Back to Journals » Clinical Epidemiology » Volume 10
Maternal depression and antidepressant use during pregnancy and the risk of autism spectrum disorder in offspring
Authors Hagberg KW ![]() , Robijn AL
, Robijn AL ![]() , Jick S
, Jick S ![]()
Received 18 July 2018
Accepted for publication 18 September 2018
Published 1 November 2018 Volume 2018:10 Pages 1599—1612
DOI https://doi.org/10.2147/CLEP.S180618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor H Sorensen
Katrina Wilcox Hagberg, Annelies L Robijn, Susan Jick
Boston Collaborative Drug Surveillance Program, Boston University School of Public Health, Lexington, MA 02421, USA
Background: Results of some studies suggest that prenatal antidepressant exposure increases the risk of autism spectrum disorder (ASD) in offspring, while other studies suggest that depression independently increases the risk of having a child with ASD. Thus, confounding by indication is a concern.
Objective: The aim of this study was to estimate the risk of ASD in offspring of women who were exposed to antidepressants and/or had depression during pregnancy compared to unexposed women.
Materials and methods: We conducted a cohort study with nested sibling case–control analysis. Using the UK Clinical Practice Research Datalink (CPRD), we identified mother–baby pairs where the mother had ≥12 months of history before the delivery date and the child had ≥3 years of follow-up. Exposures during pregnancy were classified as 1) depression treated with antidepressants, 2) untreated depression, 3) other indications for antidepressant use, and 4) 4:1 match of unexposed women with no history of depression or antidepressant use. We calculated the prevalence of ASD and relative risk (RR) with 95% CI. In the sibling analysis, we compared exposure among ASD cases to that of non-ASD siblings born to the same mother. We calculated ORs and 95% CIs for women with treated and untreated depression, compared to unexposed.
Results: We identified 2,154 offspring with ASD among 194,494 mother–baby pairs. Compared to unexposed, the RR of ASD was 1.72 (95% CI 1.54–1.93) for treated depression and 1.50 (95% CI 1.28–1.75) for untreated depression, while the RR was not elevated in women who received antidepressants for other indications (RR =0.73, 95% CI 0.41–1.29). Additional analyses to assess the effects of severity of depression suggest that the risk of ASD in offspring increases with increasing severity, not with the antidepressant treatment. The results of the sibling analysis were similar to the main analysis.
Conclusion: Women with depression during pregnancy have an increased risk of having a child with ASD, regardless of antidepressant use.
Keywords: depression, pregnancy, antidepressants, autism, autism spectrum disorder
Plain language summary
Depression is a common condition in women, often occurring during childbearing years. Women may be given antidepressants by a doctor to treat depression during pregnancy. Results of prior studies suggest that antidepressant exposure during pregnancy increases the risk of having a child with autism spectrum disorder (ASD), while results of other studies suggest that depression itself increases the chance of having a child with ASD. This study, using the UK Clinical Practice Research Datalink (CPRD), was conducted to estimate the risk of ASD in children of women who took antidepressants and/or had depression during pregnancy compared to unexposed women. The results of this study suggest that women with depression during pregnancy, regardless of antidepressant use, have an increased risk of having a child with ASD compared to women who do not have depression.
Introduction
Depression is a common condition in women, with prevalence peaking during childbearing years.1–3 Untreated depression during pregnancy may have a negative impact on the offspring,4,5 including problems involving affect, cognition, and neuroendocrine and brain function.6 Prescribing of antidepressants during pregnancy, currently estimated between 1% and 13% of pregnant women, increased steadily between 1990 and 2005 and have since remained stable.7–13 Selective serotonin reuptake inhibitors (SSRIs) are the most commonly prescribed antidepressants during pregnancy. There are concerns regarding the impact of prenatal antidepressant use on offspring because these drugs are known to cross the placenta and serotonin is critical for fetal brain development.14,15
Autism spectrum disorders (ASDs) are neurodevelopmental disorders characterized by deficits in social function and communication with the presence of restricted or repetitive behavior, interests, or activities. Epidemiological studies have shown dramatic increases in the rate of ASD diagnosis,16–18 now estimated to affect around 1% of children globally.16 The etiology of ASD is not well understood; however, both genetic and environmental factors are thought to play an important role. It has been theorized that dysfunctional serotonin signaling is a potential causal mechanism for ASD.15,19
The results of epidemiological studies of maternal prenatal antidepressant medication use (primarily SSRIs) and the risk of ASD in offspring have been mixed.20–32 Some studies found increased risks of 1.5–4.5-fold,20–22,26,28 while the results of other studies suggest that depression independently increases the risk of having a child with ASD.23–25 Thus, confounding by indication is a concern.
We conducted a cohort study using a large electronic database with mother–baby linkage to estimate the risk of ASD in offspring of women who were exposed to antidepressants and/or had depression during pregnancy compared to unexposed women. We also conducted a nested sibling case–control analysis to control for genetic risk factors, other potential confounders, and maternal predisposition to depression.
Materials and methods
Data source
This study was conducted using the CPRD, a large, population-based electronic medical database. Participating general practitioners (GPs) contributed de-identified data including medical diagnoses (recorded using Read codes), details of prescription drugs, symptoms, and specialist visits.33,34 Results of validation studies indicated that the data were of high accuracy and completeness.35–37 The mother–baby linkage has been used in previous studies on maternal drug exposures and outcomes in offspring.38–42
Source population
The source population consisted of mothers, aged 13–44 years, and their live-born, singleton infants born between 1989 and 2011. Mothers were required to have at least 12 months of recorded history before the baby’s delivery date, and the children were required to have at least 3 years of follow-up after birth. We excluded mother–baby sets where the delivery date could not be identified.
Cohort identification
The exposure period for mothers was the year before the baby’s delivery date. Cohort entry was the baby’s delivery date minus 365 days. From the source population, we identified three cohorts of exposed women: 1) those with depression treated with antidepressants (diagnosis and ≥1 antidepressant prescription during the exposure period), 2) those with untreated depression (recent history of treated depression but no antidepressants during the exposure period), and 3) those who were prescribed antidepressants for other indications (women in this group had no history of depression). Other indications for antidepressant use included anxiety, bipolar disorder, manic disorder, schizophrenia, migraine, neuralgia, fibromyalgia, insomnia, smoking cessation, or pain. To each exposed mother, we matched (4:1) unexposed women who had neither depression nor prescriptions for antidepressants prior to the baby’s delivery date and matched on mother’s year of birth (±2 years), baby’s year of birth (±2 years), and general practice attended (Figure 1).
