Back to Journals » International Journal of Women's Health » Volume 17
Maternity Care Client and Provider Experiences at Health Facilities in the Eastern Democratic Republic of Congo: Understanding Person-Centered Maternity Care Within Crisis Settings
Authors Mwene-Batu P ![]() , Mary M, Ngaboyeka G
, Mary M, Ngaboyeka G ![]() , Bigirinama R
, Bigirinama R ![]() , Chimanuka Murhima'alika C, Chiribagula CZ
, Chimanuka Murhima'alika C, Chiribagula CZ ![]() , Bisimwa Balaluka G, Tappis H
, Bisimwa Balaluka G, Tappis H ![]()
Received 8 August 2025
Accepted for publication 3 November 2025
Published 8 November 2025 Volume 2025:17 Pages 4331—4345
DOI https://doi.org/10.2147/IJWH.S559529
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Pacifique Mwene-Batu,1– 3 Meighan Mary,4,5 Gaylord Ngaboyeka,1 Rosine Bigirinama,1 Christine Chimanuka Murhima’alika,1 Christian Zalinga Chiribagula,1 Ghislain Bisimwa Balaluka,1 Hannah Tappis4,6
1Ecole Régionale de Santé Publique, Université Catholique de Bukavu, Bukavu, Democratic Republic of the Congo; 2Faculty of Medicine, Université de Kaziba, Kaziba, Democratic Republic of the Congo; 3Hôpital Provincial Général de Référence de Bukavu, Université Catholique de Bukavu, Bukavu, Democratic Republic of the Congo; 4International Health Department, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA; 5International Center for Maternal and Newborn Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA; 6Center for Humanitarian Health, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Pacifique Mwene-Batu, École Régionale de Santé Publique, Université Catholique de Bukavu, South Kivu, B.O 285, Bukavu, Democratic Republic of the Congo, Email [email protected]
Background: While infrastructure impacts are well documented, the consequences of armed conflict on working conditions of healthcare providers and experiences of women giving birth at health facilities remain under-explored.
Methodology: In 2023, we conducted a cross-sectional study in 28 health facilities in North and South Kivu provinces of Eastern Democratic Republic of Congo. To assess women’s experiences on the day of birth, we interviewed a representative sample of 231 postpartum women using an structured tool adapted from the Demographic and Health Survey (DHS) Service Provision Assessment (SPA) including a 13-item person-centered maternity care (PCMC) score. We also interviewed a representative sample of 220 maternity care providers on duty at the time of the assessment using a structured interview tool adapted from the DHS-SPA. Analysis was conducted using the Chi-square and T tests.
Results: PCMC scores averaged 24.5 out of 39, representing moderate patient-centered care. Scores were lowered by sub-optimal autonomy, privacy, and communication. In each province, half of the providers reported being satisfied with their workplace. More reported experiencing verbal abuse by other staff (41% v.28%, p=0.049) and by patients or family members (34% v 9%, p > 0.001) in North Kivu compared to South Kivu. Approximately half of providers surveyed felt safe and protected from crime when in or traveling to/from their facility. In contrast, 92% of postpartum reported feeling safe at the facility.
Conclusion: Contextualized assessment tools and targeted investments are needed to protect, support, and motivate health workers to provide PCMC in Eastern Democratic Republic of Congo. Focus areas should include safer work environments, training on patient rights and respectful care, and feedback mechanisms to align services with women’s needs.
Keywords: quality of care, conflict affected zones, person-centered care, working conditions
Background
High-quality health services are essential for achieving universal health coverage and fulfilling the third Sustainable Development Goal (SDG 3).1,2 The Lancet Global Health Commission on High Quality Health Systems underscores that access to services alone does not guarantee effective care.3 Studies have documented significant disparities in the quality of maternal and neonatal health (MNH) services—both between and within countries of comparable income levels.4–7 Simulation models suggest that improving the quality of care alone, without increasing coverage, could prevent up to a quarter of maternal deaths, neonatal deaths, and stillbirths in low- and middle-income countries (LMICs).8,9 Moreover, enhanced quality positively affects care-seeking behaviors, influencing whether, when, and where women seek care.10
A core component of high-quality care is responsiveness to the needs and values of patients—manifested through compassion, respect, and dignity in service delivery.1 To evaluate healthcare quality, the World Health Organization (WHO) uses a framework that contains eight quality domains that should be assessed, improved and monitored within the health system.11 The health system provides the structure for access to high-quality care in the two important, inter-linked dimensions of provision and experience of care.11 This dual approach is particularly relevant in LMICs, where systemic constraints often hinder both technical care and respectful, person-centered interactions.12,13 Research has documented substantial disparities in these dimensions, including reports of mistreatment during childbirth and inadequate neonatal care.13,14 Where disparities exist, measuring women’s experiences is essential to understanding and improving the quality of maternity services. The Person-Centered Maternity Care (PCMC) scale is a validated tool specifically developed to capture women’s experiences during childbirth in health facilities across LMICs.15–18 It assesses key domains such as dignity and respect, communication and autonomy, and supportive care, providing insights into how women perceive and are impacted by the care they receive, particularly in settings affected by fragility and crisis.
In the Democratic Republic of Congo (DRC), notable increases in the rate of institutional deliveries have not translated into commensurate improvements in outcomes, raising concerns about the quality of maternity care. For example, although the proportion of births at health facilities increased from 64% in 2007 to 85% in 2023, maternal mortality remains alarmingly high.19 In 2023, DRC was one of the four countries reporting more than 10,000 maternal deaths per year and accounted for 7.2% of all estimated global maternal deaths in 2023.20–22 Especially in the conflict-ridden Eastern provinces of DRC, health system disruptions due to prolonged insecurity undermine MNH service quality.23 While physical damage to facilities is well documented,23 the consequences of conflict on the safety and motivation of healthcare providers, their working conditions and environment, and patient’s experience of care on the day of delivery remain largely unexplored in such settings.24 In this study, we aimed to assess PCMC and document postpartum women’s and health providers’ perception of safety and the conditions of the health facility work environment in conflicts affected zone of North and South Kivu, DRC. We hypothesize that the conflict-affected context shapes quality at multiple levels, directly influencing women’s experience of care and compromising person-centered care through the indirect effects on provider safety and working conditions.
Methodology
Our work is a cross-sectional study involving maternity health provider interviews and postpartum exit interviews with women who recently gave birth, conducted as part of a larger cross-sectional assessment of the quality of maternal and newborn care in health facilities in conflict-affected areas of North and South Kivu provinces in the Eastern region of the DRC. Data collection was conducted in South Kivu in February 2023 and in North Kivu in October 2023.The parent study included: (1) structured exit interviews with postpartum women upon discharge from the hospital; (2) structured interviews with maternity care providers; (3) facility inventories; and (4) observation checklists. Our analysis draws on data collected from (1) and (2). The study was reviewed and approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB No:21922), and Université Catholique de Bukavu Ethical Committee in the DRC (UCB/CIES/NC/011/2023) and complied with the 1964 Declaration of Helsinki and subsequent amendments.25
Study Setting
Eastern DRC, including North Kivu and South Kivu provinces, is a region that has been plagued by decades of socio-political instability and insecurity. In North Kivu, the humanitarian situation is critical; in 2023, North Kivu was home to over 2.5 million internally displaced people, many of whom live in precarious conditions with limited access to basic health services.26 Health infrastructure is regularly affected by conflict-related destruction or abandonment, and health personnel often work in unstable environments with limited resources.26 Although similarly affected by the conflict, South Kivu faces slightly different dynamics marked by localized insecurity, structural poverty and weak governance. Armed groups remain active, particularly in rural territories where health infrastructure is scarce and health districts cover large, hard-to-reach populations.26 In addition to the indirect dysfunction of the health system due to the weakening of the eastern region of the DRC by armed conflicts on the economic, political, social and infrastructure levels, this crisis also affects the functioning of the health system due to direct and targeted attacks on health facilities, health personnel as well as patients in health facilities at the time of the attacks.26
Study Population and Sampling
The assessment was conducted in all public and private facilities, integrated into the national system, in these provinces with an average of five or more births per day reported in the national health management information system in 2022.27 Based on this criteria, 33 health facilities were selected (17 in South Kivu and 16 in North Kivu) (Figure 1). These included 28 secondary referral hospitals, 5 health centers and 5 referral health centers. However, due to ongoing conflict, five facilities (4 health centers and 1 referral health centers) in North Kivu were inaccessible at the time of data collection, resulting in a total of 28 facilities included in the study. Health centers represent the first level of care, delivering primary health care principally provided by general nurses, including basic emergency obstetric and newborn care (BEmONC). Health centers refer more complex cases to secondary referral hospitals, which offer a broader range of services including comprehensive emergency obstetric and neonatal care (CEmONC). In regions without secondary referral hospitals, some health centers are upgraded to referral health centers, which are staffed with doctors and have the surgical capacity required to provide CEmONC and are therefore qualified as referral health centers.
