Back to Journals » Research and Reports in Urology » Volume 17
Mesenteric Artery Dissection Aneurysm Associated with Apatinib in a Prostate Cancer Patient: A Case Report and Literature Review
Authors Ren T, Gu J, Wang D, Zhao L
Received 19 March 2025
Accepted for publication 10 July 2025
Published 6 August 2025 Volume 2025:17 Pages 263—270
DOI https://doi.org/10.2147/RRU.S523768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Guglielmo Mantica
Tiejun Ren, Jinjin Gu, Dingyi Wang, Lijuan Zhao
Oncology Special Ward, Luoyang Central Hospital Affiliated to Zhengzhou University, Luoyang, Henan, People’s Republic of China
Correspondence: Tiejun Ren, Oncology Special Ward, Luoyang Central Hospital Affiliated to Zhengzhou University, Luoyang, Henan, 471000, People’s Republic of China, Email [email protected]
Background: Apatinib mesylate, a VEGFR2 tyrosine kinase inhibitor, is approved for advanced liver, esophageal, gastric and other malignant tumors, but its adverse effects require attention. We report a 79-year-old male with prostatic adenocarcinoma who developed superior mesenteric artery dissecting aneurysm after combined apatinib and chemotherapy. Apatinib, an anti-angiogenic agent, synergizes with chemotherapy. After informed consent, the combination regimen was initiated. Two cycles later, the patient had tolerable intermittent abdominal pain, and CT confirmed the aneurysm. Due to progressive tumor and poor physical status, no further treatment was given as the aneurysm did not affect the disease course. This case report aims to provide insights into the safe application of apatinib in clinical practice.
Materials and Methods: The materials for the literature review were gathered through a comprehensive search conducted on PubMed. Which yielded VEGFR2 treated for prostate cancer.
Case Report: In this case report, a 79-year-old male with a height of 172 cms and a weight of 67 kgs who had been diagnosed with prostate adenocarcinoma for over three years. MRI scan indicated that bone metastases increased and enlarged compared with prior test. No significant abnormalities were observed in both physical and blood examinations. The pelvic MRI scan showed a prostatectomy changes, multiple abnormal signals in the bilateral ilium, acetabulum, femur, ischiatic bone, pubis, sacral vertebrae, and part of the lumbar vertebrae.
Conclusion: Antiangiogenic agents are being increasingly utilized in clinical practice. As clinicians, it is imperative to remain vigilant against potential complications such as arterial dissection and aneurysm, while conducting meticulous evaluations of associated risks. Notably, this article serves solely as a reference and does not advocate for the adjustment of treatment protocols on this basis.
Keywords: apatinib, anti-angiogenic drug, prostate cancer, superior mesenteric artery
Introduction
Apatinib mesylate represents the inaugural small molecule VEGFR2 tyrosine kinase inhibitor to be independently developed in China and to have demonstrated safety and efficacy in advanced cancer patients worldwide. The drug has been shown to inhibit tumor angiogenesis and was approved for the domestic market in October 2014. Currently, it is clinically approved for the treatment of advanced gastric adenocarcinoma, esophagogastric junction adenocarcinoma, liver cancer, esophageal cancer and other advanced malignant tumor. Concurrently, the adverse reactions associated with this drug have also attracted considerable attention. A review of the domestic and international literature found that common adverse effects of Apatinib include hypertension, proteinuria, hand-foot syndrome, malaise, diarrhoea, and no reports of Apatinib causing a superior mesenteric artery entrapment aneurysm. A case of apatinib induced superior mesenteric artery dissected aneurysm was analyzed and a review of the relevant literature was conducted in order to provide a reference point for the clinical safety of the drug.