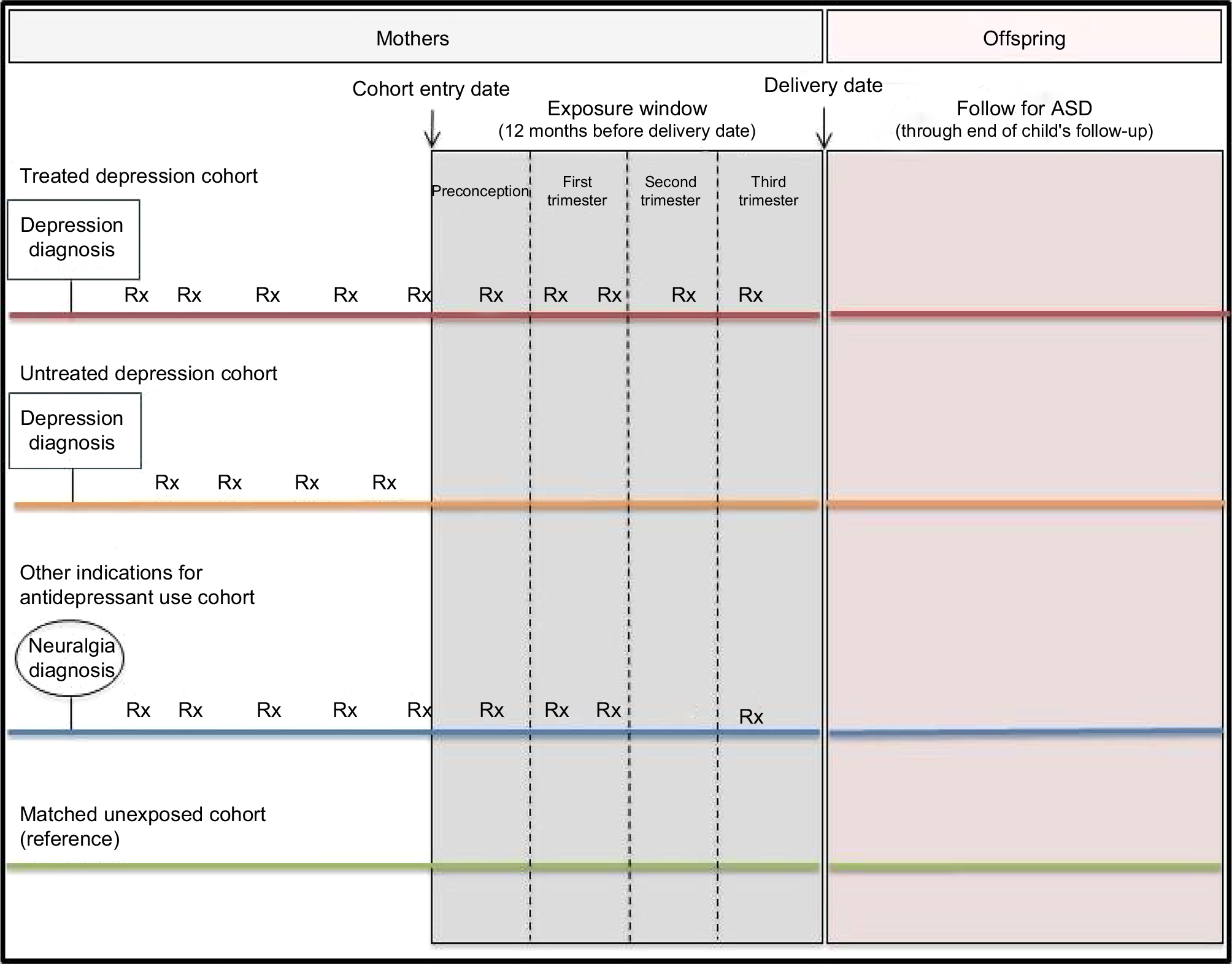 | Figure 1 Diagram of cohort identification, exposure window definition, and follow-up period. Note: Rx, antidepressant prescription. Abbreviation: ASD, autism spectrum disorder. |
Antidepressant exposure
We evaluated the timing of antidepressant use during the exposure period as follows: preconception (delivery date minus 281–365 days), first trimester (delivery date minus 191–280 days), second trimester (delivery date minus 101–190 days), and third trimester (delivery date minus 100 days; Figure 1). We calculated the prescription duration as the total number of pills prescribed divided by the number of pills prescribed per day. We also evaluated antidepressant class: SSRIs, serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), other antidepressants (eg, monoamine oxidase inhibitors, tetracyclic antidepressants, and norepinephrine and dopamine reuptake inhibitors), and multiple classes.
ASD case identification
We identified all children with at least one Read diagnostic code indicating ASD recorded at any time, including codes for autism, Asperger’s syndrome, and pervasive developmental disorder (PDD). Validation studies have indicated that over 90% of ASD diagnoses in the CPRD were confirmed upon record review.43,44 Validation results of this study have been described previously,45 and the Read codes used to identify cases are listed in Table S1.
Nested sibling case–control analysis
We conducted a sibling case–control analysis of maternal pregnancy exposures in ASD cases compared to non-ASD siblings of the same mother. This analysis controlled for genetic, time-invariant, and unmeasured confounders (eg, socioeconomic status, mother’s education, and race/ethnicity) as well as maternal predisposition to depression. From the cohort study, we identified all ASD cases who had one or more siblings. The sibling was eligible as a control if he/she was the same sex as the ASD case, had no diagnosis of ASD at any time, and had at least 3 years of follow-up after birth and if the mother had at least 12 months of recorded history before the sibling’s delivery date.
Covariates
We assessed the presence of various covariates at the cohort entry date (cohort study) and at the child’s delivery date (sibling analysis). Covariates were identified from literature review as well as by comparing characteristics between the exposed and nonexposed cohorts. We considered characteristics that changed the main effect estimate by more than 10% to be potential confounders. We evaluated the following covariates in the mothers: age, body mass index (BMI: <18.5, 18.5–24.9, 25.0–29.9, ≥30, unknown), smoking status (never, current, former, unknown), alcohol abuse, drug abuse, diabetes, hypertension, hyperlipidemia, anxiety, other psychiatric conditions (bipolar, schizophrenia), and parity. We evaluated duration of the last episode of treated depression prior to cohort entry, calculated as continuous use of any antidepressant until either cohort entry or a gap of at least 180 days between prescriptions, categorized as <12, 12–35.9, and 36+ months, or unknown duration (those who had the first depression diagnosis recorded at the start of their record and had duration of <36 months). We also evaluated the number of different antidepressants prescribed during the last episode of treated depression. Finally, we evaluated sex, birth order, and year of birth in the children.
Statistical analyses
We estimated the prevalence of ASD with 95% CIs for each cohort, calculated as the number of ASD cases divided by the number of pregnancies that resulted in live-born children who survived to age 3 years. We estimated the prevalence of ASD overall and stratified by the timing of exposure during pregnancy (trimester) and antidepressant class. The RR and 95% CI of ASD in the offspring of women with treated depression and untreated depression and women who used antidepressants for other indications, compared to unexposed, were estimated using generalized estimating equations via PROC GENMOD in SAS (SAS Institute, Cary NC, USA) to adjust for the inclusion of women with more than one pregnancy. We also calculated RRs adjusted for maternal BMI, smoking status, parity, anxiety, or other psychiatric disorders. To assess effect modification, we conducted analyses stratified by parity, maternal duration of depression history, number of different types of antidepressants prescribed in the last episode of depression, and presence or absence of anxiety/other psychiatric disorders. We conducted three sensitivity analyses restricted to 1) women with at least 3 years of recorded history prior to the baby’s delivery date, 2) children with at least 5 years of follow-up, and 3) ASD cases with additional Read codes that supported the presence of ASD (eg, specialist referrals and visits, treatment, or codes indicating developmental delay, speech delay, or behavioral problems) to assess the potential for case misclassification.
For the sibling analysis, we used conditional logistic regression to estimate ORs with 95% CIs, adjusted for child’s birth year, child’s birth order, and maternal age at delivery. All analyses were performed using SAS statistical software version 9.3 (SAS Institute Inc., Cary, NC, USA).
