Back to Journals » Patient Preference and Adherence » Volume 15
Medication Management Frameworks in the Context of Self-Management: A Scoping Review
Authors Cadel L ![]() , Cimino SR, Rolf von den Baumen T
, Cimino SR, Rolf von den Baumen T ![]() , James KA
, James KA ![]() , McCarthy L
, McCarthy L ![]() , Guilcher SJT
, Guilcher SJT ![]()
Received 25 February 2021
Accepted for publication 29 April 2021
Published 16 June 2021 Volume 2021:15 Pages 1311—1329
DOI https://doi.org/10.2147/PPA.S308223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lauren Cadel,1,2 Stephanie R Cimino,3,4 Teagan Rolf von den Baumen,1 Kadesha A James,1 Lisa McCarthy,1,2,5 Sara JT Guilcher1,3,6
1Leslie Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada; 2Institute for Better Health, Trillium Health Partners, Mississauga, Ontario, Canada; 3Rehabilitation Sciences Institute, University of Toronto, Toronto, Ontario, Canada; 4St. John’s Rehab, Sunnybrook Health Sciences Centre, North York, Ontario, Canada; 5Women’s College Research Institute, Women’s College Hospital, Toronto, Ontario, Canada; 6Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada
Correspondence: Sara JT Guilcher
Leslie Dan Faculty of Pharmacy, 144 College Street, Room 604, Toronto, ON, M5S 3M2, Canada
Tel + 1-416-946-7020
Email [email protected]
Purpose: Many individuals take multiple prescribed and unprescribed medications, also known as polypharmacy, which can be problematic. Improving medication self-management is important; however, most medication management frameworks focus on adherence and limit the integration of the core components of self-management. Therefore, the objective of this scoping review was to identify what is reported in the literature on medication management frameworks or models within the context of self-management.
Methods: Electronic databases (Medline, Embase, CINAHL and Cochrane Library) and grey literature (healthcare and government organization websites) were searched for articles that described a framework or model developed or adapted for medication management, included components of self-management and was published from January 2000 to January 2020. During the screening of titles and abstracts, 5668 articles were reviewed, 5242 were excluded and 426 were then assessed at the full-text level. Thirty-nine articles met the eligibility criteria and were included in the review.
Results: About half of the frameworks were newly developed (n=20), while the other half were adapted from, or applied, a previous model or framework (n=19). The majority of frameworks focused on medication adherence and most of the self-management domains were categorized as medical management, followed by emotional and role management.
Conclusion: Medication self-management is a complex process and often impacts multiple areas of an individual’s life. It is important for future frameworks to incorporate a comprehensive, holistic conceptualization of self-management that is inclusive of the three self-management domains – medical, emotional and role management.
Keywords: medication therapy management, self-management, framework, model, review
Introduction
The use of medication, prescribed and unprescribed, is common for the management of both acute and chronic health conditions, as well as for the maintenance of overall health.1,2 There is a high prevalence of prescription medication use worldwide, with some countries reporting an increase in medication use over the last 20 years.3–5 Among individuals taking medication, there is a large portion who are taking multiple medications (ie, polypharmacy). Polypharmacy is most commonly defined as the concomitant use of five or more medications, which often includes prescription medications, over-the-counter medications and natural health products.6 An alternative definition, also known as problematic polypharmacy7 or medication overload8 describes situations in which more medications are used than are indicated or the harms exceed the benefits.
Based on the high prevalence of medication use and polypharmacy, understanding and improving medication management is essential. Medication management can be defined as, “patient-centred care to optimize safe, effective and appropriate drug therapy”.9 Medication management involves a number of services aimed to improve clinical outcomes, such as: completing medication reviews and health assessments, monitoring treatment plans and efficacy and safety of therapy, providing education and promoting self-management.10 Self-management is a fundamental component of optimal medication management, and is defined as
an individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent in living with a chronic condition (p. 178).11
Self-management encompasses three key domains: medical, emotional and role management.12 Medical management involves tasks and responsibilities related to managing or controlling one’s condition (eg taking medication, eating healthy); emotional management involves learning to manage feelings and emotions related to one’s condition (eg fear, depression, anger); and role management includes adapting or creating new responsibilities as a result of one’s condition (eg scheduling around medication-taking, limiting or finding new hobbies).12
Over the past thirty years, the promotion of self-management of chronic conditions through programs and interventions has become increasingly common.13–17 Self-management programs and interventions commonly focus on the following areas to improve individuals’ clinical and psychosocial outcomes: education, goal setting, decision-making, seeking support and resources, self-advocating, problem solving and relationship building.12,18 Several systematic and meta reviews have noted positive outcomes of self-management programs and interventions on health outcomes for persons with diabetes,14,16,17 heart failure,19,20 asthma21,22 and depression.23 These systematic and meta reviews included studies that ranged in quality, according to the authors’ quality assessments, from low quality to very high quality.
Surprisingly, there has been limited integration of medication management and self-management, despite the effectiveness of self-management interventions and it being a fundamental component of medication management. To date, the majority of medication management frameworks are focused on patient adherence to a specific medication regimen, with a limited focus on broader concepts of self-management. Therefore, given the high use of medications and narrow focus of medication management, this scoping review sought to identify what is reported in the literature on medication management frameworks or models within the context of self-management.
Materials and Methods
A scoping review was conducted to examine the extent, range and nature of research on medication self-management frameworks, summarize current research and identify gaps in existing literature on this topic.24 This scoping review followed the methodological approach described by Levac et al25 and aligns with the methodological guidance of the Joanna Briggs Institute on conducting scoping reviews.26 The reporting guidelines of the PRISMA-ScR checklist were also followed (see Supplementary Table 1).27 A protocol was developed and registered on Open Science Framework (https://osf.io/6ckg7).
Stage 1: Identifying the Research Question
The research question guiding this scoping review was: what is reported in the literature on patient- or person-level medication management frameworks or models within the context of self-management? The three main objectives were to: (a) examine the extent to which the principles of self-management were integrated into the frameworks, (b) synthesize the key aspects of self-management principles that were captured in medication management frameworks and (c) identify any gaps in the literature to propose future studies.
Stage 2: Identifying Relevant Studies
Relevant studies were identified by searching four electronic databases (Medline (Ovid Interface), Embase (Ovid Interface), Cumulative Index to Nursing and Allied Health Literature (EBSCO Interface) and Cochrane Library from January 1, 2000, to January 8, 2020. The search strategy was developed in consultation with a librarian at the University of Toronto and adapted for each database. Keywords and medical subject headings, such as medication management, framework, model and self-management, were combined with Boolean and proximity operators (see Supplementary Table 2 for Medline search strategy). The search of electronic databases was conducted on January 8, 2020. In addition to database searches, grey literature was searched on TSpace (University of Toronto research repository) and relevant healthcare and government organization websites (eg World Health Organization, National Institute of Health). Reference lists of included articles were reviewed to ensure the inclusion of all relevant literature.
Stage 3: Study Selection
For inclusion in the scoping review, articles were required to meet the following criteria: (a) described a model or framework originally developed or adapted by authors for medication management; (b) included components of self-management; (c) peer-reviewed literature or grey literature; and (d) published between January 1, 2000, and January 8, 2020. The search was limited to the year 2000 because the majority of research on self-management occurred after this date.12 Articles were excluded if any of the following criteria were met: (a) described models of care (interventions, programs, etc.) that were not guided by a concrete model/framework related to medication self-management; (b) models/frameworks that had not been adapted to include components of medication management or self-management; (c) the model/framework was lacking details on what changes/adaptations were made to the model/framework for medication self-management; (d) models/frameworks that only included self-efficacy for medication-taking behaviour as the self-management component; (e) opinion pieces; and (f) conference abstracts or articles in which the full-text was not accessible.
Study selection was conducted using EndNote X8 for de-duplication (reference manager software) and Covidence for screening (online review management software). Following Bramer’s method, EndNote X8 was used to de-duplicate the exported articles from the database searches.28 The core study team (SJTG, LC, KAJ, TR) used a spreadsheet in Microsoft Excel 2016 to facilitate an interrater screen of a subset of titles and abstracts. All disagreements were discussed until consensus was reached and revisions were made to the eligibility criteria, as needed. Once good agreement (defined as >0.80)29 was achieved, the remainder of the titles and abstracts were imported into Covidence and divided among three reviewers (LC, KAJ, TR) to be screened by a single reviewer. After the completion of title and abstract screen, the core study team (SJTG, LC, TR, SRC) completed an interrater screen of 100 full-text articles (in subsets of 25) to test their agreement. Following each subset of 25 full-text articles, percent agreement was calculated and clarifications were made to the eligibility criteria as needed. After achieving good agreement (>0.80), all full-text articles were double-screened (two separate reviewers screened each article). Disagreements were reviewed by a third screener (senior author) to make the final decision on inclusion.
Stage 4: Charting the Data
A data extraction sheet was created in Microsoft Excel 2016, which was piloted by the extractors (LC, TR, SRC) to ensure consistency in the data extracted from the articles. Questions and disagreements were discussed until clarification or consensus was achieved. A spot check (review of extracted data) was completed (LC, TR) on 15% of the articles to ensure the accuracy of extracted information. The following data were extracted from each article: general information, study characteristics, population characteristics, framework characteristics, intervention characteristics, study outcomes and key findings.
