Back to Journals » Patient Preference and Adherence » Volume 14
Medication Evaluation in Portuguese Elderly Patients According to Beers, STOPP/START Criteria and EU(7)-PIM List – An Exploratory Study
Authors Monteiro C ![]() , Canário C, Ribeiro MÂ, Duarte AP, Alves G
, Canário C, Ribeiro MÂ, Duarte AP, Alves G ![]()
Received 23 January 2020
Accepted for publication 21 March 2020
Published 5 May 2020 Volume 2020:14 Pages 795—802
DOI https://doi.org/10.2147/PPA.S247013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Cristina Monteiro,1 Catarina Canário,2,3 Manuel Ângelo Ribeiro,3 Ana Paula Duarte,1,2 Gilberto Alves1,2
1UFBI – Pharmacovigilance Unit of Beira Interior, Faculty of Health Sciences, University of Beira Interior, Covilhã, Portugal; 2CICS-UBI – Health Sciences Research Centre, University of Beira Interior, Covilhã, Portugal; 3Associação de Socorros Mútuos-Mutualista Covilhanense, Covilhã, Portugal
Correspondence: Cristina Monteiro
UFBI – Pharmacovigilance Unit of Beira Interior, Faculty of Health Sciences, University of Beira Interior, Covilhã 6200-506, Portugal
Tel +35 1275329070
Email [email protected]
Purpose: The increase in drug prescription for the elderly raises the risk of the occurrence of potentially inappropriate medications (PIMs), thus increasing the incidence of drug-related problems. Likewise, potential prescribing omissions (PPOs) are also highly prevalent in the elderly. This study aimed at assessing the prevalence of PIMs in the elderly by using the EU(7)-PIM list, STOPP criteria version 2 and the Beers criteria version 2015, as well as the prevalence of PPOs by applying the START criteria version 2 in elderly nursing home residents and outpatients of the Eastern Central Region of Portugal.
Patients and Methods: A descriptive cross-sectional study was carried out in a sample of 90 Portuguese elderly people. Age, gender, diagnoses and medication history were collected from the patients’ clinical records. The prevalence of PIMs and PPOs was measured according to each of the criteria applied.
Results: The patients’ ages ranged from 65 to 103 years, with an average age of 84.15 years. In addition, the average number of medications prescribed was 7.6. The STOPP criteria identified 250 PIMs affecting 77 patients (85.5%), the EU(7)-PIM list detected 94 PIMs in 58 patients (64.4%) and the Beers criteria identified 69 PIMs in 51 patients (56.6%). Therefore, the STOPP criteria version 2 identified substantially more PIMs than the other two tools. Furthermore, by applying the START criteria 68 PPOs were detected in 52 patients (57.7%).
Conclusion: A high prevalence of PIMs and PPOs was observed, suggesting the need to implement actions aimed at reducing the phenomenon and thus help to improve the quality of care provided in nursing homes. The variations in prevalence with the different tools suggest the need to carefully choose the tool for medication review in the elderly.
Keywords: potentially inappropriate medications, potential prescribing omissions, EU(7)-PIM list, STOPP/START criteria version 2, Beers criteria version 2015, elderly
Introduction
Increasing drug prescription raises the risk of the occurrence of potentially inappropriate medications (PIMs) prescribing.1 In this context, several studies have suggested a high prevalence of medication prescription in the elderly, increasing the presence of drug-related problems (increased frequency of adverse events, augmented iatrogenic morbidity and mortality, and increased hospitalization rate).2–5 These problems are usually associated with inadequate dosing regimens in the elderly, with drug interactions, and even with medication duplication.2–5 Furthermore, there are increasing problems of adherence to therapy6 and an increase in health expenditures associated with polypharmacy.7–11 Inappropriate prescription is therefore considered a major health concern.3,12 In addition to the number of medications prescribed, female gender and dependency for daily life activities have also been associated with a higher prevalence of PIMs.13
Polypharmacy, defined as the use of five or more drugs,14 does not necessarily imply the presence of inappropriate prescriptions, but it has been consistently associated with a higher risk of PIMs. It was evidenced that reducing the number of drugs used, through medication review programs, may reduce the risk of PIMs.9 In this context, a recent systematic review and meta-analysis showed that the use of PIMs increases mortality (risk ratio 1.59, 95% confidence interval 1.45–1.75).15
In the elderly, in addition to PIMs, potential prescribing omissions (PPOs), ie, medications that are not prescribed but that are clinically indicated, are also highly prevalent.3
Given the pharmacoeconomic implications of polypharmacy, the British Geriatrics Society recommends medication review interventions based on the principles of geriatric assessment for all elderly people identified with indicators of greater frailty (eg, falls, delirium, and immobility) by applying an evidence-based checklist such as the STOPP (Screening Tool of Older People’s Prescriptions) and START (Screening Tool to Alert to Right Treatment) criteria.16 The STOPP criteria were developed to identify PIMs and the START criteria were designed to identify PPOs. These tools were originally developed in Ireland and published for the first time in 2008. They were developed by using the Delphi method and were organised according to the main physiological systems affected by specific drugs or drug classes.17 These criteria were recently revised by experts from 13 European countries in an attempt to extend their application. In fact, in light of the current scientific evidence, they were updated by removing some criteria and adding others and, presently, 87 STOPP criteria and 35 START criteria are established.18 These criteria have the advantage of being easy to apply and it has already been demonstrated, in different European centres, that they are reliable and reproducible.2,3 Importantly, by the application of these criteria, there has been a reduction in the number of PIMs associated adverse events, and costs in health care, as well as a decrease in the rate of iatrogenic-based hospitalization.9–11,19–21 Therefore, these tools may be effective in improving prescribing quality, and clinical, humanistic, and economic outcomes as well.22 There are also studies evidencing their reliability even when applied by pharmacists or other healthcare professionals, helping to improve the quality of care in geriatric patients.23,24
