Back to Journals » Psychology Research and Behavior Management » Volume 19
Mediating Effects of Emotion Dysregulation and Negative Perfectionism on the Link Between Adverse Parenting and Obsessive-Compulsive Personality Disorder Traits
Received 2 May 2025
Accepted for publication 27 December 2025
Published 14 January 2026 Volume 2026:19 538134
DOI https://doi.org/10.2147/PRBM.S538134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Igor Elman
Wanyi Cao,1,2 Yanhong Bao1,2
1School of Psychology, Jiangxi Normal University, Nanchang, Jiangxi, 330022, People’s Republic of China; 2Center of Mental Health Education and Research, Jiangxi Normal University, Nanchang, Jiangxi, 330022, People’s Republic of China
Correspondence: Wanyi Cao, School of Psychology, Jiangxi Normal University, Nanchang, Jiangxi, 330022, People’s Republic of China, Email [email protected]
Objective: Previous research has established adverse parental rearing as a significant risk factor for obsessive-compulsive personality disorder (OCPD). This study investigated whether maladaptive emotion regulation strategies and negative perfectionism serve as psychological mechanisms underlying this association, with particular attention to potential sequential mediation pathways.
Methods: This study adopted a cross-sectional design and multi-channel convenience sampling approach. A sample of 827 Chinese university students completed standardized measures assessing OCPD features (OCPD subscale of Personality Diagnostic Questionnaire‐4+, PDQ‐4+), parental rearing styles (short-form Egna Minnenav Barndoms Uppfostran, s-EMBU), emotion regulation strategies (Cognitive Emotion Regulation Questionnaire, CERQ), and perfectionism traits (Frost Multidimensional Perfectionism Scale, FMPS). We employed structural equation modeling based on Mplus 8.3 to examine both direct effects of adverse parenting on OCPD and indirect effects mediated through emotion regulation and perfectionism.
Results: Path analysis revealed a significant direct effect of adverse parenting on OCPD features (β=0.160, p< 0.001). The primary indirect pathway demonstrated sequential mediation: adverse parenting was associated with maladaptive emotion regulation, which predicted increased negative perfectionism, ultimately contributing to OCPD (β=0.041, p=0.006). Parallel pathways were also observed through either maladaptive emotion regulation (β=0.085, p=0.007) or negative perfectionism (β=0.052, p=0.012). The proposed mediation model explained a substantial proportion (52.66%) of the variance in OCPD features, underscoring the critical role of these psychological mechanisms in the development of OCPD pathology.
Conclusion: These findings reveal that adverse parenting contributes to OCPD both directly and through a sequential emotional-cognitive pathway where poor emotion regulation fosters perfectionist attitudes. This study identifies modifiable psychological processes—emotion regulation and perfectionism—as promising targets for early intervention aimed at reducing OCPD risk in individuals exposed to negative parenting.
Keywords: adverse parental rearing, maladaptive emotion regulation, negative perfectionism, obsessive-compulsive personality feature
Introduction
Obsessive-compulsive personality disorder (OCPD) stands as one of the most prevalent personality disorder, distinguished by an overpowering fixation on orderliness, perfectionism, and exerting control both mentally and interpersonally.1 This preoccupation often comes at the detriment of flexibility, openness to new experiences, and overall efficiency in daily functioning and relationships.2 The approximate lifetime prevalence of OCPD ranges from 2.1% to 7.9%.1 The prevalence of personality disorders among university students is higher than in the general population, with OCPD being the second most common personality disorder within this demographic.3 Although OCPD is a clinical diagnosis, subclinical OCPD traits are prevalent in non-clinical populations, particularly among college students who often exhibit perfectionistic tendencies and heightened emotional reactivity due to academic and social pressures.4 Investigating these traits in a college sample allows for the identification of early manifestations of OCPD and the underlying mechanisms in a developmentally relevant context, potentially informing early intervention strategies.
There is accumulating evidence suggesting that parental rearing practices may influence the development of OCPD.5,6 Parental rearing is generally categorized into positive aspects (eg, emotional warmth) and negative aspects (eg, rejection, over-protection, over-intervention and controlling behavior).7 A systematic review of the literature indicated that individuals with obsessive-compulsive symptoms demonstrate significantly lower levels of parental care and higher levels of parental control during childhood compared to healthy controls.8 Huang et al found that parental style, low family income and low social status contribute to the development of personality disorders in Chinese college students.9 It was suggested that parental rejection and over-protection were significantly correlated with the occurrence of OCPD in adolescents, supporting the notion that negative parental bonding is a potential environmental risk factor for the development of personality disorders.5 Furthermore, while the associations between adverse parenting and OCPD features have been documented across cultures, the expression and perception of parenting behaviors may vary significantly across sociocultural contexts. For instance, studies have shown that certain parenting styles (eg, authoritarianism) may be interpreted differently in Eastern versus Western cultures,10 potentially influencing their impact on personality development. This study, conducted in a Chinese cultural context, contributes to this cross-cultural discourse by examining these relationships within a collectivist framework, where familial expectations and perfectionistic standards may play particularly prominent roles.
Maladaptive emotion regulation, characterized by the inability to monitor and modulate one’s affective or emotion-related state to achieve goals, can override judgment and reason, leading to a lack of control.11 As a transdiagnostic factor, emotion dysregulation may contribute to both the onset and maintenance of personality pathology. Specifically, individuals with personality disorders who employ maladaptive emotion regulation strategies (eg, suppression) demonstrate significant interpersonal impairments - particularly in conflict resolution and emotional intimacy.12 These effects are pronounced in OCPD, where Steenkamp et al found elevated levels of emotion dysregulation, negative affect, and trait anger, collectively exacerbating social dysfunction.13 Edwards et al also found that maladaptive emotional schemas were associated with greater symptom severity in OCPD.14 Fitzpatrick et al found that higher emotional reactivity and lower behavioral inhibition predicted Cluster C personality disorders.12 Additionally, several treatment-relevant studies have emphasized the importance of directly targeting emotion dysregulation, suggesting that improvements in emotion regulation mediate therapeutic effects for personality disorders and reduce the likelihood of internalizing disorders.15,16 Therefore, preliminary studies have evidenced a significant association between emotion dysregulation and features of OCPD.
Negative perfectionism is a multidimensional personality trait characterized by the establishment of high personal standards, a relentless striving for perfection, and overcritical self-evaluations.17 Clinical perfectionism is considered a personality-based vulnerability factor, and the DSM-5 highlights perfectionism as an essential and indispensable feature of OCPD.1 Numerous studies have demonstrated higher levels of perfectionism in individuals with OCPD compared to the general population across both clinical and non-clinical samples. For example, Sametoglu et al found that childhood trajectories of perfectionism could effectively predict the rigid component of perfectionism in adolescent OCPD using latent growth curve modeling.18 Cheli et al addressed perfectionism as a maladaptive form of coping, suggesting it is a primary mechanism in the treatment of OCPD.19 Another study further found that negative manifestations of perfectionism were strongly tied to pathological traits of OCPD.20
Existing literature highlights the significant role of parenting style in shaping children’s emotion regulation abilities. Specifically, warm, responsive, and empathetic parenting tends to foster adaptive emotional regulation, whereas controlling, intrusive, or overprotective parenting is often linked to emotional dysregulation in both children and adolescents.21 Furthermore, frequent parental rejection may lead children to internalize the belief that parental acceptance is conditional upon perfection, thereby increasing their vulnerability to maladaptive perfectionism. This aligns with the anxious rearing model, which posits that overprotective parents, driven by their own fear of failure and excessive perfectionism, may inadvertently transmit these tendencies to their children.22 In summary, parenting behaviors—whether rejecting or overprotective—can significantly influence emotional regulation and contribute to the development of maladaptive perfectionism in offspring.
