.28,29 Credibility was supported by purposive sampling of diverse clinicians and mothers from different regions and the use of semi-structured interviews and an iterative approach in which emerging ideas were further explored and then checked with the steering group. Dependability and confirmability were strengthened by maintaining a clear audit trail of interview guides, filed notes, coding frameworks, and analytical decisions; applying inductive content analysis to derive themes; and having an external reviewer independently check codes and themes against the raw data. The involvement of two coders, the author, and the independent transcriber during the early coding stages, followed by regular analytics meetings, further supported dependability and reduced individual bias. Transferability was addressed by providing a rich description of the study setting, participants, sampling strategy, and the midwifery context in Saudi Arabia so that researchers can judge the applicability of the findings. Reflexivity was assured by the author because she is a female midwife and academic with extensive experience in midwifery practice, education, and qualitative research. Participants were informed that the interviewer was a midwife academic interested in improving midwifery services nationally and that there were no direct clinical, managerial, or assessment relationships with her. Reflexivity was also promoted by the author in keeping a reflexive journal; using open, nonleading questions; and sharing interpretation and prioritization with multidisciplinary steering group and workshop participants to minimize individual bias. The qualitive component is reported in accordance with COREQ (Consolidated Criteria for Reporting Qualitative Research).
Results
The Interview
The interview guides were organized into six sections: (1) background and experience, (2) identifying gaps and needs, (3) cultural and contextual considerations, (4) outcomes and impacts, (5) research prioritization, and (6) stakeholder engagement (7) summarizes the final thoughts on midwifery research needs and gaps in Saudi Arabia.
