Back to Journals » Patient Preference and Adherence » Volume 13
Medication adherence in pediatric transplantation and assessment methods: a systematic review
Authors Hoegy D ![]() , Bleyzac N, Robinson P, Bertrand Y, Dussart C, Janoly-Dumenil A
, Bleyzac N, Robinson P, Bertrand Y, Dussart C, Janoly-Dumenil A
Received 3 January 2019
Accepted for publication 1 March 2019
Published 7 May 2019 Volume 2019:13 Pages 705—719
DOI https://doi.org/10.2147/PPA.S200209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Delphine Hoegy,1,2 Nathalie Bleyzac,3,4 Philip Robinson,5 Yves Bertrand,3,6 Claude Dussart,1,7 Audrey Janoly-Dumenil1,2
1EA 4129 P2S Parcours Santé Systémique – Univ Claude Bernard Lyon 1, Univ Lyon 1, Lyon, France; 2Pharmacy, Hôpital Edouard Herriot, Hospices Civils de Lyon, Lyon, France; 3Institut d’Hématologie et d’Oncologie Pédiatrique, Hospices Civils de Lyon, Lyon, France; 4EMR 3738, PK/PD Modeling in Oncology, université Lyon-Sud, Lyon, France; 5Direction de la Recherche Clinique et de l’Innovation, Hospices Civils de Lyon, Lyon, France; 6U1111-CNRS UMR 5308, University of Lyon I, ENS Lyon, Lyon, France; 7Central Pharmacy, Hospices Civils de Lyon, Lyon, France
Background: Medication adherence is a major concern in public health. It is fully established that immunosuppressive therapy (IT) and concomitant medications affect transplant outcomes in the pediatric population, showing interest in adherence to this therapy. The aim of the present review was to report on medication adherence in pediatric population post-transplantation. This will enable us to know the situation in this particular population.
Methods: A literature search was performed using the MEDLINE database. Studies that were published from January 1999 to January 2016 in English language and which investigated medication adherence in pediatric transplantation were included. The type of organ and the methods used to assess medication adherence were studied.
Results: A total of 281 records were identified, from which 34 studies were selected: 38% (n=13) on kidney transplantation, 32% (n=11) on liver transplantation, and 23% (n=10) on the transplantation of other organs. Medication adherence was found to be lower than 80% in two-thirds of the studies (64%), and varied from 22% to 97%. This wide range was explained in part by the important heterogeneity of assessment methods among studies. The methods used were objective, non-objective, or combined both types. Most studies did not fully describe the data collected: the time since transplantation, the period over which adherence was assessed, the population, the medications, and the threshold discriminating adherence and non-adherence.
Conclusion: The present study found poor medication adherence in the pediatric population post-transplantation. There was a wide range of medication adherence, explained largely by the heterogeneity of assessment methods. Future studies must consider the characteristics of each methodology, but also the threshold defining adherence should be chosen on the basis of clinical outcomes, and describe all data collected to gain precision. To improve adherence in this population, it is essential to identify factors influencing medication (IT and concomitant medications) adherence.
Keywords: medication adherence, patient compliance, child, transplantation
Introduction
Adherence is defined “as the extent to which a person’s behavior […] corresponds with agreed recommendations from a health care provider”. Medication adherence averages 50% among adults suffering from chronic diseases, and as poor medication adherence compromises the therapeutic approach it is a major concern in public health.1
In adults, immunosuppressive therapy (IT) adherence averages 48% after renal transplantation, which is the most frequent transplant procedure.2 In adults and pediatric populations, IT is recognized as essential after solid organ transplantation (SOT)3,4 and hematopoietic stem cell transplantation (HSCT).5 IT is part of treatment regimen post-transplantation that includes concomitant medications to prevent infection. After SOT in pediatric patients, the risk of biopsy-proven acute rejection is doubled, the risk of hospitalization is increased by 60%, and that of organ loss by 80% when patients considered non-adherent to IT.6 Medication adherence is therefore a major concern in pediatrics. In 2009, Dew et al49 published a meta-analysis that investigated medical regimen adherence after SOT in a pediatric population; the authors included studies that reported non-adherence to IT and/or clinical appointments. The authors concluded that there was a wide range of IT adherence rates due to the heterogeneity of methodological aspects and analysis of data in published studies. However, there is no recent systematic review that has investigated adherence to both IT and concomitant medications in a pediatric population after both SOT and HSCT. The aim of the present review was therefore to report on medication adherence in pediatric populations after both SOT and HSCT. This will provide an overview in this particular population, and a special focus will be made on the assessment methods used, which can be objective methods such as drug assays, and non-objective methods such as questionnaires.1,7
Methods
The MEDLINE database was searched for relevant studies published from January 1, 1999 to January 1, 2016 using the following search strategy: (“patient compliance” [Mesh] OR “medication adherence” [Mesh] OR medication compliance) AND (pediatr* OR child) AND (transplan*). The inclusion criteria were: studies in English language, reporting on pediatric transplant patients (age <21 years at the time of transplantation), measuring medication adherence, and describing the assessment method of medication adherence. Case reports, editorials, letters, and syllabi were excluded. Systematic and non-systematic reviews, as well as meta-analysis were excluded but checked for additional studies.11,49 The selection was independently reviewed by two of the authors (DH and AJD), and disagreements were resolved by consensus.
The analysis of selected studies consisted of description of organs, mean time since transplantation, population, medications; the methods used to assess medication adherence were also investigated.
Results
The first search strategy found 281 records; 221 were excluded because they did not talk about medication adherence in pediatric transplantation. A further 19 studies were excluded because a measure of medication adherence was not reported, and 7 because results obtained in pediatric subjects were not reported separately from other populations (Figure 1). Thus, 34 studies were included.
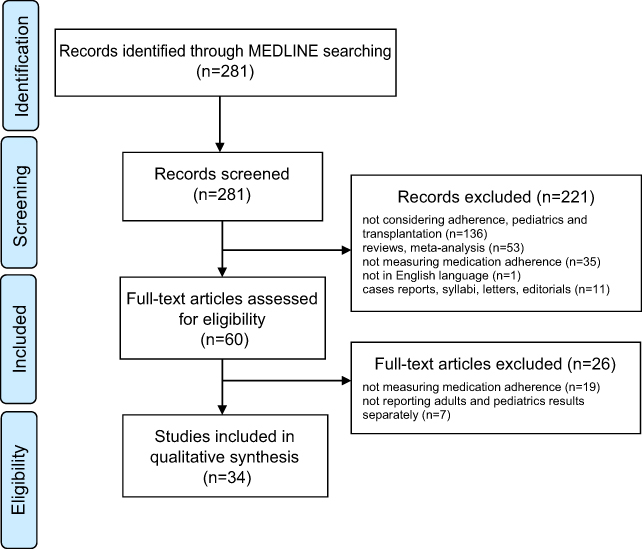 | Figure 1 Review inclusion and exclusion flowchart followed PRISMA guidelines. |
Thirteen studies concerned kidney transplantation (Table 1), and 11 liver transplantation (Table 2). Other studies reported IT adherence in heart transplantation (Table 3), HSCT (Table 4), or combined results of different organs in the same study (multi-organ studies) (Table 5).
