Back to Journals » Medical Devices: Evidence and Research » Volume 17
May Glymphatic Drainage Improve Life Quality in Progressive Multiple Sclerosis Outpatients?
Authors Mandolesi S ![]() , Niglio T
, Niglio T ![]() , Lenci C
, Lenci C
Received 27 July 2024
Accepted for publication 16 October 2024
Published 29 October 2024 Volume 2024:17 Pages 417—426
DOI https://doi.org/10.2147/MDER.S480815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sandro Mandolesi,1 Tarcisio Niglio,2 Chiara Lenci3
1Research Department of the Mediterranean Pole, Technoscience, Science and Technology Park, San Severo, Italy; 2Istituto Superiore di Sanità, Roma, Italy; 3“la Sapienza” University, Roma, Italy
Correspondence: Tarcisio Niglio, Email [email protected]
Background: The cerebral fluid-dynamic system plays a critical role in maintaining brain health and function. Recent studies identify the glymphatic system as primarily responsible for removing waste products and toxins from brain tissue. In recent years, we have achieved beneficial improvements in MS patients’ symptoms and lifestyle using a specific Fluid Dynamic Intensive MAM (FD-MAM) protocol.
Methods: We treated 40 outpatients with progressive MS, aged 45– 55 years and with EDSS scores from 6 to 9. We applied FD-MAM in 10 daily sessions over two weeks. Before and after glymphatic drainage by FD-MAM, we assessed each patient’s clinical status and quality of life using six validated questionnaires.
Results: Data from the six validated questionnaires administered to the 40 MS patients show an improvement in 83% of the scores. At the same time, we observed a shift from pathological to physiological values in 50% of the pathological scores after 10 sessions of FD-MAM protocol.
Conclusion: This study confirms the positive improvements on life quality in outpatients with progressive multiple sclerosis after one cycle of Fluid Dynamic Intensive MAM (FD-MAM) protocol. Initial follow-up on few patients treated with the FD-MAM protocol suggests that the results persist for six to ten months post-treatment. Future detailed studies, on MS outpatients’ larger cohort, are essential to assess the duration of results and its effect on glymphatic system.
Keywords: D009103 Multiple Sclerosis, D020528 Multiple Sclerosis, Chronic Progressive, D000077502 Glymphatic system, Fluid Dynamic MAM
Introduction
Multiple sclerosis (MS) is a chronic neurological disease that affects the central nervous system (CNS), which includes the brain and spinal cord. It is characterized by the immune system mistakenly attacking the protective covering of nerve fibres, called myelin. This attack leads to inflammation, demyelination (loss of myelin), and damage to the underlying nerve fibres. The exact cause of MS is not known, but it is believed to involve a combination of genetic and environmental factors. In our previous paper on governmental data, we computed the 2011–2015 Italian MS incidence in about 10,000 new patients each year.1 Some private associations estimated an Italian MS prevalence in 130,000 patients in Italy. Half of these are in the primary or secondary progressive phase.
In 20th century, the research about MS expanded significantly. Advancements in medical imaging, such as the development of the Magnetic Resonance Imaging (MRI), allowed for the visualization of MS lesions in the CNS, aiding in diagnosis and research.2 The first MRI for studying multiple sclerosis was conducted in the early 1980s.3
The 1990s marked a major milestone in MS treatment with the introduction of disease-modifying therapies (DMTs). These medications, such as interferon-beta and glatiramer acetate, aimed to reduce the frequency and severity of relapses and slow the progression of the disease.4
Research into the causes of MS, potential triggers, and genetic factors continues. Scientists are also exploring novel therapeutic approaches, including stem cell therapies and immunomodulatory treatments, to better manage and potentially cure the disease.5
MS organizations and advocacy groups have played a crucial role in raising awareness about the disease, supporting patients and caregivers, and funding research. World MS Day, observed on May 30 each year, is one example of efforts to raise awareness about MS globally.
While there is currently no cure for MS, the prognosis and quality of life for individuals with the disease have improved significantly over the years due to advances in research and treatment options. Early diagnosis and appropriate management can help individuals with MS live fulfilling lives while managing their symptoms.
In the last years, the studies on the glymphatic system opened new possibilities for MS therapy.
The glymphatic system and the cerebrospinal fluid (CSF) are both important components of the central nervous system, and they play critical roles in maintaining brain health and function. However, they are distinct systems with different functions.
In summary, the glymphatic system is a recently discovered system in the brain that relies on the flow of CSF to remove waste products and maintain brain health.5–8 CSF, on the other hand, is a clear fluid that surrounds the brain and spinal cord, serving various functions, including protection, nutrient transport, waste removal, and homeostasis. These two systems work together to support the health and function of the central nervous system.
