Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 10
Medication Utilization Patterns 90 Days Before Initiation of Treatment with Repository Corticotropin Injection in Patients with Infantile Spasms
Authors Gold LS, Nazareth TA, Yu TC, Fry KR, Mahler NH ![]() , Rava A, Waltrip II RW, Hansen RN
, Rava A, Waltrip II RW, Hansen RN
Received 5 July 2019
Accepted for publication 6 December 2019
Published 3 January 2020 Volume 2019:10 Pages 195—207
DOI https://doi.org/10.2147/PHMT.S222010
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Laura S Gold,1,2 Tara A Nazareth,3 Tzy-Chyi Yu,3 Keith R Fry,3 Nancy Ho Mahler,3 Andrew Rava,3 Royce W Waltrip II,3 Ryan N Hansen2,4
1Department of Radiology, University of Washington, Seattle, WA, USA; 2CHOICE Institute, School of Pharmacy, University of Washington, Seattle, WA, USA; 3Mallinckrodt Pharmaceuticals, Bedminster, NJ, USA; 4Department of Health Services, University of Washington, Seattle, WA, USA
Correspondence: Laura S Gold
Department of Radiology, University of Washington, Box 359558, Seattle, WA 98195-9558, USA
Tel +1 206-543-2749
Fax +1 206-543-8609
Email [email protected]
Introduction: Infantile spasms (IS) is a rare and devastating form of early childhood epilepsy. Two drugs are approved in the United States for treatment of IS, H.P. Acthar® Gel (repository corticotropin injection, RCI) and Sabril® (vigabatrin). Given real-world variation in treatment of patients with IS, this study characterized treatment patterns with IS medications and determined all-cause health care resource utilization (HCRU) during the 90 days before initiating therapy with RCI in patients with IS.
Materials and methods: Truven Health MarketScan® Research Databases were used to identify commercially insured US patients <2 years of age at RCI initiation with an IS diagnosis, per label use, from 1/1/07 to 12/31/15; presence of an electroencephalogram following diagnosis was required to assure diagnosis. Diagnosis codes and dispensed IS treatments of interest (drug classes including corticosteroids, vigabatrin, and other antiepileptic drugs [AEDs] excluding vigabatrin) before RCI initiation were evaluated.
Results: The 5 most common diagnoses other than IS observed in the study cohort (n=422) were “other convulsions,” “acute upper respiratory infection,” “esophageal reflux,” “epilepsy, unspecified,” and “abnormal involuntary muscle movements.” Among the study cohort, 51.7% received RCI first; 38.9% received 1 drug class and 9.5% received >1 drug class before RCI initiation. Other AEDs were dispensed most often, either alone (31.3%) or with other drug classes (9.3%). Mean HCRU included 11.8 all-cause outpatient visits and 4.5 medications dispensed. Patients who received RCI or corticosteroids as their initial IS treatment had the lowest and second-lowest HCRU.
Conclusion: In the 90 days before initiating RCI, patients with IS received multiple diagnoses and treatments, characterized by frequent HCRU. Use of RCI first (no prior IS medications) and AEDs first were associated with the lowest and highest HCRU, respectively, across all categories (all-cause outpatient visits, emergency department visits, hospital admissions, prescription medications).
Keywords: Infantile spasms, early diagnosis, early treatment, health care resource utilization, medication patterns
Introduction
Infantile spasms (IS; West syndrome) is a catastrophic form of childhood epilepsy with typical onset in infancy between 3 and 7 months.1–3 Although rare, IS is the most common epileptic encephalopathy of infancy, with an incidence of 1.6 to 4.5 per 10,000 live births and a worldwide prevalence of 0.015 per 1,000 population.1,2,4,5
Clinical presentation of IS is characterized by epileptic spasms that appear in clusters of short, sudden contractions of the axial musculature.1 Clusters of up to 100 of spasms can occur and are often temporally related to sleep. Although not required for diagnosis, the characteristic hypsarrhythmia pattern of high-voltage, disorganized, and asynchronous brain waves typically occurs and is observable on electroencephalogram (EEG).1,6 The EEG is also used to monitor complete resolution of the hypsarrhythmia during treatment, which together with cessation of spasms signals treatment effectiveness.7
There are several types of IS, distinguished by cause and subsequent classification of the etiology, which respond differently to treatment. Currently, the only 2 drugs approved by the US Food and Drug Administration (FDA) for treatment of IS are repository corticotropin injection (RCI; H.P. Acthar® Gel) and vigabatrin (Sabril®).9–11 RCI is more effective than vigabatrin in the short-term treatment of all types of IS except tuberous sclerosis complex (TSC), per the 2012 update of the American Academy of Neurology (AAN) and the Child Neurology Society (CNS) guideline.12 The antiepileptic drug (AED) vigabatrin is recommended for first-line treatment of TSC, a symptomatic form of IS, by the US Consensus Report of the Infantile Spasms Working Group.1,7
Because of the often-subtle initial presentation of IS and their resemblance to colic, normal startle reflex, and gastroesophageal reflux, IS may initially go unrecognized, potentially delaying diagnosis.6,16 Further delays can occur because most nonspecialist health care providers are unfamiliar with and may not recognize IS, thus leading to delayed interventions and deferred referrals to pediatric neurologists or epileptologists, with attendant developmental consequences.6,17
In addition to those challenges, real-world management of IS within the medical community has been subject to variable practice patterns partially because of insufficient evidence of their comparative effectiveness, complicated by the low number of cases, and the complex etiology of IS. A lack of clear guidance exists recommending drug selection and dosage.1,12,18,19 In addition to the approved and recommended therapies RCI and vigabatrin, patients may be also treated, often first, with other AEDs and off-label treatments that are neither specific nor approved (ie, intravenous immunoglobulin, ketogenic diet, and AEDs topiramate, valproic acid, and sulthiame) for IS.1,7,20 Inadequate management, whether because patients are refractory to treatment or treatment is delayed, can lead to neurodevelopmental delay, intellectual disability, learning difficulties, autism spectrum disorder, transition to epileptic seizures, or mortality.1,7,15,27 Almost all patients with IS of unknown cause can have normal outcomes if treatment begins within 1 month of spasm onset.7,8 Thus, rapid treatment initiation is recommended to improve long-term cognitive and developmental outcomes.1,7,8,12,13,14 The medical community is consequently focusing on shortening the length of time to diagnosis and treatment of IS and identifying the underlying cause of disease to optimize treatment and health outcomes.1,6,7,12,19
With the aim of exploring time to treatment and the patient journey leading up to appropriate treatment, the purpose of this study was to characterize real-world treatment patterns with IS medications and evaluate all-cause health care resource utilization (HCRU) during the 90 days before initiating therapy with RCI in patients with IS.
