Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Metabolic Parameters in Patients with Prader-Willi Syndrome and DiGeorge Syndrome with Respect to Psychopathological Manifestation
Authors Krefft M ![]() , Frydecka D
, Frydecka D ![]() , Śmigiel R
, Śmigiel R ![]() , Misiak B
, Misiak B
Received 25 October 2019
Accepted for publication 17 January 2020
Published 14 February 2020 Volume 2020:16 Pages 457—463
DOI https://doi.org/10.2147/NDT.S236034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Maja Krefft,1 Dorota Frydecka,1 Robert Śmigiel,2 Błażej Misiak3
1Department of Psychiatry, Wroclaw Medical University, Wroclaw, Poland; 2Department of Pediatrics, Division of Pediatrics and Rare Disorders, Wroclaw Medical University, Wroclaw, Poland; 3Department of Genetics, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Maja Krefft
Department of Psychiatry, Wroclaw Medical University, 10 Pasteur Street, Wroclaw 51-367, Poland
Tel +48509457693
Email [email protected]
Purpose: The purpose of our study was to compare the metabolic parameters in two genetic syndromes with a proven high risk of developing psychiatric comorbidities. These comorbidities, especially mood and psychotic disorders, may be associated with a risk of obesity, type 2 diabetes and other components of metabolic syndrome regardless of antipsychotic treatment.
Patients and Methods: Two groups of children diagnosed with Prader - Willi syndrome (PWS) (n = 20) and DiGeorge syndrome (DGS) (n = 18), aged 7– 18 years, were enrolled. Behavioral symptoms and co-occurring psychopathological symptoms were assessed using the Child Behavior Checklist (CBCL). The levels of following biochemical parameters were measured: glucose, insulin, high-sensitivity C-reactive protein, total cholesterol, low- and high-density lipoproteins (LDL and HDL), triglycerides and non-HDL cholesterol. Additionally, the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was calculated.
Results: There were significantly higher levels of insulin and non-HDL in patients with PWS compared to those with DGS. The scores of four CBCL subscales (social problems, thought problems, delinquent behavior and aggressive behavior) were significantly higher in PWS patients. Higher scores of the CBCL-thought problems were associated with significantly higher levels of insulin as well as HOMA-IR.
Conclusion: Patients with PWS seem to be more prone to develop subclinical metabolic dysregulation, in terms of elevated non-HDL levels and insulin levels, compared to DGS patients. Altered insulin sensitivity, present in both groups, even though it is not a specific risk factor, might be related to thought problems associated with psychosis.
Keywords: rare disease, metabolic dysregulation, lipid, psychosis, psychopathology
Introduction
Metabolic alterations are widely described in the literature with respect to the psychosis-spectrum conditions.1 Both risk and clinical manifestations of psychosis are often associated with disturbances in the levels of various cardiometabolic parameters.2,3 This phenomenon is mostly attributed to environmental factors such as pharmacotherapy with antipsychotics or unhealthy lifestyle among patients.4 However, previous meta-analyses revealed that even patients at early stages of psychosis (including drug-naive patients) or mood disorders as well as at-risk individuals already present subclinical metabolic disturbances.2,5–8 Recent studies also indicate shared genetic backgrounds of severe mental disorders and metabolic conditions, including obesity and type 2 diabetes.9
It is important to note that certain genetic syndromes that are characterized by a number of psychiatric comorbidities are also associated with a risk of obesity, type 2 diabetes and other components of metabolic syndrome. Prader-Willi syndrome (PWS) is a rare genetic disorder occurring in 1:10,000–1:30,000 births with a lack of expression of genes inherited from the paternal chromosome 15q11-13 either from paternal deletion (75%), uniparental maternal disomy (mUPD) (20%) or as a result of other chromosomal anomalies.10,11 It is a multisystemic, neurodevelopmental disorder with frequently delayed motor and intellectual development and characteristic dysmorphic features such as almond-shaped eyes downturned mouth, narrow forehead and small hands and feet as well as distinctive appearance of further symptoms with age.10,12,13 At about 2–4 years of age, the first signs of indolent hunger arise accompanied by challenging behaviors.12,14,15 Recent studies indicated that mental disorders occur in this syndrome much more often than in the general population – especially schizophrenia spectrum.16 PWS characterizes a specific behavioral profile in which many psychopathological symptoms and challenging behaviors are included. Behavioral phenotype of PWS patients