Problems with CSF circulation, such as blockages or imbalances in production and absorption, can lead to various neurological conditions, including hydrocephalus (accumulation of excess CSF), increased intracranial pressure, and other disorders that affect the functioning of the CNS.6–8
Background
For the past 12 years, intensive outpatient treatment with dynamic fluid MAM has been the standard procedure for the treatment of outpatients with primary and secondary progressive multiple sclerosis (EDSS above 6.5) in our private clinic. During 2016, we treated our first nine patients in a pilot study to standardise the ultimate FD-MAM protocol and have scientifically proven and objective results. The protocol of the study was approved by the Lazio Region Ethics Committee with resolution no. 684/CE Lazio1 on 9 June 2020.
In 2022, we codified the Intensive FD-MAM protocol by which we treated the present 40 patients in the present study. Anyway, we emphasise that:
The MAM apparatus is a device currently used in the clinical practice of rehabilitation physiotherapy.
All patients continue the drug therapies prescribed by neurologists, albeit without clinical results.
To the subject studied was not administered any experimental and/or innovative substance. The therapies approved by the official pharmacopoeia have been used in the context of good clinical practice.
No experimental and/or innovative diagnostic techniques were used on the subject studied. The diagnostic techniques officially accredited in good clinical practice were used for a correct diagnosis.
The FD-MAM intervention has been a standard procedure for treating MS patients in our clinic since 2016. This implies that this is not a clinical trial but an observational study.
In December 2023, Health Canada authorised the importation of the MAM under “Special Access”, recognising its therapeutic efficacy for a patient with multiple sclerosis for whom drug therapies were no longer effective.
Aim
The goal of this study is to confirm the positive improvements on life quality in outpatients with progressive multiple sclerosis after one cycle of Fluid Dynamic Intensive MAM (FD-MAM) protocol.
Materials
In addition to its drainage into the veins, cerebrospinal fluid (CSF) features a second drainage system known as the lymphatic system. This system primarily directs fluid into the lymph nodes located in the head, neck, and pelvis, as initially identified by Cushing, Weed, and Dandy in 1914.9,10
On 2007, the Muscular Acoustic Modulator (MAM) was developed in Rome. It is a patented device for pain treatment that utilizes a special power and frequency-modulated acoustic wave.
In 2012, we postulated that this secondary lymphatic system might experience impaired drainage in certain individuals. Subsequently, we commenced the use of the MAM device to alleviate congestion in these lymph nodes.11
Initially, our focus was on treating the pelvic and leg lymph nodes of multiple sclerosis patients, resulting in notable improvements in gait disturbances. This approach is referred to as the DrenoMAM Protocol. In 2014, we further expanded our protocols by developing another approach specifically targeting the decongestion of lymph nodes in the head and neck. This protocol, known as the AcuMAM protocol, demonstrated favourable outcomes not only in addressing chronic fatigue but also in improving aspects such as memory, drowsiness, and overall quality of life.12
In 2022, seeking to enhance the lymphatic drainage of cerebrospinal fluid, we introduced the intensive outpatient FD-MAM protocol. This comprehensive protocol involves one session of AcuMAM and one session of DrenoMAM per day, five days a week, for two weeks. Initial results pertaining to the regression of symptoms in patients with progressive multiple sclerosis have shown significant positivity.13 Our underlying hypothesis, which guides the MAM treatment on lymph nodes, posits that these nodes serve as an additional pump to the lymph propulsion system through the lymphangion. Utilizing the FD-MAM protocol, ongoing research is being conducted on other neurodegenerative diseases such as Autism, Parkinson’s, and Alzheimer’s. Preliminary results have shown encouraging positive outcomes in these exploratory studies.
Subjects and Methods
Since August 2022, all patients diagnosed with primary and secondary progressive multiple sclerosis with an Expanded Disability Status Scale (EDSS) more than 6.0 and referred to our clinic have been enrolled in this study.
The authors conducted the following procedures for each patient:
Collected and evaluated clinical history.
Used Echo-Color-Doppler to assess the arterial and venous vessels of the neck and abdomen.
Conducted a total body muscular system assessment.
Utilized body impedance analysis (BIA).
Before starting the first treatment, each patient provided informed consent for participation in the protocol. Additionally, they filled six internationally validated questionnaires:
Barthel Index (BARTHEL), indicating the degree of autonomy in daily activities.
Fatigue Severity Scale (FSS), a self-assessment test for quantifying the impact of fatigue in multiple sclerosis over time.
Epworth Sleepiness Scale (ESS), a questionnaire assessing the propensity to fall asleep in specific daytime situations.
Functional Independence Measure (FIM), considering 18 activities of daily living and measuring disability.
Multiple Sclerosis Impact Scale with 29 questions (MSIS-29), evaluating the impact of MS on the patient’s life in cognitive and motor fields.