A purposive sampling approach was used to recruit the interview participants to capture diverse, information-rich perspectives of midwifery research priorities. Table 1 presents the characteristics of the interviewed participants. A total of 35 participants were interviewed, including clinicians and consumers. The clinicians were obstetricians, midwives, and nurses, and participants were predominately female for both clinicians (81%) and consumers (100%). Among the clinicians, a large number of participants were midwives (59.3%), followed by obstetricians (22.2%) and nurses (18.5%). The majority of clinician and consumer participants were Saudi (77.7%). The clinicians’ years of practical experience clustered in the mid-career bands of 11 to 20 years (63%) with fewer being early career (3.7%) or very senior with more than 26 years of experience (7.45%). The interview participants represented 10 out of the 13 regions in Saudi Arabia, with the largest shares from Makkah (31.4%), Riyadh (20%), and Madinah (17%). Fewer contributions came from the Eastern Region (8.6%), Baha (5.7%), and Tabuk (5.7%), and Asir, Jizan, Najran, and Northern Border had one participant each (2.9%).
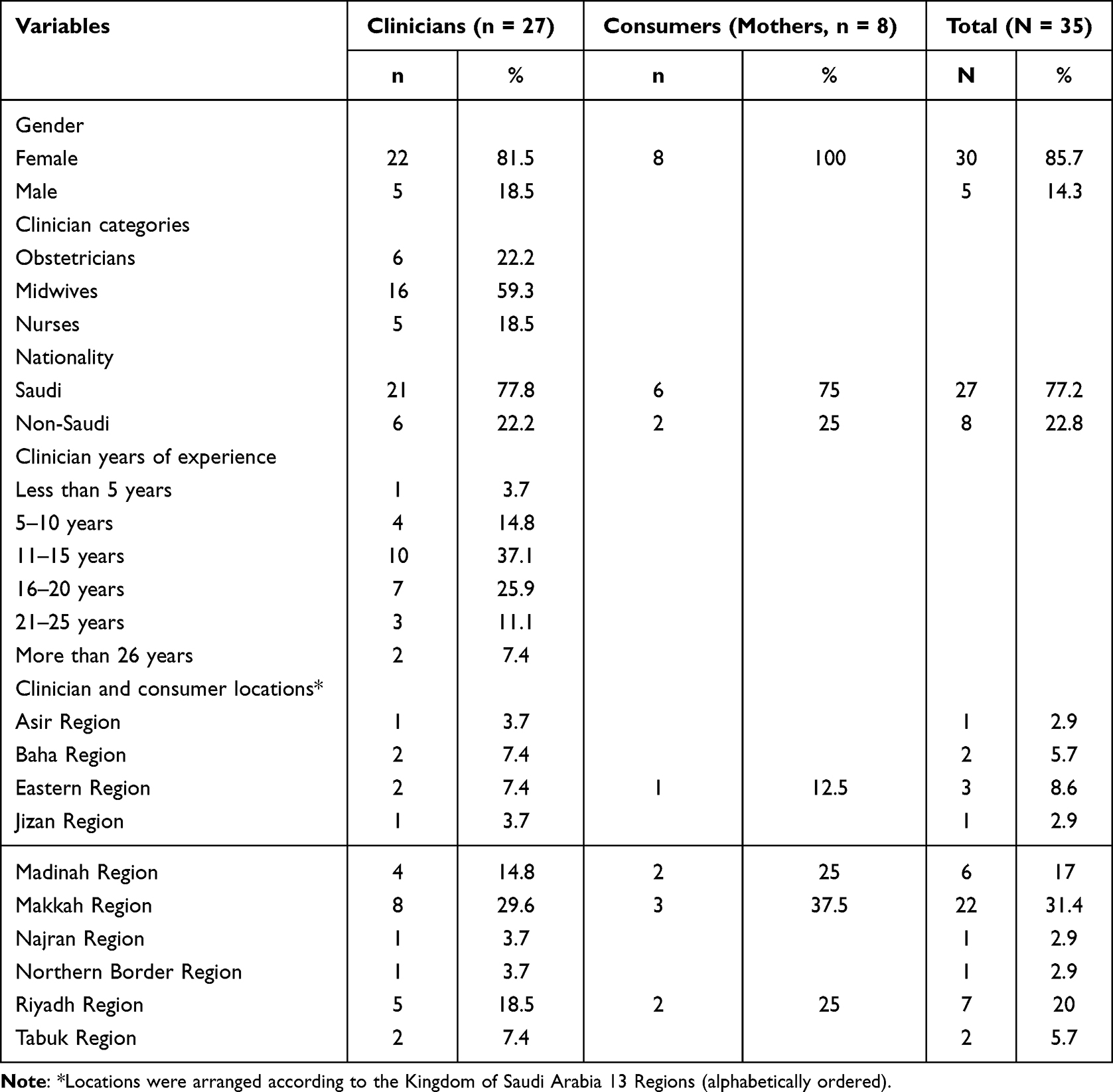 |
Table 1 Characteristics of the Interviewed Participants (N = 35) |
Participants were not recruited from three regions; therefore, priorities may underrepresent needs specific to those areas, particularly remote or smaller services. This is addressed as transferability limitation and recommends targeted follow-up engagement in future updates.
Figure 2 depicts a staged priority-setting pathway adapted from the James Lind Alliance19 approach. Interview transcripts were coded inductively. The interview guide questions from Sections 2 to 6 generated 230 topics or areas related to priorities in midwifery research in Saudi Arabia, from which 33 themes emerged to form the long list. The long list was further summarized into an interim ranking of 19 research topics (short list), from which 14 topics were unanimously agreement upon at the consensus workshop. Attended by senior nurses, midwives, and consumers, the consensus workshop used a point system (rank 1 = 10 points, rank 10 = 1 point), from which a total score was determined.
