Back to Journals » Clinical Ophthalmology » Volume 20
Measurement of Acute Intraocular Pressure Elevation Immediately After Intravitreal Anti-VEGF Injection and Analysis of Prefilled Syringe Accuracy
Received 17 December 2025
Accepted for publication 24 February 2026
Published 4 March 2026 Volume 2026:20 589783
DOI https://doi.org/10.2147/OPTH.S589783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Kaku Itoh, Misaki Negishi
Departments of Ophthalmology, Muroran City General Hospital, Muroran City, Hokkaido, Japan
Correspondence: Kaku Itoh, Departments of Ophthalmology, Muroran City General Hospital, 3-8-1 Yamate-cho, Muroran City, Hokkaido, Japan, Tel +81-143-25-3111, Fax +81-143-22-6867, Email [email protected]
Purpose: To compare and evaluate, across different agents, the risk of intraocular pressure (IOP) elevation after anti-VEGF therapy and the accuracy of prefilled syringes.
Methods: Total of 175 eyes treated with anti-VEGF drugs were enrolled for this study. An accuracy evaluation of the prefilled syringes was conducted involving 25 participants, comprising 17 physicians and 8 nurses. The anti-VEGF agents including aflibercept 2 mg, aflibercept 8 mg, brolucizumab, faricimab, and ranibizumab-BS were assessed. IOP was measured before, and at 1 and 15 minutes after intravitreal injection, and analyzed separately for each drug. Furthermore, prefilled syringes of aflibercept 2 mg, brolucizumab, and ranibizumab-BS, as well as 1-mL syringes filled with saline solution, were equipped with 30-gauge needles, followed by careful removal of air. The weight of the saline discharged according to the scale marking was measured using an electronic balance.
Results: At 1 min after intravitreal injection, the IOP was highest in the aflibercept 2 mg group, with a mean value of 52.8 mmHg. A mild inverse correlation was observed between axial length and IOP elevation at 1 min post-injection, suggesting that eyes with longer axial length exhibited less pronounced IOP increases. In the syringe accuracy analysis, the prefilled syringe of aflibercept 2 mg expelled a significantly larger volume, with a mean of approximately 0.076 mL, compared to other prefilled syringes.
Conclusion: Intravitreal injection using the aflibercept 2 mg prefilled syringe may deliver approximately 1.5 times the intended volume into the eye. This may raise safety concerns, such as the risk of transient vision loss due to marked immediate IOP elevation, and may also affect clinical outcomes and the validity of clinical trials.
Keywords: anti-VEGFs, IOP elevation, syringe accuracy
Introduction
Intravitreal anti-VEGF injection (IVI) has become the gold standard treatment for several retinal vascular diseases, including neovascular age-related macular degeneration (nAMD), diabetic macular edema (DME), retinal vein occlusion (RVO), and myopic choroidal neovascularization (mCNV).1–5 Pegaptanib was first approved by the FDA for the treatment of nAMD in 2004, but was discontinued in 2019. The era of anti-VEGF therapy was ushered in with the sequential introduction of ranibizumab in 2006; aflibercept-2mg in 2012; brolucizumab in 2019; and faricimab, which is a bispecific antibody for angiopoietin 2 and VEGF-A, in 2022. Ranibizumab-nuna or ranibizumab-BS is a biosimilar and more affordable formulation that approved in 2021. In 2024, the use of aflibercept 8 mg was approved, further offering more treatment options. Aflibercept 2 mg, brolucizumab, and ranibizumab-BS can be administered using prefilled syringes (PFS) for greater convenience.
Anti-VEGF therapy is widely favored because of its high therapeutic efficacy, safety, and simplicity.6–8 However, serious side effects, including local ophthalmic complications, such as endophthalmitis, vitreous hemorrhage, and retinal detachment, as well as vascular occlusive mechanisms that lead to systemic complications, such as transient visual loss (TVL) and central retinal artery occlusion, have been reported in a very small number of cases.1,9–12 One frequently reported complication is acute elevation of intraocular pressure (IOP) immediately after IVI; in some patients, IOP exceeding 50 mmHg, and all reported events were verified by measurements taken 5–10 min after IVI. In most patients, IOP returned to baseline within 30 min after IVI.13–15
We rarely encounter patients who complain of TVL immediately after IVI and recover after emergency anterior chamber puncture to gradually lower the IOP. This may be explained by an immediate but transient increase in IOP that exceeds the ocular artery pressure after IVI. Ocular artery occlusion directly affects the prognosis of visual function and is one of the most important complications to avoid.