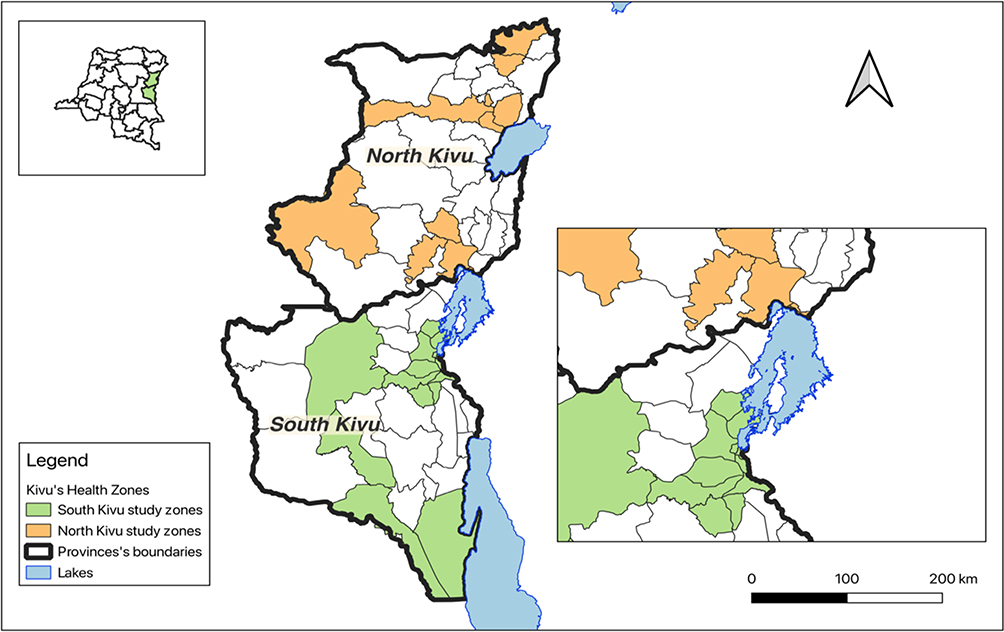 |
Figure 1 Location of health facilities meeting study inclusion criteria in North and South Kivu provinces. |
Characteristics of the selected health facilities are presented in Table 1. The majority are secondary referral hospitals (84.9% overall). In terms of management, nearly 57.6% of the facilities are privately managed, including those operated by faith-based organizations, which are integrated into the national health system. Facilities managed by government account for 39.4% of the sample.
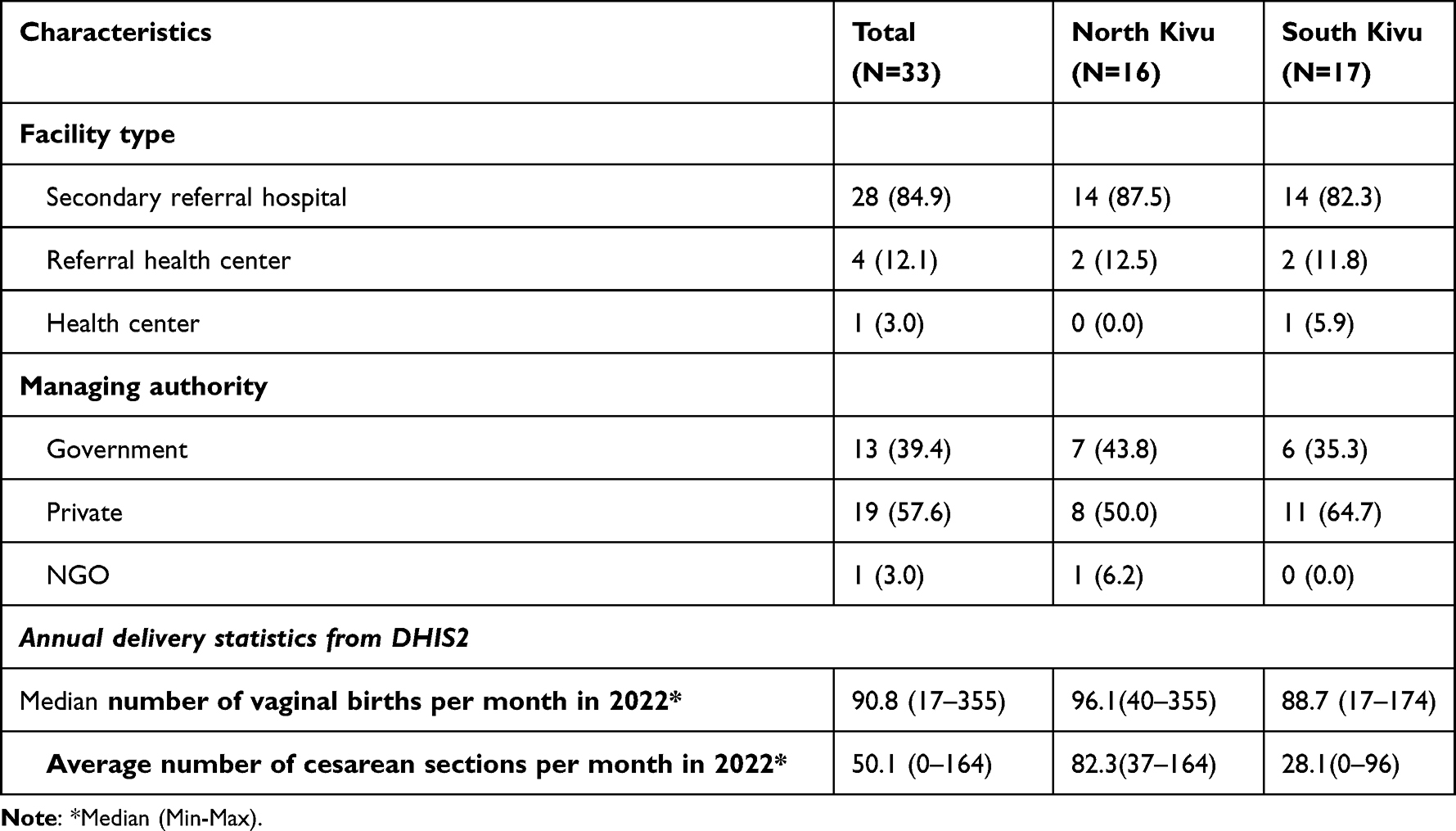 |
Table 1 Health Facility Characteristics, n (%) |
At each facility, up to 15 women were invited to participate in structured exit interviews. A target of at least 9 postpartum exit interviews with women leaving each facility after either vaginal or cesarean births was determined based on sample size calculations for the parent study; assuming a design effect of 1+ (m – 1)xrho using m = the average number of births per facility and rho = 0.1 correlation of quality-of-care outcomes within facility, we estimated that this would allow us to assess a range of primary dichotomous outcomes (eg adherence to specific standards of care) with with a margin of error of ±10 percentage points and a 95% confidence interval. The actual number of exit interviews depended on the number of eligible clients at the facility during the five days allotted for data collection at each facility. Married women and girls of any age (no age requirement as marriage is an indication of adulthood in local context) as well as unmarried girls (under 18 years old) who were accompanied by a parent or guardian who could provide consent who were discharged with their newborns within 72 hours of a live birth were invited to participate.
Up to eight maternity health providers at each facility were invited to participate in structured health provider interviews. The maximum sample size of eight was determined on the basis of national staffing guidelines for primary health care facilities and hospitals in the DRC,28 and the national team’s expectations regarding potential variation in hospital size and staffing. We excluded health providers if they: a). were trained in maternal and newborn care but not directly involved in clinical service provision (purely administrative roles, those working in other departments, etc).; and/or b). had less than three months of service provision in their facility.