Expanded Disability Status Scale (EDSS), assessing the neuro-motor disability level in people with Multiple Sclerosis. The EDSS score was evaluated by a neurologist.
No changes were made to the ongoing neuropharmacological therapy for any participant. All participants underwent an outpatient cycle of FD-MAM intensive treatment using the Levia MAM model. This cycle consisted of five consecutive sessions in the first week and five sessions in the second week, incorporating both DrenoMAM and AcuMAM treatments each day. Following the end of these ten sessions, participants refilled the questionnaires to assess any changes.
The DrenoMAM treatment is a therapeutic drainage conducted with the MAM device, aiming to alleviate congestion in the lymph nodes located in the pelvic and lower limb regions (see Figure 1A–C). This drainage is administered in both posterior and anterior postures, employing a set of 8 cups of varying sizes strategically placed on specific points of the body. A timer sends a sequence of modulated acoustic waves every 10 seconds, culminating in a total treatment duration of 10 minutes for each target area on both sides of the body.
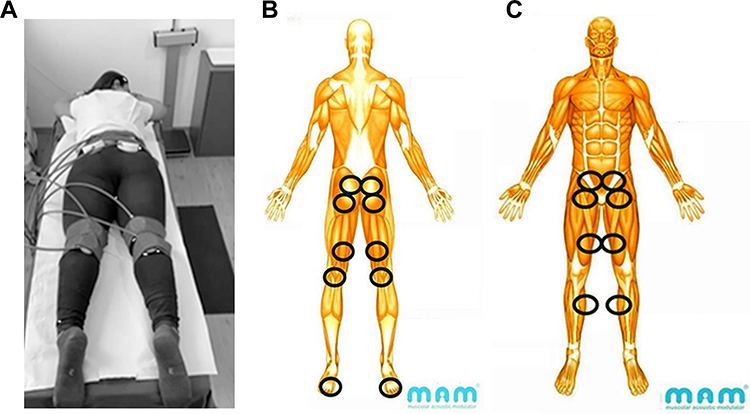 |
Figure 1 (A) DrenoMAM. (B) DrenoMAM - all points in body rear view. The blue circles are the application points of the MAM stimulation cups. (C) DrenoMAM – all points in frontal view. The blue circles are the application points of the MAM stimulation cups. |
In the posterior area, the treatment encompasses the sacrum, gluteal region, and popliteal fossa. On the other hand, the anterior area involves the inguinal region, both above and below the knee. This sequence and points of application are designed to effectively “soundproof” the areas where the primary lymph nodes responsible for draining the pelvis and lower limbs are located (see Figure 1B and C).
As for AcuMAM, this drainage involves the manual application of the MAM device’s probe to predetermined points in a specific sequence and timing at least 8 second for point. The goal is to decongest the lymph nodes in the neck and head bilaterally through targeted stimulation (see Figure 2).
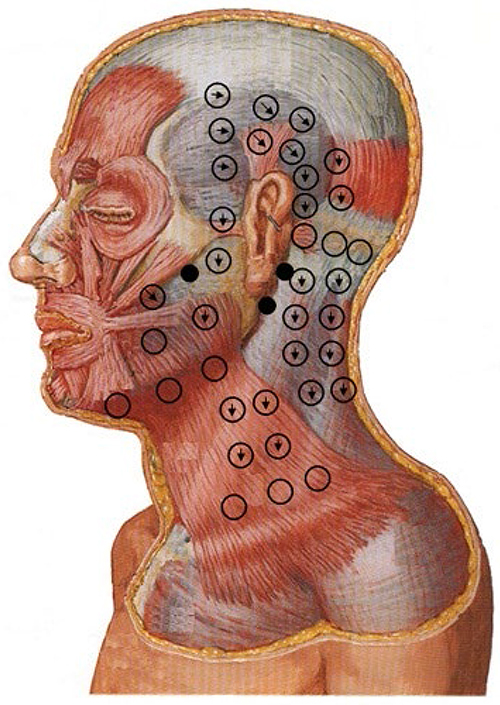 |
Figure 2 AcuMAM - stimulation points (black circles and empty circles). Black arrows in circles indicate lymphatic flow. |
There were also collected a pain map of each patient to control changing of the subjective pain symptoms during and after the FD-MAM cycle (see Figure 3A and B).
