Back to Journals » International Medical Case Reports Journal » Volume 13
MicroPulse Transscleral Laser Therapy with Kahook Dual Blade Excisional Goniotomy and Goniosynechialysis Combined with Phacoemulsification for Angle-Closure Glaucoma: A Case Report
Authors Al Habash A ![]() , Otaif W
, Otaif W ![]() , Al Somali AI
, Al Somali AI ![]() , Khoueir Z
, Khoueir Z ![]()
Received 9 August 2020
Accepted for publication 23 October 2020
Published 13 November 2020 Volume 2020:13 Pages 631—636
DOI https://doi.org/10.2147/IMCRJ.S276282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "MicroPulse TLT and KDB assisted goniosynechialysis for chronic ACG" [ID 276282].
Views: 218
Ahmed Al Habash,1 Wael Otaif,2 Abdulaziz Ismail Al Somali,3 Ziad Khoueir4,5
1Department of Ophthalmology, College of Medicine, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Ophthalmology, King Khalid University, Abha, Saudi Arabia; 3Department of Ophthalmology, King Faisal University, Al Ahsa, Kingdom of Saudi Arabia; 4Beirut Eye and ENT Specialist Hospital, Beirut, Lebanon; 5Saint- Joseph University, Faculty of Medicine, Beirut, Lebanon
Correspondence: Ahmed Al Habash
Department of Ophthalmology, College of Medicine, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, PO Box 31010, Dammam 31952, Saudi Arabia
Tel +966507017777
Email [email protected]
Purpose: To report the efficacy and safety of MicroPulse transscleral laser therapy (TLT) and Kahook Dual Blade excisional goniotomy and goniosynechialysis combined with phacoemulsification for chronic angle-closure glaucoma (ACG).
Patients and Methods: A 39-year-old hyperopic female with a known history of ACG presented with a 2-week history of blurry vision, headache, and photophobia in the right eye (RE) following surgical peripheral iridectomy at another hospital. On examination, her uncorrected visual acuity was 20/50 in the RE, and 20/25 in the left eye (LE). Goldman applanation tonometry revealed an intraocular pressure (IOP) of 51 mmHg in the RE and 12 mmHg in the LE. Ocular examination of the RE revealed conjunctival hyperemia, corneal edema, shallow anterior chamber, posterior synechia, mid-dilated non-reactive pupil, and early cataractous changes. Anterior segment examination findings in the LE were normal except for a shallow anterior chamber. Gonioscopy revealed a closed angle (Schaffer grade 0) with 360° peripheral anterior synechia in the RE and a narrow angle (Schaffer grade 2) in the LE. The cup-to-disc ratios were 0.5 RE and 0.3 LE. The patient underwent MicroPulse TLT with phacoemulsification, Kahook Dual Blade-assisted goniosynechialysis, and excisional goniotomy in the RE.
Results: At the 1-year follow-up, her IOP remained stable without the need for antiglaucoma medications. No further optic nerve or visual field deterioration was noted.
Conclusion: MicroPulse TLT combined with phacoemulsification and Kahook Dual Blade-assisted goniosynechialysis and excisional goniotomy safely reduced IOP and the need for antiglaucoma medications in chronic ACG, avoiding the complications associated with incisional glaucoma surgery.
