Back to Journals » Clinical Interventions in Aging » Volume 21
Microbial Colonization and Potential Bacterial Translocation of High-Flow Nasal Cannula Circuits During Prolonged Use in Elderly Hospitalized Patients: A Prospective Observational Study
Authors Du Y, Yang Y ![]() , Zhou Y
, Zhou Y ![]() , Han X, Yu Z, Zhao Q, Ding Y
, Han X, Yu Z, Zhao Q, Ding Y ![]() , Lu Z
, Lu Z ![]() , Zhang Q, Cheng Y, Xu G
, Zhang Q, Cheng Y, Xu G ![]()
Received 18 December 2025
Accepted for publication 27 May 2026
Published 5 June 2026 Volume 2026:21 589882
DOI https://doi.org/10.2147/CIA.S589882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yingzhen Du,1– 3,* Yang Yang,4,* Yu Zhou,5,* Xinjie Han,3,6,7,* Zhenghao Yu,3,6 Qiang Zhao,8 Yongkai Ding,1,3 Zhi Lu,9 Qi Zhang,9 Yanshuang Cheng,10 Guogang Xu6
1Department of Disease Prevention and Control, The second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Fever Clinic, The second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Medical School of Chinese PLA, Chinese PLA General Hospital, Beijing, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, The second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 5Department of Clinical Laboratory, National Clinical Research Center for Geriatric Diseases, The Second Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China; 6Health Management Institute, The second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 7Department of Respiratory and Critical Care Medicine, The Eighth Medical Center, Chinese PLA General Hospital, Beijing, People’s Republic of China; 8Department of Clinical Laboratory, The First Medical Center, Chinese PLA General Hospital, Beijing, People’s Republic of China; 9Department of Automation & Institute for Brain and Cognitive Sciences, Tsinghua University, Beijing, People’s Republic of China; 10Department of Hepatobiliary and Pancreatic Surgery, First Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanshuang Cheng; Guogang Xu, Email [email protected]; [email protected]
Background: High-flow nasal cannula (HFNC) oxygen therapy provides effective respiratory support with enhanced comfort and airway humidification. Long-term use of HFNC is increasingly adopted in respiratory oxygen therapy for elderly patients, yet Catheter-related bacterial translocation and colonization risks remain unstudied.
Methods: This prospective study enrolled 102 elderly hospitalized patients (mean age: 94.2 ± 5.1 years old) receiving HFNC therapy. Microbial samples were collected from the HFNC circuits and analyzed to assess respiratory circuit colonization. The optimal tubing replacement interval was determined through ROC curve analysis. Additionally, for one patient who developed pulmonary infection after receiving HFNC, microbial homology was evaluated between microorganisms cultured isolates from the lower respiratory tract and those from the HFNC tubing using whole-genome sequencing and antibiotic resistance gene profiling.
Results: Microbial colonization of HFNC tubing was detected in 56.9% (58/102) of patients, with prevalent pathogens including Filamentous fungi (25.9%), Methicillin-resistant Staphylococcus aureus (20.7%), and Streptococcus spp. (13.8%). The median time to tubing colonization was 136.2 ± 58.2 days. Pulmonary infections occurred significantly more frequently in the culture-positive group (37/58=63.8%) compared to the culture-negative group (17/44=38.6%; P = 0.016). ROC analysis identified 90.5 days as the study-specific optimal cutoff associated with tubing contamination. In the case study, Pseudomonas aeruginosa was isolated from both the patient’s lower respiratory tract and HFNC tubing. Homology analysis confirmed the strains were identical (ST2069, O6 serotype) and harbored six shared resistance genes (aph(3′)-IIb, crpP, catB7, blaPAO, blaOXA-488, fosA).
Conclusion: Prolonged HFNC use was associated with substantial microbial colonization of the circuit in elderly hospitalized patients. Replacing HFNC tubing at approximately 90-day intervals may reduce microbial colonization and pneumonia risk in elderly patients during HFNC therapy. The HFNC tube circuit serves as a potential reservoir for pathogenic translocation, highlighting the importance of timely tubing replacement and microbial monitoring of the tube in infection prevention protocols.
Keywords: high-flow nasal cannula, HFNC, elderly hospitalized patients, microbial colonization, tubing replacement, ROC curve analysis, prospective observational study
Introduction
High-Flow Nasal Cannula(HFNC) oxygen therapy is a respiratory support treatment method that continuously delivers regulated and relatively constant oxygen concentrations, temperatures, and humidity, with high flow rates (8 to 80 L/min) of inhaled gas.1 Compared with traditional oxygen therapy and Noninvasive Positive Pressure Ventilation (NPPV), HFNC offers improved comfort and airway humidification, making it the optimal respiratory support choice for awake elderly patients with secretion clearance impairments.2,3 Consequently, long-term use of HFNC is increasingly common in oxygen therapy for geriatric respiratory care.4 In current clinical practice, HFNC has become a frequently used noninvasive respiratory support modality and is often positioned between conventional oxygen therapy and noninvasive ventilation(NIV). One study including patients aged over 75 years specifically used HFNC in elderly patients with acute respiratory failure who had a poor response to conventional oxygen therapy or were intolerant to NIV.4 However, evidence from mechanical ventilation circuits, oxygen humidifiers, and other respiratory care devices suggests that moisture-containing respiratory equipment may act as a reservoir for microbial persistence and cross-contamination.5,6 Thus, prolonged HFNC therapy in elderly patients carries an elevated risk of device-related respiratory infections, particularly due to tubing contamination.7 Currently, there is limited research on HFNC tubing circuit microbial colonization or translocation and infection risks, and no established guidelines exist for optimal tubing replacement intervals.
To address this gap, this study aims to investigate microbial colonization patterns in HFNC circuits used by elderly patients and assess the associated risk of respiratory infections. Also determine the time threshold for significant tubing contamination using microbial monitoring and ROC curve analysis thus establish evidence-based recommendations for the optimal tubing replacement schedule. The findings will provide clinical data to support standardized HFNC management, helping to minimize infection risks and improve patient outcomes in long-term use of HFNC respiratory support.
Methods
Study Design and Patients’ Enrollment
This prospective observational study enrolled 113 elderly hospitalized patients receiving HFNC therapy at a medical center of the Chinese PLA General Hospital between June 1, 2022, and July 28, 2023. Eligibility criteria for inclusion were as follows: (1) Age >65 years; (2) Daily HFNC use ≥18 hours; (3) Ability to provide lower respiratory tract samples; (4) Availability of complete medical records. The exclusion criteria were as follows: (1) Incomplete medical records; (2) Change in HFNC tubing or ventilation method during follow-up; (3) Confirmed pulmonary infection at enrollment; (4) Inability to cooperate with follow-up; (5) Death during the study period. This study was designed as a prospective single-arm descriptive study, with the primary outcome being the positivity rate of microbial cultures from HFNC tubing samples. Based on pilot observations, the expected positivity rate was estimated to be approximately 50%. Using a two-sided α of 0.05 and an allowable error (δ) of 0.10, the required effective sample size was calculated to be 97 patients according to the formula for estimating a single proportion. To ensure adequate study precision and to account for an anticipated 15% loss to follow-up or missing data, we planned to enroll 118 elderly patients receiving HFNC therapy. During the study period, a total of 113 patients met the inclusion and exclusion criteria. The study protocol was approved by the Ethics Committee of the Chinese PLA General Hospital (Approval No. S2020-25601). This study adheres to the Declaration of Helsinki, and all participants signed informed consent forms before being enrolled in the study.