The protocol for this study was reviewed and approved by the Independent Scientific Advisory Committee (ISAC) for Medicines and Healthcare Products Regulatory Agency (MHRA) database research (protocol number 15_256), and the protocol was made available to the journal reviewers. This study is based in part on data from the CPRD obtained under license from the UK Medicines and Healthcare Products Regulatory Agency. These data are provided by patients and collected by the National Health Service (NHS) as part of their care and support. The interpretation and conclusions contained in this study are those of the author’s alone.
Results
We identified 40,387 eligible exposed mother–baby pairs, of whom 12,994 women had untreated depression, 25,778 had treated depression, and 1,615 received antidepressants for indications other than depression (32.4% for anxiety or other psychiatric disorders, 26.0% for pain, 13.9% for migraine, 11.8% for insomnia, 11.8% for smoking cessation, and 4.1% for neuralgia or fibromyalgia). To these, we matched 154,107 unexposed mother–baby pairs. Exposed women were more likely than unexposed to be current smokers and to have anxiety/other psychiatric diagnoses at cohort entry (Table 1). The mean length of recorded history in the mothers was long (>10 years) and similar for each cohort. The length of follow-up in the babies was also long (>8 years) and similar for the exposed and unexposed cohorts.
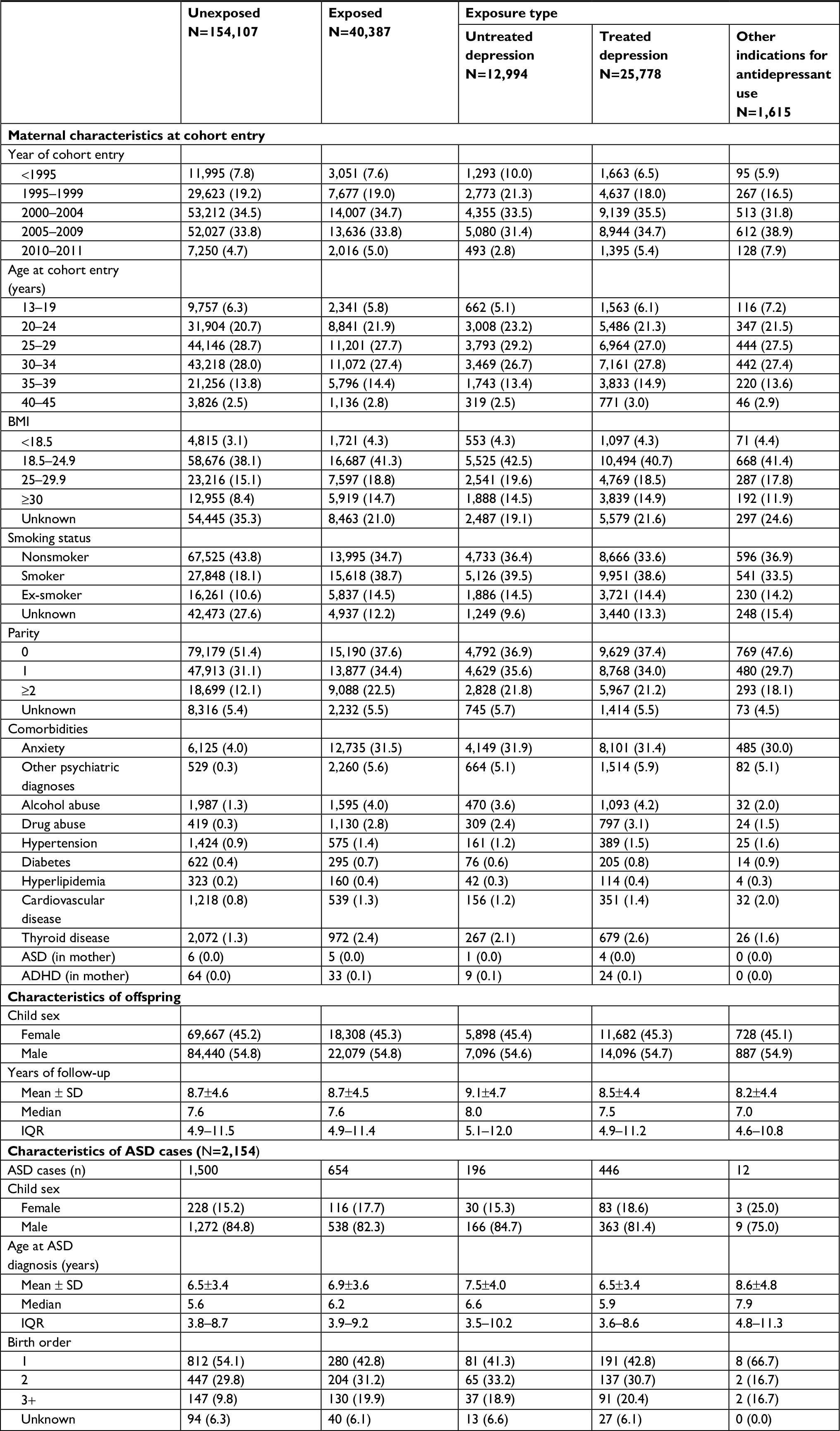 | Table 1 Characteristics of mothers and offspring, by exposure Note: Data are presented as n (%) throughout, unless otherwise indicated (mean, median, IQR). Abbreviations: ADHD, attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; BMI, body mass index; IQR, interquartile range; SD, standard deviation. |
We identified 2,154 ASD cases (Table 1). The majority of cases (84.8%) were male, and 50.7% were first born. The peak age at first ASD diagnosis was 3 years, and more than half were diagnosed before age 6 years (median 5.8 years). The prevalence of ASD, per 1,000 pregnancies, was 9.7 (95% CI 9.3–10.2) among children of unexposed women, 15.1 (95% CI 13.1–17.3) for untreated depression, 17.3 (95% CI 15.8–19.0) for treated depression, and 7.4 (95% CI 4.0–12.6) for those who received antidepressants for other indications. Compared to children of unexposed women, the adjusted RRs were 1.49 (95% CI 1.27–1.75) and 1.70 (95% CI 1.51–1.92) for children whose mothers had untreated and treated depression, respectively, and 0.73 (95% CI 0.41–1.29) for children of mothers who received antidepressants for other indications (Table 2).
 | Table 2 Prevalence of ASD by exposure during a year before delivery date Notes: aAdjusted for child sex, maternal BMI, smoking status, parity, anxiety, and other psychiatric disorders. Abbreviations: ASD, autism spectrum disorder; BMI, body mass index. |
When we evaluated the timing of antidepressant use (Table 3), there was a small increased risk for women with depression who received antidepressants during the preconception period only (RR =1.42, 95% CI 1.14–1.76), compared to unexposed, whereas the risk was higher among children of women with depression who were treated during one or more trimesters of pregnancy (RR =1.82, 95% CI 1.60–2.06). The RR was elevated for antidepressant use in all trimesters of pregnancy. When we evaluated exposure by antidepressant class (Table 3), the risks were elevated among those who were exposed to SSRIs only (1.68, 95% CI 1.46–1.92), TCAs only (1.95, 95% CI 1.58–2.40), and for users of multiple classes (1.78, 95% CI 1.29–2.45), compared to children of unexposed women. The RRs were null for children of women who received antidepressants for indications other than depression, regardless of the timing of use during pregnancy (Table 3) and antidepressant class (Table 3).
