Back to Journals » Patient Preference and Adherence » Volume 16
Medication Adherence Among Patients with Multimorbidity in the United Arab Emirates
Authors Allaham KK, Feyasa MB, Govender RD, Musa AMA ![]() , AlKaabi AJ, ElBarazi I
, AlKaabi AJ, ElBarazi I ![]() , AlSheryani SD, Al Falasi RJ, Khan MAB
, AlSheryani SD, Al Falasi RJ, Khan MAB ![]()
Received 26 December 2021
Accepted for publication 11 March 2022
Published 6 May 2022 Volume 2022:16 Pages 1187—1200
DOI https://doi.org/10.2147/PPA.S355891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Kholoud K Allaham,1 Merga Belina Feyasa,2 Romona Devi Govender,1 Anas Mahmoud Abbas Musa,3 Ahmed Juma AlKaabi,1 Iffat ElBarazi,4 Shamma Dahi AlSheryani,1,5 Reem Juma Al Falasi,1,5 Moien AB Khan1,5,6
1Department of Family Medicine, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates; 2Division of Epidemiology and Biostatistics, Department of Global Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch, South Africa; 3Department of Cardiology, Rashid Hospital, Dubai Health Authority, Dubai, United Arab Emirates; 4Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates; 5Ambulatory Healthcare Services, Abu Dhabi, United Arab Emirates; 6Primary Care, NHS Northwest London, London, TW3 3EB, UK
Correspondence: Moien AB Khan, Department of Family Medicine, College of Medicine and Health Sciences, United Arab Emirates University, P.O. Box 17666, Al Ain, United Arab Emirates, Tel +971 3 713 7544, Fax +971 3 767 2022, Email [email protected]
Background: Multimorbidity, defined as having two or more chronic diseases, has a major impact on public health and Sustainable Development Goals (SDG). This study aims to assess the prevalence of medication adherence and associated factors among patients with multimorbidity.
Methods: A questionnaire-based, cross-sectional survey was conducted by a trained interviewer across patients with multimorbidity attending outpatient clinics in two tertiary referral hospitals in the United Arab Emirates (UAE). Demographic and social variables and the outcome (self-reported adherence to long-term medication) were measured using the General Medication Adherence Scale (GMAS). Multiple logistic regression was used to assess medication adherence and associated factors.
Results: From a total of 630 participants included in this study, the estimated prevalence of high medication adherence is 78.57% (± 1.63478) with a 95% confidence interval (CI) [75.19, 81.61]. The odds of high medication adherence increased with age. The odds of high medication adherence for patients aged 66 years and older than those aged 19– 35 years is adjusted odds ratio (AOR) = 3.880, with a 95% CI [1.124, 13.390]. Patients with income more than 50,000 had the odds, AOR = 5.169 with a 95% CI [1.282, 20.843], compared to those earning less than 10,000 Dirhams (AED). Patients aged 36– 65 with health insurance coverage had higher medication adherence than groups on the other end. The number of current medications is significantly (p-value = 0.027) associated with high medication adherence with the odds of high medication adherence, AOR = 4.529 with a 95% CI [1.184, 17.326], the highest for those currently taking four medications.
Conclusion: This study highlights younger population having multimorbidity in the context of an increasing life expectancy and suboptimal therapeutic outcomes. Furthermore, the study highlights multimorbidity is associated with low medication adherence and out-of-pocket payment, and non-availability of insurance is a major hindrance to medication adherence.
Keywords: multimorbidity, medication adherence, United Arab Emirates, sustainable development goals, global burden of disease
Introduction
Multimorbidity refers to the co-occurrence of two or more chronic conditions in an individual.1 Recent systematic reviews suggest that the prevalence of multimorbidity is in the range of 23–33%, and prevalence further increases with age, estimated to be 75% or higher at the age of 70 years. As average life expectancy rises, the numbers are bound to substantially increase by 2035.2–4 Those 65 years or older are expected to live with four or more chronic diseases by 2035.5 Patients with multimorbidity are associated with increased healthcare and social services utilization,6 increased healthcare costs,7 poorer clinical outcomes,8 and increased disability and mortality.3 Thus, multimorbidity has been highlighted as a significant challenge to both the patients and healthcare providers.
Patients with multimorbidity require complex clinical care, including treatment with multiple medications (polypharmacy).9–11 Medication adherence, defined as patients taking their medications as prescribed, is essential to achieve optimal disease control.12 Non-adherence to medications includes poor initiation, implementation, and non-persistence to continue with prescribed treatment.13,14 Recent evidence-based guidelines have emphasized that medication adherence is the cornerstone for managing and preventing long-term complications in multimorbidity patients.15 Research has documented that low adherence to medications is multifactorial and multidimensional related to patients, physicians, and healthcare systems.10,11 Furthermore, the current pandemic has had a negative effect and several constrains on the patients, public and the healthcare system.16–19 Though the expenses are due to increased medication costs, there is evidence that there is a reduction in overall health care with medication adherence costs.20 Evidence from several studies suggests that higher adherence with medications was associated with decreased complications.12,21 Furthermore, evidence suggests a 26% improvement in health outcomes comparing patients between high and low medication adherence.22 In another study, 38% decreased cardiovascular disease events compared with lower medication adherence.21 In contrast, non-adherence to medications is associated with higher mortality. In the United States (US) alone, medication non-adherence amounts to an excess of $100 billion (about $310 per person in the US) in annual healthcare expenditure.23
Rapid economic and demographic transitions due to the discovery of oil have led the United Arab Emirates (UAE) to transform into a wealthy country adopting western lifestyles.24 UAE has a younger population, witnessed rapid industrial growth and modernizations, which have contributed to an increase in trends in the prevalence of non-communicable diseases (NCD) such as diabetes, hypertension, obesity, and cardiovascular disease.18,19 World Health Organization estimates that the burden of chronic diseases increases rapidly in the UAE, with one in four deaths contributing to cardiovascular disease.24 Furthermore, one in six people in the United Arab Emirates has Diabetes.25 Literature evidence suggests a higher rate of non-compliance with medications in patients with Diabetes26 and Hypertension.27 Medication compliance issues could lead to increased morbidity, mortality, and economic burden through hospitalization and increased costs due to chronic disease complications.
In 2015, United Nations member states adopted 17 Sustainable Development Goals (SDGs) and 169 target indicators as a global development agenda to achieve by 2030.28 Reducing the burden due to multimorbidity (NCD) is a critical global health and well-being agenda.29 One of the key SDG –3 targets is to reduce premature deaths due to NCDs by one-third by 2030. Furthermore, multimorbidity is associated with employment losses and poverty, creating inequity both within and across the globe. Several studies have shown improved survival and decreased morbidity in patients with multimorbidity.30,31 However, it is evident that poor adherence to medications can further increase the mortality and morbidity associated with multimorbidity.32 Hence, multimorbidity associated with poor medication adherence has a significant negative impact on health, economic, and social SDGs that contribute to a significant burden on the person, public, and society.