The Beers criteria of the American Geriatric Society, originally published in 1991, were also developed by using the Delphi method, and they have had multiple updates. These criteria were created to support the clinical prescription in individuals 65 years of age or older. In addition to the list of PIMs, the Beers criteria include medications that should be avoided or their doses adjusted based on renal function and drug interactions that could lead to damage in the elderly.25–27
Since the introduction of the first version of Beers criteria by Dr Mark Beers in 1991, several other screening tools have been developed and published in the USA, Canada and European countries. Recently, an expert-consensus PIMs list covering the drugs marketed in seven European countries (Finland and Sweden in Scandinavia, France and Spain in southern Europe, Germany and the Netherlands in central Europe, and Estonia in Eastern Europe),28 called EU(7)-PIM list (ie, European list of Potentially Inappropriate Medications) was established. This list consists of 282 chemical substances or drug classes from 34 therapeutic groups and includes recommendations for dose adjustments and therapeutic alternatives. The EU(7)-PIM list is organised in two categories, independent of the diagnosis or considering the diagnosis, and it can be applied as a screening tool to identify PIMs in databases where little clinical information is available.28
In Portugal, as in other Western countries, there has been an increase in the average lifespan and, consequently, in the number of elderly people. Given that several explicit criteria for PIMs and/or PPOs detection have been developed, which have been found to be effective and reliable tools to support medication review interventions in the elderly, it is fully justified to apply and compare them in Portuguese elderly patients. Indeed, contrary to what happens in other countries, few studies have been published in Portugal on this matter, and these only applied the Beers criteria29 and STOPP/START criteria.30,31 Actually, to the best of our knowledge, the EU(7)-PIMs list has never been applied before in Portugal and according to literature, this tool is deemed to be sensitive even when the clinical information available is minimal. So, it is important to evaluate if the EU(7)-PIMs list brings clinical benefits relatively to other tools already used in Portugal. Hence, it was considered opportune to apply and compare the results generated by these three tools in the medication review of geriatric patients institutionalized or attending a day-care centre. The primary aim of the present study was to assess and compare the prevalence of PIMs and PPOs in a sample of elderly nursing home residents or outpatients of the Eastern Central Region of Portugal using three different tools (ie, Beers criteria, STOPP/START criteria and the EU(7)-PIMs list), thus inferring if the choice of the medication review screening tool is important to detect PIMs. In addition, this study aimed to compare the obtained data with the other studies carried out in other regions of Portugal and analyse the use of drugs with potential consequences on the frail elderly.
Patients and Methods
A descriptive cross-sectional study involving the analysis of clinical records of elderly nursing home residents or outpatients attending a day-care centre in the Eastern Central Region of Portugal was performed over a period of one year.
The study was based on a convenience sample, which included elderly nursing home residents and residents with total independence (outpatients, ie, people who use the nursing home as an adult day-care centre) with age ≥65 years.
The data collected from the patient’s medical records included socio-demographic data, current diagnoses, past medical history, laboratory results, vital signs measured in nursing home (eg, blood pressure) and prescribed therapy (drug substance, index date and daily dosage). Whenever the information was missing or unclear, the responsible professional caregiver (physician or nurse) was contacted.
The medicines and the diagnosis were classified according to the Anatomical Therapeutic Chemical Classification (ATC/DDD Index 2017) and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) version 2016, respectively.
All medication included in the study was analysed by applying the Beers (version 2015), the STOPP/START criteria version 2 as well as the EU(7)-PIM list. To perform a comparison with all criteria, only patients with an established diagnosis were included. The criteria were applied by two independent researchers, a practicing clinical pharmacist and a clinician. Discrepancies in the clinical judgement were resolved by discussion involving the other researchers.
Data analysis was performed using descriptive statistics as mean and range, absolute frequency and percentages.
This study received approval from the Ethics Committee of the University of Beira Interior (n.º CE-UBI-Pj-2017-004; june 26, 2017) and was conducted in agreement with the principles of the Declaration of Helsinki; all participants provided written informed consent.
Results
Data were collected from 90 patients, of which 71 (78.9%) were female, 48 were nursing home residents and 42 used the nursing home as an adult day-care centre (Table 1). The average age (overall range) was 84.15 (65–103) years. The average number of prescribed drugs per patient was 7.6, 30 of them had taken between 5 and 9 medicines and 33 had taken 9 or more medicines. Circulatory system diseases were the most prevalent, affecting 72 (80.0%) of patients, followed by endocrine, nutritional and metabolic diseases (n = 46, 51.1%), and mental and behavioural disorders (n = 43, 47.8%). Hypertension, dyslipidaemias and dementia were the most prevalent diseases in those three groups of health problems, respectively. Detailed information on the study population is provided in Table 1.