Keywords: goniosynechialysis, Kahook Dual Blade, MicroPulse transscleral laser therapy, angle-closure glaucoma
Introduction
Primary angle-closure glaucoma (PACG) accounts for 25% of glaucoma-related visual loss worldwide.1 Angle-closure glaucoma (ACG) is caused by obstruction of the trabecular meshwork (TM) by the peripheral iris, resulting in an impaired outflow of the aqueous along with an increase in the intraocular pressure (IOP).2 The management of PACG remains controversial; however, the main treatment strategies are aimed at reduction of the IOP, opening the angle, and prevention of recurrent angle closure.3 Although trabeculectomy is the gold standard procedure for lowering IOP, it is associated with vision-threatening complications such as hypotony, aqueous misdirection, and bleb-related infections.4 Recently, research has shown that cataract extraction in PACG results in deepening of the anterior chamber and lowering of IOP.5–8 However, cataract extraction alone cannot address the synechial angle closure, and various studies have indicated that phacoemulsification combined with goniosynechialysis (GSL) and excisional goniotomy in PACG is a safe and more effective treatment for IOP reduction than cataract surgery alone.9 GSL is a surgical technique that aims to strip the peripheral anterior synechia (PAS) from the angle, exposing the TM in an attempt to restore the normal aqueous outflow. The inclusion of excisional goniotomy, which involves TM strip excision using the Kahook Dual Blade (KDB, New World Medical, Rancho Cucamonga, CA) can adequately address the trabecular dysfunction caused by chronic synechiae and scarring of outflow channels.10–14 Although phaco-GSL surgery is an effective treatment modality in PACG, it may not help in reducing the topical glaucoma treatment in the long run.15 Moreover, MicroPulse TLT appears to be an effective and safe procedure for ACG as it lowers the production of aqueous and enhances the uveoscleral outflow, with minimal collateral damage.16,17 A recent study showed that MicroPulse TLT resulted in a significant reduction of IOP and the need for antiglaucoma medications in eyes with good visual acuity.18
To the best of our knowledge, this is the first report of combined MicroPulse TLT with phacoemulsification, and KDB-assisted GSL and excisional goniotomy in a case of chronic ACG.
Case Report
A 39-year-old hyperopic with a known history of ACG presented with a 2-week history of blurry vision, headache, and photophobia in her right eye (RE). Her family and medical history were otherwise unremarkable. She underwent surgical peripheral iridectomy and was advised trabeculectomy of the right eye at another hospital, which she refused.
On presentation at our institution, she was on 0.15% brimonidine tartrate t.i.d. (ALPHAGAN® P Allergan Inc, Irvine, CA, USA), 2% dorzolamide hydrochloride-0.5% timolol maleate ophthalmic solution b.i.d. (COSOPT®; Merck & Co., Inc., Whitehouse Station, N.J., U.S.A.), and 0.03% bimatoprost q.h.s. (LUMIGAN® Allergan, Inc, Irvine, CA, USA).
Upon examination, her uncorrected visual acuity (VA) was 20/50 in the RE and 20/25 in her left eye (LE). Goldman applanation tonometry revealed an IOP of 51 mmHg in the RE and 12 mmHg in the LE. Ocular examination of the RE revealed conjunctival hyperemia, corneal edema, shallow anterior chamber, posterior synechia, mid-dilated non-reactive pupil, and early cataractous changes (Figure 1A). Anterior segment examination findings in the LE were normal, except for a shallow anterior chamber (Figure 1B). Gonioscopy revealed a closed angle (Schaffer grade 0) with a 360° PAS in the RE and a narrow angle (Schaffer grade 2) in the LE. The cup-to-disc ratios were 0.5 and 0.3 in the RE and LE, respectively. Humphrey visual field 24-2 showed a nasal step defect pattern with a mean deviation of −10.81 dB, and optical coherence tomography (OCT) demonstrated glaucomatous changes in the optic nerve and retinal nerve fiber layer. Ultrasound biomicroscopy (UBM) reported a 360° closed-angle with no signs suggesting the diagnosis of plateau iris configuration, and anterior segment optical coherence tomography (AS-OCT) showed a closed iridocorneal angle (Figure 1C).
 |
Figure 1 Pre-operative examination of both eyes. (A) Anterior segment picture of the right eye (RE) shows posterior synechiae, peripheral iridotomy, and cataractous lens. (B) Slit-lamp examination of the left eye shows narrow anterior chamber. (C) Anterior segment-optical coherence tomography of the RE shows a closed iridocorneal angle. |
Our patient demonstrated an acute ACG attack on top of her chronic ACG. Her acute ACG was treated with surgical iredectomy elsewhere, with the remaining chronic consequences. The patient was prescribed oral acetazolamide in addition to the topical glaucoma medications. The next day, her IOP was 35 mmHg in the RE. After discussing with the patient, she preferred a non-incisional, conjunctival sparing procedure with avoidance of bleb-related complications. We offered the combined approach of Micropulse TLT, phacoemulsification, posterior chamber intraocular lens (IOL) implantation, and KDB-assisted GSL with excisional goniotomy under local anesthesia in the RE.
