Back to Journals » Clinical Ophthalmology » Volume 20
Micropulse Transscleral Cyclophotocoagulation in Refractory Glaucoma: Two-year Results of a Prospective Multicenter Study
Authors Lin F, Wang Y ![]() , Duan X, Hu B, Xue Y, Ling Q, Xiaokaiti D, Zhao Z, Song Y, Fang Z, Chen Y, Jin L, Zeng L, Zhang X
, Duan X, Hu B, Xue Y, Ling Q, Xiaokaiti D, Zhao Z, Song Y, Fang Z, Chen Y, Jin L, Zeng L, Zhang X
Received 13 November 2025
Accepted for publication 20 February 2026
Published 9 March 2026 Volume 2026:20 581314
DOI https://doi.org/10.2147/OPTH.S581314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fengbin Lin,1,* Yuhong Wang,2,* Xuanchu Duan,3,* Baiyu Hu,4 Yingying Xue,2 Qiying Ling,3 Dilimulati Xiaokaiti,5 Zhenni Zhao,6 Yunhe Song,1 Zige Fang,1 Yu Chen,1 Ling Jin,1 Liuzhi Zeng,4 Xiulan Zhang1
1State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangdong Provincial Key Laboratory of Ophthalmology of Ophthalmology and Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, People’s Republic of China; 2Xiamen Eye Center of Xiamen University, Xiamen, People’s Republic of China; 3Changsha Aier Eye Hospital, Changsha, People’s Republic of China; 4Department of Ophthalmology, Chengdu First People’s Hospital, Chengdu, People’s Republic of China; 5Department of Ophthalmology Center, The First People’s Hospital of Kashi Prefecture, Xinjiang, People’s Republic of China; 6Department of Ophthalmology, Guangzhou Women and Children’s Medical Center, Guangzhou Medical, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiulan Zhang, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology of Ophthalmology and Visual Science, Guangdong Provincial Clinical Research Center for Ocular Diseases, Guangzhou, People’s Republic of China, Email [email protected] Liuzhi Zeng, Department of Ophthalmology, Chengdu First People’s Hospital, Chengdu, China, Email [email protected]
Purpose: To evaluate the efficacy and safety of micropulse transscleral cyclophotocoagulation (MP-TSCPC) for refractory glaucoma.
Patients and Methods: This prospective multicenter study included 62 eyes of 57 refractory glaucoma patients. MP-TSCPC was performed from August 2022 to May 2023. All patients had a complete ophthalmic examination preoperatively, including medical history, slit-lamp examination, best-corrected visual acuity (BCVA) assessment, and pre- and post-operative intraocular pressure (IOP) measurements. The main outcomes included IOP change, antiglaucoma medication use, the cumulative incidence of treatment success, and the postoperative complications over 24 months. Treatment success was defined as an IOP reduction of more than 20% compared with baseline or a decrease in the number of antiglaucoma medications with stable target IOP. Retreatments were classified as failures.
Results: The glaucoma subtypes included primary glaucoma (n=29) and secondary glaucoma (n=33). Prior glaucoma surgery had been performed in 48 of the 62 eyes (77.4%), with 30 of them having multiple types of surgery. Preoperatively, the mean IOP was 38.2± 10.3 mmHg and the median number of antiglaucoma medications used was 3.0 (2.0, 3.0); these values decreased to 20.9± 8.8 mmHg (a reduction of 42.7%; P< 0.001) and 2.0 (0.0, 3.0) (P< 0.001) at month 24, respectively. The treatment success rate was 77.4% at 24 months. Postoperative complications included mydriasis (n=10), conjunctival hemorrhage (n=9), mild anterior chamber inflammation (n=1), hyphema (n=1), mild ciliary body detachment (n=3), and choroidal detachment (n=1), all reversible after treatment.
Conclusion: MP-TSCPC appears to be a safe and effective treatment option for refractory glaucoma.