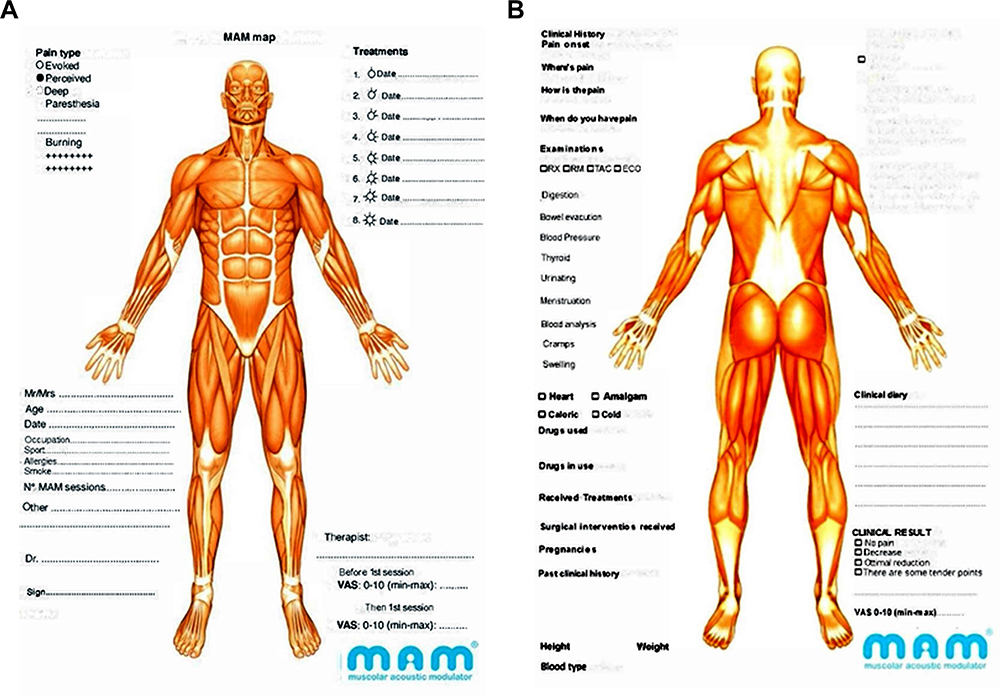 |
Figure 3 Pain map. (A) Front point of view. (B) Rear point of view. |
Statistical Analysis
Data were collected into a Microsoft Access database (Microsoft 365 MSO Version 2309 Build 16.0.16827.20130–64 bit), and they were analysed by Epi-Info 7 programs (CDC and NIH, 2022 Italian version 7.2.5.0). Statistical analysis estimated descriptive statistics, frequencies, and significance in showed differences. Chi-square Yates corrected test was used for non-continuous variables by Statcalc and Analysis programs. A p level of less than 0.05 was considered significant, and 95% confidence intervals were also calculated.
Results
Present study was performed on the period November 2022 – February 2024 about a MS patients’ sample, referred to first visit.
Out of a total of 60 subjects, only 51 had all the required pathological and clinical parameters and were selected to participate in this protocol. From the total of 51 patients, only 40 (aged 45–55; 21 female subjects plus 19 male) completed the FD-MAM protocol. The 11 drop out patients (6 female plus 5 male), who did not reappear on subsequent days, did so without stated reason.