consists of autistic traits which are becoming more and more noticeable with age.17 Another feature includes preoccupation with food, disruptive, abusive behaviors accompanied by impulsivity, stubbornness and lack of cooperation and easily getting obsessed with an idea or activity.18 Attention is drawn to a very large percentage of up to 20–60% (depending on the mechanism of the syndrome’s origin) of patients with PWS who develop psychotic disorders during their lifetime.19 The majority of patients presenting psychotic symptoms have PWS due to mUPD, while patients with deletion present more depressive disorders. It is worth mentioning that psychiatric illness in PWS tends to have atypical symptomatology with predominantly affective syndromes and psychotic symptoms are described in both groups of patients with significant advantage of patients with mUPD.20
The 22q11.2 deletion syndrome, also known as DiGeorge syndrome (DGS) is the most common chromosomal microdeletion with autosomal dominant inheritance pattern and with prevalence rate estimated at 1:4000 individuals.11,21 DGS is a cluster of congenital malformations resulting from the loss of a fragment of chromosome 22 with a variable presentation, which usually consists of cardiac and palatal abnormalities, immunodeficiency with thymic hypoplasia, dysmorphic features such as hooded eyelids or nasal dimple, endocrine disturbances with hypoparathyroidism and varying level of cognitive impairment.21 The behavioral phenotype of DGS consists of poor social skills with social withdrawal accompanied by restricted affect.22 Impaired abilities mostly include emotions processing and complex theory of mind similar to disorders of autistic spectrum.22,23 Apart from behavioral disturbances, the rate of psychosis in this syndrome is more than twenty times greater than in the general population and it is estimated that DGS may stand for 1–2% of all the schizophrenia cases worldwide.24
Given that subclinical metabolic dysregulation appears already at early stages of severe mental disorders, including mood and psychotic disorders and might be associated with intrinsic mechanisms, it might be hypothesized that this phenomenon also appears in patients with DS and PWS, and might be related to psychopathological symptoms. Therefore, in this study, we aimed to compare cardiometabolic parameters in PWS and DGS as well as investigate whether metabolic alterations in these symptoms are related to psychopathological manifestation. Our hypothesis was that metabolic dysregulation (lipid profile disturbances and the measures of insulin resistance) will be present in PWS and DGS patients representing high risk of mental illness, especially psychotic disorders.
Materials and Methods
Participants
We recruited 20 children with PWS and 18 children with DS matched for age, sex and body mass index (BMI). Participants were recruited among patients of Department of Genetics (Wroclaw Medical University, Poland) and Polish PWS and DGS Associations for patients and their families. The majority of PWS patients (n = 19) had 15q11-13 microdeletion, while mUPD was diagnosed in one PWS patient. All patients were in the norm or in the borderline of the intellectual norm, attended public or integration schools. None of the patients was diagnosed with previous or current psychotic symptoms and none of them has taken psychotropic drugs accept for one PWS patient who was on methylphenidate due to diagnosis of ADHD. The study was approved by the Ethics Committee at Wroclaw Medical University (Nr KB – 784/2017) and was conducted in accordance with the Declaration of Helsinki, the written informed consents from patients, their parents and legal guardians were collected.
Clinical Measures
Psychopathological profile of patients was assessed using the Polish version of the Child Behavior Checklist (CBCL),25 a questionnaire composed of 113 statements filled by the child’s guardian as 0 (not true), 1 (sometimes true) or 2 (often true). Results were divided into three main groups: competences, internalizing problems (consisting of anxious/depressed, withdrawn/depressed, somatic complaints domains) and externalizing problems (consisting of delinquent behavior and aggressive behavior domains) together with social problems, thought problems and attention problems domains included in total problems.26
Clinical and Biochemical Parameters
The following clinical and biochemical parameters were assessed to compare both groups of participants: 1) anthropometric measures: weight, height, body mass index (BMI), waist and hips circumference; 2) inflammatory markers: high-sensitivity C-reactive protein (hsCRP); 3) glucose homeostasis: semi-fasting glucose and insulin and 4) lipids: low- and high-density lipoproteins (LDL and HDL), non-HDL, total cholesterol and triglycerides.
