Back to Journals » Patient Preference and Adherence » Volume 19
Medication Adherence in Adults with Type 2 Diabetes: A Comprehensive Qualitative Meta-Synthesis of Factors in the MENA Region
Authors Al-Salmi N, Muliira JK, Lazarus ER ![]()
Received 7 March 2025
Accepted for publication 25 July 2025
Published 31 July 2025 Volume 2025:19 Pages 2263—2281
DOI https://doi.org/10.2147/PPA.S526844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Nasser Al-Salmi, Joshua K Muliira, Eilean Rathinasamy Lazarus
Department of Adult Health and Critical Care, College of Nursing, Sultan Qaboos University, Muscat, Oman
Correspondence: Eilean Rathinasamy Lazarus, Department of Adult Health and Critical Care College of Nursing, Sultan Qaboos University, Muscat, Oman, Tel +968 98512742, Fax +968 2441 3536, Email [email protected]; [email protected]
Purpose: Medication adherence is a critical factor in the management of Type 2 Diabetes (T2D) and plays a vital role in slowing disease progression, preventing complications and improving health outcomes. This study fills this gap by systematically integrating findings from qualitative studies to provide a comprehensive understanding of the multilevel determinants of adherence unique to the MENA sociocultural context.
Methods: A metasynthesis was conducted using a thematic synthesis approach, incorporating data from nine qualitative studies. The search was limited to research articles published in English between 2014 and 2024.
Results: The metasynthesis identified four key themes: (1) personal factors and perceptions related to the disease and medications are fundamental to adherence, (2) healthcare provider attitudes and practices can improve adherence to medications, (3) the healthcare system is a key factor for optimal adherence, and (4) sociocultural, alternative medicine, and religious practices affect adherence in the MENA region.
Conclusion: Medication adherence among adults with T2D in the MENA region is influenced by factors related to the individual patients, healthcare providers, healthcare system, and sociocultural practices. There is a need for more qualitative studies to address existing knowledge gaps about the agency of the above factors in regard to initiation and control of actions that lead to medication adherence.
Plain Language Summary: Taking medication as prescribed is very important for managing Type 2 Diabetes (T2D) and preventing complications. In the Middle East and North Africa (MENA) region, several factors can affect whether people stick to their medication plan. These factors include personal beliefs about the disease and medicine, the way doctors and healthcare workers interact with patients, the overall healthcare system, and cultural or religious practices. Understanding these factors can help improve ways to support people in taking their medication properly. More research is needed to explore how these different factors work together to affect medication adherence and to find better ways to help people manage their diabetes.
Keywords: compliance, medication adherence, MENA region, Middle East, qualitative, type 2 diabetes
Introduction
Type 2 Diabetes Mellitus (T2DM) is a significant global epidemic, affecting an estimated 537 million adults worldwide in 2019, a number projected to rise to 783 million by 2045.1 In the United States, diabetes is the seventh leading cause of death2 and the Centers for Disease Control and Prevention (CDC) (2021) estimated that 38.1 million adults aged 18 years or older (14.7% of all US adults) had diabetes.3 In low- and middle-income countries (LMICs), the burden of T2DM is even more pronounced, because they account for approximately 79% of all diabetes cases and this alarming trend is due to rapid urbanization, sedentary lifestyles, and aging populations.4
In the Middle East and North Africa (MENA) region, a total of approximately 73 million people are living with diabetes and this translates into one in every 6 adults being affected by diabetes.1 The MENA region has undergone major socioeconomic changes that have led to urbanization, and sedentary lifestyles since the discovery of oil in the past four decades. The changes in lifestyles and eating habits have led to increased prevalence in obesity, physical inactivity, and consumption of calorie-dense diets, all of which are major fuels for the diabetes epidemic.5 The IDF has projected a staggering 110% increase in the prevalence of diabetes in the MENA region by 2045, underscoring the urgent need for effective prevention and management strategies to address the growing crisis.1
Effective diabetes management requires individuals to adhere to comprehensive treatment regimens, including dietary restrictions, regular physical activity, medication adherence, and self-monitoring of blood glucose levels.6 The World Health Organization (WHO, 2003) defines adherence as
the extent to which a person’s behavior, such as taking medication, following a diet, and/or making lifestyle changes, aligns with agreed recommendations from a healthcare provider.
The WHO definition emphasizes the importance of active, voluntary, and collaborative participation by patients in a mutually acceptable plan of action to achieve therapeutic outcomes.7,8 The WHO also entrenches that increasing the effectiveness of adherence interventions may have a far greater impact on population health than any improvement in specific medical treatments.7 Therefore, it is imperative to thoroughly examine the issues that sustain poor adherence and devise effective interventions to enhance medication adherence.
Achieving optimal medication adherence can be challenging for healthcare providers, patients, and the healthcare system in all regions of the world. In developed countries, nonadherence to medication for chronic diseases like T2D ranges from 30% to 50%, and this rate is even higher in developing countries.9 The outcomes of nonadherence negatively impact the patient clinical outcomes and impose a substantial economic burden on individuals, families, and healthcare systems.10 The factors that affect medication adherence are complex and multifaceted. For instance, the patient-related factors play a critical role11 and include aspects such as low health literacy which hinder patients’ understanding of their condition and the importance of following prescribed treatment regimens.12
Moreover, financial constraints, such as limited monthly income, may prevent patients from consistently accessing necessary medications.11,13 Additionally, concerns about medication side effects can discourage adherence, as individuals may prioritize avoiding the associated discomfort over the long-term benefits of treatment.12 Addressing these contributing factors requires targeted patient education, strategies to alleviate financial burdens, and medication side effects.14
The provider-related factors that are associated with poor medication adherence include prescription of complex drug regimens, inadequate communication and explanation of side effects, and fragmented care from multiple physicians.15 On the other hand, the healthcare system-related factors might include issues such as limited clinic time which restricts healthcare providers from thoroughly educating patients and addressing their concerns;16 poor access to healthcare services such as in rural or underserved areas;17 and the lack of robust health information technology, such as electronic records or patient portals, to ensure effective communication and follow-up.18
Extensive research has been conducted globally to identify factors influencing medication adherence among individuals with T2D, including barriers and facilitators. Systematic reviews based on quantitative studies have synthesized findings from other regions of the world to provide a comprehensive overview of medication adherence.19,20 Most quantitative studies have identified measurable variables such as demographic, socioeconomic, and clinical factors associated with adherence.21,22 For instance, studies in the US and Europe emphasize patient-provider shared decision-making and digital health tools as adherence facilitators, whereas Asian research highlights familial involvement and traditional medicine integration.23 In contrast, the MENA region—characterized by fragmented healthcare systems, cultural reliance on herbal remedies, and religious interpretations of chronic disease—presents a distinct adherence landscape that remains underexplored. Existing global syntheses rarely address how these intersecting factors uniquely manifest in MENA, creating a critical gap in contextually relevant evidence to inform interventions. T2D Medication Adherence Research has largely been within Western settings, which is framed by issues of healthcare access and patient agency around adherence.24 MENA still lacks profound study on specific problems such as the fragmented systems, reliance on traditional medicine as a cultural health security and tectonic religious dimensions attached to illness.25 While having the second-highest diabetes prevalence in the world,1 MENA with lower adherence rates provides a valuable need for the region-specific understandings as explained using global theoretical frameworks (MENAs) such as Health Belief Model.26 Whereas qualitative studies have mostly explored patients’ experiences and perspectives, uncovering the influence of psychological, social, and cultural factors on medication adherence.