The results of the data collected from the questionnaires are shown in Tables 1 and 2 (see tables for details). The number of patients (pt #) included in the specified stratifications.
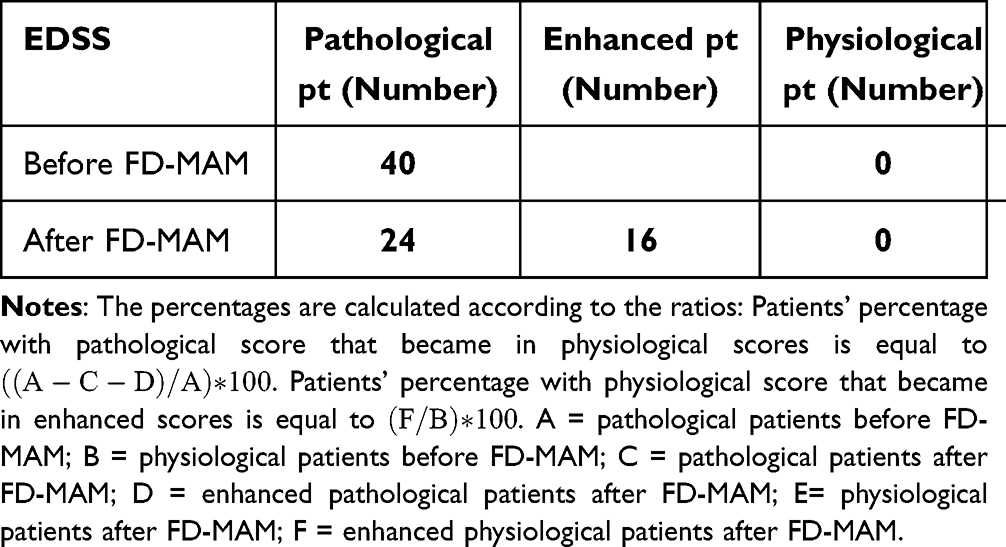 |
Table 1 Number of Patients with Pathological-Enhanced-Physiological EDSS Before and After Treatments by FD-MAM |
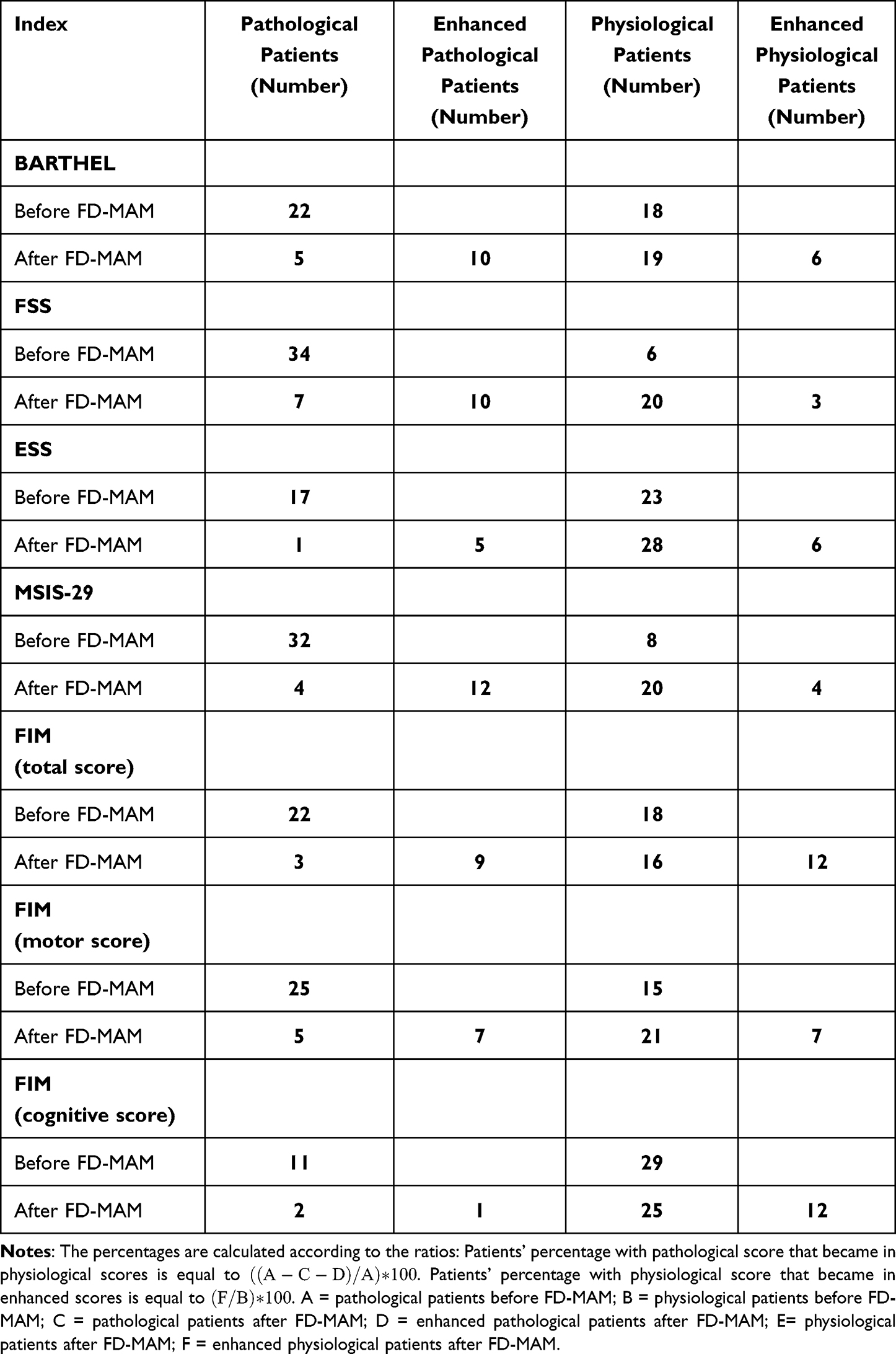 |
Table 2 Number of 40 MS Patients Stratified by Score Obtained in Validated Index Before/After FD-MAM Treatments |
On the same time, data from all questionnaires show a mean enhancement in 83% of the scores with a mean changing from pathological to physiological scoresin 50% of the scores of pathological scores. See Table 2 for details.
After 10 FD-MAM sessions, our patients showed an EDSS enhancement in 32.5% of the scores with not changing from pathological to physiological values (see Table 1). The EDSS improved scores decreased between 0.5 and 1.5 absolute values.