Case Report
A 79-years-old male with a height of 172 cm and a weight of 67 kg, had been diagnosed with prostate adenocarcinoma for over three years. In February 2020, the patient developed hematuria without obvious inducement and went to the local hospital for complete examination and radical prostatectomy. Following surgery, he commenced oral treatment with bicalutamide 150 mg once daily, with his condition remaining stable throughout. In April 2022, a PET/CT examination was conducted, which revealed the presence of multiple bone metastases. The patient was diagnosed with progressive disease (PD) and a new treatment plan was formulated, comprising the combination of Olaparib, abiraterone, goserelin and prednisone, in conjunction with radiotherapy for lumbar vertebrae metastases. In April 2023, a CT, MRI scan indicated that the bone metastasis was more advanced than previously thought, the treatment regimen was modified to include Enzalutamide 160 mg orally once a day and Goserelin 10.8mg, with denosumab combined with zoledronic acid introduced as a regular treatment for bone metastasis. In July 2023, he was admitted to the hospital for re-examination with CT, MRI indicating that bone metastases increased and enlarged compared with before, and PD was evaluated and treated with “strontium-89”. In September 2023, he was admitted to the hospital for a re-examination, during which it was observed that the CT and MRI scans had revealed increased bone metastases compared with those conducted previously. The replacement treatment regimen was “Tislelizumab 200mg + apatinib 0.25g once daily + Goserelin 10.8mg” for 1 cycle. In October 2023, the PSA was elevated, given the lack of therapeutic efficacy and the patient’s development of interstitial lung changes, advanced age, and frailty, Tislelizumab was discontinued and the treatment regimen was changed to “apatinib 0.25g once daily + albumin-bound paclitaxel 0.2g d1,8+ cisplatin 20mg d1,8 q21d” which was administered for two cycles. Gastrointestinal reactions, including grade III bone marrow depression and mild nausea, were observed following the administration of the medication. Following the administration of the drug, gastrointestinal reactions such as myelosuppression and mild nausea were observed. Symptomatic treatment was initiated, and the adverse effects improved, resulting in the patient’s discharge from the hospital. The patient had no history of hypertension and connective tissue disease, denied a history of food or drug allergies.
A physical examination was conducted in November 2023 in a hospital setting. The patient’s temperature was 36.3°C, heart rate was 76 times per minute, respiratory rate was 17 times per minute, and blood pressure was 134/83 mmHg. A routine blood examination revealed mild anemia, with hemoglobin levels of 110 g/L. No significant abnormalities were observed in the blood biochemistry results. The free prostate specific antigen (fPSA) level was 9.42 ng/mL, the total prostate specific antigen (PSA) level was 50.44 ng/mL, and the complexed prostate specific antigen (cPSA) level was 35.31 ng/mL. Thoracolumbar enhanced MRI (November,2023):1. Bony hyperplasia of thoracic and lumbar vertebrae, with a slight lateral curvature of the thoracic and lumbar vertebrae.2. Multiple metastatic tumors of C7-L4 vertebrae and S1-4. There is an increase in the number and size of vertebral lesions compared to previous observations.3. A hemangioma was observed in the L1 vertebrae. 4.Yellow myeloid changes were noted in the L4-sacral vertebrae. 5.A herniated intervertebral disc was identified in the L1/2-L4/5 region. 6.Exudative changes were observed in the lumbar dorsal erector ridge muscle, with a predilection for the right side. Pelvic MRI (November,2023): 1. Prostatectomy changes. 2. There were multiple abnormal signals in the bilateral ilium, acetabulum, femur, ischiatic bone, pubis, sacral vertebrae and part of the lumbar vertebrae. In consideration of the possibility of metastatic disease, the lesions exhibited a greater degree of enlargement and number than previously observed. 3.Left inguinoscrotal hernia.4. Exudative changes in the bilateral iliopsoas muscle and right vertical spinal muscle.4. Small amounts of fluid in the hip joint cavity bilaterally. Thoracic and abdominal CT (November,2023): 1. Metastatic tumours of the thoracic and lumbar spine. 2. Mild interstitial pneumonia changes. 3. Pulmonary nodule. 4. Mild pneumonia in both lungs. 5. New superior mesenteric artery dissection aneurysm was identified (Figure 1–5). The clinical diagnosis was as follows:1. Multiple bone metastases following radical prostatic adenocarcinoma. 2. Metastases to the bones. 3. Newly developed superior mesenteric artery entrapment aneurysm. 4. Atrial fibrillation. 5. Chronic obstructive pulmonary disease. 6. Mild anemia. Due to advanced age, continuous progression of the disease, and the occurrence of superior mesenteric artery dissecting aneurysm this time, the patient refused further treatment for the aneurysm and was discharged after only receiving symptomatic treatment.