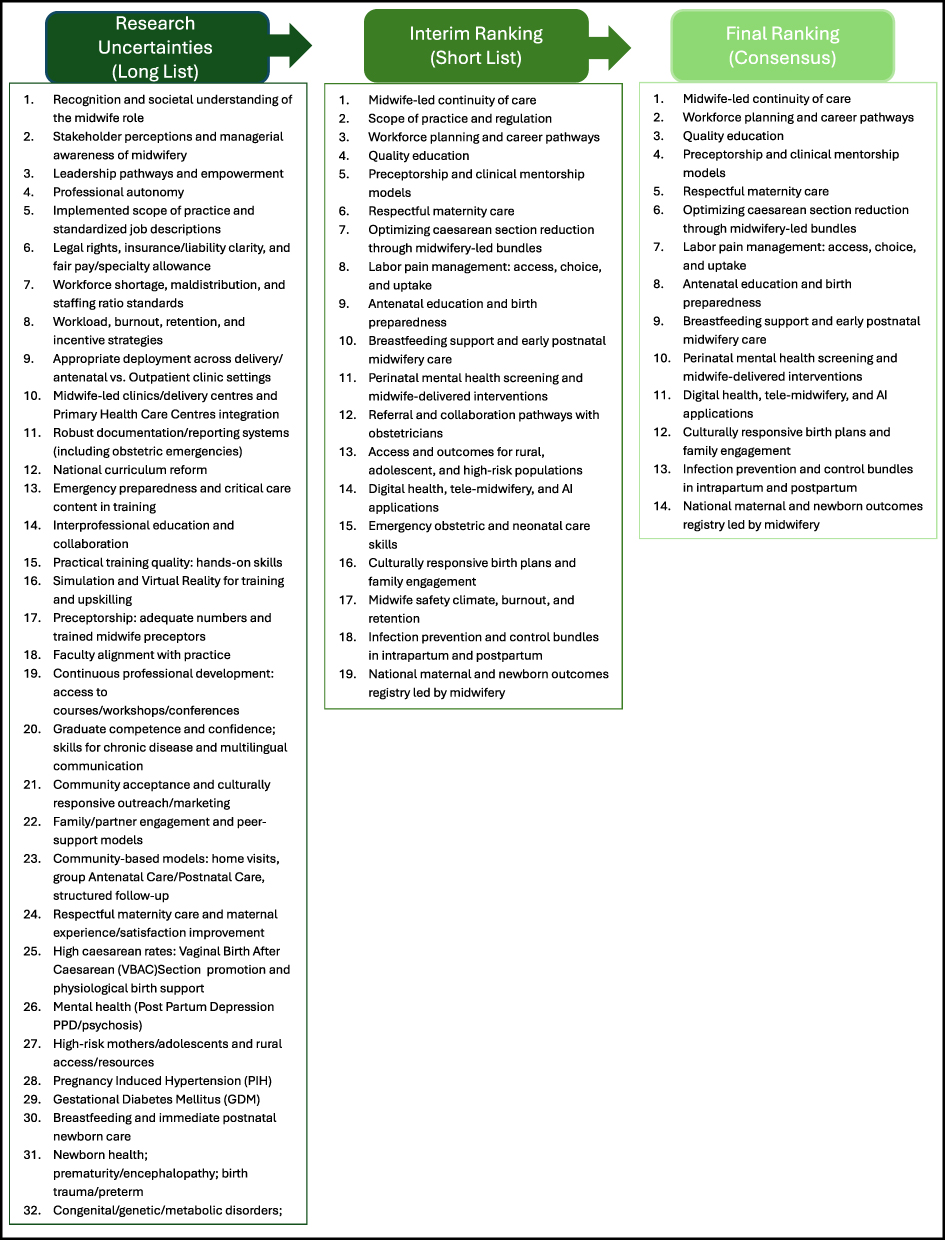 |
Figure 2 Initial midwifery research topics and ranking process. |
After structured group discussions, topics were re-ranked using the same scoring system, and the top-10 priorities were agreed upon consensus.
Table 2 presents the top-10 research priorities in midwifery research in Saudi Arabia. The ranking sheds light on the importance of the midwifery workforce and professional recognition, maternal and neonatal care, competency-based education, culturally responsive models, equitable access for high-risk groups, digital health, and enabling health system and policy research, all of which are perceived as critical areas to improve maternity and midwifery outcomes in Saudi Arabia.