The Present Study: Aims and Hypotheses
Although the relationship between parental rearing and OCPD features is well-demonstrated, the underlying psychological mechanisms and their structural relationships remain less clear. Specifically, two competing theoretical models can be proposed: (1) A model in which adverse parenting leads to emotion dysregulation, which in turn fosters negative perfectionism, ultimately contributing to OCPD features; and (2) A model in which adverse parenting first cultivates negative perfectionism, which subsequently impairs emotion regulation capacity, culminating in OCPD features. The present cross-sectional study aims to empirically test and compare the fit of these two alternative mediation models to ascertain which provides a more plausible account of the observed relationships. This model comparison approach can inform future longitudinal research designed to definitively establish temporal sequences. The present study systematically investigated the relationships among adverse parenting practices, maladaptive emotion regulation, negative perfectionism, and OCPD features. As illustrated in Figure 1, we hypothesized that: (1) Maladaptive emotion regulation (M1) and/or negative perfectionism (M2) wound mediate the association between adverse parenting practices (X) and OCPD features (Y). (2) Two distinct chain mediation pathways would emerge: Pathway 1, adverse parenting → maladaptive emotion regulation → negative perfectionism → OCPD features; Pathway 2, adverse parenting → negative perfectionism → maladaptive emotion regulation → OCPD features. In addition, we first compared sociodemographic and clinical variables between the OCPD screening-positive and screening-negative groups. This approach allows us to characterize the clinical profile of our sample and establish the comorbidity patterns between OCPD and other psychopathological symptoms, thereby providing a solid foundation for subsequent mechanistic modeling.
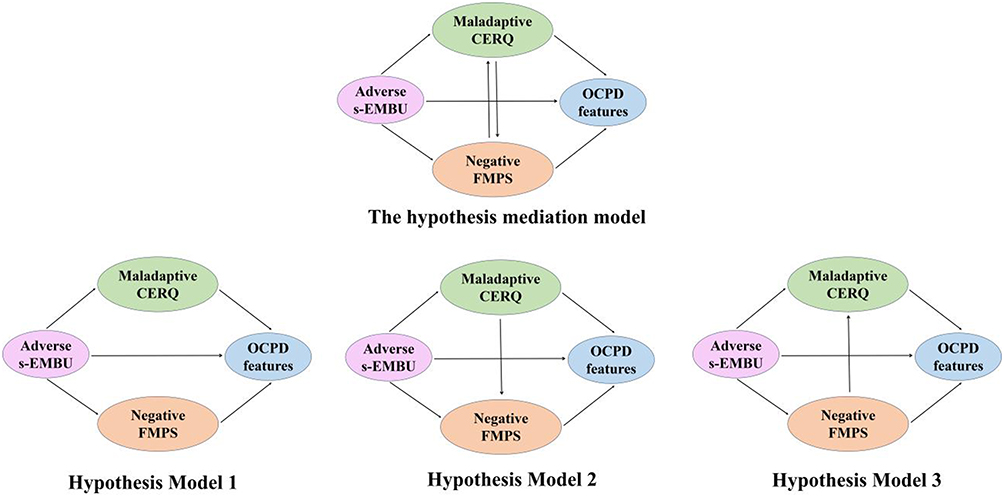 |
Figure 1 The hypothetical models: Exploring the role of maladaptive emotion regulation and negative perfectionism between adverse parental styles and OCPD features. |
Materials and Methods
Participants
We implemented a multi-channel convenience sampling approach, including university-approved mental health screening programs, psychology department research participant pools, voluntary recruitment notices in student activity areas. Data collection was carefully scheduled from October to December 2023 to avoid examination periods that might exacerbate symptoms and capture baseline functioning during regular academic weeks. Inclusion criteria in this study consisted of: (a) Full-time undergraduate students aged 16–28 years; (b) No current psychiatric treatment. And exclusion criteria in this study was: (a) Surveys with >10% missing data (ensuring data completeness); (b) Invalid response patterns (detected through embedded validity indicators). A cohort of 901 undergraduates were recruited from three universities located in Jiangxi and Hainan Province. Among them, 58 participants were excluded from the final analysis due to missing more than 10% of the items,23 and an additional 16 participants were excluded for random responding. Ultimately, 827 participants (264 males and 563 females) were included in the statistical analysis, with ages ranging from 16 to 28 years old (mean = 19.31, standard deviation [SD] = 1.26). The study protocol was approved by the ethics committee of school. Each participant was fully informed about the study’s purpose and provided an informed consent form, which was performed in accordance with the Declaration of Helsinki.
Research Design
This study adopted a cross-sectional design to examine the relationships among key variables at a single time point. The cross-sectional approach allows for the exploration of associations and mediation effects between variables.
Instrument
Personality Diagnostic Questionnaire‐4+ (PDQ-4+)
The PDQ‐4+ is a self‐report assessment scale for personality disorders, aligned with DSM‐IV criteria.24,25 In the current study, the OCPD subscale of PDQ‐4+ was utilized to screen participants for OCPD. This subscale comprises eight items, each answered with a “yes” (scored as 1) or “no” (scored as 0), such as “I am such a perfectionist that it interferes with my work”. The total score on the OCPD subscale ranges from 0 to 8, with scores of 4 or higher indicating a positive screening for OCPD. The reliability of the OCPD subscale in this study was found to be good (Cronbach’s α = 0.72).
Chinese Version of the Short-Form Egna Minnenav Barndoms Uppfostran (s-EMBU)
The s-EMBU was developed by Perris et al26 and translated into Chinese by Jiang et al.27 To evaluate parental rearing practices and behaviors, we utilized the Chinese version of s-EMBU. This scale contains 42 items, divided into the paternal (eg, My father wanted to control everything I did) and maternal (eg, My mother punished me for no good reason) versions. Responses are provided on a 4-point Likert scale (1 = never; 2 = seldom; 3 = often; 4 = most of the time). Each version includes three subscales scored separately without a total score: emotional warmth (7 items), rejection (6 items), and overprotection (8 items). Higher scores indicate a greater tendency toward that particular parenting style. In this study, only the subscales of rejection and overprotection were used to measure adverse parenting. The Cronbach’s alpha coefficients were 0.78 for fathers and 0.77 for mothers.
Cognitive Emotion Regulation Questionnaire (CERQ)
The 36-item CERQ was designed to assess nine specific cognitive emotion regulation strategies in response to negative events.28,29 Each item is rated on a 5‐point Likert scale ranging from 1 “never” to 5 “most of the time”. The CERQ is divided into maladaptive and adaptive subscale. The maladaptive subscale includes rumination, self‐blame, blaming others and catastrophizing, while the adaptive subscale comprises positive refocusing, acceptance, positive reappraisal, refocus on planning, and putting into perspective. In the current research, only the maladaptive subscale (CERQ-M) was used to measure negative emotion regulation strategies, such as “I feel that I am the one who is responsible for what has happened”. The Cronbach’s alpha coefficient for the CERQ-M in this study was 0.84.