Summarising all the scores obtained in all validated questionnaires used, we can state that after FD-MAM treatments (see Figure 4 for details).
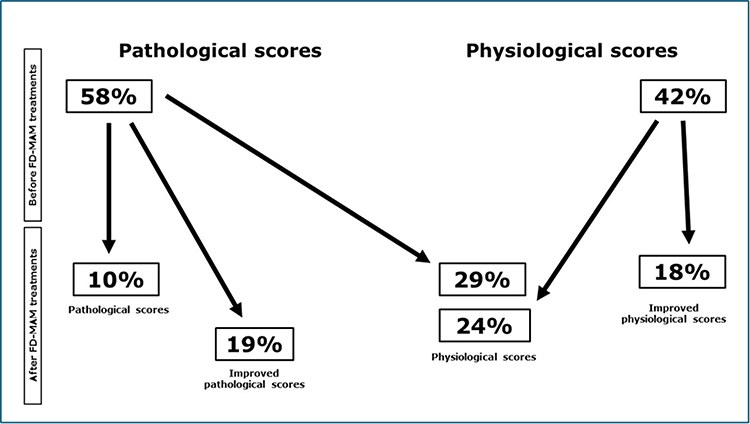 |
Figure 4 Percentage of all scores from 40 MS patients obtained in validated index before/after FD-MAM treatments. |
Scores remain pathological in 1 out 10 all measurements.
Scores improve in 1 out 3 of all initially pathological measurements, even if they do not reach physiological values.
Initial pathological scores become physiological in 1 out 2 measures after treatments.
At the same time, physiological scores remain at the same value in 1 out 2 measurements, while they improve in the remaining 1 out 2.
Discussion
Neuropharmacological therapy started in the late 1990s, and from the early medications, such as interferon beta, there has been gradual progress in recent years towards the newer generation of drugs referred to as “disease-modifying”. These drugs are used in the relapsing-remitting (RR) phase, and for the first-generation interferon, some studies have already reported poor efficacy in slowing the progression of the disease.14 In recent years, for the primary and secondary progressive phase of the disease, two drugs have been introduced to the market, siponimod and ocrelizumab.15,16
Therefore, our study aims to find a treatment for these patients who had currently no therapeutic options to reverse the clinical progression at this stage of the disease. We have reversed the pattern of pathogenesis and instead of trying to block the immune system’s reactions against nervous tissue, we have hypothesized that the immune attack could be due to the accumulation of substances for the cellular metabolism of the brain and spinal cord that could not be properly drained from their interstitial space. We hypothesized that restoring the physiological drainage of nervous tissue it could decrease the immune attack. Therefore, after a deep study of the cerebrospinal fluid drainage system, we theorized our treatment method.
The drainage of cerebrospinal fluid through the lymphatic system has been considered as an alternative route to the venous system since 1914 by Cushing, Weed, and Dandy.9,10 In 2012, the term “Glymphatic” was coined for the first time by Lijf. In 2015, Louveau, using two-photon intravital electron microscopy, highlighted the glymphatic system and meningeal lymphatics.17 Recent MRI studies with intrathecal gadobutrol contrast administration showed the drainage of this system into the head and neck lymph nodes.18
In 2012, we hypothesized that the drainage of interstitial fluid in the brain and spinal cord could be hindered or blocked at the level of extracranial and extraspinal lymph nodes. We hypothesized, too, that lymph nodes, in addition to their immune defence function, could also serve as essential pumping mechanisms for lymph flow towards the major supraclavicular venous drainage sites, such as the thoracic duct and the right lymphatic duct. To reactivate this lymph node drainage function, we utilized the MAM device, which has a dual effect on both the lymph nodal and lymphatic vessel muscular system by its mechanical vibration, used synergistically with customized protocols (DrenoMAM and AcuMAM). To determine the normalcy of circadian cerebrospinal fluid (CSF) drainage, a perfusion test should be conducted on these patients. If the CSF elastance index exceeds 0.3, and the pressure surpasses 30 mmHg, it indicates a potential blockage or hindrance in drainage. Why might CSF drainage face obstruction or hindrance? Our hypothesis centres on lymph node congestion. What could trigger this congestion? We posit that it may stem from a reaction to bacterial, fungal, or viral infections. Following the lymph nodes’ defence response to such infections, there is a return to their normal volume and function, and we speculate that the affected tissue or organ may undergo a potential full recovery. We theorized that the adverse effects of infections on the lymph nodes might be the underlying cause of relapses in the Relapsing-Remitting stage of Multiple Sclerosis (MS). Our current supposition, supported by FD-MAM results, suggests that cerebrospinal fluid (CSF) lymph drainage may be more effective than venous drainage. Zamboni’s venous hemodynamic studies which led to the definition of chronic cerebrospinal venous insufficiency (CCSVI) were a milestone in the evaluation of MS with a new perspective compared to the classic one in force until then of the autoimmune cause of the disease. The results on the symptoms of patients treated with his protocols, the venous angioplasty (TPA) of the jugular veins and Azygos have opened a new path to the interpretation of the disease. His “brave dreams” study, although not entirely positive, has stimulated new lines of vascular research into the disease.19 Seeking further insights, we conducted the “tap test” on certain patients with MS-SP or MS-PP, considering the potential presence of Normal Pressure Hydrocephalus in these individuals.20 In 2022, following a decade of developing the MAM method, we introduced the intensive outpatient FD-MAM protocol. This protocol had previously demonstrated symptom regression in inpatients with progressive MS as early as 2017,12 even without intensive treatment. Consequently, we initiated a study with the primary objective of confirming the protocol’s effectiveness in reversing the symptoms observed in these patients. To date, no physiotherapeutic, pharmacological, or invasive procedure has proven effective in ameliorating the symptoms of patients in this specific clinical phase.21 The initial outcomes following the first cycle of the intensive outpatient FD-MAM protocol revealed significant improvement in pathological scores. In our study, we targeted the lymph nodes in the head, neck, and pelvis of 40 subjects in the progressive stage of multiple sclerosis, with an Expanded Disability Status Scale score ranging from 6 to 9, employing the MAM intensive outpatient FD-MAM protocol.