Data Collection
For postpartum exit interviews, clients were approached in the postpartum ward/room when preparing for discharge. Those willing to participate were asked to accompany a female study team member to a private room for informed consent and a brief (approximately 15 minutes) interview in their preferred language (French or Kiswahili).
Informed consent was obtained from all married participants (marriage is an indication of adulthood in local context, allowing for independent consent regardless of age). Participant assent and parent/guardian consent were obtained for all unmarried participants under 18 years of age. Respondents gave their consent either by written signature or by fingerprint, depending on their literacy level. Every precaution was taken to preserve the climate of trust and confidentiality of the information gathered.
All eligible MNH providers who were on duty on the days of the assessment were informed about the purpose of the study and then invited to participate. If more than eight MNH providers were on duty at the time of the assessment, participants were selected for interviews at random. At high volume facilities with 24/7 delivery services, skilled birth attendants on both day-shift and night-shift were invited to participate, as well as skilled birth attendants working across antenatal care, labor and delivery and postnatal care services. Those selected to participate agreed to a convenient time to speak with data collectors (eg start or end of shift) so that interviews did not interfere with patient care duties. The health provider interviews were conducted using a standardized questionnaire, originally developed in English and subsequently translated into French. The interview lasted about 25 minutes.
Data collection was conducted by eight teams, each composed of two people. One team member was responsible for the exit interviews and another for the interview with healthcare providers. Team members included public health professionals with 2+ years of research experience who underwent a 5-day training on the study procedures, including recruitment, informed consent, interviewing and data collection tools. Data were collected using a pre-tested electronic questionnaire deployed through the REDCap platform.29
Variables of Interest
The study builds upon a series Maternal and Newborn Health Quality of Care Surveys initially conducted by the USAID-funded Maternal and Child Health Integrated Program from 2010 to 2012 in seven African countries,30 and subsequently expanded in evaluations supported by the World Bank, UNICEF and USAID in Central and South Asia.31,32 The assessment tools were enhanced to incorporate client exit interviews and the health worker interview, using a structured instrument adapted from the Demographic and Health Survey Service Provision Assessment (SPA), revised in 202233 with additional content added to capture health worker experiences, women’s perceptions of safety in the health facility and surrounding environment and considerations related to conflict-affected contexts.
The postpartum exit interviews inquired about women’s experience during labor and delivery, including the 13-item shortened PCMC scale, developed and validated by Afulani et al.34 Person-centered care takes into account respect and dignity, autonomy, communication, supportive care, and finally, trust. Each item is rated on a 4-point frequency scale: 0 (“no, never”), 1 (“yes, sometimes”), 2 (“yes, most of the time”), and 3 (“yes, all the time”). The total score is obtained by summing the ratings of the 13 items, yielding an overall score ranging from 0 to 39. Scores are classified as: weak (<19.5 points or <50%), moderate (19.5–29.25 points or 50–70%) or strong PCMC (>29.5 points or >75%). In addition, we also assessed women’s perceptions of safety in the health facility and surrounding environment.
MNH provider interviews gathered information on the participants’ characteristics, perception of the working environment (level of satisfaction with working in the facility, lack of respect for healthcare personal, abuse by other staff members/ by patients or family members and feels respected by colleagues/ the community) and their perception of safety, with additional items specifically addressing challenges in conflict-affected settings.
Data Analysis
The PCMC scale incorporated in the Demographic Health Survey (DHS) Service Provision Assessment has not been validated for cesarean births. Thus, this analysis focuses on the subset of respondents discharged within 24 hours after a vaginal birth. All MNH provider participants were included in the analysis. Data were analyzed using Stata 16 software.35 Categorical variables were summarized using counts and proportions, and quantitative variables as means and standard deviations or medians with interquartile range (25th and 75th percentiles), depending on their distribution. The comparison between proportions of categorical variables were assessed using Pearson’s chi-square test or Fisher’s exact test, as appropriate. Comparison in means and median between the two subgroups (North Kivu, an area with many active conflicts to South Kivu, a relatively stable area) were evaluated using Student’s t-test and The Mann–Whitney U-test based on the conditions of application.
Results
Characteristics of Exit Interview Participants (Postpartum Women and Girls)
A total of 231 women and girls participated in the postpartum exit interviews (Table 2). Participants reported a median age of 25 years and approximately one quarter (26%) had a primary school level education. More than half of participants were multiparous, with less than 25% primiparous. Less than 10% were not in a marital union. These characteristics did not differ between provinces. Nearly 20% of participants reported that they or a household member were displaced during the year prior to data collection, with significant differences in displacement by province (North Kivu: 25% and South Kivu: 14%; p=0.027). In addition, women in South Kivu more frequently had planned to give birth in the facility (93%) compared to those in North Kivu (80%; p=0.002).
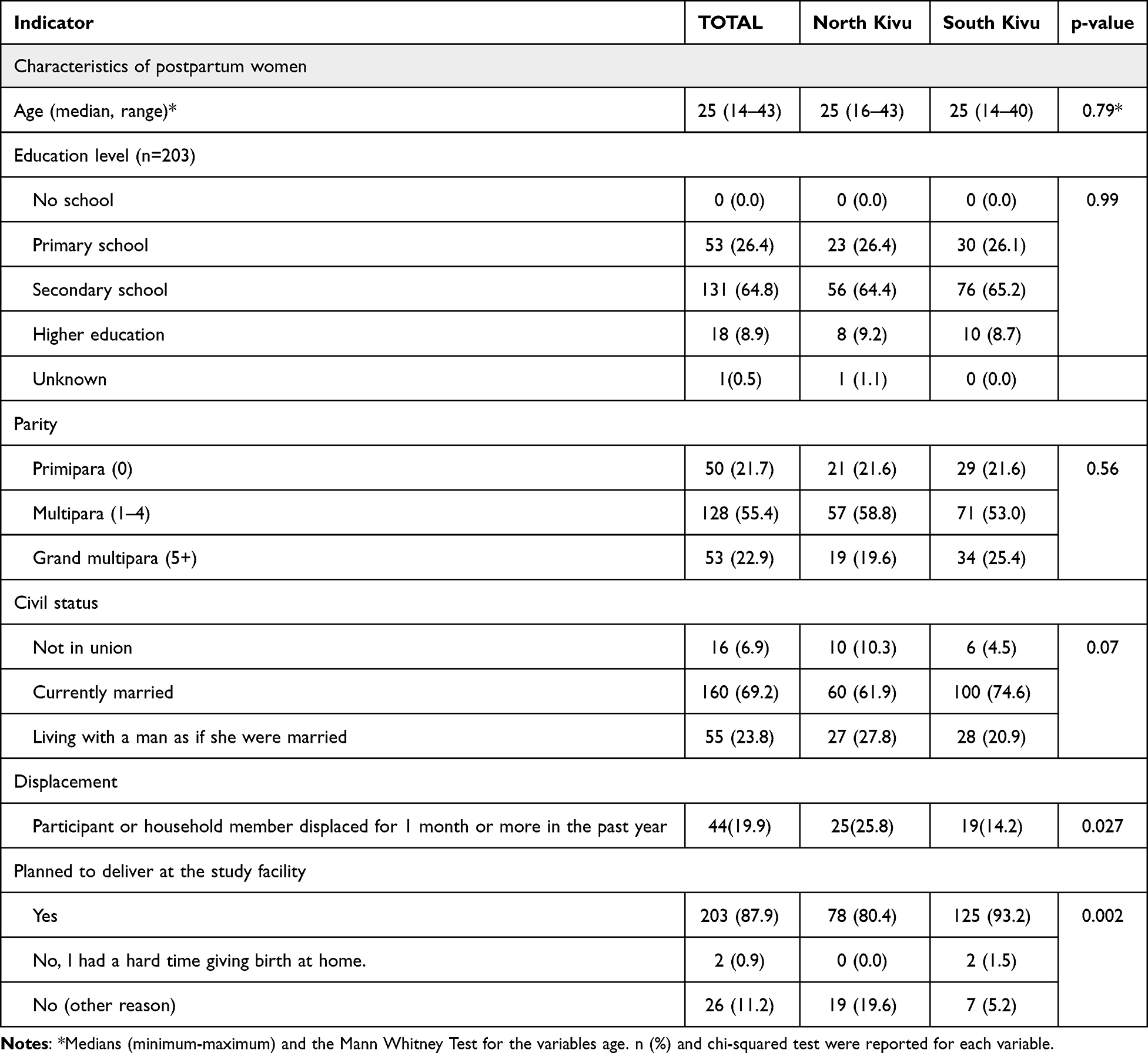 |
Table 2 Characteristics of Postpartum Exit Interview Participants (n=231), n (%) Unless Otherwise Noted |
Participant Experiences of Care During Birth Using the PCMC Scale
The overall average PCMC score was 24.5 out of 39, representing moderate patient-centered care (within range of 50–75%). The overall PCMC score was statistically different by province (North Kivu: 20.5 and South Kivu: 27.9; p=0.024); nonetheless, both scores represented moderate PCMC. Significant differences were also identified for all but two item-specific scores (ie, participants felt they could ask all their questions and discuss how they were feeling with the health providers). Of note, higher PCMC scores were reported for every item in South Kivu (Table 3).