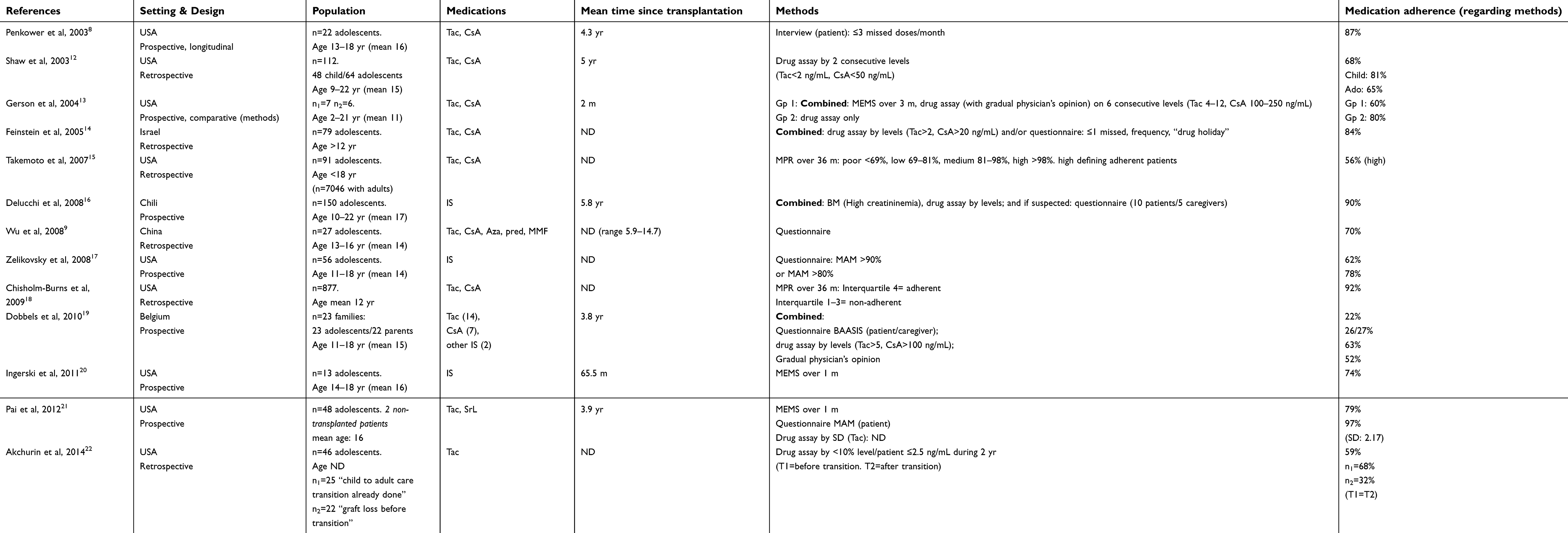 | Table 1 Medication adherence and assessment methods in kidney transplantation |
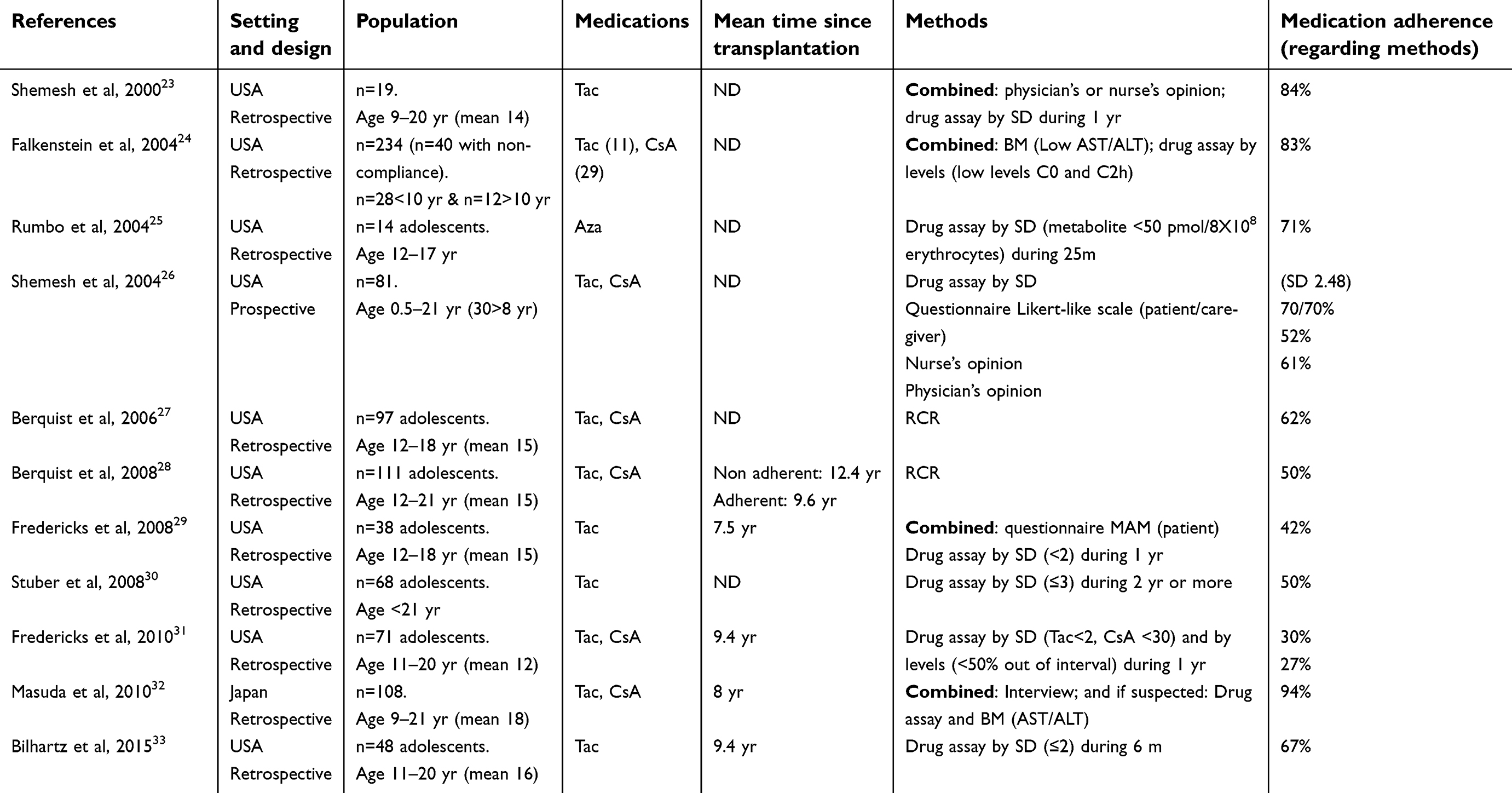 | Table 2 Medication adherence and assessment methods in liver transplantation |
 | Table 3 Medication adherence and assessment methods in heart transplantation |
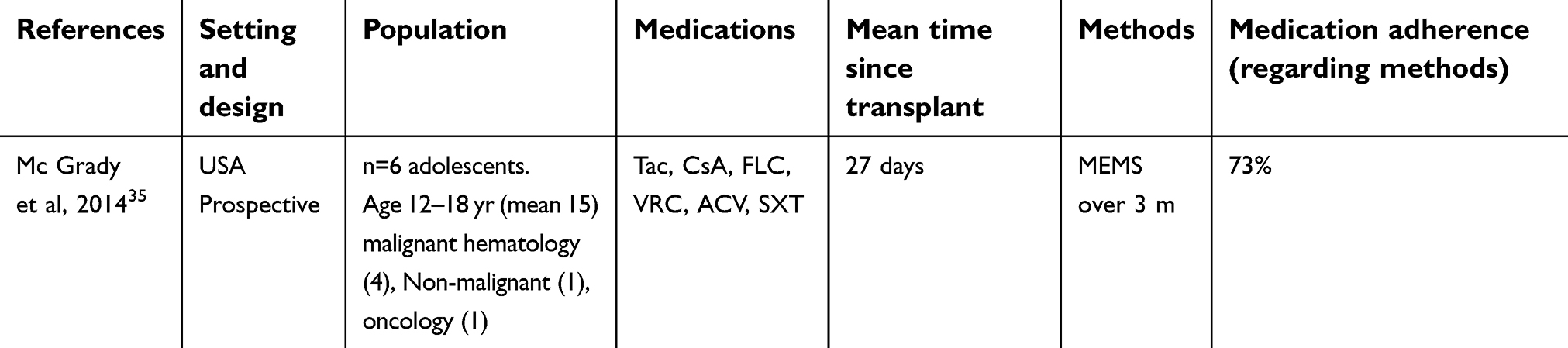 | Table 4 Medication adherence and assessment methods in hematopoietic stem cell transplantation |
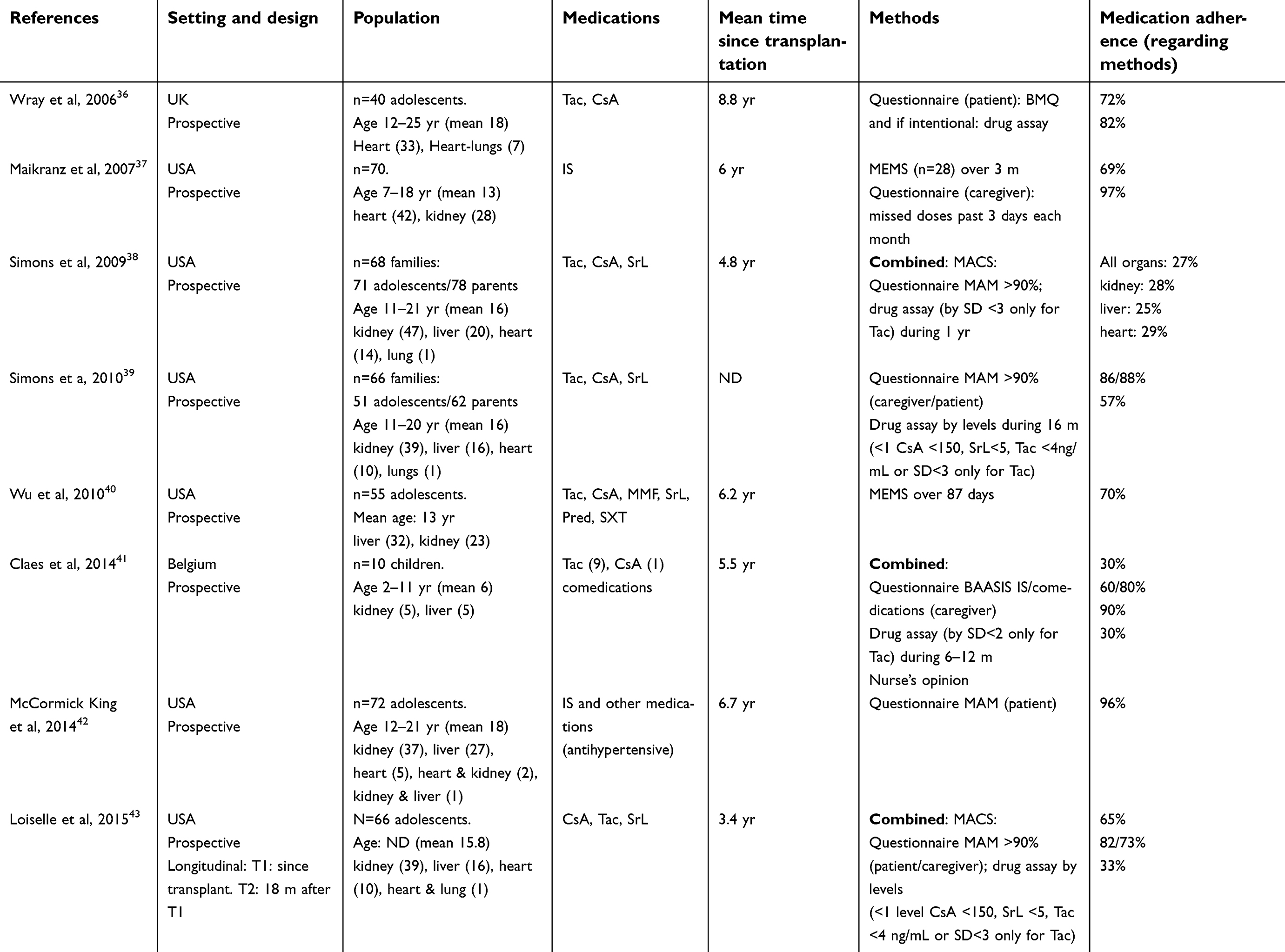 | Table 5 Medication adherence and assessment methods in multi-organ studies |
Among all types of organ, medication adherence ranged from 22%19to 97%.21 Medication adherence was found to be lower than 80% in 22 studies, between 80% and 90% in 5 studies,8,12,14,23,24 and 90% or greater in 7 studies.16,18,21,32,34,37,42 Among these 7 studies, 3 focused on kidneys,16,18,21 1 on liver,32 1 on heart,34 and 2 were multi-organ.37,42
Twenty studies reported the mean time of medication adherence measurement since transplantation, which ranged from 27 days35 to 9.4 years.31,33The majority of these studies (n=12) examined medication adherence 5 years or later after transplantation, and among these medication adherence ranged from 27%31 to 97% .37
The majority of studies (n=23) reported data for adolescents (≥10 years of age) only. Two studies reported data for children, in whom adherence was 30%41 and 91%.34 One study stratified according to the patient’s age, and concluded that medication adherence was poorer among adolescents (65%) than in children (81%).12
All included studies concerned IT. Twenty-two studies measured adherence to cyclosporine (CsA), 26 to tacrolimus (Tac), and 21 to both CsA and Tac. Three studies measured also concomitant medications: antibiotics, antivirals, antihypertensives for instance, without separated IT and concomitant medication adherence measures.35,41,42 One study compared IT to concomitant medications: IT adherence was poorer (60% vs 80%).41
Assessment methodologies
Period over which adherence was assessed
The majority of studies (n=24) reported the period over which adherence was assessed; this ranged from 7 days17,42 to 36 months.15,18The period was related to the method used: medication event monitoring systems (MEMS) generally examined adherence over a 1–6-month period,13,20,21,35,37medication possession ratio (MPR) over a 36-month period,15,18 and medication adherence measure (MAM) questionnaire over a 7-day period.17,42 Five studies13,20,21,35,37 examined medication adherence in a 3–6-month period: medication adherence ranged from 60%13 to 73%.35 Eight studies15,18,22,23,29–31,38examined medication adherence over a 1–2.5-year period: medication adherence ranged from 27%38to 92%.18
Objective methods