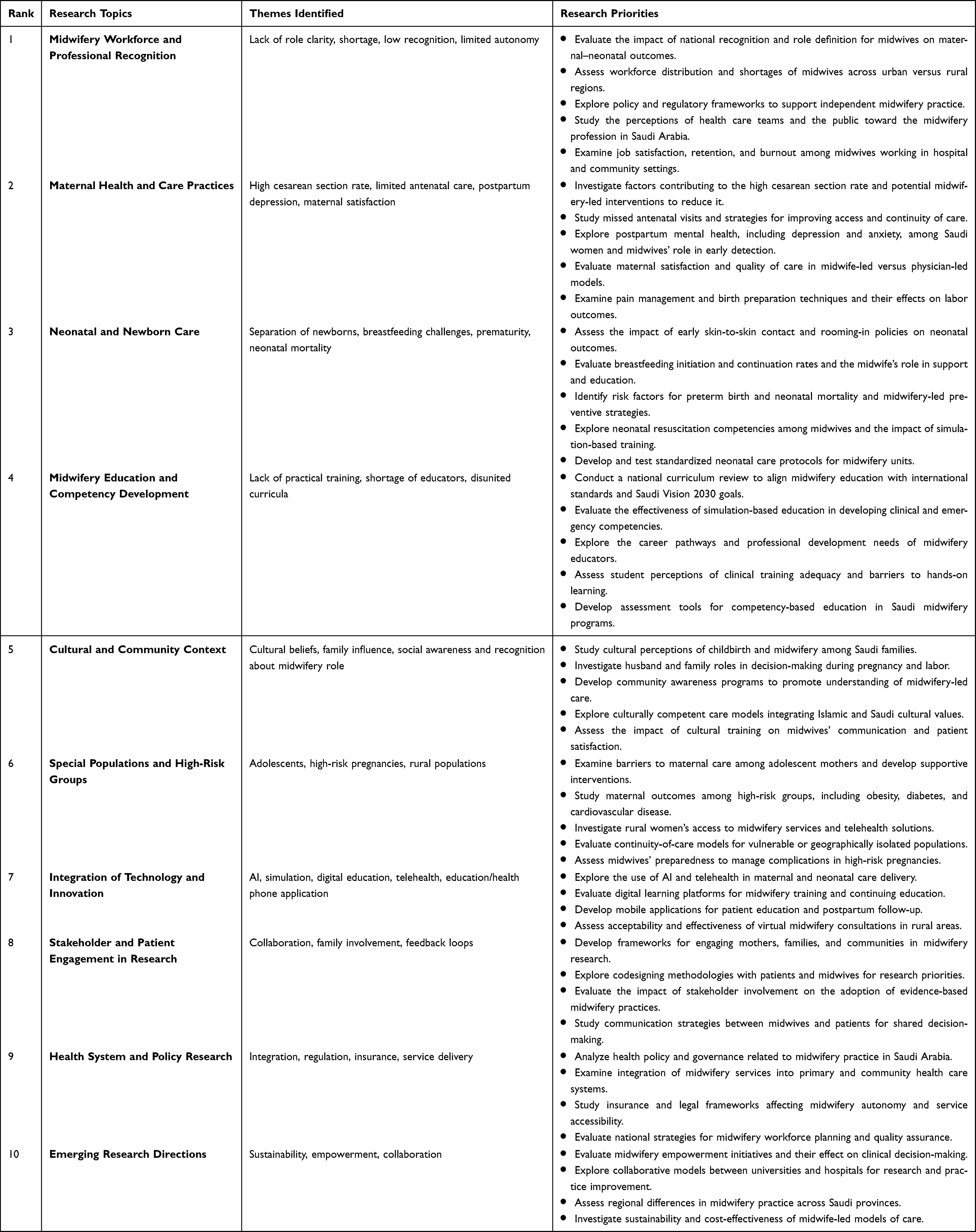 |
Table 2 Top-10 Research Priorities |
The top-10 priority-setting partnership approach shaped the final ranking converged into workforce, clinical care, education, community context, vulnerable populations, technology, engagement, and policy.
The top priority was midwifery workforce and professional recognition, emphasizing role definition, fair regulation and autonomy, maldistribution/shortage, retention and burnout, and public and interprofessional understanding of midwifery. Proposed studies include evaluating national recognition policies, mapping workforce gaps, and assessing job satisfaction and burnout. The second research priority topic was maternal health and care practices, targeting high cesarean rates, missed antenatal care, postpartum mental health, maternal satisfaction, and pain management. Recommended work includes evaluating midwifery-led intervention for cesarean reduction and evaluating model-of-care quality and birth-preparation strategies.
Neonatal and newborn care ranked third, prioritizing skin-to-skin contact and rooming-in, breastfeeding support, prematurity and neonatal mortality prevention, resuscitation competencies, and standardized neonatal protocols. The fourth topic was midwifery education and competency development, which called for a national curriculum review aligned with international standards and Vision 2030, robust simulation for emergency skills, clearer educator pathways, and competency-based assessment tools. The fifth topic, cultural and community context, prioritized research on cultural beliefs, family decision-making, community awareness of midwife-led care, culturally competent models, and communication training. The sixth topic, special populations and high-risk groups, focused on adolescents, high-risk pregnancies (eg, obesity, diabetes, Cardiovascular diseases), rural access, continuity-of-care model, and midwives’ preparedness for complications. The seventh topic, integration of technology and innovation, highlighted AI, tele-midwifery health, digital learning, and patient-facing mobile applications, including virtual consultations, especially for rural settings.