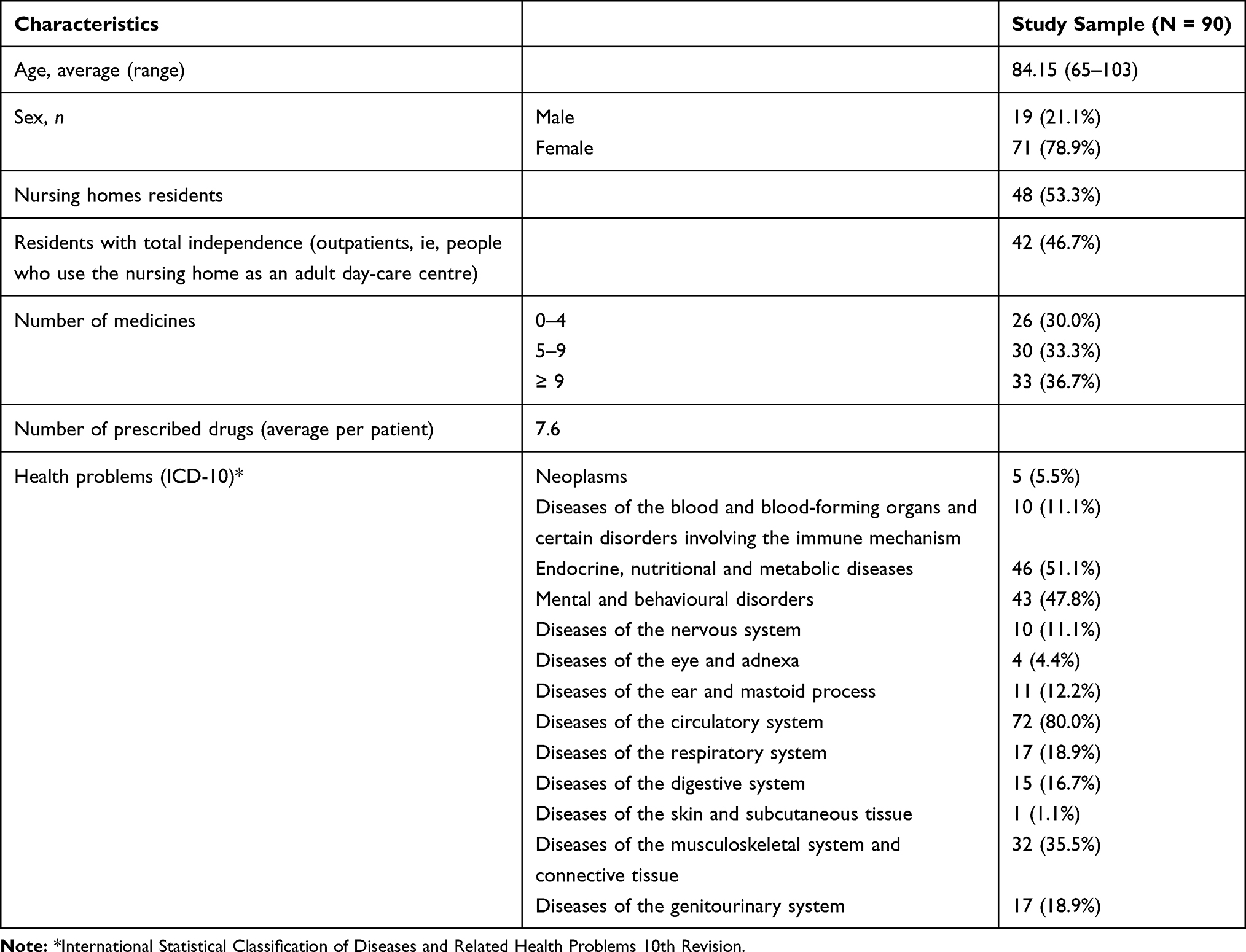 |
Table 1 Characteristics of the Study Sample (N = 90) |
The application of the Beers criteria version 2015 identified 69 PIMs in 51 (56.6%) patients, considering the panel’s recommendations and specificity.25 Most of patients presented one PIM and in 14 patients two or three PIMs were detected (Table 2). In the STOPP criteria, the diagnosis information is important to evaluate the inappropriateness of medications.18 By applying the STOPP criteria 250 PIMs were identified in 77 (85.5%) patients. The number of them having one or more PIMs was 17 and 60, respectively, and the majority of patients presented 4 PIMs (Table 2). The application of EU(7)-PIM list considering diagnosis identified 94 PIMs and, in the 90 patients, 58 (64.4%) had PIMs associated and 35 had one PIM prescribed (Table 2).