Although studies have examined factors influencing medication adherence in various regions of the world, there have no study that has sufficiently focused on the MENA region, leading to its underrepresentation in the literature. The MENA region has unique environmental, socioeconomic, religious, and cultural differences that might impact medication nonadherence.27 Although these factors may vary across countries and populations, understanding the regional variations is crucial for developing effective, culturally sensitive interventions. A comprehensive understanding of medication adherence can be achieved by synthesizing existing qualitative studies exploring individual and provider perspectives on factors contributing to medication nonadherence in the MENA region.
Qualitative studies provide insights into the underlying barriers, perceptions, and factors influencing adherence behaviors. The aim of this meta-synthesis was to synthesize findings from qualitative studies of the factors influencing medication adherence among adults with T2D in the MENA region. Therefore, the meta-synthesis was aimed to answer the question: What factors influence medication adherence among adults with Type 2 Diabetes (T2D) in the MENA region?
Methods
The study employed a qualitative meta-synthesis approach to systematically analyze existing qualitative research to address the above research question. The process involved identifying the research question, conducting a comprehensive literature search, selecting relevant studies, critically appraising their quality, summarizing key findings, and synthesizing the evidence to identify common themes and insights.28
Data Sources and Searches
This meta-synthesis review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive literature search was conducted across six databases: CINAHL, PubMed, PsycINFO, Science Direct, Psychology and Behavioral Sciences Collection, and SocINDEX. The search was limited to English-language research articles published between 2014 and 2024. The search terms included compliance, adherence, medication adherence, MENA region, Middle East, North Africa, qualitative, Type 2 Diabetes, and Diabetes Mellitus. The inclusion criteria focused on original research articles published in peer-reviewed journals that were conducted within the Middle East or North Africa. The complete search process and study selection are illustrated in Figure 1.
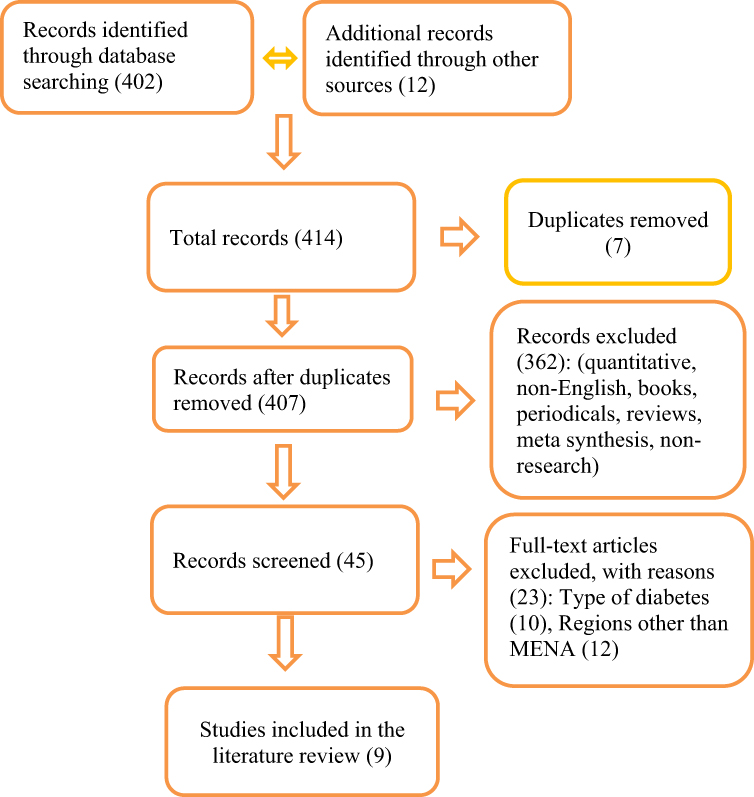 |
Figure 1 Search process and study selection of research article. |
Study Selection
Abstracts were screened based on specific inclusion criteria to ensure relevance and quality. The inclusion criteria were as follows:
- studies must be original and utilized a qualitative or mixed-methods research approach;
- conducted within the MENA region;
- involve adult participants with type 2 diabetes; and
- examine factors influencing medication adherence.
Articles meeting the above criteria were subjected to a comprehensive review. Additionally, the reference lists of key articles were examined to uncover other studies that might have been missed during the initial database searches. The exclusion criteria included
- quantitative studies,
- non-research articles,
- review articles, books, editorials, and studies that did not explicitly define the type of diabetes under investigation.
- Furthermore, studies conducted outside the MENA region were excluded to maintain the focus of the review.
Data Extraction and Quality Synthesis
Articles meeting the inclusion criteria were assessed for quality attributes by two doctoral level researchers. In cases of disagreement, consensus was achieved through discussion and collaborative review. The quality appraisal was conducted using the tool which is available in public domain developed by Letts et al (2007), which evaluates qualitative studies across 17 specific quality domains.29 These domains are categorized into broader areas, including study design, qualitative methodology, sampling strategies, data collection methods, data analysis, study implications, and overall research rigor. Detailed findings from the quality appraisal are provided in the appendices (See Data quality appraisal Appendix 1–9).
Data Synthesis and Analysis
In this meta-synthesis study, we utilized the Noblit and Hare (1988) approach for data synthesis. This approach involved employing Reciprocal Translational Analysis (RTA), a process in which key findings from the studies are translated into overarching concepts or metaphors.30 Initially, each selected study was analyzed to extract essential information, including the study’s purpose, country of origin, design, methods, participant characteristics, and key findings (see Table 1).