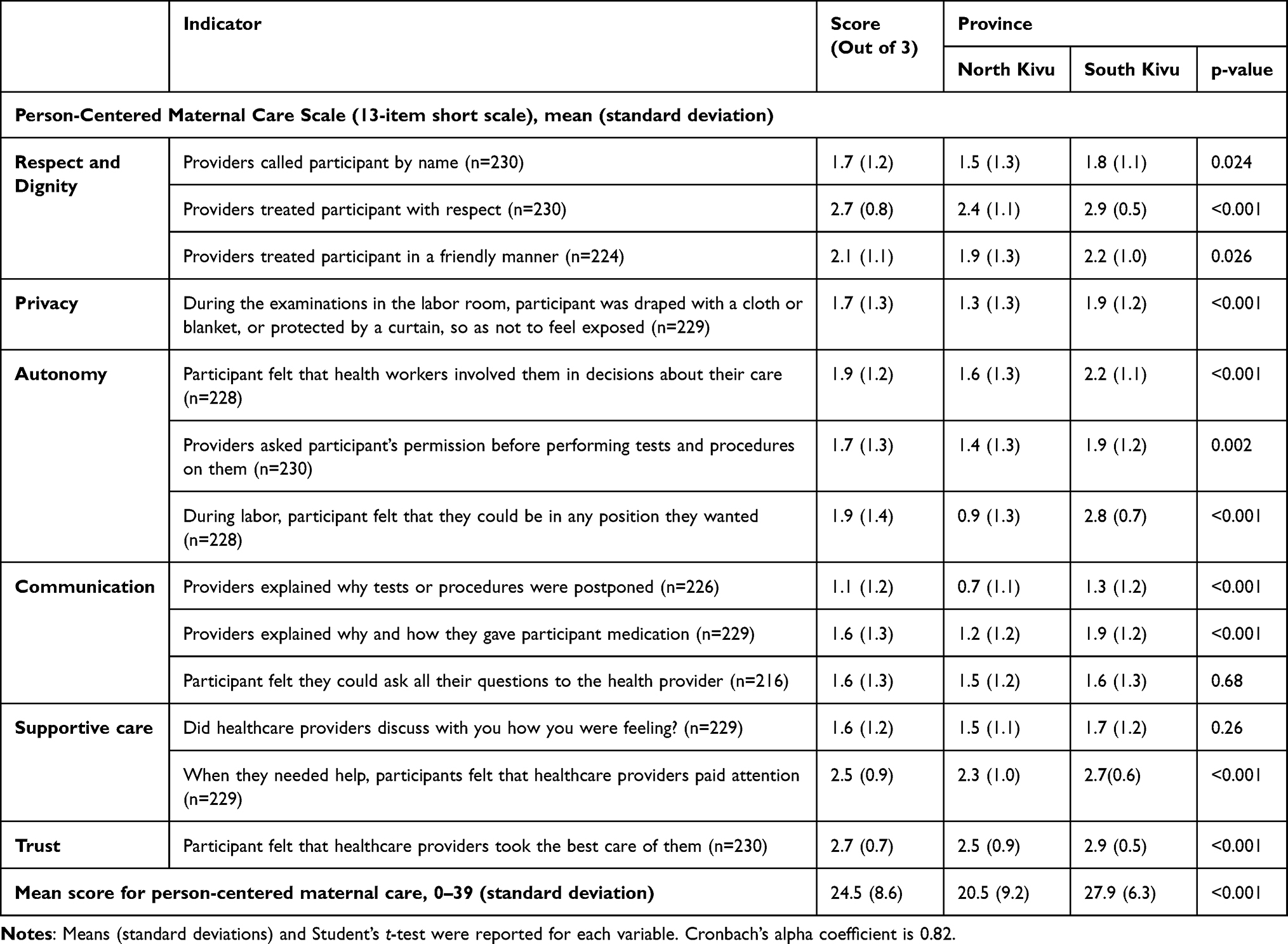 |
Table 3 Person-Centered Maternity Care Scale, Disaggregated by Province, n (%) |
Characteristics of Health Providers
A total of 220 health providers were interviewed (116 in North Kivu and 104 in South Kivu) with a median age of 38.5 years and 13 years of professional experience (Table 4); there was no statistically significant differences in age or experience of providers by province. Among them, 81.4% were nurses, 18.2% physicians and only one was a specialist (obstetrician; 0.4%). Health providers in South Kivu were more likely to be female (84%) compared to North Kivu (68%, p=0.007).
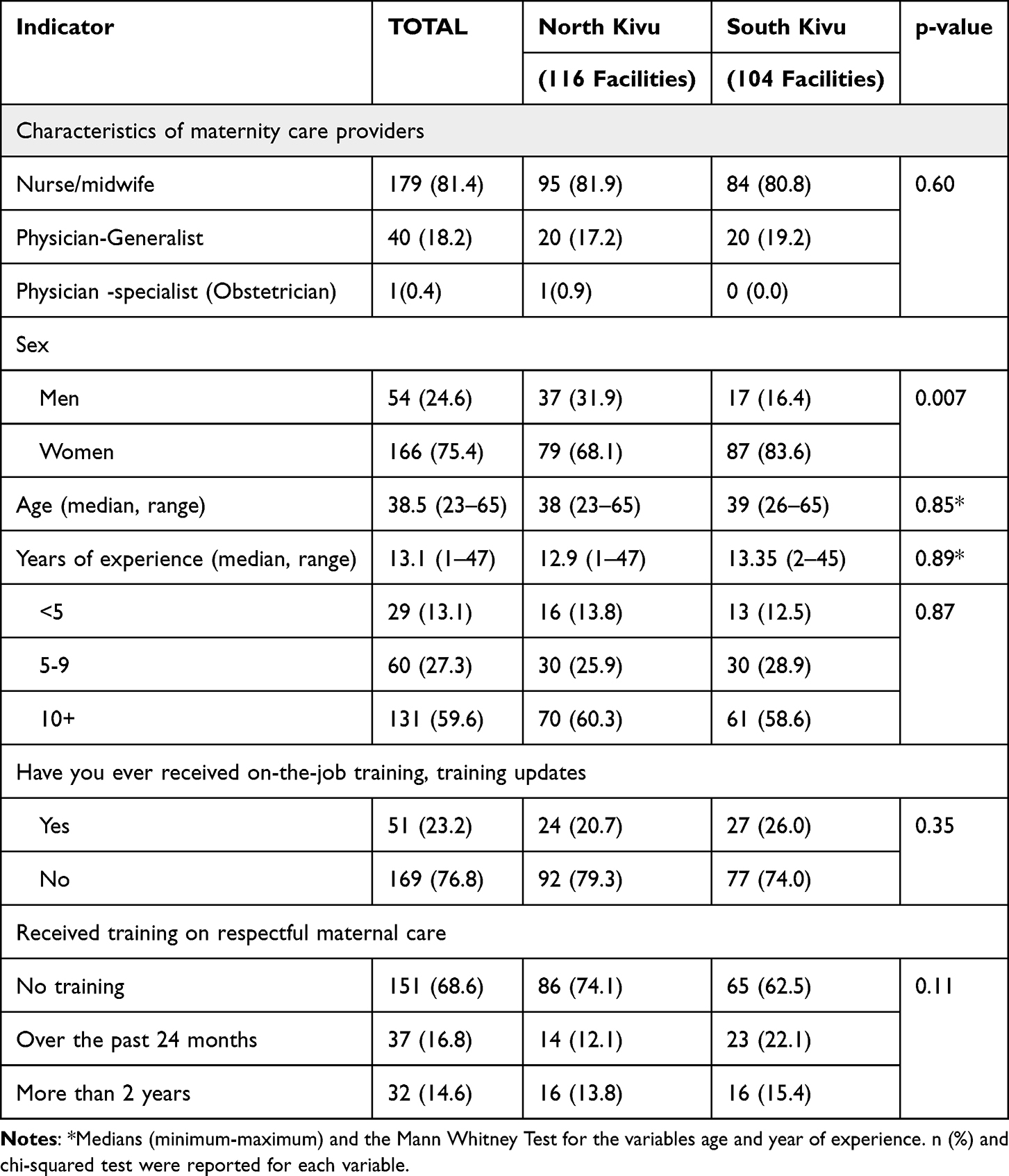 |
Table 4 Characteristics of Interviewed Health Providers Across 28 Facilities (N=220), n (%) Unless Otherwise Noted |
Perception of the Work Environment by MNH Providers
To understand the context of these PCMC scores, we assessed MNH providers’ perception of their work environment (Table 5). In each province, only half of the MNH providers reported being satisfied with their workplace. Furthermore, nearly 10% of MNH providers considered lack of respect to be a problem in their workplace, with significant differences between respect at the health facility in North Kivu (16.3%) and South Kivu (3.8%; p=0.006). Significantly more MNH providers reported experiencing verbal abuse by other staff members (41%) and by patients or family members (34%) in North Kivu compared to those in South Kivu, 28% and 9% respectively (p=0.049 and p<0.001). Very few participants reported experiencing physical abuse in both provinces. Despite report of verbal and physical abuse, over 90% of MNH providers believed they were generally respected by colleagues (92%) and the communities they serve (96%).