Most currently available anti-VEGF drugs are injected into the eye at a volume of 0.05 mL. However, aflibercept 8 mg needs to be injected at a volume of 0.07 mL, raising concerns about the risk of IOP elevation. Previous reports have indicated that in approximately 45% patients, intravitreal administration of 0.07 mL pegaptanib increased IOP to >50 mmHg within 2 min.16 Although PFS are considered to enable more accurate delivery of injection volume, we could not identify any studies that have specifically evaluated their actual accuracy. In this study, we aimed to improve the risk assessment of elevated IOP after anti-VEGF therapy and to examine the accuracy of PFS, considering that IOP increase is assumed to depend on injection volume.
Materials and Methods
This study was approved by the institutional review board of Muroran City General Hospital, Japan (approved number: 2024–04), and was performed according to the the Declaration of Helsinki tenets and national laws for the protection of personal data. Informed consent was obtained from all study participants from April 2024 to March 2025.
Anti-VEGF Injection
In this study, the anti-VEGF agents including aflibercept 2 mg, aflibercept-8 mg, brolucizumab, faricimab, and ranibizumab-BS were assessed. Among them, aflibercept 2 mg, brolucizumab, and ranibizumab-BS were packed in PFS equipped with 30G needles. Conversely, aflibercept 8 mg and faricimab were in vial preparations and administered using 1-mL tuberculin syringes equipped with 30G needles. Each anti-VEGF agent was injected into the vitreous body. The PFS formulations were adjusted to the specified dose using scale markings. For the vial formulations, 0.07 mL of aflibercept 8 mg and 0.05 mL of faricimab were measured and injected.
Biometric Measurement
IOP was measured by a handheld tonometer (iCare IC200; iCare Finland Oy) using an impact rebound technique. The probe was positioned 5–7 mm in front of the cornea, and six consecutive measurements were performed. The software excluded the highest and lowest IOP readings and automatically generated the average of the remaining four readings. The average IOP was recorded. IOP was measured before and after IVI at 1 and 15 min. All measurements were performed in a sitting position by an orthoptist. In addition, the axial length was measured using non-optical devices prior to the IOP measurement.
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured before IVI. The mean arterial blood pressure (MABP) was calculated as 1/3 (SBP−DBP). The ocular perfusion pressure (OPP) was calculated as 2/3 (MABP−IOP).17 Patients in whom the IOP after IVI higher than the OPP were considered at high risk of TVL.
Analysis of the Accuracy of Prefilled Syringes
This study was conducted with 25 participants. Among them, only three were ophthalmologists in order to emphasize the importance of IOP measurements by staff members without preconceived notions.
Thoroughly cleaned and used PFS and container samples were used in this study. A total of five PFS each of aflibercept 2 mg and ranibizumab-BS were prepared, and the examiners were asked to select them randomly. In addition, twenty-five unused PFS of brolucizumab were prepared. The PFS was filled with saline solution, which had a specific gravity of 1.004, and fitted with a 30G needle, followed by careful removal of air. The weight of the saline discharged according to the scale marking was measured using an electronic balance. Similarly, 1-mL tuberculin syringes (Terumo) were filled with saline solution and fitted with a 30G needle. Saline volumes of 0.05, 0.07, and 0.10 mL were measured and discharged, and weight was recorded.
Statistical Analysis
All statistical analyses were performed using GraphPad Prism 7 (GraphPad Software, San Diego, CA, USA). The anti-VEGF drugs were compared in terms of age, axial length, and IOP parameters using one-way analysis of variance, and in terms of sex using chi-square test. The correlation between IOP and axial length was determined using by Pearson’s coefficient. Statistical significance was considered for P values <0.05.