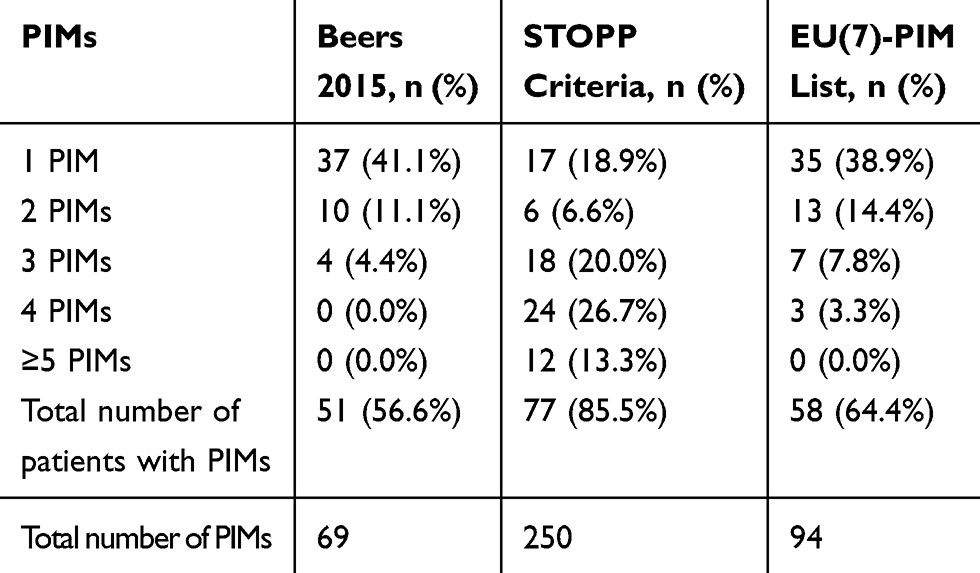 |
Table 2 Summary of Patients with Potentially Inappropriate Medications (PIMs) Identified in the Study Sample (N = 90) by Beers’ (Version 2015), STOPP Criteria (Version 2) and EU(7)-PIM List |
The drugs most commonly associated with PIMs when applying the Beers criteria were short- and intermediate-acting benzodiazepines (20 and 28 patients had been prescribed with alprazolam and lorazepam, respectively). Some patients had taken two short- and intermediate-acting benzodiazepines and one long-acting benzodiazepine. We found 7 individuals with a diagnosis of dementia that had taken one or two benzodiazepines, one person had taken zolpidem, three people had taken two benzodiazepines and two had taken an antipsychotic and an anticholinergic agent. Analyzing the “falls” history one patient had been prescribed with alprazolam, zolpidem and amitriptyline, another patient had tapentadol and two had benzodiazepines (lorazepam, alprazolam). Considering the PIMs to be used with caution in older adults, 54 patients had mirtazapine and 34 had been prescribed diuretics (Table 3). In short, medication acting on the central nervous system (CNS) was responsible for the majority of the PIMs.
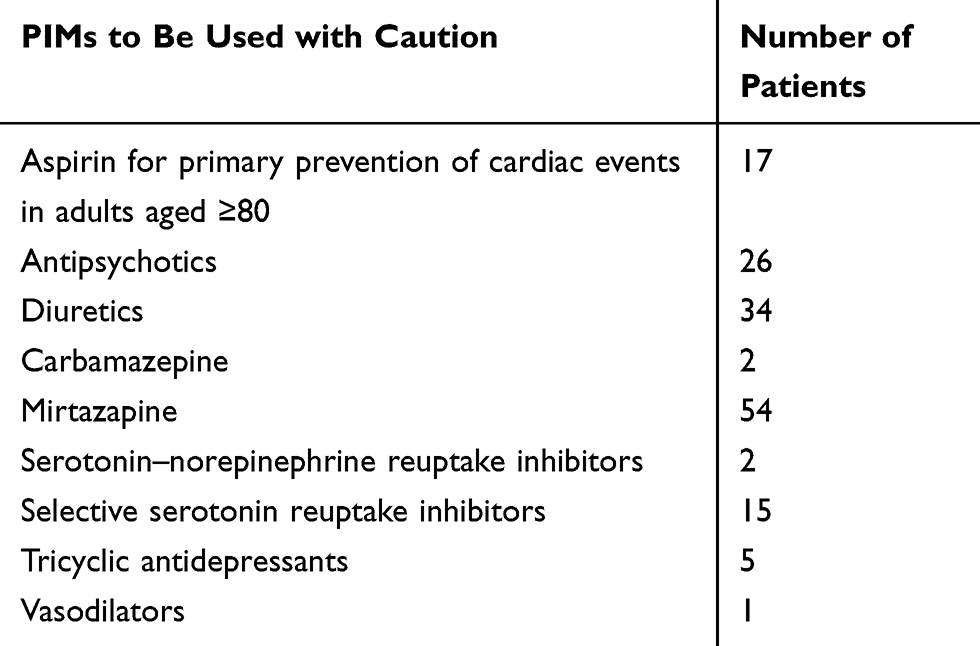 |
Table 3 Results Observed by the Application of 2015 American Geriatrics Society Beers Criteria for Potentially Inappropriate Medications (PIMs) to Be Used with Caution in Older Adults |
The PIMs most frequently identified by applying the STOPP criteria were drugs prescribed beyond the recommended duration, specifically benzodiazepines taken for 4 weeks or longer, the most prescribed being lorazepam and alprazolam (Table 4). The elderly have an increased risk of falls and benzodiazepines and neuroleptics were the agents most found as PIMs in these people. Nursing home residents (64.6%) had taken benzodiazepines and 37.5% neuroleptics. In outpatients, we found 54.8% with benzodiazepines and 23.8% with neuroleptics. Olanzapine was the neuroleptic drug most found in the nursing home residents, and in the outpatients was quetiapine. Duplicated drug class prescription was also observed, particularly two or more benzodiazepines and two or more neuroleptics.