Clinical Data Collection, Microbial Sampling and Analysis
Demographic and clinical data were collected from enrolled patients, including gender, age, smoking history, comorbidities, complete blood count and biochemistry results. HFNC tubing samples were collected weekly from all participants. Microbiological specimens were collected from three sites of the HFNC circuit system: the humidification chamber, the heated breathing circuit at 6–8 cm distal to the humidification chamber (distal tubing), and the heated breathing circuit at 6–8 cm proximal to the nasal cannula (proximal tubing). For sampling of the humidification chamber, a sterile cotton swab was used to collect liquid from the chamber. For sampling of the breathing circuit, a sterile swab moistened with sterile normal saline was inserted into the inner lumen and rotated along the inner wall for five full turns over a depth of 6–8 cm. The collected specimens were inoculated onto blood agar plates and China blue agar plates, and incubated at 37°C for 48 h for microbiological culture and surveillance analysis. Routine clinical microbiological cultures were performed mainly to detect common hospital-acquired pathogens. Specifically, HFNC tubing samples were cultured for common aerobic bacteria and fungi recoverable under standard laboratory conditions, including yeasts and molds. These cultures were used to evaluate the microbial colonization rate and the spectrum of clinically relevant organisms in the HFNC tubing. Systematic screening for viruses, anaerobic bacteria, mycobacteria, or other atypical pathogens was not performed.
Monitoring of Pulmonary Infections and Microbial Homology Analysis
Pulmonary infection during the follow-up period was considered a secondary outcome, and the incidence of pulmonary infections was analyzed. The diagnosis of pulmonary infection was made with reference to the Chinese expert consensus on the diagnosis and treatment of pneumonia in the elderly (2024 Edition).8 Specifically, pulmonary infection was recognized based on a combination of new or worsening respiratory symptoms/signs, new radiographic infiltrates, and supportive laboratory or microbiological evidence.
For patients who developed pulmonary infections, microbial homology analysis was conducted between pathogens isolated from lower respiratory tract specimens (sputum) and those from HFNC tubing cultures. Genomic DNA was extracted from two Pseudomonas aeruginosa clinical isolates and subjected to whole-genome sequencing (WGS) on the Illumina NovaSeq platform with 150 bp paired-end reads. Raw sequencing reads were quality-filtered to remove low-quality bases, adapter sequences, and ambiguous nucleotides prior to assembly. De novo genome assembly was performed using SPAdes (v3.15.5). Multilocus sequence typing (MLST), O-antigen serotyping, and antimicrobial resistance gene profiling were subsequently performed using web-based tools available on the Center for Genomic Epidemiology (CGE) platform (http://www.genomicepidemiology.org/services/). Specifically, sequence types were assigned using the CGE MLST 2.0 tool with the Pseudomonas aeruginosa-specific MLST scheme; O-serogroup prediction was performed using PAst 1.0, which classifies isolates based on a BLAST analysis of the O-specific antigen (OSA) gene cluster; and acquired antimicrobial resistance genes were identified using ResFinder 4.6.0, with a minimum nucleotide identity threshold of 90% and a minimum gene length coverage of 60%. For SNP-based clonal relatedness analysis, quality-filtered paired-end reads were mapped to the complete reference genome of P. aeruginosa PAO1 (NCBI RefSeq accession NC_002516.2) using the Snippy pipeline (v4.6.0). A core genome SNP alignment was constructed using snippy-core across all isolates. To minimize false-positive SNP calls attributable to horizontal gene transfer, recombination regions were identified and masked using Gubbins (v3.3.1), with FastTree employed as the phylogenetic tree builder. Pairwise core genome SNP distances were subsequently calculated from the recombination-filtered alignment using snp-dists. In accordance with validated genomic thresholds established for nosocomial P. aeruginosa outbreak investigations, isolates differing by ≤ 25 recombination-filtered core genome SNPs were classified as clonally related, whereas those exceeding this threshold were considered genetically distinct.9,10
ROC Curve Analysis
Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal timing for tubing replacement based on the occurrence of microbial contamination during treatment. The presence or absence of microbial growth in tubing cultures served as the classification criterion. For each candidate cutoff value of tubing-use duration, sensitivity was calculated as the proportion of culture-positive patients correctly identified, and specificity was calculated as the proportion of culture-negative patients correctly identified. Sensitivity, specificity, and the area under the curve (AUC) were calculated to identify the most predictive time threshold for tubing contamination.
Statistical Analysis
Baseline characteristics of the study population, including demographic and clinical data, were summarized using descriptive statistics. Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed variables are presented as mean ± standard deviation (SD), whereas non-normally distributed variables are presented as median (interquartile range, IQR). Categorical variables were expressed as frequencies and percentages. ROC curve analysis was employed to evaluate the optimal timing for tubing replacement using microbial positivity in HFNC tubing samples as the classification criterion. The analysis included calculation of sensitivity, specificity, and area under the curve (AUC) to establish the contamination time threshold. The optimal cutoff point for tubing replacement was determined by maximizing Youden’s index from the ROC curve. All analyses were conducted using SAS (version 9.4) and R (version 3.6.3) statistical software. A two-tailed p-value <0.05 was considered statistically significant.
Results
Patient Demographic and Clinical Characteristics
Of the initial 113 enrolled patients, 11 were excluded from the final analysis, including 1 due to incomplete medical records, 4 due to change in HFNC tubing or ventilation modality during follow-up, 2 due to confirmed pulmonary infection at enrollment, 2 due to inability to complete follow-up, and 2 due to death during the study period. In this study, most participants were very elderly bedridden patients who required long-term oxygen therapy, improvement of airway mucus clearance, and optimization of pulmonary mechanics. All included patients were conscious and able to cooperate with HFNC treatment, and prolonged HFNC use was determined by the treating physicians based on clinical evaluation. The mean age was 94.2 ± 5.1 years. The median follow-up time of this cohort was 67 days. There were 58 patients (58/102=56.9%) in the microbial culture positive group and 44 patients (44/102=43.1%) in the culture negative group. Demographic and clinical characteristics of enrolled patients are presented in Tables 1–4 separately. The study flow is shown in Figure 1.