Procedure
The procedures used in this case followed the tents of the Declaration of Helsinki and were approved by the Ethics Committee of King Fahad Hospital of the University, Khobar, Saudi Arabia. A written informed consent was obtained from the patient before starting the surgical treatment.
The surgery was performed by a single surgeon (A.H.) under local anesthesia with a peribulbar block. The local anesthetic agents included 2% lignocaine with 1:200,000 adrenaline in a 1:1 ratio and 0.5% bupivacaine. First, MicroPulse TLT was performed using the Cyclo G6 laser system with the MicroPulse treatment mode (IRIDEX, Mountain View, CA, USA). Xylocaine gel was applied over 360° of the conjunctiva prior to treatment (Figure 2A). The Cyclo G6 was programmed to 2100 mW at a 31.3% duty cycle, and the MicroPulse P3® fiberoptic handpiece (IRIDEX, Mountain View, CA USA) was connected to the Cyclo G6 to deliver laser energy 3.8 mm posterior to the limbus. The MicroPulse P3 probe was held with a firm, steady pressure over the conjunctiva while continuously sliding it back and forth 12 times for 120 s (each sweep in one direction was about 10 s) over 5 clock hours in the superior 180° and then repeated in the inferior 180° sparing the 3 and 9 o’clock position.
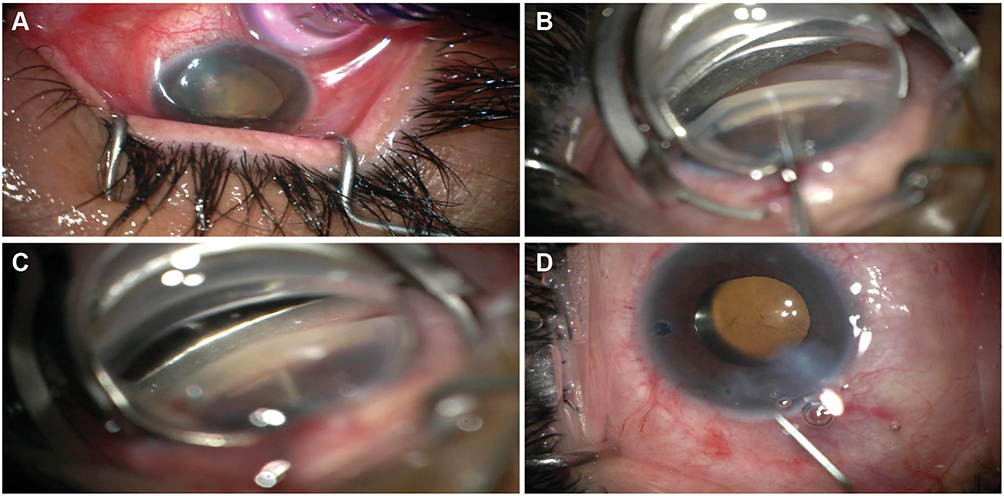 |
Figure 2 Intra-operative pictures of the surgical procedures. (A) MicroPulse transscleral laser therapy using the Cyclo G6 laser system. (B) Kahook Dual Blade (KDB) assisted goniosynechialysis. (C) KDB-assisted excisional goniotomy. (D) Removal of ophthalmic viscoelastic device and blood reflux with irrigation/aspiration. |
Lens extraction was then performed using a routine phacoemulsification technique. After implantation of the IOL, the microscope was tilted 45° toward the surgeon, while the patient’s head was rotated away from the surgeon about 30–45°. Then, a Volk Transcend Vold Gonio (TVG) surgical lens was used to visualize the nasal aspect of the angle, followed by injection of ophthalmic viscoelastic devices (OVDs) into the anterior chamber to deepen the nasal angle. KDB was then inserted through the main corneal incision and advanced toward the nasal angle; GSL was performed and the footplate of KDB was used to disrupt the PAS and expose the TM for KDB-assisted goniotomy, in which the pointed tip of the KDB was advanced to engage and excise a strip of TM. (Figure 2B and C).
