Back to Archived Journals » Chronic Wound Care Management and Research » Volume 6
Martorell ulcer: chronic wound management and rehabilitation
Received 6 February 2019
Accepted for publication 26 June 2019
Published 23 July 2019 Volume 2019:6 Pages 83—88
DOI https://doi.org/10.2147/CWCMR.S172427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Marco Romanelli
Mark Mansour,1 Afsaneh Alavi2
1Schulich School of Medicine & Dentistry, Western University, London, Ontario, Canada; 2Division of Dermatology, Department of Medicine, Women’s College Hospital, University of Toronto, Toronto, Ontario, Canada
Abstract: Martorell hypertensive ischemic leg ulcers (HYTILU) are a rare lower extremity wound which exclusively occurs in patients with long-standing hypertension. Its pathophysiology is due to local skin infarctions caused by arteriolosclerosis of the dermis and subcutis. The differential diagnosis for a lower extremity wound is broad; however, Martorell HYTILU must primarily be distinguished from calciphylaxis and pyoderma gangrenosum. Diagnosis is accomplished by its clinical presentation, traditionally on the dorsolateral leg, its comorbidity with chronic arterial hypertension, and findings of arteriolosclerosis on histopathology. Given its rarity, there has been very little research conducted on interventions for its management and rehabilitation. Treatment primarily involves analgesia and surgical intervention usually with split-thickness skin grafting. The current review aims to summarize the current evidence on Martorell HYTILU and provide recommendations on its management.
Keywords: Martorell ulcer, hypertensive ischemic leg ulcer, atypical ulcer, wound healing
Introduction
Chronic wounds are a major public health concern associated with significant morbidity and mortality.1 Wounds of the lower extremities can be of hematologic, malignant, or infectious etiology, but are most commonly caused by peripheral arterial occlusive disease.
Martorell hypertensive ischemic leg ulcer (HYTILU) is a rare and likely under-recognized lower extremity wound characterized by progressive and painful necrotic ulceration. HYTILU was first described by Fernandes Martorell in a cohort of four obese, hypertensive women.2 Studies on Martorell HYTILU tend to be conducted in Europe due to the greater awareness of the disease compared to other regions of the world.3,4 Martorell HYTILU will likely become more prevalent due to the growing global prevalence of obesity and hypertension.
Martorell HYTILU classically presents in patients over the age of 50 with long-standing, often well-controlled, arterial hypertension. In modern case series, women and men are equally affected, although a female predominance was originally observed. Patients with Martorell HYTILU often have comorbid obesity and type II diabetes mellitus.4 Key clinical features include livedo reticularis and a necrotic wound occurring on either the dorsolateral surface of the leg or over the Achilles tendon. Approximately 50% of patients have bilateral involvement, sometimes occurring months to years apart.4 The lesion initially presents as dusky, painful plaque, often combined with a livedoid pattern on the surrounding skin (Figure 1). The ulcer has a characteristic necrotic base and violaceous border and it may be superficial or reach the entire depth of the subcutis.5 Characteristically the Martorell HYTILU is associated with excruciating pain that is out of proportion for the size of the ulcer. Martorell HYTILU is a disease of subcutaneous arterioles and is associated with increased local vascular resistance, hyperpulsality of leg arteries, and normal ankle-brachial index.6 Half of the patients present with peripheral arterial disease of the affected leg; however, Martorell HYTILU may also occur as an isolated skin infarction in the absence of any relevant atherosclerosis of thigh, popliteal or leg arteries. Martorell HYTILU has a tendency to spread rather than deepen as the arteriolosclerosis does not affect small vessels deeper than the subcutaneous fat. Diagnosis of Martorell HYTILU is usually made by a combination of its characteristic clinical presentation and the presence of arteriolosclerosis on histopathology.
 |
Figure 1 Martorell HYTILU on the dorsolateral leg. A shallow, well-demarcated ulceration with a violaceous border and areas of necrosis. |
Early recognition and prompt intervention are necessary to prevent unnecessary pain and suffering to the patient. Due to the under-recognition of the condition, there is a paucity of research on its management. The current review aims to summarize the currently described strategies in the English literature for the prevention, management, and rehabilitation of patients presenting with a Martorell HYTILU.