Materials and Methods
Study Design
A retrospective cohort analysis was conducted on patients diagnosed with IS who were treated with RCI in the United States, using Truven Health Analytics MarketScan® Commercial Claims and Encounters Databases. Because this was a retrospective analysis of deidentified claims data, no Institutional Review Board approval or patient consent were needed.
Data Source
Truven Health Analytics MarketScan® Commercial Claims and Encounters Databases contain deidentified individual patient-level data (medical and pharmacy claims as well as insurance enrollment information) for individuals covered by employer-sponsored commercial health insurance in the United States. Inpatient and outpatient claims include procedure- and visit-level details from medical claims such as International Classification of Diseases, 9th and 10th Revisions, Clinical Modification (ICD-9-CM and ICD-10-CM) diagnosis and procedure codes, Current Procedural Terminology (CPT) codes, dates of service, and financial expenditure information for both the patients and their insurance plans. The pharmacy claims provide prescription medication dispensation details that include National Drug Code and generic identifiers of the drugs dispensed, dates of dispensation, quantities and days (of medication) supply, and payment details for each claim. Eligibility and demographics information about each patient, including age (only available to the nearest year), gender, type of insurance plan, geographic region, and enrollment status by month, are also available.
Patient Selection
Patients were included in the study cohort if they had a diagnosis code for IS (ICD-9-CM=345.60; ICD-10-CM=G40.821, G40.822), were treated with ≥1 medication for IS at least 1 of which was RCI, were ˂2 years of age when initiating treatment with RCI as per the RCI label (the index date), and were enrolled in their insurance plan for at least 90 days before the index date.22,23 Additionally, patients had to have undergone at least 1 EEG (see Supplement 2 for CPT codes) following their IS diagnosis to ensure that the EEG was being used for purposes of monitoring treatment and resolution of the hypsarrhythmia rather than for diagnostic purposes.23 Patients with IS were excluded from the study cohort if they had a diagnosis of TSC (ICD-9-CM code 759.5; ICD-10-CM code Q85.1), given RCI is recommended treatment for IS not due to TSC.22
Treatment-Specific Subgroups
Pharmacy claims during the 90 days preceding the index date were used to identify treatments of interest, which were categorized by drug class. Each drug class could reflect use of ≥1 drug from that class. Use of intravenous immunoglobulin (IVIG) was also evaluated. Distinct treatment-specific subgroups were identified based on the medication(s) received in the 90 days prior to initiation of RCI. Each patient in the study cohort was assigned to 1 treatment-specific subgroup.
Patient characteristics were stratified by the treatment-specific subgroups and were evaluated descriptively. The most common diagnoses other than IS that were observed in the 90 days before initiating treatment with RCI were identified. To facilitate this analysis, the ICD-10-CM codes were converted to ICD-9-CM codes using a publicly available crosswalk tool to find the most common diagnoses.24
Health Care Resource Utilization
Unique dates of claims (ie, while multiple office visits or tests may have occurred on a single day, only 1 encounter was counted per day for each patient) were counted to reflect HCRU per person per month in the 90 days preceding RCI initiation, although this could potentially lead to underestimation of HCRU. The following HCRU categories were examined by treatment group: 1) Outpatient visits by location (ie, office, hospital, other), 2) Outpatient visits to specialists (allergists, cardiologists, endocrinologists, gastroenterologists, geneticists, hematologists, neonatologists, nephrologists, neurologists, oncologists, ophthalmologists, orthopedists, otolaryngologists, pulmonologists, rheumatologists, surgeons, toxicologists, and urologists) and nonspecialist health care providers (pediatricians, family practice, internal medicine); 3) Emergency department visits; and 4) hospital/inpatient admissions. Since patients could have received multiple outpatient services on the same date (ie, visited both a specialist and a nonspecialist on the same date), the sum of all categories of outpatient visits may be greater than the total all-cause outpatient visits. In addition, all medications filled during the 90 days before RCI therapy were counted.
Statistical Analyses
Descriptive analysis was conducted using SAS 9.3 (Cary, NC). Mean and standard deviation (SD) were reported for count or continuous variables. Numbers and percents were reported for categorical variables.