As the prevalence of multimorbidity rises, reflecting the unhealthy lifestyles and ageing in the UAE, patients with multimorbidity constitute a significant challenge to the healthcare system. Hence, there is a need to measure the relationship between multimorbidity and medication adherence. However, there is a paucity of literature regarding multimorbidity and medication adherence in the UAE. The study’s primary objective is to quantify medication adherence among patients with multimorbidity. Furthermore, we aim to evaluate the factors associated with multimorbidity and medication adherence in the United Arab Emirates population.
Methods
Study Design and Participants
A cross-sectional survey design was used. Only people with more than one chronic disease and who consented to participate completed the questionnaire through a structured interview by a trained clinical researcher. Participants were recruited from visitors attending outpatient clinics in two hospitals, namely, Dubai and Rashid Hospital. Dubai and Rashid hospital are one of the major tertiary referral hospitals in the UAE. Patients from different geographical locations from the UAE visit these two hospitals to manage complex chronic diseases. After piloting the questionnaire on 36 participants the survey questionnaire was reviewed and adjusted for minor grammatical changes. Data collection took place between February 2021 – September 2021.
Sample Size
Sample size was calculated to be 563 with a 5% level of significance and 80% power to detect a minimum of 5% difference. To substantiate missing data and other human factors, we have added 10% contingency in the collection of data resulting in 620 patients, and fortunately, we were able to recruit 630 patients.
Inclusion and Exclusion Criteria
All patients having two or more diseases and on medications, aged ≥ 18 years, and attending a hospital-based outpatient service in Dubai Hospital and Rashid Hospital, Dubai, during February 2021 – September 2021 were included in the study. Patients with multimorbidity that limited their communications were excluded.
Ethical Approval
Ethical approval was obtained before the commencement of the study from the Dubai Scientific research ethics committee, United Arab Emirates (Approval Number DSREC-01/2021_20). Study was conducted anonymously in accordance with Declaration of Helsinki guidelines.
Measurements
The survey tool comprises the following sections:
- A Demographic section that included age, gender, height, weight, employment status, and ethnicity,
- General Medication Adherence Scale (GMAS) which is an 11-item questionnaire that provides a convenient and affordable way of tracking compliance by an indirect approach. The GMAS adopted a combination of subjective and objective measures. The 11 items are subdivided into (1) Non–adherence due to patient behavior (Five items) (2) Pill burden and additional disease (four items), and (3) payment-related non–adherence (two items). We used the GMAS survey because of its studied results, which yielded values related to validation aspects. The GMAS instrument has been validated in several studies with different chronic diseases with good psychometric properties.33–36
Each item in the General Medication Adherence Scale (GMAS) has four Likert scores, and the maximum score for adherence that could be achieved is 33, with a minimum score of 0 and a maximum score of 3. The sum of all items yields a final score used to form the two categories of the outcome variable, medication adherence, as “Low adherence” if GMAS score ≤ 26 and “High Adherence” if GMAS score ≥ 27.37 In this study, GMAS had a good reliability, Cronbach’s alpha (α = 0.8492).