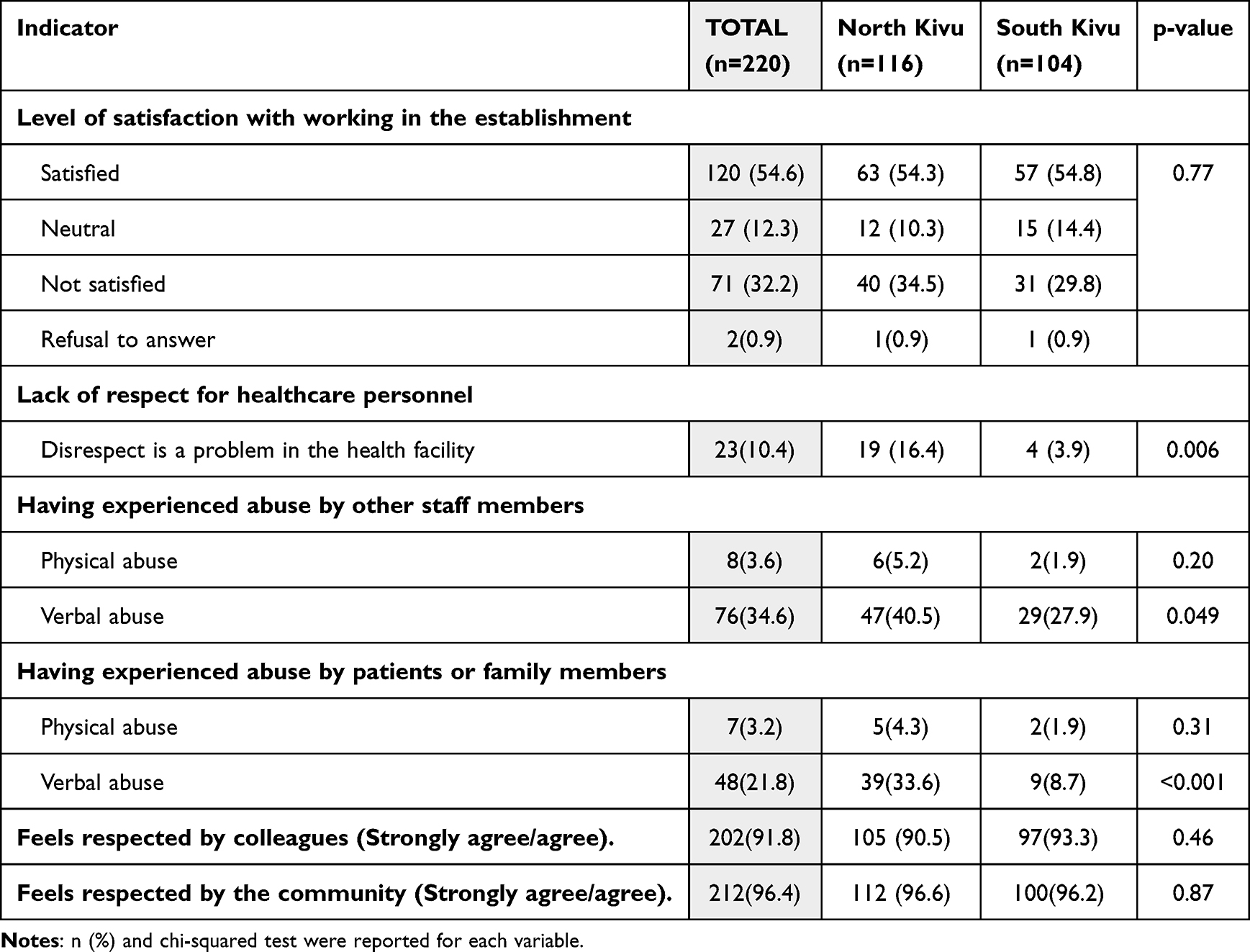 |
Table 5 Perception of the Work Environment by Maternity Care Providers, Disaggregated by Province (N=220), Data Reported as n (%) |
Perception of Safety by Maternity Care Providers and Postpartum Women
Table 6 outlines perceptions of safety from both the MNH provider and women’s perspectives. Only about half of MNH providers felt safe and protected from crime when they were in their facility (53%) or when traveling to and/or from it (50%). In addition, a majority of providers reported that the area surrounding the facility was marked by repeated violence (61%) and that the level of violence in the area has increased significantly over the prior year (52%). These perceptions differed significantly by province, with more MNH providers in South Kivu reporting feeling safe and less reporting existing and/or increasing violence compared to North Kivu. However, postpartum women’s perceptions of safety did not align with the MNH providers. Overall, women more frequently reported feeling safe at the facility (92%) and while en route to or from the facility (86%). Reports also did not vary by province, with the exception of their perception of increased violence. Significantly more women in North Kivu reported significant increases in violence over the prior year (30%) compared to those in South Kivu (8%; p<0.001).