Results
A total of 5,004 patients in the Truven Health Analytics MarketScan® Research Databases during 2007–2015 had an IS diagnosis (Figure 1). A total of 231 patients with IS (5% of all patients with IS diagnoses) were excluded because they were diagnosed with TSC. After further excluding all individuals who had never received RCI, individuals receiving RCI who were 2 years or older (ie, who were above the age specified in the RCI label), those who were not enrolled for at least 90 days before the index date, and those who did not meet the EEG criteria, 422 patients with IS who were treated with RCI comprised the study cohort.
 |
Figure 1 Flow of patients with infantile spasms. This flow chart illustrates the process for obtaining the cohort of patients with electroencephalogram (EEG)-verified infantile spasms. Abbreviations: CPT, current procedural terminology; RCI, repository corticotropin injection; Rx, prescription. |
As shown in Table 1, RCI was the first treatment dispensed to 51.7% of the study cohort (No other drug classes). Almost 39% of the study cohort received the following drugs of interest before receiving RCI: AEDs to 31.3%, corticosteroids to 5.5%, and vigabatrin to 2.1%. Approximately 9.5% of the study cohort received multiple drug classes before receiving RCI; 9.0% received 2 drug classes and 0.5% received 3 drug classes. No patients received treatment with IVIG.
 |
Table 1 Prescription Medication Patterns Before Initiating Repository Corticotropin Injectiona,b |
Five distinct treatment-specific subgroups were identified, based on the medication(s) received in the 90 days prior to initiation of RCI: 1) No IS Medications – defined by not having received any of the IS treatments of interest noted below – before/other than RCI, 2) Vigabatrin Only, 3) AEDs Only – defined as AEDs excluding vigabatrin (see Supplement 1 for list of drug names included in this category), 4) Corticosteroids Only (see Supplement 1 for list of drug names included in this category), and 5) Multiple Drug Classes (≥2 types from the other groups). Characteristics of the full cohort, stratified by receipt of IS treatment(s) before initiating RCI therapy, are shown in Table 2. Most patients in the study cohort were male (57.1%), received RCI at <1 year of age (83.2%), and were covered by a preferred provider organization (PPO) health insurance plan (60.0%). Although patients resided throughout the country, the South was the most common area of residence (37.0%).
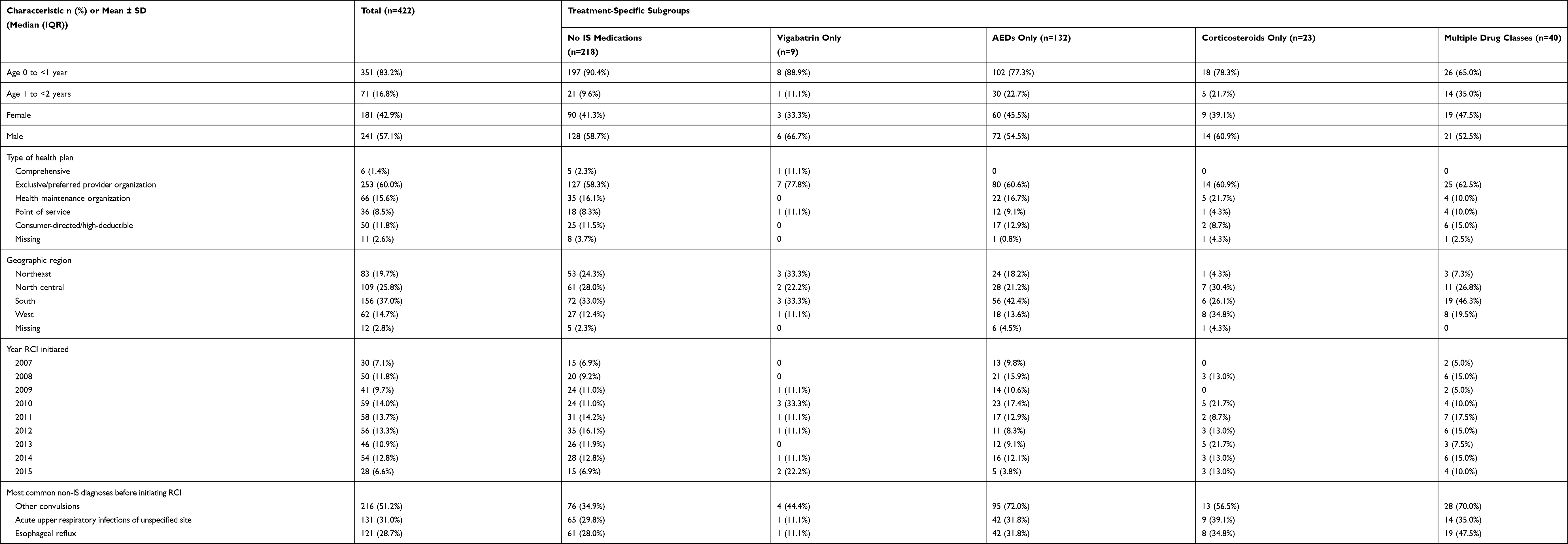 |
Table 2 Characteristics of the Full Cohort of Patients with IS Stratified by Medications Taken Before Initiating Repository Corticotropin Injection Therapy |
The most common diagnoses other than IS within the study cohort of IS patients were “other convulsions” (51.2%), followed by “acute upper respiratory infections” (31.0%), “esophageal reflux” (28.7%), “epilepsy, unspecified” (25.4%), and “abnormal involuntary muscle movements” (22.7%). The diagnosis of “epilepsy, unspecified” was also more common in the AEDs Only and the Multiple Drug Classes subgroups, relative to the other subgroups (44.7% and 60.0%, respectively). Although patients in the No IS Medications subgroup also received these diagnoses, far fewer received a diagnosis of “epilepsy, unspecified” (8.3%).