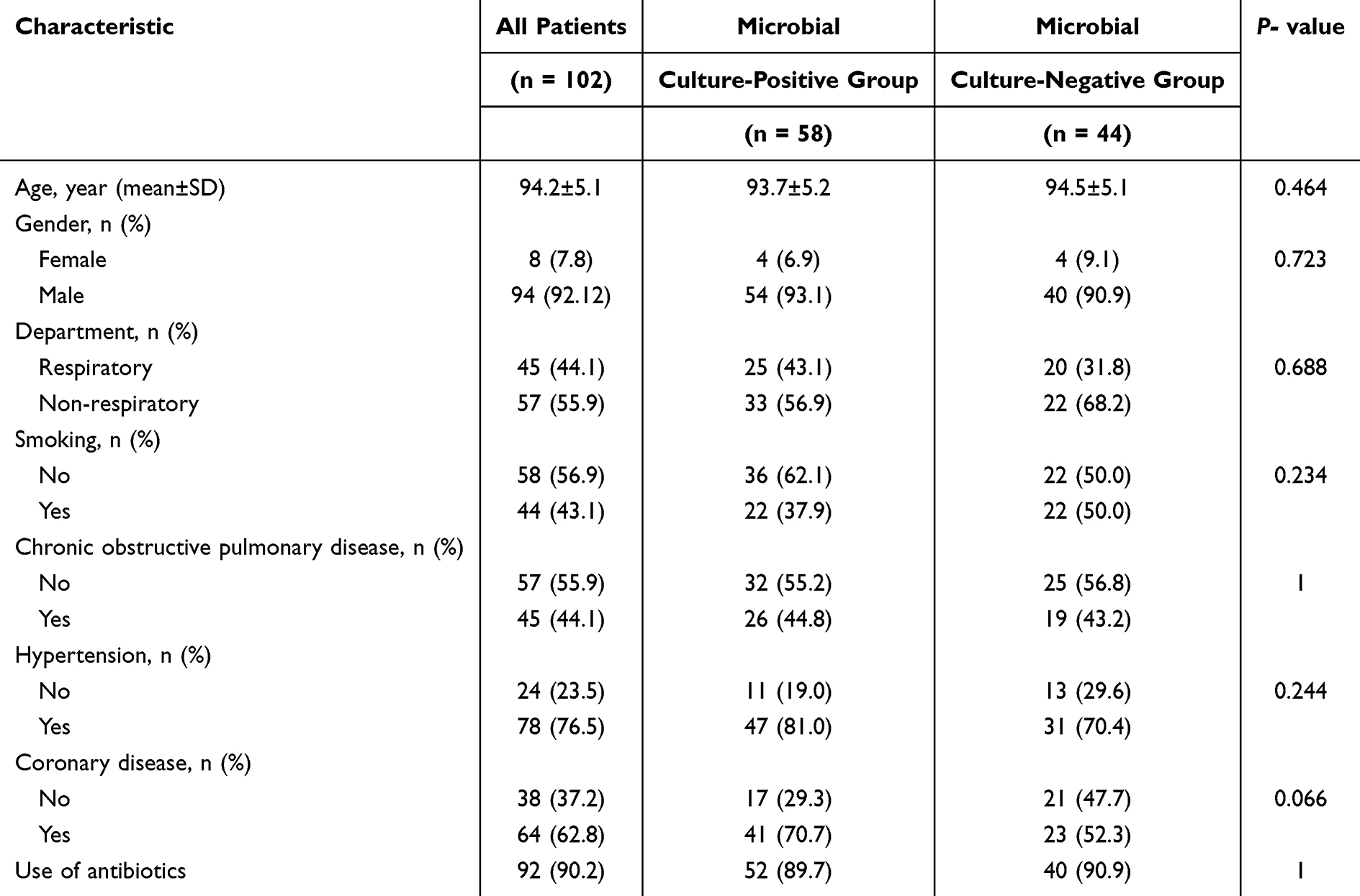 |
Table 1 Baseline Demographic Characteristics of the Enrolled Patients |
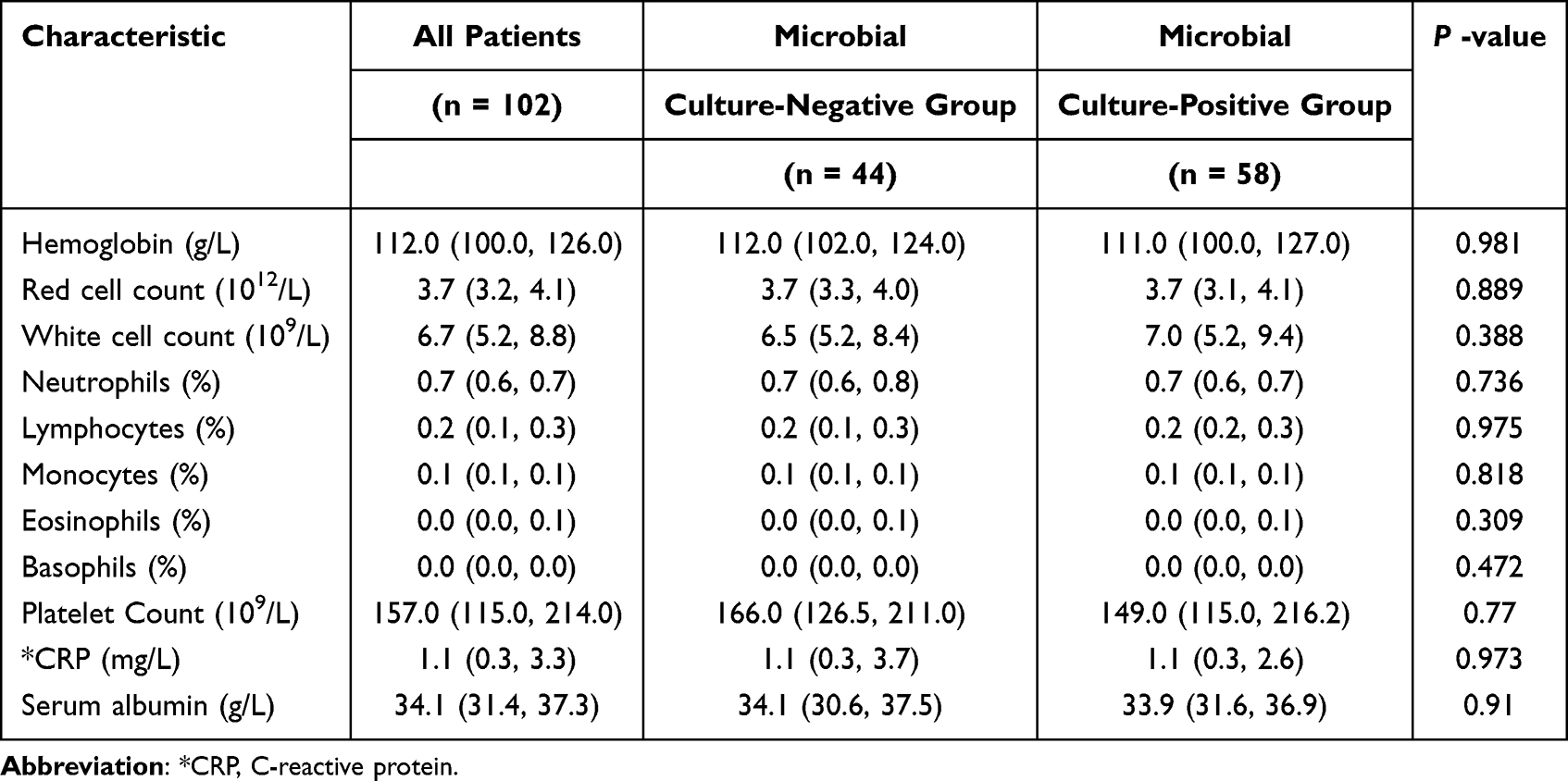 |
Table 2 Laboratory Characteristics of the Enrolled Patients |
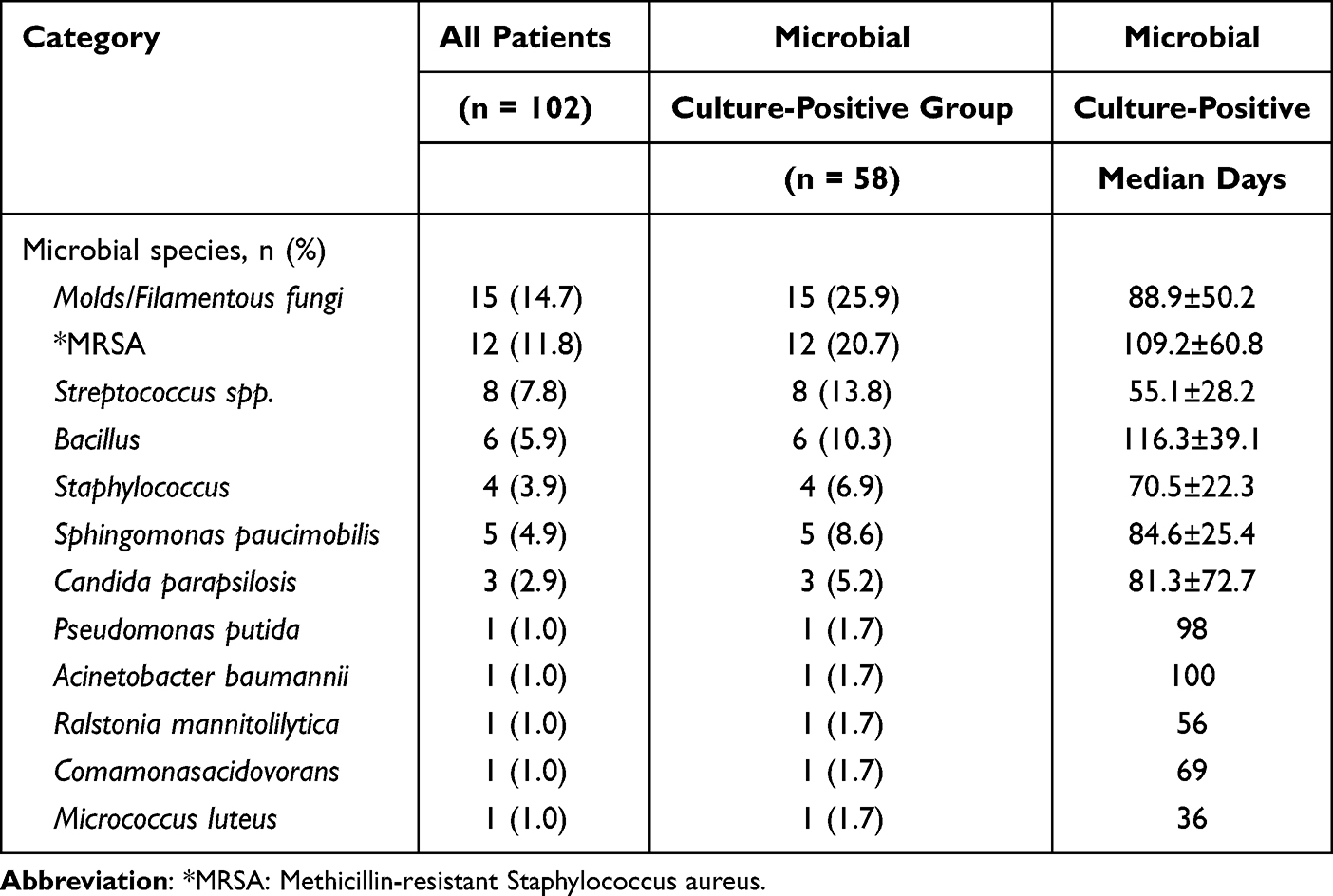 |
Table 3 Types of Cultured Microorganisms and Duration of Positive Cultures |
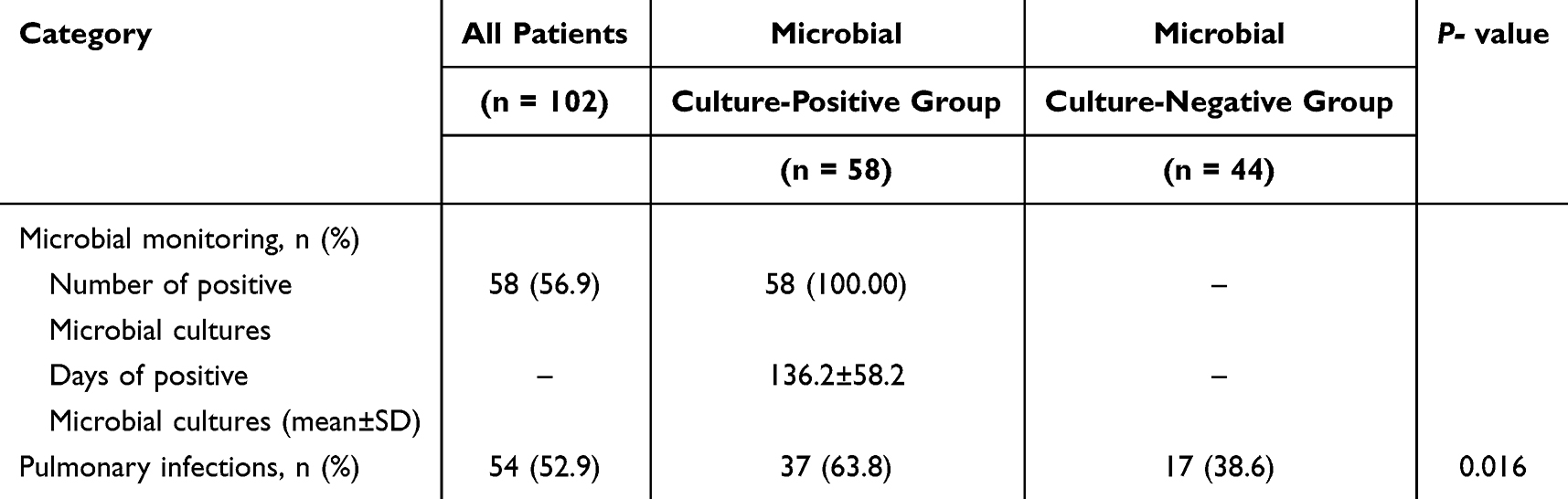 |
Table 4 Microbial Surveillance of HFNC Tubing and Incidence of Pulmonary Infections |
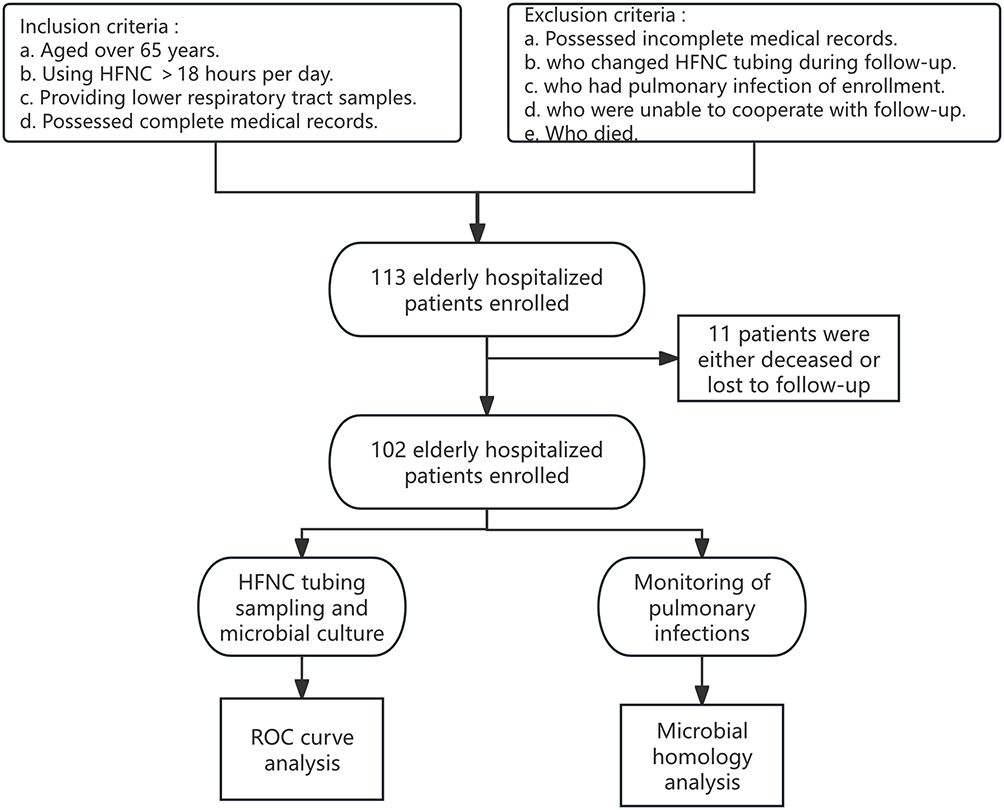 |
Figure 1 The flowchart of study. |
Microbial Contamination Patterns
As Figure 2 and Table 3 shown: Microbial colonization was detected in 56.9% (58/102) of HFNC tubing samples. The pathogens identified were: Molds/Filamentous fungi (25.9%, median days: 88.9±50.2), Methicillin-resistant Staphylococcus aureus (MRSA) (20.7%, median days: 109.22±60.8), Streptococcus spp. (13.8%, median days: 55.1±28.2), Bacillus (10.3%, median days: 116.3±39.1), Staphylococcus (6.9%, median days: 70.5±22.3), Sphingomonas paucimobilis (8.6%, median days: 84.6±25.4), Candida parapsilosis (5.2%, median days: 81.3±72.7), Pseudomonas putida (1.7%, median days: 98.0), Acinetobacter baumannii (1.7%, median days: 100.0), Ralstonia mannitolilytica (1.7%, median days: 56.0), Comamonasacidovorans (1.7%, median days: 69.0), Micrococcus luteus (1.7%, median days: 36.0). The mean time to microbial detection in HFNC tubing was 136.2 ±58.2 days (Table 4).