Diagnosis of Martorell HYTILU
The differential diagnosis for a lower extremity wound is vast and are most commonly associated with large arterial or venous disease. Ulceration due to peripheral arterial disease may be excluded via a vascular assessment, such as by Doppler ultrasound. However, half of HYTILU patients have concomitant peripheral arterial occlusive disease. Martorell HYTILU must be distinguished from pyoderma gangrenosum (PG), necrotizing vasculitis and calciphylaxis. Calciphylaxis in normal renal and parathyroid function (ie, eutrophication or non-uremic calciphylaxis) are probably related to HYTILU. Calciphylaxis is defined by the presence of end-stage kidney disease, and eutrophication by proximal (ie, central) skin infarctions without end-stage kidney disease. Differentiating Martorell HYTILU from these conditions is of the utmost importance as it delays the necessary treatment for Martorell HYTILU, and in some cases, the treatment for other conditions such as PG may exacerbate Martorell HYTILU.
To aid in the diagnosis, a deep incisional elliptical biopsy (5×0.5 cm) including all of the skin layers and subcutaneous fat across the necrotic area of the ulcer into normal skin may be performed.7 Key histopathologic characteristics are thickened arteriole walls with severe stenosis of arteriole lumens, arteriolar thrombosis, skin infarction, and medial calcinosis.7 The histologic characteristics of Martorell HYTILU are shared with calciphylaxis. It is not possible to distinguish the two diseases on histopathology alone, and what ultimately distinguishes these diseases is that renal impairment necessitates a diagnosis of calciphylaxis over Martorell HYTILU.
PG often has a similar clinical presentation to Martorell HYTILU due to its similar morphology and significant associated pain. In a cohort examined by Hafner et al, approximately 50% of all patients with a Martorell HYTILU were initially referred with suspected PG.4 Both diseases present similarly as a central necrotic ulcer with an inflammatory, violaceous border; however, the wound margin is not pustular in Martorell HYTILU.8 PG typically presents as liquefaction necrosis with a superficial moist appearance, whereas HYTILU presents as a black, dry infarction. A misdiagnosis of PG can occur due to an inadequate biopsy which may show dermal necrosis without subcutaneous arteriolosclerosis or medial calcification. In terms of location, Martorell HYTILU only occurs on the dorsolateral shin or Achilles’ tendon whereas PG may occur anywhere. The associated clinical features of Martorell HYTILU and PG also differ. By definition, all patients with Martorell HYTILU have hypertension and may have other cardiovascular comorbidities, whereas that is not necessarily the case in those with PG. In contrast, PG may be idiopathic or associated with inflammatory bowel disease, rheumatoid arthritis, or myeloid leukemia. Those with PG may present with neutrophilia or an elevated serum C-reactive protein.9 The treatment of the two diseases acts in opposition, as PG is responsive to systemic corticosteroids whereas Martorell HYTILU is not. In fact, treatment with systemic corticosteroids often exacerbates Martorell HYTILU and can result in local and septic infection. A combination of the presence of cardiovascular risk factors, the location of the ulcer, and a full thickness biopsy demonstrating arteriolosclerosis should favor a diagnosis of Martorell HYTILU over PG.
Martorell HYTILU shares a common histopathological and clinical picture to calciphylaxis and eutrophication, best described in a review paper by Hafner in 2016.8 Calciphylaxis has a varied initial morphology but generally presents with an erythematous or violaceous plaque with livedo or retiform purpura.10 In its late stages, it progresses to a necrotic ulcer with eschar or gangrene.10 The shared pathophysiology of calciphylaxis, eutrophication, and HYTILU is a localized skin infarction leading to tissue necrosis.8 Clinically, all share a similar pattern of skin infarctions and necrotizing livedo. On histopathology, all conditions have ischemia, subcutaneous arteriolosclerosis, hyperplasia of the arteriole wall musculature, and narrowed lumen diameter. In addition, all conditions share the same risk factors of arterial hypertension, diabetes mellitus, secondary or tertiary hyperparathyroidism in association with end-stage renal disease, and oral anticoagulation with vitamin K antagonists. Martorell HYTILU, calciphylaxis, and eutrophication are however distinguished based on their etiology. Calciphylaxis occurs in those with chronic renal disease or after kidney transplantation. Calciphylaxis may also be divided into distal and proximal (ie, central) forms, of which the distal form more clinically resembles Martorell HYTILU as it also occurs primarily on the dorsolateral leg and over the Achilles’ tendon. Meanwhile, the proximal form largely on the thigh, the abdomen, and breasts. Calciphylaxis is associated with acral gangrene, affecting largely the appendages and penis. Despite the highly similar presentation of Martorell HYTILU, calciphylaxis, and eutrophication, all these diseases largely follow the same treatment algorithm.