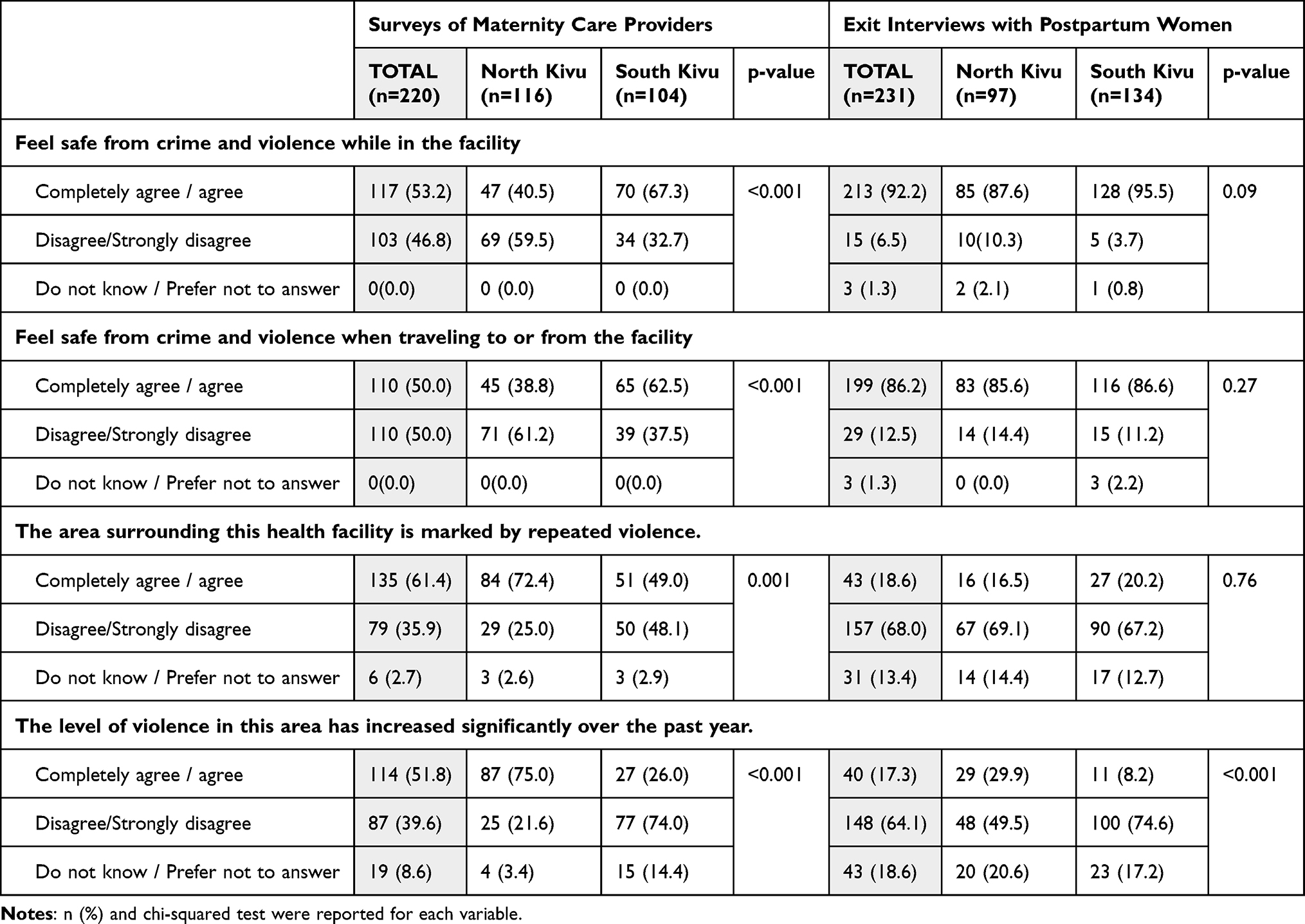 |
Table 6 Health Providers’ and Postpartum Women’s Perception of Safety, Disaggregated by Province, n (%) |
Discussion
Our study is the first to assess PCMC within the context of active conflict and offers critical insights into how women experience maternity care and how both women and health providers perceive the unstable geopolitical context. Our results show that maternity care is moderately person-centered according to the PCMC score, and the score is worse in facilities located in the province with ongoing conflict and fragile conditions (i.e, North Kivu). Indeed, armed conflict has significant consequences on the psychological health of the population, including post-traumatic stress and anxiety, which can be exacerbated by patients’ concerns about their health.36,37 Moreover, exposure to intense stress, violence and secondary trauma, health professionals in active conflict zones experience a deterioration in their psychological well-being, affecting their ability to provide adequate care.38–40 This can also lead to a progressive decline in the quality of care provided to populations, fatigue as well as a decline in their level of compassion towards patients. This may have a negative impact on the level of use and attendance of MNH services in conflict affected zones.
Women’s perception of care is often based more on how they are treated than on the technical quality of clinical management. As shown in previous studies, the decision to use a particular facility is strongly influenced by personal or second-hand experience or that of their relatives and neighbors, rather than by the care offered by the facilities or health providers.41 Moreover, many women resort to avoiding the nearest health facilities to seek better quality care further on, which underscores the need to improve the perceived and actual quality of care in local facilities.5,42 Thus, to improve the perceived quality of services and make them more women-centered, healthcare providers must be aware of women’s needs and preferences for maternal and newborn health services. This requires institutionalizing community engagement mechanisms such as regular dialogue, and feedback systems (suggestion boxes, patient administration services, listening and reporting units, and hospital hotlines). Additionally, there are social accountability mechanisms, such as community scorecards and citizen report cards, or more governance-centered interventions, like problem driven iterative adaptation, that can be used.43 In order to provide entry points to improve the care process by taking into account women’s perceptions and needs and thus improve person-centered care.
Although disparities were observed between provinces, lower scores were found in three main areas of the PCMC score: privacy during labor, autonomy (participation in decision-making, consent for procedures and freedom of movement during labor), and communication regarding delays and medications. These findings align with those from a multicenter study conducted in Kenya, Ghana, and India, where the lowest scores were also recorded for communication and autonomy. For example, more than 70% of women in India reported that providers never asked for their consent before procedures.16 Communication was also lacking in our context, with scores lower than those observed in South Kivu but comparable to the low levels reported in countries like Ghana or India, where more than half of the women stated they had not received explanations about procedures or medications.16 This weakness, common in many low-income settings, is also confirmed in the global review, where communication and autonomy were consistently the lowest-rated domains, with scores as low as 18.1/100 in some African studies.44
Although women are well represented in the health workforce overall as health providers in North and South Kivu, they were relatively less present in areas with ongoing active conflicts (in North Kivu). This may be attributed to gender differences in perceived safety, as previous studies have shown that female providers are less likely to work in insecure settings due to safety concerns.45 Indeed, this could well be explained by a disparity that has been observed according to gender and especially in areas with active conflicts where aggressions are more often frequent and reported by women than by men, whether from patients or other colleagues in terms of verbal violence and aggression, humiliation and shouting /screaming.24
Nearly half of healthcare providers surveyed were dissatisfied with their working conditions, and a significant proportion of them reported having experienced verbal abuse from their colleagues and the community; a phenomenon much more pronounced in North than in South Kivu. Although rare (3%), physical assaults were reported, with North Kivu again appearing more affected, both from colleagues and patients. This difference may be linked to the more persistent conflicts plaguing North Kivu.24,46
Similar violence targeting health workers by patients, colleagues, or armed groups has been documented in other conflict-affected countries like Uganda, Ethiopia, Syria, Yemen, Palestine, and Iraq.38,47–51 Indeed, to deliver quality care, healthcare providers must themselves be in good mental health and in a healthy environment, both severely compromised in conflict zones. Exposed to intense stress, violence, and secondary trauma, these professionals experienced a decline in psychological well-being, affecting their ability to provide adequate care.24,38–40
Unlike postpartum women who feel relatively safe inside facilities, providers remain vulnerable both at work and during commutes. Both groups report increasing insecurity around health centers, particularly in North Kivu—a region in near-constant conflict—compared to South Kivu.37 While some providers’ resilience enables them to manage stress constructively, contributing to the overall resilience of the healthcare system, these mechanisms should not lead to neglecting this crucial human resource, as they are not always sufficient to prevent burnout and compassion fatigue. This can also lead to a gradual decline in the quality of care provided to vulnerable populations.24,38,39,47,52,53
Our findings suggest that PCMC cannot be improved until healthcare providers have supportive and safe working environments. Furthermore, there is a need to understand patients’ experiences of care, while prioritizing patient and provider safety and supportive working environments. Improvements in the subdomain of privacy during labor, autonomy and communication could be indirectly enhanced when providers feel safe, supported, and have the time and resources for more supportive interactions with patients. Conflict-sensitive training for healthcare providers may also help them navigate these complex settings while maintaining standards of respectful care. Continuous professional development programs for maternity care providers should include modules on patients’ rights (autonomy, privacy, communication), active listening, and conflict resolution, particularly in conflict-affected settings where interpersonal trust is fragile.
The structural challenges in providing maternity care in DRC and other conflict-affected contexts begs the question as to whether the PCMC scale is a useful tool for improving maternal health services, especially when health systems may have limited capacity to provide any care. Centering patient experience is important for all health services; however contextual considerations related to security and health facility environment need to be considered. A systematic review of assessments using the PCMC scale revealed that only 3 of 41 studies globally were undertaken in conflict-affected regions since its development in 2017.44 All three studies were undertaken in the Amhara region of Ethiopia,54–56 which has experienced population displacement due to inter-communal conflicts;57 yet none addressed the effects of the conflict on the health system and health providers’ capacity to provide PCMC. Our study critically examines PCMC alongside the health facility environment and the security context and highlights not only areas for improvement within key domains of PCMC, but investment needed to ensure a safe and supportive workplace that is conducive to PCMC.