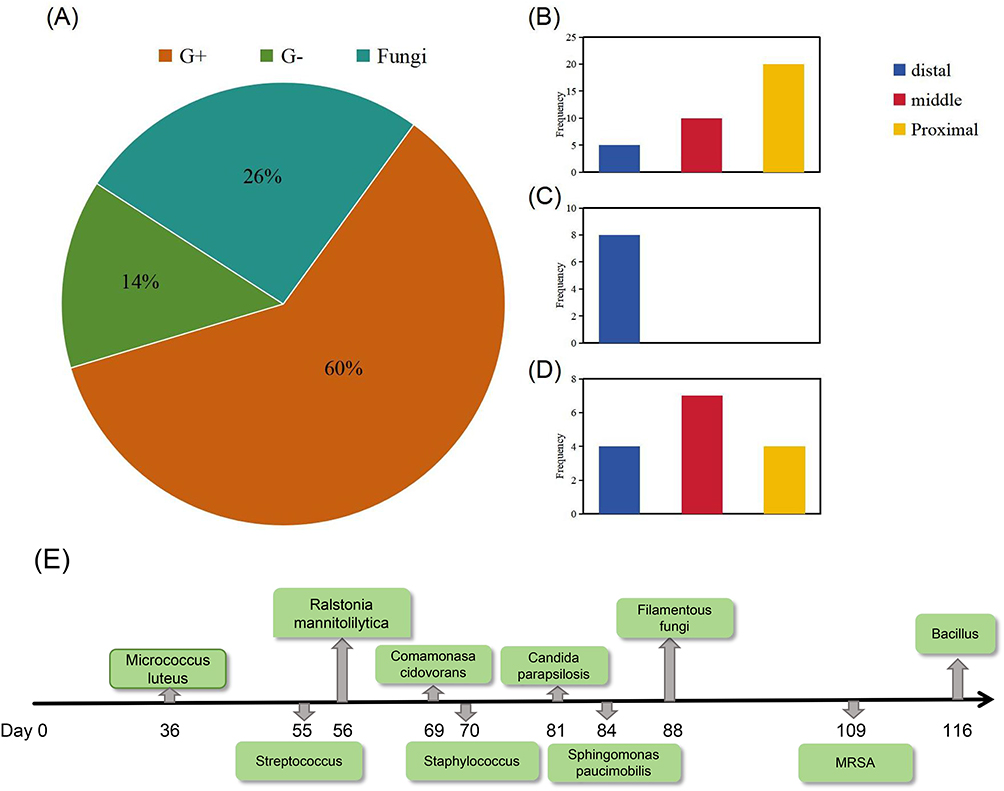 |
Figure 2 Microbial surveillance status and microbial species. (A) Pie chart of microbial species in culture-positive samples. (B) Detection of Gram-positive bacteria at different positions of the HFNC circuit. (C) Detection of Gram-negative bacteria at different positions of the HFNC circuit. (D) Detection of fungi at different positions of the HFNC circuit. (E) Microbial timeline of the positive microbial culture group. |
Analysis of Laboratory Test Results Between Microbial Culture Positive and Negative Groups
There was no statistically significant difference in the blood test results between the microbial culture positive and negative groups (P > 0.05) (Figure 3). Specifically, there were no differences observed in the following parameters: Hemoglobin, Red cell count, White cell count, Neutrophils percentage, Lymphocytes percentage, Monocytes percentage, Eosinophils percentage, Basophils percentage, Platelet Count, CRP (C-reactive protein), Serum albumin, NPAR (Neutrophil percentage-to-albumin ratio), NLR (Neutrophil-to-lymphocyte ratio), PLR (Platelet-to-lymphocyte ratio), and MLR (Monocyte-to-lymphocyte ratio).
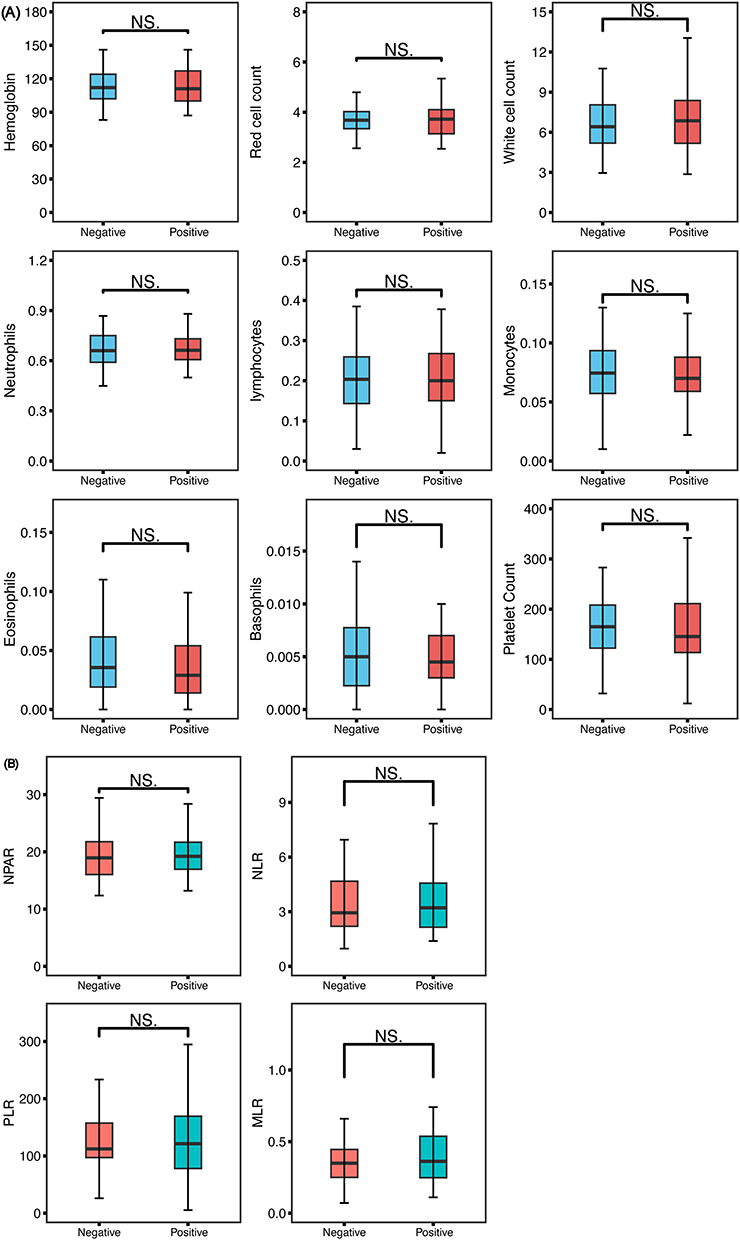 |
Figure 3 Laboratory parameter analysis of patients in the positive and negative microbial culture groups. (A) Boxplot of blood test parameters and microbial culture results. (B) Boxplot of blood test parameters ratios and microbial culture results. (P>0.05.). Abbreviations: NS, Not significant; NPAR, Neutrophil percentage-to-albumin ratio; NLR, Neutrophil-to-lymphocyte ratio; PLR, Platelet-to-lymphocyte ratio; MLR, Monocyte-to-lymphocyte ratio. |
Optimal Tubing Replacement Timing Analysis
ROC curve analysis identified day 90.5 as the study-specific optimal cutoff associated with tubing contamination (AUC=0.767, 95% CI: 0.669–0.864) (Figure 4). This timepoint demonstrated balanced sensitivity and specificity for predicting microbial contamination while effectively minimizing infection risk.