Stage 5: Collating, Summarizing and Reporting the Results
Extracted data were compared across variables. Descriptive numerical analysis and thematic analysis were conducted and are presented below. The data were also critically analyzed to identify current gaps in the literature and develop suggestions for future research, practice and policy.
Results
Search Results
The database searches identified 8683 articles and no additional articles were found from the grey literature searches (see Figure 1). Following the removal of duplicates, 5668 articles remained for title and abstract screening. The full-text of 426 articles were reviewed. Following full-text review, 39 articles met all of the criteria and were included in the scoping review (see Table 1 for study characteristics of included articles).
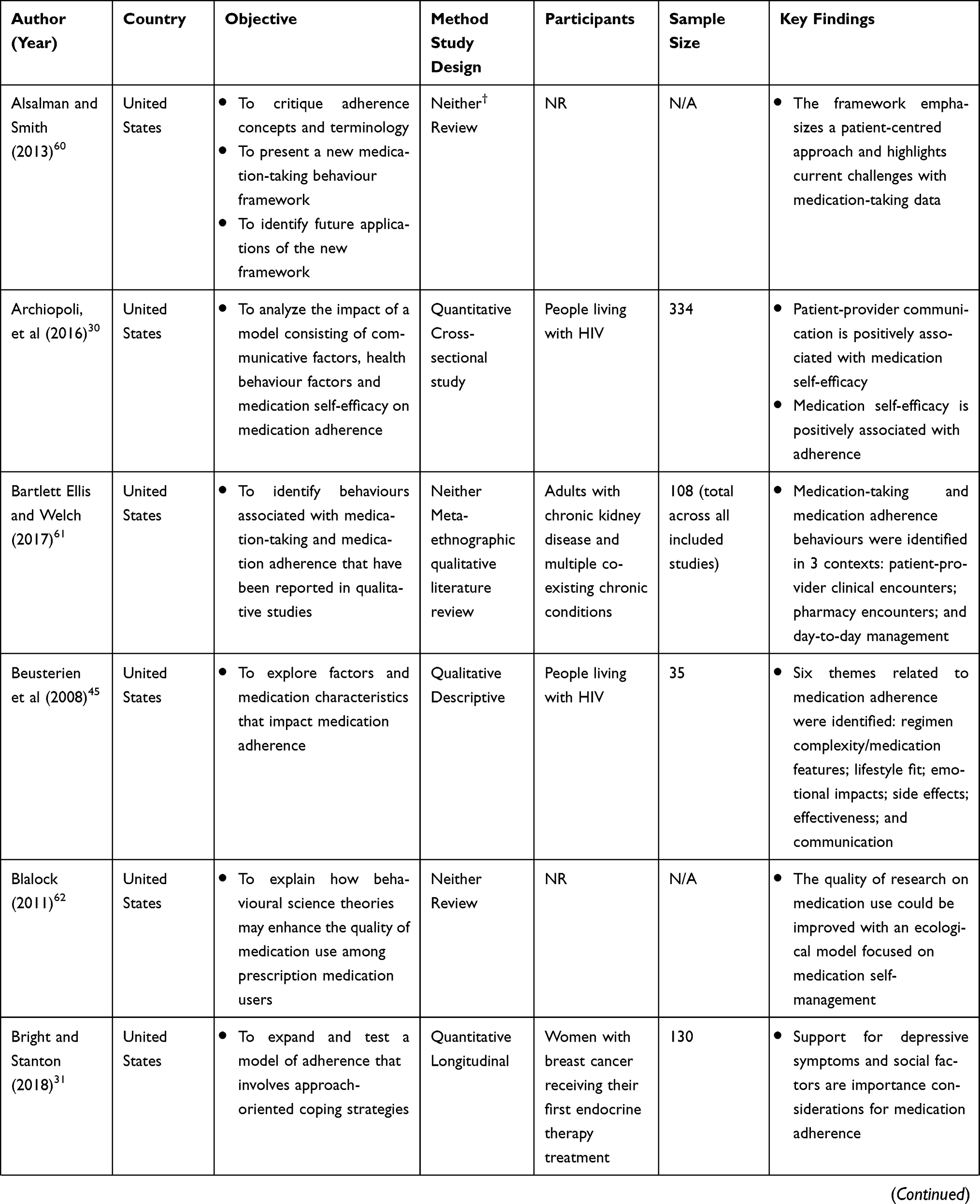 | 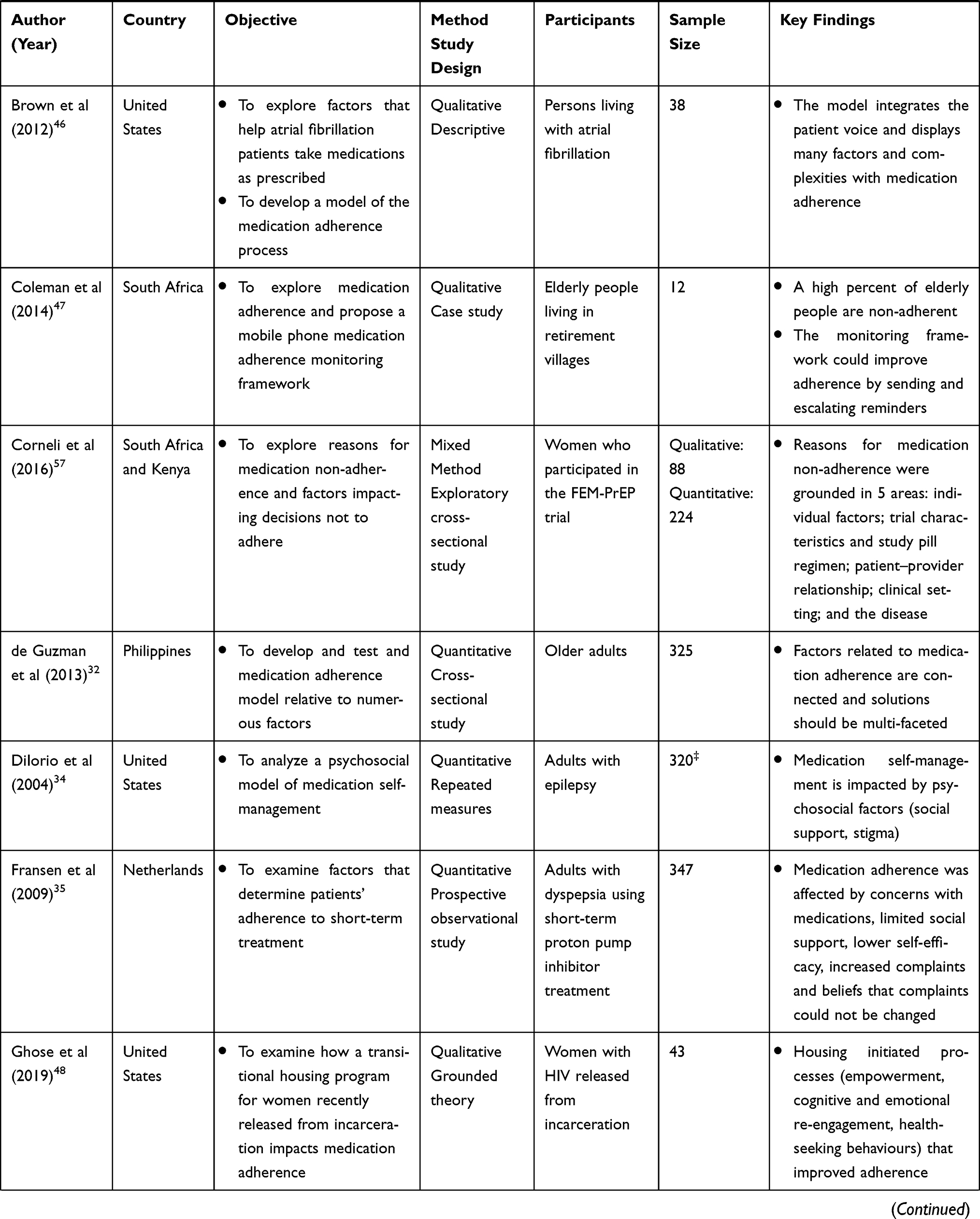 | 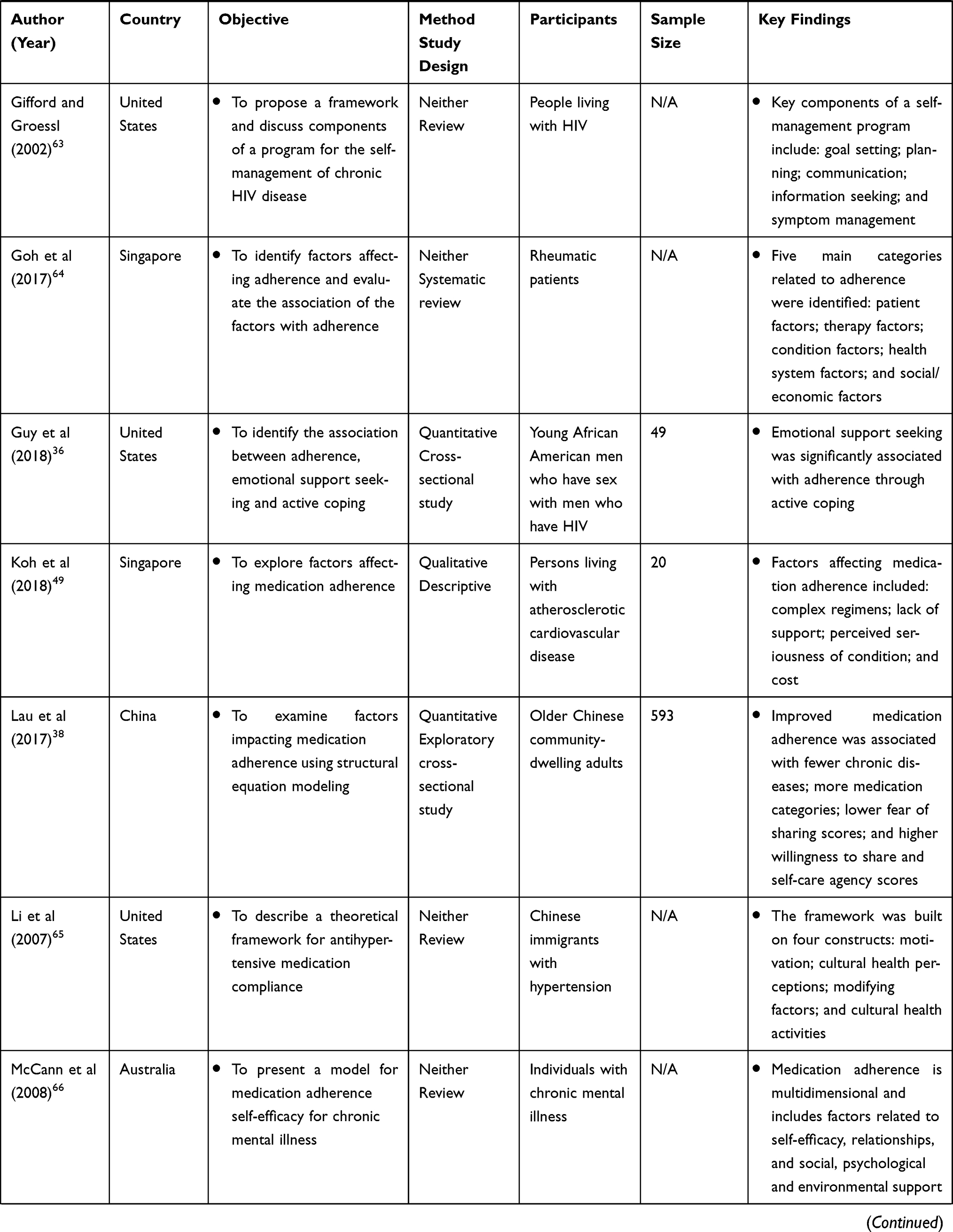 | 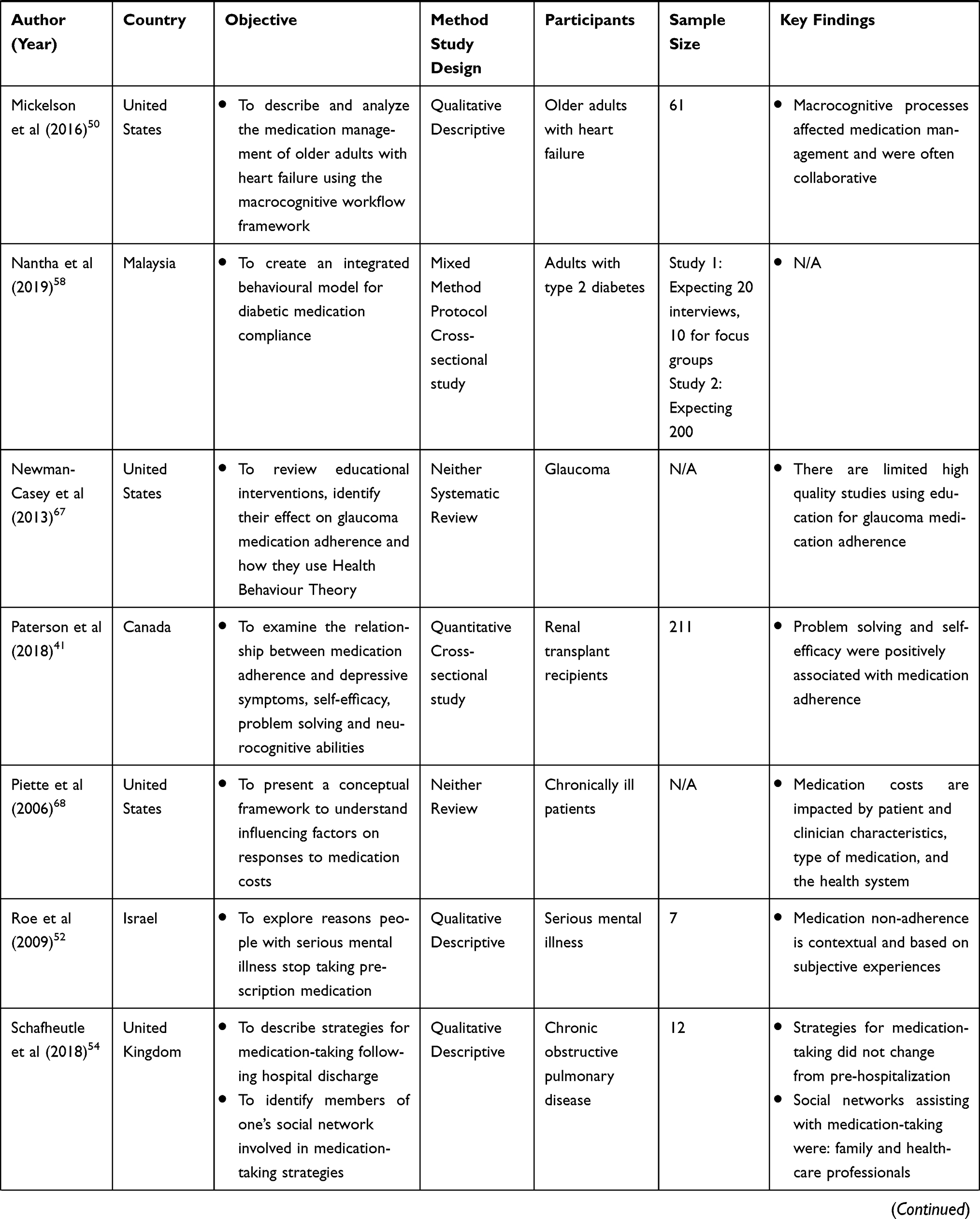 | 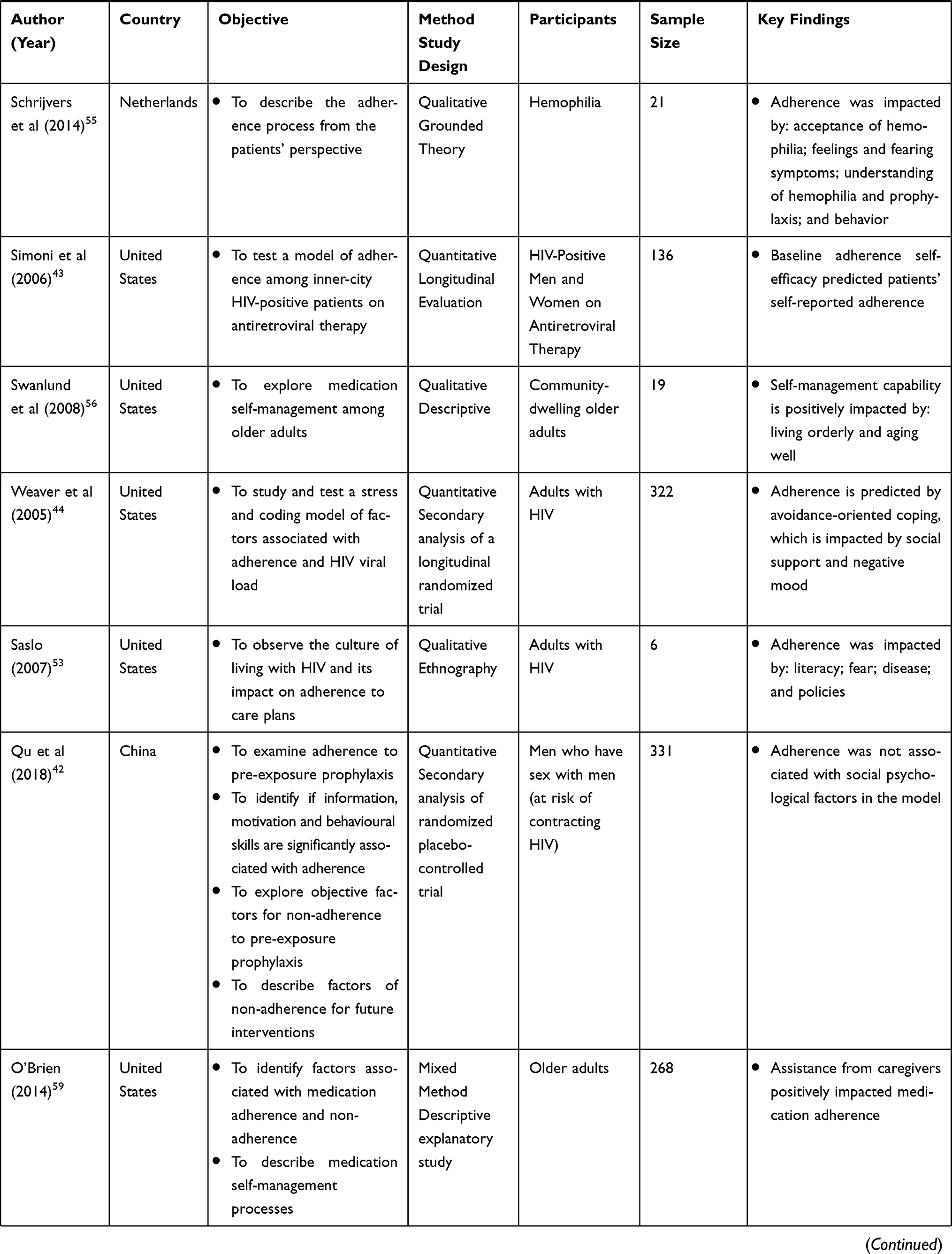 | 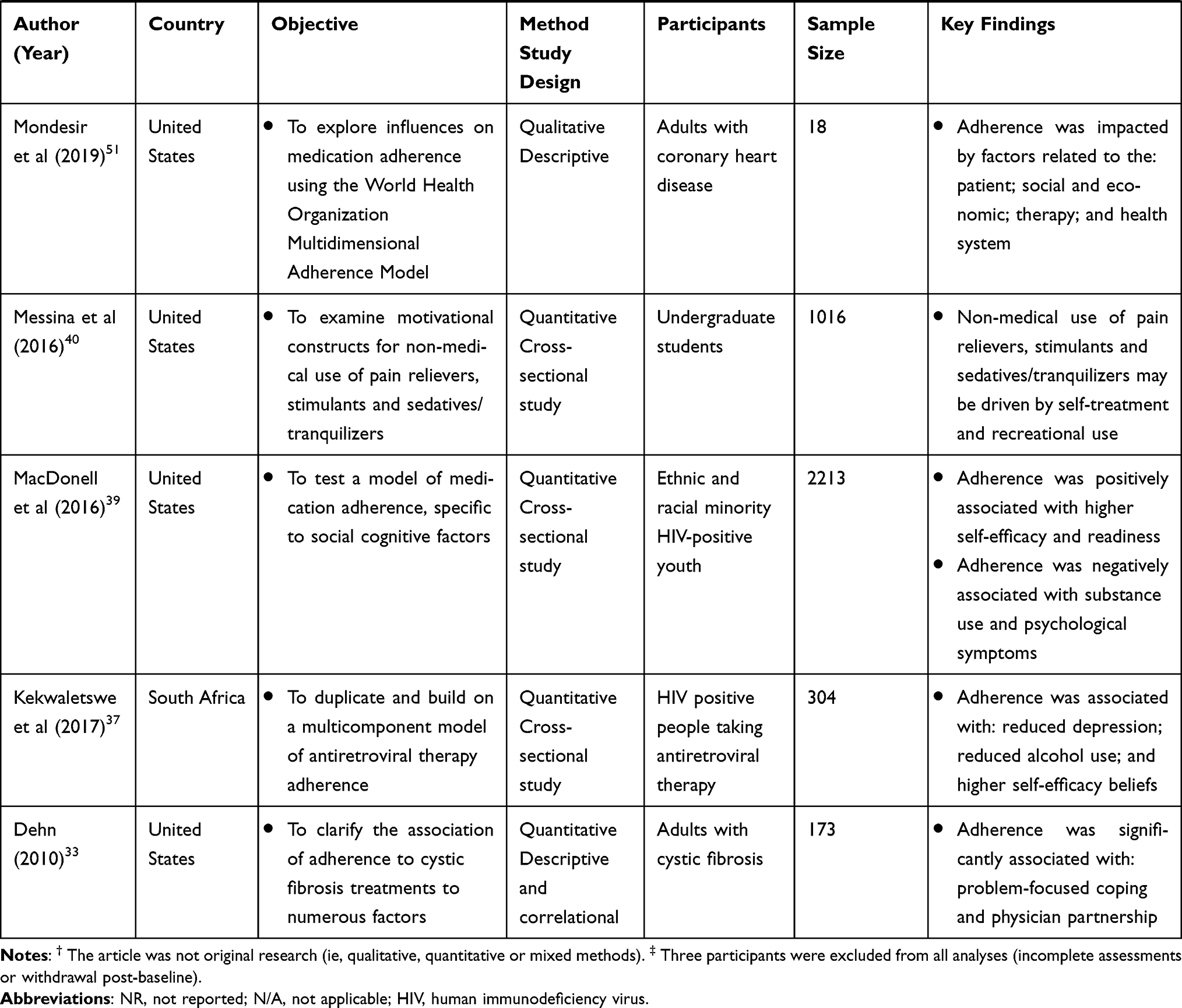 |