Frost Multidimensional Perfectionism Scale (FMPS)
The 35-item FMPS was employed to assess both positive and negative perfectionism.17 This instrument encompasses six distinct subscales: concern over mistakes (CM; nine items), doubts about actions (DA; four items), parental expectations (PE; five items), and parental criticism (PC; four items), personal standards (PS; seven items) and organization (OR; six items). The participants’ responses to the items, such as “I should be upset if I make a mistake”, were structured using a five-point scale, ranging from “totally disagree (1)” to “totally agree (5)”. The construct of positive perfectionism is represented by the sum of scores from the PS and OR subscales, whereas the negative perfectionism dimension is derived from the aggregated scores of the CM, DA, PC and PE subscales. Elevated scores on these dimensions signify a heightened degree of either maladaptive or adaptive perfectionism. In this study, we employed the Chinese version of the negative FMPS questionnaire, which demonstrated good reliability with a Cronbach’s alpha coefficient of 0.90.
Beck Depression Inventory (BDI)
The BDI is a 21‐item self‐report questionnaire designed to evaluate the severity of depression experienced in the past week.30 Each item (eg sadness) is accompanied by a standard 4‐point Likert scale (“absent (0)” to “severe (3)”), with total scores ranging from 0 to 63. Higher score on the BDI indicate more severe depressive symptoms. This study confirmed that the BDI had excellent internal consistency, with a Cronbach’s alpha coefficient of 0.89.
State-Trait Anxiety Inventory (STAI)
The STAI is a self‐report questionnaire using a 4‐point Likert scale (“almost never (1)” to “almost always (4)”) to evaluate participants’ state anxiety and trait anxiety.31,32 It consists of two 20‐item (eg, “I am presently worrying over possible misfortunes”) subscales: the State‐Anxiety Inventory (SAI) and Trait‐Anxiety Inventory (TAI). Each subscale’s total score ranges from 20 to 80, with higher scores indicating more severe anxiety symptoms. In this study, both the SAI (Cronbach’s α = 0.92) and TAI (Cronbach’s α = 0.91) subscales demonstrated good internal consistency.
Subjective Socio-Economic Status (SSES)
The SSES is a 2‐item self‐report questionnaire designed to measure individuals’ perceptions of their economic and social status.33,34 Each item (eg “How would you rate your family’s financial status compared to others in your country?”) is rated on a ten‐point Likert scale ranging from 1 “lowest” to 10 “highest”, with higher scores indicating better economic or social status. In this study, the Cronbach’s alpha coefficient for the SSES was 0.66.
Statistical Analyses
First, the analyses were conducted using SPSS 25 (SPSS Inc., Chicago, IL, United States) and Mplus 8.3. Based on the cutoff score of the OCPD subscale of the PDQ‐4+, patients with an OCPD score higher than 4 points were classified as the screening‐positive OCPD (SP‐OCPD) group, while those with lower scores were classified as the screening‐negative OCPD (SN‐OCPD) group. Independent-sample t-tests were used to compare the differences in scores on the s-EMBU, FMPS, CERQ‐M subscale, BDI, SAI, TAI, and SSES between the SP‐OCPD and SN‐OCPD group. Participants who reported the absence of a father (n=12) or mother (n=8) figure during their upbringing were assigned a code of 99 on the respective s-EMBU scales to denote missing data. These cases were excluded from subsequent analyses involving those specific variables. All missing data were checked before analysis and imputed using the mean values of each item.
Second, partial correlation analyses and path analysis using maximum likelihood estimation were conducted to examine the relationships among adverse parental bonding, negative perfectionism, emotion dysregulation, and OCPD features, with depression and anxiety that were significantly different between two groups being defined as covariates. Observed variables were represented in rectangles, while latent variables were depicted in circles. To determine the significance of parameter estimates, bias‐corrected bootstrapped with 5000 bootstrap samples and a 95% confidence interval (CI) was employed, as this method has been shown to provide an optimal balance between statistical power and Type I error rates.35 If the 95% CI did not intersect with zero, it indicated that the effect was statistically significant. Model fit was assessed by examining individual path coefficients and various fit indices. Several indices were used to evaluate the model fit: The chi-square/degree of freedom ratio (χ2), the comparative fit index (CFI), the Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA) and standardized root mean-square residual (SRMR). Generally, a model is considered acceptable if it has a CFI ≥ 0.90, TLI ≥ 0.90, SRMR ≤ 0.08 and RMSEA ≤ 0.08.36 We compared the three models with fit indices (data-driven) and theoretical basis (experience-driven) to decide the optimal model.
Results
Group Differences in Sociodemographic and Clinical Variables
Based on the criteria established by the OCPD subscale of PDQ‐4+, the sample was segmented into two distinct cohorts: the SP‐OCPD group comprising 306 individuals and the SN‐OCPD group with 521 participants, which the positive rate for OCPD was 37% in the total sample. No statistically significant differences were observed in terms of age, sex ratio, subjective economic status and subjective social status between these two groups (all p >0.05; Table 1). The SP‐OCPD group exhibited significantly higher scores on the BDI, SAI, TAI, and overall scale as well as each factor of the adverse s-EMBU, CERQ‐M and negative FMPS compared to the SN‐OCPD group (all p<0.001; Cohen’s d=0.56~0.92; Table 1).