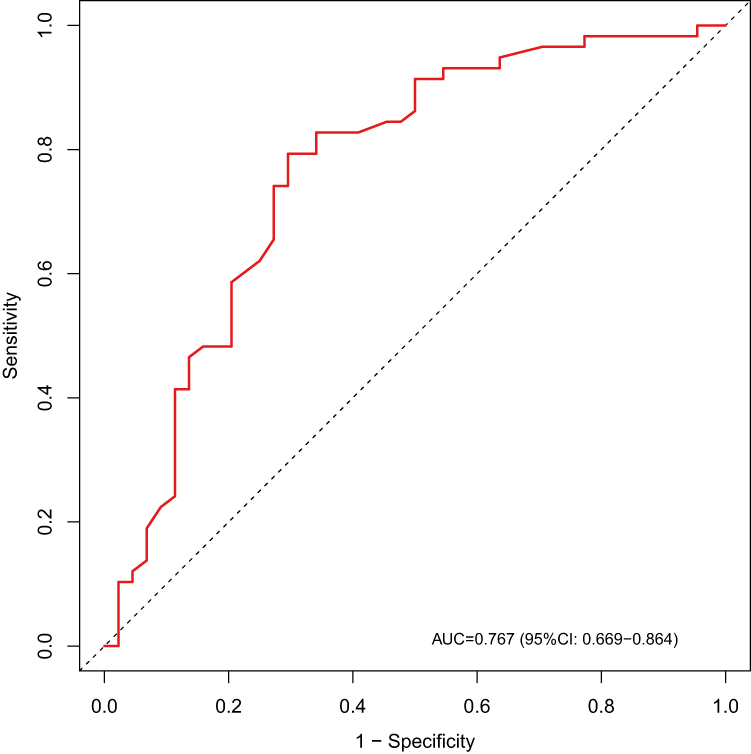 |
Figure 4 ROC Curve analysis. (Using the positivity of tubing system cultures as the classification criterion, the time threshold for tubing contamination was determined to be 90.5 days.) (AUC= 0.767; 95% CI: 0.669–0.864). |
Incidence of Pulmonary Infections and Microbial Homology Analysis
The incidence of pulmonary infections among HFNC patients was 52.9% (54/102) (Table 4). In one 92-year-old male patient with pneumonia (Figure 5 demonstrates the patient’s chest CT findings), we identified genetically homologous Pseudomonas aeruginosa strains in both sputum and HFNC tubing samples. BLAST analysis confirmed that both strains were Pseudomonas aeruginosa ST2069, O6 serotype, carrying six shared resistance genes: aph(3′)-IIb, crpP, catB7, blaPAO, blaOXA-488, and fosA (Figures 6 and 7). Using the Pseudomonas aeruginosa PAO1 reference genome as the reference strain for SNP-based phylogenetic analysis, a total of 20,535 SNP sites were identified. Compared with the reference genome, the two strains differed by 20,534 and 20,530 SNP sites, respectively, while only six SNP site differences were found between the two strains. Therefore, the two strains were preliminarily determined to be homologous.
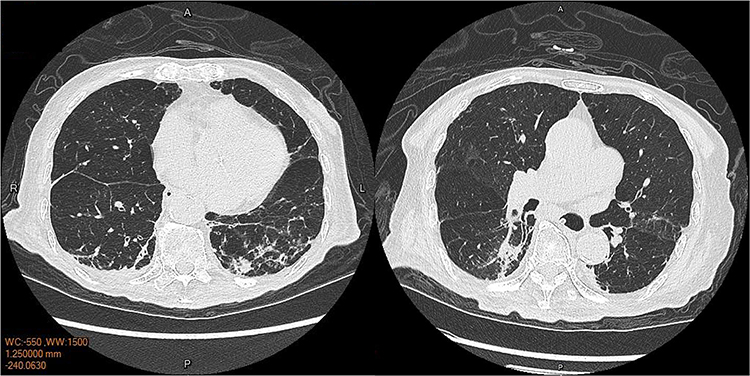 |
Figure 5 Chest CT of a pneumonia patient after HFNC application. (A: Anterior, P: Posterior, R: Right, L: Left). |
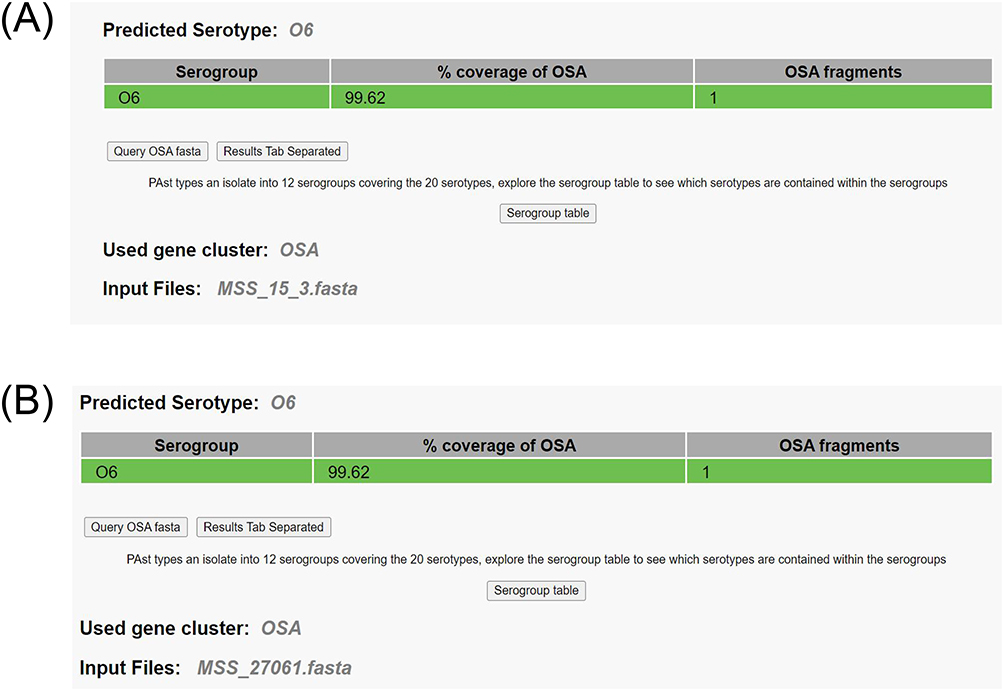 |
Figure 6 The sequence-based serotyping of Pseudomonas aeruginosa isolated from the patient’s lower respiratory tract samples (A) and the ventilator tubing (B) (Both isolates (MSS_15_3 and MSS_27061) were predicted as serogroup O6, with 99.62% coverage of the O-specific antigen (OSA) locus, based on the OSA gene cluster). |
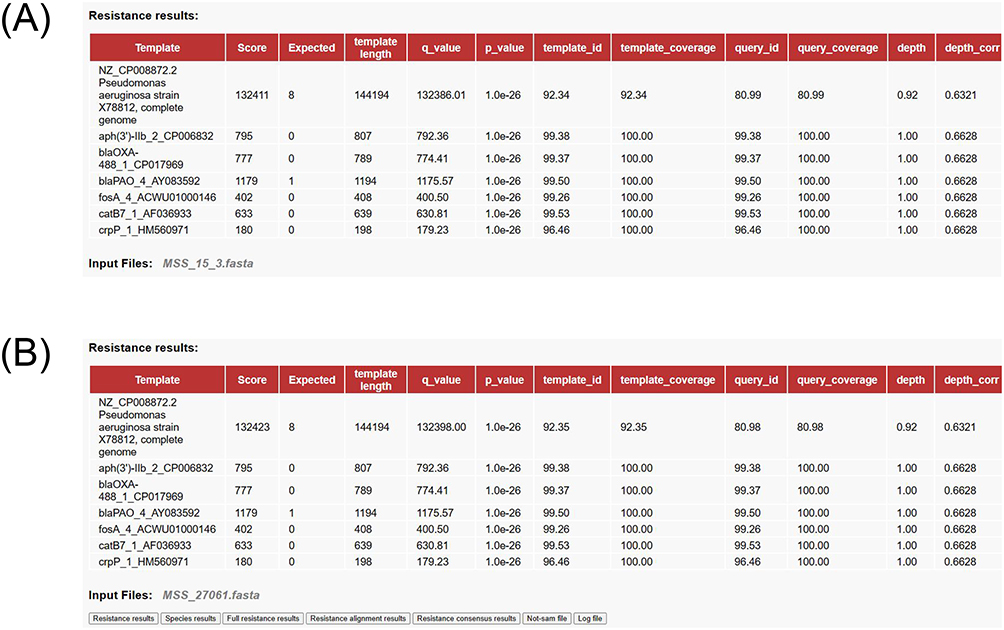 |
Figure 7 Antimicrobial resistance gene profiling of Pseudomonas aeruginosa isolated from the patient’s lower respiratory tract samples (A) and the ventilator tubing (B) (Both isolates (MSS_15_3 and MSS_27061) harbored an identical set of six resistance genes: aph(3′)-IIb, blaOXA-488, blaPAO, fosA, catB7, and crpP). |
Discussion
This prospective study systematically evaluates microbial colonization patterns in elderly patients receiving HFNC therapy. By integrating microbial surveillance data with ROC curve analysis, we aim to establish evidence-based tubing replacement protocols. Furthermore, microbial homology analysis of paired lower respiratory tract and tubing samples from pneumonia cases will elucidate potential transmission pathways. These findings will inform optimized infection-control strategies for HFNC use in geriatric populations.
The concept of HFNC was first introduced in the 1990s, when researchers began exploring the potential of delivering high-flow oxygen via nasal cannula.11 Early studies primarily focused on the effects of HFNC in patients with acute respiratory failure, demonstrating its ability to significantly improve oxygenation and respiratory efficiency.12 As respiratory therapy technologies advanced, the design and functionality of HFNC devices have undergone continuous refinement, particularly in terms of flow control, humidification, and heating.13,14 Studies have shown that HFNC yields significant benefits in conditions such as acute respiratory distress syndrome (ARDS) and acute exacerbations of chronic obstructive pulmonary disease (COPD).15 In the 2010s, the clinical application of HFNC gradually expanded to the neonatal and pediatric populations, particularly in the treatment of neonatal respiratory distress syndrome.16 During the COVID-19 pandemic, HFNC received widespread attention, with many hospitals adopting it as a crucial respiratory support method to reduce the need for intubation in critically ill patients.17 Today, HFNC represents a standard respiratory intervention, with ongoing innovations refining its clinical implementation. Although HFNC tubing is generally designated by manufacturers as a single-use disposable component, and prolonged use or reuse after cleaning is usually not recommended, prolonged HFNC support may still be encountered in real-world geriatric practice, particularly among very elderly bedridden patients with chronic respiratory support needs. In this setting, clinicians face a practical gap between manufacturer recommendations and long-term care demands. At present, there is no clear evidence-based consensus regarding the optimal replacement interval for HFNC tubing during prolonged use in elderly hospitalized patients.