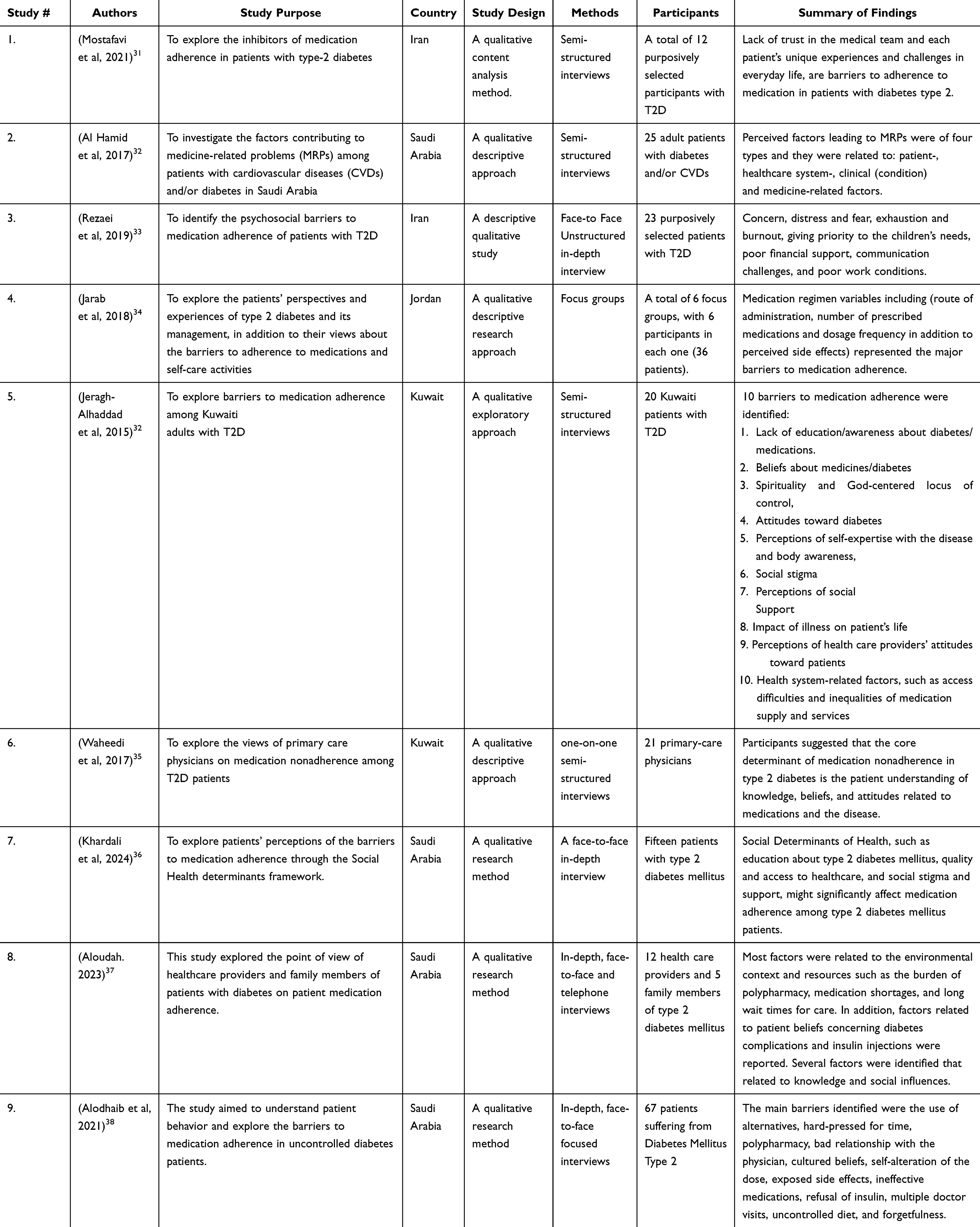 |
Table 1 Study Characteristics and Findings from Qualitative Research on Medication Adherence in Adults with T2D in the MENA Region |
Following this initial analysis, each study was read multiple times to conduct a thematic content analysis. Themes directly related to the meta-synthesis research question were identified, highlighted, and compiled. Similar themes across the studies were indexed and grouped to develop a comprehensive conceptual framework. This process, referred to as Lines-of-Argument (LOA) synthesis, involved integrating findings across studies to build a cohesive and comprehensive understanding of the research question, illustrating the whole through its constituent parts.39 The identified themes, supporting articles, and relevant quotations were then systematically organized into a final reciprocal translation table (see Table 2), providing a structured synthesis of the qualitative evidence.
 |
Table 2 Thematic Analysis of Factors Affecting Medication Adherence Among Adults with T2D in the MENA Region |
Ethical Approval and Consent to Participate
This study is a meta-analysis of previously published data and does not involve direct human participants. Therefore, ethical approval and informed consent were not required. All data included in this study were obtained from publicly available sources that had already received ethical approval from their respective institutions. The quality appraisal was conducted using the publicly available tool by Letts et al, which is expressly permitted for unrestricted use in research publications without requiring copyright permission from McMaster University or payment of fees. This aligns with the tool’s original publication terms.
Results
From an initial pool of 414 articles identified through database searches and other sources, such as open-access journals, 407 studies were deemed eligible for screening. The titles of articles were first reviewed to exclude quantitative studies, non-English publications, books, periodicals, reviews, meta-syntheses, and non-research articles. Following this initial screening, 362 articles were excluded, leaving 45 studies for full-text evaluation. These 45 articles underwent a detailed review against the inclusion criteria, leading to further refinement. Of these, 12 articles focused on Type 1 Diabetes or were unspecified, while 24 studies were conducted in countries outside the MENA region. Ultimately, nine studies from six different MENA region countries met the inclusion criteria and were incorporated into this meta-synthesis.31–38,40
The nine studies included in this metasynthesis were published between 2015 and 2024, and were conducted across different MENA geographical regions, providing a comprehensive understanding of barriers to medication adherence among patients with T2D. The studies included a total of 169 participants with T2D and 21 primary-care physicians. Two studies were conducted in Kuwait,35,40 four in Saudi Arabia,32,36–38 one in Jordan,34 and two in Iran.31,33 The primary methods utilized to identify factors influencing medication adherence were semi-structured interviews, in-depth interviews, and focus groups.