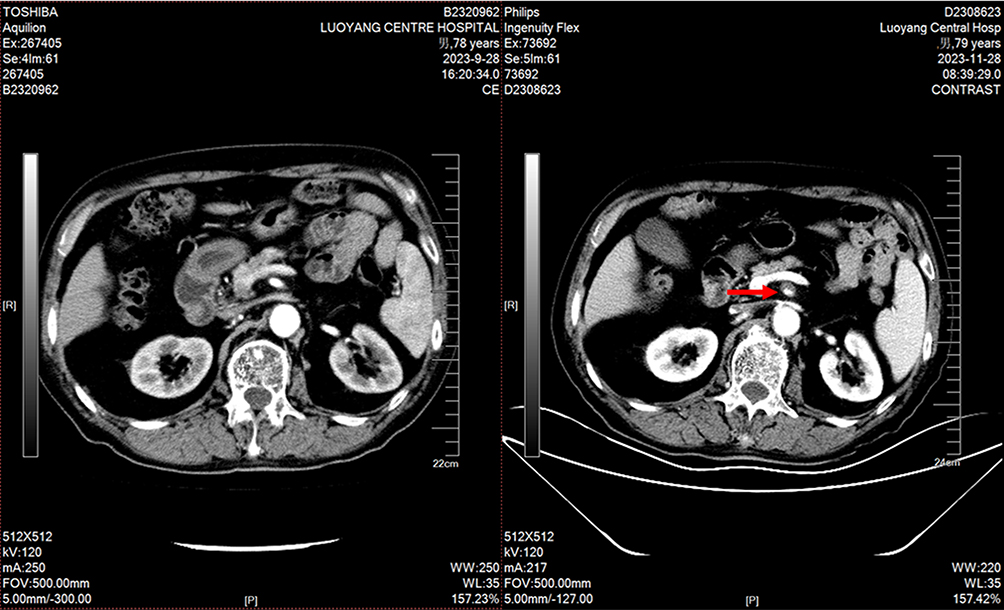 |
Figure 1 CT scan images of ISMAD. The left side shows no ISMAD before treatment (im61), and the right side shows new ISMAD after treatment (im61). The red arrows point to ISMAD. |
 |
Figure 2 CT scan images of ISMAD. The left side shows no ISMAD before treatment (im62), and the right side shows new ISMAD after treatment (im62). The red arrows point to ISMAD. |
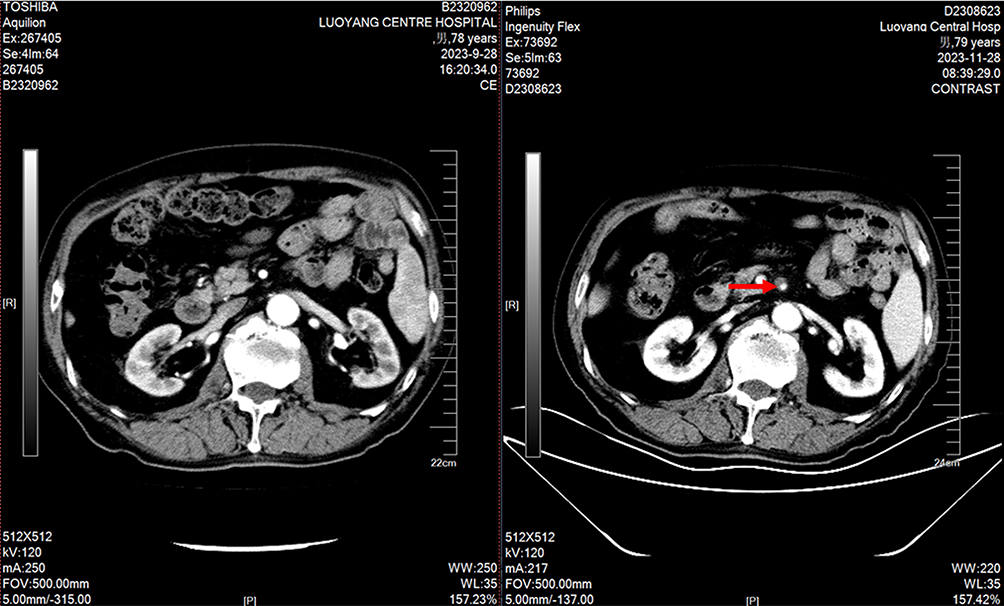 |
Figure 3 CT scan images of ISMAD. The left side shows no ISMAD before treatment (im64), and the right side shows new ISMAD after treatment (im63). The red arrows point to ISMAD. |
 |
Figure 4 CT scan images of ISMAD. The left side shows no ISMAD before treatment (im70), and the right side shows new ISMAD after treatment (im71). The red arrows point to ISMAD. |
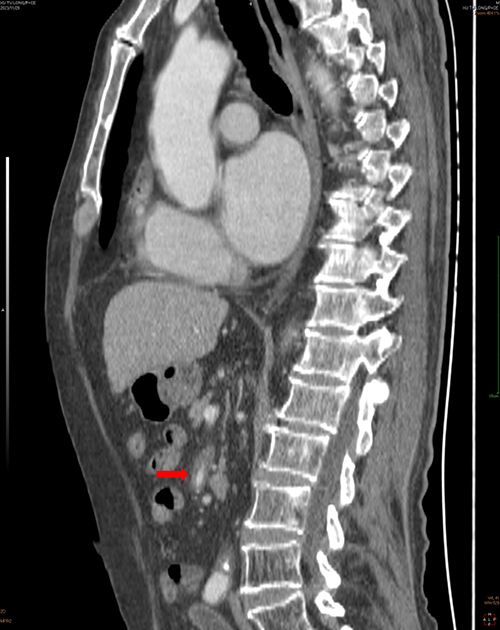 |
Figure 5 The three-dimensional reconstruction image of the CT scan in the sagittal plane. The red arrows point to ISMAD. |
Discussion
Apatinib is a small-molecule oral anti-angiogenic preparation that exhibits high selectivity in binding and inhibiting vascular endothelial growth factor and neovascularization.1 The drug is currently approved for the treatment of gastric adenocarcinoma, esophagogastric junction adenocarcinoma, advanced esophageal cancer and advanced liver cancer.2,3 A number of clinical studies have also demonstrated the efficacy of this treatment in malignant tumors, including those of the breast and lung.4–6 However, the safety and late adverse effects of anti-angiogenic drugs, a novel class of drugs introduced to the clinic in the past decade, have yet to be fully elucidated and warrant further investigation.
Isolated superior mesenteric artery dissection (ISMAD) is a rare vascular disease that affects the superior mesenteric artery without involving the aorta. Previously, the prevalence of this disease was believed to be exceedingly low.7 However, with the advent of more sophisticated diagnostic techniques, the detection rate of this disease has been on the rise. It is noteworthy that the incidence of this disease in East Asia is higher than that observed in Europe and the United States.8,9 Since the initial description of this disease by Bauersfeld et al10 in 1947, there have been approximately 1000 cases reported worldwide. The disease is most commonly observed in men aged between 50 and 70 years,11,12 and its clinical manifestations are non-specific. Some patients present with periumbilical pain. The pain is primarily attributed to the compression of the true lumen of the superior mesenteric artery, which is caused by the lesion of the dissection and intestinal ischemia. Secondly, the abdominal nerve plexus is stimulated by an artery tear and inflammatory reaction during the formation of dissection.13 A considerable proportion of patients diagnosed with ISMAD (26%) present with no clinical manifestations and are only incidentally identified during abdominal CT examinations. Such patients may occasionally present with symptoms such as nausea, vomiting, abdominal distension and diarrhea. It is not uncommon for the clinical symptoms to be inconsistent with the physical signs, and it is not uncommon for no positive signs to be found during a physical examination, which is indicative of the phenomenon