Multiple studies have demonstrated comparable efficacy between High-Flow Nasal Cannula HFNC and Non-Invasive Ventilation (NIV) in preventing post-extubation respiratory failure and reintubation among patients with both hypoxemic and hypercapnic respiratory failure.18 As a non-invasive alternative to invasive mechanical ventilation, HFNC significantly reduces risks associated with intubation and ventilator-associated complications.19 However, the extended exposure of HFNC circuits to environmental pathogens raises concerns about microbial colonization risks, particularly when improper circuit maintenance or connection contamination occurs.
Our investigation revealed a 56.9% microbial culture positivity rate in HFNC circuits, with predominant isolates including Filamentous fungi, methicillin-resistant Staphylococcus aureus, and Streptococcus spp. This contamination rate may be related to several factors in our study population: 1) the inclusion of elderly patients with diminished self-care capacity, predisposing them to frequent nasal cannula dislodgement and subsequent environmental pathogen exposure; and 2) prolonged HFNC utilization durations. Notably, the identified microorganisms correspond with typical nosocomial pathogens,20 mirroring ventilator-associated pneumonia (VAP) microbiology profiles where Gram-negative pathogens (Pseudomonas aeruginosa and Acinetobacter spp.) predominate, alongside Gram-positive organisms like Staphylococcus aureus.21
Current evidence indicates that extended application of HFNC therapy may increase susceptibility to secondary pulmonary infections.22,23 Notably, a critical knowledge gap persists regarding the relationship between microbial colonization in HFNC circuits and subsequent respiratory infections in clinical populations. Our findings demonstrate a significantly elevated incidence of pulmonary infections in patients with positive microbial cultures compared to those with negative cultures. This statistically significant difference underscores the clinical relevance of circuit contamination, particularly in elderly patients requiring prolonged HFNC therapy where age-related immunosenescence may amplify infection risks.24 To substantiate this observation, we conducted microbial homology analysis in a representative case involving a 92-year-old male pneumonia patient. Comparative BLAST analysis revealed genetic homology between Pseudomonas aeruginosa strains isolated from both the patient’s sputum and the HFNC circuit. The observed homology between Pseudomonas aeruginosa isolated from the lower respiratory tract and HFNC tubing demonstrates strain identity, but does not establish the exact direction of transmission. The contamination may have been: ① from the HFNC circuit to the patient, ② from the patient to the HFNC circuit, ③ related to shared environmental or healthcare-associated contamination. This microbiological evidence supports the hypothesis that colonized circuits can serve as reservoirs for pathogenic microorganisms to translocation, potentially initiating lower respiratory tract infections.20
Current infection control protocols classify the HFNC system (comprising nasal cannula, heated humidification chamber, and connecting tubing) as single-use disposable medical devices intended for short-term applications.25,26 However, critical gaps persist in clinical guidance regarding system replacement frequency during extended therapeutic use. Neither international guidelines nor expert consensus documents provide evidence-based recommendations for maintenance protocols in prolonged HFNC therapy scenarios. Our ROC curve analysis identified 90.5 days as the study-specific optimal cutoff associated with tubing contamination. From a clinical perspective, this finding may be more appropriately interpreted as suggesting a replacement interval of approximately 90 days, pending validation in larger prospective studies. These data provide preliminary evidence to inform standardized management protocols, potentially mitigating infection risks associated with circuit colonization.
Limitation
There are three principal limitations warrant consideration: 1) The modest sample size from a single-center cohort necessitates validation through large-scale multicenter trials. 2) Conducted within a geriatric healthcare setting (mean age 94.2 ± 5.1 years old), findings may not extrapolate to younger populations due to age-related immunological differences. 3) Preliminary homology analysis (n=1 pneumonia case) between Pseudomonas aeruginosa isolates from sputum and circuitry requires confirmation through expanded microbial sampling. Future prospective studies with larger sample sizes are needed to validate these results, for example: Establish causal relationships through longitudinal microbial surveillance; Validate replacement intervals across diverse clinical populations; Investigate cost-benefit ratios of replacement protocols.