The eighth topic, stakeholder and patient engagement in research, advanced codesigning of research with mothers and midwives, building frameworks for collaboration and engagement, and evaluating how involvement accelerates uptake of evidence-based practices and shared decision-making. The ninth topic, health system and policy research, included integration of midwifery into primary/community care and building legal/insurance frameworks that support autonomy and national workforce planning and quality assurance. The 10th and final topic, emerging research directions, emphasized empowerment and leadership, university–hospital research collaboration, regional practice variation, and sustainability and cost-effectiveness of midwife-led models.
Discussion
The priority-setting partnership framework was the lens used to identify the top-10 midwifery research topics in Saudi Arabia. Partnering with consumers and clinicians in the research helped to determine research priorities of direct relevance to health care services that align with national and international standards for stakeholder involvement in research. By systematically engaging clinicians and consumers from multiple regions and practice settings, the findings provide context-specific research topics that reflect the realities of midwifery practice, education, policy, and delivery in the Saudi context.
Consistent with international evidence, the top priority area from participants was the midwifery workforce and professional recognition. The State of the World’s Midwifery6 report has demonstrated that scaling up midwifery-led care and evidence-based interventions could avert a substantial proportion of maternal and neonatal deaths and stillbirths. However, this potential outcome would not be achieved in settings where there are few midwives and they are poorly recognized or constrained in scope of practice. The study findings are in agreement with other studies conducted in Saudi Arabia15,16 emphasized on the underscore the workforce planning, retention strategies, and policies that support midwives’ autonomy and fair compensation are fundamental issues for the midwifery profession in Saudi Arabia.
Maternal health and care practices and neonatal care are among the top-priority research topics according to the research findings. The Lancet Global Health article has shown that midwifery-led models of care are associated with reduced unnecessary interventions, including cesarean sections, and improved maternal satisfaction and newborn outcomes.3 The priority of research on midwifery-led bundles, including cesarean sections,30–32 missed antenatal visits,33 early skin-to-skin contact,34–38 rooming-in policies and breastfeeding challenges,39,40 and postpartum mental health,41–43 indicates an urgent need for intervention studies that investigate the midwifery profession and address these challenges in Saudi Arabia. While our pervious research project36,38 examined health care provider’s, mother perceived barriers and facilitators to implement skin-to-skin contact in Saudi Arabia, the present study addresses a different project aim to establish national midwifery research priority agenda. This study is novel in applying a priority-setting partnership approach to generate a ranked set of national midwifery research priorities informed by both clinicians and consumers.
Midwifery education and competency development had a high ranking, reflecting concerns about curriculum alignment, adequacy of clinical training, and availability of qualified educators. These results are consistent with those of regional Delphi studies in nursing and midwifery, which have repeatedly identified workforce capability and education as core research domains.43–47 Participants in this study called for a national curriculum review against international standards and Vision 2030, robust simulation-based education, and competency-based assessments.
The cultural and community context, where family and religious values shape maternity experiences, was ranked as a research priority to improve midwifery practice in Saudi Arabia. Similar work from Saudi Arabia and the Eastern Mediterranean region has shown that culturally responsive care and family involvement are central to women’s preferences and satisfaction.44,48 Evidence from Saudi Arabia shows that women’s experiences of shared decision-making often involve husbands and family members, indicating a need to evaluate decision-support approaches that protect women’s autonomy while acknowledging family participation.49 Moreover, Saudi studies in respectful maternity care highlight that dignity, communication, and consent are strongly associated with women’s satisfaction and vary across health care sectors and specific interventions that align respectful care with socio-religious norms.48
Midwifery research in Saudi Arabia must generate locally grounded insights on the integration of midwifery-led care embedded in Saudi culture and religious norms.