The findings of the studies identified various barriers to medication adherence. The studies conducted in Kuwait identified key barriers to medication adherence, including lack of education, beliefs about medications, social stigma, lack of access to healthcare services40 and found that patient understanding, knowledge, and beliefs about medication were major factors that contribute to nonadherence.35 In Jordan, the highlighted barriers that impede adherence were medication regimen factors like the route of administration, frequency of medication, and perceived side effects.34 The studies conducted in Iran identified concerns of care providers such as fear, distress, inadequate financial support, poor work conditions,33 and trust issues with healthcare providers as key challenges and primary barriers to medication adherence.31 The findings demonstrate that medication adherence among T2D patients is influenced by a complex interplay of social, psychological, economic, and systemic factors.
One of the studies conducted in Saudi Arabia found that the barriers to medication adherence were categorized into patient, healthcare system, clinical, and medicine-related factors.32 The other study identified barriers that could be fitted under the above categories and these include polypharmacy, medication shortages, long wait times, poor communication between providers and patients, social factors such as stigma and misconceptions about insulin, alongside lack of education about diabetes and its treatments.37 The social determinants of health such as education, healthcare access, social stigma, and support, were also emphasized as key drivers of nonadherence in another study conducted in Saudi Arabia.36 The use of alternative treatments, polypharmacy, poor relationships with physicians, and self-adjustment of doses were also reported.38 The other factors like side effects, ineffective medications, refusal of insulin, and forgetfulness were also key barriers, compounded by a lack of education on diabetes management. Understanding these barriers can inform the development of tailored interventions to address the challenges faced by patients with T2D.
The metasynthesis reciprocal translation process led to the identification of four newly derived main themes. These themes were categorized based on shared commonalities and their source of influence, incorporating both patient and healthcare provider perspectives. The four identified themes are as follows:
1. Personal factors and perceptions related to the disease and medications are fundamental to adherence.
2. HCPs’ attitudes and practices can improve adherence to medications.
3. Healthcare systems (HCSs) are a key factor in achieving optimal adherence.
4. Sociocultural and religious practices influence adherence in the MENA region.
Theme 1: Personal Factors and Perceptions Related to the Disease and Medications are Fundamental to Adherence
An individual’s knowledge, experiences, and perceptions play a significant role in determining adherence to T2D medications. Understanding these personal factors is essential for designing interventions that address individual needs and improve medication adherence. This theme was identified in all reviewed studies and encompasses factors linked to individual knowledge, perceptions, health beliefs, self-efficacy, health literacy, economic status, and psychological well-being. Based on the analysis, five subthemes were derived: perceptions of the disease, perceptions of medications, self-efficacy, cost of medications, and psychological factors such as forgetfulness, depression, powerlessness, and a fatalistic outlook.
Perceptions of the Disease
Perceptions about the disease were found to directly influence medication adherence decisions. These perceptions included factors such as the severity of the disease, acceptance, chronic nature, and personal experiences with diabetes complications. Some participants identified personal experiences of complications—whether their own or their relatives’—as facilitators of medication adherence. Conversely, viewing T2D as a chronic, incurable condition often led to nonadherence. One participant explained,
I know that it does progress, no matter what you do (p. 304).34
Many participants expressed difficulty in accepting their diagnosis, particularly when their understanding of T2D was incomplete. Reports from other studies confirmed that a lack of sufficient knowledge about T2D and its complications was common among participants.33,35,40 A primary care provider noted,Some patients still don’t understand what diabetes is, even after providing them with an explanation (p. 1415).35
Similarly, Aloudah (2023) highlighted that misconceptions and lack of understanding about the role of medications contributed to nonadherence, as some patients believed lifestyle changes alone could control their diabetes (p. 975).37 Furthermore, Alodhaib et al identified that patients’ cultural beliefs and misunderstanding of disease severity also impacted their willingness to adhere to medication, with some preferring alternative treatments (p. 6).38Perceptions of Medications
Beliefs about medications were identified as a significant barrier to adherence. Medication factors such as type, route of administration, frequency, polypharmacy, side effects, and misconceptions about medication benefits or risks impacted adherence levels. Many participants reported nonadherence due to concerns about side effects or beliefs about medication effects. One participant refused insulin, stating,
One of my relatives says that it totally destroys the pancreas (p. 6).32
Misconceptions, lack of knowledge, and misinformation about medications further compounded the issue. A female participant noted,It is no use taking medicines after the problem has come (p. 4).33
These findings suggest that lack of understanding and negative beliefs about medication efficacy or side effects can lead to missed doses. Similarly, Aloudah reported that some participants refused to use insulin due to fears of its harmful effects, with a participant stating,I am afraid it may hurt my kidneys (p. 6).37
Alodhaib et al also highlighted that these misunderstandings about the efficacy of medications led to delayed adherence and the use of alternatives. One participant said,I tried cinnamon in water, and I saw its benefit, thus reducing the dose (p. 6).38
These findings suggest that lack of understanding and negative beliefs about medication efficacy or side effects can lead to missed doses.Cost of Medications
The financial burden associated with medication costs emerged as another barrier to adherence. Considering the chronic nature of T2D, patients are often required to maintain lifelong medication regimens. However, access to free or affordable medications varies across healthcare systems in the MENA region. Many participants cited low income and the high cost of medications as barriers. One participant explained,
Continuous intake and regular purchase of medicine is not possible for me (p. 6).32
This financial strain contributed to nonadherence, highlighting the need to address the economic barriers that prevent consistent access to treatment. In Saudi Arabia, participants in a study by Alodhaib et al also emphasized financial difficulties as a key barrier to adherence, noting that some patients were unable to afford necessary medications (p. 6–7).38 Similarly, Aloudah (2023) identified high medication costs as a significant challenge for patients, especially those with low income, impacting their ability to purchase and consistently use medications (p. 7).37Forgetfulness and Psychological Status
Psychological factors such as forgetfulness, depression, feelings of powerlessness, and a fatalistic outlook also negatively influenced adherence levels. Participants reported feelings of emotional distress, low self-worth, and hopelessness. One participant expressed despair, stating,
It’s enough, let me die. If I have to die, it is my fate (p. 1417).35
The emotional and psychological barriers highlight a need for emotional and mental health support and strategies to improve coping mechanisms in T2D patients. Similarly, Alodhaib et al noted that psychosocial stressors like distress and the burden of managing diabetes led to self-neglect and avoidance of medication (p. 16).38Self-Efficacy
Self-efficacy was identified as a crucial subtheme influencing adherence. Self-efficacy refers to an individual’s confidence in their ability to manage their condition and adhere to treatment. Several participants expressed confidence in their ability to adjust their medication regimens independently. One participant explained that,
One should make his own modifications in addition to that of the doctor. (p. 6).33
Similarly, a Jordanian participant stated,It’s up to yourself if you take your medication or not (p. 303).34
These findings underscore the importance of self-confidence, individual responsibility, and a sense of control over one’s condition and the critical role they can play towards improving medication adherence. Similarly, Alodhaib et al noted that patients with uncontrolled diabetes often engaged in self-adjustment of doses, reflecting a belief in their ability to control their treatment (p. 16).38Theme 2: HCPs’ Attitudes and Practices Can Improve Adherence to Medications
This theme explores how healthcare providers (HCPs) can act as either facilitators or barriers to medication adherence. HCPs are strategically positioned to promote adherence interventions by monitoring patient health outcomes and knowledge levels about treatments and other unique treatment needs. This is especially crucial because several provider-related factors contribute to low adherence levels, as reported by both HCPs and individuals with T2D. The five subthemes derived from this theme are trust versus mistrust of HCPs, ignoring patient perspectives, one patient being managed by multiple care providers, the importance of adequate communication and patient education, and language barriers.