Conclusion
Prolonged HFNC use was associated with substantial microbial colonization of the circuit in elderly hospitalized patients. Our findings suggest that HFNC tubing replacement at approximately 90-days intervals may be considered as a preliminary strategy for prolonged use in elder hospitalized patients. Although this threshold still requires validation in larger further prospective investigations. The HFNC circuit serves as a potential site of translocation for pathogenic colonization in elderly patients, particularly those with immunosenescence, necessitating stringent microbial surveillance and protocolized tubing replacement as critical components of infection control strategies.
Data Sharing Statement
The data are available from the corresponding author on reasonable request (Guogang Xu: [email protected]).
Ethical Approval and Consent to Participate
This research was approved and waived the consent by the Ethics Committee of Chinese PLA General Hospital (NO. S2020-25601). All participants signed informed consent forms before being enrolled in the study. All authors confirm this study adheres to the Declaration of Helsinki. Clinical trial number: not applicable.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This retrospective study was supported by National Clinical Research Center for Geriatric Diseases Open Project: NCRCG-PLAGH-2022012 and NCRCG-PLAGH-2023004; Beijing Natural Science Foundation: L222014.
Disclosure
All authors in this study declare no competing conflicts.
References
1. Lewis SR, Baker PE, Parker R, Smith AF. High-flow nasal cannulae for respiratory support in adult intensive care patients. Cochrane Database Syst Rev. 2021;3(3):CD010172. doi:10.1002/14651858.CD010172.pub3
2. Oczkowski S, Ergan B, Bos L, et al. ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure. Eur Respir J. 2022;59(4):2101574. doi:10.1183/13993003.01574-2021
3. Zhao H, Wang H, Sun F, Lyu S, An Y. High-flow nasal cannula oxygen therapy is superior to conventional oxygen therapy but not to noninvasive mechanical ventilation on intubation rate: a systematic review and meta-analysis. Crit Care. 2017;21(1):184. doi:10.1186/s13054-017-1760-8
4. Carratala JM, Diaz-Lobato S, Brouzet B, et al. Efficacy and safety of high-flow nasal cannula therapy in elderly patients with acute respiratory failure. Pulmonology. 2024;30(5):437–14. doi:10.1016/j.pulmoe.2023.01.004
5. Yamashita K, Nishiyama T, Yokoyama T, Abe H, Manabe M. A comparison of the rate of bacterial contamination for prefilled disposable and reusable oxygen humidifiers. J Crit Care. 2005;20(2):
6. Coppadoro A, Bellani G, Foti G. Non-pharmacological interventions to prevent ventilator-associated pneumonia: a literature review. Respir Care. 2019;64(12):1586–1595. doi:10.4187/respcare.07127
7. Baldomero AK, Melzer AC, Greer N, et al. Effectiveness and harms of high-flow nasal oxygen for acute respiratory failure: an evidence report for a clinical guideline from the American College of Physicians. Ann Intern Med. 2021;174(7):952–966. doi:10.7326/M20-4675
8. Respiratory Branch of Chinese Geriatrics S. Chinese expert consensus on the diagnosis and treatment of pneumonia in the elderly (2024 Edition). Zhonghua Jie He He Hu Xi Za Zhi. 2025;48(1):18–34. doi:10.3760/cma.j.cn112147-20240611-00328
9. Romano-Bertrand S, Virieux-Petit M, Mauffrey F, Senn L, Blanc DS. Defining a genomic threshold for investigating Pseudomonas aeruginosa hospital outbreak. J Hosp Infect. 2025;161:119–129. doi:10.1016/j.jhin.2025.04.028
10. Grana-Miraglia L, Hu X, Volling C, et al. Genomic and epidemiological identification of Pseudomonas aeruginosa transmission chains and in hospital ICUs. Genome Biol. 2026;27(1). doi:10.1186/s13059-026-04005-1
11. Sreenan C, Lemke RP, Hudson-Mason A, Osiovich H. High-flow nasal cannulae in the management of apnea of prematurity: a comparison with conventional nasal continuous positive airway pressure. Pediatrics. 2001;107(5):1081–1083. doi:10.1542/peds.107.5.1081
12. Maia IS, Weigert RM, Mattei EDB, et al; Investigators R, the BA. High-flow nasal oxygen vs noninvasive ventilation in patients with acute respiratory failure: the RENOVATE randomized clinical trial. JAMA. 2025;333(10):875–890. doi:10.1001/jama.2024.26244
13. Frat JP, Marchasson L, Arrive F, Coudroy R. High-flow nasal cannula oxygen therapy in acute hypoxemic respiratory failure and COVID-19-related respiratory failure. J Intensive Med. 2023;3(1):20–26. doi:10.1016/j.jointm.2022.07.005
14. Armarego M, Forde H, Wills K, Beggs SA. High-flow nasal cannula therapy for infants with bronchiolitis. Cochrane Database Syst Rev. 2024;3(3):CD009609. doi:10.1002/14651858.CD009609.pub3
15. Agusti A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
16. Nolasco S, Manti S, Leonardi S, Vancheri C, Spicuzza L. High-flow nasal cannula oxygen therapy: physiological mechanisms and clinical applications in children. Front Med. 2022;9:920549. doi:10.3389/fmed.2022.920549
17. Attaway AH, Scheraga RG, Bhimraj A, Biehl M, Hatipoglu U. Severe covid-19 pneumonia: pathogenesis and clinical management. BMJ. 2021;372:n436. doi:10.1136/bmj.n436
18. Ni YN, Luo J, Yu H, et al. Can high-flow nasal cannula reduce the rate of reintubation in adult patients after extubation? A meta-analysis. BMC Pulm Med. 2017;17(1):142. doi:10.1186/s12890-017-0491-6
19. Tan D, Walline JH, Ling B, et al. High-flow nasal cannula oxygen therapy versus non-invasive ventilation for chronic obstructive pulmonary disease patients after extubation: a multicenter, randomized controlled trial. Crit Care. 2020;24(1):489. doi:10.1186/s13054-020-03214-9
20. Suleyman G, Alangaden GJ. Nosocomial fungal infections: epidemiology, infection control, and prevention. Infect Dis Clin North Am. 2021;35(4):1027–1053. doi:10.1016/j.idc.2021.08.002
21. Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med. 2020;46(5):888–906. doi:10.1007/s00134-020-05980-0
22. Pitre T, Zeraatkar D, Kachkovski GV, et al. Noninvasive oxygenation strategies in adult patients with acute hypoxemic respiratory failure: a systematic review and network meta-analysis. Chest. 2023;164(4):913–928. doi:10.1016/j.chest.2023.04.022
23. Petkar S, Wanjari D, Priya V. A comprehensive review on high-flow nasal cannula oxygen therapy in critical care: evidence-based insights and future directions. Cureus. 2024;16(8):e66264. doi:10.7759/cureus.66264
24. Muller-Werdan U, Nuding S, Ost M. Assessing inflammageing. Curr Opin Clin Nutr Metab Care. 2017;20(5):346–348. doi:10.1097/MCO.0000000000000391
25. Vega ML, Pisani L. Nasal high flow oxygen in acute respiratory failure. Pulmonology. 2021;27(3):240–247. doi:10.1016/j.pulmoe.2021.01.005
26. Rochwerg B, Einav S, Chaudhuri D, et al. The role for high flow nasal cannula as a respiratory support strategy in adults: a clinical practice guideline. Intensive Care Med. 2020;46(12):2226–2237. doi:10.1007/s00134-020-06312-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.