Thirty-one studies assessed medication adherence using objective methods: drug assays (n=21), MEMS (n=6), MPR (n=2). A total of 21 studies used drug assays (Table 6) among which 2 did not mention the type of drug assay (level or SD).32,36 The 21 other studies considered either drug or metabolite levels in plasma, serum, or blood (n=10), and/or the SD that reports drug or metabolite levels over a period of time (n=11). SD studies (performed only for Tac) found medication adherence from 27%38 to 90%.41Studies using levels reported medication adherence that ranged from 27%31 to 84%.14 Six other studies used MEMS,13,20,21,35,37,40 which is a specific medication device recording date and timing of each use, and reported medication adherence ranged from 69%37 to 79%21 (Table 6).Two studies used MPR: medication adherence reported was 56%15 and 92%.18
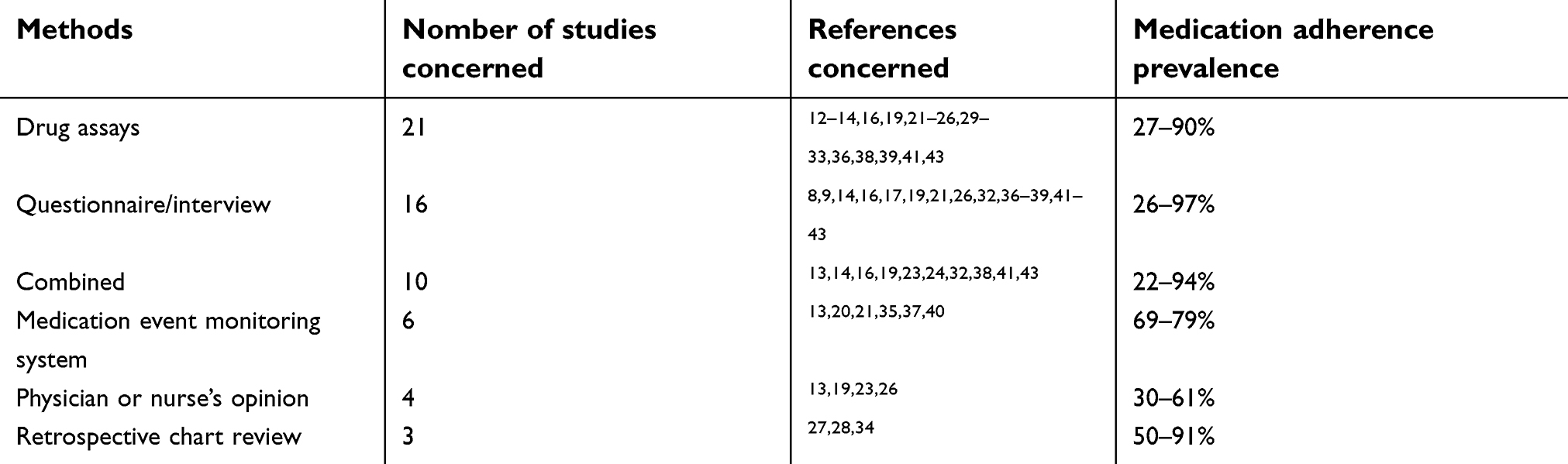 | Table 6 Methods used to assess medication adherence |
Non-objective methods
Twenty studies assessed medication adherence by non-objective methods: questionnaires or interviews (n=16), the opinion of physicians and/or nurses (n=4), retrospective chart review (RCR; n=3). RCR evaluated the number of patient records documenting medication non-adherence: the medication adherence reported in the 3 studies was 50%,28 62%,27 and 91%.34 Among the 4 studies using the opinion of physicians and/or nurses,13,19,23,26 2 reported medication adherence by this method: 52%19 and 61%.26 The medication adherence, reported by the 16 studies using questionnaires and interviews ranged from 26%19 to 97%.21 Six studies used the MAM questionnaire,17,21,38,39,42,43 which is a specific and validated pediatric tool for adherence post-transplantation that evaluates the number of missed or late doses during the previous 7 days. The medication adherence from MAM questionnaire-studies ranged from 65%17 to 97%.21 Furthermore, a total of 7 studies reported caregiver or parent’s medication adherence. Among these, 3 studies compared patient and caregiver reports and found results that were close: 26% and 27%,19 70% and 70%,26 and 86% and 88%.39
Combined methods
Sixteen studies used several assessment methods and a total of 10 studies combined these to calculate medication adherence.13,14,16,19,23,24,32,38,41,43 With this methodology, medication adherence ranged from 22%19 to 94%,32 and 5 studies reported medication adherence greater than 80%.14,16,23,24,32 Four studies detailed precisely the combination of techniques.19,38,41,43
One combination technique defined non-adherence as below a threshold for at least one item used.19,41 Two studies used a combination of drug assays, nurse/physician’s opinion, and basal adherence assessment scale for immunosuppressive medication, a validated questionnaire on a 6-point scale. Medication adherence obtained with this combination technique was 22%19 and 30%.41 Another combination technique created balance scores of different methods, such as the multidimensional adherence classification system (MACS),38,43 which is a validated tool combining the MAM questionnaire and drug assay. Two studies used this technique: medication adherence was 27%38 and 65%.43