Semi-fasting blood samples (10 mL, after 3–4 hrs fasting) were collected from all patients participating in the study, centrifuged at 2500 rpm for 10 min to collect serum that was stored in aliquots at −80°C. The Konelab 60 analyzer (Argenta) was used to measure the levels of glucose, total cholesterol and triglycerides based on colorimetric methods. The levels of LDL were calculated with the Friedewald equation.27 Insulin levels were analyzed with the electrochemiluminescence method (Cobas e411 analyzer, Roche). The levels of hsCRP were determined using the immunonephelometric method (BN2 analyzer, Siemens). The Homeostatic Model Assessment (HOMA) method was used to indicate the insulin resistance and β-cell function estimated from semi-fasting glucose and insulin levels.28,29
Statistics
Between-group differences in the distribution of categorical variables and continuous variables were assessed using the χ2 test and the Mann–Whitney U-test, respectively. Bivariate correlations were tested using the Spearman’s rank correlation coefficients. The Benjamini–Hochberg method with the false discovery rate of 25% was used due to multiple testing. Results of bivariate tests were considered statistically significant if the p-value was ≤0.017. Significant differences in biochemical parameters were further tested using the analysis of co-variance (ANCOVA) with diagnostic group (PWS vs DGS patients) as an independent variable and BMI as a co-variate. Moreover, linear regression analysis was performed to assess bivariate correlations to control for the effects of BMI. The alpha criterion level was set at 0.05 in the ANCOVA and linear repression analyses. Statistical analysis was performed using the Statistical Package for Social Sciences, version 20 (SPSS Inc., Chicago, Illinois, USA).
Results