After a cycle of 10 consecutive sessions, assessments by Barthel, ESS, FIM, MSIS-29, and FSS validated questionnaires demonstrated an enhancement in 83% of the scores with a change from pathological to physiological values in 50% of the scores. These results suggest that the FD-MAM protocol may be considered a valid approach for treating MS patients and for enhancing their lifestyle.
This is not a study about glymphatic system. Our hypothesis is that FD-MAM treatment of lymph node stations could improve the glymphatic drainage that leads to a significant improvement in life quality of patients with progressive multiple sclerosis.
Conclusion
This study presents the results obtained in 40 patients with progressive MS. After 10 sessions of the FD-MAM protocol, data from the six validated questionnaires, administered before and after treatments, showed an improvement in 83% of the scores with a shift from pathological to physiological values in 50% of the pathological scores.
A preliminary ongoing follow-up study on our MS outpatients, treated by the FD-MAM protocol, shows results lasting approximately six to ten months after the conclusion of treatment (unpublished data). Our hypothesis regarding the long-term persistence of clinical results in these patients is that the unblocking of lymph node stations treated with the FD-MAM protocol will remain permanent, unless a new infectious-inflammatory episode occurs that could re-block the drainage of these lymph nodes.
These findings are encouraging, and further studies involving enough MS patients will be necessary to assess the duration of results. A further study focused on the changes in Glymphatic System drainage using the DTI-ALPS index22 and NfL dosage23 before and after FD-MAM treatment of these patients will be necessary to validate our hypothesis that the treatment’s effect on their quality of life is due to the improvement of Glymphatic drainage.
Preliminary studies on further courses, after the first cycle of FD-MAM, show additional improvements in MS patients with EDSS scores between 6 and 7 (unpublished data).
At the same time, the high social and public health costs decreased in this progressive and terminal phase of MS due to the improvement of symptoms in these patients treated with MAM. These positive effects extend beyond the patients themselves, positively impacting the quality of life for both the individual’s undergoing treatments and their families.
These results on symptom improvement can be considered a first step for progressive MS therapy.
Ethics and Conflicts of interest
The study was performed in respect of the Helsinki Declaration, and it was approved by the Lazio Region Ethics Committee by resolution No. 684/EC Lazio1 on 9th June 2020. This Research Received No External Funding. The authors of the present study, and their family members, do not present possible conflicts of interest in the study itself.