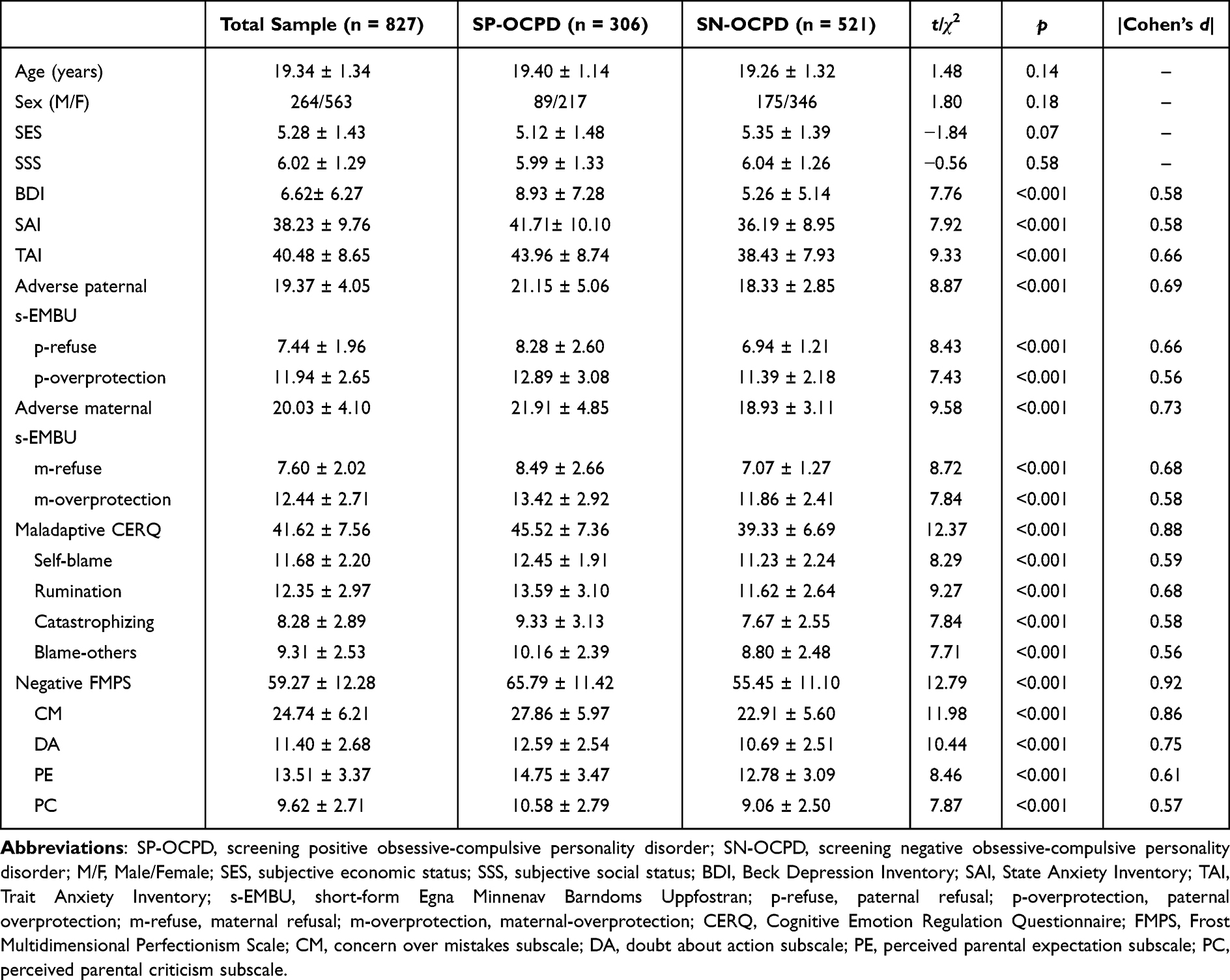 |
Table 1 Differences in Demographic and Psychological Variables Between SP-OCPD and SN-OCPD |
Correlation Analysis on the Various Scales and Measurement Model
Pearson correlation analysis revealed significant positive correlations between adverse paternal s-EMBU, adverse maternal s-EMBU, maladaptive CERQ, negative FMPS, and OCPD. Details are presented in Table 2. Prior to testing the main structural model, we evaluated the construct validity of the measurement model using Confirmatory Factor Analysis (CFA) with the four latent variables. We assessed convergent validity by examining the Composite Reliability (CR) and Average Variance Extracted (AVE) for each construct. As summarized in Table 3, all CR values exceeded the recommended threshold of 0.70, indicating good internal consistency. Furthermore, all AVE values were above 0.50, supporting adequate convergent validity.37
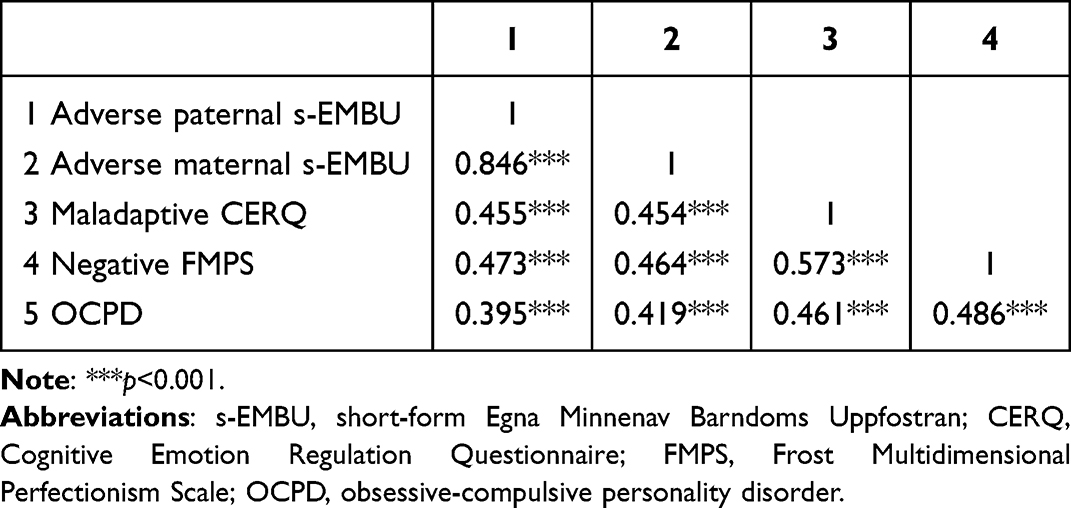 |
Table 2 Correlation Analysis of the Scores on the Various Scales |
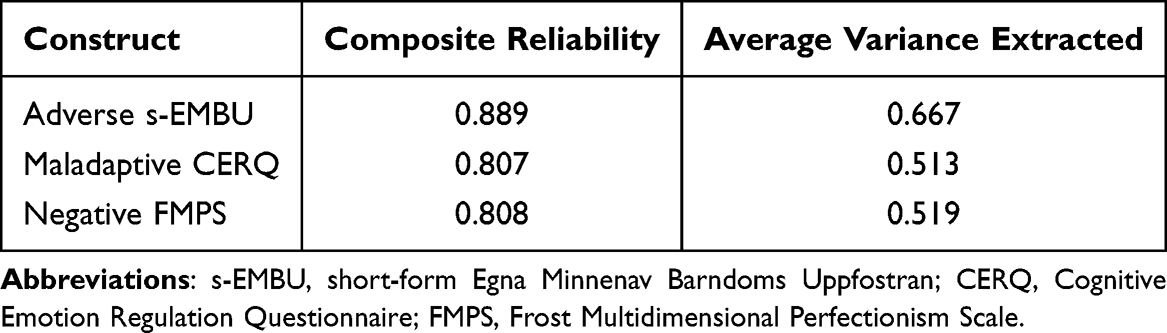 |
Table 3 Reliability and Convergent Validity of the Measurement Model |
Mediation Analysis Using Structural Equation Models (SEM)
In this study, we conducted SEM analysis to test three hypothetical mediation models (see Figure 1). All of them included measures of adverse parental styles, maladaptive emotion regulation, negative perfectionism and OCPD features.
For hypothetical Model 1, the SEM results showed that maladaptive emotion regulation and negative perfectionism mediated the relationship between adverse parental styles and OCPD features, but Model 1 did not fit the data well with the model fit indices not achieving the criterion (see Figure 2).