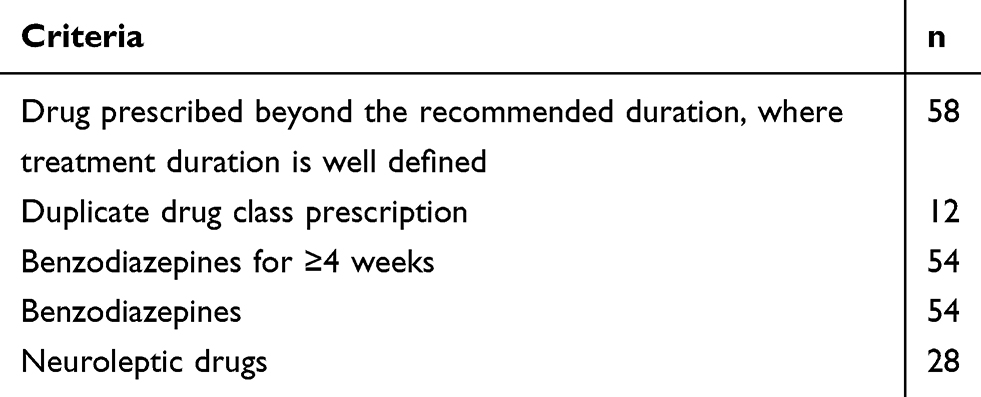 |
Table 4 Number of Patients with Potentially Inappropriate Medications (PIMs) Identified by the STOPP Criteria (Top Five) |
The most frequently identified PIMs using the EU(7)-PIM list involved anxiolytics (lorazepam > 1 mg/day and alprazolam), hypnotics and sedatives (zolpidem) in prolonged use.
The application of the START criteria identified 68 PPOs when considering the diagnosis. In addition, 52 patients had PPOs and, among these, 39 had one PPO (Table 5). The majority of PPOs involved the annual administration of seasonal trivalent influenza vaccine, detecting 36 patients who had not taken this vaccine. The bone anti-resorptive or anabolic therapy in patients with documented osteoporosis and/or previous history of fragility fracture(s) and antiplatelet therapy with a documented history of coronary, cerebral or peripheral vascular disease were the other PPOs most found (8 patients).
 |
Table 5 Summary of Patients with Potential Prescribing Omissions (PPOs) Identified in the Study Sample (N = 90) by START Criteria (Version 2) Considering the Diagnosis |
Discussion
In Portugal, as in many other countries, patient care is a priority and demands policy measures to foster clinical practice improvement and better quality of life for the patient.32 The majority of the elderly patients evaluated were taking at least one or more inappropriate drugs.5,29-31,33,34 In a polymedicated elderly person, it is important to use tools that detect the majority of PIMs to avoid any potential problems associated with inappropriate medication and thus improve their quality of life. According to literature, adverse events associated with the use of drugs occur in 15% or more of the elderly population and could be prevented.35 A recent study concluded that PIMs and polypharmacy are frequently observed in hospital-discharged patients increasing the risk of unplanned hospital readmission.36 The drugs most frequently associated with inappropriate prescribing are antiplatelet agents with over-prescribing and omission, and benzodiazepines in prolonged use.37,38 In addition, the long-term use of non-steroidal anti-inflammatory drugs has also been identified by applying the STOPP criteria.6 In Portugal, a study about institutionalized people found a total of 484 drug-related problems (DRP) in 31 elderly patients (median: 15 DRP/patient).31 Another study showed that the prevalence of PIMs, regardless of the tool used, was high.30 Our study was the only to make a detailed comparison of the detected PIMs using three different screening tools and provides useful insights regarding the prevalence of inappropriate prescription in an elderly population belonging to the Eastern Central Region of Portugal.
In the present study, we found patients polymedicated with multiple comorbidities, very similar to others studies.19,31,36 The fact that we had more women than men in our sample leads us to hypothesize that women tend to live longer and be more prone to have physical or psychological complaints.
Applying the STOPP version 2 criteria we detected significantly more PIMs in comparison with the EU(7)-PIM list and Beers criteria version 2015. The higher number of PIMs identified by the STOPP version 2 criteria may be due to the high sensitivity of these criteria for the European reality.39 In addition, there were significant differences in the number of PIMs detected depending on the tool used. In fact, the STOPP criteria are the screening tool that detected a higher number of PIMs.30 These results seem to be in accordance with a study carried out in Croatia, in which the application of the STOPP version 2 criteria identified significantly more PIMs than the EU(7)-PIM list.39 On the other hand, in a study in Lithuania, the EU(7)-PIM list detected more PIMs than the Beers criteria version 2015, such as a study conducted at the Gerontology Center Belgrade.40,41
Regardless of the existing differences in the number of PIMs detected with the above-mentioned protocols, with all of them it was observed that benzodiazepines prescribing was the most prevalent PIM and that the drugs acting on the CNS were responsible for the majority of the PIMs found. In addition, a notable proportion of PIMs was also associated with drugs targeting the CNS, which adversely affects the stability or mobility of patients. These results are in agreement with those obtained in other similar studies carried out in Portugal and other European countries.5,29-31,33,38,41
In our study, in contrast to the others performed in Portugal, alprazolam and lorazepam were the two drugs most commonly prescribed as PIMs. In the study performed in pharmacies in Lisbon, diazepam and ticlopidine were the drugs associated with inappropriateness.29 The consumption of benzodiazepines and neuroleptics was higher in the nursing home residents, in fact, previous research has reported an increased risk of mental health issues among the elderly living in residential care facilities,42 which could explain our results.