The microscope and the patient’s head were rotated to their original position, and the viscoelastic and blood reflux from Schlemm’s canal was removed from the eye using the irrigation/aspiration handpiece (Figure 2D). The entire surgical procedure was uneventful (see Supplementary Video S1, which demonstrates the surgical steps).
Post-operative care included 1% topical prednisolone acetate (q2h tapered over 8 weeks) and a fourth-generation topical fluoroquinolone (moxifloxacin) 4 times daily for a week. The best-corrected visual acuity (BCVA) and IOP were recorded at day 1, week 1, and 3, 6, 9, and 12 months postoperatively as follows:
Post-operative day 1: IOP: 18 mmHg RE and 17 mmHg LE without glaucoma medications. The anterior chamber was deep with a slit of hyphema, and the IOL was in place.
One week later: IOP: 16 mmHg RE and 13 mmHg LE. BCVA: 20/50 RE and 20/20 LE.
Post-operative week 3: IOP: 12 mmHg RE and 15 mmHg LE. BCVA: 20/40 RE and 20/20 LE. Slit-lamp examination revealed a clear cornea with a deep anterior chamber (Figure 3A). Post-operative AS-OCT of the RE revealed a deep anterior chamber with a surgically created cleft in the TM (Figure 3B).
 |
Figure 3 Post-operative examination of the right eye (RE). (A) Post-operative slit-lamp examination of the RE shows deep anterior chamber with a clear cornea, and intraocular lens in place. (B) Post-operative anterior segment-optical coherence tomography of the RE shows deep anterior chamber with surgically created cleft in the trabecular meshwork (arrow). |
The IOP remained stable on subsequent follow-up visits over 1 year. At the last follow-up, the BCVA was 20/20 and the was IOP 15 mmHg in the RE; the patient did not require antiglaucoma medication. Neither optic nerve nor visual field progression was noted.
Discussion
Previous studies have reported that lens thickening, a shallow anterior chamber, and a short axial length are key risk factors for PACG.19,20 Of these, the lens thickness is especially important in the pathophysiology of the condition as either the anterior-posterior dimension of the lens increases or the depth of the anterior chamber decreases by the lens being in a more anterior position. As a consequence, the angle is overcrowded, and with a shallow anterior chamber, a pupillary block results from the iridolenticular apposition. The lens vault (LV) has been identified as a potential biometric parameter. There is a strong association between LV, which is the lens position relative to the scleral spur, and angle closure.21 The efficacy and safety of lens extraction to manage PACG, even in patients without cataract, have been reported in many studies.5–7
However, satisfactory IOP control cannot be achieved in all eyes by lens extraction alone. Factors that may influence the success rate include duration of angle closure, as well as its extent and severity. The prognosis is likely to be worse in patients with chronic PAS. In these patients, the IOP can be reduced effectively through GSL surgery, which can remove the anterior iris adhesions from the TM, with an approximately 80% success rate.13
Despite the success rate of GSL, it is unable to address the dysfunctional trabecular meshwork occurring as a result of chronic PAS, inflammation, fibrous tissue metaplasia of the TM, and GSL-initiated iatrogenic damage. In patients with a dysfunctional TM, excisional goniotomy can promote direct aqueous outflow through Schlemm’s canal by removal of an inner wall of the TM; the outflow can then follow the distal pathway. Both goniotomy and GSL can be performed using a KDB, which reduces the duration of surgery and enhances the safety because of the need for a single instrument rather than the use of multiple surgical instruments. According to Dorairaj et al, clinically and statistically significant reductions in intraocular pressure in angle-closure glaucoma cases can be achieved by cataract extraction in conjunction with KDB-assisted GSL with excisional goniotomy. Furthermore, this combined intervention reduces the necessity for patients to take IOP-lowering medications.10,13 However, the mean baseline IOP in their study was 25.5 mmHg, which was reduced by 47.2% at a 12-month follow-up. Our patient demonstrated a high baseline IOP of 51 mmHg despite the maximum number of glaucoma medications. Therefore, we hypothesize that adding MicroPulse TLT can provide the necessary efficacy for lowering the IOP and glaucoma medication in this eye. Based on our observation and safety profile, the addition of Micropulse TLT to phaco/KDB-assisted GSL and excisional goniotomy provided a significant reduction in both IOP and topical glaucoma medication. Hence, we recommend adding MicroPulse TLT to this combined approach, particularly in patients with high baseline IOP and glaucoma medications. MicroPulse TLT has demonstrated a significant IOP and glaucoma medication reduction in different glaucoma subtypes as well as in eyes with good central visual acuity while establishing a good safety profile.16–18 Such an approach would enable aqueous inflow and outflow to be managed simultaneously, which would minimize the need for glaucoma drainage surgery and glaucoma medications. Moreover, as the procedure does not involve or injure the conjunctiva, drainage surgery can be performed later, if required.