Keywords: refractory glaucoma, micropulse transscleral cyclophotocoagulation, prospective study, multicenter study
Introduction
Glaucoma is the leading cause of irreversible blindness in the world.1,2 It has been estimated that 111.8 million people worldwide will be affected by glaucoma in 2040.3 Glaucoma is unevenly distributed globally, with the highest incidence found among the Asian population, accounting for about half of all cases worldwide.3
Lowering intraocular pressure (IOP) is currently the only known effective option for treating glaucoma.4,5 The IOP can be lowered by medical treatment, laser therapy, or incisional surgery, according to different types and stages of glaucoma.4,5 However, for patients with uncontrolled, refractory glaucoma, or for whom other glaucoma treatments have failed, a cyclodestructive procedure (ie, cyclocryocoagulation, cyclodiathermy, or trans-scleral cyclophotocoagulation [TSCPC]) is often the final option.6,7 However, these procedures can lead to serious complications, such as persistent hypotony, persistent intraocular inflammation, hyphema, decreased visual acuity, and phthisis bulbi.8,9
Micropulse transscleral cyclophotocoagulation (MP-TSCPC) is an innovative laser treatment that involves applying laser energy to ocular tissue in short bursts followed by rest periods, effectively breaking up the continuous wave beam into repetitive pulses.10,11 This method is designed to dissipate energy between each pulse, which is hypothesized to reduce energy accumulation in the tissues and mitigate potential damage to surrounding tissues.10,11 Several previous studies have shown that MP-TSCPC can effectively lower IOP in patients with refractory glaucoma, with fewer severe complications compared to conventional cyclodestructive procedures.12–18 A recent meta-analysis further corroborated these findings, reporting that while MP-TSCPC and continuous wave cyclophotocoagulation offer similar efficacy in IOP control, MP-TSCPC demonstrated a greater safety profile.19 Additionally, our preliminary results demonstrate promising efficacy of the procedure in refractory glaucoma.20 At the six-month follow-up, the procedure achieved a 43.7% reduction in IOP, with a treatment success rate of 83.6% of eyes.20 However, given that this treatment remains relatively new in Mainland China, long-term safety and efficacy data are still limited. This report extends the analysis of clinical outcomes of MP-TSCPC in Chinese patients with refractory glaucoma, with follow-up data spanning up to 24 months.
Material and Methods
Study Design and Participants
This was a prospective, observational multicenter study conducted in China. It included patients who received MP-TSCPC for glaucoma from four different glaucoma centers: Zhongshan Ophthalmic Center, Chengdu First People’s Hospital, Xiamen Eye Center of Xiamen University, and Changsha Aier Eye Hospital, between August 2022 and May 2023. The study was approved by the Ethical Committee of Zhongshan Ophthalmic Center (ID: 2022KYPJ225) and followed the tenets of the Declaration of Helsinki. Before undergoing any surgical procedure, all subjects provided written informed consent.
The inclusion criteria for the study were as follows: (1) age ≥18 years; (2) patients with moderate to advanced glaucoma were offered treatment with MP-TSCPC. This alternative was applicable for patients whose glaucoma remained uncontrolled (presence of glaucomatous visual field progression or failure to reach the target IOP), despite having taken the maximum tolerated topical with or without systemic antiglaucoma medication or previously undergoing glaucoma surgery, as well as for those who were unable to tolerate any antiglaucoma medications. Additionally, patients on maximum topical with or without systemic antiglaucoma medication who faced high risks with glaucoma surgery were included, intending to reduce their dependence on antiglaucoma medication; (3) a minimum of 24 months follow-up. Patients were excluded if they had active conjunctivitis, active uveitis, or were under active treatment for another ophthalmic condition. Patients required a secondary treatment (other than MP-TSCPC) during the follow-up were also excluded. The severity of glaucoma was classified according to the Hodapp-Parrish-Anderson criteria: a mean deviation (MD) greater than −6 dB was considered mild, between −6 dB and −12 dB was considered moderate, and an MD of −12 dB or less was considered severe.21,22
All patients had a complete ophthalmic examination preoperatively, including glaucoma type, previous glaucoma surgery, number of antiglaucoma medications, slit-lamp examination (including pupil size), best-corrected visual acuity (BCVA) assessment, and IOP measurements with Goldmann applanation tonometry.