As shown in Table 2, there was a mean ± SD of 11.8 ± 10.1 all-cause outpatient visits during the 90 days before RCI initiation; most of these were to nonspecialist providers (10.3 ± 9.6 to nonspecialists vs. 2.6 ± 3.4 to specialists) and occurred in the month before RCI initiation. Nearly twice as many outpatient health care visits occurred in the physician office setting (6.6 ± 5.9) compared with the hospital setting (3.5 ± 3.9) or another location (3.6 ± 7.4) (Table 2). The per-patient average ± SD was 1.0 ± 0.8 hospital admissions and 4.5 ± 5.0 prescription medications during the 90 days before RCI initiation, most of which (mean of 2.1 per person) were dispensed in the month before the index date.
Among the 5 treatment-specific subgroups, patients in the Multiple Drug Classes subgroup before initiating RCI therapy had the largest all-cause total HCRU: Mean number of total outpatient visits (16.6 ± 10.1), hospital admissions (1.4 ± 1.4), as well as prescription medications (11.0 ± 7.1) per person (Table 2). Patients in the No IS Medications subgroup had the lowest all-cause HCRU: Mean number of total outpatient visits (9.9 ± 9.8), hospital admissions (0.9 ± 0.6), emergency department visits (0.3 ± 0.7), and prescription medications (2.1 ± 2.8) per person. After that, patients in the Corticosteroids Only subgroup had the next lowest HCRU of the remaining treatment groups: Mean number of total outpatient visits (10.0 ± 6.5), hospital admissions (1.0 ± 0.8), emergency department visits (0.5 ± 0.7), and prescription medications (4.7 ± 3.0) per person. Patients in the Vigabatrin Only subgroup had the following HCRU: Mean number of total outpatient visits (14.2 ± 10.9), hospital admissions (1.3 ± 1.3), emergency department visits (0.4 ± 1.0), and prescription medications (4.3 ± 3.3) per person. Patients in the AEDs Only subgroup had next to the highest HCRU: Mean number of total outpatient visits (13.5 ± 10.4), hospital admissions (1.0 ± 0.8), emergency department visits (0.4 ± 0.8), and prescription medications (6.4 ± 4.9) per person.
As seen in Figure 2, in the 30 days before initiating RCI treatment, outpatient visits to specialists and nonspecialists were highest among all treatment-specific subgroups. The Multiple Drug Classes subgroup had the most outpatient visits to specialists and nonspecialists per person; those in the No IS Medications subgroup or Corticosteroids Only subgroup had the fewest visits to specialists and nonspecialists in each 30-day period. Similar patterns are illustrated in Figures 3 and 4, for outpatient visits stratified by location and prescription medications dispensed per person, respectively; as expected, across the entire 90-day period, patients in the Multiple Drug Classes subgroup had the highest number of prescription medications per person, whereas patients in the No IS Medications subgroup had the lowest number of prescription medications per person.