3. The Self‐Administered Co-Questionnaire (SCQ) is a short, detailed survey that includes 12 medical conditions to determine a patient’s comorbidities.38 This survey tool provides an alternative that constitutes an alternative method for comorbidity measurements to traditional methods that are often based mainly on information from the health record or administrative details. This questionnaire provides an advantage over other methods of comorbidity assessments by avoiding drawbacks such as incomplete medical records and low reporting consistency. The SCQ is a reproducible comorbidity measure with a meaningful relationship with a traditional hospital record-based comorbidity measure.38,39
To reduce risk of bias during the interview, study was not conducted during the month of Ramadan as during the month, people who fast from dawn to dusk, take the medications thrice and there is a chance to miss or change in routine to take the pills causing a bias in our study. Clinical researcher is a medically trained postgraduate doctor who is bilingual in Arabic and English. The survey questions were both available in English and Arabic to reduce any bias.
Data Analysis
Descriptive statistics including mean and standard deviation (SD) for quantitative variables and percentages for categorical variables were used. We performed multiple logistic regression to evaluate factors associated with medication adherence (Table 1). Covariates were included in the multiple logistic regression model based on the literature and knowledge in the area. These analyses were performed using Stata software, version 16.0 (StataCorp LLC, College Station, TX)40 with a two-tailed level of statistical significance set at p-value ≤ 0.05.
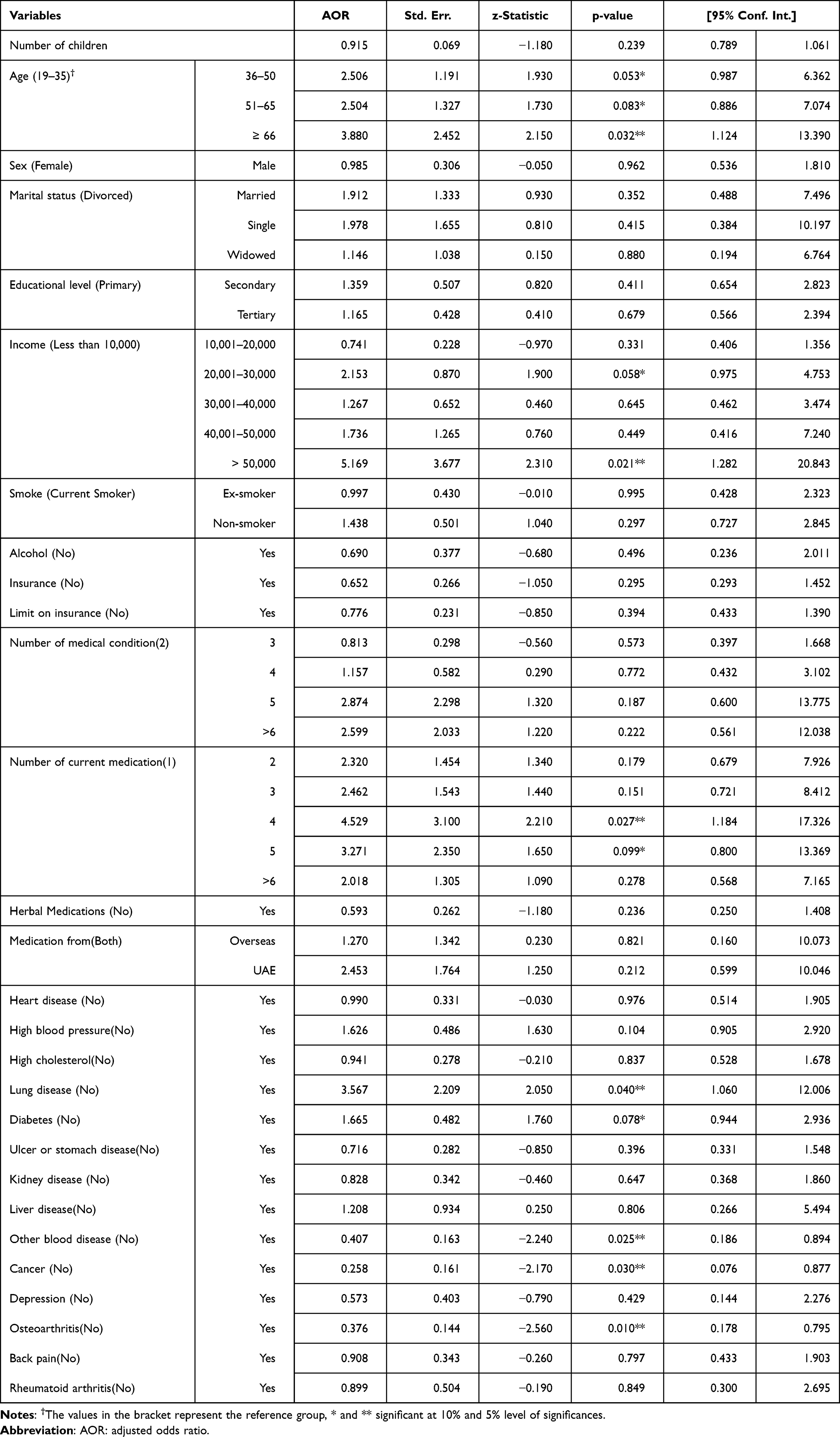 |
Table 1 Logistic Regression Examining Factors Associated with Medication Adherence of Patients with Morbidity |
Results
Adherence to Medication
A total of 630 participants were included in this study. The prevalence of high medication adherence is estimated to be 78.57% (±1.63478) with a 95% CI of [75.19, 81.61]. The age composition of participants ranges from 19 to 97 years old, with the average age of the participants being 53.82 (±0.5285) years and a 95% CI [52.78, 54.86].
Patients’ Sociodemographic Characteristics and Clinical Characteristics
Though the proportion of patients with medication adherence increases with age, age is not significantly associated with medication adherence (Table 2). About 80% of males were adherent, whereas 75.62% for females. A statistically significant association is observed between medication adherence and nationality. The medication adherence for UAE nationals is significantly (p-value < 0.001) higher than that of expatriates. Although most (95%) of the patients do not drink alcohol, about 81% of those who drink alcohol were adherent to medication. Adding to that, there is no statistically significant difference in the prevalence of high medication adherence among teetotalers compared to those who drink alcohol. Household income is significantly (p-value < 0.001) associated with medication adherence. Of those patients whose income is less than 10,000 a month, about 75% were adherent to medication; whereas 95% of those who earn 40,001–50,000 were adherent to medication. Occupation of the patients also has a significant (p-value = 0.029) association with high medication adherence. Among the retired patients, about 86% had high adherence to medication.
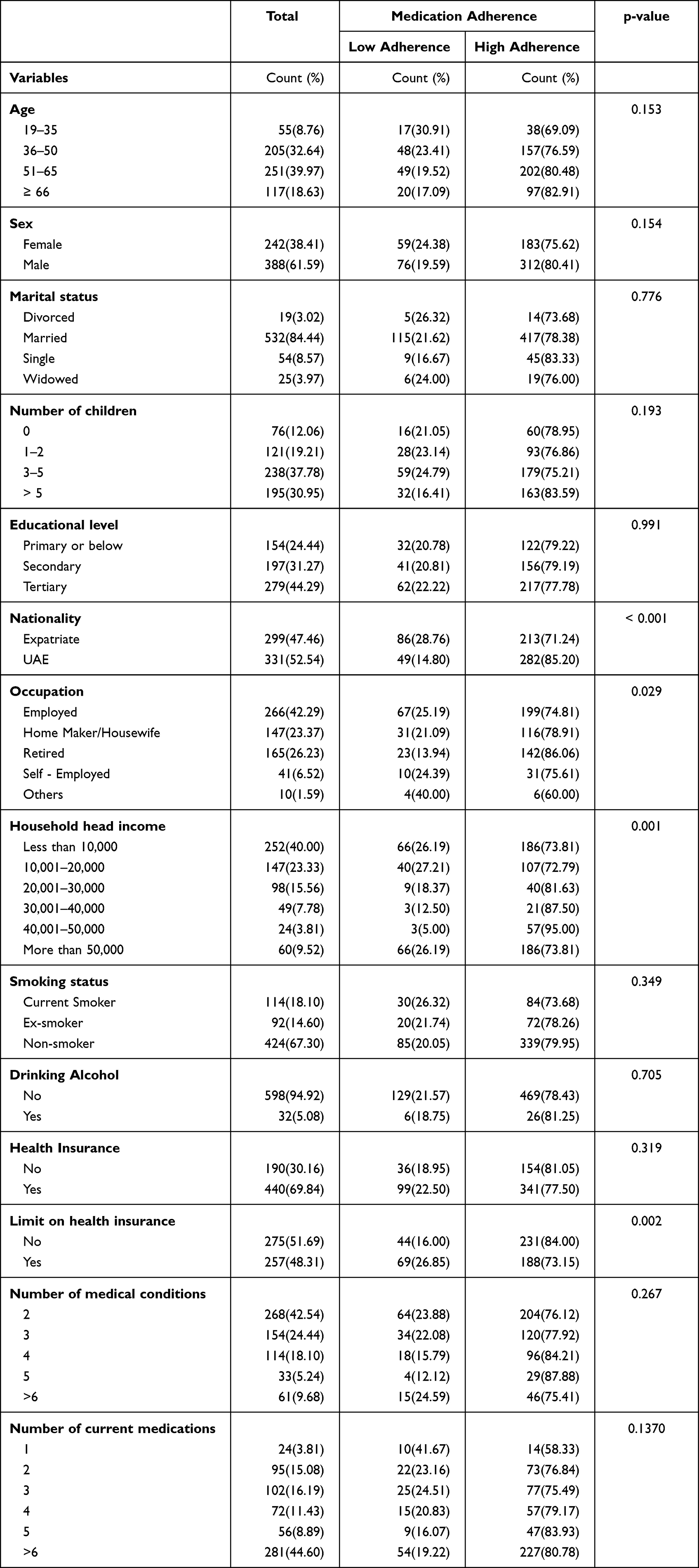 |
Table 2 Sociodemographic Characteristics and Clinical Characteristics of Patients |
Almost 70% of the patients have health insurance coverage, among which 77.5% were adherent to medication. Limit on health insurance is statistically significantly (p-value = 0.002) associated with high medication adherence. On the other hand, about a quarter of the patients who had a limit on health insurance coverage were found to have low medication adherence.