Surgical Procedure and Postoperative Care
All patients were treated by a standardized treatment protocol. Treatments were performed by 4 experienced glaucoma surgeons (X.Z., Z.Z., Y.W, and X.D.) under topical or general anesthesia, depending on the patient’s condition and general health status. General anesthesia was reserved for patients with poor health who could not tolerate topical anesthesia. Patients underwent MP-TSCPC treatment (First generation probe, MicroPulse P3 probe, Iridex cyclo G6 laser system, Mountain View, CA), with an output of 2000 mW at a duration of 80 seconds per hemisphere and at a 31.3% duty cycle. Both hemispheres were treated with the MP3 probe continuously moved with steady pressure on the ocular globe. During treatment, 3 and 9 o’clock hours, areas of previous glaucoma surgery (filtering and drainage implant areas), and sites of scleral thinning were avoided. In situations where retreatment was necessary, identical parameters were used.
Postoperatively, patients were prescribed topical steroids eye drops (prednisone acetate 1%) and ointment (tobramycin and dexamethasone) for 2 weeks. Antiglaucoma medications were discontinued, reduced, or continued on a case-by-case basis by the surgeons.
Outcome Measures
Follow-up examinations were performed on day 1, week 1, and months 1, 3, 6, 12, and 24. The main outcomes included IOP change, the change of antiglaucoma medications use, the cumulative incidence of treatment success, and the postoperative complications. Treatment success was defined as an IOP reduction of more than 20% compared with baseline or a decrease in the number of antiglaucoma medications with stable target IOP.14,16,17 Treatment failure was defined as the inability to achieve the critical level of treatment success or the need for repeated MP-TSCPC or subsequent glaucoma procedures to control IOP.14,16,17 The postoperative complications include corneal pathology, anterior chamber inflammation, mydriasis, choroidal detachment, or other ocular abnormalities. Anterior chamber inflammation was defined as the presence of anterior chamber cells of grade 1 or higher based on the Standardization of Uveitis Nomenclature grading system.23 Normal pupil diameter ranged from 2 to 4 mm at baseline. Mydriasis was defined as an increase in pupil diameter of ≥2 mm compared with the screening visit, or a pupil diameter >5 mm during postoperative follow-up.
Statistical Analysis
Each eligible eye in the study was considered as the unit of analysis. Mixed effects models were utilized to account for the inter-eye correlation within the same patient. The normality of the distribution of continuous variables was assessed using the Shapiro–Wilk test. Continuous data are presented as either the mean ± standard deviation (SD) or median with quartiles, while categorical variables are depicted as the count and percentage. Postoperative IOP was compared to preoperative IOP using the paired t-test. Post- and pre-operative BCVA and the number of medications were compared using the Wilcoxon matched-pair signed-rank test. Statistical analyses were performed using Stata version 16 (StataCorp, College Station, Texas, USA). A P value < 0.05 was considered statistically significant.
Results
Demographic and Characteristics of the Patients
A total of 62 eyes of 57 patients were included in the study (Table 1). The mean age was 49.8±17.1 years, with 32 (56.1%) being females. The distribution of glaucoma types was as follows: primary glaucoma, 46.8% (29/62); neovascular glaucoma, 24.2% (15/62); glaucoma secondary to uveitis, 6.4% (4/62); glaucoma secondary to iridocorneal endothelial syndrome, 4.8% (3/62); glaucoma following vitreoretinal surgery, 4.8% (3/62); glaucoma secondary to cataract surgery, 4.8% (3/62); glaucoma after perforating keratoplasty, 1.6% (1/62); glaucoma related to lens dislocation, 1.6% (1/62); steroid-induced glaucoma, 1.6% (1/62); glaucoma secondary to ocular trauma, 1.6% (1/62); and glaucoma following nanopthalmos, 1.6% (1/62). Prior to MP-TSCPC, 48 of the 62 eyes (77.4%) had undergone previous surgeries, with 30 of them having multiple types of surgery. The prior surgeries included peripheral iridectomy (1), trabeculectomy (16), Ahmed valve implant (12), goniotomy (3), TSCPC (1), ultrasound cyclo-plasty (11), XEN Gel Implant (1), Ex-PRESS implant (5), Co2 laser-assisted sclerectomy surgery (1), and PEI (26). Additionally, there were 5 eyes (8.1%) with moderate glaucoma and 57 eyes (91.9%) with severe glaucoma. Snellen VA was 20/40 (0.3 LogMAR) or better in 14.5% (9/62) and 10/200 (1.3 LogMAR) or worse in 69.4% (43/62).