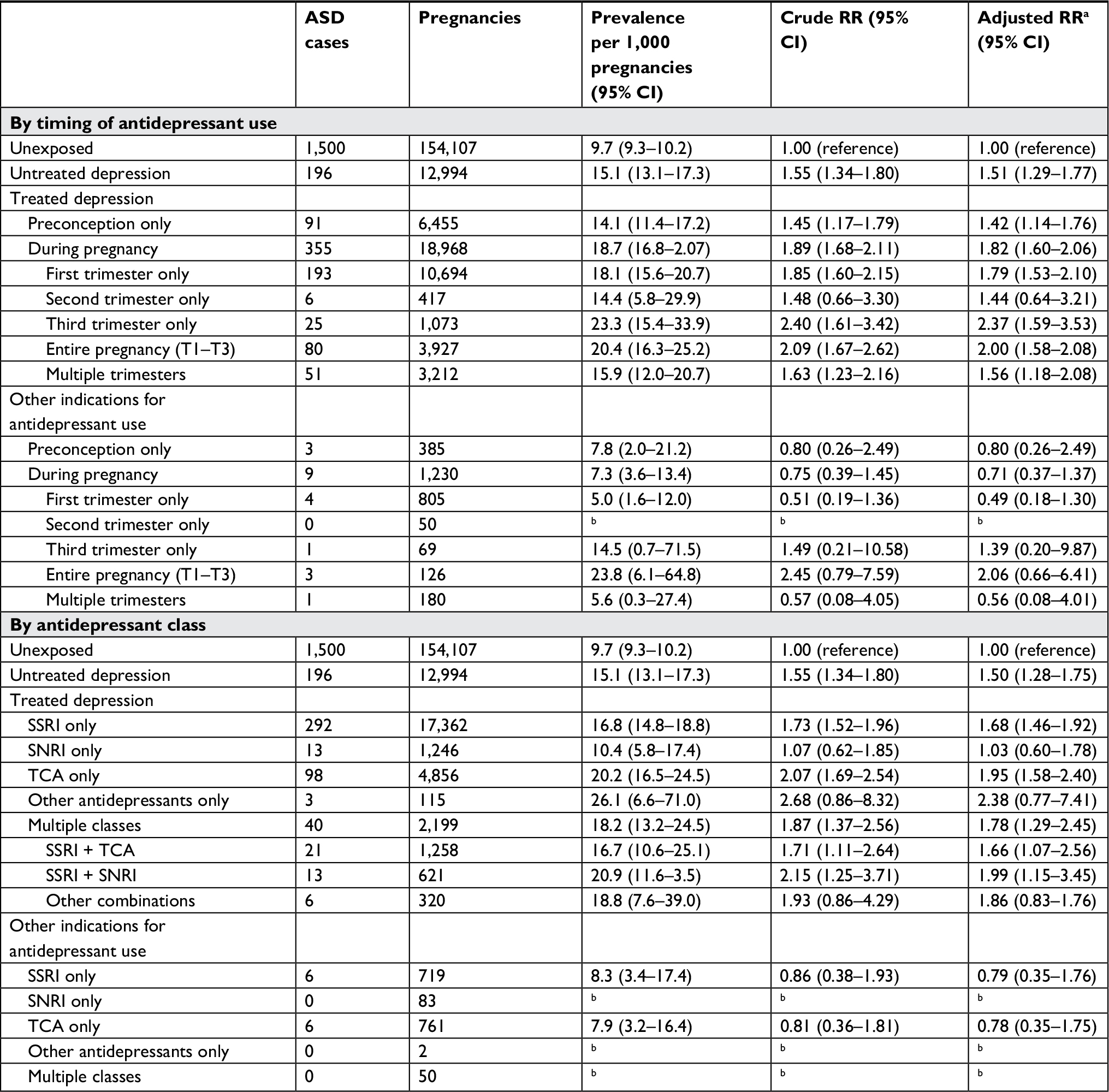 | Table 3 Prevalence of ASD by exposure, stratified by timing of antidepressant use and antidepressant class Notes: aAdjusted for child sex, maternal BMI, smoking status, parity, anxiety, and other psychiatric disorders. bToo few cases to calculate a stable estimate. Abbreviations: ASD, autism spectrum disorder; BMI, body mass index; SNRI, serotonin and norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant. |
We conducted three analyses to evaluate effect modification by the severity of depression (Table 4). The risk of ASD increased with longer duration of depression before cohort entry for both treated and untreated depression, although the rates were slightly higher among children of women with treated depression. We also stratified the estimates by the number of different antidepressants prescribed before cohort entry: compared to children of unexposed women, the risk of ASD was elevated among children of women who were prescribed two or more different types of antidepressants before cohort entry, regardless of having treated or untreated depression during pregnancy. Finally, among children of women with treated or untreated depression, the risk of ASD was elevated regardless of the presence of anxiety/other psychiatric disorders; however, the risks were higher among depressed women with comorbid anxiety/psychological disorder. In contrast, among children of unexposed women and women who used antidepressants for other indications, the risk of ASD was only elevated among those whose mothers had comorbid anxiety/psychological disorder.
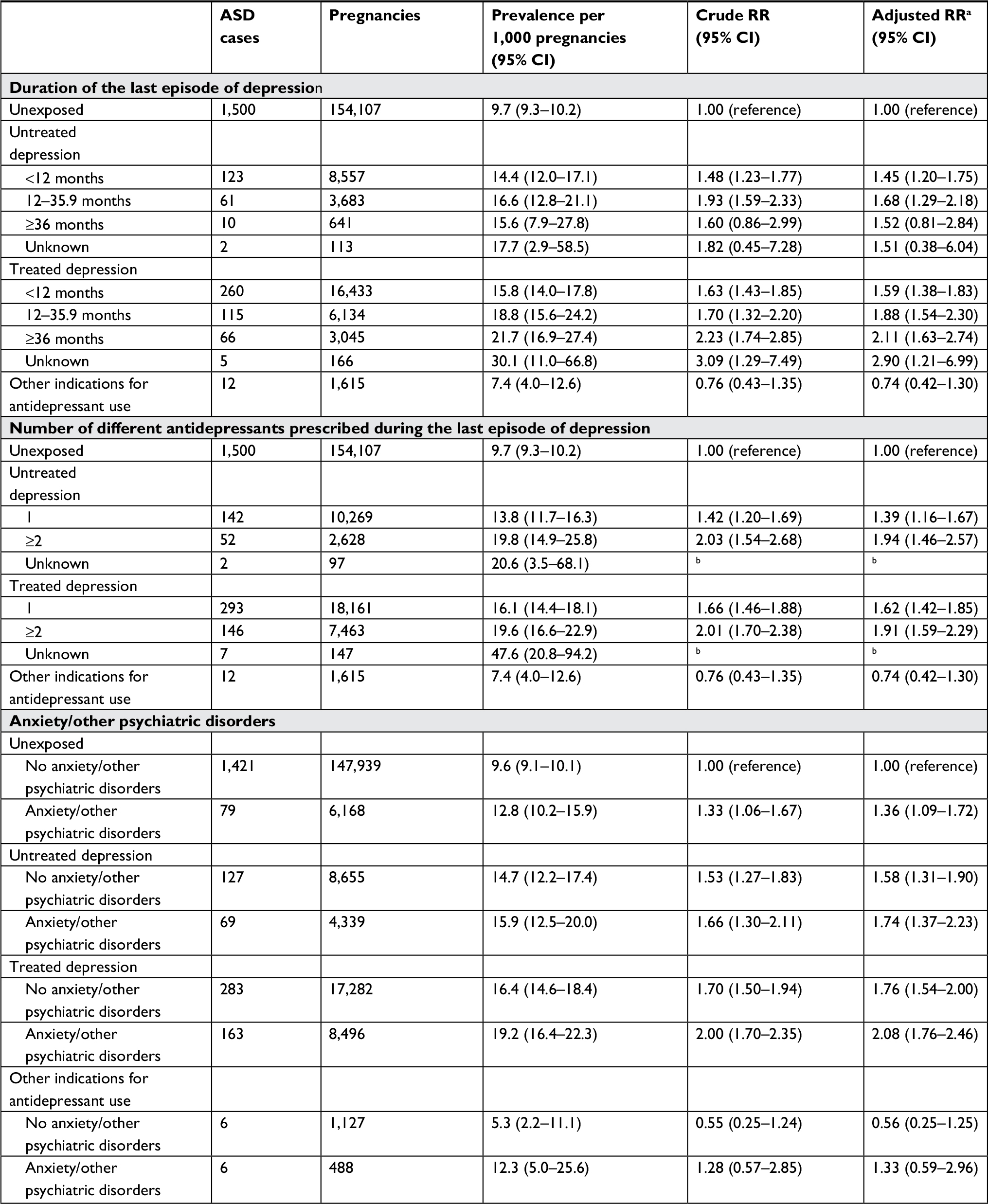 | Table 4 Prevalence of ASD by exposure, stratified by the duration of the last episode of depression before cohort entry, number of antidepressants prescribed during the last episode of depression before cohort entry, and the presence of anxiety and/or other psychiatric disorders Notes: aAdjusted for child sex, maternal BMI, smoking status, parity, anxiety, and other psychiatric disorders. bToo little data to calculate a stable estimate. Abbreviations: ASD, autism spectrum disorder; BMI, body mass index. |
The results were similar to the main analysis when we stratified by parity (no prior births, ≥1 prior birth) and in all three sensitivity analyses, where we restricted the population to 1) children of women who had at least 3 years of recorded history in which to assess exposure, 2) children who had at least 5 years of follow-up in which to assess the impact of follow-up time requirements, and 3) cases with other supporting evidence to assess case misclassification.
Nested sibling case–control analysis
There were 601 same-sex siblings who did not have an ASD diagnosis matched to 531 ASD cases (Table S2). After adjusting for child’s birth year, birth order, and maternal age at delivery, the risk of ASD in offspring of mothers with untreated depression was 1.18 (95% CI 0.64–2.20) and 1.53 (95% CI 0.89–2.62) for treated depression, compared to unexposed.
Discussion
The results of our study suggest that women with depression during pregnancy have an increased risk of having a child with ASD compared to unexposed women. The risk was slightly higher among women with treated depression (RR =1.70) compared to untreated depression (RR =1.49); however, the finding that the risk of ASD was not elevated in women who were prescribed antidepressants for other indications (RR =0.73) provides evidence that antidepressants are not themselves associated with the increased risk. Rather, the results of our study suggest that the slight increase in risk with antidepressant use reflects differences in the underlying severity of depression.
Numerous published studies have reported an increased risk of ASD in offspring associated with prenatal antidepressant use, although the magnitude of effects varied widely.20–32 In studies that accounted for potential confounding by indication, the observed increase in risk with the use of antidepressants was attenuated when results were adjusted for maternal affective disorders.23–26,28,32,33 Hviid et al23 reported that adjustment for psychiatric diagnoses contributed the biggest change in effect (crude incidence rate ratio [IRR] =1.62, 95% CI 1.23–2.13 vs fully adjusted IRR =1.20, 95% CI 0.90–1.61). Clements et al27 reported an independent effect of maternal major depressive disorder of 1.74 (95% CI 