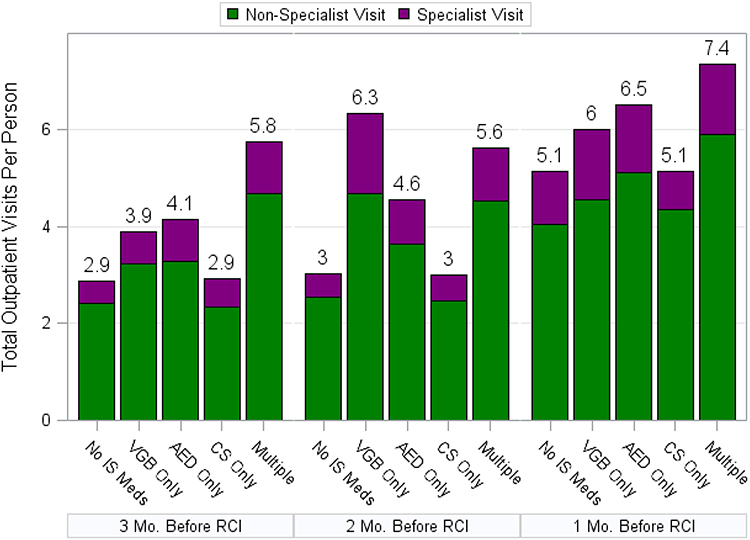 |
Figure 2 Outpatient visits to specialists and nonspecialists. Outpatient visits to specialists and nonspecialists are shown for each of the 5 treatment-specific subgroups, stratified by month during the 90-day preindex period. Abbreviations: AED, antiepileptic drug; CS, corticosteroids; IS, infantile spasms; RCI, repository corticotropin injection; VGB, vigabatrin. |
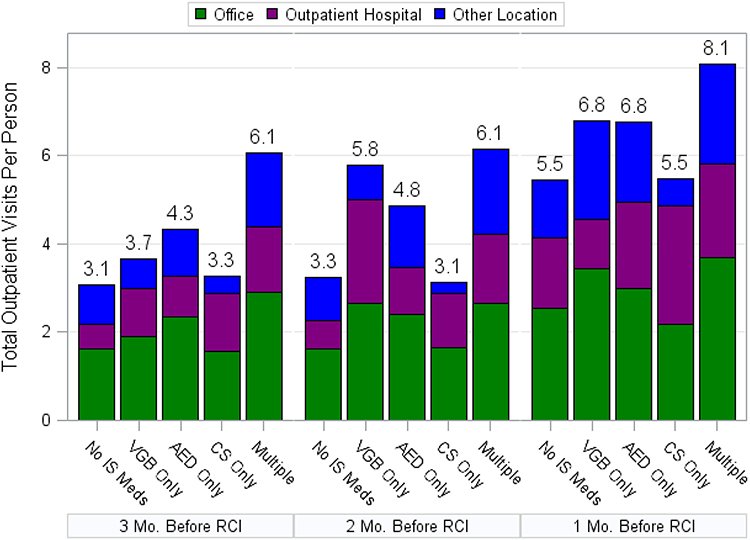 |
Figure 3 Outpatient visits are shown by setting, including the office, outpatient hospital, or other location. Outpatient visits are shown for each of the 5 treatment-specific subgroups, stratified by month during the 90-day preindex period. Abbreviations: AED, antiepileptic drug; CS, corticosteroids; IS, infantile spasms; RCI, repository corticotropin injection; VGB, vigabatrin. |
 |
Figure 4 Prescription medications that were dispensed. Prescription medications that were dispensed are shown for each of the5 treatment-specific subgroups, stratified by month during the 90-day preindex period. Abbreviations: AED, antiepileptic drug; CS, corticosteroids; IS, infantile spasms; RCI, repository corticotropin injection; VGB, vigabatrin. |
All treatment-specific subgroups had similar low emergency department use per person during the 90-day period (Figure 5). Figure 5 shows that emergency department use peaks in the 60 days before RCI use for patients in the Vigabatrin Only and Multiple Drug Classes subgroups and in the 30 days prior for all other subgroups. Hospital inpatient admissions were similarly at their highest point for all 5 treatment-specific subgroups in the 30 days before RCI initiation, although the Vigabatrin Only subgroup also had high inpatient admissions during the 60 days prior (Figure 6).
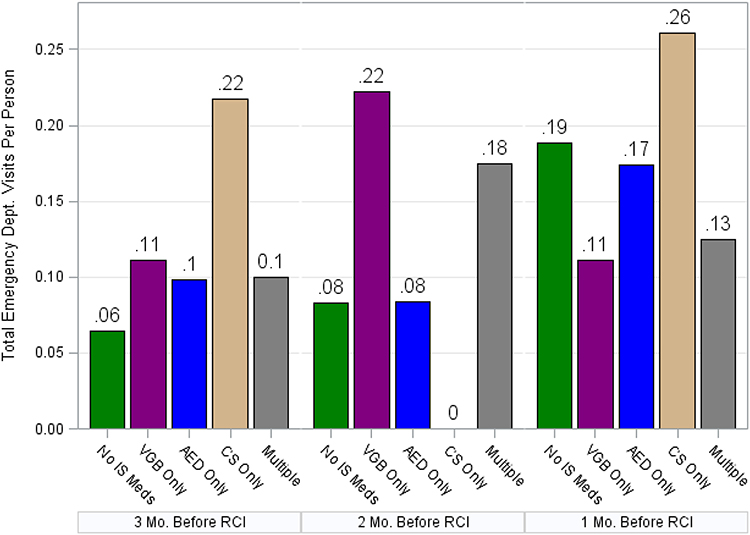 |
Figure 5 Emergency department visits. Emergency department visits are shown for each of the 5 treatment-specific subgroups, stratified by month during the 90-day preindex period. Abbreviations: AED, antiepileptic drug; CS, corticosteroids; IS, infantile spasms; RCI, repository corticotropin injection; VGB, vigabatrin. |
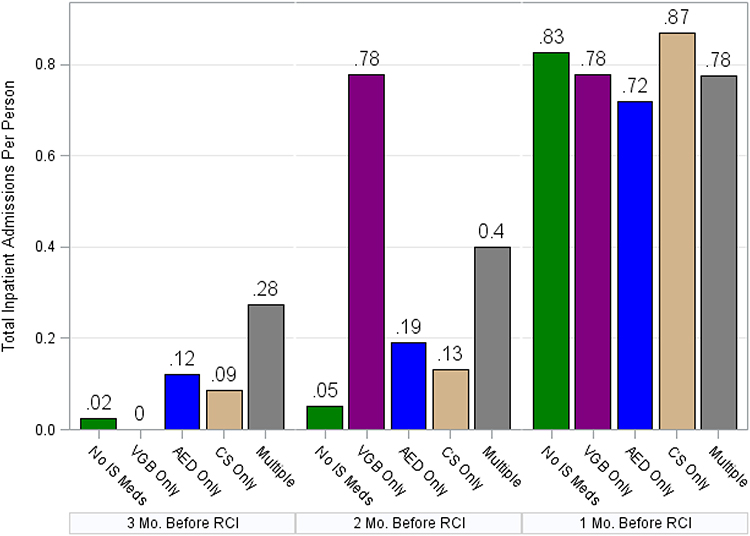 |
Figure 6 Hospital admissions. Hospital inpatient admissions are shown for each of the 5 treatment-specific subgroups, stratified by month during the 90-day preindex period. Abbreviations: AED, antiepileptic drug; CS, corticosteroids; IS, infantile spasms; RCI, repository corticotropin injection; VGB, vigabatrin. |
Discussion
Numerous health care encounters occurred in the 90 days before initiation of RCI therapy in our cohort of IS patients. All measures of HCRU (outpatient visits, inpatient visits, emergency department visits, and prescription medications) increased with time and across all treatment-specific subgroups evaluated, with per-person-per-month HCRU peaking in the 30 days before initiation of RCI therapy.