Results
Patients
During the study period, total of 175 eyes diagnosed with nAMD, RVO, DME, or mCNV and treated with anti-VEGF drugs as the preferred approach were enrolled. The background characteristics of the study population are summarized in Table 1. Overall, most patients were men, but there were more women than men in the ranibizumab-BS group. Selection bias may have been introduced, considering that ranibizumab-BS was used as first-line treatment for mCNV and that group comprised a relatively high proportion of eyes with longer axial length.
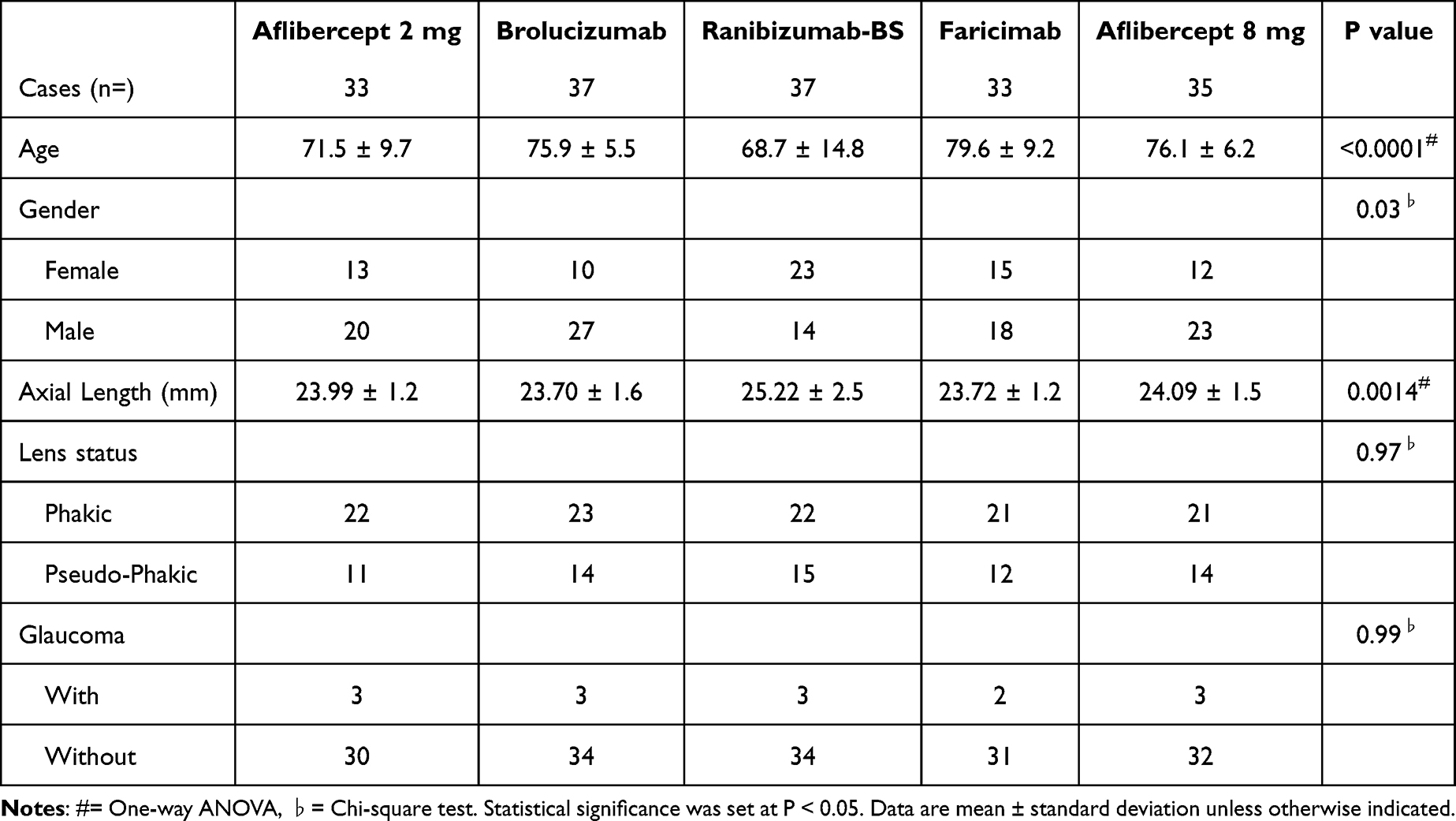 |
Table 1 Baseline Characteristics |
Comparison of IOP Changes Among Different IVI Medications
IOP fluctuations before and after IVI using the different drugs are presented in Figure 1.