Discussion
To the best of our knowledge, this is the first time a systematic review has focused on medication adherence in a pediatric population after both SOT and HSCT. A total of 34 studies investigated medication adherence after transplantation over the last 16 years in pediatric populations, which is low considering the number of studies in other chronic diseases.44 Irrespective of the transplanted organ, medication adherence ranged widely among studies. It remained poor with two-thirds studies (64%) describing medication adherence lower than 80%, highlighting the importance of considering medication adherence in the pediatric population post-transplantation.
Data for HSCT, a relatively frequent procedure, is reported only in one study,35 whereas two studies reported data for heart-lung transplantation which is a rare procedure.34,36 This may be related to the short period required of IT after HSCT, as compared to the indefinite period required after SOT. Nevertheless, IT is essential for good prognosis after HSCT,5 and it is therefore of great interest to evaluate medication adherence after such transplantations.
All studies in this review investigated adherence to IT, underlining the importance of this concern in the post-transplantation period. Despite the need for an effective prevention of infections after transplantation, for instance, only 3 studies reported adherence to concomitant medications such as antibiotics.35,41,42 In adults, Russel et al have considered that adherence to a medication – measured by MEMS – allowed the extrapolation of results to the comedications.45 However in pediatrics, it is more appropriate to evaluate medication adherence for individual drugs41,46 as aspects such as medication flavor or form (syrup or pill) could cause different behaviors in children.7 It would be interesting that the 3 studies found in this review did compare IT adherence to concomitant medication adherence.
Most studies reported data for adolescents, which reflects a concern regarding medication adherence in this specific population after SOT and HSCT. Only one study compared data for children and adolescents, which is regrettable. This study revealed that medication adherence in children (81%) is higher than in adolescents (65%).12 The adolescence period of life is known to decrease medication adherence by several reasons;7 for instance, Dobbels et al enunciate the transition to adulthood health care system as an important factor of non-adherence during adolescence.10 This is confirmed by a study included in this present review which found that IT adherence after transition (32%) is lower than before (68%).32 In addition, adolescence is a time when difficulties in the parent–patient relationship are important.7 Regarding it, the unfrequent comparison of adolescent and caregiver reports on medication adherence (3 studies in this review using subjective methods) would be interested to consider more.