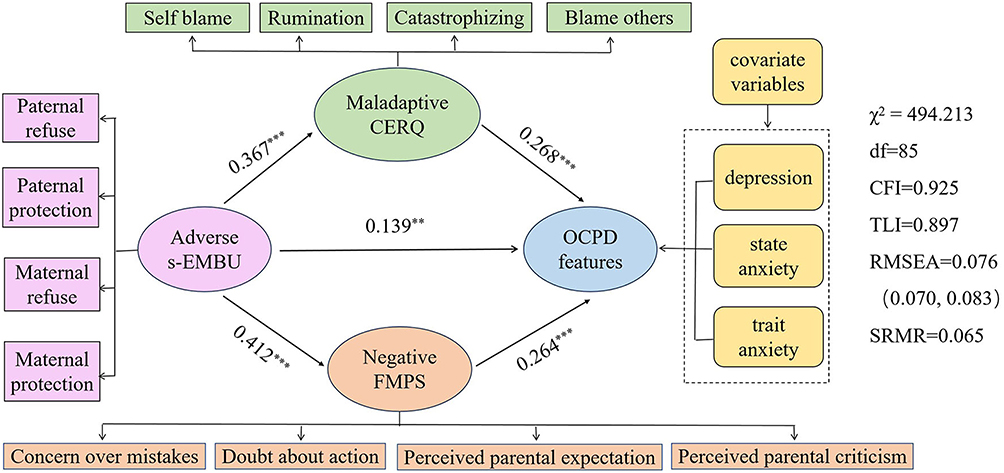 |
Figure 2 Model 1: parallel mediation analysis between parental styles and OCPD features. **p<0.01, ***p<0.001. Abbreviations: s-EMBU, short-form Egna Minnenav Barndoms Uppfostran; CERQ, Cognitive Emotion Regulation Questionnaire; FMPS, Frost Multidimensional Perfectionism Scale; OCPD, obsessive-compulsive personality disorder. |
For hypothetical Model 2, a path from negative perfectionism to maladaptive emotion regulation was added to Model 1. While adverse parental styles, maladaptive emotion regulation strategies, and negative perfectionism each exerted direct influences on OCPD traits, and three chained mediation pathways — linking adverse parenting styles through maladaptive emotion regulation (p = 0.011), negative perfectionism (p = 0.001) and from negative perfectionism to maladaptive emotion regulation (p = 0.012) — significantly impacted OCPD features (Figure 3), it is important to note that Model 2 did not adequately fit the data, as indicated by model fit indices falling short of the established criteria.
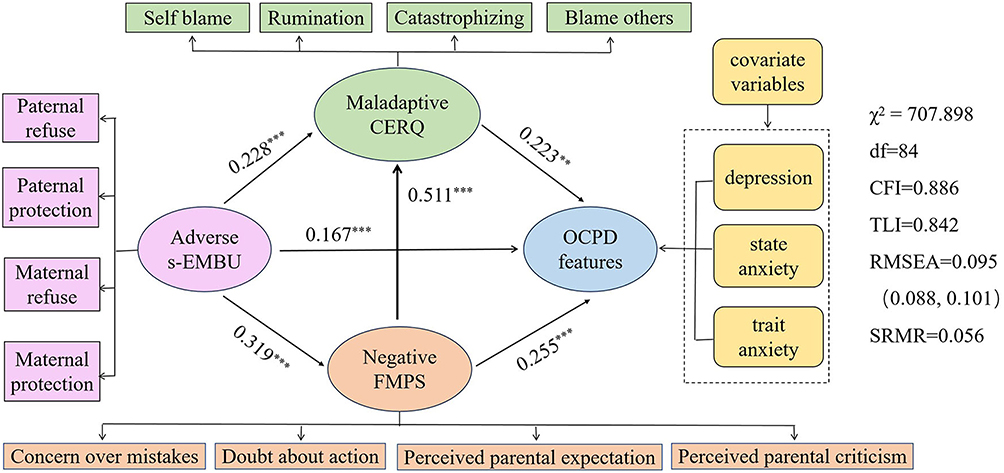 |
Figure 3 Model 2: The influencing direction of maladaptive CERQ and negative FMPS was different compared to hypothetical Model 2. **p<0.01, ***p<0.001. Abbreviations: s-EMBU, short-form Egna Minnenav Barndoms Uppfostran; CERQ, Cognitive Emotion Regulation Questionnaire; FMPS, Frost Multidimensional Perfectionism Scale; OCPD, obsessive-compulsive personality disorder. |
For hypothetical Model 3, a path from maladaptive emotion regulation to negative perfectionism was added to Model 1, results showed that all the model fit indices achieved the criterion, suggesting the hypothesis model fitted the data well (see Figure 4). Adverse parental styles (p < 0.001), maladaptive emotion regulation (p = 0.003), and negative perfectionism (p = 0.001) all had direct effect on OCPD features, and there were three chained mediation pathways significantly affecting OCPD features from adverse parental rearing through maladaptive emotion regulation and/or negative perfectionism (empirical 95% confidence interval did not overlap with zero; Figure 4 and Table 4). The direct path from adverse parental styles to OCPD features was significant (β = 0.160, p < 0.001, effect size = 47.34%). The indirect effect of adverse parental styles on OCPD features was not only through maladaptive emotion regulation (β = 0.085, p = 0.007, effect size = 25.15%) or negative perfectionism (β = 0.052, p = 0.012, effect size = 15.38%), but also mediated from maladaptive emotion regulation to negative perfectionism (β = 0.041, p = 0.006, effect size = 12.13%).
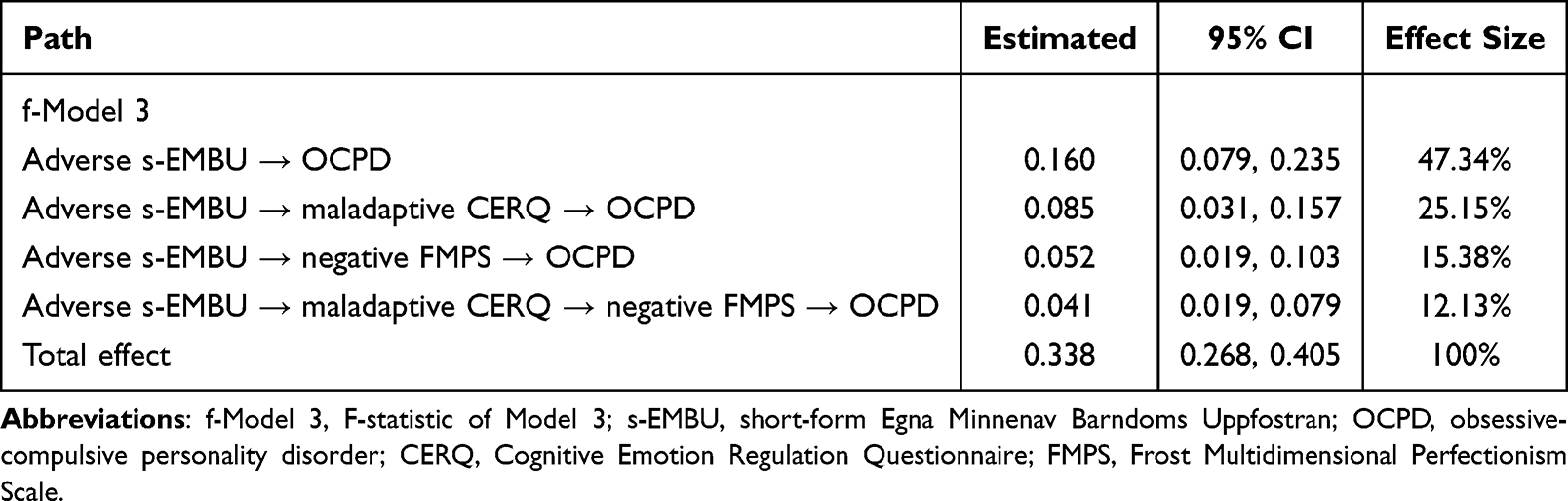 |
Table 4 Standardized Indirect Effects and 95% Confidence Interval |
 |
Figure 4 Model 3: A path from maladaptive CERQ to negative FMPS was added on the basis of hypothetical Model 1. **p<0.01, ***p<0.001. Abbreviations: s-EMBU, short-form Egna Minnenav Barndoms Uppfostran; CERQ, Cognitive Emotion Regulation Questionnaire; FMPS, negative Frost Multidimensional Perfectionism Scale; OCPD, obsessive-compulsive personality disorder. |
Discussion
This study examined the underlying mechanisms of adverse parental styles on OCPD traits by investigating the mediating roles of maladaptive emotion regulation and/or negative perfectionism. This study not only confirms the direct effect of adverse parental rearing on OCPD features but, more importantly, reveals a significant chain mediating pathway. The core finding indicates that adverse parental rearing impairs an individual’s emotion regulation capacity, which in turn increases the level of negative perfectionism, ultimately leading to the development of OCPD features. This result elucidates a potential psychological mechanism and temporal sequence underlying this relationship, providing a more nuanced understanding of how maladaptive parenting practices contribute to OCPD pathology.