General characteristics of the sample are presented in Table 1. Both groups of participants had similar age, the number of males and females as well as anthropometric parameters (BMI, waist circumference and hip circumference). The levels of insulin and non-HDL were significantly higher in PWS patients compared to those with DGS. Patients with PWS had also higher levels of HOMA-IR and LDL than individuals with DGS. However, these differences did not reach statistical significance after the Benjamini-Hochberg correction. The ANCOVA revealed significant effects of diagnostic group (PWS vs DGS, F = 4.99, p = 0.033) on insulin levels after co-varying for BMI (F = 3.26, p = 0.080). In addition, the effects of diagnostic group (PWS vs DGS) on non-HDL appeared to be significant (F = 5.53, p = 0.025) after controlling for the effects of BMI (F = 0.13, p = 0.721). Similarly, the scores of four CBCL subscales (social problems, thought problems, delinquent behavior and aggressive behavior) were significantly higher in PWS patients in comparison with DGS patients.
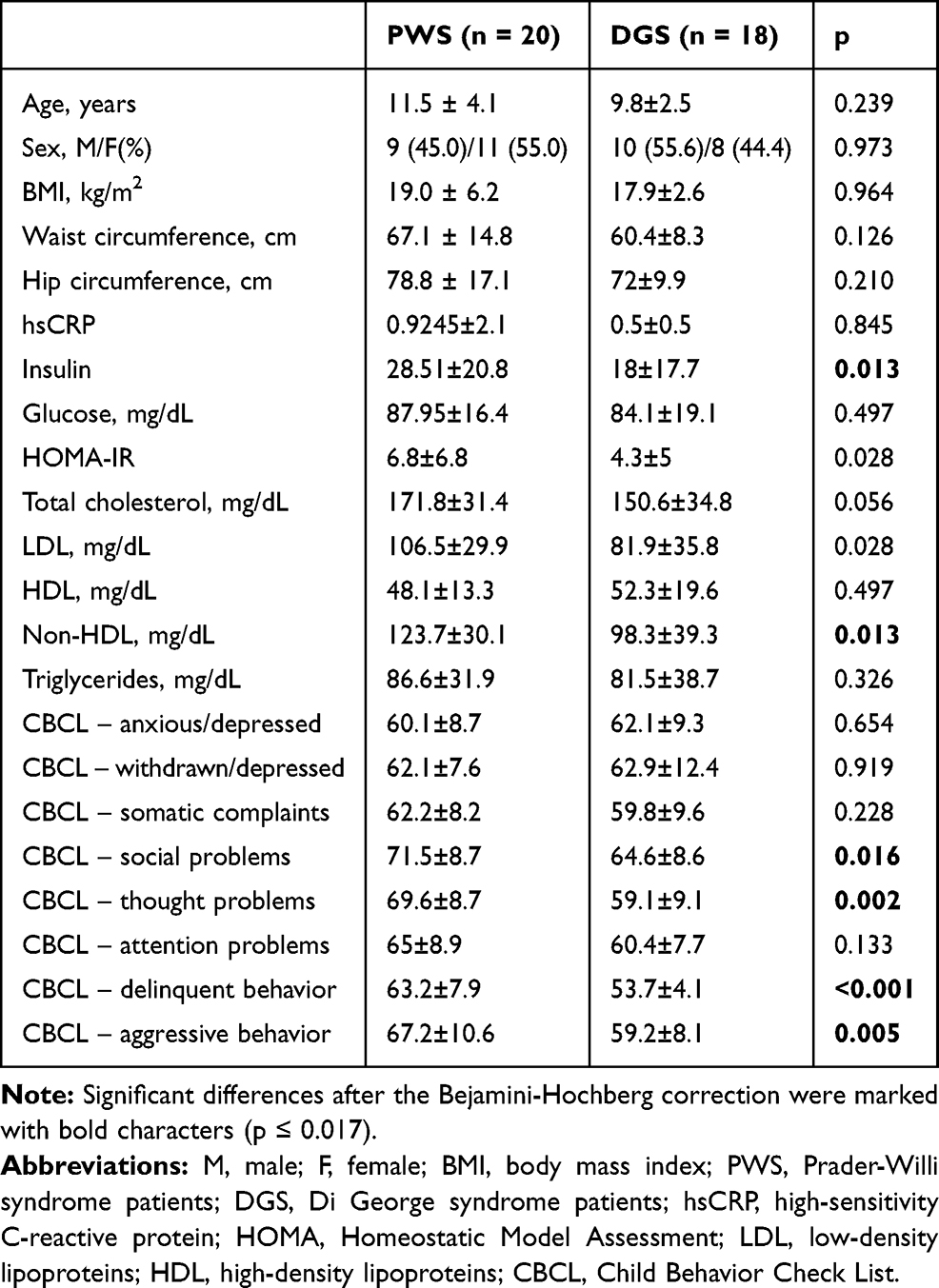 |
Table 1 General Characteristics of the Sample |
Correlations between biochemical parameters and scores of specific CBCL subscales in all participants are provided in Table 2. There were significant positive correlations between the scores of CBCL-thought problems and the levels of insulin as well as HOMA-IR. Linear regression analysis revealed that the correlation between insulin levels and the score of CBCL-thought problems was significant (B = 2.24, p = 0.035) after controlling for the effects of BMI (B = 1.39, p = 0.173). Similarly, the correlation between HOMA-IR and the score of CBCL-thought problems appeared to be significant (B = 2.13, p = 0.042) after adjustment for BMI effects (B = 1.02, p = 0.223). There was also a negative correlation between the scores of CBCL-thought problems and HDL levels. However, this correlation appeared to be non-significant after correction for multiple testing.