The people involved in this study are all employees and/or retirees of private clinics or public administrations, and they did not receive extra funding for the present study. Family members of the authors involved in the present study did not receive funding for this study either.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Authors did not use generative artificial intelligence (AI) and AI-assisted technologies in the writing process.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Niglio T, Mandolesi S, De Lucia O, d’Alessandro A. The incidence of the multiple sclerosis in Italy: 2011-2015. Clin Ter. 2022;173(5):453–457.PMID: 36155732. doi:10.7417/CT.2022.2462
2. Smith HJ. The history of magnetic resonance imaging and its reflections in Acta Radiologica. Acta Radiol. 2021;62(11):1481–1498.PMID: 34657480. doi:10.1177/02841851211050857
3. Millar JH. Multiple sclerosis. Br Med J. 1980;280(6208):184–185.PMID: 7357321. doi:10.1136/bmj.280.6208.184-d
4. Sørensen PS. Balancing the benefits and risks of disease-modifying therapy in patients with multiple sclerosis. J Neurol Sci. 2011;311 Suppl 1:S29–S34. PMID: 22206763. doi:10.1016/S0022-510X(11)70006-5
5. Ringstad G, Valnes LM, Dale AM, et al. Brain-wide glymphatic enhancement and clearance in humans assessed with MRI. JCI Insight. 2018;3:e121537. PMID: 29997300. PMCID: PMC6124518. doi:10.1172/jci.insight.121537
6. Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4:147ra111. doi:10.1126/scitranslmed.3003748
7. Møllgård K, Beinlich FRM, Kusk P, et al. A mesothelium divides the subarachnoid space into functional compartments. Science. 2023;379(6627):84–88.PMID: 36603070. doi:10.1126/science.adc8810
8. Carotenuto A, Cacciaguerra L, Pagani E. Glymphatic system impairment in multiple sclerosis: relation with brain damage and disability. Brain. 2022;145(8):2785–2795.PMID: 34919648. doi:10.1093/brain/awab454
9. Cushing H. Studies on the cerebro-spinal fluid: i. Introd J Med Res. 1914;31:1–19. PMID: 19972189.
10. Weed LH. Studies on cerebro-spinal fluid. No. IV: the dual source of cerebro-spinal fluid. J Med Res. 1914;31:93–118. PMID: 19972195.
11. d’Alessandro A, Niglio T, Desogus A, d’Alessandro A, Mandolesi D. New acoustic wave therapy improves quality of life in patients with multiple sclerosis and chronic cerebrospinal venous insufficiency. Ann Ital Chir. 2015;86(4):336–339. PMID: 26343352.
12. Mandolesi S, d’Alessandro A, Niglio T, et al. Rehabilitation in Secondary Progressive Multiple Sclerosis in Patients: early Outcomes. J Tradit Med Clin Natur. 2017;6(3):1–4. doi:10.4172/2573-4555.1000229
13. Mandolesi S, Niglio T, d’Alessandro A, Fabiani SS, Siqueira T, Lenci C. Improvements in one severe progressive multiple sclerosis patient quality of life after an intensity fluid dynamic treatment. Clin Ter. 2023;174(3):224–230. doi:10.7417/CT.2023.2524
14. Ebers GC, Traboulsee A, Li D, et al. Investigators of the 16-year Long-Term Follow-Up Study. Analysis of clinical outcomes according to original treatment groups 16 years after the pivotal IFNB-1b trial. J Neurol Neurosurg Psychiatry. 2010;81(8):907–912.PMID: 20562430. doi:10.1136/jnnp.2009.204123
15. Kappos L, Bar-Or A, Cree BAC, et al. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, Phase 3 study. Lancet. 2018;391(10127):1263–1273. doi:10.1016/S0140-6736(18)30475-6
16. Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N Engl J Med. 2017;376(3):209–220.PMID: 28002688. doi:10.1056/NEJMoa1606468
17. Louveau A, Smirnov I, T.j. K, et al. Structural and functional features of central nervous system lymphatic vessels. Nature. 2015;523:337–341. doi:10.1038/nature14432
18. Eide PK, Vatnehol SAS, Emblem KE, Ringstad G. Magnetic resonance imaging provides evidence of glymphatic drainage from human brain to cervical lymph nodes. Sci Rep. 2018;8:7194. doi:10.1038/s41598-018-25666-4
19. Zamboni P, Galeotti R, Salvi F, et al.; Brave Dreams Research Group. Effects of Venous Angioplasty on Cerebral Lesions in Multiple Sclerosis: expanded Analysis of the Brave Dreams Double-Blind, Sham-Controlled Randomized Trial. J Endovasc. 2020;27(1). PMCID: PMC6970429.
20. Petrella G, Czosnyka M, Smielewski P, et al. In vivo assessment of hydrocephalus shunt. Acta Neurol Scand. 2009;120(5):317–323.PMID: 19456302. doi:10.1111/j.1600-0404.2009.01176.x
21. Sutliff MH, Bennett SE, Bobryk P, et al. Rehabilitation in multiple sclerosis: commentary on the recent AAN systematic review. Neurol Clin Pract. 2016;6:475–479. doi:10.1212/CPJ.0000000000000318
22. Naganawa S, Taoka T. The Glymphatic System: a Review of the Challenges in Visualizing its Structure and Function with MR Imaging. Magn Reson Med Sci. 2022;21(1):182–194. doi:10.2463/mrms.rev.2020-0122
23. Szilasiová J, Rosenberger J, Fedičová M, et al. Neurofilament Light Chain Levels Are Associated with Disease Activity Determined by No Evident Disease Activity in Multiple Sclerosis Patients. Eur Neurol. 2021;84(4):272–279. doi:10.1159/000515806
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.