This study revealed that individuals in SP-OCPD group reported more adverse paternal and maternal styles than those in SN-OCPD group. Furthermore, it provided evidence supporting a direct effect of adverse parental rearing on OCPD features, which confirmed and extended prior studies. Adverse parenting patterns—characterized by low emotional warmth, high criticism, and overprotection—may disrupt the development of a secure base and age-appropriate autonomy. This potentially fosters a rigid cognitive style and an excessive need for control in offspring, which are core characteristics of OCPD. For example, Ibarra et al discovered a positive association between maternal overprotection and obsession-compulsion symptom.38 Another study indicated that the cluster C personality disorders were significantly linked to parental rearing styles, characterized by lower care and higher protection.39 Additionally, research has shown that success factors (eg harmonious relationships) within the family environment are significantly negatively correlated with OCPD as diagnosed by the Personality Diagnositc Questionnaire.3 These findings represent that adverse parental rearing has an impact on the characteristics of OCPD.
In addition to the direct effect, this study also found that the adverse parenting bonding affecting OCPD features could be explained by three pathways through emotion dysregulation and/or negative perfectionism. The first mediation pathway through which adverse parenting rearing affecting OCPD features was maladaptive emotion regulation. SP-OCPD individuals are prone to utilizing maladaptive ER strategies in response to negative or stressful events, including rumination, catastrophizing, and both other-blame and self-blame tendencies.13 Poor patent-child relationships may increase the likelihood of disrupted emotional development, potentially leading to impaired ER capacities.40 Thus, adverse parental bonding may impair emotion regulation under stress, leading to rumination, blame attribution, and heightened negative affect. This persistent regulatory effort depletes cognitive resources and heightens emotional distress, which may directly manifest as OCPD features such as rigid control, preoccupation with details, and reluctance to delegate, as individuals over-compensate through behavioral and cognitive restraint to manage internal chaos.41 Prior research suggests OCPD individuals often suppress emotions yet display intense outbursts when distressed.42 To sum up, emotion dysregulation may constitute one of the developmental pathways from adverse parental styles to OCPD features.
The second mediating factor through which adverse parental bonding influences OCPD traits was negative perfectionism. Although the effect size for the specific indirect pathway from adverse parenting to OCPD traits via negative perfectionism was relatively small (β = 0.052), it remains theoretically and clinically noteworthy. In the multifactorial etiology of OCPD, most individual pathways are likely to demonstrate small effects, as the disorder arises from a confluence of numerous genetic, environmental, and psychological factors. The identification of any significant pathway provides a valuable piece of the etiological puzzle. Prior research has demonstrated that parental overprotection is positively correlated with various maladaptive outcomes in children,43 including obsessive-compulsive symptoms.44 Specifically, parenting styles shape an individual’s self-efficacy in decision-making and exacerbate an excessive fear of failure,45 as excessive parental control often conveys implicit messages emphasizing unrealistically high standards and an aversion to mistakes.46 Mechanistically, when parents habitually intervene to resolve their child’s challenges or eliminate obstacles, the child may adopt perfectionistic behaviors as a compensatory strategy. This tendency serves to mitigate feelings of inadequacy, prevent perceived rejection or abandonment, and foster a sense of social acceptance and belonging.47 These perfectionistic cognitions directly contribute to OCPD core traits, including perfectionism that interferes with task completion, excessive devotion to work, and inflexibility regarding moral issues.2 In a word, negative perfectionism mediates the effect of adverse parental bonding on OCPD traits to a certain extent.
The final mediation pathway through which adverse parenting styles influenced OCPD traits involved maladaptive emotion regulation, followed by negative perfectionism. Notably, the path coefficient from maladaptive emotion regulation to negative perfectionism was particularly strong (β = 0.477), underscoring the substantial mediating role of these sequential factors. These findings align with and extend upon Mentalization Theory’s framework of personality development, demonstrating how maladaptive emotion regulation and negative perfectionism collectively mediate the relationship between adverse parenting and OCPD traits. Our results provide empirical support for the theoretical proposition that while adverse parent-child relationships constitute a significant developmental risk factor, they represent neither a necessary nor sufficient condition for OCPD pathogenesis. The emergence of OCPD traits involves complex transactional processes wherein predisposing factors interact with maladaptive contextual features through mediating psychological mechanisms. A supportive parent-child relationship fosters individuals’ ability to interpret their own and others’ mental states, enhances emotional regulation skills and cultivates healthy perfectionism.48 Conversely, individuals exposed to adverse parenting styles often lack adaptive strategies to modulate emotional intensity or duration and may struggle to engage in goal‐directed behaviors during distress.49 Such maladaptive parenting can disrupt the formation of secure emotional bonds, leading to heightened sensitivity to imperfection, excessive preoccupancy with others’ expectations, and perennial concerns about committing errors.50 In the theoretical justification, contemporary developmental psychopathology frameworks posit that emotion regulation capacities emerge earlier than cognitive schemas like perfectionism.51 And childhood emotion dysregulation predicts later maladaptive perfectionism.52 Empirical evidence indicates that overcontrolling parenting styles are significantly associated with maladaptive emotion regulation strategies, particularly catastrophizing and external blame attribution.40 These dysfunctional coping mechanisms may exacerbate negative emotional experiences and increase emotional instability in individuals with adverse rearing, potentially contributing to the development of perfectionistic concerns and OCPD features.
Our findings highlight several key clinical implications. First, parental rearing styles significantly influence the development of OCPD traits, with our results identifying maladaptive emotion regulation and negative perfectionism as key mediating mechanisms. This suggests that early interventions targeting these specific factors may help mitigate the risk of developing OCPD pathology. Second, given their role in perpetuating OCPD features, maladaptive emotion regulation strategies represent critical early intervention targets. Cognitive behavior therapy may be particularly effective at this stage, as it helps individuals with OCPD recognize dysfunctional regulatory patterns, reframe them adaptively, and implement healthier behavioral responses.