of “separation of symptoms and signs”.14 In a study by Froment et al,15 it was found that 5 out of 29 patients (17.2%) exhibited periumbilical vascular murmurs, which could be considered a diagnostic indicator. The diagnosis of this disease is primarily based on clinical symptoms and imaging examination, with auxiliary examinations including vascular enhanced CT, subtraction angiography (DSA), color ultrasound, and so forth. The precise etiology of superior mesenteric artery dissection aneurysm remains uncertain. It is hypothesized that hypertension, atherosclerosis, vascular injury, inflammation, abnormal vascular wall development, trauma and other factors may be involved,16 although there are also patients with no obvious risk factors. In terms of treatment, asymptomatic ISMAD is managed according to international guidelines, which recommend a conservative approach, including fasting, fluid rehydration, stomach care and blood pressure control.17 In cases of superior mesenteric artery dissection aneurysms that meet the criteria for surgical intervention, endovascular treatment is the preferred option. Endovascular treatment encompasses the use of stents, stents combined with spring coil embolization.18 Surgical intervention should be considered for patients presenting with existing intestinal necrosis, rupture of the superior mesenteric artery (SMA), and endovascular treatment failure.19 The prognosis for ISMAD is favourable, with a mortality rate of 0.69% among 721 patients, as evidenced by a review of 51 published studies.9 This patient with prostate adenocarcinoma had no risk factors for the disease, such as hypertension or coronary heart disease, prior to the initiation of medication. Despite undergoing multi-line standard anti-tumor therapy, the patient’s condition continued to deteriorate. Given the patient’s and his family members’ strong desire for treatment, apatinib was empirically applied with the aim of achieving tumor control. Following the administration of the antiangiogenic drug apatinib, an intermittent periumbilical dull pain was observed, with a score of 2. This pain was not related to eating or defecation, and no analgesic treatment was administered. Following three cycles of treatment, an enhanced abdominal computed tomography scan revealed the presence of new superior mesenteric artery dissection aneurysms. This led us to hypothesis that apatinib may have played a role in the development of these lesions. To date, there have been few studies conducted on the subject of aneurysms caused by anti-angiogenic targeted drugs in either domestic or international contexts. A review of domestic and foreign literature revealed several case reports on aortic dissection caused by anti-angiogenic drugs20–24 and a pharmacovigilance study in Japan.25 The majority of cases were attributed to aortic dissection aneurysms induced by bevacizumab, sunitinib, sorafenib, axitinib, anlotinib, and so forth. No reports of Isolated superior mesenteric artery dissection caused by anti-angiogenic drugs were identified. In terms of mechanism of action, Apatinib differs to some extent from Bevacizumab, Sunitinib, Sorafenib, etc. Apatinib, as a highly selective VEGFR-2 receptor inhibitor, inhibits the growth of tumours by blocking this receptor, and the side effects