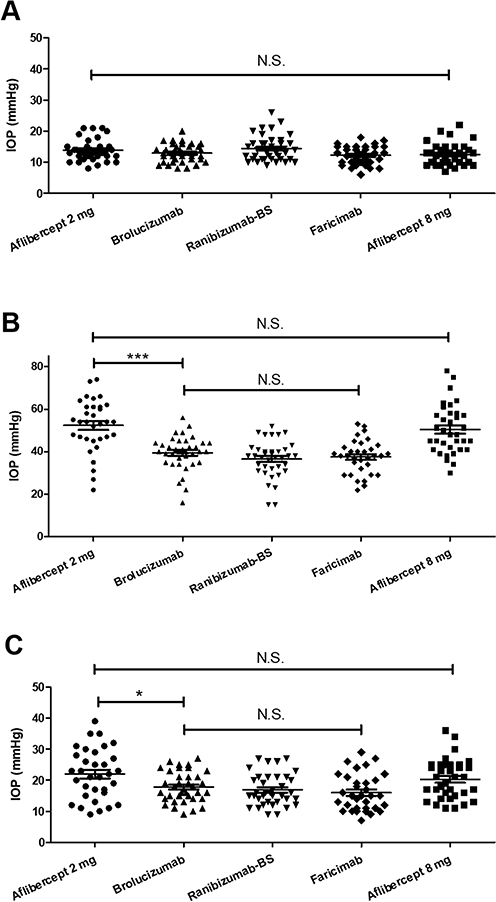 |
Figure 1 Drug-specific IOP fluctuations before and after IVI. (A) The mean IOPs before IVI do not significantly differ among the drugs. (B) At 1 min after IVI, the mean IOP is highest in the aflibercept 2 mg group (52.4 mmHg), but is not significantly different from that in the aflibercept 8 mg group (50.5 mmHg). Conversely, the mean IOPs are significantly lower in the Brolucizumab (36.4 mmHg), ranibizumab-BS (36.5 mmHg), and faricimab (37.5 mmHg) groups. (C) At 15 min after IVI, the mean IOP is seen to decrease in most patients. (*P < 0.05, ***P < 0.005. N.S., not statistically significant.). |
There were no significant differences in IOP among the groups before IVI. At 1 minute after IVI, the highest mean IOP was observed in the aflibercept 2 mg group (52.4 mmHg), which was similar to that in the aflibercept 8 mg group (50.5 mmHg), but was significantly higher than that in the brolucizumab (39.4 mmHg), ranibizumab-BS (36.5 mmHg), and faricimab (37.5 mmHg) groups. The notably small elevations in IOP (≤25 mmHg) in the graph in some patients were considered to be attributable to backflow immediately after IVI. Most patients exhibited IOP reduction 15 min after IVI, but the decrease was relatively mild in the aflibercept groups, which may be attribute to the relatively high IOP elevation 1 min after IVI.
The IOP after IVI exceeded the OPP in the aflibercept 2 mg (n = 2 eyes) and 8 mg (n = 2 eyes) groups. No emergent procedures, including anterior chamber paracentesis, were required, because none of these patients reported subjective symptoms, such as visual blackout. Furthermore, no difference in intraocular pressure elevation was observed based on the presence or absence of glaucoma treatment.