This study has several limitations that warrant consideration. First, as a cross-sectional design, it cannot establish causal relationships among adverse parenting, maladaptive emotion regulation, negative perfectionism, and OCPD traits. Longitudinal studies are needed to clarify these dynamics. Second, all psychological variables were assessed via self-report measures, which may introduce bias. Future research should incorporate objective assessments (eg, structured clinical interviews, behavioral tasks) to enhance validity. Third, the sample consisted of a general population, limiting generalizability to clinical OCPD cohorts. Replication in diagnosed individuals is essential. Fourth, the interpretation of these findings must be tempered with cultural sensitivity, as parenting norms and the expression of emotions vary substantially across societies. Future research should prioritize cross-cultural comparisons to disentangle the universal from culture-specific pathways in the development of OCPD features. Finally, while maladaptive emotion regulation and negative perfectionism partially mediated the link between adverse parenting and OCPD, additional mediating mechanisms (eg, attachment styles, cognitive flexibility) should be explored to fully elucidate this pathway.
Conclusions
These findings demonstrate that adverse parenting influences OCPD development through both direct and indirect psychological pathways. The predominant mechanism involves the sequential mediation of maladaptive emotion regulation followed by negative perfectionism, suggesting that early emotional dysregulation may establish cognitive frameworks conducive to perfectionist thinking patterns. This study makes a significant contribution to personality disorder research by identifying and testing a sequential affective-cognitive mediation pathway in a non-clinical sample, thereby highlighting potential early developmental mechanisms that may precede clinical OCPD diagnosis. However, it is important to note that the cross-sectional nature of our data precludes definitive causal inferences. The proposed directional pathways, while theoretically grounded and statistically supported, require verification through longitudinal or experimental designs to confirm the temporal sequence and causal relationships among the variables. These results highlight actionable intervention targets for at-risk youth; specifically, evidence-based programs focusing on enhancing emotion regulation skills (eg, mindfulness-based emotion regulation training) and modifying maladaptive perfectionism (eg, cognitive-behavioral therapy for perfectionism) could disrupt this pathological cascade. Furthermore, broader implications extend beyond individual-level therapy to include community-based psychoeducational initiatives and parenting intervention programs designed to promote adaptive rearing practices and reduce early adverse experiences.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Ethical Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Jiangxi Normal University.
Informed Consent
Prior to their participation in the study, all participants provided written informed consent. This consent form comprehensively outlined the study procedures and explicitly stated that the collected data would be used for academic research and publication. All participants were assured of the confidentiality and anonymity of their data.
Acknowledgments
The authors would like to thank all the participants and their families for their support.
Funding
This project supported by Jiangxi Provincial Natural Science Foundation. Grant number: 20242BAB20276.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
2. Reinhardt P, Ellbin S, Carlander A, Hadzibajramovic E, Jonsdottir IH, Bagge AL. Is the road to burnout paved with perfectionism? The prevalence of obsessive-compulsive personality disorder in a clinical longitudinal sample of female patients with stress-related exhaustion. J Clin Psychol. 2024;80(2):391–13. doi:10.1002/jclp.23617
3. Hui L, Xiting H, Gang D, Youguo C, Xiaogang W. A cross-sectional study of Chinese college students’ personality disorders. J Psychol Sci. 2008;02:277–281. doi:10.16719/j.cnki.1671-6981.2008.02.059
4. Mervo B, Demetrovics Z, Kun B. Role of Obsessive-Compulsive Personality Disorder in work addiction, burnout and physical health. J Behav Addict. 2023;12:103.
5. Cheng HG, Huang YQ, Liu ZR, Liu BH. Associations linking parenting styles and offspring personality disorder are moderated by parental personality disorder, evidence from China. Psychiatry Res. 2011;189(1):105–109. doi:10.1016/j.psychres.2010.12.006
6. Brander G, Rydell M, Kuja-Halkola R, et al. Association of perinatal risk factors with obsessive-compulsive disorder: a population-based Birth cohort, sibling control study. JAMA Psychiatry. 2016;73(11):1135–1144. doi:10.1001/jamapsychiatry.2016.2095
7. Kidd KN, Prasad D, Cunningham JEA, Cardoso TD, Frey BN. The relationship between parental bonding and mood, anxiety and related disorders in adulthood: a systematic review and meta-analysis. J Affect Disord. 2022;307:221–236. doi:10.1016/j.jad.2022.03.069
8. Brander G, Pérez-Vigil A, Larsson H, Mataix-Cols D. Systematic review of environmental risk factors for Obsessive-Compulsive Disorder: a proposed roadmap from association to causation. Neurosci Biobehav Rev. 2016;65:36–62. doi:10.1016/j.neubiorev.2016.03.011
9. Huang XT, Ling H, Yang BJ, Dou G. Screening of personality disorders among Chinese college students by personality diagnostic questionnaire-4+. J Pers Disord. 2007;21(4):448–454. doi:10.1521/pedi.2007.21.4.448
10. Lee HJ, Mendoza NB. Does parental support amplify growth mindset predictions for student achievement and persistence? Cross-cultural findings from 76 countries/regions. Soc Psychol Educ. 2025;28(1):88. doi:10.1007/s11218-025-10038-4
11. Cole PM, Ramsook KA, Ram N. Emotion dysregulation as a dynamic process. Dev Psychopathol. 2019;31(3):1191–1201. doi:10.1017/S0954579419000695
12. Fitzpatrick S, Dixon-Gordon KL, Turner CJ, Chen SX, Chapman A. Emotion dysregulation in personality disorders. Curr Psychiatry Rep. 2023;25(5):223–231. doi:10.1007/s11920-023-01418-8
13. Steenkamp MM, Suvak MK, Dickstein BD, Shea MT, Litz BT. Emotional functioning in obsessive-compulsive personality disorder: comparison to borderline personality disorder and healthy controls. J Pers Disord. 2015;29(6):794–808. doi:10.1521/pedi_2014_28_174
14. Edwards E, Leahy R, Snyder S. Patterns of emotional schema endorsement and personality disorder symptoms among outpatient psychotherapy clients. Motiv Emot. 2023;47(3):412–422. doi:10.1007/s11031-022-10000-3
15. Khaleghi M, Leahy RL, Akbari E, Mohammadkhani S, Hasani J, Tayyebi A. Emotional schema therapy for generalized anxiety disorder: a single-subject design. Int J Cogn Ther. 2017;10(4):269–282. doi:10.1521/ijct.2017.10.4.269
16. Morvaridi M, Mashhadi A, Shamloo ZS, Leahy RL. The effectiveness of group emotional schema therapy on emotional regulation and social anxiety symptoms. Int J Cogn Ther. 2019;12(1):16–24. doi:10.1007/s41811-018-0037-6