Table 1 Characteristics of Included Articles (n=39) |
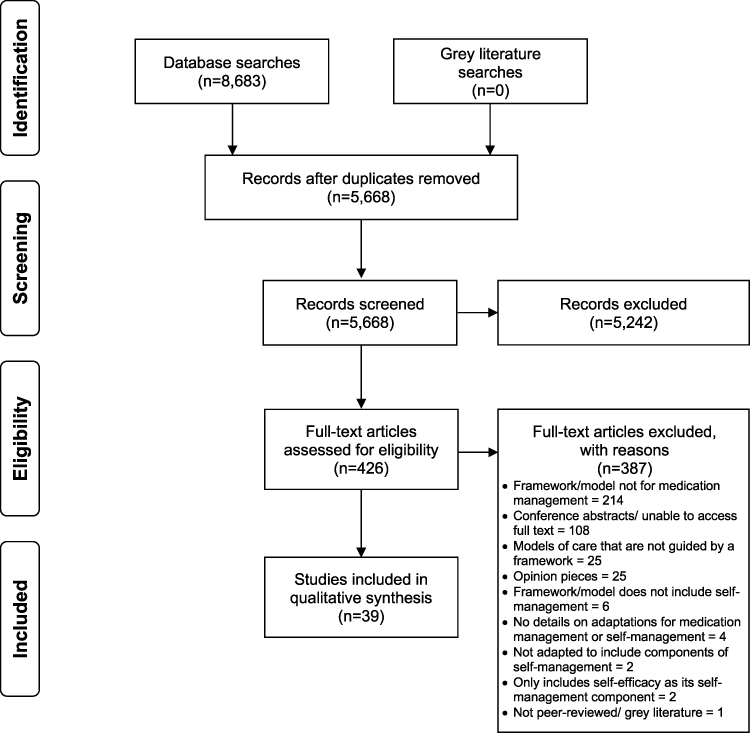 |
Figure 1 PRISMA flow diagram of included articles. |
Study Characteristics
There was a fairly even distribution between quantitative (n=15)30–44 and qualitative (n=12)45–56 study designs, with few mixed method studies (n=3)57–59 and several other article types (eg reviews; n=9).60–68 From 2013 to 2019, there was an increase in the number of articles published yearly (total=24),30–32,36–42,47–51,54,55,57–61,64,67 when compared to the 11 years prior (2002 to 2012; total=15).33–35,43–46,52,53,56,62,63,65,66,68 The studies identified were conducted across 12 different countries: the United States (n=24),30,31,33,34,36,39,40,43–46,48,50,51,53,56,59–63,65,67,68 China (n=2),38,42 the Netherlands (n=2),35,55 Singapore (n=2),49,64 South Africa (n=2),37,47 South Africa and Kenya (n=1),57 Australia (n=1),66 Canada (n=1),41 Israel (n=1),52 Malaysia (n=1),58 Philippines (n=1)32 and the United Kingdom (n=1).54 Of the 39 articles, only one study involved more than one country.57
The majority of frameworks or models were developed, adapted or applied to adults and older adults, but two were for a younger population (adolescents and young adults).36,39 The most common target populations were adults with HIV (n=10)30,36,37,43–45,53,57,63 and cardiovascular disease (n=5).46,49–51,65 Of the included articles that had a study population (n=30), the majority reported the age and sex or gender of participants.30–38,41–46,51,56 There was a fairly even distribution of males and females, with mean ages ranging from 21 to 81 years. Other demographic characteristics reported in about half of the studies were ethnicity/race30,31,33,34,36,39–46,48–51,56,59,67 and education level.30–38,41–46,51,55,56 The most common ethnicities/races studied were Caucasian and African American among individuals who had at least some college education. Demographic characteristics that were not consistently reported included: income level, marital status, household composition, employment status and comorbidities. The overall sample sizes ranged from 6 to 2213 (mean=265; median=136).