In contrast, in similar studies carried out in Portugal, no patient was using ticlopidine, and only one patient, with complicated peptic ulcer disease or erosive peptic oesophagitis, was using a PPI.18,31 However, the decrease in the use of PPI is due, most likely, to the new recommendations on the safety of its use.43
Another worrying aspect of detected PIMs was the duplicated drug classes at the top of the list, which was mainly represented by benzodiazepines and antipsychotics, similarly to those observed in a study carried out in Lisbon and Alentejo, in Portugal.30 In this context, it is important to mention that the average consumption of these two drug classes in Portugal is higher than in most European countries,32 having potential consequences on the frail elderly.33,38,44
The Beers criteria version of 2015 include the table “for Non-Anti-Infective Medications That Should Be Avoided or Have Their Dosage reduced with Varying Levels of Kidney Function in Older Adults,”25 but we did not assess patients in this context. However, we detected cases of patients taking drugs from this table, but there was no registration of creatinine clearance values in their clinical records and therefore it was not possible to assess whether the use of these drugs was or not potentially inappropriate.
The most commonly detected PPOs were associated with the area of cardiovascular prevention, specifically the absence of antiplatelet therapy, and in flu prevention the missing annually seasonal trivalent influenza vaccine.45 In this context, the flu vaccine is strongly recommended and is free of charge on the National Health Service in Portugal for people aged 65 or older.46 However, in some nursing homes, the administration of the influenza vaccine is only carried out on patients who have a medical prescription or in patients whose responsible relatives have given permission. A study performed in elderly patients that visited their primary care physician showed that the absence of antiplatelet therapy was, also, a highly ranked PPO based on START criteria.38
Another important group with omissions was the musculoskeletal system medication, but in our study, it was not attributed to the absence of vitamin D, rather to the absence of a bone anti-resorptive or anabolic therapy, in contrast to the study performed in nursing homes located in the region of Lisbon and Alentejo.30 In the analysis of medical data, we did not detect any contraindication to the use of this class of drugs.
In addition to the high prevalence of polymedication in the study population, a notable proportion of PIMs was detected. Depending on the screening tools applied, the prevalence of PIMs varied significantly. In this context, the STOPP criteria identified more PIMs in this sample than the other two tools, and it should, therefore, be preferred.30,39 Furthermore, these results suggest that there is the need for urgent interventions to improve instructions for safe drug use in elderly patients, to decrease the number of drugs whenever possible, and to increase the appropriateness of the medication regimen. Prescribing, in the future, will likely become an act supported by drug screening tools to alert doctors about potential PIMs.
Nonetheless, there were some limitations intrinsic to this study. The main one was the small sample size, which is a regional sample, which is not representative of the national population as a whole. In addition, incomplete documentation of patients’ current diagnoses and biochemical information in analysing the clinical records may have led to a lower rate of PIMs reported in some cases, or a higher rate of reporting in others (ie, where a medicine was clinically indicated but the patient’s clinical data did not support the indication). All the protocols to identify PIMs also have inherent limitations to their use. For example, there may be a difference between recommendations derived from evidence and what is in the individual patient’s best interest.47 On the other hand, the differences between the protocols and the medicines used in the countries where these tools were originally developed can also be important.
Conclusion
It is urgent to perform actions to reduce PIMs and PPOs and therefore to improve care quality. STOPP version 2 criteria identified substantially more PIMs than the EU(7)-PIM list and Beers criteria. The variations in prevalence detected with the different tools indicate that a careful choice of the tool for medication review in the elderly is important. High consumption of benzodiazepines and antipsychotics was found, having potential consequences on the frail elderly, suggesting the need for the implementation of medication review programs and interventions to improve instructions for a safer drug use in the elderly. Reducing the number of medications whenever possible, and increasing the appropriateness of the medication regimen is needed. Although screening tools will never replace the clinical assessment and judgement, they can be used as a systematic approach for improving prescribing practices in older populations. Incorporating the use of these tools by other health professionals, like nurses and pharmacists, into everyday practice could play an important role in improving the quality of pharmacotherapy and review medication of elderly nursing home residents.
Acknowledgments
The authors would like to thank the elderly patients who participated in this study and the physicians and nurses who had a fundamental contribution to obtain the clinical information required for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Laroche M, Charmes J, Nouaille Y, Picard N, Merle L. Is inappropriate medication use a major cause of adverse drug reactions in the elderly? Br J Clin Pharmacol. 2006;63(2):177–186. doi:10.1111/j.1365-2125.2006.02831.x
2. O´Connor MN, Gallagher P, O´Mahony D. Inappropriate prescribing. Criteria, detection and prevention. Drugs Aging. 2012;29(6):437–452. doi:10.2165/11632610-000000000-00000
3. Gallagher P, Baeyens J, Topinkova E, et al. Inter-rater reliability of STOPP (Screening Tool of Older Persons ’ Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment) criteria amongst physicians in six European countries. Age Ageing. 2009:603–606. doi:10.1093/ageing/afp097.