Trust versus Mistrust of HCPs
Participants highlighted varied experiences with healthcare providers. Although most patients reported full trust in their providers, others expressed mistrust in providers’ medical advice or medication prescriptions. For instance, a participant explained:
When I [my sugar level] am at 70 (mg/dl), the doctors continue to prescribe the same dosage [two tablets] … But I plan to decrease it [the dose]. (p. 5).31
These trust issues can directly influence patients’ adherence to their medication regimens. Additionally, the lack of support from healthcare providers was identified as a significant barrier to medication adherence.37 Patients felt neglected by their providers, which led to decreased motivation to follow treatment recommendations (p. 975–977). Furthermore, Alodhaib et al emphasized that a poor relationship with healthcare providers and lack of trust in medical advice contributed to self-adjustment of medication doses among patients (p. 6–7).38Ignoring Patient Perspective
This subtheme refers to situations in which providers fail to consider or acknowledge patients’ perspectives, and this can undermine adherence. This is reflected through actions and behaviors of the HCPs that are paternalistic, lack of compassion, or inattentiveness. One participant shared:
When I try to discuss something about my medications, he just doesn’t care or pay attention. (p. 1497).40
Such behaviors can erode trust and negatively impact adherence levels.Multiple Care Providers
Participants identified that having multiple physicians or frequent changes in providers leads to discontinuity of care, which directly affects adherence by disrupting consistent treatment regimens.40 Similarly, in Aloudah (2023), patients reported that seeing multiple doctors, resulting in confusion and lack of continuity in their care, which negatively impacted their medication adherence (p. 7).37 Alodhaib et al also highlighted that visit to different healthcare providers created inconsistent treatment advice and patient confusion, further complicating medication adherence (p. 7–8).38
Importance of Education
Both patients and HCPs emphasized the need for improved medication education. Many HCPs acknowledged their time constraints in providing comprehensive patient education. One healthcare provider expressed: “I need to educate more.” (p. 1417).35 Additionally, patients expressed a desire for more information about their medications and treatment regimens.32,34 Alodhaib et al (2021, p. 16) also noted that patients with uncontrolled diabetes expressed frustration with a lack of education regarding medication use and its importance.38 Furthermore, Aloudah (2023, p. 973–982) highlighted that patients’ adherence was often hindered by their poor understanding of how medications interact with their condition, signaling the need for better educational support for both patients and healthcare providers.37
Communication and Language Barriers
Communication and language difficulties were reported as significant barriers in the MENA region, with several participants noting challenges in understanding their medication or treatment due to language differences with their HCPs. For example, patients reported that language barriers hindered their ability to comprehend the medications prescribed to them.35–38
Theme 3: HCS is a Key Factor for Optimal Adherence
This theme highlights how the quality and level of development of the healthcare system (HCS) can improve adherence to T2D medication regimens. The studies reviewed suggest that the effectiveness of healthcare systems in the MENA region significantly influences medication adherence, with notable variation across countries. While Gulf Cooperation Council (GCC) countries feature well-developed healthcare systems, other nations such as Syria, Yemen, and Egypt struggle with underdeveloped systems, largely due to political instability and economic challenges. Three subthemes were identified as being key influencers within healthcare systems and these include availability and accessibility of medications, provision of diabetes education, and trust and satisfaction with HCSs.