The inclusion of technology and innovation, particularly AI, telehealth in midwifery and maternity, digital learning, and mobile applications, demonstrates a forward-looking approach in the profession. Internationally, digital health interventions in maternal and newborn care are growing quickly to accommodate the geographically dispersed populations and are aligned with global inclusion of digital innovations.50
This study has several strengths. It used a structured, transparent framework; integrated qualitive and quantitative data; and included participants from different professions covering 10 out of the 13 regions of Saudi Arabia, thereby capturing a wide range of maternity and midwifery perspectives and experiences. The iterative process of coding, validation, and consensus workshops enhanced the credibility of the final top-10 list.
The purposive sampling approach, while appropriate for depth and diversity, may have introduced selection bias; clinicians and mothers with a particular interest in midwifery or research may have been more likely to participate. Participants from some regions were underrepresented, which may limit the generalizability of the findings by regions and would be recommended for future engagement.
Despite these limitations, the identified priorities for midwifery offer a pragmatic, comprehensive, endorsed road map for stakeholders, academics, health professionals, health institutions, and health services. Future research should translate these topics into specific, fundable research and evaluate the impact of the research on maternal and neonatal outcomes. By aligning midwifery research with national health and Vision 2030 reforms, this study provides a critical step toward strengthening midwifery’s contribution to high-quality, equitable maternity care in Saudi Arabia.
The operational next steps include translating each priority domain into specific, fundable research questions with defined populations, outcomes, and study designs; mapping priorities to reasonable stakeholders (eg, Ministry of Health, Saudi Commission for Health Specialties, universities, and maternity service leaders); and establishing a national midwifery research implementation plan with annual reporting. A planned 5-year review repeat the prioritization steps with refreshed stakeholder sampling, track indicators such as funded projects aligned to priorities, publications, implementations of midwifery-led models and selected maternal-newborn outcome metrics and update the ranked list accordingly.
Conclusion
This study is the first, to our knowledge, to utilize a modified James Lind Alliance Priority Setting Partnership to identify national midwifery research priorities for health care services in Saudi Arabia. Bringing together midwives, nurses, obstetricians, academics, clinicians, and mothers from multiple regions, the study generated a stakeholder-driven, context-specific agenda.
The resulting top-10 priorities converged overarching the following domains: midwifery workforce and professional recognition, maternal health and care practices, neonatal and newborn care, midwifery education and competency development, community and cultural context, equity for high-risk and underserved populations, technology and digital innovation, health system and policy leadership, and emerging directions. The identified research topics offer a practical road map for researchers, funders, educational institutions, and policymakers to align future projects, capacity-building, and investment in areas of greatest perceived need and impact. By involving both clinicians and consumers in the research process, the study creates a valuable tool to address the unique needs of midwives and health care consumers and guide future midwifery research to improve health care delivery and outcomes, in alignment with Saudi Vision 2023’s priorities for strengthening health system quality, patient-centered care, and workforce development.
Disclosure
The author reports no conflicts of interest in this work.
References
1. International Confederation of Midwives (ICM). International code of ethics for midwives. 2014.
2. Hanney SR, González-Block MA. Health research improves healthcare: now we have the evidence and the chance to help the WHO spread such benefits globally. Health Res Policy Syst. 2015;13(1):12. doi:10.1186/s12961-015-0006-y
3. Nove A, Friberg IK, De Bernis L, et al. Potential impact of midwives in preventing and reducing maternal and neonatal mortality and stillbirths: a lives saved tool modelling study. Lancet Glob Health. 2021;9(1):e24–15. doi:10.1016/S2214-109X(20)30397-1
4. Bridges J, Harris R, Maben J, Arthur A. Research that supports nursing teams 1: how research can improve patient care and nurse wellbeing. Nurs Times. 2020;116(10):23–25.
5. Erickson JI, Pappas S. The value of nursing research. JONA. 2020;50(5):243–244. doi:10.1097/NNA.0000000000000876
6. UNFPA, WHO, ICM. The State of the World’s Midwifery 2021. 2021.
7. Grigoletto V. Evidence-based practice in midwifery: bridging research with clinical care. J Nurs Care. 2025;694.
8. Elzeblawy HH. Evidence-based practice in midwifery and maternity nursing for excellent quality of care outcomes. Am J Nurs. 2020;8(6):606–607.