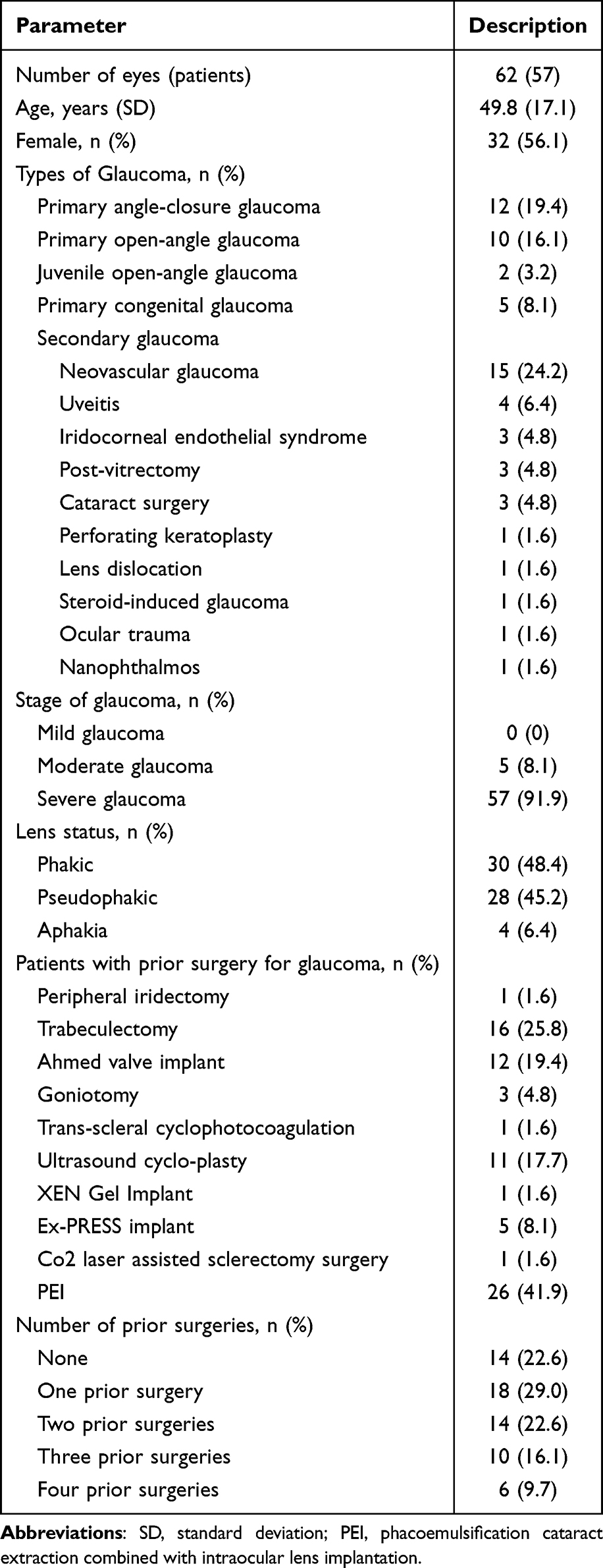 |
Table 1 Baseline Demographics and Characteristics of the Study Participants |
Change of IOP, Number of Medications, and BCVA
The average pre-surgery IOP was 38.2±10.3 mmHg, which significantly decreased to 21.2±8.2 mmHg the day after the operation. This IOP-lowering effect persisted for 24 months, with the IOP averaging 20.9±8.8 mmHg, resulting in a remarkable reduction of 17.4±12.0 mmHg. On average, this reduction represented a percentage decrease of 42.7±23.9%. It is noteworthy that there was a statistically significant decrease in IOP at all recorded time points (Table 2 and Figure 1, P<0.001).