Overall, the median number of current medications increased with age. The median number of current medications for patients with high medication adherence in the age group 19–35 is higher for females compared to males, and the same is true for patients in the age group 36–50 (Figure 1).
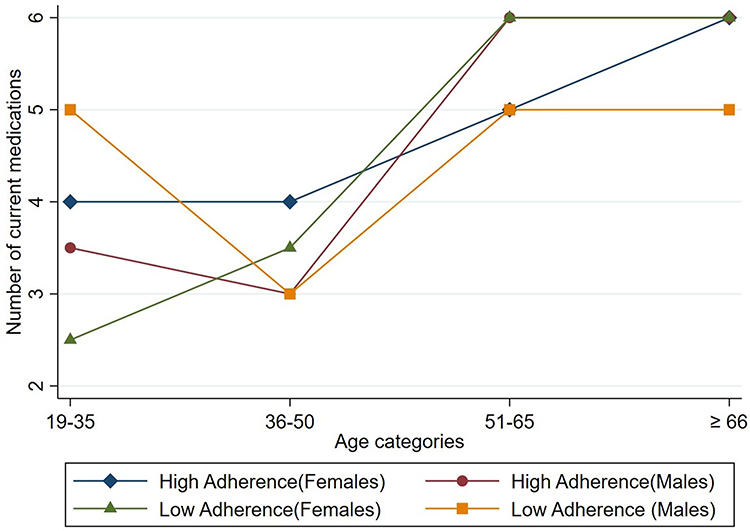 |
Figure 1 Median number of current medications by gender, age, and medication adherence. |
Among patients with a family history of hypertension, a significantly (p-value = 0.001) higher proportion (about 78%) of them were adherent to medication. A majority (78%) of patients with type 2 diabetes were adherent to medication. About three in four patients from a family with a heart disease history were adherent to medication. More than three-fourths of patients with a family history of dyslipidemia were adherent to medication (Table 3).
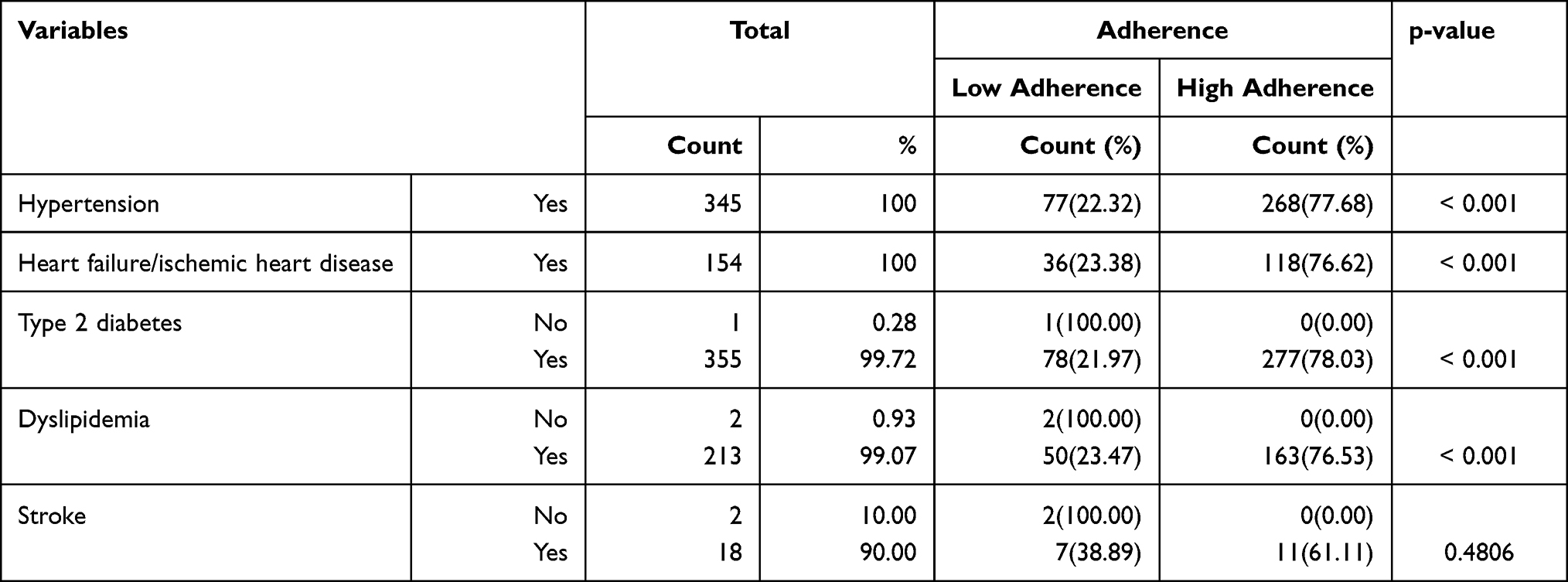 |
Table 3 Prevalence of Adherence to Medication by Family History |
It is evident from Figure 2 that the percentage of patients with health insurance coverage is higher among the highly adherent group across all age categories. Moreover, high medication adherent patients in the age range from 36 to 65 were found to have higher health insurance coverage compared to the others.
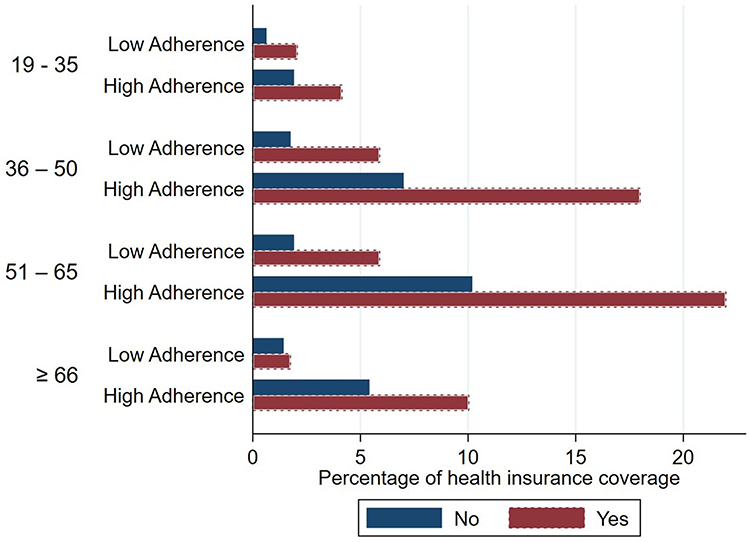 |
Figure 2 Percentage of medication adherence by insurance coverage and age categories. |
Co-Morbidity
As presented in Table 4, about one-quarter of the patients have heart disease, of which 80.13% were able to control its effect. A majority (90%) of the patients reported anemia or other blood-related diseases, of which 90% had received treatment. Among patients who have a blood pressure problem, almost 5% reported limiting their activities. Only a few, close to 3% of the patients, have reported depression. Although most of the patients reported that they had received the treatment, the majority reported that they could not control the disease.