Correlation Between 1-Minute Post-IVI IOP and Axial Length
As demonstrated in Figure 2, there was a negative correlation between IOP at 1 min post-IVI and axial length (r = −0.23, P = 0.0018). Our result showed that a longer axial length, which can indicate large ocular volume, was associated with a small elevation in IOP immediately after IVI. Based on these results, the ranibizumab BS group may exhibit bias in IOP fluctuations attributable to axial length, as it includes a higher proportion of eyes with long axial length.
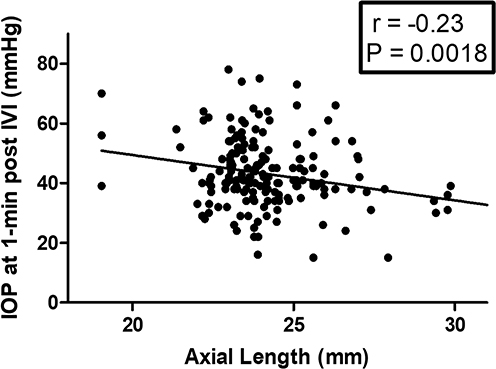 |
Figure 2 Association between IOP at 1 min post-IVI and axial length. There is a negative correlation between IOP at 1 min post-IVI and axial length (r = −0.23, P = 0.0018). |
Evaluation of the Accuracy of Prefilled and 1-mL Tuberculin Syringes
As shown in Figure 3, the PFS of aflibercept 2 mg delivered an average dose of 0.076 g (approximately 0.076 mL), which was not significantly different from the discharge volume when using a 1-mL tuberculin syringe targeting 0.07 mL (mean 0.075 mL). Compared with aflibercept 2 mg PFS, the PFS of other medications delivered smaller mean volumes (0.057 mL for brolucizumab and 0.048 mL for ranibizumab-BS). These findings suggested that the PFS of aflibercept 2 mg may discharge approximately 1.5 times the intended volume (0.050 mL).
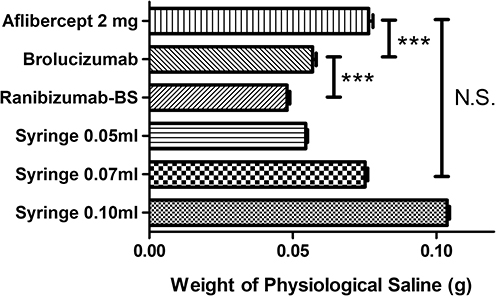 |
Figure 3 Evaluation of the accuracy of PFS and 1-mL tuberculin syringes. The mean reflux volumes from PFS are 0.076 mL for aflibercept 2 mg, 0.057 mL for brolucizumab, and 0.048 mL for ranibizumab-BS. The PFS volume of aflibercept 2mg is significantly greater than that of the other anti-VEGF drugs and is not significantly different from the target discharge volume of 0.07 mL using a 1-mL syringe. (***P < 0.005. N.S., not statistically significant.). |
Figure 4 shows the actual aflibercept 2 mg PFS used in Japan, but it was filled with saline for this study. The discharge volume was 0.076 mL when the plunger was aligned with the dome edge of the stopper at the mark, and 0.056 mL when the plunger was further advanced beyond the mark to reduce the volume.