Additional research is needed to assess the validity of the PCMC scale in conflict-affected contexts and determine if additional constructs need to be explored. Our study suggests that the layered dynamics resulting from living and working in a conflict-affected context (eg, structural challenges, possible psychosocial impacts on patients and health providers, and unsupportive workplace environments) may directly or indirectly impact PCMC. The inclusion of additional items related to these dynamics may make the PCMC scale more salient to stakeholders in such contexts. Our study also opted to use the short PCMC scale to minimize data collection burden; however, the short scale has not been evaluated in any other crisis-affected settings and merits further validation.44
Some methodological limitations should be considered when interpreting these findings of our study. A primary limitation is the potential for selection bias. First, there is a risk of selection bias, by excluding health facilities with fewer deliveries which may operate under different conditions, we may have inadvertently overlooked critical insights. Additionally, data collection was confined to selected health zones within the two provinces (South and North Kivu), chosen primarily for accessibility in terms of geography and security. This topographic restriction may limit the generalizability of the results to other, potentially more insecure or remote health areas. Another bias is that of the social desirability of the part of women which would have influenced on the one hand the responses of clients to avoid any conflict or accusatory remarks towards the health structure and the providers who are sometimes close to them. Finally, the exclusion of women with cesarean deliveries, and those experienced stillbirths and newborn deaths may also have contributed to selection bias; it is likely that experiences of care for these women differed from those included in our study. Future research is therefore needed to document experiences of care for all women giving birth at facilities in this context, particularly those with adverse birth outcomes.
Conclusion
This study highlights that maternity care on conflict-affected settings continues to face significant challenges in delivering person-centered care, particularly in terms of communication, privacy and autonomy and safety, which negatively affects the quality of care and further fragments an already weakened health system. Our findings underscore the importance of addressing provider safety and well-being, which are essential for ensuring service continuity and sustaining a resilient health system.
Prioritizing respectful and dignified care during and after childbirth is vital to improving maternal health in fragile settings. Governments and humanitarian actors should establish clear communication and support protocols that define how providers interact with women and families, ensure consistent counseling, and strengthen referral and follow-up systems. Mental health services should be integrated into routine maternal and newborn care, to address the psychological distress often linked to childbirth complications and conflict exposure. Promoting equity and access requires reducing financial and geographic barriers, supporting mobile and community-based outreach, and ensuring that marginalized women (such as displaced or adolescent mothers) receive targeted support. Training providers in culturally and gender-sensitive practices, such as respectful communication, privacy protection, and inclusion of birth companions, can further enhance women’s experiences and contribute to better maternal outcomes.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB No:21922), and Université Catholique de Bukavu Ethical Committee in the DRC (UCB/CIES/NC/011/2023). All study procedures have conformed to the principles embodied in the Declaration of Helsinki. Written informed consent was obtained in-person from all respondents in advance of data collection.
Acknowledgments
We thank all the participants who took part in this study and made it possible. We also thank the research team from the Regional School of Health at the Catholic University of Bukavu, the teams from the Provincial Health Division of North and South Kivu, the team from the Directorate of Studies and Planning of the Ministry of Health, the team from the National Program for Reproductive Health of the Ministry of Health of the DRC, and the International Rescue Committee DRC office who all collaborated and supported research implementation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the UK International Development of the British Government (PO 8613) as part of the EQUAL research program consortium.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World health statistics 2016: monitoring health for the SDGs, sustainable development goals [Internet]. [cited May 18, 2025]. Available from: https://www.who.int/publications/i/item/9789241565264.
2. Strategies toward ending preventable maternal mortality (EPMM) [Internet]. [cited May 18, 2025]. Available from: https://www.who.int/publications/i/item/9789241508483.
3. Kruk ME, Pate M. The lancet global health commission on high quality health systems 1 year on: progress on a global imperative. Lancet Glob Health. 2020;8(1):e30–2. doi:10.1016/S2214-109X(19)30485-1
4. Howell EA. Reducing disparities in severe maternal morbidity and mortality. Clin Obstet Gynecol. 2018;61(2):387–399. doi:10.1097/GRF.0000000000000349
5. Anindya K, Marthias T, Vellakkal S, et al. Socioeconomic inequalities in effective service coverage for reproductive, maternal, newborn, and child health: a comparative analysis of 39 low-income and middle-income countries. EClinicalMedicine. 2021;40:101103. doi:10.1016/j.eclinm.2021.101103
6. Kassie AM, Eakin E, Endalamaw A, Zewdie A, Wolka E, Assefa Y. Effective coverage of maternal and neonatal healthcare services in low-and middle-income countries: a scoping review. BMC Health Serv Res. 2024;24(1):1601. doi:10.1186/s12913-024-12085-7
7. Shaw D, Guise JM, Shah N, et al. Drivers of maternity care in high-income countries: can health systems support woman-centred care? Lancet Lond Engl. 2016;388(10057):2282–2295. doi:10.1016/S0140-6736(16)31527-6
8. Chou VB, Walker N, Kanyangarara M. Estimating the global impact of poor quality of care on maternal and neonatal outcomes in 81 low- and middle-income countries: a modeling study. PLoS Med. 2019;16(12):e1002990. doi:10.1371/journal.pmed.1002990
9. Collins JH, Allott H, Ng’ambi W, et al. An individual-based modelling study estimating the impact of maternity service delivery on health in Malawi. Nat Commun. 2025;16(1):3925. doi:10.1038/s41467-025-59060-2
10. Amare NS, Mekuriyaw AM, Tesema GW, Ambaw YL. Intention to give birth in the health institutions and associated factors among women who gave birth in the last 6 months in Debre Berhan town, North Showa zone, Ethiopia: a community-based cross-sectional study. Front Med. 2022;9:917678. doi:10.3389/fmed.2022.917678
11. Organization WH Standards for improving quality of maternal and newborn care in health facilities. World Health Organization; 2016 [cited July 5, 2025]. Available from: https://iris.who.int/handle/10665/249155.
12. Asefa A, McPake B, Langer A, Bohren MA, Morgan A. Imagining maternity care as a complex adaptive system: understanding health system constraints to the promotion of respectful maternity care. Sex Reprod Health Matt. 2020;28(1):e1854153. doi:10.1080/26410397.2020.1854153
13. Reddy B, Thomas S, Karachiwala B, et al. A scoping review of the impact of organisational factors on providers and related interventions in LMICs: implications for respectful maternity care. PLOS Glob Public Health. 2022;2(10):e0001134. doi:10.1371/journal.pgph.0001134
14. Sacks E. Defining disrespect and abuse of newborns: a review of the evidence and an expanded typology of respectful maternity care. Reprod Health. 2017;14(1):66. doi:10.1186/s12978-017-0326-1
15. Person-centered maternity care | M4MGMT [Internet]. [cited July 5, 2025]. Available from: https://m4mgmt.org/person-centered-maternity-care/.
16. Afulani PA, Phillips B, Aborigo RA, Moyer CA. Person-centred maternity care in low-income and middle-income countries: analysis of data from Kenya, Ghana, and India. Lancet Glob Health. 2019;7(1):e96–109. doi:10.1016/S2214-109X(18)30403-0
17. Naito YT, Fukuzawa R, Ganchimeg T, et al. Validation of the person-centered maternity care scale at governmental health facilities in Cambodia. PLoS One. Mersha A, editor. 2023;18(7):e0288051. doi:10.1371/journal.pone.0288051
18. Afulani PA, Feeser K, Sudhinaraset M, Aborigo R, Montagu D, Chakraborty N. Toward the development of a short multi‐country person‐centered maternity care scale. Int J Gynecol Obstet. 2019;146(1):80–87. doi:10.1002/ijgo.12827
19. RDC-Institut National de la Statistique, École de Santé Publique de Kinshasa et ICF. Enquête Démographique et de Santé de République Démocratique du Congo 2023–2024: Rapport final. Kinshasa, RDC et Rockville, Maryland, USA: ICF; 2024.
20. Mwene-Batu P, Ndokabilya E, Lembebu JC, et al. Maternal mortality in Eastern Democratic Republic of Congo: a 10-year multi-zonal institutional death review. BMC Public Health. 2024;24(1):2280. doi:10.1186/s12889-024-19804-z
21. World Bank. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, world bank group and UNDESA/population division. 2021. Available from: https://www.who.int/publications-detail-redirect/9789240068759.