Availability and Accessibility of Medications
Availability and accessibility of medications was a common factor identified by multiple studies.31,32,34,35,40 Participants expressed challenges when medications were unavailable or were not offered free of charge. These issues caused some individuals to reduce their doses or switch to alternative medications. One participant explained:
The smaller one was not available for 4 months. So, during that time it has to be bought. Sometimes there are cases when out of fear that I wouldn’t completely get the medicine I would decrease the dose from 4 to 2. So, I make it 1 in the morning and evening. (p. 5)32
Additionally, Alodhaib et al found that medication availability was a challenge, with patients reducing doses or using alternatives like traditional remedies (p. 6–7).38 Aloudah (2023) reported that medication shortages and long wait times at healthcare facilities led patients to seek medications from other sources or skip doses (p. 7).37
Provision of Diabetes Education
Quality and accessibility of diabetes education were identified as crucial for improving medication adherence.32–35,37,38 A lack of adequate time for education and inconsistent communication between healthcare providers and patients were barriers. For instance, participants from Saudi Arabia reported the following:
They write down my medicine on a piece of paper to get them but they never explained anything. The doctor is always busy and thinks that we understand his writing. (p. 5)32
Trust and Satisfaction with HCSs
Trust in healthcare systems and satisfaction with their services were identified as additional barriers to medication adherence. The lack of trust was especially prevalent in governmental healthcare services.37,38 Participants expressed dissatisfaction with the quality and reliability of services, particularly when comparing private and governmental health sectors. One participant shared:
Medications at the Ministry of Health are not that effective (p. 1489).40
These findings emphasize that healthcare system factors such as availability of medications, the quality of diabetes education, and trust in healthcare providers significantly affect adherence behaviors among patients with T2D in the MENA region.Theme 4: Sociocultural and Religious Practices Affect Adherence in the MENA Region
This theme addresses the common cultural and religious practices that can significantly influence medication adherence among patients with type 2 diabetes in the MENA region. The region is characterized by diverse religious practices and cultural norms. While the majority of its population are Muslims, other faiths such as Christianity and Judaism are also practiced. Most individuals in this region speak Arabic and share common cultural traditions. Four subthemes emerged under this main theme:
God’s Centered Locus of Control
Participants reported that their disease and its management are deeply connected to faith. Some individuals expressed that their condition and healing are determined by Allah’s will. One participant stated:
Of course I accept it (his diabetes). Because Allah gave it to me. My faith makes it easier to deal with it (p. 97).40
Additionally, religious practices such as fasting during Ramadan or participating in Hajj and Umrah impacted adherence to medications. One Saudi participant explained:I never take it (medicine) during Hajj or Umrah because walking during Hajj and Umrah relieves me (p. 7).32
Subtheme Summary: Religious healing and cultural barriers related to beliefs in divine influence affect adherence decisions.Social Effect
Participants showed varied responses regarding the social impact on adherence. Social support was a major facilitator, as it provided moral encouragement, reminders to take medications, assistance in obtaining medicines, and coverage of work responsibilities during hypoglycemic episodes. Mostafavi et al, described this support:
Social support in the form of moral support of adherent behavior, reminding to take medications, availing medications (in kind or providing funds), and covering work to avoid falls because of hypoglycemia. (p. 6)31
Conversely, social factors had a negative impact due to rumors, myths, and misinformation spreading through social networks. A physician reflected:
They tell them that this medicine affects the kidney and that they should not take it. They listen to what their friend says (p. 1416).35
Subtheme Summary: Social support improves medication adherence, while rumors and stigma can impair adherence. Fear of social stigma and negative social perceptions also emerged as barriers.Complementary Treatments and Religious Practices as Alternative Therapies
Several participants believed that diet and exercise alone could manage their condition. Alternative therapies, such as homeopathy, ayurvedic medicine, and herbal remedies, were also frequently reported by participants as alternatives to conventional treatments. These practices were often rooted in cultural beliefs and religious views. One participant explained: “They believe other remedies can substitute for proven medications”.33,37 Subtheme Summary: Complementary treatments and religious or cultural beliefs lead to the use of alternative therapies rather than conventional medication. This reliance affects medication adherence patterns.
Discussion
This qualitative metasynthesis provides a comprehensive and detailed exploration of the factors influencing medication adherence among adults with T2D in the MENA region. The identified factors, as reported by both patients and healthcare providers, can be categorized into four main themes: personal-related factors, healthcare provider-related factors, healthcare system-related factors, and social and religious factors.
This metasynthesis identifies personal factors, such as knowledge deficits and health beliefs about disease and medication, which align with findings from previous studies.41–45 Similarly, the healthcare provider and healthcare system -related factors identified by our review are consistent with those reported in developed countries like Canada, the USA, Europe, and Australia.46,47 However, the social and religious factors are unique to the MENA region and require further investigation using rigorous methods. The social and religious factors such as faith-based beliefs, cultural practices, and social support systems seem to have a strong influence on medication adherence in the MENA region. While these social and religious factors are context-specific, the other findings related to personal, HCP, and HCS-related factors are transferable and can inform interventions in other settings and populations with careful contextual adaptation.
By synthesizing the qualitative literature, several key gaps in knowledge have been identified. Further qualitative studies are needed to explore the impact of cultural and religious practices on medication adherence in the MENA region. In this context, family involvement in care planning is particularly important, as many elderly individuals in the MENA region are cared for by family members. Understanding the role of family caregiving in adherence behaviors could provide critical insights.
Additionally, social factors like social stigma (particularly among insulin users) and social effects from communal gatherings significantly influence adherence but have only been explored minimally in the MENA region. For instance, Brazeau et al and Gu et al highlight these influences, but evidence in the MENA region remains limited. Future research should determine whether these factors are widespread or limited to specific countries and design culturally sensitive, patient-centered strategies to improve adherence.48,49
Moreover, none of the reviewed studies applied a theoretical framework to guide research. Theories such as the Theory of Planned Behavior, Social Cognitive Theory, or the Health Belief Model could increase the precision of interventions and provide structure for research design, data collection, analysis, and offer insights into adherence behaviors.50 Future studies should adopt such theories to ensure a systematic understanding of medication adherence and effectiveness of evidence-based interventions.
Strengths and Limitations
This metasynthesis provides a comprehensive and nuanced understanding of the factors influencing medication adherence among adults with T2D in the MENA region. By integrating findings from multiple qualitative studies, it offers rich insights into common barriers and facilitators to adherence from the patient and healthcare provider perspectives. The study identified four main themes of personal-related factors, healthcare provider-related factors, healthcare system-related factors, and social and religious factors. The main themes provide a framework for understanding adherence patterns. Additionally, the metasynthesis highlights the role of cultural and contextual influences, and this can be used to guide future interventions tailored to diverse patient populations.
This metasynthesis has several limitations that should be considered when interpreting its findings. The MENA region encompasses a variety of healthcare systems that differ in terms of healthcare services availability, accessibility, and development. Variations in health expenditures, the availability of medications, and the level of healthcare system development may influence medication adherence. These systemic disparities highlight the complexity of the healthcare landscape in the MENA region and suggest possible differences in adherence patterns due to contextual factors. Additionally, the studies included in this metasynthesis were conducted in only five MENA countries, despite the fact that the region consists of 23 countries. This limited geographic representation restricts the generalizability of the findings, as the experiences and challenges faced by patients and providers in other unrepresented MENA countries may differ. The metasynthesis included only studies published in articles written in English and could have left out those written in Arabic and other languages used in the MENA region. Future studies should systematically compare income/healthcare systems across MENA subregions. Therefore, the findings offer valuable insights into adherence patterns, but caution is needed when applying these results broadly across the entire MENA region.
Conclusion
This qualitative meta-synthesis identifies a complex interplay of personal, cultural, economic, and systemic factors influencing medication adherence among adults with Type 2 Diabetes (T2D) in the MENA region. Key barriers include psychological distress, limited healthcare access, social stigma, and the understudied role of religious and cultural practices, such as traditional medicine use. The findings highlight an urgent need for culturally tailored interventions, including community health worker (CHW)-led education programs and provider training in cultural competency. Clinically, simplifying medication regimens and addressing herb-drug interactions could significantly improve adherence. Future research should prioritize longitudinal studies to evaluate the effectiveness of context-specific strategies, particularly those integrating religious and community leaders, to address the region’s unique socio-cultural dynamics and sustainably enhance health outcomes.