 |
Table 2 Changes of Intraocular Pressure from Baseline and Surgical Outcomes at Each Time Point |
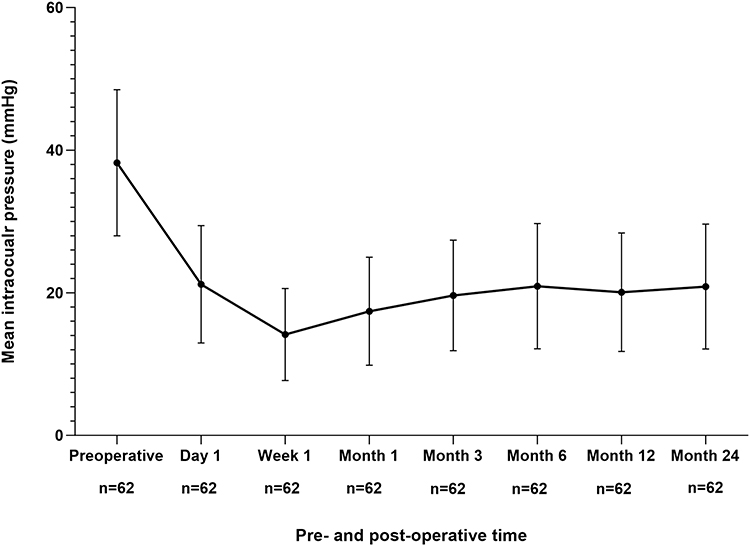 |
Figure 1 Mean and standard deviation of intraocular pressure for eyes following micropulse transscleral cyclophotocoagulation. |
The median number of medications taken by the patients was 3.0 (2.0, 3.0) preoperatively, which decreased to a median of 2.0 (0.0, 3.0) by the time of their final visit (P<0.001). Preoperatively, only 12.9% of eyes were medication-free, but this improved significantly to 32.3% post-surgery. Out of the 62 eyes, 31 (50%) had a decrease in the number of IOP-lowering medications after surgery (Table 3).
 |
Table 3 Number of Eyes Receiving Antiglaucoma Medication at Preoperative and at the 24-month Postoperative |
The BCVA preoperatively and at month 24 postoperatively were 2.70 (0.70, 3.70) and 2.70 (0.98, 3.95) LogMAR, respectively. There was no significant difference in BCVA after the surgery (P=0.625).
Success Rate and Postoperative Complications
The 24-month follow-up revealed a cumulative success rate of 77.4% (48 out of 62 eyes, Figure 2). Three eyes, two with uncontrolled IOP after primary congenital glaucoma surgeries, one after JOAG surgery, underwent a second MP-TSCPC treatment, resulting in their reclassification as failures. Nevertheless, following the second treatment, all of them experienced a significant reduction in IOP.
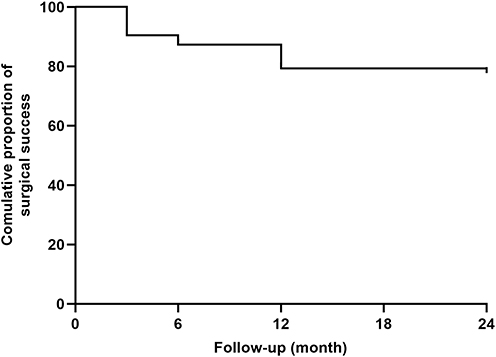 |
Figure 2 Kaplan-Meier analysis showed the estimated rates of success in controlling intraocular pressure during the follow-up. |
During the study period, a total of 25 complications occurred in 24 eyes (Table 4), inclusive of mydriasis (10 eyes, 16.1%), conjunctival hemorrhage (9 eyes, 14.5%), mild anterior chamber inflammation (1 eye, 1.6%), hyphema (1 eye, 1.6%), mild ciliary body detachment (3 eyes, 4.8%), and limited choroidal detachment (1 eye, 1.6%). All complications developed within one month postoperatively. Furthermore, the majority of these complications resolved gradually with pharmacologic treatment. Excluding eyes with no light perception at baseline, no patients had wipeout or a visual acuity decrease of more than 2 Snellen lines postoperatively. No other vision-threatening complications were present, such as suprachoroidal hemorrhage, vitreous hemorrhage, or phthisis bulbi.