MicroPulse TLT is a recently introduced novel intervention that can significantly reduce the risks of complications endangering vision and does not hinder the reduction of aqueous humor production.22 Many clinical and experimental studies have proposed and elucidated the mechanisms of action of Micropulse TLT. One such mechanism is the selective destruction of the pigmented cells of the ciliary body, which lessens the secretion of aqueous humor. Another possible mechanism is the increase in the uveoscleral outflow. A third mechanism is alteration in the structure of the trabecular meshwork and the outflow pathway by stimulating contraction of the ciliary muscle’s longitudinal fibers and by pulling and rotating the scleral spur internally and posteriorly.16,18 MicroPulse TLT offers a flexible approach to manage glaucoma at various stages. Evidence shows that as the approach is not associated with serious complications, it can be performed in patients with early-stage PACG and good visual potential.16–18
In patients with visually significant cataracts, progressive glaucomatous damage, or uncontrolled IOP, the standard PACG procedure involves a combination of trabeculectomy and cataract surgery. The benefit of combining these procedures is a single surgical event reduces the cost and visual rehabilitation is typically achieved within 6–8 weeks. However, owing to increased inflammation, the bleb failure rate of phaco-trab surgery is high. Other risks include several vision-threatening complications, such as blebitis, hypotony, and shallow anterior chamber. Furthermore, the procedure is associated with a long-term risk of bleb-related-endophthalmitis.23 In this report, we propose a blebless procedure where MicroPulse TLT is performed together with phacoemulsification with IOL implantation, and GSL combined with KDB to regulate the IOP in extensive synechial ACG. With a combined approach involving MicroPulse TLT, phacoemulsification, KDB-assisted GSL, and excisional goniotomy to facilitate simultaneous aqueous inflow and outflow in patients with severe synechial angle closure, the IOP can be reduced effectively. Furthermore, the requirement of subsequent drainage surgery is reduced by this approach.
To the best of our knowledge, this is the first report where the above-mentioned techniques have been proposed as a combined approach to treat this blinding disease. However, further research is required, and randomized control studies with larger samples and longer follow-up durations are warranted to verify the effectiveness of this approach.
Informed Consent
A signed written informed consent for publication of clinical images and details were obtained from the patient.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. doi:10.1136/bjo.2005.081224
2. Foster PJ, Aung T, Nolan WP, et al. Defining occludable angles in population surveys: drainage angle width, peripheral anterior synechiae, and glaucomatous optic neuropathy in east Asian people. Br J Ophthalmol. 2004;88:486–490. doi:10.1136/bjo.2003.020016
3. Congdon NG, Friedman DS. Angle-closure glaucoma: impact, etiology, diagnosis, and treatment. Curr Opin Ophthalmol. 2003;14:70–73. doi:10.1097/00055735-200304000-00002
4. DeBry PW, Perkins TW, Heatley G, et al. Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol. 2002;120:297–300. doi:10.1001/archopht.120.3.297
5. Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388:1389–1397. doi:10.1016/S0140-6736(16)30956-4
6. Tham CCY, Kwong YYY, Baig N, et al. Phacoemulsification versus trabeculectomy in medically uncontrolled chronic angle-closure glaucoma without cataract. Ophthalmology. 2013;120:62–67. doi:10.1016/j.ophtha.2012.07.021
7. Chen PP, Lin SC, Junk AK, et al. The effect of phacoemulsification on intraocular pressure in glaucoma patients: a report by the American Academy of Ophthalmology. Ophthalmology. 2015;122:1294–1307.