1.35–2.23), inclusion of which in the model attenuated the effect of antidepressant use during pregnancy from 1.49 (95% CI 1.01–2.18) to 1.10 (95% CI 0.70–1.70). In three studies that conducted analyses restricted to women with a history of psychiatric disorders, antidepressant use during pregnancy was not associated with a material increase in ASD risk.22,26,28 Two recent studies estimated that the risk of having a child with ASD was around 1.4 among women who used antidepressants before (but not during) pregnancy, while the risk among women exposed during pregnancy was around 1.60 to 1.75.31,32 These are similar to our estimates among women with untreated (1.49) and treated depression (1.70). Finally, if antidepressant use does increase the risk of ASD, the elevation should be present among women who were prescribed antidepressants for other indications; however, in our study, there was no increased risk of having an offspring with ASD among these women. Overall, the results of these studies suggest that the observed increase in risk is associated with depression, not its treatment.
The results of our various stratified analyses suggest that there are differences in risk by the severity of depression. By definition, the untreated depression cohort is likely to have less severe depression than those in the treated depression cohort; thus, the observed difference in risk may reflect differences in depression severity. In addition, the risk of ASD among women who received SSRIs only (RR =1.68), which in the UK are often prescribed as first-line treatment, was slightly lower than that of women who were prescribed TCAs only (RR =1.95), which are often prescribed as second-line therapy.46 Finally, the risk of having a child with ASD was higher for women who were prescribed two or more different types of antidepressants before cohort entry as well as among women with anxiety or other psychiatric disorders, regardless of antidepressant exposure during pregnancy. This interpretation is supported by the results of other published studies that used specialist care records to ascertain depression status.24,25,29 Finally, three studies reported higher risks with SSRI exposure in the second and third trimester of pregnancy.25,29,32 In our analysis, the risk estimates were slightly higher for women with depression who were prescribed antidepressants during the third trimester or for the entire pregnancy than for women with depression who were prescribed antidepressants during first trimester only. It is possible that higher risk estimates that persist into late pregnancy reflect effects of depression severity, as women with more severe depression may not be able to discontinue antidepressant treatment during pregnancy.
Heritability is known to be a strong risk factor for ASD,47 and genetic studies suggest that ASD and depression may share specific single-nucleotide polymorphisms;48 thus, the increase in ASD in offspring of women with depression may reflect genetic predisposition. Sibling study designs offer a way to control for genetics as well as other unmeasured time-invariant factors. Sørensen et al22 reported that, among 2,765 families in which at least one child had ASD, the risk of ASD in children exposed to antidepressants for any indication during pregnancy was 1.1 (95% CI 0.5–2.3) compared to their unexposed siblings. In their sibling comparison, Sujan et al31 reported that the risk of ASD in children exposed to antidepressants in the first trimester was 0.83 (95% CI 0.62–1.13) compared to unexposed siblings. Brown et al32 estimated that the risk of ASD in children exposed to two or more antidepressant prescriptions was 1.60 (95% CI 0.69–3.74) compared to unexposed siblings. In our sibling analysis based on 136 discordant sibling pairs, the risk of having a child with ASD among women with untreated depression (RR =1.18, 95% CI 0.64–2.20) was similar to that of the Sørensen et al’s study, whereas the magnitude of effect was slightly higher among women with treated depression (RR =1.53, 95% CI 0.89–2.62), an estimate that was similar to that of the Brown et al’s study. These sibling analyses suggest that after controlling for genetics and time-invariant confounders, prenatal antidepressant use does not significantly increase the risk of ASD in offspring, although there may remain a difference in risk by the severity of depression during pregnancy.