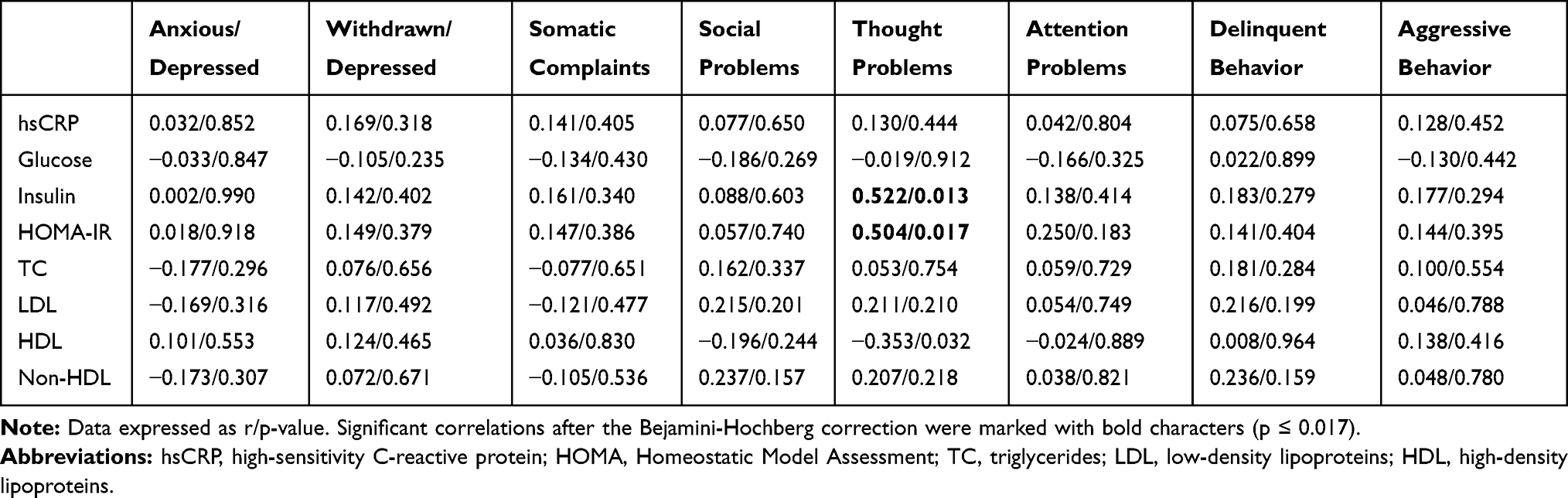 |
Table 2 Bivariate Correlations Between Metabolic Parameters and the Measures of Psychopathology in PWS Patients |
Discussion
In our study, we found elevated levels of non-HDL as well as insulin resulting in heightened HOMA-IR in PWS patients compared to DGS patients, even after controlling for the effects of BMI differences. We attempted to compare two genetic syndromes with a proven high risk of developing psychotic disorders.19,24
Research indicate that drug-naive patients with clinically high risk for developing psychosis present also higher predisposition of developing signs of metabolic syndrome such as higher rates of elevated levels non-HDL cholesterol concentrations as well as increased fasting levels of blood glucose.24 Meta-analysis on dyslipidemia in drug-naive patients with first episode of schizophrenia showed subclinical lipid profile alterations. Lower levels of low-density lipoprotein (LDL), HDL and total cholesterol, as well as significantly higher levels of triglycerides in patients at early phase of schizophrenia-spectrum disorders were demonstrated.6 The results of this meta-analysis are consistent with our study, in which we showed a statistically significant increase in non-HDL cholesterol levels which stands for the total concentration of all atherogenic lipoproteins. A recent study by Keinänen et al indicated that lipid metabolism dysregulation in drug-naïve first-episode psychosis patients is related to atherogenic lipoproteins with higher LDL cholesterol, total cholesterol and triglycerides.30 Dyslipidemia is indicated also as one of the contributors to cognitive impairment in schizophrenia spectrum patients.31 Further research on patients with genetic disorders should be focused on correlations between cognitive performance and dyslipidemia in vulnerable populations. This is crucial as dyslipidemia can contribute to brain structural changes that are already present in adolescence, which are preventable or treateable.31
Meta-analysis on biochemical measures of prediabetic states in drug-naïve patients with first episode psychosis revealed impaired glucose tolerance and insulin resistance compared to healthy controls.32 These results depend not only on the patient’s lifestyle, prescribed pharmacotherapy or access to health services, but might also have an intrinsic background. First episode psychosis might be connected to abnormal glycemic profile due to inflammatory pathways. The inflammatory process with increased concentrations of inflammatory cytokines is involved both in schizophrenia-spectrum disorders and the type 2 diabetes. When considering the relationship between psychotic disorders and dysglycemia, mediating or moderating inflammatory factors should be mentioned. Inflammation, as a mediator, may lead to dysglycemia which often appears in psychosis. Moderating model assumes that both dysglycemia and psychosis emerge with a joint participation of inflammatory mechanisms. However, in our study, we did not find elevated level of hsCRP, that could have indicated the presence of inflammation in the studied groups. Another finding of common factor for psychosis and impaired glucose tolerance is the PI3K/AKT/mTOR pathway, an intracellular signaling pathway, involved both in insulin sensitivity and dopamine regulation.33 HOMA model provides information on insulin resistance, which tends to be present in antipsychotic-naïve patients with schizophrenia.34 This information is consistent with the results of our study where we found statistically significant elevation in insulin concentration as well as in HOMA-IR in patients with genetic disorders prone to develop psychosis. What is particularly interesting, we found significant correlations