8. Moghimi S, Latifi G, ZandVakil N, et al. Phacoemulsification versus combined phacoemulsification and viscogonioplasty in primary angle-closure glaucoma. J Glaucoma. 2015;24:575–582. doi:10.1097/IJG.0000000000000196
9. Alaghband P, Rodrigues IA, Goyal S. Phacoemulsification with intraocular implantation of lens, endocyclophotocoagulation, and endoscopic-goniosynechialysis (PIECES): a combined technique for the management of extensive synechial primary angle closure glaucoma. J Curr Glaucoma Pract. 2018;12:45–49. doi:10.5005/jp-journals-10028-1243
10. Dorairaj S, Tam MD, Goundappa BK. Twelve-month outcomes of excisional goniotomy using the Kahook Dual Blade in eyes with angle-closure glaucoma. Clin Ophthalmol. 2019;13:1779–1785. doi:10.2147/OPTH.S221299
11. Tun TA, Baskaran M, Perera SA, et al. Swept-source optical coherence tomography assessment of iris-trabecular contact after phacoemulsification with or without goniosynechialysis in eyes with primary angle closure glaucoma. Br J Ophthalmol. 2015;99:927–931. doi:10.1136/bjophthalmol-2014-306223
12. Shao T, Hong J, Xu J, et al. Anterior chamber angle assessment by anterior-segment optical coherence tomography after phacoemulsification with or without goniosynechialysis in patients with primary angle closure glaucoma. J Glaucoma. 2015;24:647–655. doi:10.1097/IJG.0000000000000061
13. Harasymowycz PJ, Papamatheakis DG, Ahmed I, et al. Phacoemulsification and goniosynechialysis in the management of unresponsive primary angle closure. J Glaucoma. 2005;14:186–189. doi:10.1097/01.ijg.0000159131.38828.85
14. Lai JS. The role of goniosynechialysis in the management of chronic angle-closure glaucoma. Asia Pac J Ophthalmol (Phila). 2013;2:277–278. doi:10.1097/APO.0b013e3182a8146b
15. Wang N, Jia SB. Phacoemulsification with or without goniosynechialysis for angle-closure glaucoma: a global meta-analysis based on randomized controlled trials. Int J Ophthalmol. 2019;12:826–833.
16. Al Habash A, Alahmadi AS. Outcome of MicroPulse® transscleral photocoagulation in different types of glaucoma. Clin Ophthalmol. 2019;13:2353–2360. doi:10.2147/OPTH.S226554
17. Zaarour K, Abdelmassih Y, Arej N, et al. Outcomes of Micropulse transscleral cyclophotocoagulation in uncontrolled glaucoma patients. J Glaucoma. 2019;28:270–275. doi:10.1097/IJG.0000000000001174
18. Varikuti VNV, Shah P, Rai O, et al. Outcomes of Micropulse transscleral cyclophotocoagulation in eyes with good central vision. J Glaucoma. 2019;28:901–905. doi:10.1097/IJG.0000000000001339
19. Aung T, Nolan WP, Machin D, et al. Anterior chamber depth and the risk of primary angle closure in 2 East Asian populations. Arch Ophthalmol. 2005;123:527–532. doi:10.1001/archopht.123.4.527
20. Wojciechowski R, Congdon N, Anninger W, et al. Age, gender, biometry, refractive error, and the anterior chamber angle among Alaskan Eskimos. Ophthalmology. 2003;110:365–375. doi:10.1016/S0161-6420(02)01748-7
21. Nongpiur ME, He M, Amerasinghe N, et al. Lens vault, thickness, and position in Chinese subjects with angle closure. Ophthalmology. 2011;118:474–479. doi:10.1016/j.ophtha.2010.07.025
22. Aquino MCD, Barton K, Tan AMWT, et al. Micropulse versus continuous wave transscleral diode cyclophotocoagulation in refractory glaucoma: a randomized exploratory study. Clin Exp Ophthalmol. 2015;43:40–46. doi:10.1111/ceo.12360
23. Tham CCY, Kwong YY, Leung DYL, et al. Phacoemulsification vs phacotrabeculectomy in chronic angle-closure glaucoma with cataract complications. Arch Ophthalmol. 2010;128:303–311.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.