Drug classes were used to define treatment-specific subgroups to obtain insight into heterogeneity in therapeutic management and associated HCRU. Over half of the study cohort (51.7%) received RCI as their first IS medication (the No IS Medications subgroup, who received no other IS drug class before RCI initiation). Of the 38.9% of the total cohort that received 1 IS drug class before RCI, AEDs were the drug class dispensed most commonly, to 31.3% (of the 38.9%), or 12.2% of the total cohort. Approximately 9.5% of the study cohort received 2 or more IS drug classes. One or more specific medications may have been dispensed from a particular drug class and therefore may have actually resulted in a higher number of treatments received.
When HCRU was examined by treatment-specific subgroup, the number of drug classes received prior to RCI was generally positively associated with the volume of all-cause HCRU observed. The RCI-first subgroup (ie, No IS Medications subgroup) had the lowest total all-cause outpatient visits, followed by the Corticosteroids Only subgroup, and the Multiple Drug Classes subgroup had the highest overall all-cause outpatient visits. The Corticosteroids Only subgroup had 2.6 more prescription fills on average than the RCI-first subgroup. In addition to receiving the fewest prescription fills, patients whose initial treatment was RCI also had the lowest number of inpatient visits.
Among those receiving 1 drug class before RCI, the Vigabatrin Only subgroup (who received Vigabatrin as the first IS drug class prior to RCI initiation) and the AEDs Only subgroup (who received AEDs as the first IS drug class prior to RCI initiation) had the highest total all-cause outpatient visits. Those in the Multiple Drug Classes subgroup, who received multiple IS drug classes prior to RCI initiation, had the highest HCRU in all but 1 of the settings evaluated (ie, emergency department visits); that is, they had the highest prescription burden as well as more all-cause visits and hospital admissions.
It is unclear whether patients in certain treatment-specific subgroups may have had more complex health states or seizure types, explaining the high rates of epilepsy-related diagnoses observed. For example, the AEDs Only and Multiple Drug Classes subgroups had the highest number of diagnoses of “other convulsions” (ie, 72.0% and 70.0%, respectively) and “epilepsy, unspecified” (ie, 44.7% and 60%, respectively); in keeping, they also had the highest number of nonspecialist and specialist visits among all other treatment-specific subgroups before RCI initiation. In particular, the Multiple Drug Classes subgroup had higher outpatient use in the prior 30 days and relatively higher hospital inpatient admissions during the entire preceding 90-day period, indicating an unfortunate peak in health care use and burden of illness before RCI initiation.
The presence of these diagnoses and the trends in HCRU indicate that complex seizure types may have complicated IS diagnosis and/or warranted such use of therapy (eg, AEDs Only subgroup, the Multiple Drug Classes subgroup) in some patients. However, given the common preceding diagnoses observed with some patients, number of nonspecialist visits, and low awareness of IS among many practitioners, recognition of IS was likely delayed in some patients for reasons of underdiagnoses or misdiagnosis. Diagnoses often mistaken for IS (eg, reflux) were among those we commonly observed and were therefore assumed to be delayed IS diagnosis. Further, if IS was not correctly identified at the first presentation, AEDs other than vigabatrin may have been used for general therapeutic management of seizures.7 This would delay timely receipt of appropriate therapy, affording greatest potential effectiveness to patients with IS1 and imposing a critical and untimely burden on patients, their family, and the health care system. In all treatment-specific subgroups, the exact percentages of patients initially misdiagnosed or underdiagnosed and the percentage of patients with complex seizure types, as well as the details of their seizures and seizure types, cannot be accurately estimated due to limited clinical data contained in administrative claims.