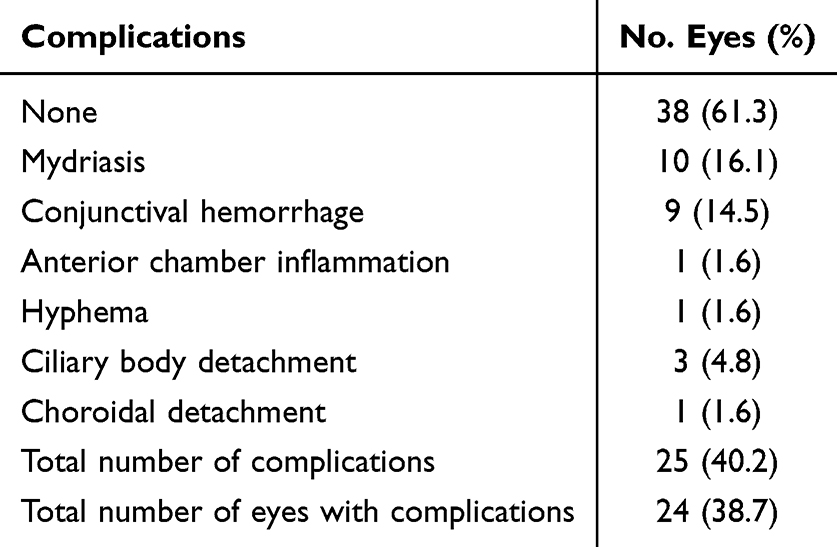 |
Table 4 Postoperative Complications of Patients Over 24 Months of Follow-Up |
Discussion
This is the first multicenter study from Mainland China to evaluate the long-term efficacy and safety of MP-TSCPC for refractory glaucoma. Our report demonstrated that the procedure was effective and well-tolerated. After 24 months of follow-up, treatment was successful in 77.4% of eyes, with significant reductions in both IOP and the requirement for antiglaucoma medications. Mild postoperative complications were observed in 24 eyes (38.7%), all of which resolved completely after treatment.
Previous studies have shown that MP-TSCPC has good efficacy in treatment of refractory glaucoma.14,16 Chen et al observed that out of 60 eyes treated with MP-TSCPC, the success rate was 75.0% at the 24-month follow-up, with an average reduction in IOP of 46.5%.16 Similarly, Crom et al evaluated 141 eyes from 136 Caucasian glaucoma patients and found success rates of 72.3% and 80% at 12 and 24 months, respectively.14 In support of the above results, the current study demonstrated a 42.7% decrease in IOP and an 77.4% success rate at the 24-month mark following MP-TSCPC. This suggests the efficacy of MP-TSCPC among individuals in Mainland China was equivalent to that reported in prior studies.
Furthermore, we observed a 50% reduction in the need for antiglaucoma medications, with the median dropping from 3.0 to 2.0 medications at 24 months after MP-TSCPC. These outcomes align closely with earlier studies, which demonstrated a decline in the average number of medications from 3.6±1.4 before intervention to 3.1±1.4 at month 12,24 and from 3.8±0.2 at baseline to 2.6±1.4 at month 24.16 Fewer medications are positively correlated with patient adherence and quality of life.25 The ability of MP-TSCPC to lower IOP and reduce the need for medication suggests that it may be a viable treatment option for individuals with uncontrolled glaucoma who are already using the maximum tolerated topical with or without systemic antiglaucoma medications.
No major complications, such as hypotony, were observed following the treatment. The most frequent issues were mydriasis and conjunctival hemorrhage, affecting 16.1% and 14.5% of eyes, respectively. But these were successfully resolved with pilocarpine or topical steroids, consistent with the findings of previous studies.14,17,24 During the first month after surgery, three eyes developed ciliary body detachment and one eye had choroidal detachment. To the best of our knowledge, these complications have not been previously described after MP-TSCPC. The reason for this may be the variation in laser effects among individuals, despite adequate energy provision. Further study is required to explore this possibility.
In our study, 3 out of 62 eyes needed to undergo retreatment of MP-TSCPC and were classified as failures, consistent with findings in previous studies.12,26–28 After retreatment, all of these eyes achieved successful treatment. This supports previous research suggesting that repeated MP-TSCPC is a safe and effective option for patients when the initial treatment fails.17
The study possesses several strengths. It is the first to present outcomes of MP-TSCPC in a Mainland Chinese population with a full two-year follow‑up. The multicenter design enhances the generalizability of the findings, while the prospective nature ensures high data integrity. Furthermore, the absence of patient loss to follow‑up and the availability of complete outcome data at 24 months reinforce the reliability and robustness of the results. However, the study also had some limitations. Firstly, the study enrolled only Mainland Chinese patients, which limits the generalizability of the findings. Secondly, there was a lack of comparative data to validate the effectiveness of this surgical method in comparison to traditional glaucoma surgery, consistent with its design as a descriptive study rather than a hypothesis-testing trial. Thirdly, the treatment success criterion, defined as a >20% IOP reduction from baseline or medication reduction with stable IOP, has inherent limitations. While this criterion is widely used in prior MP-TSCPC studies to ensure cross-study comparability,14,16,17 it does not account for absolute IOP levels or individualized target IOP. Finally, excluding patients who needed non-MP-TSCPC secondary treatments during follow-up may lead to a slight overestimation of the single initial MP-TSCPC success rate.