Framework Characteristics
Approximately half of the included articles developed and presented a new framework (n=20), while the other half adapted previously existing frameworks, or applied them to their findings (n=19; see Table 2 for framework characteristics). New frameworks and models were developed by research teams through the use of statistical modeling (structural equation models, confirmatory factor models, measurement models, path analysis; n=8), data collected from interviews and focus groups (n=6) and literature syntheses (n=4). One new framework was developed from literature syntheses and focus groups and one framework lacked sufficient details on how it was developed. Adapted frameworks were most commonly based on social cognitive theory, behaviour change models and medication adherence models. Similar to newly developed frameworks, adapted frameworks were often based on quantitative surveys (n=7), literature syntheses (n=4), qualitative data from interviews and focus groups (n=3) or a combination (n=3). No frameworks were developed or adapted through co-design sessions with participants.
 | 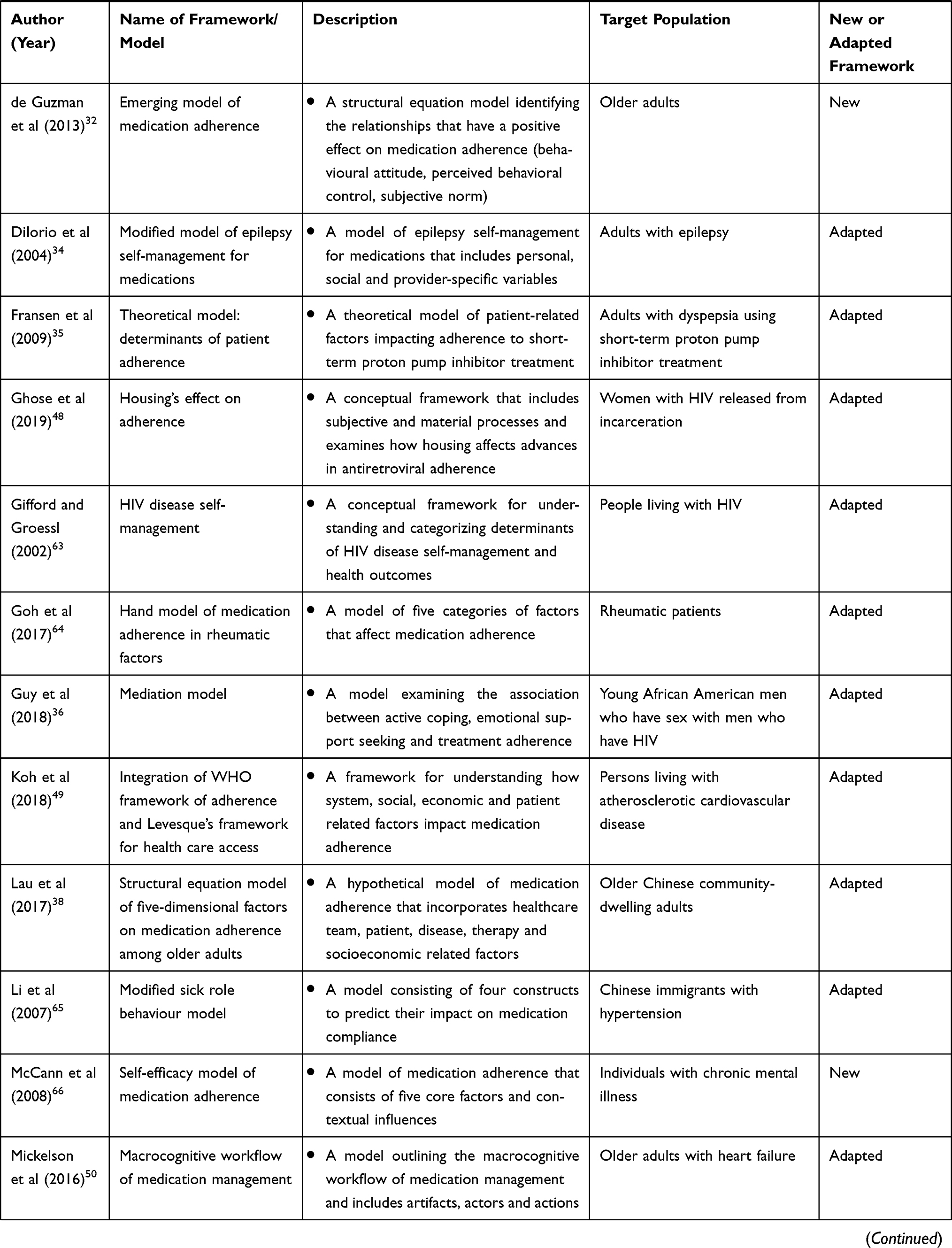 | 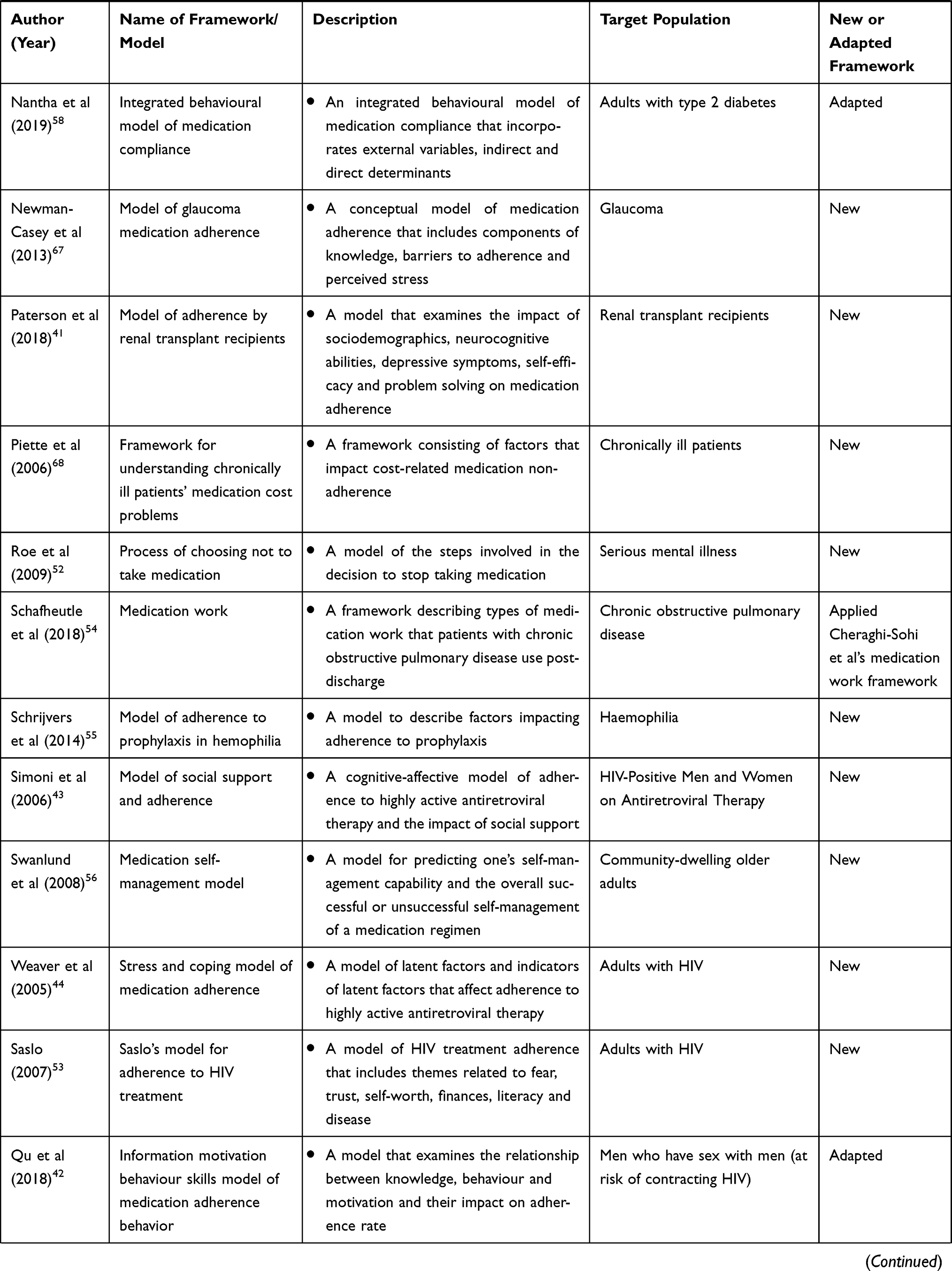 | 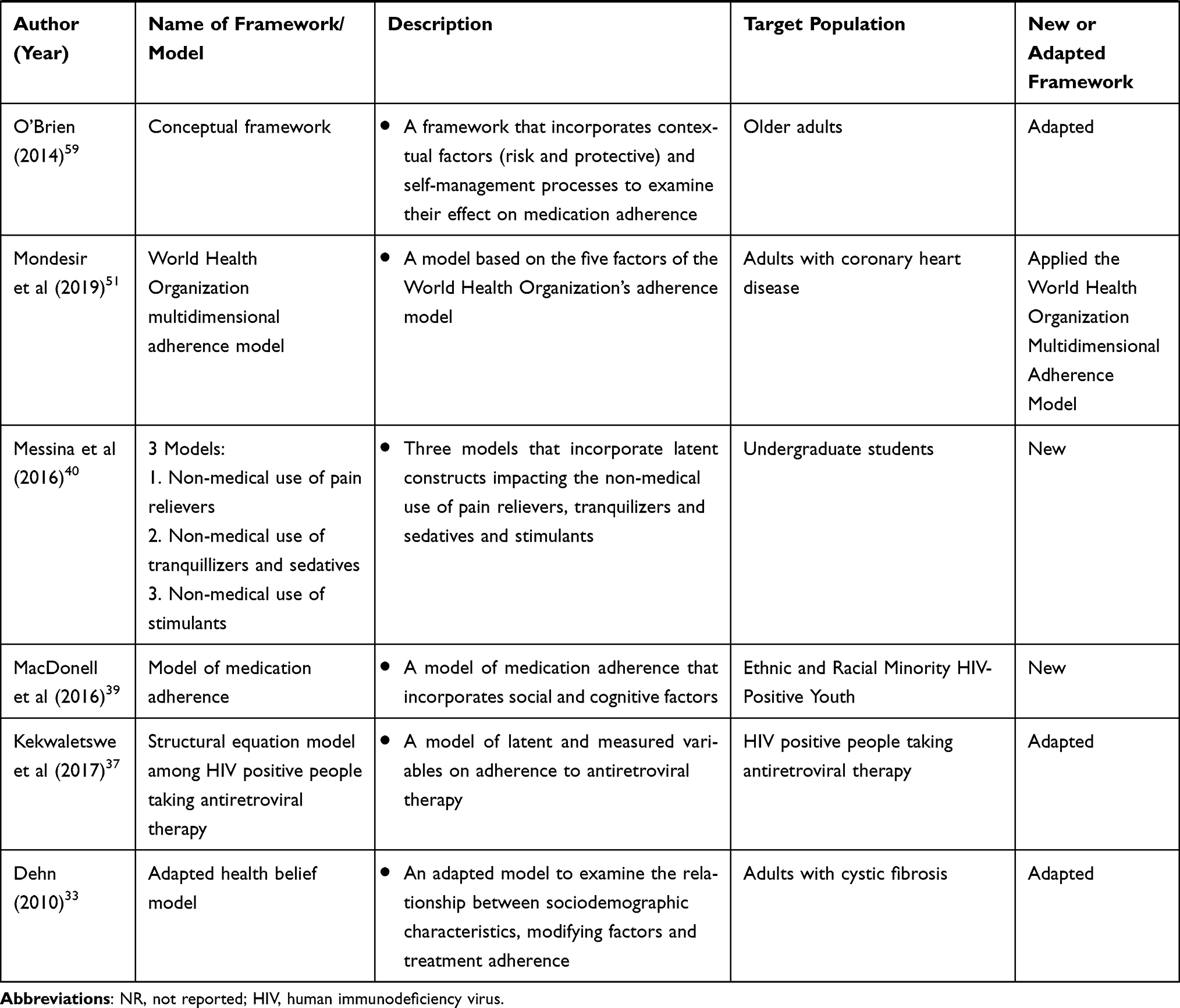 |
Table 2 Framework Characteristics |
The majority of self-management domains (eg adherence; self-efficacy; depression; and seeking advice, support and relationships) included in the frameworks were categorized as medical management (eg medication/treatment adherence, medication/adherence self-efficacy, medication-taking behaviour), followed by emotional management (eg depression, emotional impact) and role management (eg problem solving, day-to-day management, spirituality). Across all frameworks, developed, adapted and applied, the most common domains (not limited to self-management) were related to adherence, self-efficacy, depression, social support and regimen complexity/factors (eg number and size of pills, frequency of refills). There were no major differences between the framework domains from quantitative and qualitative studies.
Discussion
This scoping review analyzed the range and nature of research on medication self-management frameworks. Within the three self-management domains (ie, medical, emotional and role management), the vast majority focused on medical management (eg adherence, medication-taking behaviour, medication self-efficacy, relationships with healthcare providers), with a limited focus on emotional and role management. Further, within medical management, the majority of studies focused specifically on medication adherence and lacked a comprehensive, holistic conceptualization of self-management. Given the prevalence of individuals taking medications and the potential for problematic polypharmacy,7,69 it is important that research and clinical practice conceptualizes medication management beyond adherence to promote person-centred care.
While limited, there were a few frameworks that included a more holistic approach to medication self-management.50,56,62 For example, Blalock used behavioural science theories (eg social cognitive theory, theory of social support, Health Belief Model) to describe how to improve medication use among individuals requiring pharmacotherapy.62 An ecological model was used to present factors impacting medication use at five levels – characteristics of the patient; services from providers; support from family, friends and small groups; characteristics of the community and health care system; and social policy and government regulations. Blalock then proposed a framework specific to medication self-management that built on the ecological model and Fisher’s self-management model70 to incorporate specific intervention goals at each level. The author highlighted the value of using this as a guiding framework for medication self-management, but also identified the need to further develop it as knowledge evolves.
A more holistic framework for medication self-management was also presented by Mickelson et al.50 A qualitative study was conducted among older adults with heart failure to describe the medication management work process (effort and time to produce or accomplish something) and adapt Unertl et al’s Workflow Elements Model.71 The adapted model contained five main process, each containing subprocesses: sensemaking (information gathering, adapting mental models, story building), planning (generating action plans, adapting plans, anticipatory thinking), monitoring (problem detection, tracking), decision making (applying rules, pattern matching, mental stimulation, making trade-offs) and coordinating (reconciling information, managing interdependencies, negotiating). Furthermore, these frameworks highlight the intrinsic complexities of medication management that are critical to consider when developing programs, interventions and initiatives targeting medication self-management.
Importantly, medication-taking has a substantial impact on an individual’s life.72 For example, a systematic review was conducted by Mohammed et al to explore medication burden among patients with experience taking medications.72 This review identified patients’ experiences with medication-related burden (ie, burden caused by medication routines, medication characteristics, adverse events, healthcare system, social life), medication-related beliefs (individual attitudes, coping skills, outside influences) and medication-taking practices (following instructions, accepting medication use, modifying care plans). Further, Mohammed et al’s review highlighted the impact of medications and medication burden on the day-to-day lives of individuals taking medications, as it interfered with their daily activities and influenced their beliefs, attitudes and overall quality of life. The impact of medication management on an individual’s life extends beyond medical management to include emotional and role management. Therefore, it is critical for medication self-management frameworks to be all-encompassing of the self-management domains.