between insulin concentration, HOMA-IR and the CBCL thought problems domain. It has been shown in the study on individuals identified as at risk of psychosis, that it is one of the two domains from CBCL questionnaire that may serve as a potential psychosis risk screening.35 Thought Problems subscale in CBCL also proved to be a clinically useful for identifying psychotic symptoms in children in comparative studies with the rationally derived DSM-oriented psychotic symptoms scale (DOPSS).36 The study on early-onset psychosis conducted on teenage population by Jensen et al also indicated that elevated metabolic risk with dyslipidemia may be present even prior to pharmacotherapy.37
There are some limitations in this study that need to be discussed. The sample of our study was limited to 20 PWS patients and 18 DGS patients due to the rarity of the syndromes as well as exclusion of patients with lower levels of intellectual functioning. We were also unable to determine whether metabolic disturbances appear only in some subgroups of patients with PWS or DGS. An important limitation is that we were not able to obtain fasting blood samples from the patients and thus semi-fasting samples, 3–4 hrs after meal, were collected. However, it has been found that there is a significant correlation in the measures of insulin resistance or sensitivity between semi-fasting and fasting blood samples.29 Similarly, there are recommendations that non-fasting blood samples could be routinely used for the assessment of plasma lipid profiles.38 In favor of our results stands the fact that all patients with Prader–Willi syndrome remained under the care of a dietitian and maintained a restrictive diet with low glycemic index and reduced fat content in order to prevent weight gain. Both groups were comparable in terms of weight and BMI. In the PWS group, two patients had weight and BMI above 95 percentile, of which only one patient was obese. Another limitation is that the vast majority of PWS patients (19:1) had deletion etiology of the syndrome and psychotic symptoms are more characteristic to PWS due to mUPD etiology. It is also important to note that we did not include a group of healthy children. Finally, a cross-sectional study design does not allow to conclude regarding causal associations between metabolic disturbances and co-morbid psychopathological symptoms in both groups of patients.
Conclusion
Our results indicate that patients with PWS may be more prone to develop subclinical metabolic dysregulation, in terms of elevated non-HDL levels and insulin levels, compared to DGS patients. In both groups of patients, altered insulin sensitivity, even though it is not a specific risk factor, might be related to psychosis risk, which needs further research. These results may indicate that the metabolic alterations are linked to psychosis regardless of predisposing conditions. Longitudinal studies in larger cohorts of patients with PWS and DGS are needed to establish causal associations. The comparison with other at-risk populations is needed to confirm whether our observations reflect the outcome of intrinsic processes associated with the pathophysiology of psychosis.
Data Sharing Statement
Data is not available for online access. Readers who wish to gain access to the data should contact the corresponding author of this article.
Acknowledgments
We want to thank all of the patients from both the research and control groups as well as their families for all help and patience. Additional thanks goes to foundation “Potrafię pomóc”, Foundation for Children with Rare Diseases and the Polish Assistance Association for People with the Prader-Willi Syndrome and the Association 22q11 Poland for support and help in recruiting patients.