Conclusion
In summary, our study demonstrated that, after 24 months of follow-up, MP-TSCPC is a safe and effective treatment for lowering IOP and reducing the need for antiglaucoma medications in patients with refractory glaucoma from Mainland China. These findings support MP-TSCPC as a favorable treatment option for patients with uncontrollable IOP despite maximum tolerated medical therapy, or failed glaucoma surgery.
Ethical Approval
This study complied with the principles of the Declaration of Helsinki and conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. It was approved by the Ethics Committee of Zhongshan Ophthalmic Center (approval ID: 2022KYPJ225). All participants provided written informed consent prior to undergoing any surgical intervention.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Science and Technology Program of Guangzhou, China (2024A03J0250 and 2023A03J0908), Guangdong Basic Research Center of Excellence for Major Blinding Eye Diseases Prevention and Treatment (2024-PIZC-016), the National Natural Science Foundation of China (82571203), and Guangzhou Regional Clinical High-Tech Project (2026P-GX005). The funding/support organizations had no role in the design or conduct of this research.
Disclosure
The authors report no conflicting interest in this work.
References
1. Steinmetz JD, Bourne RRA, Briant PS. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9(2):e144–10. doi:10.1016/S2214-109X(20)30489-7
2. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
3. Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
4. Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern®. Ophthalmology. 2021;128:71–P150.
5. Gedde SJ, Chen PP, Muir KW, et al. Primary Angle-Closure Disease Preferred Practice Pattern®. Ophthalmology. 2021;128(1):P30–P70. doi:10.1016/j.ophtha.2020.10.021
6. Chen MF, Kim CH, Coleman AL. Cyclodestructive procedures for refractory glaucoma. Cochrane Database Syst Rev. 2019;3(3):Cd012223. doi:10.1002/14651858.CD012223.pub2
7. Dastiridou AI, Katsanos A, Denis P, et al. Cyclodestructive Procedures in Glaucoma: a Review of Current and Emerging Options. Adv Ther. 2018;35(12):2103–2127. doi:10.1007/s12325-018-0837-3
8. Kosoko O, Gaasterland DE, Pollack IP, et al. Long-term outcome of initial ciliary ablation with contact diode laser transscleral cyclophotocoagulation for severe glaucoma. The Diode Laser Ciliary Ablation Study Group. Ophthalmology. 1996;103(8):1294–1302. doi:10.1016/S0161-6420(96)30508-3
9. Ramli N, Htoon HM, Ho CL, et al. Risk factors for hypotony after transscleral diode cyclophotocoagulation. J Glaucoma. 2012;21(3):169–173. doi:10.1097/IJG.0b013e318207091a
10. Tan AM, Chockalingam M, Aquino MC, et al. Micropulse transscleral diode laser cyclophotocoagulation in the treatment of refractory glaucoma. Clin Exp Ophthalmol. 2010;38(3):266–272. doi:10.1111/j.1442-9071.2010.02238.x
11. Ma A, Swy Y, Wong JKW. Micropulse laser for the treatment of glaucoma: a literature review. Survey Ophthalmol. 2019;64(4):486–497. doi:10.1016/j.survophthal.2019.01.001
12. Aquino MC, Barton K, Tan AM, et al. Micropulse versus continuous wave transscleral diode cyclophotocoagulation in refractory glaucoma: a randomized exploratory study. Clin Exp Ophthalmol. 2015;43(1):40–46. doi:10.1111/ceo.12360
13. Emanuel ME, Grover DS, Fellman RL, et al. Micropulse Cyclophotocoagulation: initial Results in Refractory Glaucoma. J Glaucoma. 2017;26(8):726–729. doi:10.1097/IJG.0000000000000715