are mainly hypertension and proteinuria. Bevacizumab is an anti-VEGF monoclonal antibody that neutralises all VEGF subtypes and blocks binding to its receptor, and is widely used in colorectal and ovarian cancers, etc., with the main adverse effects being bleeding and hypertension.26 Sunitinib is a multi-target tyrosine kinase inhibitor against VEGFR, PDGFR, KIT, etc., with both anti-angiogenesis and direct inhibition of tumourigenesis, which has a wider indication, but the adverse reactions are relatively more complicated, commonly including cardiotoxicity and thyroid function abnormality.27 Several studies have reported the efficacy of bevacizumab in prostate adenocarcinoma. Bevacizumab blocks tumour angiogenesis by inhibiting the VEGF signalling pathway and can be used in combination therapy for hormone-refractory prostate cancer.28 Studies have shown that combining docetaxel and prednisone significantly prolongs patients’ median survival, but with an increased risk of adverse effects, such as hypertension, proteinuria and bleeding. Preliminary trials suggest that combining radiotherapy or immunotherapy may enhance efficacy, with attention to toxicity.28 No reports of superior mesenteric artery dissection aneurysms caused by anti-angiogenic drugs were identified. The pharmacovigilance study in Japan also demonstrated a correlation between the use of anti-angiogenic drugs and the occurrence of arterial dissection and aneurysm. This indicates that anti-angiogenic drugs may be a contributing factor in the development of arterial dissection and aneurysm.
Combined with the mechanism of action of antiangiogenic drugs and related studies, the possible causes of aneurysms and arterial clips are analyzed as follows: 1. Anti-angiogenic drugs have been demonstrated to induce increased blood pressure and to inhibit the healing of damaged vascular endothelial cells.29 2. Anti-angiogenic drugs enhance vascular contraction by inhibiting nitric oxide-mediated vasodilation and increasing endothelin-1 secretion by vascular endothelial cells, thereby increasing arterial stiffness.30,31 3. Vascular endothelial growth factor (VEGF) as a growth factor and blocking it causes vascular aging.32 4. The effect of anti-angiogenic drugs on vascular structure may also increase the risk of vascular rupture and vascular wall hematoma, as evidenced by research.29 In summary, antiangiogenic drugs cause damage and hardening of the vessel wall and inhibit its repair through various pathways, which in turn leads to arterial clips and aneurysm formation.
Conclusion
As the clinical use of antiangiogenic drugs increases, it is important for clinicians to be aware of the potential for life-threatening complications such as arterial dissection and aneurysm, and to carefully assess the associated risks. This is merely a case report. Additionally, the patient’s combined use of chemotherapeutic agents, radiation therapy, elevated PSA, and systemic chronic inflammation may all potentially contribute to the development of superior mesenteric artery dissecting aneurysm. There is also a possibility of ISMAD occurring accidentally. Therefore, a causal relationship cannot be established. This article only provides reference for clinicians and does not recommend adjusting treatment protocols accordingly.