There is a compelling need among pediatricians and those treating infants in community practices to recognize or consider IS quickly and to refer patients to pediatric neurologists and epileptologists for diagnosis and timely treatment.25 Initiatives are underway in the United States to improve early recognition and treatment of IS. In a past quality improvement initiative to increase the number of patients with IS who are receiving initial treatment with approved first-line therapy, after introduction of their management protocol, 100% of patients with IS initiated therapy with a first-line treatment, resulting in an improved remission rate at 3 months after diagnosis (78.8% after implementation of the management protocol vs 30.6% before).3 In another initiative, the Infantile Spasms Action Network developed a campaign to raise awareness of IS. Research conducted with pediatric neurologists/epileptologists, pediatricians, nurse practitioners, and parents/caregivers of infants diagnosed with IS informed the campaign’s key messages with a call to action of STOP: See the signs, Take a video, Obtain diagnosis, and Prioritize treatment to bring about a sense of urgency.26
Early diagnosis and initiation of approved therapy to expedite and streamline treatment during a critically short therapeutic window may help to reduce unnecessary HCRU for patients with IS and their families in the short term and potentially positively impact long-term prognosis of IS in the longer term.1,13,20 For example, 1 study showed that a shorter lead time between spasm onset and treatment (7 days or less vs 8–14 days, 15–30 days, 1–2 months, or >2 months) for IS significantly improved patients’ Vineland Adaptive Behavior Scale scores, which measures patients’ ability to cope with environmental changes, demonstrate independence, and learn new skills.24 Another study indicated that infants who had shorter periods in which they were experiencing spasms, and therefore shorter times of epileptic encephalopathy, had improved neurodevelopmental outcomes relative to patients who had longer periods in which they experienced spasms.7,8
The population of patients with IS taking RCI in this study may not be representative of the general population of patients with IS. Because we relied on health insurance claims data, we did not have access to data such as seizure types, EEG test results, or chart notes that may have provided important clinical details. Counting of claims by date rather than by occurrence likely led to an underestimation of HCRU but eliminated the possibility of overcounting. Additionally, claims data are not as reliable as chart reviews for assessing information like provider specialty, and our counts of visits to neurologists may have been underestimates. Reliance on claims data may also have resulted in underidentification of IS and TSC cases because these conditions are not always coded reliably. This was confirmed to be the case with TSC, the prevalence of which was only 5% of total IS cases in the study (half of the expected TSC population in the United States).1,7 The sample sizes for some treatment-specific subgroups, particularly Vigabatrin Only and Corticosteroids Only before RCI initiation, were small, at approximately ≤5% of the total sample. However, cohorts with IS are characteristically extremely small given the prevalence of the condition. Diagnoses were assumed to be purposeful and indicate known conditions or lack thereof. In all subgroups, the exact percentage of patients initially misdiagnosed and the percentages of patients with complex seizure types, as well as the details of their seizures and seizure types, cannot be accurately estimated.
Furthermore, although our data indicated that patients had filled prescription medications of interest, we could not confirm that medications were actually taken. In addition, the rationale and health conditions associated with each prescription of interest studied here could not be ascertained; this would impact our conclusions, in particular for patients taking corticosteroids, given their broad use for many conditions. Also, by evaluating trends in HCRU by drug class rather than by specific medications, we may have underestimated the volume of medication use in this cohort and types and the duration of those drugs used. Similarly, other medications may have been used off-label that were not included in our analysis as treatments of interest. Although visits to specialists and nonspecialists may together serve as potential proxies for delayed diagnoses and possibly severity and/or complexity of the patient’s health, due to limitation of the data, additional granularity permitting further insights was not available. Additionally, specialist in claims were often not well recorded; therefore, specialist visits could be low due to missing data.
Conclusion
Diagnosis and appropriate treatment of IS are subject to delays that negatively affect outcomes, with long-term neurodevelopmental consequences. This study provided a better understanding of the treatment patterns, diagnoses, and health care resource use during the 90 days before RCI initiation, with the ultimate goal of recognizing the complexity and heterogeneity of the patient journey and the critical delays faced by caregivers and patients leading up to diagnosis of IS and initiation of IS treatment. Patients with IS who first receive AEDs (except vigabatrin) or multiple classes of drugs often have an increased number of diagnoses, with higher percentages of diagnoses commonly mistaken for IS, more office visits to health care providers (with a higher percentage of nonspecialist to specialist visits), and higher all-cause HCRU across most categories compared with patients with IS who received RCI therapy first, with no other IS medications prior. This underscores the need for earlier and improved recognition and targeted treatment of IS to improve patient outcomes, as well as focused efforts towards increased awareness among various health care provider types.
Abbreviations
AAN, American Academy of Neurology; AED, antiepileptic drug; CNS, Child Neurology Society; CPT, Current Procedural Terminology; EEG, electroencephalogram; FDA, Food & Drug Administration; HCRU, health care resource utilization; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification; IS, infantile spasm; IVIG, intravenous immunoglobulin; RCI, repository corticotropin injection; TSC, tuberous sclerosis complex.
Acknowledgments
The authors acknowledge Tamara K. Marshall, MD, for clinical input in the study design and analysis.
Disclosure
Laura S. Gold has received salary funding from Mallinckrodt Pharmaceuticals to compensate her for the time spent to conduct this research. Tara Nazareth was an employee and stockholder of Mallinckrodt Pharmaceuticals at the time of this research. Tzy-Chyi Yu is an employee and stockholder of Mallinckrodt Pharmaceuticals. Keith R. Fry is an employee and stockholder of Mallinckrodt Pharmaceuticals. Nancy Ho Mahler is an employee and stockholder of Mallinckrodt Pharmaceuticals. Royce W. Waltrip II is an employee and stockholder of Mallinckrodt Pharmaceuticals. Ryan N. Hansen has received consulting fees from Mallinckrodt Pharmaceuticals. Andrew Rava was a student intern with Mallinckrodt at the time of this research. The authors report no other conflicts of interest in this work.
References
1. Pellock JM, Hrachovy R, Shinnar S, et al. Infantile spasms: a U.S. consensus report. Epilepsia. 2010;51(10):2175–2189. doi:10.1111/j.1528-1167.2010.02657.x
2. Trevathan E, Murphy CC, Yeargin-Allsopp M. The descriptive epidemiology of infantile spasms among Atlanta children. Epilepsia. 1999;40(6):748–751. doi:10.1111/epi.1999.40.issue-6
3. Fedak EM, Patel AD, Heyer GL, Wood EG, Mytinger JR. Optimizing care with a standardized management protocol for patients with infantile spasms. J Child Neurol. 2015;30(10):1340–1342.