14. de Crom R, Slangen C, Kujovic-Aleksov S, et al. Micropulse Trans-scleral Cyclophotocoagulation in Patients With Glaucoma: 1- and 2-Year Treatment Outcomes. J Glaucoma. 2020;29(9):794–798. doi:10.1097/IJG.0000000000001552
15. Ariga M, Nivean, Nivean PD, et al. Micropulse trans-scleral diode laser cyclophotocoagulation in refractory glaucoma: an initial experience in Indian eyes. Intl Ophthalmol. 2021;41(8):2639–2645. doi:10.1007/s10792-021-01697-1
16. Chen HS, Yeh PH, Yeh CT, et al. Micropulse transscleral cyclophotocoagulation in a Taiwanese population: 2-year clinical outcomes and prognostic factors. Graefes Arch Clin Exp Ophthalmol. 2022;260(4):1265–1273. doi:10.1007/s00417-021-05468-7
17. Lim EJY, Aquino CM, Lun KWX, et al. Efficacy and Safety of Repeated Micropulse Transscleral Diode Cyclophotocoagulation in Advanced Glaucoma. J Glaucoma. 2021;30(7):566–574. doi:10.1097/IJG.0000000000001862
18. de Crom R, Kujovic-Aleksov S, Webers CAB, et al. Long-Term Treatment Outcomes of Micropulse Transscleral Cyclophotocoagulation in Primary and Secondary Glaucoma: a 5-Year Analysis. Ophthalmol Ther. 2025;14:323–335. doi:10.1007/s40123-024-01080-0
19. Chavez MP, Guedes GB, Pasqualotto E, et al. Micropulse Transscleral Laser Treatment Versus Continuous Wave Transscleral Cyclophotocoagulation for the Treatment of Glaucoma or Ocular Hypertension: a Meta-Analysis. J Glaucoma. 2025;34(8):575–584. doi:10.1097/IJG.0000000000002583
20. Lin F, Hu B, Ling Q, et al. Efficacy and safety of micropulse transscleral cyclophotocoagulation in the treatment of refractory glaucoma: a prospective multicenter observational study. Clin Experiment Ophthalmol. 2024;42:527–531.
21. European Glaucoma Society Terminology and Guidelines for Glaucoma. Chapter 2: classification and terminologySupported by the EGS Foundation: part 1: foreword; Introduction; Glossary; Chapter 2 Classification and Terminology. Br J Ophthalmol. 2017;101(5):73–127. doi:10.1136/bjophthalmol-2016-EGSguideline.002
22. Lee EJ. Monitoring Progression in Advanced Glaucoma. Ophthalmology. 2020;127(8):1053. doi:10.1016/j.ophtha.2020.03.002
23. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509–516.
24. Radhakrishnan S, Wan J, Tran B, et al. Micropulse Cyclophotocoagulation: a Multicenter Study of Efficacy, Safety, and Factors Associated With Increased Risk of Complications. J Glaucoma. 2020;29(12):1126–1131. doi:10.1097/IJG.0000000000001644
25. Sleath B, Blalock SJ, Carpenter DM, et al. Ophthalmologist-patient communication, self-efficacy, and glaucoma medication adherence. Ophthalmology. 2015;122(4):748–754. doi:10.1016/j.ophtha.2014.11.001
26. Williams AL, Moster MR, Rahmatnejad K, et al. Clinical Efficacy and Safety Profile of Micropulse Transscleral Cyclophotocoagulation in Refractory Glaucoma. J Glaucoma. 2018;27(5):445–449. doi:10.1097/IJG.0000000000000934
27. Al Habash A, AlAhmadi AS. Outcome Of MicroPulse(®) Transscleral Photocoagulation In Different Types Of Glaucoma. Clin Ophthalmol. 2019;13:2353–2360. doi:10.2147/OPTH.S226554
28. Tekeli O, Köse HC. Outcomes of micropulse transscleral cyclophotocoagulation in primary open-angle glaucoma, pseudoexfoliation glaucoma, and secondary glaucoma. EurJ Ophthalmol. 2021;31(3):1113–1121. doi:10.1177/1120672120914231
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.