Ethical Approval and Consent to Participate
This study does not require any ethical approval. However, the quality appraisal was conducted using the publicly available tool by Letts et al, which is expressly permitted for unrestricted use in research publications without requiring copyright permission from McMaster University or payment of fees. This aligns with the tool’s original publication terms.
Acknowledgment
The study acknowledges all the cited authors in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was required to conduct the study.
Disclosure
The authors declare that they have no competing interest.
References
1. International Diabetes Federation. IDF Diabetes Atlas. 8th ed. International Diabetes Federation. 2017. Available from: https://diabetesatlas.org/upload/resources/previous/files/8/IDF_DA_8e-EN-final.pdf.
2. Li S, Wang J, Zhang B, Li X, Liu Y. Diabetes mellitus and cause-specific mortality: a population-based study. Diabetes Metab J. 2019;43(3):319–341. doi:10.4093/dmj.2018.0060
3. Centers for Disease Control and Prevention. New CDC report: more than 100 million Americans have diabetes or prediabetes. 2017. Available from: https://archive.cdc.gov/www_cdc_gov/media/releases/2017/p0718-diabetes-report.html.
4. Al-Worafi YM. Epidemiology and burden of diabetes mellitus in developing countries. In: Handbook of Medical and Health Sciences in Developing Countries: Education, Practice, and Research. Cham, Switzerland: Springer International Publishing; 2023:1–27.
5. Koliaki C, Dalamaga M, Liatis S. Update on the obesity epidemic: after the sudden rise, is the upward trajectory beginning to flatten? Curr Obes Rep. 2023;12(4):514–527. doi:10.1007/s13679-023-00527-y
6. Mercado E. Level of awareness, adherence to diet, self-monitoring, and medication regimen among diabetic patients: a basis for improving diabetes specialty clinic services. J Health Med Inform. 2019;10(2).
7. World Health Organization. Adherence to Long-Term Therapies: evidence for Action. World Health Organization; 2003. Available from: https://iris.who.int/handle/10665/42682.
8. Singh P. Medication adherence: adjunct to patient outcomes. J Pract Cardiovasc Sci. 2017;3(1):8–10. doi:10.4103/jpcs.jpcs_10_17
9. Shalaeva EV, Bano A, Kasimov U, Janabaev B, Laimer M, Saner H. Impact of persistent medication adherence and compliance with lifestyle recommendations on major cardiovascular events and one-year mortality in patients with type 2 diabetes and advanced stages of atherosclerosis: results from a prospective cohort study. Glob Heart. 2023;18(1):61. doi:10.5334/gh.1273
10. Hassan Y, Al-Temimi AA, Ramli R, Saad MFM, Aziz NA. Difficulties facing the patients and extra burden for healthcare providers by non-adherence to the medications: a comprehensive review. Indian J Pharm Educ Res. 2019;53(4 Suppl):s487–s499. doi:10.5530/ijper.53.4s.143
11. Hadia R, Sajan C, Saggu V, et al. Promoting medication adherence: strategies for patient engagement and education. Mod Res Pharm Sci. 2024;99:134.
12. Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
13. Fernandez-Lazaro CI, Adams DP, Fernandez-Lazaro D, et al. Medication adherence and barriers among low-income, uninsured patients with multiple chronic conditions. Res Social Adm Pharm. 2019;15(6):744–753. doi:10.1016/j.sapharm.2018.09.006
14. Ghassab-Abdollahi N, Nadrian H, Shaseb E, et al. Medication adherence, medication beliefs, and social support among illiterate and low-literate community-dwelling older adults with polypharmacy. Fam Med Prim Care Rev. 2023;25(4).
15. Guilcher SJT, Everall AC, Patel T, et al. Medication adherence for persons with spinal cord injury and dysfunction from the perspectives of healthcare providers: a qualitative study. J Spinal Cord Med. 2019;42(sup1):215–225. doi:10.1080/10790268.2019.1637644
16. Guan M, Li R, Wang B, et al. Healthcare professionals’ perspectives on the challenges with managing polycystic ovary syndrome: a systematic review and meta-synthesis. Patient Educ Couns. 2024;123:108197. doi:10.1016/j.pec.2024.108197
17. Hall GL, Heath M. Poor medication adherence in African Americans is a matter of trust. J Racial Ethn Health Disparities. 2021;8(4):927–942. doi:10.1007/s40615-020-00850-3
18. Adegoke BO, Odugbose T, Adeyemi C. Assessing the effectiveness of health informatics tools in improving patient-centered care: a critical review. Int J Chem Pharm Res Updates. 2024;2(2):1–11. doi:10.53430/ijcpru.2024.2.2.0022
19. Jaam M, Ibrahim MIM, Kheir N, Awaisu A. Factors associated with medication adherence among patients with diabetes in the Middle East and North Africa region: a systematic mixed studies review. Diabetes Res Clin Pract. 2017;129:1–15. doi:10.1016/j.diabres.2017.04.015
20. McGovern A, Tippu Z, Hinton W, et al. Systematic review of adherence rates by medication class in type 2 diabetes: a study protocol. BMJ Open. 2016;6(2):e010469. doi:10.1136/bmjopen-2015-010469
21. Al-Noumani H, Al-Harrasi M, Jose J, Al-Naamani Z, Panchatcharam SM. Medication adherence and patients’ characteristics in chronic diseases: a national multi-center study. Clin Nurs Res. 2022;31(3):426–434. doi:10.1177/10547738211033754
22. Dorcélus L, Bernard J Jr, Georgery C, et al. Factors associated with antiretroviral therapy adherence among people living with HIV in Haiti: a cross-sectional study. AIDS Res Ther. 2021;18(1):81. doi:10.1186/s12981-021-00405-4
23. Jolles MP, Richmond J, Thomas KC. Minority patient preferences, barriers, and facilitators for shared decision-making with health care providers in the USA: a systematic review. Patient Edu Counseling. 2019;102(7):1251–1262. doi:10.1016/j.pec.2019.02.003
24. Scarton L, Nelson T, Yao Y, et al. Association of medication adherence with HbA1c control among American Indian adults with type 2 diabetes using tribal health services. Diabetes Care. 2023;46(6):1245–1251. doi:10.2337/dc22-1885
25. Bobga Billa JK. Challenges and opportunities in managing Type 2 Diabetes Mellitus in Sub-Saharan Africa: the cases of Nigeria and South Africa. [Doctoral dissertation]. Hochschule für Angewandte Wissenschaften Hamburg; 2023.