4. Sidenvall R, Eeg-Olofsson O. Epidemiology of infantile spasms in Sweden. Epilepsia. 1995;36(6):572–574. doi:10.1111/epi.1995.36.issue-6
5. Luthvigsson P, Olafsson E, Sigurthardottir S, Hauser WA. Epidemiologic features of infantile spasms in Iceland. Epilepsia. 1994;35(4):802–805. doi:10.1111/j.1528-1157.1994.tb02514.x
6. Wheless JW, Gibson PA, Rosbeck KL, et al. Infantile spasms (West syndrome): update and resources for pediatricians and providers to share with parents. BMC Pediatr. 2012;12:108. doi:10.1186/1471-2431-12-108
7. Riikonen R. Recent advances in the pharmacotherapy of infantile spasms. CNS Drugs. 2014;28(4):279–290. doi:10.1007/s40263-014-0139-5
8. Kivity S, Lerman P, Ariel R, Danziger Y, Mimouni M, Shinnar S. Long-term cognitive outcomes of a cohort of children with cryptogenic infantile spasms treated with high-dose adrenocorticotropic hormone. Epilepsia. 2004;45(3):255–262. doi:10.1111/epi.2004.45.issue-3
9. American Academy of Neurology. Treating infantile spasms: AAN summary of evidence-based guidelines for families and caregivers; 2012. Available from: https://www.aan.com/Guidelines/Home/GetGuidelineContent/553.
10. Epilepsy Foundation. Vigabatrin (Sabril) approved by FDA; 2014. Available from: https://www.epilepsy.com/article/2014/3/vigabatrin-sabril-approved-fda.
11. U.S. Food and Drug Administration. Drug approval package: H.P. Acthar Gel (repository corticotropin) Injection; 2010. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/022432_hp_acthar_gel_toc.cfm.
12. Go CY, Mackay MT, Weiss SK, et al. Evidence-based guideline update: medical treatment of infantile spasms. Report of the guideline development subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2012;78(24):1974–1980.
13. Lombroso CT. A prospective study of infantile spasms: clinical and therapeutic correlations. Epilepsia. 1983;24(2):135–158. doi:10.1111/epi.1983.24.issue-2
14. Lux AL, Edwards SW, Hancock E, et al. The United Kingdom Infantile Spasms Study (UKISS) comparing hormone treatment with vigabatrin on developmental and epilepsy outcomes to age 14 months: a multicentre randomised trial. Lancet Neurol. 2005;4(11):712–717. doi:10.1016/S1474-4422(05)70199-X
15. Mackay MT, Weiss SK, Adams-Webber T, et al. Practice parameter: medical treatment of infantile spasms: report of the American Academy of Neurology and the Child Neurology Society. Neurology. 2004;62(10):1668–1681. doi:10.1212/01.WNL.0000127773.72699.C8
16. Auvin S, Hartman AL, Desnous B, et al. Diagnosis delay in West syndrome: misdiagnosis and consequences. Eur J Pediatr. 2012;171(11):1695–1701. doi:10.1007/s00431-012-1813-6
17. American Academy of Pediatrics. Diagnosis and management of infantile spasms; 2019. Available from: https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/infantile-spasms/Pages/default.aspx.
18. Nelson GR. Management of infantile spasms. Transl Pediatr. 2015;4(4):260–270. doi:10.3978/j.issn.2224-4336.2015.09.01
19. D’Alonzo R, Rigante D, Mencaroni E, Esposito S. West syndrome: a review and guide for paediatricians. Clin Drug Investig. 2018;38(2):113–124. doi:10.1007/s40261-017-0595-z
20. Gold LS, Schepman PB, Wang WJ, et al. Healthcare costs and resource utilization in patients with infantile dpasms treated with H.P. Acthar Gel(ρ). Adv Ther. 2016;33(8):1293–1304. doi:10.1007/s12325-016-0361-2
21. ICD9Data.com. 2012 ICD-9-CM diagnosis code 759.5; 2012. Available from: http://www.icd9data.com/2012/Volume1/740-759/759/759.5.htm.
22. Natus Neurology. Neurology diagnostics EEG – 2014 reimbursement; 2014. Available from: https://studylib.net/doc/18564534/neurology-diagnostics-eeg—2014-reimbursement.
23. ICD10Data.com. Convert ICD-9-CM codes to ICD-10-CM/PCS, or convert ICD-10-CM/PCS codes to ICD-9-CM; 2018. Available from: https://www.icd10data.com/Convert.
24. O’Callaghan FJ, Lux AL, Darke K, et al. The effect of lead time to treatment and of age of onset on developmental outcome at 4 years in infantile spasms: evidence from the United Kingdom Infantile Spasms Study. Epilepsia. 2011;52(7):1359–1364. doi:10.1111/j.1528-1167.2011.03127.x
25. Hussain SA, Lay J, Cheng E, Weng J, Sankar R, Baca CB. Recognition of infantile spasms is often delayed: the ASSIST study. J Pediatr. 2017;190:215–221.e211. doi:10.1016/j.jpeds.2017.08.009
26. Child Neurology Foundation. Infantile spasms awareness; 2018. Available from: https://www.childneurologyfoundation.org/programs/infantilespasms/.
27. Widjaja E, Go C, McCoy B, Snead OC. Neurodevelopmental outcome of infantile spasms: A systematic review and meta-analysis. Epilepsy Res. 2015;109:155–162.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.