Author Contributions
All authors contributed to data analysis and drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Davison J, O’Gorman A, Brennan L, Cotter DR. A systematic review of metabolite biomarkers of schizophrenia. Schizophr Res. 2018;195:32–50. doi:10.1016/j.schres.2017.09.021
2. Emanuele E, Martinelli V, Abbiati V, Fusar-Poli P, Politi P. Biochemical markers of impending psychosis. Curr Pharm Des. 2012;18(4):505–509. doi:10.2174/138161212799316000
3. Ramsay H, Barnett JH, Murray GK, et al. Cognition, psychosis risk and metabolic measures in two adolescent birth cohorts. Psychol Med. 2018;48(15):2609–2623. doi:10.1017/S0033291718001794
4. Xu H, Zhuang X. Atypical antipsychotics-induced metabolic syndrome and nonalcoholic fatty liver disease: a critical review. Neuropsychiatr Dis Treat. 2019;15:2087–2099. doi:10.2147/NDT.S208061
5. Kucerova J, Babinska Z, Horska K, Kotolova H. The common pathophysiology underlying the metabolic syndrome, schizophrenia and depression. A review. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159(2):208–214. doi:10.5507/bp.2014.060
6. Misiak B, Stańczykiewicz B, Łaczmański Ł, Frydecka D. Lipid profile disturbances in antipsychotic-naive patients with first-episode non-affective psychosis: a systematic review and meta-analysis. Schizophr Res. 2017;190:18–27. doi:10.1016/j.schres.2017.03.031
7. Wysokiński A, Strzelecki D, Kłoszewska I. Levels of triglycerides, cholesterol, LDL, HDL and glucose in patients with schizophrenia, unipolar depression and bipolar disorder. Diabetes Metab Syndr. 2015;9(3):168–176. doi:10.1016/j.dsx.2015.04.004
8. Waloszek JM, Byrne ML, Woods MJ, et al. Early physiological markers of cardiovascular risk in community based adolescents with a depressive disorder. J Affect Disord. 2015;175:403–410. doi:10.1016/j.jad.2015.01.008
9. Postolache TT, Del Bosque-Plata L, Jabbour S, Vergare M, Wu R, Gragnoli C. Co-shared genetics and possible risk gene pathway partially explain the comorbidity of schizophrenia, major depressive disorder, type 2 diabetes, and metabolic syndrome. Am J Med Genet B Neuropsychiatr Genet. 2019;180(3):186–203. doi:10.1002/ajmg.b.32712
10. Cassidy SB. Prader-Willi syndrome. J Med Genet. 1997;34(11):917–923. doi:10.1136/jmg.34.11.917
11. Verhoeven WMA, Tuinier S. Clinical perspectives on the genetics of schizophrenia: a bottom-up orientation. Neurotox Res. 2008;14(2–3):141–150. doi:10.1007/BF03033806
12. Abdilla Y, Andria Barbara M, Calleja-Agius J. Prader-Willi Syndrome: background and Management. Neonatal Netw. 2017;36(3):134–141. doi:10.1891/0730-0832.36.3.134
13. Curfs LM, Fryns JP. Prader-Willi syndrome: a review with special attention to the cognitive and behavioral profile. Birth Defects Orig Artic Ser. 1992;28(1):99–104.
14. Reddy LA, Pfeiffer SI. Behavioral and emotional symptoms of children and adolescents with Prader-Willi Syndrome. J Autism Dev Disord. 2007;37(5):830–839. doi:10.1007/s10803-006-0210-2
15. Driscoll DJ, Miller JL, Schwartz S, Cassidy SB. Prader-Willi syndrome. 1993. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20301505.
16. Guinovart M, Coronas R, Caixàs A. Psychopathological disorders in Prader-Willi syndrome. Endocrinol Diabetes Nutr. 2019. doi:10.1016/j.endinu.2019.03.004
17. Song DK, Sawada M, Yokota S, et al. Comparative analysis of autistic traits and behavioral disorders in Prader-Willi syndrome and Asperger disorder. Am J Med Genet A. 2015;167A(1):64–68. doi:10.1002/ajmg.a.36787
18. Jauregi J, Laurier V, Copet P, Tauber M, Thuilleaux D. Behavioral profile of adults with Prader-Willi syndrome: correlations with individual and environmental variables. J Neurodev Disord. 2013;5(1):18. doi:10.1186/1866-1955-5-18
19. Larson FV, Whittington J, Webb T, Holland AJ. A longitudinal follow-up study of people with Prader–Willi syndrome with psychosis and those at increased risk of developing psychosis due to genetic subtype. Psychol Med. 2014;44(11):2431–2435. doi:10.1017/S0033291713002961
20. Soni S, Whittington J, Holland AJ, et al. The phenomenology and diagnosis of psychiatric illness in people with Prader-Willi syndrome. Psychol Med. 2008;38(10):1505–1514. doi:10.1017/S0033291707002504
21. McDonald-McGinn DM, Sullivan KE, Marino B, et al. 22q11.2 deletion syndrome. Nat Rev Dis Prim. 2015;1:15071. doi:10.1038/nrdp.2015.71
22. Weisman O, Feldman R, Burg-Malki M, et al. Comparing the broad socio-cognitive profile of youth with Williams syndrome and 22q11.2 deletion syndrome. J Intellect Disabil Res. 2017;61(12):1083–1093. doi:10.1111/jir.12424
23. Costa GM, Ganthous G, Santos AO, Giacheti CM. Caracterização do perfil comportamental e de competência social de indivíduos com a síndrome del22q11.2. Rev CEFAC. 2015;17(4):1062–1070. doi:10.1590/1982-021620151746014
24. Squarcione C, Torti MC, Di Fabio F, Biondi M. 22q11 deletion syndrome: a review of the neuropsychiatric features and their neurobiological basis. Neuropsychiatr Dis Treat. 2013;1873. doi:10.2147/NDT.S52188
25. Wolańczyk T. Zaburzenia Emocjonalne I Behawioralne u Dzieci I Młodzieży Szkolnej w Polsce. Warszawa: Akademia Medyczna. 2002.