17. Frost RO, Marten P, Lahart C, Rosenblate R. The dimensions of perfectionism. Cognit Ther Res. 1990;14(5):449–468. doi:10.1007/BF01172967
18. Sametoglu S, Denissen JJA, De Clercq B, De Caluwe E. Towards a better understanding of adolescent obsessive-compulsive personality traits and obsessive-compulsive symptoms from growth trajectories of perfectionism. Dev Psychopathol. 2022;34(4):1468–1476. doi:10.1017/S0954579421000195
19. Cheli S, MacBeth A, Popolo R, Dimaggio G. The intertwined path of perfectionism and self-criticism in a client with obsessive-compulsive personality disorder. J Clin Psychol. 2020;76(11):2055–2066. doi:10.1002/jclp.23051
20. Mansur-Alves M, Machado GM, Rodrigues WDS, Neufeld CB, Carvalho LDF. Perfectionism dimensions: a network analysis of their relationships with affect and obsessive-compulsive pathological personality traits. Scand J Psychol. 2022;63(3):165–172. doi:10.1111/sjop.12798
21. Rademacher A, Zumbach J, Koglin U. Parenting style and child aggressive behavior from preschool to elementary school: the mediating effect of emotion dysregulation. Early Child Educ J. 2025;53(1):63–72. doi:10.1007/s10643-023-01560-1
22. Feng LL, Zhang LL, Zhong H. Perceived parenting styles and mental health: the multiple mediation eEffect of perfectionism and altruistic behavior. Psychol Res Behav Manag. 2021;14:1157–1170. doi:10.2147/PRBM.S318446
23. Peng WR, Liu ZX, Liu Q, et al. Insecure attachment and maladaptive emotion regulation mediating the relationship between childhood trauma and borderline personality features. Depress Anxiety. 2021;38(1):28–39. doi:10.1002/da.23082
24. Hyler SE, Skodol AE, Oldham JM, Kellman HD, Doidge N. Validity of the Personality Diagnostic Questionnaire-Revised: a replication in an outpatient sample. Compr Psychiatry. 1992;33(2):73–77. doi:10.1016/0010-440X(92)90001-7
25. Yang J, Bagby M, Costa PT, Ryder AG, Herbst JH. Assessing the DSM-IV structure of personality disorder with a sample of Chinese psychiatric patients. J Pers Disord. 2002;16(4):317–331. doi:10.1521/pedi.16.4.317.24127
26. Perris C, Jacobsson L, Lindstrom H, von Knorring L, Perris H. Development of a new inventory assessing memories of parental rearing behaviour. Acta Psychiatr Scand. 1980;61(4):265–274. doi:10.1111/j.1600-0447.1980.tb00581.x
27. Jiang J, Zhengrong L, Bijing J, Yan X. Revision of the short-form Egna Minnenav Barndoms Uppfostran for Chinese. Psychol Dev Educ. 2010;26(1):94–99. doi:10.16187/j.cnki.issn1001-4918.2010.01.017
28. Garnefski N, Kraaij V, Spinhoven P. Negative life events, cognitive emotion regulation and emotional problems. Pers Individ Dif. 2001;30(8):1311–1327. doi:10.1016/S0191-8869(00)00113-6
29. Zhu X, Auerbach RP, Yao S, Abela JRZ, Xiao J, Tong X. Psychometric properties of the Cognitive Emotion Regulation Questionnaire: Chinese version. Cogn Emot. 2008;22(2):288–307. doi:10.1371/journal.pone.0150206
30. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
31. Spielberger CD. Manual for the State–Trait Anxiety Inventory (Form Y). Palo Alto, CA: Consulting Psychologists Press; 1983.
32. Shek DT. The Chinese version of the State-Trait Anxiety Inventory: its relationship to different measures of psychological well-being. J Clin Psychol. 1993;49(3):349–358. doi:10.1002/1097-4679(199305)49:3<349::aid-jclp2270490308>3.0.co;2-j
33. Adler NE, Ostrove JM. Socioeconomic status and health: what we know and what we don’t. Ann N Y Acad Sci. 1999;896(1):3–15. doi:10.1111/j.1749-6632.1999.tb08101.x
34. Tianyu C, Shuqiao Y, Liangwei X. Validity and reliability of the Chinese version of the Subjective Socioeconomic Status Scale in a general adult population. Chin Ment Health J. 2014;28(11):869–874.
35. Cheung GW, Lau RS. Testing mediation and suppression effects of latent variables - Bootstrapping with structural equation models. Organ Res Methods. 2008;11(2):296–325. doi:10.1177/1094428107300343
36. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
37. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. 1981;24(2):337–346. doi:10.2307/3151312
38. Ibarra P, Alemany S, Fatjó-Vilas M, et al. The BDNF-Val66Met polymorphism modulates parental rearing effects on adult psychiatric symptoms: a community twin-based study. Eur Pshychiatry. 2014;29(5):293–300. doi:10.1016/j.eurpsy.2014.03.001
39. Timmerman IGH, Emmelkamp PMG. Parental rearing styles and personality disorders in prisoners and forensic patients. Clin Psychol Psychother. 2005;12(3):191–200. doi:10.1002/cpp.449
40. Tani F, Pascuzzi D, Raffagnino R. The relationship between perceived parenting style and emotion regulation abilities in adulthood. J Adult Dev. 2018;25(1):1–12. doi:10.1007/s10804-017-9269-6
41. Esfahan MM, Ayasrah MN, Ghayoumi F, Motaharinasab A, Tayim N, Aghaei Z. The network structure of relationship obsessive-compulsive disorder presentations: the interplay between ROCD symptoms with maladaptive and non-maladaptive personality traits. Psychiatr Q. 2024;95(3):321–339. doi:10.1007/s11126-024-10079-6
42. Hengartner MP, Müller M, Rodgers S, Rössler W, Ajdacic-Gross V. Can protective factors moderate the detrimental effects of child maltreatment on personality functioning? J Psychiatr Res. 2013;47(9):1180–1186. doi:10.1016/j.jpsychires.2013.05.005
43. Raffagnato A, Angelico C, Fasolato R, Sale E, Gatta M, Miscioscia M. Parental bonding and children’s psychopathology: a transgenerational view point. Children-Basel. 2021;8(11):1012. doi:10.3390/children8111012
44. Goli E, Abdekhodaie MS, Mashhadi A, Bigdeli I. The role of parent-child interaction patterns in the development of obsessive-compulsive disorder: a literature review study. J Fundam Ment Heal. 2020;22(1):5–20.
45. Hibbard DR, Walton GE. Exploring the development of perfectionism: the influence of parenting style and gender. Soc Behav Pers. 2014;42(2):269–278. doi:10.2224/sbp.2014.42.2.269
46. Hayes KN, Turner LA. The relation of helicopter parenting to maladaptive perfectionism in emerging adults. J Fam Issues. 2021;42(12):2986–3000. doi:10.1177/0192513X21993194
47. Hewitt PL. Perfecting, belonging, and repairing: a dynamic-relational approach to perfectionism. Can Psychol Can. 2020;61(2):101–110. doi:10.1037/cap0000209
48. Ricker BT, Sanchez CR, Cooley JL, Barnett JE, Gunder EM. Interactive effects of parental support and psychological control on children’s emotion regulation. J Fam Psychol. 2024;38(6):956–965. doi:10.1037/fam0001235
49. Singh P. Emotion regulation difficulties, perceived parenting and personality as predictors of health-risk behaviours among adolescents. Curr Psychol. 2023;42(15):12896–12911. doi:10.1007/s12144-021-02536-3
50. Brás M, Antunes J, Reis A, Carmo C. Perfectionism and emotion regulation in the study of suicidal ideation in Portuguese young adults. Behav Sci. 2024;14(9):846. doi:10.3390/bs14090846
51. Milojevich HM, Norwalk KE, Sheridan MA. Deprivation and threat, emotion dysregulation, and psychopathology: concurrent and longitudinal associations. Dev Psychopathol. 2019;31(3):847–857. doi:10.1017/S0954579419000294
52. Malivoire BL, Kuo JR, Antony MM. An examination of emotion dysregulation in maladaptive perfectionism. Clin Psychol Rev. 2019;71:39–50. doi:10.1016/j.cpr.2019.04.006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.