9. Saudi Commission for Health Specialties (SCFHS). The Scope of Nursing and Midwifery Practice in Saudi Arabia. 2024.
10. Shadap A. Evidence based practice in midwifery care. Int J Obstet Gynaecol Nurs. 2022;4:01–4. doi:10.33545/26642298.2022.v4.i1a.75
11. Ministry of Health (MOH). Saudi Midwifery Clinic Standards. Midwifery Department, editor. 2021.
12. Ministry of Health (MOH). The Saudi Birth Centre Standards. Midwifery Department, editor. 2021.
13. Ministry of Health (MOH). The Saudi Home Birth Standards. Midwifery Department, editor. 2021.
14. Ministry of Health (MOH). Saudi Childbirth Initiative (SCI) Mother Baby-Family Friendly Maternity Care Facility (MBFMF) Initiative Guidebook. 2023.
15. Altaweli R, Shaban I, Paine P. REPORT ON THE MIDWIFERY WORKFORCE IN THE MOH, SAUDI ARABIA, FOR 2019. Pract Midwife. 2020;23(8). doi:10.55975/NIXW5570
16. Al-Shahrani HNF, Alshahrani HD, Al-Masaad NMM, et al. Critical analysis of midwives’ impact on maternal and neonatal health in Saudi Arabia. J Ecohumanism. 2024;3(8):2349–2357. doi:10.62754/joe.v3i8.4981
17. World Health Organization (WHO). A systematic approach for undertaking a research priority-setting exercise: guidance for WHO staff. 2020.
18. Saudi National Institute of Health (NIH). Health research priorities report. 2025.
19. Alliance JL. The James Lind Alliance Guidebook: Version 10.
20. Janerka C, Mellan M, Wright R, Gill FJ, Leslie GD. Nursing and midwifery research priorities for an Australian health service: a priority-setting partnership approach. Collegian. 2023;30(5):693–700. doi:10.1016/j.colegn.2023.08.004
21. Ayman G, Strachan JA, McLennan N, et al. The top 10 research priorities in diabetes and pregnancy according to women, support networks and healthcare professionals. Diabetic Med. 2021;38(8):e14588. doi:10.1111/dme.14588
22. National Health and Medical Research Council (NHMRC). Guidelines for guidelines: engaging stakeholders. 2018. Available from: https://www.nhmrc.gov.au/guidelinesforguidelines/plan/engaging-stakeholders.
23. Baltussen R, Jansen MP, Mikkelsen E, et al. Priority setting for universal health coverage: we need evidence-informed deliberative processes, not just more evidence on cost-effectiveness. Int J Health Policy Manag. 2016;5(11):615. doi:10.15171/ijhpm.2016.83
24. Fleurence RL, Torgerson DJ. Setting priorities for research. Health Policy. 2004;69(1):1–10. doi:10.1016/j.healthpol.2003.11.002
25. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
26. Graneheim UH, Lindgren B-M, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
27. Mörelius E, Munns A, Smith S, et al. Pediatric and child health nursing: a three-phase research priority setting study in Western Australia. J Pediatric Nurs. 2022;63:39–45. doi:10.1016/j.pedn.2021.12.016
28. Morse JM. Critical analysis of strategies for determining rigor in qualitative inquiry. Qual Health Res. 2015;25(9):1212–1222. doi:10.1177/1049732315588501
29. Cypress BS. Rigor or reliability and validity in qualitative research: perspectives, strategies, reconceptualization, and recommendations. Dimens Crit Care Nurs. 2017;36(4):253–263. doi:10.1097/DCC.0000000000000253
30. Sriram S, Almutairi FM, Albadrani M. Midwife-led versus obstetrician-led perinatal care for low-risk pregnancy: a systematic review and meta-analysis of 1.4 million pregnancies. J Clin Med. 2024;13(22):6629. doi:10.3390/jcm13226629
31. Fitriana F, Ningrum AG, Izzati D, et al. Impact of the midwife-led care model on mode of birth: a systematic review and meta-analysis. Br J Midwifery. 2024;32(7):370–379. doi:10.12968/bjom.2024.32.7.370
32. Hanahoe M. Midwifery-led care can lower caesarean section rates according to the Robson ten group classification system. Eur J Midwifery. 2020;4:7. doi:10.18332/ejm/119164