An important aspect to consider when interpreting data is the measurement method employed. At the time of writing no “gold standard” method exists,1,7 which explains the heterogeneity of those used in this review. Surprisingly, 16 studies used only 1 method whereas it is known that no single method is optimal.1,7 For example, drug assays will not detect patients who take their medications only before clinical visits. Conversely, MEMS is a longitudinal method taking into account “drug holidays” (when a patient discontinues medication of his/her own accord). Nevertheless, patients cannot be blinded to MEMS; it interferes with daily life and causes anxiety.45 In pediatric patients, all these methods have additional drawbacks. For instance, MEMS-based studies may be too difficult to be feasible in pediatric patients who are unable to take pills,20,21,35,40 and drug assay methods are invasive so this may be a limiting factor in pediatric patients.46 Yet, 23 of the 34 studies used this method, which could indicate that this is not a drawback too hard to surpass. In this review, only 10 studies (32%) used combined methods – 4 were published before 2005 and 6 after 2008 – suggesting that this is yet to become the preferred method. Among these studies, only a minority described precisely the combination method although this is essential to interpret data as the different combination techniques have different aims. One of the combination techniques has a high sensitivity: it underestimates medication adherence but misses less frequently non-adherent patients.19,41 Whereas the other combination technique used a well-balanced score (MACS),38,43 which allows categorization of patients according to their adherence.47