4. Klarin I, Wimo A, Fastbom J. The association of inappropriate drug use with hospitalisation and mortality. Drugs Aging. 2005;22(1):69–82. doi:10.2165/00002512-200522010-00005
5. Onder G, Liperoti R, Fialova D, et al. Polypharmacy in nursing home in Europe: results from the SHELTER study. J Gerontol a Biol Sci Med Sci. 2012;67(6):698–704. doi:10.1093/gerona/glr233
6. Marroquín EC, Iglesia NM, Cobos LP. Adecuación dela Prescripción Farmaceutica en Personas de 65 Años o más en Centros de salud Docentes de Cáceres. Rev Esp Salud Pública. 2012;86(4):419–434. doi:10.4321/S1135-57272012000400009
7. Bradley MC, Fahey T, Cahir C, et al. Potentially inappropriate prescribing and cost outcomes for older people: a cross-sectional study using the Northern Ireland Enhanced Prescribing Database. Eur J Clin Pharmacol. 2012;68(10):1425–1433. doi:10.1007/s00228-012-1249-y
8. Delgado Silveira E, Garcia M, Montero-Errasquin B, Cruz-Jentoft AJ, Gallagher PF, Sachez Castelhano C. Inappropriate prescription in older patients: the STOPP/START criteria. Rev Esp Geriatr Gerontol. 2009;44(5):273–279. doi:10.1016/j.regg.2009.03.017
9. Cahir C, Fahey T, Teeling M, Teljeur C, Feely J, Bennett K. Potentially inappropriate prescribing and cost outcomes for older people: a national population study. BJCP. 2010;69(5):543–552. doi:10.1111/j.1365-2125.2010.03628.x
10. Hyttinen V, Jyrkka J, Valtonen H. A systematic review of the impact of potentially inappropriate medication on health care utilization and costs among older adults. Med Care. 2016;54(10):950–964. doi:10.1097/MLR.0000000000000587
11. Heider D, Matschinger H, Meid AD, et al. The impact of potentially inappropriate medication on the development of health care costs and its moderation by the number of prescribed substances. Results of a retrospective matched cohort study. PLoS One. 2018:1–12. doi:10.1371/journal.pone.0198004.
12. Spinewine A, Schmader KE, Barber N, et al. Appropriate prescribing in elderly people: how well can it be measured and optimised? Lancet. 2007;370(9582):173–184. doi:10.1016/S0140-6736(07)61091-5
13. Kara Ö, Arık G, Kızılarslanoglu MC, et al. Potentially inappropriate prescribing according to the STOPP/START criteria for older adults. Aging Clin Exp Res. 2016;28(4):761–768. doi:10.1007/s40520-015-0475-4
14. Kuijpers MAJ, Van Marum RJ, Egberts ACG, Jansen PAF, Oldy T. Relationship between polypharmacy and underprescribing. BJCP. 2007;65(1):130–133. doi:10.1046/j.0306-5251.2007.02961.x
15. Muhlack DC, Hoppe LK, Weberpals J, Brenner H, Schöttker B. The association of potentially inappropriate medication at older age with cardiovascular events and overall mortality: a systematic review and meta-analysis of cohort studies. J Am Med Dir Assoc. 2017;18(3):211–220. doi:10.1016/j.jamda.2016.11.025
16. Road W, House TB, Trust F, Yorkshire W. Best practice guidelines for the management of frailty: a British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing. 2014;43(6):744–747. doi:10.1093/ageing/afu138
17. Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther. 2008;46(2):72–83. doi:10.5414/cpp46072
18. O´Mahony D, O´Sullivan D, Byrne S, O´Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2014;1–6. doi:10.1093/ageing/afu145
19. Naveiro-Rilo JC, Diez-Juárez D, Flores-Zurutuza ML, Molina-Mazo R, Alberte-Pérez C. Intervencion en ancianos con multimorbilidad y polimedicados: resultados en la prescripcio n y en la calidad de vida. Rev Calid Asist. 2014;29(5):256–262. doi:10.1016/j.cali.2014.06.002
20. Dalleur O, Boland B, Losseau C, et al. Reduction of potentially inappropriate medications using the STOPP criteria in frail older inpatients: a randomised controlled study. Drugs Aging. 2014;31(4):291–298. doi:10.1007/s40266-014-0157-5
21. Unutmaz GD, Soysal P, Tuven B, Isik AT. Costs of medication in older patients: before and after comprehensive geriatric assessment. Clin Interv Aging. 2018;13:607–613. doi:10.2147/CIA.S159966
22. Hill-Taylor B, Walsh KA, Stewart S, Hayden J, Byrne S, Sketris IS. Effectiveness of the STOPP/START (Screening Tool of Older Persons’ potentially inappropriate Prescriptions/Screening Tool to Alert doctors to the Right Treatment) criteria: systematic review and meta-analysis of randomized controlled studies. J Clin Pharm Ther. 2016;41(2):158–169. doi:10.1111/jcpt.12372
23. Gillespie U, Alassaad A, Hammarlund-Udenaes M, et al. Effects of pharmacists ’ interventions on appropriateness of prescribing and evaluation of the instruments ’ (MAI, STOPP and STARTs ’) ability to predict hospitalization — analyses from a randomized controlled trial. PLoS One. 2013;8:5. doi:10.1371/journal.pone.0062401
24. Sullivan DO, Mahony DO, Connor MNO, et al. The impact of a structured pharmacist intervention on the appropriateness of prescribing in older hospitalized patients. Drugs Aging. 2014;31:471–481. doi:10.1007/s40266-014-0172-6
25. Samuel MJ. American Geriatrics Society 2015 updated beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227–2246. doi:10.1111/jgs.13702
26. Salbu RL, Feuer J. A closer look at the 2015 Beers Criteria. J Pharm Pract. 2017;30(4):419–424. doi:10.1177/0897190016663072