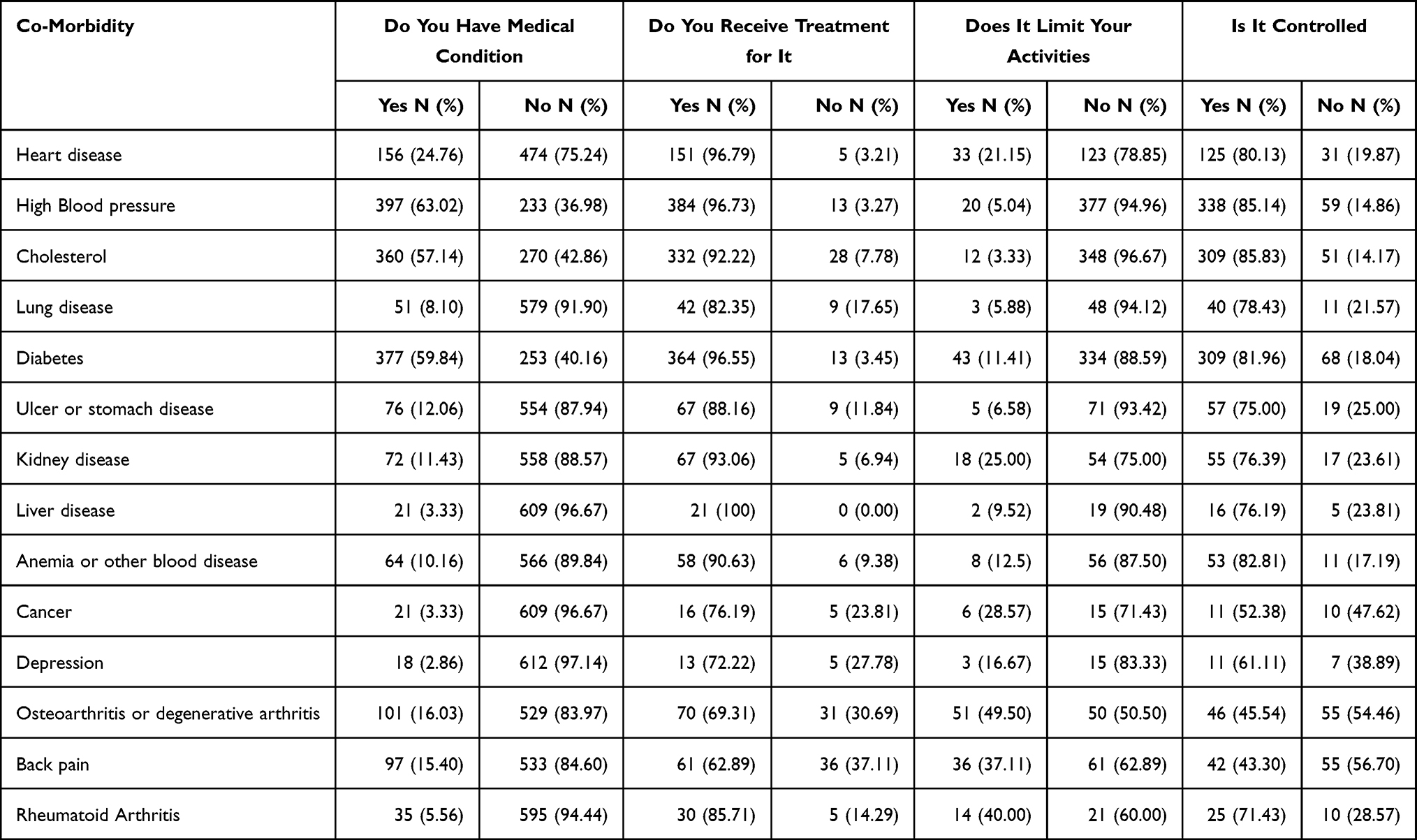 |
Table 4 Specific Co-Morbidity (The Self ‐ Administered Co-Morbidity Questionnaire) |
Factors Associated with Medication Adherence
Patients’ age is significantly associated with medication adherence after accounting for other factors. For patients in the age group 36–50, the odds of medication adherence are more than two-fold compared to those in the age group 19–35, the same holds for the higher age groups. The odds of medication adherence for patients who are 66 years and older is about fourfold compared to those aged 19–35 years. Although the odds of adherence to medication for male patients is lower by about 1%, compared to female patients, the difference is not statistically significant. For patients who earn more than 50,000, the odds, AOR = 5.169 with a 95% CI [1.282, 20.843], of medication adherence, are significantly (p-value = 0.021) higher by more than fivefold than those earning less than 10,000. Non-smoking patients have higher odds of medication adherence than current smokers, although the association is not statistically significant.
The odds of medication adherence for non-smokers is lower by almost 30%, compared to smokers. For both patients with health insurance coverage and limit on health insurance, the odds of medication adherence are lower than their counterparts.
The number of current medications has a quadratic relationship with the odds of medication adherence. The odds ratio, AOR = 4.529 with a 95% CI [1.184, 17.326], was the highest for those currently taking four medications. The odds of medication adherence are significantly (p-value = 0.027) higher by more than fourfold than those taking one medication.
Patients with lung disease or diabetes had higher medication adherence odds than those who do not have those diseases. Cancer patients had significantly (p-value =0.030) lower odds, AOR=0.258, CI [0.076, 0.877], of medication adherence compared to their counterpart. Patients with osteoarthritis had significantly (p-value = 0.010) lower odds, AOR = 0.376 with a 95% CI [0.178, 0.795], of medication adherence, compared to those who did not have the condition.
Discussion
In this study, the prevalence of medication adherence was estimated to be 78.57%. We have explored the factors associated with multimorbidity and medication adherence in the UAE Nationality, household income and occupation were found to significantly influence higher medication adherence among patients with multi-morbidities. High adherence increased with age and with increased limit to health insurance.