26. Fallatah AH. Exploring Type Two Diabetes Mellitus in the Kingdom of Saudi Arabia: Studying the Socio-economic Environment. [Doctoral dissertation]. University of Southampton; 2020.
27. Oates GR, Juarez LD, Hansen B, Kiefe CI, Shikany JM. Social risk factors for medication nonadherence: findings from the CARDIA study. Am J Health Behav. 2020;44(2):232–243. doi:10.5993/AJHB.44.2.10
28. Shaheen N, Shaheen A, Ramadan A, et al. Appraising systematic reviews: a comprehensive guide to ensuring validity and reliability. Front Res Metrics Anal. 2023;8:1268045. doi:10.3389/frma.2023.1268045
29. Letts L, Wilkins S, Law M, et al. Guidelines for critical review form: qualitative studies (Version 2.0). McMaster University Occupational Therapy Evidence-Based Practice Research Group. 2007;1–12.
30. Noblit GW. Meta-Ethnography: Synthesizing Qualitative Studies. Stage Publication; 1988.
31. Mostafavi F, Alavijeh FZ, Salahshouri A, Mahaki B. The psychosocial barriers to medication adherence of patients with type 2 diabetes: a qualitative study. BioPsychoSocial Med. 2021;15:1–11. doi:10.1186/s13030-020-00202-x
32. Al Hamid AM, Ghaleb M, Aljadhey H, Aslanpour Z. Factors contributing to medicine-related problems in adult patients with diabetes and/or cardiovascular diseases in Saudi Arabia: a qualitative study. BMJ Open. 2017;7(11):e017664. doi:10.1136/bmjopen-2017-017664
33. Rezaei M, Valiee S, Tahan M, Ebtekar F, Ghanei Gheshlagh R. Barriers of medication adherence in patients with type-2 diabetes: a pilot qualitative study. Diabetes Metab Syndr Obes. 2019;12:589–599. doi:10.2147/DMSO.S197159
34. Jarab AS, Mukattash TL, Al-Azayzih A, Khdour M. A focus group study of patient’s perspective and experiences of type 2 diabetes and its management in Jordan. Saudi Pharm J. 2018;26(3):301–305. doi:10.1016/j.jsps.2018.01.013
35. Waheedi M, Jeragh-Alhaddad FB, Awad AI, Enlund H. “Patients’ understanding is the problem”: physicians’ views of nonadherence among Arabs with type 2 diabetes. Patient Prefer Adher. 2017;11:1413–1421. doi:10.2147/PPA.S138468
36. Khardali A, Aladwani A, Alzahrani F, et al. Exploring patients’ perspective of barriers to diabetic medication adherence in Jazan, Saudi Arabia, using the social determinants of health model. SAGE Open Med. 2024;12:20503121241271820. doi:10.1177/20503121241271820
37. Aloudah NM. A qualitative study on the perception of medication adherence by the social circles of patients with type 2 diabetes. Patient Prefer Adher. 2023;17:973–982. doi:10.2147/PPA.S404092
38. Alodhaib G, Alhusaynan I, Mirza A, Almogbel Y. Qualitative exploration of barriers to medication adherence among patients with uncontrolled diabetes in Saudi Arabia. Pharmacy. 2021;9(1):16. doi:10.3390/pharmacy9010016
39. Barnett-Page E, Thomas J. Methods for the synthesis of qualitative research: a critical review. BMC Med Res Methodol. 2009;9:59. doi:10.1186/1471-2288-9-59
40. Jeragh-Alhaddad FB, Waheedi M, Barber ND, Brock TP. Barriers to medication taking among Kuwaiti patients with type 2 diabetes: a qualitative study. Patient Prefer Adher. 2015;9:1491–1503. doi:10.2147/PPA.S86719
41. Lo DF, Gawash A, Shah KP, et al. Voices of wisdom: geriatric interviews on self-management of type 2 diabetes in the United States—A systematic review and metasynthesis. J Diabetes Res. 2024;2024(1):2673742. doi:10.1155/2024/2673742
42. Jackson MG. African Americans reasons for noncompliance with effective diabetes treatment plan: a qualitative study in chronic care [dissertation]. Colorado Springs, CO: Colorado Technical University; 2022.
43. Gupta SK, Lakshmi PVM, Chakrapani V, Rastogi A, Kaur M. Understanding the diabetes self-care behaviour in rural areas: perspective of patients with type 2 diabetes mellitus and healthcare professionals. PLoS One. 2024;19(2):e0297132. doi:10.1371/journal.pone.0297132
44. Yoon S, Kwan YH, Yap WL, et al. Factors influencing medication adherence in multi-ethnic Asian patients with chronic diseases in Singapore: a qualitative study. Front Pharmacol. 2023;14:1124297. doi:10.3389/fphar.2023.1124297
45. Al Salmi N. Predictors of Medication Adherence Among Omani Adults With Type 2 Diabetes [dissertation]. University of Colorado Denver, Anschutz Medical Campus; 2022.
46. Ong SE, Koh JJK, Toh SAES, et al. Assessing the influence of health systems on type 2 diabetes mellitus awareness, treatment, adherence, and control: a systematic review. PLoS One. 2018;13(3):e0195086. doi:10.1371/journal.pone.0195086
47. Simacek K, Curran C, Fenici P, Garcia-Sanchez R. Patient perceptions of their glycemic control and its influence on type 2 diabetes outcomes: an international survey of online communities. Patient Prefer Adher. 2019;13:295–307. doi:10.2147/PPA.S186801
48. Brazeau AS, Nakhla M, Wright M, et al. Stigma and its impact on glucose control among youth with diabetes: protocol for a Canada-wide study. JMIR Res Protoc. 2016;5(4):e242. doi:10.2196/resprot.6629
49. Gu L, Wu S, Zhao S, et al. Association of social support and medication adherence in Chinese patients with type 2 diabetes mellitus. Int J Environ Res Public Health. 2017;14(12):1522. doi:10.3390/ijerph14121522
50. Sirur R, Richardson J, Wishart L, Hanna S. The role of theory in increasing adherence to prescribed practice. Physiother Can. 2009;61(2):68–77. doi:10.3138/physio.61.2.68
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.