Management of Martorell HYTILU
The management of Martorell HYTILU is as follows: control of cardiovascular risk factors, cessation of vitamin K antagonists, analgesia, surgical debridement, and negative-pressure wound therapy. Early surgical management, as opposed to conservative treatment modalities, is ideal to promote wound healing and minimize severe, prolonged pain.3 The low incidence of Martorell HYTILU has prevented any large-scale trials of treatment options from being conducted, so most therapeutics have been exclusively studied in case reports and case series. A summary of the evidence is described in Table 1.
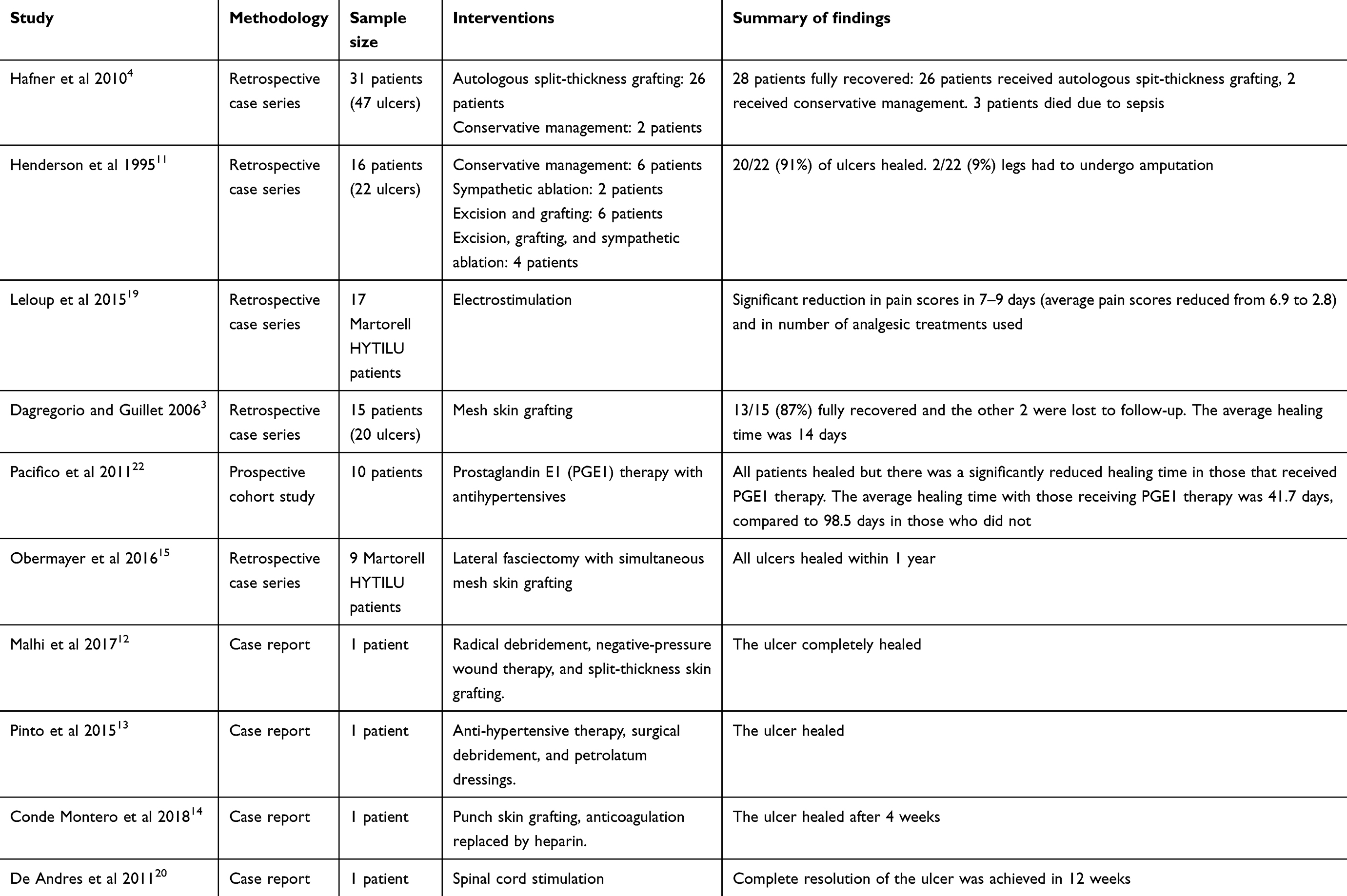 |
Table 1 Summary of interventions for martorell hypertensive ischemic leg ulcer |
Surgical management
Early surgical management is the most valuable definitive treatment for Martorell HYTILU. Ulcers >3 cm in diameter benefit from surgical debridement of necrotic tissue followed by split-thickness grafting. Smaller ulcers may heal on their own following debridement. A dramatic improvement in pain symptoms is usually seen following skin grafting and wounds usually heal completely within several weeks. Antibiotics are often needed since overt wound infection often occurs during the course of treatment, particularly in early during debridement and application of negative-pressure wound therapy.
Hafner et al described a successful surgical and wound-care protocol in 31 patients with Martorell HYTILU.4 Patients underwent bedside-debridement under local anesthesia or necrosectomy under local or general anesthesia. Negative-pressure wound therapy was used in 18 of the 31 patients, and 26 patients received autologous split-thickness skin grafts. Pain relief and complete resolution of the ulcers were seen in 28 patients.
Dagregorio and Guillet had shown efficacy in the usage of mesh split-thickness skin grafts as curative treatment of Martorell HYTILU in a retrospective series of 20 ulcers in 15 patients.3 A complete debridement of all necrotic tissue followed by mesh skin grafting under anesthesia was performed on all 15 patients. Split-thickness skin grafts within a dermatome were harvested and expanded to a 3:1 ratio with a mesher. After 1 week, there was a complete absence of pain in all patients and complete resolution of 14 of the 20 ulcers was seen after a mean hospital stay of 16 days.
