Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Microplasma radiofrequency technology combined with triamcinolone improved the therapeutic effect on Chinese patients with hypertrophic scar and reduced the risk of tissue atrophy
Received 12 January 2016
Accepted for publication 8 March 2016
Published 10 May 2016 Volume 2016:12 Pages 743—747
DOI https://doi.org/10.2147/TCRM.S104109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Shui Yu, Hengjin Li
Department of Dermatology, Chinese People’s Liberation Army General Hospital and Hainan Branch, Sanya, People’s Republic of China
Objective: The current study aimed to assess the value of microplasma radiofrequency technology combined with triamcinolone for the therapy of Chinese patients with hypertrophic scar.
Methods: A total of 120 participants with hypertrophic scars were enrolled in the current study. Participants were divided into two groups based on sex, and then randomly and evenly divided into four groups (Groups A, B, C, and D). Participants in Group A received microplasma radiofrequency technology combined with triamcinolone. Participants in Group B received microplasma radiofrequency technology combined with normal saline. Participants in Groups C and D received triamcinolone (40 and 10 mg/mL) injected directly into scar. Experienced physicians evaluated the condition of scars according to the Vancouver Scar Scale 1 month before and after the therapy.
Results: There was no difference in age, sex, area, height and location of scars, and Vancouver Scar Scale scores before the therapy between any groups (P>0.05 for all). Vancouver Scar Scale scores after the therapy were significantly lower than those before the therapy in all groups (P<0.05 for all). Vancouver Scar Scale scores after the therapy in Group A were significantly lower than those after the therapy in Groups B and C (P<0.05 for all). Vancouver Scar Scale scores after the therapy in Group B were significantly higher than those after the therapy in Group C (P<0.05 for all) and similar to those after the therapy in Group D (P>0.05 for all). Incidences of tissue atrophy after the therapy were significantly lower in Groups A and B than in Group C (P<0.05 for all) and similar among Groups A, B, and D (P>0.05 for all).
Conclusion: Microplasma radiofrequency technology combined with triamcinolone improved the therapeutic effect on Chinese patients with hypertrophic scar and reduced the risk of tissue atrophy compared with the use of either microplasma radiofrequency technology or triamcinolone injection alone.
Keywords: hypertrophic scar, microplasma radiofrequency technology, tissue atrophy, triamcinolone
Introduction
Hypertrophic scar is the excessive deposition of extracellular matrix, including collagen, as the result of the wound healing process going out of control and extending beyond the skin surface but limited to the original scope, accompanied by congestion, itch, pain, and other clinical symptoms. Because of the effect of hypertrophic scar on body appearance and impairment of functional activity, dermatologists are in a continued pursuit to seek an effective and safe therapy for hypertrophic scar. Current therapies for hypertrophic scar, such as drug, surgery, isotope, laser, pressure, and cryotherapy, not only have limited efficacy but also lead to secondary damage including tissue atrophy.1–4 The most widely used glucocorticoid injection is difficult to operate, and injecting glucocorticoids unevenly or into normal tissue often results in tissue atrophy and other adverse reactions.5,6 So, it is necessary to explore a new method to import glucocorticoids into scar tissue. Microplasma radiofrequency technology, a recently presented therapy for hypertrophic scars, can stimulate the plasma and form microchannels in the corium layer.7–9 Triamcinolone is a long-acting glucocorticoid with good efficacy in eliminating hypertrophic scar, and it can be imported into the scar tissue through microplasma radiofrequency technology.1 Comprehensive therapy combining two or more kinds of conventional therapies has received more and more attention in recent years because of its better therapy efficacy and lower rates of adverse reactions. There are very few studies on the combined use of microplasma radiofrequency technology and triamcinolone in the therapy of hypertrophic scar all over the world, especially in the People’s Republic of China. The current study aimed to assess the value of microplasma radiofrequency technology combined with triamcinolone for the therapy of hypertrophic scar.