Abbreviations
cPSA, complexed prostate-specific antigen; DSA, subtraction angiography; fPSA, free prostate-specific antigen; PD, progressive disease; PSA, prostate specific antigen; ISMAD, isolated superior mesenteric artery dissection.
Data Sharing Statement
The data generated in this study are not publicly available due to personal data protection regulations but can be obtained from the corresponding author upon reasonable request.
Ethical Statement
This study is approved by the Medical Ethics Committee of Luoyang Central Hospital (LWLL-2024-07-17). The Ethics Committee of Luoyang Central Hospital approved the publication of the details of this case. The patient provided informed consent for both the treatment and the publication of this article. The publication of this case report and all accompanying figures has been approved by the patient after obtaining informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Scott AJ, Messersmith WA, Jimeno A. Apatinib: a promising oral antiangiogenic agent in the treatment of multiple solid tumors. Drugs Today. 2015;51:223. doi:10.1358/dot.2015.51.4.2320599
2. Li J, Qin S, Xu J, et al. Randomized, double-blind, Placebo-Controlled Phase III trial of apatinib in patients with chemotherapy-refractory advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction. JCO. 2016;34:1448–1454. doi:10.1200/JCO.2015.63.5995
3. Scott LJ. Apatinib: a review in advanced gastric cancer and other advanced cancers. Drugs. 2018;78:747–758. doi:10.1007/s40265-018-0903-9
4. Li -D-D, Tao Z, Wang B-Y, et al. Apatinib plus vinorelbine versus vinorelbine for metastatic triple-negative breast cancer who failed first/second-line treatment: the NAN trial. Npj Breast Cancer. 2022;8:110. doi:10.1038/s41523-022-00462-6
5. He Y, Li C, Zhang F, et al. Clinical study on the second-line treatment of advanced esophageal squamous cell carcinoma with camrelizumab combined with apatinib and irinotecan: a single-arm, multicenter, Phase II study. JCO. 2022;40:319. doi:10.1200/JCO.2022.40.4_suppl.319
6. Pan Y, Jiang F, Du Y, et al. A clinical study of camrelizumab combined with chemotherapy and sequential apatinib in the second-line treatment of patients with advanced non-small cell lung cancer. JCO. 2021;39:e21051–e21051. doi:10.1200/JCO.2021.39.15_suppl.e21051
7. Björck M, Koelemay M, Acosta S, et al. Editor’s choice – management of the diseases of mesenteric arteries and veins. Eur J Vasc Endovascular Surg. 2017;53:460–510. doi:10.1016/j.ejvs.2017.01.010
8. Wang J, He Y, Zhao J, et al. Systematic review and meta-analysis of current evidence in spontaneous isolated celiac and superior mesenteric artery dissection. J Vascular Surg. 2018;68:1228–1240.e9. doi:10.1016/j.jvs.2018.05.014
9. Kimura Y, Kato T, Inoko M. Outcomes of treatment strategies for isolated spontaneous dissection of the superior mesenteric artery: a systematic review. Ann Vasc Surg. 2018;47:284–290. doi:10.1016/j.avsg.2017.07.027
10. Bauerseld SR. Dissecting aneurysm of the aorta: a presentation of fifteen cases and a review of the recent literature. Ann Intern Med. 1947;26:873. doi:10.7326/0003-4819-26-6-873
11. Sun J, Qiu C, Wu Z, et al. Preliminary result of stents implantation for spontaneous isolated dissection of the superior mesenteric artery: a prospective single-arm study. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020;49:383–388. doi:10.3785/j.issn.1008-9292.2020.06.05
12. Mizuno A, Iguchi H, Sawada Y, et al. Real clinical management of patients with isolated superior mesenteric artery dissection in Japan. J Cardiol. 2018;71:155–158. doi:10.1016/j.jjcc.2017.08.006
13. Kong D, Wu L, Wang J, et al. Treatment of 18 cases of spontaneous is olated superior mesenteric artery dissection. Chin J Curr Adv General Surg. 2023;05:389–391+395.