Henderson et al reported resolution in 12 patients after wound excision and autologous skin grafting from the thigh.11 Four of these patients needed sympathectomy following surgery for pain management. Cases reported by Malhi et al and Lima Pinto et al also demonstrated full wound healing following surgical debridement to the fascia, split-thickness skin grafting, and/or negative-pressure wound therapy.12,13
For superficial forms of HYTILU, punch split-thickness grafts represent an elegant and technically less demanding solution. Conde Montero et al achieved complete wound healing 4 weeks after 4 and 6 mm punch split-thickness grafting under local anesthesia.14
For recalcitrant Martorell ulcers, a peroneal nerve-sparing lateral fasciectomy with simultaneous mesh split-thickness grafting may also be considered.15 The procedure described by Obermayer et al has been shown to completely heal all 9 legs treated within 1 year.
Control of cardiovascular risk factors
All patients with Martorell HYTILU have hypertension and a large majority have type 2 diabetes mellitus. A component of the pathophysiology of Martorell HYTILU is the combination of arteriolosclerosis and vasoconstriction. The hypertension is often longstanding, and patients usually have been taking antihypertensives for several years or decades. At presentation, patients may have a controlled or an elevated systolic arterial blood pressure (>180 mmHg). It is thought that Martorell HYTILU may be a late-stage complication of hypertension due to the advancements in antihypertensives, allowing patients to survive decades with the disease.11,16 Angiotensin-converting enzyme inhibitors and calcium channel blockers are appropriate choices for antihypertensive therapy in Martorell HYTILU due to the reduction in localized vasoconstriction.17,18 Management of hypertension with antihypertensive medication such as beta-blockers may also improve wound healing in these patients. Although there is no definitive research in this area, aggressive control of arterial blood pressure and serum glucose likely reduces the likelihood of developing or having a recurrence of Martorell HYTILU. Hypertensive peaks are often linked to excruciating pain in patients with active disease but this usually improves soon after the first skin graft. Blood pressure control during acute hypertensive disease is valuable for cardiovascular outcomes but probably does not influence the wound healing of HYTILU since the skin infarction is already established.