27. Steinman MA, Beizer JL, Dubeau CE, Laird RD, Lundebjerg NE, Mulhausen P. How to use the American Geriatrics Society 2015 Beers Criteria - a guide for patients, clinicians, health systems, and payors. J Am Geriatr Soc. 2015;63(11):e1–7. doi:10.1111/jgs.13701
28. Renom-Guiteras A, Meyer G, Thürmann PA. The EU(7)-PIM list: a list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur J Clin Pharmacol. 2015;71(7):861–875. doi:10.1007/s00228-015-1860-9
29. de Oliveira Martins S, Soares MA, Foppe Van Mil JW, Cabrita J. Inappropriate drug use by Portuguese elderly outpatients - Effect of the Beers criteria update. Pharm World Sci. 2006;28(5):296–301. doi:10.1007/s11096-006-9046-2
30. da Costa FA, Periquito C, Carneiro MC, Oliveira P, Fernandes AI, Cavaco-Silva P. Potentially inappropriate medications in a sample of Portuguese nursing home residents: does the choice of screening tools matter? Int J Clin Pharm. 2016;38(5):1103–1111. doi:10.1007/s11096-016-0337-y
31. Silva C, Ramalho C, Luz I, Monteiro J, Fresco P. Drug-related problems in institutionalized, polymedicated elderly patients: opportunities for pharmacist intervention. Int J Clin Pharmacol. 2015;37:327–334. doi:10.1007/s11096-014-0063-2
32. Ravera S, Hummel SA, Stolk P, Heerdink RE, de Gier J. The use of driving impairing medicines: a European survey. Eur J Clin Pharmacol. 2009;65:1139–1147. doi:10.1007/s00228-009-0695-7
33. Huang AR, Mallet L, Rochefort CM, Eguale T, Buckeridge D, Tamblyn R. Medication-related falls in the elderly: causative factors and preventive strategies. Drugs Aging. 2012;29(5):359–376. doi:10.2165/11599460-000000000-00000
34. Toepfer S, Bolbrinker J, Konig M, Steinhagen-Thiessen E, Kreutz R, Demuth I. Potentially inappropriate medication in older participants of the Berlin Aging Study II (BASE- II) – sex differences and associations with morbidity and medication use. PLoS One. 2019;14(12):1–12. doi:10.1371/journal.pone.0226511
35. Pretorius RW, Gataric G, Swedlund SK, Miller JR. Reducing the risk of adverse drug events in older adults. Am Fam Physician. 2013;87(5):331–336.
36. Brunetti E, Aurucci ML, Boietti E, et al. Clinical implications of potentially inappropriate prescribing according to STOPP/START version 2 criteria in older polymorbid patients discharged from geriatric and internal medicine wards: a prospective observational multicenter study. J Am Med Dir Assoc. 2019;20(11):
37. Paci J, Alfaro M, Alonso F, San- Martín M. Prescripción inadecuada en pacientes polimedicados mayores de 64 años en atención primaria. Aten Primaria. 2015;47(1):38–47. doi:10.1016/j.aprim.2014.03.013
38. Stojanović M, Vuković M, Dimitrijević S. GheOP 3 S tool and START/STOPP criteria version 2 for screening of potentially inappropriate medications and omissions in nursing home residents. J Eval Clin Pract. 2020;26:158–164. doi:10.1111/jep.13107
39. Mucalo I, Hadžiabdić MO, Brajković A, et al. Potentially inappropriate medicines in elderly hospitalised patients according to the EU(7)-PIM list, STOPP version 2 criteria and comprehensive protocol. Eur J Clin Pharmacol. 2017;73(8):991–999. doi:10.1007/s00228-017-2246-y
40. Grina D, Briedis V. The use of potentially inappropriate medications among the Lithuanian elderly according to Beers and EU(7)-PIM list – a nationwide cross-sectional study on reimbursement claims data. J Clin Pharm Ther. 2017;42(2):195–200. doi:10.1111/jcpt.12494
41. Stojanovic M, Vukovic M, Jovanovic M, Dimitrijevic S, Radenkovic M. Potentially inappropriate medications in nursing home residents: a comparison of two approaches. Eval Heal Prof. 2020;22:1–6. doi:10.1177/0163278719900653
42. Gleeson H, Hafford-letchfield T, Quaife M, et al. Preventing and responding to depression, self- harm, and suicide in older people living in long term care settings: a systematic review. Aging Ment Health. 2019;23(11):1467–1477. doi:10.1080/13607863.2018.1501666
43. Infarmed. Comunicado de imprensa 1/1 inibidores da bomba de protões (IBP) campanha visa alertar para os riscos dos medicamentos para a acidez do estômago[press release 1/1 proton pump inhibitors (IBP) visa warning campaign for risks of drugs for stomach acidity]. Available from: http://www.infarmed.pt/documents/15786/1879176/Comunicado+-+Campanha+IBP/bb11fdf6-cb41-408a-a186-99bca397fc46.
44. Dalleur O, Spinewine A, Henrard S, Losseau C, Speybroeck N, Boland B. Inappropriate prescribing and related hospital admissions in frail older persons according to the STOPP and START criteria. Drugs Aging. 2012;29(10):829–837. doi:10.1007/s40266-012-0016-1
45. Barry PJ, Gallagher P, Ryan C, O’Mahony D. START (screening tool to alert doctors to the right treatment)— an evidence-based screening tool to detect prescribing omissions in elderly. Age Ageing. 2007;36:632–638. doi:10.1093/ageing/afm118
46. DGS. Guidance no 018/2017, 26 September 2017, Available from: https://www.dgs.pt/paginas-de-sistema/saude-de-a-a-z/gripe/normas-e-orientacoes.aspx.
47. Golomb BA, Chan VT, Evans MA, Koperski S, White HL, Criqui MH. The older the better: are elderly study participants more non-representative? A cross-sectional analysis of clinical trial and observational study samples. BMJ Open. 2012;2:6. doi:10.1136/bmjopen-2012-000833
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.