Strengths of our population-based study include use of the CPRD, a large, validated, longitudinal primary care database known for highly accurate diagnoses, completeness of drug prescribing information, and mother–baby linkage. All information on diseases and drug exposures was recorded prospectively; therefore, there is no risk of recall bias. We evaluated the effect of all types of commonly prescribed antidepressants, not just SSRIs. We matched the cohorts on year of entry to control for confounding related to changes in prescribing of antidepressants during pregnancy and in ASD diagnostic criteria and screening practices during the study period. ASD diagnoses in the CPRD have been shown to be of high validity,43–45 and the prevalence of ASD among unexposed women in our study was similar to that reported in other studies.16,49–52 We found known risk factors to be independently associated with ASD (eg, child sex and parity), providing further confidence in the data quality. We relied on GP-recorded diagnoses of depression and ASD, rather than being restricted to diagnoses made in secondary or specialty care settings. Therefore, our study represents a range of depression and ASD severity, and it is unlikely that these diagnoses are underreported in these data. The mean length of recorded history in the mothers (~10 years) and follow-up in the babies (~8 years) was long and similar for each cohort; thus, we are unlikely to have misclassified exposure status in the mothers or to have missed ASD cases. We were able to control for genetics, unmeasured time-invariant factors, and maternal predisposition for depression by conducting a sibling analysis. Finally, we carefully controlled for confounding by indication by creating separate cohorts of pregnant women with treated and untreated depression and with other indications for antidepressant use. Although this last cohort of women was small (n=1,615), this was the first time this association has been evaluated in a cohort of pregnant women who used antidepressants for other indications of use.
We did not have complete information on fathers and, therefore, were unable to evaluate the effects of paternal risk factors on this association. We were unable to evaluate the effect of other indications for antidepressant use in the sibling analysis because of small numbers (n=2). Drug information in the CPRD covers written, but not dispensed prescriptions; therefore, we cannot be sure that women used all the prescribed antidepressants. Exposure misclassification may have occurred if a woman stopped using her prescription soon after she found out she was pregnant, particularly in the analysis by the timing of exposure; however, the RRs did not materially change among those with repeated prescriptions. We did not evaluate the effect of antidepressant dose in this study; this should be evaluated in future research on this association. We did not have information on socioeconomic status or race/ethnicity and, therefore, we could not explore these as covariates. However, the population of the UK is predominantly white, and we matched on general practice attended which may have controlled for socioeconomic status to some degree because people who attend the same practices tend to live in the same communities. Finally, there is concern about the potential for detection bias in all studies evaluating this association; that is, children of mothers with depression may be screened more frequently by their GPs. However, it is unlikely that differential case ascertainment by exposure occurred because the length of follow-up in children was long (~8 years) and the age at ASD diagnosis was similar for all cohorts. In addition, only 0.3% of the babies in our study were born after the publication of the first study that suggested an association between prenatal antidepressant use and ASD; thus, changes in screening practices by maternal exposure status are unlikely to have materially impacted our study results.
Conclusion
The results of our study suggest that, compared to unexposed women, women with depression during pregnancy have an increased risk of having a child with ASD, regardless of antidepressant use. It is reassuring that 97% of woman who used antidepressants during pregnancy in this study did not have a child with ASD. Future research directions include further investigation into severity of depression on this association, evaluation of antidepressant dose, and replication of the analysis in pregnant women who use antidepressants for other indications among a large cohort of women.
Acknowledgments
This study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award number R01HD084680. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. All the authors had independence from the funding source. Part of this study was presented as a podium presentation at the 33rd International Conference on Pharmacoepidemiology & Therapeutic Risk Management, Palais des congrès de Montréal, Montréal, Canada, August 26–30, 2017.
Disclosure
The authors report no conflicts of interest in this work.
References