The challenge of ensuring that patients adhere to lifelong therapy for chronic conditions has seen many different interventions implemented over the past few decades. Chronic conditions currently dominate the burden of illness in our society, and poor medication adherence affects the potential of effective treatments to improve patients’ health and quality of life. Patients and patient factors were primarily thought to be the main reason for the failure of medication adherence. Research has documented that low adherence to medications is multifactorial and multidimensional related to patients, physicians, and healthcare systems. In this study, medication adherence was around 79% compared to developed countries (50%)41 while results on medication adherence obtained from Spain was 55.5%,42 China at 53%43 and 48% among American patients was much higher.42 There may be many explanations for this outcome in our study, but it should not be confused with therapeutic control for these illnesses. Although just a speculation our high medication adherence may be related to a positive doctor–patient relationship. In a study conducted by Svensson et al adherence to antihypertensive medication was related to faith in the physician, which suggests that the quality of the provider–patient relationship was also an important determinant.44
Some of the sociodemographic factors were that were statistically significant were nationality, occupation, household income (those earning > AED 50000, the AOR = 5.169, 95% CI [1.282–20.843]), and health insurance. After adjustment for several variables, we found age, income, and the number of current medications as independent factors for adherence. Other studies have different factors depending on the outcome variables measured. In the Spanish study (2019), older age, lower number of pharmacies used for medication refills, having received complete treatment information, having adequate knowledge about the medication regimen, and self-perception of a good quality of life were independent factors associated with adherence.42 A study conducted in Saudi Arabia among patients with diabetes was positively associated with age and education.45 These differing results demonstrate the diversity among the determinants for non-adherence to medications.
In 2015, 901 million persons were 60 years and older globally, most living in developing countries. It is expected that by 2050, 20% of the total population, ie, 1802 million, will be above 60 years.46 The average life expectancy from 2010 to 2015 in developing countries was 68 years and 78 years in the developed countries,47 while according to the World Data Atlas, the life expectancy in 1971 in the UAE increased from 62.1 years to 78.12 years by 2020 with an average annual growth of 0.47%.48,49 The average age of the participants with multimorbidity in this study was 54 years old and, together with the increasing life expectancy, gives a picture of increasing longevity leading to long-term individual health consequences as well as for the health system and economy. As expected older patients are more likely to have comorbidities. Thus, medication adherence was associated with increasing age which was supported by a regional study.45 While a recent study found partial-to-poor adherence in patients on medications for comorbidity45 interestingly. This study showed those that were 66 years and older are four times more likely to adhere to their medications (AOR = 3.880 95% CI [1.124–13.390]) which is a welcoming outcome in the UAE behind a backdrop of a plethora of research showing that patients’ non-adherent to medications have increased visits, in some instances four times higher, to the emergency rooms, inpatient and outpatient departments.30 In a systematic review this could be supported with that age having a concave relation to adherence, ie, adherence is lowest in very young and very old people, which may explain our findings.50
It was predicted that non-communicable diseases (NCD) would account for 80% of the world’s public health burden.51,52 Recent systematic reviews suggest that the prevalence of multimorbidity is in the range of 23%–33%.2–4 Persons 65 years or older are expected to live with four or more chronic diseases by 2035.5 The highest percentages with non-communicable diseases in this study were hypertension, diabetes mellitus, hyperlipidemia, and cardiovascular disease with 63%, 60%, 57%, and 25% with self-reported illness control of 15%, 82%, 86%, and 80%, respectively. Unfortunately, most studies outlined medication adherence to a single medical illness and less on medications for multimorbidity. In this study, 78.03% of patients were adherent to their anti-diabetic medication, and despite this, only 50.95% say that their diabetes mellitus is controlled. In a regional study, Saudi Arabia documented only 35.8% adhering to their anti-diabetic medication. The CODE-2 study (Cost of Diabetes in Europe – Type 2) conducted in Europe reported that only 28% of patients treated for diabetes had achieved good glycemic control which is much lower than recorded here.53 In a recent study conducted in the UAE among patients with hypertension, the overall adherence to antihypertensive treatment was 42% while we documented a higher rate at 78% with 85% at suboptimal hypertension control.27 The UAE has an incidence for major CVD is 12.7 per 1000 person-years,54 with 25% of this cohort positively affirming CVD. Almost all of this cohort are being treated (97%) at least 80% have indicated that their CVD event is controlled. In a study assessing the impact of medication adherence on CVD outcomes, the non-adherent patients had double the risk of a major CVD event30 Results from studies show a disconnect between medication adherence and therapeutic outcomes. This confirms the complexity of managing multimorbidity patients and the problems related to poor medication adherence. Treatment plans in patients with multimorbidity are complex and are often compromised by many barriers and challenges. These include socio-economic causes, healthcare professionals, health systems, disease characteristics and therapies, and patient factors. Such challenges have been magnified with the current pandemic.16,19 Addressing these problems will assist in improving medication adherence.
Strengths and Limitations
To our knowledge, this is the first study conducted among multimorbidity patients in the UAE with a large sample from tertiary referral hospitals. The study further estimated the prevalence estimates of medication adherence while controlling for other variables. WHO and United Nations associated SDGs recognize multimorbidity and poor adherence to medications as a significant challenge for public health. Our results call for implementing a tool such as surveys to improve patient-related outcome measures due to improved adherence. There are some limitations to this study. First, in self-reported surveys, patients may overestimate their adherence to medications due to social desirability bias. Nevertheless to mitigate such effect in our study a well-trained interviewer and a robust validated questionnaire with identified options to questions would have reduced such bias.55 Second, a bias due to self-reported measures can affect the results. Third, we recruited participants from two large referral hospitals from the Emirates of Dubai. Though our study was multi – centre and many participants were from different UAE geographical locations, it may not be an accurate representative sample. Hence, a large systematic multi-centric study across in different regions of the UAE would be required for generalizability of the results. Furthermore, WHO has categorized potential reasons for medication nonadherence into five dimensions which include patient, condition, therapy, socioeconomic, and health system–related factors.56 Thus, adding a qualitative methodology for future research will enrich and improve the robustness in understanding the multidimensional factors related to medication adherence.
Implications for Practice
Medication and lifestyle adherence are the most important modifiable factors that compromise even the best treatment outcomes. Clinical interventions should encompass assessment tools and strategies to promote behavior change as suggested in a study that training programs can increase clinicians’ awareness of factors impacting on medication adherence.10 In a meta-analysis conducted by Roter et al, interventions that combined cognitive, behavioral, and affective components were most effective.57 It is well-documented that the doctor–patient relationship is the cornerstone to improved health outcomes and central to this is physician compassion and empathy.58,59 Our study highlights the relationship between medication adherence and multimorbidity with many SDGs goals and targets, particularly SDG 3 (Good Health and Well-being), SDG 8 (Decent Work and Economic Growth), SDG 15 (Reduced Inequality) and SDG17 (Partnerships to achieve the Goal). By implementing appropriate evidence-based policies and guidelines, key policymakers can influence medication adherence, better health outcomes, and quality of life. Policymakers can address variables that include the availability and accessibility of services, support for patient education, data and information management, community support to patients, and adequate training provided to health service providers.60 Furthermore, our study calls on policymakers for Universal Health Coverage to provide health system financial options and service patterns to patients with multimorbidity.61 Such cost-effective economic interventions with insurance and policies are needed to achieve the SDG targets. Sustainable investments by the policymakers to achieve such goals will add more benefit in averting premature deaths and significant health catastrophes such as stroke and ischemic heart disease and strengthen the national income through employment and increased productivity.62
Our findings highlight the need for further studies on patients with multimorbidity and their associated needs who may be associated with higher clinical care. Furthermore, it would be imperative to analyse through cost-effective analysis and modelling the economic costs involved with lack of medical insurance cover and how cost-effective measures can be implemented to prevent any disastrous consequences on the health and economy due to poor adherence.