Analgesia
One of the distinguishing symptoms of Martorell HYTILU compared to other lower extremity ulcers is the presence of excruciating pain. Pain management is a necessary component of treatment to minimize the suffering associated with Martorell HYTILU. The ultimate goal of analgesia is to minimize the pain experienced by the patient while reducing the usage of opioids to avoid dependence. Generally, the most effective treatment of the pain associated with Martorell HYTILU is treatment of the ulcer itself through debridement and skin grafting.4 Patients usually experience a dramatic reduction in pain a few days post-operatively.7 In the series reported by Hafner et al, all patients reported an 8–10 on a visual analog pain scale (possible scores ranging from 0 to 10). Patients in that series were treated with NSAIDs, oral or transcutaneous morphine derivatives, tricyclic antidepressant agents, and pregabalin.4 Despite the wide variety of analgesia available, opioids are often necessary, but inadequate, for pain control.4,14
Although split-thickness skin grafting has been shown to be a definitive treatment for the pain experienced in Martorell HYTILU, some patients may not be suitable candidates for the procedure. This may either be due to the presence of comorbidities which do not make the patient appropriate for surgery, a lack of viable skin, or an inappropriate wound bed to place the graft on. In these cases, other forms of analgesia may be used instead. The use of electrostimulation for pain relief has been investigated in a single retrospective study by Leloup et al on a cohort of 73 patients with leg ulcers of varied etiologies, 17 of which had Martorell HYTILU.19 Electrostimulation is believed to encourage wound healing by promoting angiogenesis, physiologic wound debridement, and granulation by restoring the skin’s electric field. The dressing is worn for 2–3 days at a time and electro stimulations are conducted for 20–30 mins twice a day for at least 7 days. In the 17 patients with Martorell HYTILU, a statistically significant reduction in numerical pain ratings by the end of the treatment period was observed. Electrostimulation was well-tolerated and a small but significant reduction in the usage of morphine derivatives for analgesia was found. A single case report of the usage of a spinal cord stimulator for analgesia has been reported.20 Spinal cord stimulation works by reducing efferent sympathetic activity, thereby preventing vasoconstriction of peripheral arterioles. As the pathophysiology of Martorell HYTILU results in a stenosis of arterioles, reducing peripheral vasoconstriction provides a pain-relieving effect. Generally, spinal cord stimulation has been shown to be a safe and effective option for analgesia in peripheral vascular disease.21 Complete resolution of the ulcer and pain symptoms was achieved by 12 weeks.
Conclusion
Martorell HYTILU is a challenging diagnosis best made through a combination of the clinical presentation and histopathology. Patients with chronic hypertension without renal impairment presenting with a necrotic ulcer of the dorsolateral shin should have Martorell HYTILU considered on the differential diagnosis. A deep elliptical biopsy showing skin infarction and subcutaneous arteriolosclerosis is diagnostic of Martorell HYTILU. Management should be focused on optimizing antihypertensive therapy, analgesia, and debridement with split-thickness skin grafting. Surgical management is the definitive treatment for Martorell HYTILU and should occur promptly to minimize spread of the ulcer and unnecessary pain to the patient.
Disclosure
AA has acted as a consultant/advisor and has received grants and personal fees from AbbVie; and personal fees from Galderma, Janssen, LEO Pharma, Novartis and Valeant, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763–771. doi:10.1111/wrr.2009.17.issue-6
2. Martorell F. Las ulceras supramaleolares por arteriolitis de las grandes hipertensas. Actas (Reun Cientif Cuerpo Facul) Inst Policlinico Barcelona. 1945;1:6–9.