22. Trends in maternal mortality estimates 2000 to 2023: estimates by WHO, UNICEF, UNFPA, world bank group and UNDESA / population division. Available from: https://www.unfpa.org/sites/default/files/pub-pdf/9789240108462-eng.pdf.
23. Malembaka EB, Altare C, Bigirinama RN, et al. The use of health facility data to assess the effects of armed conflicts on maternal and child health: experience from the Kivu, DR Congo. BMC Health Serv Res. 2021;21(Suppl 1):195. doi:10.1186/s12913-021-06143-7
24. Lembebu C, Ngaboyeka G, Bisimwa G, et al. Working conditions and environment of maternal and neonatal healthcare providers in the context of armed conflicts and humanitarian crises of Eastern DR Congo. Discov Health Syst. 2025;4(1):40. doi:10.1007/s44250-025-00216-8
25. Gandevia B, Tovell A. DECLARATION OF HELSINKI. Med J Aust. 1964;2:320–321.
26. Democratic republic of the congo: ituri, North Kivu, South Kivu - scale up response report (reporting period july - december 2023) | OCHA. 2024 [cited July 5, 2025]. Available from: https://www.unocha.org/publications/report/democratic-republic-congo/democratic-republic-congo-ituri-north-kivu-south-kivu-scale-response-report-reporting-period-july-december-2023.
27. Health - DHIS2. [cited Jul 5, 2025]. Available from: https://dhis2.org/health/.
28. Ministère de Santé Publique SG République Démocratique du Congo. Recueil Des Normes De Creation, D’organisation Et De Fonctionnement Des Structures De La Zone De Sante En Republique Democratique Du Congo; 2019.
29. Harris PA. Research Electronic Data Capture consortium. 2019. Available from: https://www.project-redcap.org/.
30. Maternal and Newborn Quality of Care Surveys [Internet]. MCHIP. [cited May 18, 2025]. Available from: https://mchip.net/qocsurveys/.
31. Agha S, Fitzgerald L, Fareed A, et al. Quality of labor and birth care in Sindh Province, Pakistan: findings from direct observations at health facilities. PLoS One. Dandona R, editor. 2019;14(10):e0223701. doi:10.1371/journal.pone.0223701
32. Afghanistan national maternal and newborn health quality of care assessment 2016. [cited May 18, 2025]. Available from: https://www.unicef.org/afghanistan/sites/unicef.org.afghanistan/files/2018-02/afg-report-MNH-QoC2016.pdf.
33. The DHS program - Service Provision Assessments (SPA) [Internet]. [cited May 18, 2025]. Available from: https://www.dhsprogram.com/methodology/Survey-Types/SPA.cfm.
34. Afulani PA, Diamond-Smith N, Golub G, Sudhinaraset M. Development of a tool to measure person-centered maternity care in developing settings: validation in a rural and urban Kenyan population. Reprod Health. 2017;14(1):118. doi:10.1186/s12978-017-0381-7
35. StataCorp. 2025. Stata Statistical Software: release 19. College Station, TX: StataCorp LLC. In. Available from: https://www.stata.com/support/faqs/resources/citing-software-documentation-faqs/.
36. Bapolisi A, Maurage P, Cishugi MT, et al. Predictors of acute stress disorder in victims of violence in Eastern Democratic Republic of the Congo. Eur J Psychotraumatology. 2022;13(2):2109930. doi:10.1080/20008066.2022.2109930
37. Makali SL, Lembebu JC, Boroto R, et al. Violence against health care workers in a crisis context: a mixed cross-sectional study in Eastern Democratic Republic of Congo. Confl Health. 2023;17(1):44. doi:10.1186/s13031-023-00541-w
38. Elnakib S, Elaraby S, Othman F, et al. Providing care under extreme adversity: the impact of the Yemen conflict on the personal and professional lives of health workers. Soc Sci Med. 2021;272:113751.
39. Murthy RS, Lakshminarayana R. Mental health consequences of war: a brief review of research findings. World Psychiatry off J World Psychiatr Assoc WPA. 2006;5(1):25–30.
40. Ameh CA, Bishop S, Kongnyuy E, Grady K, Van den Broek N. Challenges to the provision of emergency obstetric care in Iraq. Matern Child Health J. 2011;15(1):4–11. doi:10.1007/s10995-009-0545-3
41. Ganle JK, Parker M, Fitzpatrick R, Otupiri E. A qualitative study of health system barriers to accessibility and utilization of maternal and newborn healthcare services in Ghana after user-fee abolition. BMC Pregnancy Childbirth. 2014;14(1):425. doi:10.1186/s12884-014-0425-8
42. Ahmed S, Creanga AA, Gillespie DG, Tsui AO. Economic status, education and empowerment: implications for maternal health service utilization in developing countries. Shea BJ. editor. PLoS One. 2010;5(6)e11190. doi:10.1371/journal.pone.0011190
43. Friis-hansen E, Marie S, Ravnkilde C. Social Accountability Mechanisms and Access to Public Service Delivery in Rural Africa.Danish. Copenhagen, Denmark: Institute for International Studies; 2013. doi:10.13140/2.1.3270.5929
44. Odiase OJ, Smith K, Ogunfunmi G, Afulani PA. Assessment of the person-centered maternity care scale: a global systematic review. EClinicalMedicine. 2025;82:103145. doi:10.1016/j.eclinm.2025.103145
45. Witter S, Namakula J, Wurie H, et al. The gendered health workforce: mixed methods analysis from four fragile and post-conflict contexts. Health Policy Plan. 2017;32(suppl_5):v52–62. doi:10.1093/heapol/czx102
46. Kraemer MUG, Pigott DM, Hill SC, et al. Dynamics of conflict during the Ebola outbreak in the Democratic Republic of the Congo 2018-2019. BMC Med. 2020;18(1):113. doi:10.1186/s12916-020-01574-1
47. Namakula J, Witter S. Living through conflict and post-conflict: experiences of health workers in northern Uganda and lessons for people-centred health systems. Health Policy Plan. 2014;29(Suppl 2):ii6–14. doi:10.1093/heapol/czu022
48. Legesse AY, Hadush Z, Teka H, et al. Lived experience of healthcare providers amidst war and siege: a phenomenological study of ayder comprehensive specialized hospital of tigray, Northern Ethiopia. BMC Health Serv Res. 2024;24(1):292. doi:10.1186/s12913-024-10655-3
49. Ekzayez A, Alhaj Ahmad Y, Alhaleb H, Checchi F. The impact of armed conflict on utilisation of health services in north-west Syria: an observational study. Confl Health. 2021;15(1):91. doi:10.1186/s13031-021-00429-7
50. Kitaneh M, Hamdan M. Workplace violence against physicians and nurses in Palestinian public hospitals: a cross-sectional study. BMC Health Serv Res. 2012;12(1):469. doi:10.1186/1472-6963-12-469
51. Lafta RK, Falah N. Violence against health-care workers in a conflict affected city. Med Confl Surviv. 2019;35(1):65–79. doi:10.1080/13623699.2018.1540095
52. Witter S, Wurie H, Chandiwana P, et al. How do health workers experience and cope with shocks? Learning from four fragile and conflict-affected health systems in Uganda, Sierra Leone, Zimbabwe and Cambodia. Health Policy Plan. 2017;32(suppl_3):iii3–13. doi:10.1093/heapol/czx112
53. Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol. 2004;59(1):20–28. doi:10.1037/0003-066X.59.1.20
54. Atance D, Claramunt MM, Varea X, Aburto JM. Convergence and divergence in mortality: a global study from 1990 to 2030. PLoS One. 2024;19(1):e0295842. doi:10.1371/journal.pone.0295842
55. Dagnaw FT, Kehali KY, Agago TA, Hailemeskel HS. Person-centered maternity care among mothers who gave birth in South Wollo zone public hospitals, Northeastern Ethiopia: a mixed-method study. Health Serv Insights. 2022;15:11786329221127946. doi:10.1177/11786329221127946
56. Dagnaw FT, Tiruneh SA, Azanaw MM, Desale AT, Engdaw MT. Determinants of person-centered maternity care at the selected health facilities of Dessie town, Northeastern, Ethiopia: community-based cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1):
57. Ethiopia Humanitarian Response Plan (January-December 2019) – Ethiopia. ReliefWeb. 2019 [cited July 5, 2025]. Available from: https://reliefweb.int/report/ethiopia/2019-ethiopia-humanitarian-response-plan-january-december-2019.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.