An additional difficulty for the interpretation of data in the present review is the definition of medication adherence which differed between each selected study, as synthetized in the Supplementary material (Table 7). It is interesting to note that many studies did not define a threshold discriminating medication adherence and non-adherence, and when they did so this was rarely based on clinical outcomes. Generally, 80% of taken medication is the arbitrary threshold discriminating medication adherence and non-adherence.1 To be relevant this threshold should be correlated to clinical outcomes, which was a posteriori investigated in 2 studies included herein; these found a close relationship between IT adherence and graft survival (p=0.017;18 p=0.0248) and also mortality (p=0.009).48 Also, Stuber et al30 constructed ROC curve to try answering about the appropriate SD cut-off for Tac.
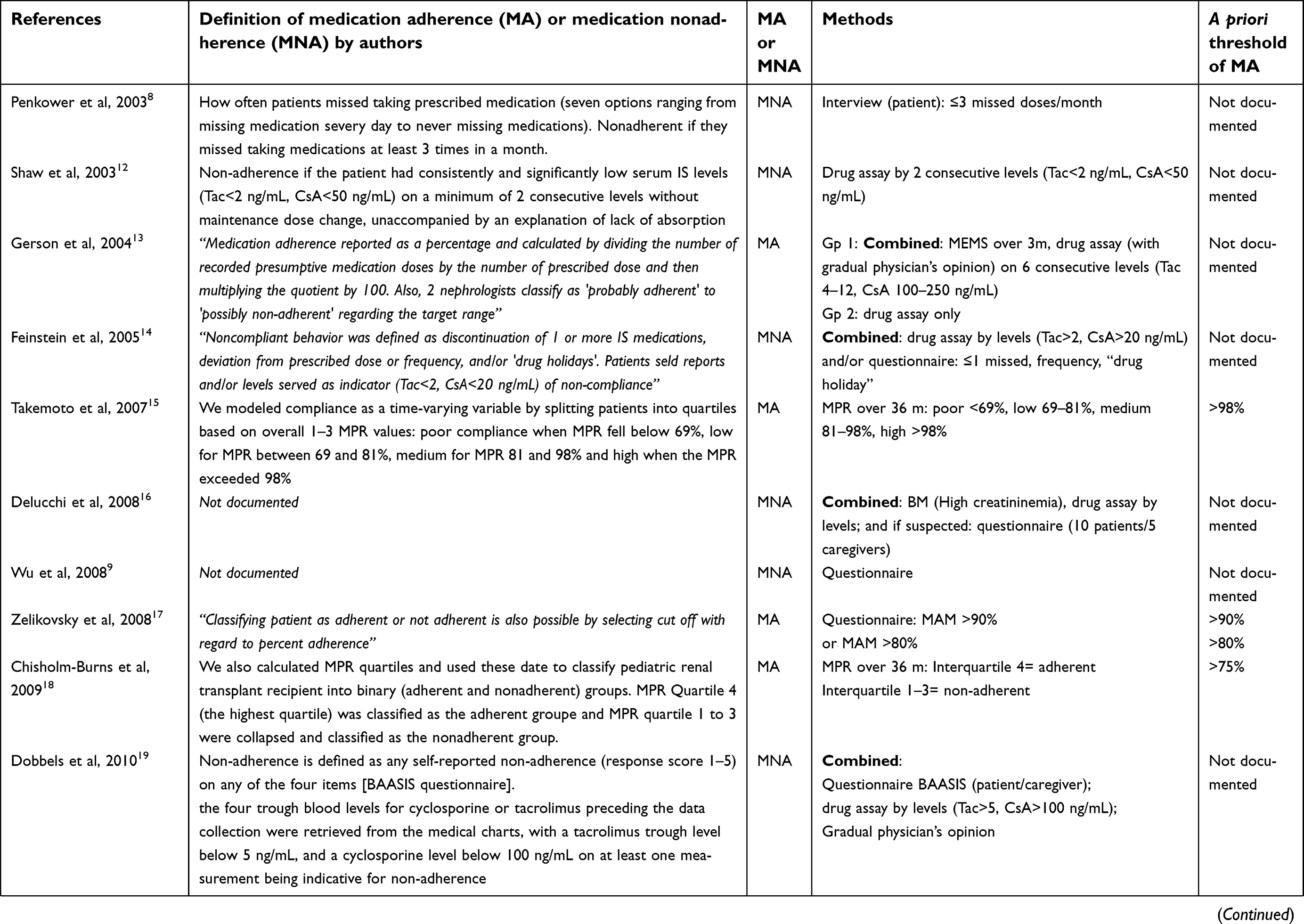 | 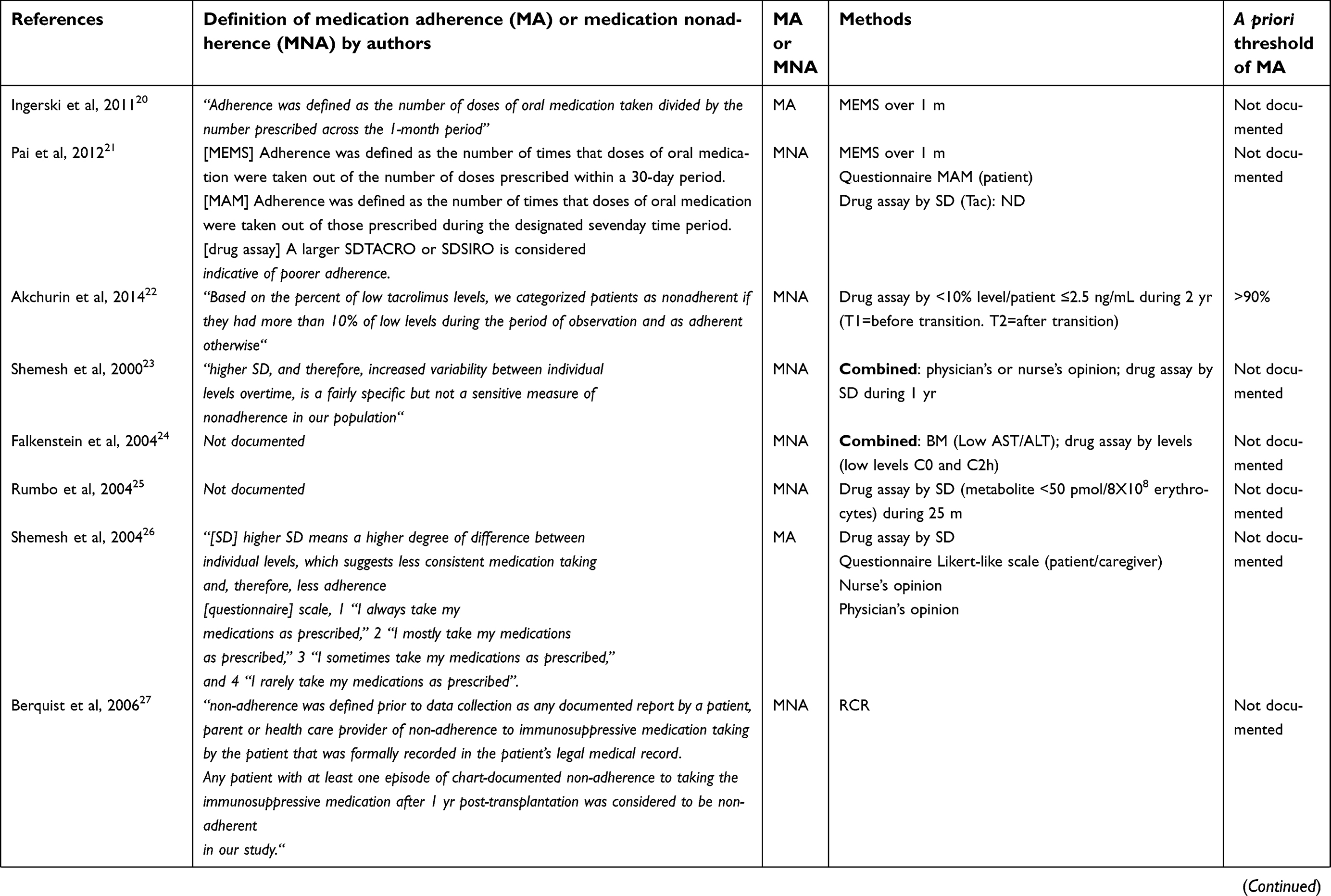 | 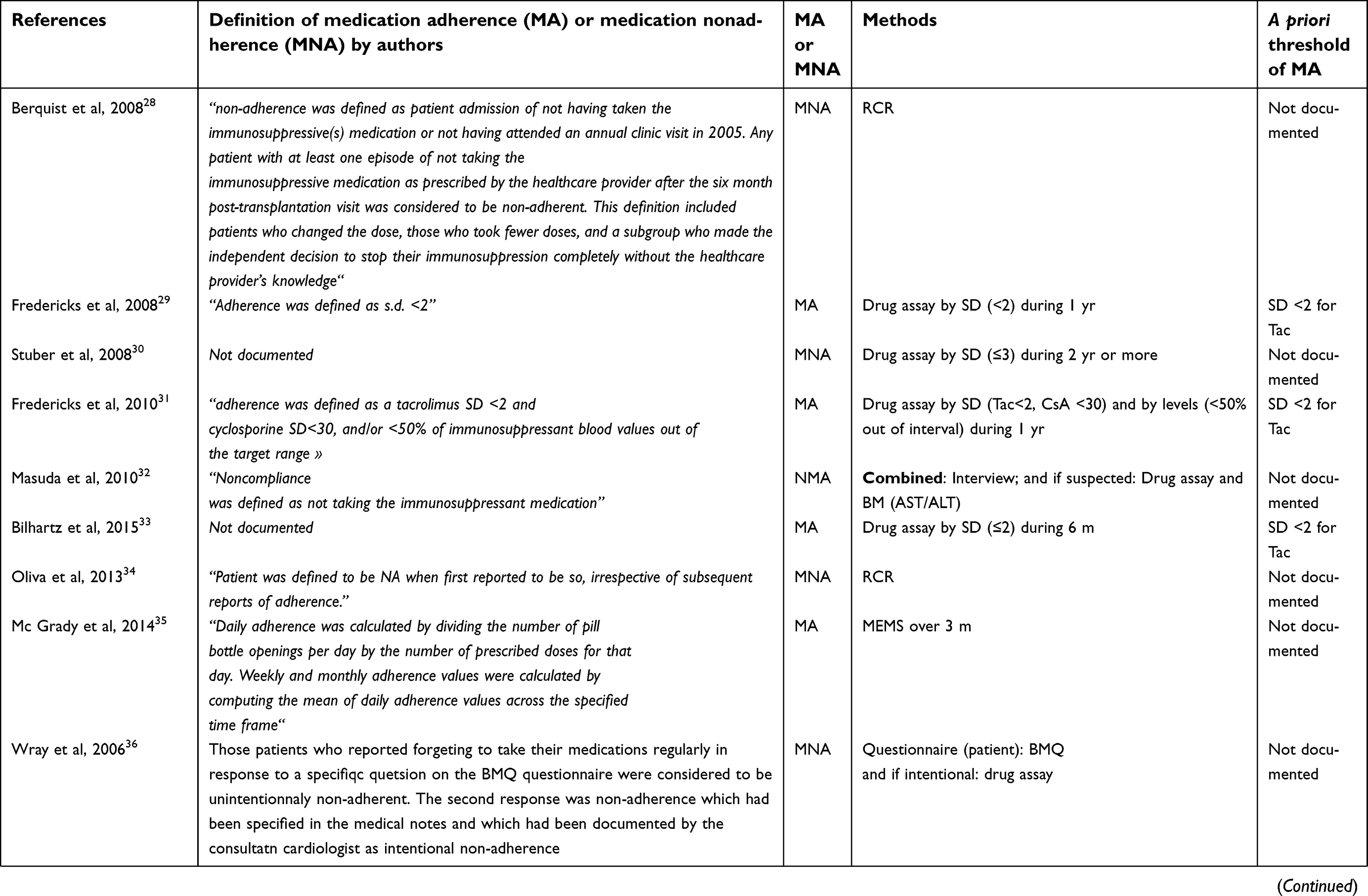 | 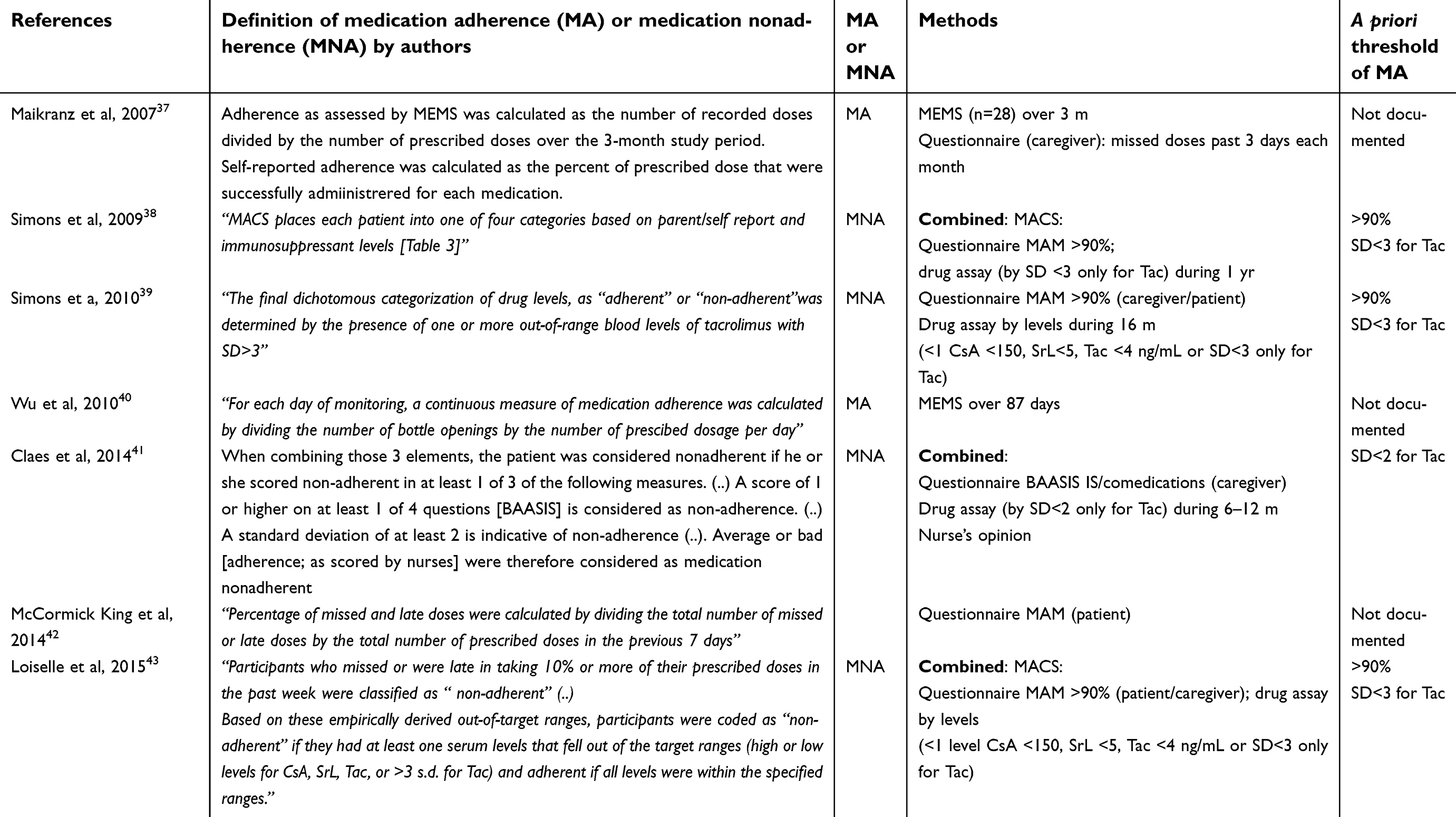 | Table 7 Assessment methods and definition of medication adherence or non-adherence by authors |
Limitations
This review included studies from the MEDLINE database only. Given the topic of this review, studies are essentially published in PubMed and research on other database is unlikely to have added additional relevant articles. An additional point is that this review is not a meta-analysis. Dew Ma et al published a meta-analysis in 2009 focusing on medication adherence after pediatric SOT only.49 The authors recognized that there was a lack of studies in certain transplantation types (lung, intestine) and noted the heterogeneity in published articles concerning methodological aspects and the analysis of data. This still seems to be the case 10 years later.