3. Dagregorio G, Guillet G. A retrospective review of 20 hypertensive leg ulcers treated with mesh skin grafts. J Eur Acad Dermatol Venereol. 2006;20:166–169. doi:10.1111/j.1468-3083.2006.01399.x
4. Hafner J, Nobbe S, Partsch H, et al. Martorell hypertensive ischemic leg ulcer: a model of ischemic subcutaneous arteriolosclerosis. Arch Dermatol. 2010;146:961–968. doi:10.1001/archdermatol.2010.156
5. Vuerstaek JD, Reeder SW, Henquet CJ, Neumann HA. Arteriolosclerotic ulcer of martorell. J Eur Acad Dermatol Venereol. 2010;24:867–874. doi:10.1111/j.1468-3083.2009.03553.x
6. Duncan HJ, Faris IB. Martorell’s hypertensive ischemic leg ulcers are secondary to an increase in the local vascular resistance. J Vasc Surg. 1985;2:581–584. doi:10.1016/0741-5214(85)90013-8
7. Alavi A, Mayer D, Hafner J, Sibbald RG. Martorell hypertensive ischemic leg ulcer: an underdiagnosed entity. Adv Skin Wound Care. 2012;25:563–572. doi:10.1097/01.ASW.0000423442.08531.fb
8. Hafner J. Calciphylaxis and martorell hypertensive ischemic leg ulcer: same pattern – one pathophysiology. Dermatology. 2016;232:523–533. doi:10.1159/000448245
9. Kolios AGA, Hafner J, Luder C, et al. Comparison of pyoderma gangrenosum and martorell hypertensive ischaemic leg ulcer in a swiss cohort. Br J Dermatol. 2018;178:e125–e126. doi:10.1111/bjd.15901
10. Nigwekar SU, Thadhani R, Brandenburg VM. Calciphylaxis. N Engl J Med. 2018;378(18):1704–1714. doi:10.1056/NEJMc1711583
11. Henderson CA, Highet AS, Lane SA, Hall R. Arterial hypertension causing leg ulcers. Clin Exp Dermatol. 1995;20:107–114. doi:10.1111/j.1365-2230.1995.tb02666.x
12. Malhi HK, Didan A, Ponosh S, Kumarasinghe SP. Painful leg ulceration in a poorly controlled hypertensive patient: a case report of martorell ulcer. Case Rep Dermatol. 2017;9:95–102. doi:10.1159/000468977
13. Lima Pinto AP, Silva NA
14. Conde Montero E, Guisado Muñoz S, Pérez Jerónimo L, Peral Vazquez A, Montoro Lopez JJ. Martorell hypertensive ischemic ulcer successfully treated with punch skin grafting. Wounds. 2018;30:E9–E12.
15. Obermayer A, Maier A, Zacherl J, Hitzl W, Steinbacher F. Lateral fascietomy sparing the superficial peroneal nerve with simultaneous mash graft in non-healing lateral leg ulcers of diverse vascular origins: surgical technique, short- and long-term results from 44 legs. Eur J Vasc Endovasc Surg. 2016;42:225–232. doi:10.1016/j.ejvs.2016.02.023
16. Fogola N, Pataro EF, Zerbos FC, Acrich MW. Hypertensive ulcer. J Cardiovasc Surg. 1971;12:406–410.
17. Graves JW, Morris JC, Sheps SG. Martorell’s hypertensive leg ulcer: case report and concise review of the literature. J Hum Hypertens. 2001;15:279–283. doi:10.1038/sj.jhh.1001154
18. Nikolova K. Treatment of hypertensive venous leg ulcers with nifedipine. Meth Find Exp Clin Pharmacol. 1995;17:545–549.
19. Leloup P, Toussaint P, Lembelembe JP, Celerier P, Maillard H. The analgesic effect of electrostimulation (WouldEL®) in the treatment of leg ulcers. Int Wound J. 2015;12:706–709. doi:10.1111/iwj.12211
20. De Andres J, Villanueva VL, Mazzinari G, Fabregat G, Asensio JM, Monsalve V. Use of a spinal cord stimulator for treatment of martorell hypertensive ulcer. Reg Anesth Pain Med. 2011;36:83–86. doi:10.1097/AAP.0b013e31820308b2
21. Cameron T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: a 20-year literature review. J Neurosurg. 2004;100:254–267.
22. Pacifico F, Acernese CA, Di Giacomo A. PGE(1) therapy for martorell’s ulcer. Int Wound J. 2011;8:140–144. doi:10.1111/j.1742-481X.2010.00760.x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.