Methods
Study participants
A total of 120 Chinese participants with hypertrophic scars were enrolled in the current study. They were aged older than 18 years, and half of them were male and the other half were female. They had no basic diseases or contraindications to glucocorticoids. All their hypertrophic scars were present for >1 year without significantly fading for >6 months and were higher than the skin surface and were associated with the symptoms of congestion, itch, and pain. These hypertrophic scars were located in head and face, chest and back, and limbs, respectively. Participants were divided into two groups based on sex, and then randomly and evenly divided into four groups (Groups A, B, C, and D). Participants in Group A received microplasma radiofrequency technology combined with triamcinolone (40 mg/mL). Participants in Group B received microplasma radiofrequency technology combined with normal saline. Participants in Group C received triamcinolone (40 mg/mL) injected directly and slowly into the scar.8 Participants in Group D received triamcinolone (10 mg/mL) injected directly and slowly into the scar.10 A course of therapy included the standard therapy administered five times with an interval of 1 month between each administration for all groups. The study protocol was approved by the Ethics Committee of Chinese People’s Liberation Army General Hospital and performed according to the Declaration of Helsinki. Each participant provided written informed consent to be included in the study.
Microplasma radiofrequency technology
A plasma beam scar therapy apparatus (Accent XL; Alma Lasers Ltd., Caesarea, Israel) with a roller head was used. The roller head was rolled on the skin from different directions five times to form microchannels in the scar tissue. The apparatus was used at 60–70 W and 4–6 mA.7 Triamcinolone (Group A) or normal saline (Group B) was smeared on the rolling region and imported into scar tissue by microplasma radiofrequency technology.
Vancouver Scar Scale
Experienced physicians evaluated the condition of scars according to the Vancouver Scar Scale 1 month before and after the therapy. Vancouver Scar Scale is a 15-point scoring system scored as follows: color (0, similar to the rest of skin; 1, shallower than the rest of skin; 2, mixed color; 3, deeper than the rest of skin), vascular distribution (0, similar to the rest of skin; 1, pink; 2, red; 3, purple), thickness (0, normal; 1, >0–1 mm; 2, >1–2 mm; 3, >2–3 mm; 4, >4 mm), and flexibility (0, normal; 1, soft [with deformation under the least pressure]; 2, supple [with deformation under pressure]; 3, hard [with resistance to pressure and without deformation]; 4, bending [with retraction during stretching like a rope]; 5, contracture [with permanent shortening leading to distortion and disability]). They were summed for a total Vancouver Scar Scale score ranging from 0 to 15, and a higher score indicated a heavier scar.11 Participants were asked not to tell the dermatologists their grouping situation.
Statistical analysis
Continuous variables were presented as mean (standard deviation) or median (interquartile range). Categorical variables were presented as number (percentage). Continuous variables were compared using Student’s t-test or Mann–Whitney U-test. Categorical variables were compared using chi-square test. A P-value <0.05 was deemed as statistically significant. Statistical analysis was performed using SPSS 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Participant features and Vancouver Scar Scale scores before and after the therapy are shown in Table 1. There was no difference in age, sex, area, height and location of scars, and Vancouver Scar Scale scores before the therapy between any groups (P>0.05 for all). Vancouver Scar Scale scores after the therapy were significantly lower than those before the therapy in all groups (P<0.05 for all). Vancouver Scar Scale scores after the therapy in Group A were significantly lower than those after the therapy in Groups B, C, and D (P<0.05 for all). Vancouver Scar Scale scores after the therapy in Group B were significantly higher than those after the therapy in Group C (P<0.05 for all). Vancouver Scar Scale scores after the therapy in Group B were similar to those after the therapy in Group D (P>0.05 for all). Incidences of tissue atrophy after the therapy were significantly lower in Groups A and B than in Group C (P<0.05 for all). Incidences of tissue atrophy after the therapy were similar among Groups A, B, and D (P>0.05 for all).