Nulman I, Rovet J, Stewart DE, et al. Neurodevelopment of children exposed in utero to antidepressant drugs. N Engl J Med. 1997;336(4):258–262. | ||
Wisner KL, Gelenberg AJ, Leonard H, Zarin D, Frank E. Pharmacologic treatment of depression during pregnancy. JAMA. 1999;282(13):1264–1269. | ||
Emslie G, Judge R. Tricyclic antidepressants and selective serotonin reuptake inhibitors: use during pregnancy, in children/adolescents and in the elderly. Acta Psychiatr Scand Suppl. 2000;403:26–34. | ||
Goodman SH. Depression in mothers. Annu Rev Clin Psychol. 2007;3:107–135. | ||
Dunkel Schetter C. Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Annu Rev Psychol. 2011;62:531–558. | ||
El Marroun H, White T, Verhulst FC, Tiemeier H. Maternal use of antidepressant or anxiolytic medication during pregnancy and childhood neurodevelopmental outcomes: a systematic review. Eur Child Adolesc Psychiatry. 2014;23(10):973–992. | ||
Cooper WO, Willy ME, Pont SJ, Ray WA. Increasing use of antidepressants in pregnancy. Am J Obstet Gynecol. 2007;196(6):544.e1-5. | ||
Alwan S, Reefhuis J, Rasmussen SA, Friedman JM. Patterns of antidepressant medication use among pregnant women in a United States population. J Clin Pharmacol. 2011;51(2):264–270. | ||
Bakker MK, Kölling P, van den Berg PB, de Walle HE, de Jong van den Berg LT. Increase in use of selective serotonin reuptake inhibitors in pregnancy during the last decade, a population-based cohort study from the Netherlands. Br J Clin Pharmacol. 2008;65(4):600–606. | ||
El Marroun H, Jaddoe VW, Hudziak JJ, et al. Maternal use of selective serotonin reuptake inhibitors, fetal growth, and risk of adverse birth outcomes. Arch Gen Psychiatry. 2012;69(7):706–714. | ||
Munk-Olsen T, Gasse C, Laursen TM. Prevalence of antidepressant use and contacts with psychiatrists and psychologists in pregnant and postpartum women. Acta Psychiatr Scand. 2012;125(4):318–324. | ||
Bobo WV, Epstein RA, Hayes RM, et al. The effect of regulatory advisories on maternal antidepressant prescribing, 1995-2007: an interrupted time series study of 228,876 pregnancies. Arch Womens Ment Health. 2014;17(1):17–26. | ||
Petersen I, Gilbert RE, Evans SJ, Man SL, Nazareth I. Pregnancy as a major determinant for discontinuation of antidepressants: an analysis of data from The Health Improvement Network. J Clin Psychiatry. 2011;72(7):979–985. | ||
Gentile S. Prenatal antidepressant exposure and the risk of autism spectrum disorders in children. Are we looking at the fall of Gods? J Affect Disord. 2015;182:132–137. | ||
Harrington RA, Lee LC, Crum RM, Zimmerman AW, Hertz-Picciotto I. Serotonin hypothesis of autism: implications for selective serotonin reuptake inhibitor use during pregnancy. Autism Res. 2013;6(3):149–168. | ||
Baxter AJ, Brugha TS, Erskine HE, Scheurer RW, Vos T, Scott JG. The epidemiology and global burden of autism spectrum disorders. Psychol Med. 2015;45(3):601–613. | ||
Hagberg KW, Jick H. Autism in the UK for birth cohorts 1988–2001. Epidemiology. 2010;21(3):426–427. | ||
Kaye JA, del Mar Melero-Montes M, Jick H. Mumps, measles, and rubella vaccine and the incidence of autism recorded by general practitioners: a time trend analysis. BMJ. 2001;322(7284):460–463. | ||
Mulder EJ, Anderson GM, Kema IP, et al. Platelet serotonin levels in pervasive developmental disorders and mental retardation: diagnostic group differences, within-group distribution, and behavioral correlates. J Am Acad Child Adolesc Psychiatry. 2004;43(4):491–499. | ||
Croen LA, Grether JK, Yoshida CK, Odouli R, Hendrick V. Antidepressant use during pregnancy and childhood autism spectrum disorders. Arch Gen Psychiatry. 2011;68(11):1104–1112. | ||
Eriksson MA, Westerlund J, Anderlid BM, Gillberg C, Fernell E. First-degree relatives of young children with autism spectrum disorders: some gender aspects. Res Dev Disabil. 2012;33(5):1642–1648. | ||
Sørensen MJ, Grønborg TK, Christensen J, et al. Antidepressant exposure in pregnancy and risk of autism spectrum disorders. Clin Epidemiol. 2013;5:449–459. | ||
Hviid A, Melbye M, Pasternak B. Use of selective serotonin reuptake inhibitors during pregnancy and risk of autism. N Engl J Med. 2013;369(25):2406–2415. | ||
Rai D, Lee BK, Dalman C, Golding J, Lewis G, Magnusson C. Parental depression, maternal antidepressant use during pregnancy, and risk of autism spectrum disorders: population based case-control study. BMJ. 2013;346:f2059. | ||
Gidaya NB, Lee BK, Burstyn I, Yudell M, Mortensen EL, Newschaffer CJ. In utero exposure to selective serotonin reuptake inhibitors and risk for autism spectrum disorder. J Autism Dev Disord. 2014;44(10):2558–2567. | ||
Harrington RA, Lee LC, Crum RM, Zimmerman AW, Hertz-Picciotto I. Prenatal SSRI use and offspring with autism spectrum disorder or developmental delay. Pediatrics. 2014;133(5):e1241–e1248. | ||
Clements CC, Castro VM, Blumenthal SR, et al. Prenatal antidepressant exposure is associated with risk for attention-deficit hyperactivity disorder but not autism spectrum disorder in a large health system. Mol Psychiatry. 2015;20(6):727–734. | ||