14. Akyildiz H, Akcan A, Oztürk A, et al. The correlation of the D-dimer test and biphasic computed tomography with mesenteric computed tomography angiography in the diagnosis of acute mesenteric ischemia. Am J Surg. 2009;197:429–433. doi:10.1016/j.amjsurg.2008.02.011
15. Froment P, Alerci M, Vandoni RE, et al. Stenting of a spontaneous dissection of the superior mesenteric artery: a new therapeutic approach? CVIR. 2004;27. doi:10.1007/s00270-003-0158-y
16. Wu X, Wang T, Chen M. Percutaneous endovascular treatment for isolated spontaneous superior mesenteric artery dissection: report of two cases and literature review. Cathet Cardio Intervent. 2009;73:145–151.
17. Wang K, Chen W, Shi H, et al. Mesenteric artery remodeling after conservative management in patients with isolated mesenteric artery dissection. J Vasc Interv Radiol. 2019;30:1964–1971. doi:10.1016/j.jvir.2019.05.005
18. Li N, Lu QS, Zhou J. Diagnosis and endovascular stent graft treatment of spontaneous isolated superior mesenteric artery dissection. Chinese J of General Sur. 2012;21(12):1485–1488.
19. Jianping GU. Chinese College of Interventionalists Committee on Peripheral Vascular Intervention. Expert consensus on the management of isolated superior mesenteric artery dissection. Chin J Radiol. 2021;55(4):7.
20. Niwa N, Nishiyama T, Ozu C, et al. Acute aortic dissection in a patient with metastatic renal cell carcinoma treated with axitinib. Acta Oncologica. 2015;54:567–568. doi:10.3109/0284186X.2014.963887
21. Funahashi Y, Sassa N, Inada-Inoue M, et al. Acute aortic dissection in a patient receiving multiple tyrosine kinase inhibitors for 5 years. Aktuel Urol. 2014;45:132–134. doi:10.1055/s-0033-1363274
22. Hatem R, Bebawi E, Schampaert E. Potential sunitinib-induced coronary artery and aortic dissections. Cana J Cardiol. 2017;33:830.e17–830.e18. doi:10.1016/j.cjca.2017.03.002
23. Xu L, Wang B, Ding W. Abdominal aortic dissection during sorafenib therapy for hepatocellular carcinoma. Clin Res Hepatol Gastroenterol. 2017;41:e24–e25. doi:10.1016/j.clinre.2016.12.005
24. Wang S, Chen M, Zhang X, et al. Aneurysm and artery dissection following the use of vascular endothelial growth factor inhibitor: a real‐world analysis using a spontaneous reporting system. JAHA. 2021;10:e020844. doi:10.1161/JAHA.121.020844
25. Oshima Y, Tanimoto T, Yuji K, et al. Association between aortic dissection and systemic exposure of vascular endothelial growth factor pathway inhibitors in the Japanese adverse drug event report database. Circulation. 2017;135:815–817. doi:10.1161/CIRCULATIONAHA.116.025144
26. Liolis E, Mulita F, Koutras A, Makatsoris T, Sivolapenko G. Exploring bevacizumab’s role in gynecological cancers: an up-to-date narrative review focusing on ovarian cancer. Mater Sociomed. 2024;36(4):268–279. PMID: 39963442; PMCID: PMC11830232. doi:10.5455/msm.2024.36.268-279
27. Heraudet L, Domblides C, Daste A, et al. Safety of sunitinib in patients with renal cell carcinoma following nephrectomy. Expert Opin Drug SAF. 2020;19:799–806. doi:10.1080/14740338.2020.1774551
28. Cereda V, Formica V, Roselli M. Issues and promises of bevacizumab in prostate cancer treatment. Expert Opin Biol Ther. 2018;18(6):707–717. Epub 2018 May 30. PMID: 29781343. doi:10.1080/14712598.2018.1479737
29. Bonnet C, Sibon I. Potential role of anti-VEGF targeted therapies in cervical artery dissection: a case report. Revue Neurologique. 2015;171:677–679. doi:10.1016/j.neurol.2015.03.010
30. Lenihan DJ, Kowey PR. Overview and management of cardiac adverse events associated with tyrosine kinase inhibitors. Oncologist. 2013;18:900–908. doi:10.1634/theoncologist.2012-0466
31. Olsson A-K, Dimberg A, Kreuger J, et al. VEGF receptor signalling ? In control of vascular function. Nat Rev Mol Cell Biol. 2006;7:359–371. doi:10.1038/nrm1911
32. Guyon J, Gouverneur A, Maumus-Robert S, et al. Association between antiangiogenic drugs used for cancer treatment and artery dissections or aneurysms. JAMA Oncol. 2021;7:775. doi:10.1001/jamaoncol.2021.0210
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.