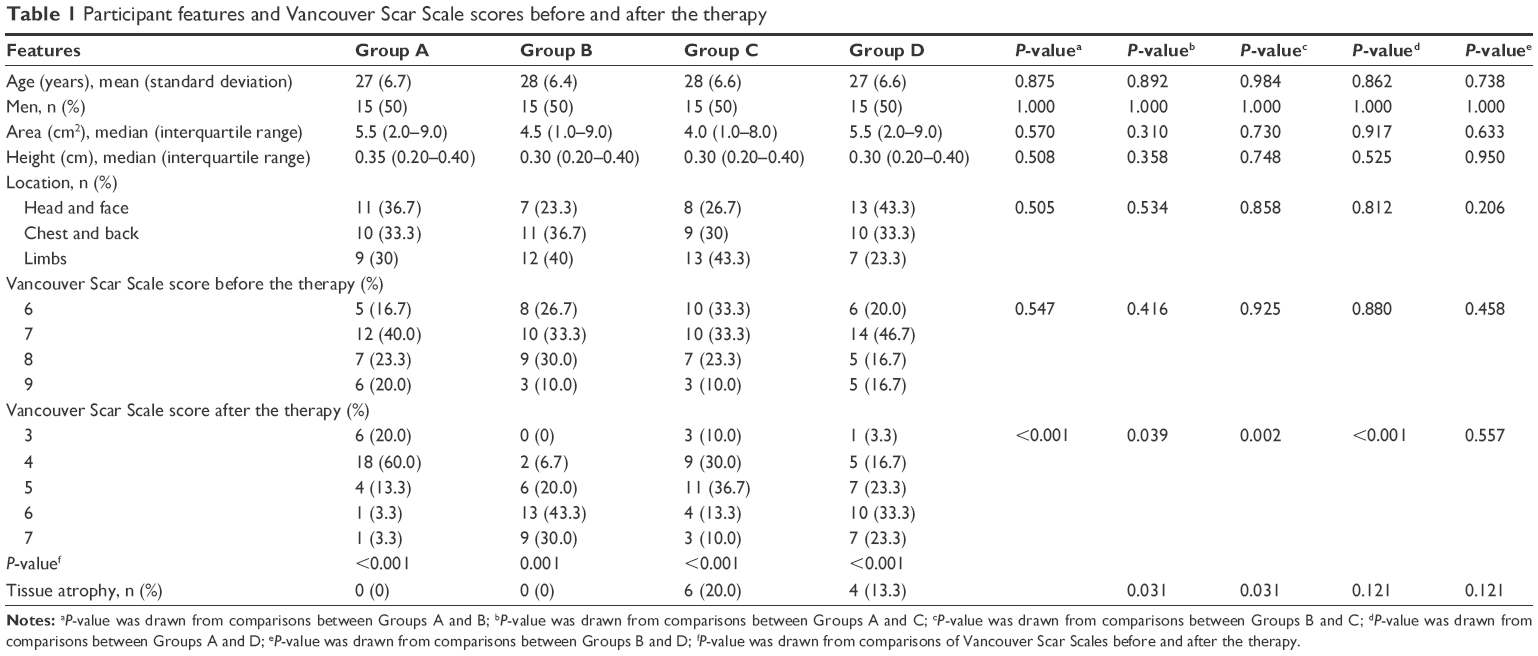 | Table 1 Participant features and Vancouver Scar Scale scores before and after the therapy |
Discussion
Lately, microplasma radiofrequency technology has become commercially available and clinically acceptable as novel fractional lasers in dermatology.7 Its roller head has several rows of equidistantly and closely arrayed needles, leaving a thin layer of air space above the skin surface. Plasma is similar to the gaseous state, including some ionized molecules, and very sensitive to electromagnetic fields, and radiofrequency wave stimulates the spark plasma between the needles and skin surface. Various effects can be achieved, from vaporization to heating of scar tissue, through the interaction between spark plasma and scar tissue. Spark plasma mildly peels the cuticular layer and forms the microchannel in corium layer. The depth and diameter of microchannel depend on the energy of radiofrequency and duration of pulse, and these are generally 100–150 and 80–120 μm, respectively. The multipoint radiofrequency technology improves the traditional radiofrequency technology, which only produces high-energy flake discharge, and increases the temperature in each tiny focus with stimulating spark plasma.8
Scar is a natural part of dermal healing process and consists of a network of fibrous collagen tissue laid down in response to injury to the dermis. In some genetically susceptible individuals, the process of scar tissue formation is excessive, and there is an oversecretion of collagen.2 The use of glucocorticoids injection is, to date, the core therapy available for the management of excessive tissue production in scar. As the most effective regimen for management of hypertrophic scar, the therapeutic value of triamcinolone on hypertrophic scar has been reported in the literature.1 Triamcinolone inhibits the expression of vascular endothelial growth factor to restrain the fibroblast proliferation, increases the collagen breakdown, and promotes the scar tissue degradation.12 However, the most commonly applied triamcinolone injection is difficult to operate, and injecting triamcinolone unevenly or into normal tissue often leads to adverse reactions including tissue atrophy and poor management of hyperplastic scar.5,6 Microplasma radiofrequency technology and its thermal effect stimulate fibroblasts to synthesize the new collagen fibers and matrixes in scar tissue on the one hand and rearrange the disordered collagen fibers to make scar tissue closer to normal skin on the other hand.9 Moreover, microplasma radiofrequency technology stimulates the plasma and forms the microchannel in corium layer, and triamcinolone can be absorbed effectively and evenly by scar tissue through microplasma radiofrequency technology.1 The combined use of microplasma radiofrequency