Frameworks that took into account the participants’ sociodemographic and clinical characteristics are lacking based on our scoping review. Medication self-management may be impacted by micro, meso and macro level factors. Micro, or individual, level factors can impact medication use and the potential for polypharmacy, as age, gender, cognitive and physical ability and multimorbidity have been noted in the literature to affect medication-taking behaviour.73–78 For example, a systematic review was conducted by Smaje et al (2018) to identify factors associated with medication adherence in older patients and found that older age, multimorbidity, cognitive impairment and being male were negatively associated with adherence.74 Additionally, characteristics of a medication regimen, including complexity, dose, frequency and side effects can also impact medication adherence.79–83 Increased regimen complexity results in reduced medication adherence, as identified in a systematic review by Pantuzza et al (2017) that examined evidence on the association between medication regimen complexity and adherence.79 Similarly, a qualitative study conducted by O’Donovan et al (2019) in the United Kingdom explored the impact and management of medication side effects among individuals 18 or older who had experienced side effects.84 It was identified that participants used non-adherent behaviours as a method of coping with side effects. Further, many of these individual level factors have also been identified as having an impact on general self-management,85–87 which adds a layer of complexity to medication self-management.
Macro or system level factors can also have an impact on medication self-management. This review identified that, to date, the majority of frameworks for medication self-management were from the United States (n=24), with an overall lack of global representation. Medication self-management may look different in different regions or countries based on healthcare system and funding structures, insurance coverage and support from and access to healthcare providers.88,89 In an analysis of health data from 1980 to 2016, Sarnak et al compared drug spending and trends in the United States, Australia, Canada, France, Germany, the Netherlands, Norway, Sweden, Switzerland and the United Kingdom.88 The United States had considerably higher prescription drug spending and drug prices than the other high-income countries. Americans were also more likely to experience high out-of-pocket costs for medications. High out-of-pocket medication costs can impact medication self-management, as an inability to afford medications may lead to cost-related nonadherence.90 It is important to acknowledge contextual factors in the development and application of medication self-management frameworks. In addition, more work is needed to explore what sociodemographic and clinical characteristics, as well as what system level factors impact medication self-management in order to understand if, and how, frameworks can be applied to different populations in different contexts.
Future Work
This scoping review highlighted several gaps in the literature and areas for future work. First, it is important for future research to develop a framework for medication self-management that directly incorporates patients’ and providers’ voices (ie, through co-design) and can be applied to a broader population of individuals taking medications. Integrating the thoughts, experiences, beliefs and concerns of persons with lived experience and providers is important, as patients are the ones self-managing and impacted by these processes on a day-to-day basis and providers are supporting patients with their health conditions and medications. More specifically, co-design would allow for the collaborative development of a framework that meets the needs of patients and providers. Second, a framework that encompasses all components of medication and self-management should be developed and validated. Current frameworks mostly focus on adherence, rather than incorporating the impact of experiences, beliefs and preferences on self-management behaviour. Frameworks guide research and consequently clinical practice recommendations.91,92 Advancing the collective knowledge on medication self-management can help patients and providers navigate self-management and related self-management support.
Limitations
There are a few limitations of this scoping review that should be noted. First, it is possible that relevant articles were missed based on the databases and grey literature searched. Second, our search was conducted in English, so it is possible that articles published in other languages were not identified. Third, some may note that a critical appraisal of included articles was not undertaken. However, critical appraisal is a less common and optional component for scoping reviews.27
Conclusion
Medication self-management is complex and has the potential to impact multiple aspects of an individual’s life, including mental and physical well-being, as well as day-to-day activities. The majority of frameworks included in this review focus on medical management, with few incorporating components of emotional and role management. It is important to acknowledge the impact medication self-management can have on all aspects of one’s life and focus future work on developing and validating holistic frameworks for medication self-management that can be applied to a broad population.