33. Alanazy W, Brown A. Individual and healthcare system factors influencing antenatal care attendance in Saudi Arabia. BMC Health Serv Res. 2020;20(1):49. doi:10.1186/s12913-020-4903-6
34. Abdulghani N, Amir LH, Edvardsson K. Observational study found that skin-to-skin contact was not common after vaginal birth in Saudi Arabia. Acta Paediatrica. 2020;109(8):1681–1682. doi:10.1111/apa.15232
35. Abdulghani N, Amir LH, Edvardsson K, Cooklin A. It’s time for global action to reinforce mother-infant skin-to-skin contact policy. Acta Paediatrica. 2020;109(8):1689. doi:10.1111/apa.15369
36. Abdulghani N, Cooklin A, Edvardsson K, Amir LH. Mothers’ perceptions and experiences of skin-to-skin contact after vaginal birth in Saudi Arabia: a cross-sectional study. Women Birth. 2022;35(1):e60–e7. doi:10.1016/j.wombi.2021.02.001
37. Abdulghani N, Edvardsson K, Amir LH. Worldwide prevalence of mother-infant skin-to-skin contact after vaginal birth: a systematic review. PLoS One. 2018;13(10):e0205696. doi:10.1371/journal.pone.0205696
38. Abdulghani N, Edvardsson K, Amir LH. Health care providers’ perception of facilitators and barriers for the practice of skin-to-skin contact in Saudi Arabia: a qualitative study. Midwifery. 2020;81:102577. doi:10.1016/j.midw.2019.102577
39. Murad A, Renfrew MJ, Symon A, Whitford H. Understanding factors affecting breastfeeding practices in one city in the Kingdom of Saudi Arabia: an interpretative phenomenological study. Int Breastfeed J. 2021;16(1):9. doi:10.1186/s13006-020-00350-4
40. Alissa N, Alshareef M, editors. Factors influencing exclusive breastfeeding in Saudi Arabia. In: Healthcare. MDPI; 2024.
41. Zarroug M, Altaf MF, Shaikh S, et al. The prevalence and risk factors of postpartum depression among Saudi Arabian women—a systematic review and meta-analysis. In: Healthcare. MDPI; 2025.
42. Alsulami A, Orabi A, Timraz S. Saudi women’s perspectives on postpartum depression. Front Glob Womens Health. 2024;5:1326130. doi:10.3389/fgwh.2024.1326130
43. Almuqbil M, Kraidiye N, Alshmaimri H, et al. Postpartum depression and health-related quality of life: a Saudi Arabian perspective. PeerJ. 2022;10:e14240. doi:10.7717/peerj.14240
44. Sun C, Dohrn J, Oweis A, et al. Delphi survey of clinical nursing and midwifery research priorities in the eastern Mediterranean region. J Nurs Scholarsh. 2017;49(2):223–235. doi:10.1111/jnu.12280
45. Aungsuroch Y, Nhu XHT, Linh TTK, Polsook R, Navicharern R, Gunawan J. Identifying nursing research priorities in Vietnam: a modified Delphi study. Front Nurs. 2019;6(4):249–259. doi:10.2478/FON-2019-0044
46. Aungsuroch Y, Songnavong C, Tantikosoom P, et al. Determining nursing research priorities in Lao people’s democratic republic: a modified delphi study. Nurs Midwifery Stud. 2020;9(3):157–162. doi:10.4103/nms.nms_87_19
47. Almatrafy WH, ALsolami F. Exploring midwives’ perception about their competency during the second and third stages of labour: a qualitative study. Nurs Commun. 2023;7:35. doi:10.53388/IN2023035
48. Alghamdi RS, Perra O, Boyle B, Stockdale J. Perceived treatment of respectful maternity care among pregnant women at healthcare facilities in the Kingdom of Saudi Arabia: a cross-sectional study. Midwifery. 2023;123:103714. doi:10.1016/j.midw.2023.103714
49. Alruwaili TA, Fooladi E, Crawford K. Women and husbands’ experiences and expectations of shared decision-making during pregnancy and childbirth in Saudi Arabia: a qualitative study. Midwifery. 2025;148:104533. doi:10.1016/j.midw.2025.104533
50. Yakout S, Jahla I. Artificial intelligence: innovation and midwifery education, practice, and research in Arab region; systematic review based findings. J Popul Ther Clin Pharmacol. 2023;30:198–214.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.