technology and triamcinolone can achieve good therapeutic effect for hypertrophic scar and help avoid obvious adverse reactions including tissue atrophy. The current study applied the objective and effective Vancouver Scar Scale as evaluation standard for hypertrophic scar and provided evidence for the therapeutic effect and safety of microplasma radiofrequency technology combined with triamcinolone on improvement of Chinese patients with hypertrophic scar superior to use of either microplasma radiofrequency technology or triamcinolone alone.
Conclusion
Collectively, the current study demonstrated that microplasma radiofrequency technology combined with triamcinolone improved the therapeutic effect on Chinese patients with hypertrophic scar and reduced the risk of tissue atrophy compared with use of either microplasma radiofrequency technology or triamcinolone injection alone.
Disclosure
The authors report no conflicts of interest in this work.
References
Berman B, Flores F. The therapy of hypertrophic scars and keloids. Eur J Dermatol. 1998;8(8):591–595. | ||
Jalali M, Bayat A. Current use of steroids in management of abnormal raised skin scars. Surgeon. 2007;5(3):175–180. | ||
Waibel J, Beer K. Ablative fractional laser resurfacing for the treatment of a third-degree burn. J Drugs Dermatol. 2009;8(3):294–297. | ||
Sklar LR, Burnett CT, Waibel JS, Moy RL, Ozog DM. Laser assisted drug delivery: a review of an evolving technology. Lasers Surg Med. 2014;46(4):249–262. | ||
Kelly AP. Medical and surgical therapies for keloids. Dermatol Ther. 2004;17(2):212–218. | ||
Mutalink S. The therapy of keloids and hypertrophic scars. Indian J Dermatol Venereol. 2005;71(1):3–8. | ||
Xin F, Li-hong L, Alexiades-Armenakas M, et al. Histological and electron microscopic analysis of fractional micro-plasma radio-frequency technology effects. J Drugs Dermatol. 2013;12(11):1210–1214. | ||
Halachmi S, Orenstein A, Meneghel T, Lapidoth M. A novel fractional micro-plasma radio-frequency technology for the therapy of facial scars and rhytids: a pilot study. J Cosmet Laser Ther. 2010;12(5):208–212. | ||
Foster KW, Moy RL, Fincher EF. Advances in plasma skin regeneration. J Cosmet Dermatol. 2008;7(3):169–179. | ||
Carvalhaes SM, Petroianu A, Ferreira MA, de Barros VM, Lopes RV. Assessment of the treatment of earlobe keloids with triamcinolone injections, surgical resection, and local pressure. Rev Col Bras Cir. 2015;42(1):9–13. | ||
Sood RF, Hocking AM, Muffley LA, et al. Genome-wide association study of postburn scarring identifies a novel protective variant. Ann Surg. 2015;262(4):563–569. | ||
Russell SB, Russell JD, Trupin JS. Hydrocortisone induction of system A amino acid transport in human fibroblasts from normal dermis and keloid. J Biol Chem. 1984;259:11464–11469. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.