26. Achenbach TM. Integrative guide to the 1991 CBCL/4-18 YSR, and TRF profiles. Univ Vermont Dep Psychol Pediatr. 1991.
27. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18(6):499–502. doi:10.1093/clinchem/18.6.499
28. Antuna-Puente B, Disse E, Rabasa-Lhoret R, Laville M, Capeau J, Bastard J-P. How can we measure insulin sensitivity/resistance? Diabetes Metab. 2011;37(3):179–188. doi:10.1016/j.diabet.2011.01.002
29. Hancox RJ, Landhuis CE. Correlation between measures of insulin resistance in fasting and non-fasting blood. Diabetol Metab Syndr. 2011;3(1):23. doi:10.1186/1758-5996-3-23
30. Keinänen J, Suvisaari J, Reinikainen J, et al. Low-grade inflammation in first-episode psychosis is determined by increased waist circumference. Psychiatry Res. 2018;270:547–553. doi:10.1016/j.psychres.2018.10.022
31. Kolenic M, Franke K, Hlinka J, et al. Obesity, dyslipidemia and brain age in first-episode psychosis. J Psychiatr Res. 2018;99:151–158. doi:10.1016/j.jpsychires.2018.02.012
32. Perry BI, McIntosh G, Weich S, Singh S, Rees K. The association between first-episode psychosis and abnormal glycaemic control: systematic review and meta-analysis. Lancet Psychiatry. 2016;3(11):1049–1058. doi:10.1016/S2215-0366(16)30262-0
33. Perry BI, Upthegrove R, Thompson A, et al. Dysglycaemia, inflammation and psychosis: findings from the UK ALSPAC birth Cohort. Schizophr Bull. 2019;45(2):330–338. doi:10.1093/schbul/sby040
34. Cohn TA, Remington G, Zipursky RB, Azad A, Connolly P, Wolever TMS. Insulin resistance and adiponectin levels in drug-free patients with schizophrenia: a preliminary report. Can J Psychiatry. 2006;51(6):382–386. doi:10.1177/070674370605100608
35. Simeonova DI, Nguyen T, Walker EF. Psychosis risk screening in clinical high-risk adolescents: a longitudinal investigation using the child behavior checklist. Schizophr Res. 2014;159(1):7–13. doi:10.1016/j.schres.2014.07.046
36. Salcedo S, Rizvi SH, Freeman LK, Youngstrom JK, Findling RL, Youngstrom EA. Diagnostic efficiency of the CBCL thought problems and DSM-oriented psychotic symptoms scales for pediatric psychotic symptoms. Eur Child Adolesc Psychiatry. 2018;27(11):1491–1498. doi:10.1007/s00787-018-1140-1
37. Jensen KG, Correll CU, Rudå D, et al. Pretreatment cardiometabolic status in youth with early-onset psychosis: baseline results from the TEA trial. J Clin Psychiatry. 2017;78(8):e1035–e1046. doi:10.4088/JCP.15m10479
38. Nordestgaard BG, Langsted A, Mora S, et al. Fasting is not routinely required for determination of a lipid profile: clinical and laboratory implications including flagging at desirable concentration cut-points-a joint consensus statement from the European Atherosclerosis Society and European Federa. Eur Heart J. 2016;37(25):1944–1958. doi:10.1093/eurheartj/ehw152
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.