Conclusion
This study highlighted a young population having multimorbidity in increasing life expectancy and suboptimal therapeutic outcomes. Furthermore, the study highlights that out-of-pocket payment and non-availability of insurance are major hindrances to medication adherence. Medication non-adherence is a significant public health crisis, and by increasing the effectiveness of adherence interventions, the health of populations will be more positively impacted than any specific medical treatment could achieve. Such improvement can further be achieved by wise investments by policymakers in multimorbidity prevention and treatment with a vision to obtain a return on investment by achieving SDG.
Acknowledgments
The authors thank all the patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was supported by the United Arab Emirates University Research Grant (Grant Code – G0000356/12M090-NP-21-13). The funder did not have a role in the design, collection, analysis, interpretation of data, and/or writing of this manuscript.
Disclosure
The authors report no conflicts of interest for this work and declare that there are no financial and commercial conflicts of interest that could be perceived as prejudicing the impartiality of this study.
References
1. Johnston MC, Crilly M, Black C, Prescott GJ, Mercer SW. Defining and measuring multimorbidity: a systematic review of systematic reviews. Eur J Public Health. 2019;29(1):182–189. doi:10.1093/eurpub/cky098
2. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
3. Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM. Prevalence of multimorbidity in community settings: a systematic review and meta-analysis of observational studies. J Comorbidity. 2019;9:2235042X19870934. doi:10.1177/2235042X19870934
4. Violan C, Foguet-Boreu Q, Flores-Mateo G, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS One. 2014;9(7):e102149–e102149. doi:10.1371/journal.pone.0102149
5. Kingston A, Robinson L, Booth H, Knapp M, Jagger C. MODEM project. Projections of multi-morbidity in the older population in England to 2035: estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing. 2018;47(3):374–380. doi:10.1093/ageing/afx201
6. Lee JT, Hamid F, Pati S, Atun R, Millett C. Impact of noncommunicable disease multimorbidity on healthcare utilisation and out-of-pocket expenditures in middle-income countries: cross sectional analysis. PLoS One. 2015;10(7):e0127199.
7. Yoon J, Zulman D, Scott JY, Maciejewski ML. Costs associated with multimorbidity among VA patients. Med Care. 2014;52 Suppl 3(Suppl 3):S31–S36. doi:10.1097/MLR.0000000000000061
8. Sasseville M, Smith SM, Freyne L, et al. Predicting poorer health outcomes in older community-dwelling patients with multimorbidity: prospective cohort study assessing the accuracy of different multimorbidity definitions. BMJ Open. 2019;9(1):e023919–e023919. doi:10.1136/bmjopen-2018-023919
9. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357–363.
10. Maffoni M, Traversoni S, Costa E, et al. Medication adherence in the older adults with chronic multimorbidity: a systematic review of qualitative studies on patient’s experience. Eur Geriatr Med. 2020;11(3):369–381. doi:10.1007/s41999-020-00313-2
11. Kurczewska-Michalak M, Lewek P, Jankowska-Polańska B, et al. Polypharmacy management in the older adults: a scoping review of available interventions. Front Pharmacol. 2021;12:734045. doi:10.3389/fphar.2021.734045
12. Walsh CA, Cahir C, Tecklenborg S, Byrne C, Culbertson MA, Bennett KE. The association between medication non‐adherence and adverse health outcomes in ageing populations: a systematic review and meta‐analysis. Br J Clin Pharmacol. 2019;85(11):2464–2478. doi:10.1111/bcp.14075
13. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
14. Vrijens B, Dima AL, Van Ganse E, et al. What we mean when we talk about adherence in respiratory medicine. J Allergy Clin Immunol Pract. 2016;4(5):802–812. doi:10.1016/j.jaip.2016.05.019
15. Kernick D, Chew-Graham CA, O’Flynn N. Clinical assessment and management of multimorbidity: NICE guideline. Br J Gen Pract. 2017;67(658):235–236. doi:10.3399/bjgp17X690857
16. Ismail L, Materwala H, Znati T, Turaev S, Khan MAB. Tailoring time series models for forecasting coronavirus spread: case studies of 187 countries. Comput Struct Biotechnol J. 2020;18:2972–3206. doi:10.1016/j.csbj.2020.09.015
17. Tsenoli M, Moverley Smith JE, Khan M. A community perspective of COVID-19 and obesity in children: causes and consequences. Obes Med. 2021;22:100327. doi:10.1016/j.obmed.2021.100327
18. Khan MA, Menon P, Govender R, et al. Systematic review of the effects of pandemic confinements on body weight and their determinants. Br J Nutr. 2021:1–74. doi:10.1017/S0007114521000921.
19. Al Falasi RJ, Khan AM. The impact of COVID-19 on Abu Dhabi and its primary care response. Aust J Gen Pract. 2020;49. doi:10.31128/AJGP-COVID-35.
20. Sokol MC, McGuigan KA, Verbrugge RR, Epstein RS. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005;43(6):521–530. doi:10.1097/01.mlr.0000163641.86870.af
21. Mazzaglia G, Ambrosioni E, Alacqua M, et al. Adherence to antihypertensive medications and cardiovascular morbidity among newly diagnosed hypertensive patients. Circulation. 2009;120(16):1598–1605. doi:10.1161/CIRCULATIONAHA.108.830299
22. Robin DiMatteo M, Giordani PJ, Lepper HS, Croghan TW. Patient adherence and medical treatment outcomes: a meta-analysis. Med Care. 2002;40(9):794–811. doi:10.1097/00005650-200209000-00009
23. Kini V, Ho PM. Interventions to improve medication adherence: a review. JAMA. 2018;320(23):2461–2473. doi:10.1001/jama.2018.19271
24. Hajat C, Harrison O, Shather Z. A profile and approach to chronic disease in Abu Dhabi. Global Health. 2012;8(1):18. doi:10.1186/1744-8603-8-18
25. Atlas D. International Diabetes Federation. IDF Diabetes Atlas.
26. Al-Haj Mohd MMM, Phung H, Sun J, Morisky DE. Improving adherence to medication in adults with diabetes in the United Arab Emirates. BMC Public Health. 2016;16(1):857. doi:10.1186/s12889-016-3492-0
27. Bhagavathula AS, Shah SM, Aburawi EH. Medication adherence and treatment-resistant hypertension in newly treated hypertensive patients in the United Arab Emirates. J Clin Med. 2021;10(21):5036. doi:10.3390/jcm10215036
28. Assembly G. United Nations: transforming our world: the 2030 agenda for sustainable development. New York, NY, USA: UN; 2015.