Data Sharing Statement
All data analyzed in this scoping review are included in this published article and its supplementary files.
Ethics Approval and Informed Consent
Not applicable.
Acknowledgments
The authors would like to thank the University of Toronto librarian, Glyneva Bradley-Ridout, for her expertise and assistance in developing the search strategy.
Funding
Dr Guilcher is supported by a Canadian Institutes of Health Research Embedded Clinician Scientist Salary Award on Transitions in Care. Kadesha James is supported by the Dean’s Graduate Scholarship (2019-2021) at the Leslie Dan Faculty of Pharmacy, University of Toronto.
Disclosure
The authors report no potential competing interests with respect to the research, authorship and/or publication of this article.
References
1. Chao Y-S, Wu C-J, Wu H-C, Chen W-C, Marengoni A. Drug trends among non-institutionalized Canadians and the impact of data collection changes in the Canadian Health Measures Survey 2007 to 2015. PLoS One. 2019;14(4):4. doi:10.1371/journal.pone.0214718
2. Feely A, Lix LM, Reimer K. Estimating multimorbidity prevalence with the Canadian Chronic Disease Surveillance System. Res Policy Pract. 2017;37:7.
3. Holloway K, van Dijk L. The World Medicines Situation 2011: Rational Use of Medicine. Geneva: World Health Organization; 2011.
4. Kantor ED, Rehm CD, Haas JS, Chan AT, Giovannucci EL. Trends in prescription drug use among adults in the United States from 1999-2012. JAMA. 2015;314(17):1818–1831.
5. Zhang F, Mamtani R, Scott FI, Goldberg DS, Haynes K, Lewis JD. Increasing use of prescription drugs in the United Kingdom. Pharmacoepidemiol Drug Saf. 2016;25(6):628–636.
6. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17:1.
7. Duerden M, Avery T, Payne R. Polypharmacy and Medicines Optimisation: Making It Safe and Sound. London, United Kingdom: The King’s Fund;2013.
8. Lown Institute. Medication Overload: America’s Other Drug Problem. How the Drive to Prescribe is Harming Older Adults. Massachusetts, USA: Lown Institute; 2019.
9. Canadian Pharmacists Association. Medication Management. 2017. Available from: https://www.pharmacists.ca/education-practice-resources/professional-development/medication-management/.
10. Burns A, American Pharmacists Association. Medication therapy management in pharmacy practice: core elements of an MTM service model (version 2.0). J Am Pharm Assoc. 2008;48(3):341–353. doi:10.1331/JAPhA.2008.08514
11. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. doi:10.1016/S0738-3991(02)00032-0
12. Lorig KR, Holman HR. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7.
13. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. 2008;31(Supplement 1):S97.
14. Captieux M, Pearce G, Parke HL, et al. Supported self-management for people with type 2 diabetes: a meta-review of quantitative systematic reviews. BMJ Open. 2018;8(12):e024262.
15. Glazier RH, Bajcar J, Kennie NR, Willson K, Systematic A. Review of interventions to improve diabetes care in socially disadvantaged populations. Diabetes Care. 2006;29(7):1675.
16. Greenwood DA, Gee PM, Fatkin KJ, Peeples M, Systematic A. Review of reviews evaluating technology-enabled diabetes self-management education and support. J Diabetes Sci Technol. 2017;11(5):1015–1027.
17. Mohamed A, Staite E, Ismail K, Winkley K. A systematic review of diabetes self-management education interventions for people with type 2 diabetes mellitus in the Asian Western Pacific (AWP) region. Nurs Open. 2019;6(4):1424–1437.
18. Audulv Å, Ghahari S, Kephart G, Warner G, Packer TL. The Taxonomy of Everyday Self-management Strategies (TEDSS): a framework derived from the literature and refined using empirical data. Patient Educ Couns. 2019;102(2):367–375.
19. McGreal MH, Hogan MJ, Walsh-Irwin C, Maggio NJ, Jurgens CY. Heart failure self-care interventions to reduce clinical events and symptom burden. Res Rep Clin Cardiol. 2014;5:243–257.
20. Jonkman Nini H, Westland H, Groenwold Rolf HH, et al. Do self-management interventions work in patients with heart failure? Circulation. 2016;133(12):1189–1198.
21. Pinnock H, Parke HL, Panagioti M, et al. Systematic meta-review of supported self-management for asthma: a healthcare perspective. BMC Med. 2017;15(1):64.
22. Hodkinson A, Bower P, Grigoroglou C, et al. Self-management interventions to reduce healthcare use and improve quality of life among patients with asthma: systematic review and network meta-analysis. BMJ. 2020;370:m2521.
23. van Grieken RA, van Tricht MJ, Koeter MWJ, van den Brink W, Schene AH. The use and helpfulness of self-management strategies for depression: the experiences of patients. PLoS One. 2018;13(10):e0206262–e0206262.
24. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
25. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69.
26. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. 2020;18(10):2119–2126.
27. Tricco AC, Lillie E, Zarin W, et al. Prisma extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473.
28. Bramer WM, Giustini D, de Jonge GB, Holland L, Bekhuis T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. 2016;104(3):240–243.
29. McHugh ML. Interrater reliability: the kappa statistic. Biochemia Medica. 2012;22(3):276–282.
30. Archiopoli A, Ginossar T, Wilcox B, Avila M, Hill R, Oetzel J. Factors of interpersonal communication and behavioral health on medication self-efficacy and medication adherence. AIDS Care. 2016;28(12):1607–1614.
31. Bright EE, Stanton AL. Prospective investigation of social support, coping, and depressive symptoms: a model of adherence to endocrine therapy among women with breast cancer. J Consult Clin Psychol. 2018;86(3):242–253.
32. de Guzman AB, Guevara KIJ, Guiang FJB, et al. Developing a model of medication adherence among Filipino elderly. Educ Gerontol. 2013;39(5):298–313.
33. Dehn CP Coping styles and physician partnership in adults with cystic fibrosis: relation to treatment adherence. 2010;Ph.D.:162 p-162.
34. DiIorio C, Shafer PO, Letz R, et al. Project EASE: a study to test a psychosocial model of epilepsy medication management. Epilepsy Behav. 2004;5(6):926–936.
35. Fransen GAJ, Mesters I, Janssen MJR, Knottnerus JA, Muris JWM. Which patient-related factors determine self-perceived patient adherence to prescribed dyspepsia medication? Health Educ Res. 2009;24(5):788–798.
36. Guy AA, Niel K, Du Bois SN. Emotional support, active coping, and ART adherence in young African American men who have sex with men: a pilot mediation model. J Assoc Nurs AIDS Care. 2018;29(4):612–618.
37. Kekwaletswe CT, Jordaan E, Nkosi S, Morojele NK. Social support and the mediating roles of alcohol use and adherence self-efficacy on Antiretroviral Therapy (ART) adherence among ART recipients in Gauteng, South Africa. AIDS Behav. 2017;21(7):1846–1856.
38. Lau Y, Htun TP, Chan KS, Klainin-Yobas P. Multidimensional factors affecting medication adherence among community-dwelling older adults: a structural-equation-modeling approach. J Public Health (Germany). 2017;25(1):113–122.
39. MacDonell KK, Jacques-Tiura AJ, Naar S, Fernandez MI. Predictors of self-reported adherence to antiretroviral medication in a multisite study of ethnic and racial minority HIV-positive youth. J Pediatr Psychol. 2016;41(4):419–428.
40. Messina BG, Dutta NM, Silvestri MM, et al. Modeling motivations for non-medical use of prescription drugs. Addict Behav. 2016;52:46–51.
41. Paterson TSE, O’Rourke N, Jean Shapiro R, Thornton WL. Medication adherence in renal transplant recipients: a latent variable model of psychosocial and neurocognitive predictors. PLoS One. 2018;13(9):e0204219.
42. Qu D, Zhong X, Xiao G, Dai J, Liang H, Huang A. Adherence to pre-exposure prophylaxis among men who have sex with men: a prospective cohort study. Int J Infect Dis. 2018;75:52–59.
43. Simoni JM, Frick PA, Huang B. A longitudinal evaluation of a social support model of medication adherence among HIV-positive men and women on antiretroviral therapy. Health Psychol. 2006;25(1):74–81.
44. Weaver KE, Llabre MM, Duran RE, et al. A stress and coping model of medication adherence and viral load in HIV-positive men and women on highly active antiretroviral therapy (HAART). Health Psychol. 2005;24(4):385–392.
45. Beusterien KM, Davis EA, Flood R, Howard K, Jordan J. HIV patient insight on adhering to medication: a qualitative analysis. AIDS Care. 2008;20(2):244–252.
46. Brown TM, Siu K, Walker D, Pladevall-Vila M, Sander S, Mordin M. Development of a conceptual model of adherence to oral anticoagulants to reduce risk of stroke in patients with atrial fibrillation. J Manag Care Pharm. 2012;18(5):351–362.
47. Coleman A. Medication adherence of elderly citizens in retirement homes through a mobile phone adherence monitoring framework (Mpamf) for developing countries: a case study in South Africa. Indian J Pharm Educ Res. 2014;48(3):6–11.