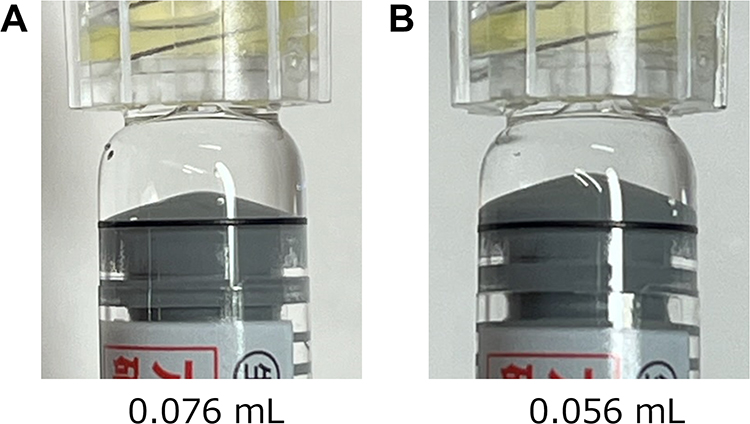 |
Figure 4 Photographs of saline-filled aflibercept 2 mg PFS used in Japan. (A) The plunger dome edge aligns with the reference mark on the syringe. Discharge from this position results in a reflux volume of 0.076 mL. (B) The plunger is positioned considerably beyond the reference mark on the syringe. Discharge from this position yields a reflux volume of 0.056 mL. |
Discussion
The number of reports on the relationship between IVI and IOP, particularly immediately after IVI, remain limited. Paris et al measured IOP 30 seconds after IVI and reported that IOP spike was smaller with faricimab than with aflibercept, and no significant difference was observed between the 2 and 8 mg doses of aflibercept.18 Furthermore, a relatively large ocular volume was reported to be associated with a relatively small magnitude of acute IOP elevation after IVI.19 These previously reported findings were generally consistent with the results of this study. Although multiple factors may contribute to IOP elevation after IVI including injection dynamics, reflux, needle design, and formulation characteristics such as viscosity, these results suggest that the primary determinant of post-injection IOP elevation may be the injection volume.
The use of PFS has become the predominant method of administration of contemporary anti-VEGF therapy. The reported advantages of PFS include procedural simplicity and reduced injection time, potential reduction in the risk of infectious endophthalmitis through simplified handling, and improved accuracy of the administered dose.6,7,20–22 However, compared with the vial formulation of aflibercept 2 mg, the PFS formulation has been reported to carry specific risks, including a higher likelihood of spike-like increases in IOP immediately after IVI and approximately 5-fold greater risk of transient visual acuity reduction.11,12,23 Possible explanations for these observations include the larger barrel diameter of the PFS compared with that of other formulations, which may increase the margin of error during dose alignment, and the lower injection force required, which may facilitate more rapid injection of the solution.11
The results of this study suggested that, on average, approximately 0.076 mL of aflibercept 2 mg is delivered into the eye when using PFS as research implications. This volume corresponds to approximately 1.5 times the prescribed dose of 0.050 mL. The volume overload resulting from this excessive drug delivery may account for the higher likelihood of IOP elevation compared with other agents, the comparable IOP increase after aflibercept 8 mg, and the previously discussed risks associated with PFS as clinical implications.
The potential impact on clinical outcomes resulting from inadvertent administration of approximately 3 mg of aflibercept when using the 2-mg PFS formulation is an additional concern. The Phase 3 PULSAR study reported that compared with the 2-mg formulation, the administration of 8 mg of aflibercept achieved extended treatment intervals in approximately 53% of patients with nAMD.24 Similarly, in the Phase 2/3 PHOTON study, treatment with aflibercept 8 mg in patients with DME demonstrated promising results on extended dosing intervals.25 These findings suggested that an increased delivered drug volume may influence clinical efficacy. Moreover, although numerous clinical trials, including head-to-head efficacy comparisons and noninferiority studies, on aflibercept 2 mg have been conducted, their results may have actually reflected clinical outcomes of an effective 3 mg dose, thereby, raising concerns about the validity of the findings.8,26–29 Although some variability in IVI volume due to procedural technique cannot be entirely excluded, it remains questionable whether an average overdose of 1.5 times the prescribed volume can be reasonably regarded as a tolerable margin of error. It is also concerning that, to date, many clinical studies of various scales using the aflibercept 2 mg formulation have not clearly specified whether the vial or the PFS was used, and some studies may have included a mixture of both. At the very least, when administering aflibercept 2 mg using PFS, care should be taken to avoid over alignment beyond the dosage mark, and clinicians should remain vigilant about the possibility of postoperative transient visual acuity reduction.