Conclusion
This review revealed the poor medication adherence in the pediatric population post-transplantation, and underlined also the wide range of medication adherence reported in the literature. The heterogeneity of assessment methods explained at least in part this wide range found. Future studies must weigh the advantages and disadvantages of each methodology and describe all data collected to gain precision. It is also essential that the threshold discriminating adherence and non-adherence must be chosen on the basis of clinical outcomes. Beyond the observation of poor medication adherence, there is an obvious need to improve this situation. For that it is essential to identify factors of medication non-adherence to propose adapted interventions and so try to improve medication adherence in adolescents and children after SOT and HSCT.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2003.
2. Chisholm MA, Vollenweider LJ, Mulloy LL, et al. Renal transplant patient compliance with free immunosuppressive medications. Transplantation. 2000;70:1240–1244.
3. Neu AM. Special issues in pediatric kidney transplantation. Adv Chronic Kidney Dis. 2006;13:62–69. doi:10.1053/j.ackd.2005.10.001
4. Kerkar N, Emre S. Issues unique to pediatric liver transplantation. Clin Liver Dis. 2007;11:323–335. doi:10.1016/j.cld.2007.04.001
5. Locatelli F, Zecca M, Rondelli R, et al. Graft versus host disease prophylaxis with low-dose cyclosporine-A reduces the risk of relapse in children with acute leukemia given HLA-identical sibling bone marrow transplantation: results of a randomized trial. Blood. 2000;95:1572–1579.
6. Connelly J, Pilch N, Oliver M, et al. Prediction of medication non-adherence and associated outcomes in pediatric kidney transplant recipients. Pediatr Transplant. 2015;19:1–8. doi:10.1111/petr.12479
7. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. doi:10.1056/NEJMra050100
8. Penkower L, Dew MA, Ellis D, Sereika SM, Kitutu JMM, Shapiro R. Psychological distress and adherence to the medical regimen among adolescent renal transplant recipients. Am J Transplant. 2003;3:1418–1425. doi:10.1046/j.1600-6135.2003.00226.x
9. Wu ZX, Yang SL, Wu WZ, et al. The long-term outcomes of pediatric kidney transplantation: a single-centre experience in China. Pediatr Transplant. 2008;12:215–218. doi:10.1111/j.1399-3046.2007.00814.x
10. Dobbels F, Van Damme-Lombaert R, Vanhaecke J, De Geest S. Growing pains: non-adherence with the immunosuppressive regimen in adolescent transplant recipients. Pediatr Transplant. 2005;9:381–390. doi:10.1111/j.1399-3046.2005.00356.x
11. Dobbels F, Ruppar T, De Geest S, Decorte A, Van Damme-Lombaerts R, Fine RN. Adherence to the immunosuppressive regimen in pediatric kidney transplant recipients: a systematic review. Pediatr Transplant. 2010;14:603–613. doi:10.1111/j.1399-3046.2010.01299.x
12. Shaw RJ, Palmer L, Blasey C, Sarwal M. A typology of non-adherence in pediatric renal transplant recipients. Pediatr Transplant. 2003;7:489–493.
13. Gerson AC, Furth SL, Neu AM, Fivush BA. Assessing associations between medication adherence and potentially modifiable psychosocial variables in pediatric kidney transplant recipients and their families. Pediatr Transplant. 2004;8:543–550. doi:10.1111/j.1399-3046.2004.00215.x
14. Feinstein S, Keich R, Becker-Cohen R, Rinat C, Schwartz SB, Frishberg Y. Is noncompliance among adolescent renal transplant recipients inevitable? Pediatrics. 2005;115:969–973. doi:10.1542/peds.2004-0211
15. Takemoto SK, Pinsky BW, Schnitzler MA, et al. A retrospective analysis of immunosuppression compliance, dose reduction and discontinuation in kidney transplant recipients. Am J Transplant. 2007;7:2704–2711. doi:10.1111/j.1600-6143.2007.01966.x
16. Delucchi A, Gutierrez H, Arrellano P, Slater C, Meneses M, López I. Factors that influence nonadherence in immunosuppressant treatment in pediatric transplant recipients: a proposal for an educational strategy. Transplant Proc. 2008;40:3241–3243. doi:10.1016/j.transproceed.2008.03.125
17. Zelikovsky N, Schast AP, Palmer J, Meyers KEC. Perceived barriers to adherence among adolescent renal transplant candidates. Pediatr Transplant. 2008;12:300–308. doi:10.1111/j.1399-3046.2007.00886.x
18. Chisholm-Burns MA, Spivey CA, Rehfeld R, Zawaideh M, Roe DJ, Gruessner R. Immunosuppressant therapy adherence and graft failure among pediatric renal transplant recipients. Am J Transplant. 2009;9:2497–2504. doi:10.1111/j.1600-6143.2009.02793.x
19. Dobbels F, Decorte A, Roskams A, Van Damme-Lombaerts R. Health-related quality of life, treatment adherence, symptom experience and depression in adolescent renal transplant patients. Pediatr Transplant. 2010;14:216–223. doi:10.1111/j.1399-3046.2009.01197.x
20. Ingerski L, Perrazo L, Goebel J, Pai ALH. Family strategies for achieving medication adherence in pediatric kidney transplantation. Nurs Res. 2011;60:190–196. doi:10.1097/NNR.0b013e318215fdfe
21. Pai AL, Rausch J, Tackett A, Marsolo K, Drotar D, Goebel J. System for integrated adherence monitoring: real-time non-adherence risk assessment in pediatric kidney transplantation. Pediatr Transplant. 2012;16:329–334. doi:10.1111/j.1399-3046.2012.01657.x
22. Akchurin OM, Melamed ML, Hashim BL, Kaskel FJ, Del Rio M. Medication adherence in the transition of adolescent kidney transplant recipients to the adult care. Pediatr Transplant. 2014;18:538–548. doi:10.1111/petr.12289
23. Shemesh E, Lurie S, Stuber ML, et al. A pilot study of posttraumatic stress and nonadherence in pediatric liver transplant recipients. Pediatrics. 2000;105:E29. doi:10.1542/peds.105.2.e29
24. Falkenstein K, Flynn L, Kirkpatrick B, Casa-Melley A, Dunn S. Non-compliance in children post-liver transplant. Who are the culprits? Pediatr Transplant. 2004;8:233–236. doi:10.1111/j.1399-3046.2004.00136.x
25. Rumbo C, Shneider BL, Emre SH. Utility of azathioprine metabolite measurements in post-transplant recurrent autoimmune and immune-mediated hepatitis. Pediatr Transplant. 2004;8:571–575. doi:10.1111/j.1399-3046.2004.00230.x
26. Shemesh E, Shneider BL, Savitzky JK, et al. Medication adherence in pediatric and adolescent liver transplant recipients. Pediatrics. 2004;113:825–832.