29. Nugent R, Bertram MY, Jan S, et al. Investing in non-communicable disease prevention and management to advance the Sustainable Development Goals. Lancet. 2018;391(10134):2029–2035. doi:10.1016/S0140-6736(18)30667-6
30. Bansilal S, Castellano JM, Garrido E, et al. Assessing the impact of medication adherence on long-term cardiovascular outcomes. J Am Coll Cardiol. 2016;68(8):789–801. doi:10.1016/j.jacc.2016.06.005
31. Foley L, Larkin J, Lombard-Vance R, et al. Prevalence and predictors of medication non-adherence among people living with multimorbidity: a systematic review and meta-analysis. BMJ open. 2021;11(9):e044987. doi:10.1136/bmjopen-2020-044987
32. Simpson SH, Eurich DT, Majumdar SR, et al. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ. 2006;333(7557):15. doi:10.1136/bmj.38875.675486.55
33. Kwan YH, Weng SD, Loh DHF, et al. Measurement properties of existing patient-reported outcome measures on medication adherence: systematic review. J Med Internet Res. 2020;22(10):e19179. doi:10.2196/19179
34. Naqvi AA, Hassali MA, Rizvi M, et al. Development and validation of a novel General Medication Adherence Scale (GMAS) for chronic illness patients in Pakistan. Front Pharmacol. 2018;9:1124. doi:10.3389/fphar.2018.01124
35. Naqvi AA, Hassali MA, Jahangir A, Nadir MN, Kachela B. Translation and validation of the English version of the general medication adherence scale (GMAS) in patients with chronic illnesses. J Drug Assess. 2019;8(1):36–42. doi:10.1080/21556660.2019.1579729
36. Wang Y, Wang X, Wang X, Naqvi AA, Zhang Q, Zang X. Translation and validation of the Chinese version of the general medication adherence scale (GMAS) in patients with chronic illness. Curr Med Res Opin. 2021;37(5):829–837. doi:10.1080/03007995.2021.1901680
37. Naqvi AA, Mahmoud MA, AlShayban DM, et al. Translation and validation of the Arabic version of the General Medication Adherence Scale (GMAS) in Saudi patients with chronic illnesses. Saudi Pharmaceut J. 2020;28(9):1055–1061. doi:10.1016/j.jsps.2020.07.005
38. Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The self-administered comorbidity questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Care Res. 2003;49(2):156–163. doi:10.1002/art.10993
39. Diederichs C, Berger K, Bartels DB. The measurement of multiple chronic diseases—a systematic review on existing multimorbidity indices. J Gerontol a Biol Sci Med Sci. 2011;66(3):301–311. doi:10.1093/gerona/glq208
40. StataCorp. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC; 2019.
41. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;11. doi:10.1002/14651858.CD000011.pub4
42. Fernandez-Lazaro CI, García-González JM, Adams DP, et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Fam Pract. 2019;20(1):1–12. doi:10.1186/s12875-019-1019-3
43. Li YT, Wang HH, Liu KQ, et al. Medication adherence and blood pressure control among hypertensive patients with coexisting long-term conditions in primary care settings: a cross-sectional analysis. Medicine. 2016;95(20). doi:10.1097/MD.0000000000003572.
44. Svensson S, Kjellgren KI, Ahlner J, Säljö R. Reasons for adherence with antihypertensive medication. Int J Cardiol. 2000;76(2):157–163. doi:10.1016/S0167-5273(00)00374-0
45. AlQarni K, AlQarni EA, Naqvi AA, et al. Assessment of medication adherence in Saudi patients with type II diabetes mellitus in Khobar City, Saudi Arabia. Front Pharmacol. 2019;10:1306. doi:10.3389/fphar.2019.01306
46. Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–562. doi:10.1016/S0140-6736(14)61347-7
47. Nations U. World population prospects 2019. Department of Economic and Social Affairs; 2019:141.
48. Wang H, Abbas KM, Abbasifard M, et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1160–1203.
49. World Bank. Life expectancy at birth, total (years) - United Arab Emirates | data. Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=AE.
50. Gast A, Mathes T. Medication adherence influencing factors—an (updated) overview of systematic reviews. Syst Rev. 2019;8(1):112. doi:10.1186/s13643-019-1014-8
51. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. World Health Organization; 2013. Available from: https://www.who.int/nmh/events/ncd_action_plan/en/.
52. Nauman J, Soteriades ES, Hashim MJ, et al. Global incidence and mortality trends due to adverse effects of medical treatment, 1990–2017: a systematic analysis from the global burden of diseases, injuries and risk factors study. Cureus. 2020;12(3):e7265.
53. Liebl A, Neiss A, Spannheimer A, et al. Complications, co-morbidity, and blood glucose control in type 2 diabetes mellitus patients in Germany-results from the CODE-2TM study. Exp Clin Endocrinol Diabetes. 2002;110(01):10–16. doi:10.1055/s-2002-19988
54. Al-Shamsi S, Regmi D, Govender RD. Incidence of cardiovascular disease and its associated risk factors in at-risk men and women in the United Arab Emirates: a 9-year retrospective cohort study. BMC Cardiovasc Disord. 2019;19(1):1–9. doi:10.1186/s12872-019-1131-2
55. Grimm P. Social desirability bias. Wiley international encyclopedia of marketing; 2010. doi:10.1002/9781444316568.wiem02057.
56. World Health Organization. Adherence to long-term therapies: evidence for action; 2003. Available from: https://apps.who.int/iris/handle/10665/42682.
57. Roter DL, Hall JA, Merisca R, Nordstrom B, Cretin D, Svarstad B. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36(8):1138–1161. doi:10.1097/00005650-199808000-00004
58. Deniz S, Akbolat M, Çimen M, Ünal Ö. The mediating role of shared decision-making in the effect of the patient–physician relationship on compliance with treatment. J Patient Exp. 2021;8:23743735211018064. doi:10.1177/23743735211018066
59. Świątoniowska-lonc N, Polański J, Tański W, Jankowska-Polańska B. Impact of satisfaction with physician–patient communication on self-care and adherence in patients with hypertension: cross-sectional study. BMC Health Serv Res. 2020;20(1):1–9. doi:10.1186/s12913-020-05912-0
60. Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. 2018;6(11):e1196–e1252.
61. Sum G, Hone T, Atun R, et al. Multimorbidity and out-of-pocket expenditure on medicines: a systematic review. BMJ Glob Health. 2018;3(1):e000505. doi:10.1136/bmjgh-2017-000505
62. Bertram MY, Sweeny K, Lauer JA, et al. Investing in non-communicable diseases: an estimation of the return on investment for prevention and treatment services. Lancet. 2018;391(10134):2071–2078. doi:10.1016/S0140-6736(18)30665-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.