In conclusion, this study highlighted the association between IVI volume and immediate post-injection IOP, the potential risks inherent in IVI, and concerns regarding dosing accuracy of PFS, underscoring the importance of continued clinical vigilance. Limitations of this study include its single-center design, which inherently restricts the number of cases and the research environment. Additionally, the potential for case selection bias cannot be entirely excluded. Moreover, in studies utilizing spent PFS using physiological saline, it was difficult to adjust viscosity and temperature in the same manner as with actual pharmaceutical solutions. As novel formulations and PFS systems emerge in the future, further rigorous investigation is essential, not only regarding clinical efficacy, but also with respect to its accuracy and associated risks. Ultimately, the development and implementation of safer, more user friendly, and highly accurate treatment strategies remain critical objectives for advancing clinical practice.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
None of the authors has any conflicts of interest to disclose for this work.
References
1. Fung AE, Rosenfeld PJ, Reichel E. The international intravitreal bevacizumab safety survey: using the internet to assess drug safety worldwide. British J Ophthalmol. 2006;90(11):1344–8. doi:10.1136/bjo.2006.099598
2. Kim LA, D’Amore PA. A brief history of anti-VEGF for the treatment of ocular angiogenesis. Ame J Pathol. 2012;181(2):376–379. doi:10.1016/j.ajpath.2012.06.006
3. Campochiaro PA, Aiello LP, Rosenfeld PJ. Anti–vascular endothelial growth factor agents in the treatment of retinal disease. Ophthalmology. 2016;123(10):S78–s88. doi:10.1016/j.ophtha.2016.04.056
4. Luu KT, Seal J, Green M, Winskill C, Attar M. Effect of anti-VEGF therapy on the disease progression of neovascular age-related macular degeneration: a systematic review and model-based meta-analysis. J Clin Pharmacol. 2022;62(5):594–608. doi:10.1002/jcph.2002
5. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. New England J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
6. Lee DJ, Scruggs BA, Faridi A, Sánchez E, Thomas M. Survey of intravitreal injection outcomes amongst ophthalmologists using pre-filled aflibercept syringes. Clin Experim Ophthalmol. 2022;50(7):803–805. doi:10.1111/ceo.14125
7. Finkelstein M, Katz G, Zur D, Rubowitz A, Moisseiev E. The effect of syringe-filling technique on the risk for endophthalmitis after intravitreal injection of anti-VEGF agents. Ophthalmologica. 2022;245(1):34–40. doi:10.1159/000518236
8. Tadayoni R, Paris LP, Danzig CJ, et al. Efficacy and safety of faricimab for macular edema due to retinal vein occlusion: 24-week results from the BALATON and COMINO trials. Ophthalmology. 2024;131(8):950–960. doi:10.1016/j.ophtha.2024.01.029
9. Haug SJ, Hien DL, Uludag G, et al. Retinal arterial occlusive vasculitis following intravitreal brolucizumab administration. Ame J Ophthalmol Case Reports. 2020;18:100680. doi:10.1016/j.ajoc.2020.100680
10. Witkin AJ, Hahn P, Murray TG, et al. Occlusive retinal vasculitis following intravitreal brolucizumab. J Vitreoretinal Dis. 2020;4(4):269–279. doi:10.1177/2474126420930863
11. Lee DJ, Scruggs BA, Sánchez E, Thomas M, Faridi A. Transient vision loss associated with prefilled aflibercept syringes: a case series and analysis of injection force. Ophthalmol Sci. 2022;2(2):100115. doi:10.1016/j.xops.2022.100115
12. Klaas JE, Bui V, Maierhofer N, et al. Risk of transient vision loss after intravitreal aflibercept using vial-prepared vs. the novel prefilled syringe formulation. Front Med. 2023;10:1295633. doi:10.3389/fmed.2023.1295633
13. Kim JE, Mantravadi AV, Hur EY, Covert DJ. Short-term intraocular pressure changes immediately after intravitreal injections of anti–vascular endothelial growth factor agents. Am J Ophthalmol. 2008;146(6):930–4.e1. doi:10.1016/j.ajo.2008.07.007