27. Berquist RK, Berquist WE, Esquivel CO, et al. Adolescent non-adherence: prevalence and consequences in liver transplant recipients. Pediatr Transplant. 2006;10:304–310. doi:10.1111/j.1399-3046.2005.00451.x
28. Berquist RK, Berquist WE, Esquivel CO, Cox KL, Wayman KI, Litt IF. Non-adherence to post-transplant care: prevalence, risk factors and outcomes in adolescent liver transplant recipients. Pediatr Transplant. 2008;12:194–200. doi:10.1111/j.1399-3046.2007.00809.x
29. Fredericks EM, Magee JC, Opipari-Arrigan L, Shieck V, Well A, Lopez MJ. Adherence and health-related quality of life in adolescent liver transplant recipients. Pediatr Transplant. 2008;12:289–299. doi:10.1111/j.1399-3046.2008.00901.x
30. Stuber ML, Shemesh E, Seacord D, Washington J, Hellemann G, McDiarmid S. Evaluating non-adherence to immunosuppressant medications in pediatric liver transplant recipients. Pediatr Transplant. 2008;12:284–288. doi:10.1111/j.1399-3046.2008.00923.x
31. Fredericks EM, Dore-Stites D, Well A, et al. Assessment of transition readiness skills and adherence in pediatric liver transplant recipients. Pediatr Transplant. 2010;14:944–953. doi:10.1111/j.1399-3046.2010.01349.x
32. Masuda Y, Mita A, Ohno Y, et al. Noncompliance with medications in pediatric patients after living-donor liver transplantation. Transplant Proc. 2010;42:4191–4192. doi:10.1016/j.transproceed.2010.09.087
33. Bilhartz JL, Lopez MJ, Magee JC, Shieck VL, Eder SJ, Fredericks EM. Assessing allocation of responsibility for health management in pediatric liver transplant recipients. Pediatr Transplant. 2015;19:538–546. doi:10.1111/petr.12466
34. Oliva M, Singh TP, Gauvreau K, Vanderpluym CJ, Bastardi HJ, Almond CS. Impact of medication non-adherence on survival after pediatric heart transplantation in the U.S.A. J Heart Lung Transplant. 2013;32:881–888. doi:10.1016/j.healun.2013.03.008
35. McGrady ME, Williams SN, Davies SM, Pai ALH. Adherence to outpatient oral medication regimens in adolescent hematopoietic stem cell transplant recipients. Eur J Oncol Nurs. 2014;18:140–144. doi:10.1016/j.ejon.2013.11.007
36. Wray J, Waters S, Radley-Smith R, Sensky T. Adherence in adolescents and young adults following heart or heart-lung transplantation. Pediatr Transplant. 2006;10:694–700. doi:10.1111/j.1399-3046.2006.00554.x
37. Maikranz JM, Steele RG, Dreyer ML, Stratman AC, Bovaird JA. The relationship of hope and illness-related uncertainty to emotional adjustment and adherence among pediatric renal and liver transplant recipients. J Pediatr Psychol. 2007;32:571–581. doi:10.1093/jpepsy/jsl046
38. Simons LE, McCormick ML, Mee LL, Blount RL. Parent and patient perspectives on barriers to medication adherence in adolescent transplant recipients. Pediatr Transplant. 2009;13:338–347. doi:10.1111/j.1399-3046.2008.00940.x
39. Simons LE, McCormick ML, Devine K, Blount RL. Medication barriers predict adolescent transplant recipients’ adherence and clinical outcomes at 18-month follow-up. J Pediatr Psychol. 2010;35:1038–1048. doi:10.1093/jpepsy/jsq025
40. Wu YP, Aylward BS, Steele RG. Associations between internalizing symptoms and trajectories of medication adherence among pediatric renal and liver transplant recipients. J Pediatr Psychol. 2010;35:1016–1027. doi:10.1093/jpepsy/jsq014
41. Claes A, Decorte A, Levtchenko E, Knops N, Dobbels F. Facilitators and barriers of medication adherence in pediatric liver and kidney transplant recipients: a mixed-methods study. Prog Transplant. 2014;24(4):311–321. doi:10.7182/pit2014873
42. McCormick King ML, Mee LL, Gutiérrez-Colina AM, Eaton CK, Lee JL, Blount RL. Emotional functioning, barriers, and medication adherence in pediatric transplant recipients. J Pediatr Psychol. 2014;39:283–293. doi:10.1093/jpepsy/jst074
43. Loiselle KA, Gutierrez-Colina AM, Eaton CK, et al. Longitudinal stability of medication adherence among adolescent solid organ transplant recipients. Pediatr Transplant. 2015;19:428–435. doi:10.1111/petr.12480
44. Kim SH, Gerver SM, Fidler S, et al. Adherence to antiretroviral therapy in adolescents living with HIV: systematic review and meta-analysis. Aids. 2014;28:1945–1956. doi:10.1097/QAD.0000000000000316
45. Russell CL, Conn VS, Ashbaugh C, Madsen R, Hayes K, Ross G. Intrasubject medication adherence patterns. Clin Nurs Res. 2007;16:153–163. doi:10.1177/1054773806296429
46. Chisholm MA, Mulloy LL, DiPiro JT. Comparing renal transplant patients’ adherence to free cyclosporine and free tacrolimus immunosuppressant therapy. Clin Transplant. 2005;19:77–82. doi:10.1111/j.1399-0012.2004.00301.x
47. Simons LE, Gilleland J, Blount RL, et al. Multidimensional Adherence Classification System (MACS): initial development with adolescent transplant recipients. Pediatr Transplant. 2009;13:590–598. doi:10.1111/j.1399-3046.2008.01038.x
48. Chartrand C, Servando ES, Chartrand S. Risk factors for acute rejection after pediatric heart transplantation. Transplant Proc. 2001;33:1732–1734.
49. Dew MA, Dabbs AD, Myaskovsky L, et al. Meta-analysis of medical regimen adherence outcomes in pediatric solid organ transplantation. Transplantation. 2009;88(5):736–746. doi:10.1097/TP.0b013e3181b2a0e0
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.