Malm H, Brown AS, Gissler M, et al. Gestational Exposure to Selective Serotonin Reuptake Inhibitors and Offspring Psychiatric Disorders: A National Register-Based Study. J Am Acad Child Adolesc Psychiatry. 2016;55(5):359–366. | ||
Boukhris T, Sheehy O, Mottron L, Bérard A. Antidepressant Use During Pregnancy and the Risk of Autism Spectrum Disorder in Children. JAMA Pediatr. 2016;170(2):117–124. | ||
Castro VM, Kong SW, Clements CC, et al. Absence of evidence for increase in risk for autism or attention-deficit hyperactivity disorder following antidepressant exposure during pregnancy: a replication study. Transl Psychiatry. 2016;6:e708. | ||
Sujan AC, Rickert ME, Öberg AS, et al. Associations of maternal antidepressant use during the first trimester of pregnancy with preterm birth, small for gestational age, autism spectrum disorder, and attention-deficit/hyperactivity disorder in offspring. JAMA. 2017;317(15):1553–1562. | ||
Brown HK, Ray JG, Wilton AS, Lunsky Y, Gomes T, Vigod SN. Association Between Serotonergic Antidepressant Use During Pregnancy and Autism Spectrum Disorder in Children. JAMA. 2017;317(15):1544–1552. | ||
Lawson DH, Sherman V, Hollowell J. The General Practice Research Database. Scientific and Ethical Advisory Group. QJM. 1998;91(6):445–452. | ||
Herrett E, Gallagher AM, Bhaskaran K, et al. Data Resource Profile: Clinical Practice Research Datalink (CPRD). Int J Epidemiol. 2015;44(3):827–836. | ||
Jick H, Jick SS, Derby LE. Validation of information recorded on general practitioner based computerised data resource in the United Kingdom. BMJ. 1991;302(6779):766–768. | ||
Jick H, Terris BZ, Derby LE, Jick SS. Further validation of information recorded on a general practitioner based computerized data resource in the united kingdom. Pharmacoepidemiol Drug Safety. 1992;1(6):347–349. | ||
Jick SS, Kaye JA, Vasilakis-Scaramozza C, et al. Validity of the general practice research database. Pharmacotherapy. 2003;23(5):686–689. | ||
Vasilakis-Scaramozza C, Aschengrau A, Cabral H, Jick SS. Antidepressant use during early pregnancy and the risk of congenital anomalies. Pharmacotherapy. 2013;33(7):693–700. | ||
Vasilakis-Scaramozza C, Aschengrau A, Cabral HJ, Jick SS. Antihypertensive drugs and the risk of congenital anomalies. Pharmacotherapy. 2013;33(5):476–482. | ||
Vasilakis-Scaramozza C, Aschengrau A, Cabral HJ, Jick SS. Asthma drugs and the risk of congenital anomalies. Pharmacotherapy. 2013;33(4):363–368. | ||
Getz KD, Anderka MT, Werler MM, Jick SS. Maternal pre-pregnancy body mass index and autism spectrum disorder among offspring: a population-based case-control study. Paediatr Perinat Epidemiol. 2016;30(5):479–487. | ||
Hak E, Mulder B, Schuiling-Veninga CC, de Vries TW, Jick SS. Use of acid-suppressive drugs in pregnancy and the risk of childhood asthma: bidirectional crossover study using the general practice research database. Drug Saf. 2013;36(11):1097–1104. | ||
Black C, Kaye JA, Jick H. Relation of childhood gastrointestinal disorders to autism: nested case-control study using data from the UK General Practice Research Database. BMJ. 2002;325(7361):419–421. | ||
Fombonne E, Heavey L, Smeeth L, et al. Validation of the diagnosis of autism in general practitioner records. BMC Public Health. 2004;4:5–13. | ||
Hagberg KW, Jick SS. Validation of autism spectrum disorder diagnoses recorded in the Clinical Practice Research Datalink, 1990–2014. Clin Epidemiol. 2017;9:475–482. | ||
NICE Clinical Guideline [webpage on the Internet]. Depression in Adults: Recognition and Management. Available from: https://www.nice.org.uk/guidance/cg90. Accessed July 1, 2016. | ||
Chaste P, Leboyer M. Autism risk factors: genes, environment, and gene-environment interactions. Dialogues Clin Neurosci. 2012;14(3):281–292. | ||
Cross-Disorder Group of the Psychiatric Genomics Consortium. Identification of risk loci with shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet. 2013;381(9875):1371–1379. | ||
Rutter M. Incidence of autism spectrum disorders: changes over time and their meaning. Acta Paediatr. 2005;94(1):2–15. | ||
Mattila ML, Kielinen M, Linna SL, et al. Autism spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria: an epidemiological study. J Am Acad Child Adolesc Psychiatry. 2011;50(6):583–592. | ||
Kim YS, Leventhal BL, Koh YJ, et al. Prevalence of autism spectrum disorders in a total population sample. Am J Psychiatry. 2011;168(9):904–912. | ||
Grigoriadis S, Vonderporten EH, Mamisashvili L, et al. The impact of maternal depression during pregnancy on perinatal outcomes: a systematic review and meta-analysis. J Clin Psychiatry. 2013;74(4):321–341. |
Supplementary materials
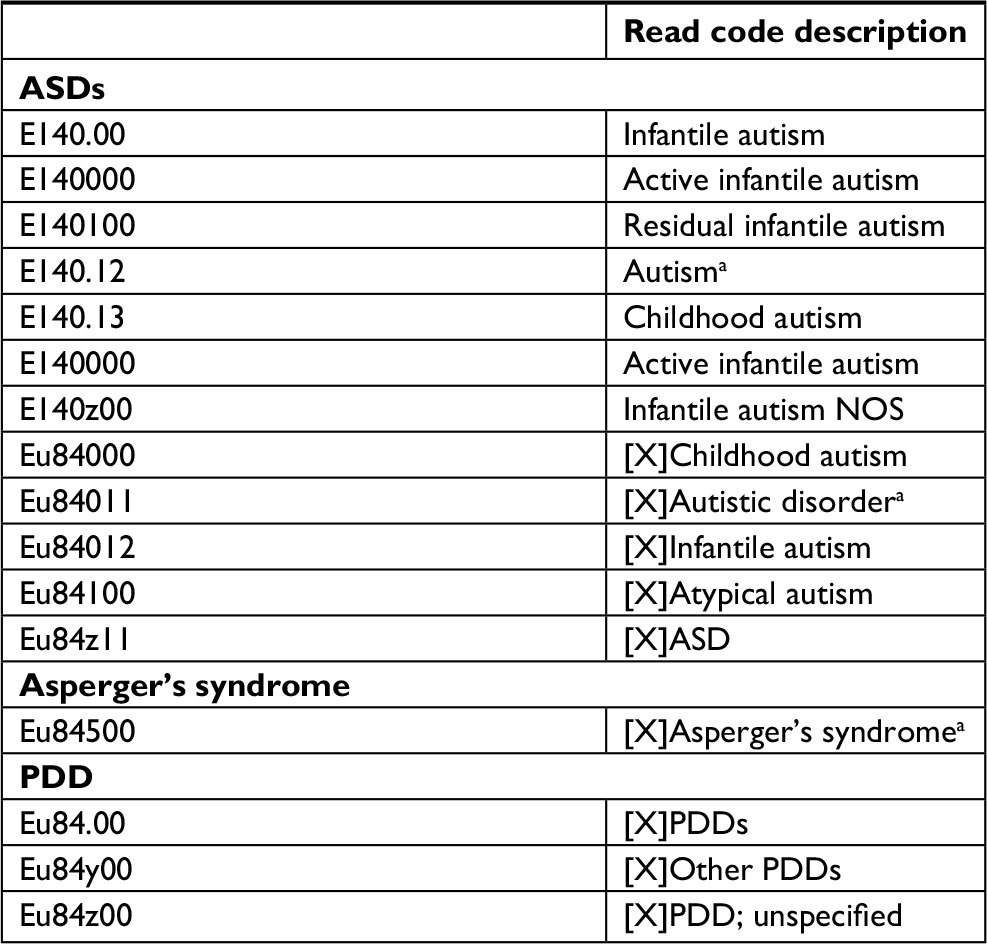 | Table S1 Read codes indicating ASDs Note: aIndicates Read codes most frequently used by GPs to indicate ASD in the CPRD. Abbreviations: ASD, autism spectrum disorder; CPRD, Clinical Practice Research Datalink; GPs, general practitioners; NOS, not otherwise specified; PDD, pervasive developmental disorder. |
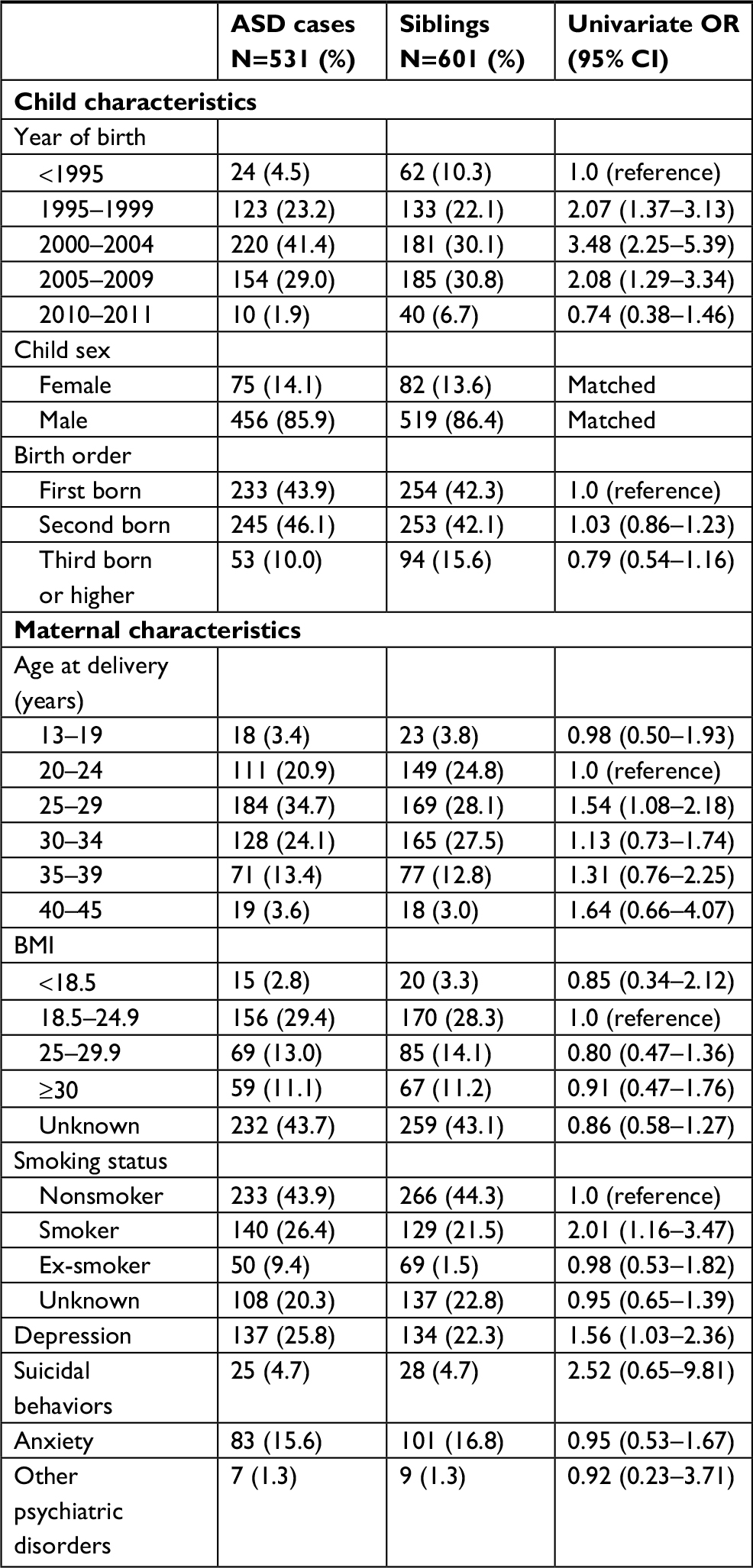 | Table S2 Sibling analysis: characteristics of ASD cases and same-sex siblings Abbreviation: BMI, body mass index. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.