14. Kampougeris G, Spyropoulos D, Mitropoulou A. Intraocular pressure rise after anti-VEGF treatment: prevalence, possible mechanisms and correlations. J Curr Glaucoma Prac. 2013;7(1):19–24. doi:10.5005/jp-journals-10008-1132
15. LoBue SA, Gindina S, Saba NJ, Chang T, Davis MJ, Fish S. Clinical features associated with acute elevated intraocular pressure after intravitreal anti-VEGF injections. Clin Ophthalmol. 2023;17:1683–1690. doi:10.2147/opth.S414212
16. Knip MM, Välimäki J. Effects of pegaptanib injections on intraocular pressure with and without anterior chamber paracentesis: a prospective study. Acta Ophthalmol. 2012;90(3):254–258. doi:10.1111/j.1755-3768.2010.01904.x
17. Nagaoka T, Sato E, Takahashi A, Yokota H, Sogawa K, Yoshida A. Impaired retinal circulation in patients with type 2 diabetes mellitus: retinal laser Doppler velocimetry study. Invest Ophthalmol Vis Sci. 2010;51(12):6729–6734. doi:10.1167/iovs.10-5364
18. Paris A, Volpe G, Perruchoud-Ader K, Casanova A, Menghini M, Grimaldi G. Short-term intraocular pressure changes after intravitreal aflibercept 2 mg, aflibercept 8 mg and faricimab: a prospective, comparative study. British J Ophthalmol. 2025;109(5):600–605. doi:10.1136/bjo-2024-326053
19. Koçak N, Gürpınar A, Yeter V. Effect of estimated individual vitreous volume on intraocular pressure spikes after intravitreal anti-vascular endothelial growth factors injection. Ophthalmic Res. 2024;1–15. doi:10.1159/000543071
20. Souied E, Nghiem-Buffet S, Leteneux C, et al. Ranibizumab prefilled syringes: benefits of reduced syringe preparation times and less complex preparation procedures. Euro J Ophthalmol. 2015;25(6):529–534. doi:10.5301/ejo.5000629
21. Sassalos TM, Paulus YM. Prefilled syringes for intravitreal drug delivery. Clin Ophthalmol. 2019;13:701–706. doi:10.2147/opth.S169044
22. Loewenstein I, Goldstein M, Moisseiev J, Moisseiev E. Accuracy and precision of intravitreal injections of anti–vascular endothelial growth factor agents in real life. Retina. 2019;39(7):1385–1391. doi:10.1097/iae.0000000000002170
23. Loscos-Giménez I, Rego-Lorca D, Bassaganyas-Vilarrasa F, Crespí-Vilimelis J, Díaz-Cascajosa J, Segarra JIV. New prefilled syringe aflibercept design. A cause of symptomatic IOP spike after aflibercept PFS? Romanian J Ophthalmol. 2024;68(3):219–224. doi:10.22336/rjo.2024.41
24. Lanzetta P, Korobelnik J-F, Heier JS, et al. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (PULSAR): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial. Lancet. 2024;403(10432):1141–1152. doi:10.1016/s0140-6736(24)00063-1
25. Brown DM, Boyer DS, Do DV, et al. Intravitreal aflibercept 8 mg in diabetic macular oedema (PHOTON): 48-week results from a randomised, double-masked, non-inferiority, phase 2/3 trial. Lancet. 2024;403(10432):1153–1163. doi:10.1016/s0140-6736(23)02577-1
26. Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. doi:10.1016/j.ophtha.2019.04.017
27. Brown DM, Wykoff CC, Boyer D, et al. Evaluation of intravitreal aflibercept for the treatment of severe nonproliferative diabetic retinopathy: results from the PANORAMA randomized clinical trial. JAMA Ophthalmol. 2021;139(9):946–955. doi:10.1001/jamaophthalmol.2021.2809
28. Stahl A, Sukgen EA, Wu W-C, et al. Effect of intravitreal aflibercept vs laser photocoagulation on treatment success of retinopathy of prematurity: the FIREFLEYE randomized clinical trial. JAMA. 2022;328(4):348–359. doi:10.1001/jama.2022.10564
29. Bressler SB, Barve A, Ganapathi PC, et al. Aflibercept biosimilar MYL-1701P vs reference aflibercept in diabetic macular edema: the INSIGHT randomized clinical trial. JAMA Ophthalmol. 2024;142(10):952–960. doi:10.1001/jamaophthalmol.2024.3458
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.