48. Ghose T, Ali S, Shubert V, Stanton M, Walker L, Chaudhuri S. “It’s my Room and my Life”: housing’s Influence on Medication Adherence for HIV-positive Women Released from Incarceration. J Health Care Poor Underserved. 2019;30(1):182–201.
49. Koh JJK, Cheng RX, Yap Y, et al. Access and adherence to medications for the primary and secondary prevention of atherosclerotic cardiovascular disease in Singapore: a qualitative study. Patient Prefer Adherence. 2018;12:2481–2498.
50. Mickelson RS, Unertl KM, Holden RJ. Medication management: the macrocognitive workflow of older adults with heart failure. JMIR Human Factors. 2016;3(2):e27.
51. Mondesir FL, Levitan EB, Malla G, et al. Patient perspectives on factors influencing medication adherence among people with Coronary Heart Disease (CHD) and CHD risk factors. Patient Prefer Adherence. 2019;13:2017–2027.
52. Roe D, Goldblatt H, Baloush-Klienman V, Swarbrick M, Davidson L. Why and how people decide to stop taking prescribed psychiatric medication: exploring the subjective process of choice. Psychiatr Rehabil J. 2009;33(1):38–46.
53. Saslo MC Ethnography of adherence to plans of care in the HIV positive patient. 2007;D.N.S.:112 p-112 p.
54. Schafheutle EI, Fegan T, Ashcroft DM. Exploring medicines management by COPD patients and their social networks after hospital discharge. Int J Clin Pharm. 2018;40(5):1019–1029.
55. Schrijvers L, Kars M, Beijlevelt-van Der Zande M, Peters M, Schuurmans M, Fischer K. Perspectives of patients with hemophilia on adherence to prophylaxis: a grounded theory approach. Haemophilia. 2014;20(SUPPL. 3):118.
56. Swanlund SL, Scherck KA, Metcalfe SA, Jesek-Hale SR. Keys to successful self-management of medications. Nurs Sci Q. 2008;21(3):238–246.
57. Corneli A, Perry B, McKenna K, et al. Participants’ explanations for nonadherence in the FEM-PrEP clinical trial. J Acquir Immune Defic Syndr. 2016;71(4):452–461.
58. Nantha YS, Haque S, Nantha HS, Swarna nantha Y, Swarna Nantha H. The development of an integrated behavioural model of patient compliance with diabetes medication: a mixed-method study protocol. Fam Pract. 2019;36(5):581–586.
59. O’Brien A-M Factors associated with medication adherence in frail urban older adults: a descriptive and explanatory study. 2014;Ph.D.:180 p-180 p.
60. Alsalman AJ, Smith WR. Expanding the framework of assessing adherence and medication-taking behavior. J Pain Palliat Care Pharmacother. 2013;27(2):114–124.
61. Bartlett Ellis RJ, Welch JL. Medication-taking behaviours in chronic kidney disease with multiple chronic conditions: a meta-ethnographic synthesis of qualitative studies. J Clin Nurs. 2017;26(5–6):586–598.
62. Blalock SJ. The theoretical basis for practice-relevant medication use research: patient-centered/behavioral theories. Res Social Admin Pharm. 2011;7(4):317–329.
63. Gifford AL, Groessl EJ. Chronic disease self-management and adherence to HIV medications. J Acquir Immune Defic Syndr. 2002;31(SUPPL. 3):S163–S166.
64. Goh H, Kwan YH, Seah Y, Low LL, Fong W, Thumboo J. A systematic review of the barriers affecting medication adherence in patients with rheumatic diseases. Rheumatol Int. 2017;37(10):1619–1628.
65. Li WW, Stotts NA, Froelicher ES. Compliance with antihypertensive medication in Chinese immigrants: cultural specific issues and theoretical application. Res Theory Nurs Pract. 2007;21(4):236–254.
66. McCann TV, Clark E, Lu S. The self-efficacy model of medication adherence in chronic mental illness. J Clin Nurs. 2008;17(11):329–340.
67. Newman-Casey PA, Weizer JS, Heisler M, Lee PP, Stein JD. Systematic review of educational interventions to improve glaucoma medication adherence. Semin Ophthalmol. 2013;28(3):191–201.
68. Piette JD, Heisler M, Horne R, Caleb Alexander G. A conceptually based approach to understanding chronically ill patients’ responses to medication cost pressures. Soc Sci Med. 2006;62(4):846–857.
69. Gallagher P, Lang PO, Cherubini A, et al. Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol. 2011;67(11):1175–1188.
70. Fisher EB, Brownson CA, O’Toole ML, Shetty G, Anwuri VV, Glasgow RE. Ecological approaches to self-management: the case of diabetes. Am J Public Health. 2005;95(9):1523–1535.
71. Unertl KM, Novak LL, Johnson KB, Lorenzi NM. Traversing the many paths of workflow research: developing a conceptual framework of workflow terminology through a systematic literature review. J Am Med Inform Assoc. 2010;17(3):265–273.
72. Mohammed MA, Moles RJ, Chen TF. Medication-related burden and patients’ lived experience with medicine: a systematic review and metasynthesis of qualitative studies. BMJ Open. 2016;6(2):e010035.
73. Shruthi R, Jyothi R, Pundarikaksha HP, Nagesh GN, Tushar TJA. Study of medication compliance in geriatric patients with chronic illnesses at a tertiary care hospital. J Clin Diagn Res. 2016;10(12):FC40–FC43.
74. Smaje A, Weston-Clark M, Raj R, Orlu M, Davis D, Rawle M. Factors associated with medication adherence in older patients: a systematic review. AGING MEDICINE. 2018;1(3):254–266.
75. Turner A, Hochschild A, Burnett J, Zulfiqar A, Dyer CB. High prevalence of medication non-adherence in a sample of community-dwelling older adults with adult protective services-validated self-neglect. Drugs Aging. 2012;29(9):741–749.
76. Cárdenas-Valladolid J, Martín-Madrazo C, Salinero-Fort MA, et al. Prevalence of adherence to treatment in homebound elderly people in primary health care. Drugs Aging. 2010;27(8):641–651.
77. Altıparmak S, Altıparmak O. Drug-using behaviors of the elderly living in nursing homes and community-dwellings in Manisa, Turkey. Arch Gerontol Geriatr. 2012;54(2):e242–e248.
78. Manteuffel M, Williams S, Chen W, Verbrugge RR, Pittman DG, Steinkellner A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J Women’s Health. 2014;23(2):112–119.
79. Pantuzza LL, Ceccato M, Silveira MR, Junqueira LMR, Reis AMM. Association between medication regimen complexity and pharmacotherapy adherence: a systematic review. Eur J Clin Pharmacol. 2017;73(11):1475–1489.
80. Ayele AA, Tegegn HG, Ayele TA, Ayalew MB. Medication regimen complexity and its impact on medication adherence and glycemic control among patients with type 2 diabetes mellitus in an Ethiopian general hospital. BMJ Open Diabetes Res Care. 2019;7(1):e000685.
81. Coleman CI, Limone B, Sobieraj DM, et al. Dosing frequency and medication adherence in chronic disease. J Manag Care Pharm. 2012;18(7):527–539.
82. Dibonaventura M, Gabriel S, Dupclay L, Gupta S, Kim E. A patient perspective of the impact of medication side effects on adherence: results of a cross-sectional nationwide survey of patients with schizophrenia. BMC Psychiatry. 2012;12:20.
83. Milan R, Vasiliadis H-M. The association between side effects and adherence to antidepressants among primary care community-dwelling older adults. Aging Ment Health. 2020;24(8):1229–1236.
84. O’Donovan B, Rodgers RM, Cox AR, Krska J. ‘You feel like you haven’t got any control’: a qualitative study of side effects from medicines. J Patient Saf Risk Manage. 2019;24(1):13–24.
85. Cramm JM, Twisk J, Nieboer AP. Self-management abilities and frailty are important for healthy aging among community-dwelling older people; a cross-sectional study. BMC Geriatr. 2014;14(1):28.
86. Mathew R, Gucciardi E, De Melo M, Barata P. Self-management experiences among men and women with type 2 diabetes mellitus: a qualitative analysis. BMC Fam Pract. 2012;13(1):122.
87. Shao J-H, Chen S-H. Who did it better? Gender differences in effects of a dietary self-management intervention for older community-dwelling adults. J Women Aging. 2019;1–14.
88. Sarnak DO, Squires D, Kuzmak G, Bishop S. Paying for Prescription Drugs Around the World: why Is the U.S. an Outlier? Issue Brief. 2017;2017:1–14.
89. Canada’s Premiers. The pan-Canadian Pharmaceutical Alliance. 2020; https://www.canadaspremiers.ca/pan-canadian-pharmaceutical-alliance-archives/.
90. Gupta S, McColl MA, Guilcher SJ, Smith K. Cost-related nonadherence to prescription medications in Canada: a scoping review. Patient Prefer Adherence. 2018;12:1699–1715.
91. American Academy of Family Physicians. Clinical Practice Guideline Manual. 2017. Available from: https://www.aafp.org/family-physician/patient-care/clinical-recommendations/cpg-manual.html#:~:text=Definition%3A%20Clinical%20practice%20guidelines%20are,harms%20of%20alternative%20care%20options.
92. Rycroft-Malone J, Bucknall T. Using theory and frameworks to facilitate the implementation of evidence into practice. Worldviews Evid Based Nurs. 2010;7(2):57–58.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.